hypertension -complications and social impact hypertension -complications and social impact dr. ho...
TRANSCRIPT

1
Hypertension Hypertension -- Complications Complications and Social Impactand Social Impact
Dr. Ho Hung Kwong, Duncan 何鴻光何鴻光何鴻光何鴻光MBBS(HK), MRCP(UK),
FHKAM(Med), FHKCP, FRCP(Edin)FAHA, FSCAI
Specialist in Cardiology
Definition and classification of Definition and classification of hypertension: JNC VIIhypertension: JNC VII
Hypertension is defined as blood pressure ≥140/90 mmHg
or ≥100≥160Stage 2 hypertension
or 90-99140-159Stage 1 hypertension
or 80-89120-139Prehypertension
and <80<120Normal
Diastolic
(mmHg)
Systolic
(mmHg)
Category
JNC VII. JAMA 2003;289:2560-2572

2
Prevalence of HypertensionPrevalence of Hypertension
Prevalence of hypertension*: Prevalence of hypertension*: North America and EuropeNorth America and Europe
0
10
20
30
40
50
60
70
80
United
Sta
tes
Canad
a
Europ
eIta
ly
Sweden
Englan
dSpa
in
Finlan
d
Germ
any
Pre
vale
nce
(%)
MenWomenTotal
Wolf-Maier K, et al. JAMA 2003;289:2363-2369* BP ≥140/90 mmHg or treatment with antihypertensive medication

3
Prevalence of hypertension: AsiaPrevalence of hypertension: Asia
01020304050607080
China
(200
0/20
01)
Taiwan
(199
4)
Hong K
ong
(199
7)
Singap
ore
(199
8)
Mala
ysia
(199
6)
Thaila
nd (1
991)
Philipp
ines
(199
9)
Indo
nesia
(199
4)
India
(Mum
bai, 1
999)
Japa
n (19
92-9
5)
Pre
vale
nce
(%)
Men
Women
Total
Gu DF, et al. Hypertension 2002;40:920-927; Singh RB, et al. J Hum Hypertens 2000;14:749-763; Janus ED. Clin Exp Pharmacol Physiol1997;24:987-988; National Health Survey 1998, Singap ore. Epidemiology and Disease Department, Ministry of Health, Singapore.; Lim TO, et al.
Singapore Med J 2004;45:20-27; Tatsanavivat P, et al. Int J Epidemiol 1998;27:405-409; Muhilal H. Asia Pacific J Clin Nutr 1996;5:132-134; Gupta R. J Hum Hypertens 2004;18:73-78; Asai Y, et al. Nippon Koshu Eisei Zasshi 2001;48:827-836 [in Japanese]
Hypertension control rates around the worldHypertension control rates around the world
<140/90 mmHg (%)United States 27France 24Canada 22Italy 9Egypt 8England 6Korea 5China 3Poland 2
<160/95 mmHg (%)Germany 23Finland 21Spain 20Australia 19Scotland 18India 9Zaire 3
JNC VI. Arch Intern Med 1997;157:2413-2446; Joffres MR, et al. Am J Hypertens 1997;10:1097-1102; Colhoun HM, et al. J Hypertens 1998;16:747-752; Chamotin B, et al. Am J Hypertens 1998;11:759-762;
Marques-Vidal P, et al. J Hum Hypertens 1997;11:213-220

4
National Health and Nutrition National Health and Nutrition Examination Survey (NHANES) Examination Survey (NHANES)
34%27%29%10%Control†
59%54%55%31%Treatment
70%68%73%51%Awareness
1999-2000
III
(Phase 2 1991-94)
III
(Phase 1 1988-91)
II
(1976-80)
Trends in awareness, treatment and control of high blood pressure in adults aged 18-74*
* High blood pressure * High blood pressure defined asdefined as SBP ≥140 mmHg or SBP ≥140 mmHg or DBP ≥90 mmHg or takingDBP ≥90 mmHg or taking antihypertensiveantihypertensive medicationmedication† SBP <140 mmHg and DBP <90 mmHg† SBP <140 mmHg and DBP <90 mmHg
Unpublished data for 1999Unpublished data for 1999 ––2000 compiled by M. 2000 compiled by M. WolzWolz , , National Heart, Lung and Blood Institute: JNC VINational Heart, Lung and Blood Institute: JNC VI
At-a-Glance Summary TablesMales and Cardiovascular Diseases
Heart Disease and Stroke Statistics – 2006 Update, American Heart Association

5
Impact of HypertensionImpact of Hypertension
Millimetres matter …Millimetres matter …
“A 2“A 2 --mmHg reduction in DBP would mmHg reduction in DBP would
result in … a 6% reduction in the risk of result in … a 6% reduction in the risk of
CHD and a 15% reduction in the risk of CHD and a 15% reduction in the risk of
stroke and stroke and TIAsTIAs ””
Cook NR, et al. Arch Intern Med 1995;155:701-709DBP, diastolic blood pressure; CHD, coronary heart disease; DBP, diastolic blood pressure; CHD, coronary heart disease; TIA, transient TIA, transient ischaemicischaemic attackattack

6
Millimetres matter …Millimetres matter …
“For individuals 40“For individuals 40 --70 years of age, each 70 years of age, each
increment of 20 mmHg in systolic BP or increment of 20 mmHg in systolic BP or
10 mmHg in diastolic BP doubles the risk 10 mmHg in diastolic BP doubles the risk
of CVD across the entire BP range from of CVD across the entire BP range from
115/75 to 185/115 mmHg”115/75 to 185/115 mmHg”
JNC VII. JAMA 2003;289:2560-2572BP, blood pressure; CVD, cardiovascular diseaseBP, blood pressure; CVD, cardiovascular disease
Hypertension: A risk factor for Hypertension: A risk factor for cardiovascular diseasecardiovascular disease
9.5
3.3 2.45.0
2.03.5 2.1
45.5
21.3
12.4
6.2
9.97.3
13.9
6.3
22.7
0
5
10
15
20
25
30
35
40
45
50
Men Women Men Women Men Women Men Women
Bie
nnia
l age
-adj
uste
d ra
te
per
1,00
0 su
bjec
ts NormotensiveHypertensive
Coronarydisease
Stroke Peripheral arterydisease
Cardiacfailure
Kannel WB. JAMA 1996;275:1571-1576
Risk ratio: 2.0 2.2 3.8 2.6 2.0 3.7 4.0 3.0

7
EndEnd --Stage Renal Disease (ERSD)Stage Renal Disease (ERSD)
ESRD (also called end-stage kidney disease) is a condition closely related to high blood pressure, and occurs when the kidneys can no longer function normally on their own.
• The incidence of reported ESRD has almost doubled in the past 10 years. (NHLBI, from usrds.org Web site)
• 82,588 patients died from ESRD in 2003.• Diabetes continues to be the most common
reported cause of ESRD.
AtherosclerosisAtherosclerosis

8
Other Related DiseaseOther Related Disease
Relative importance of SBP and DBP as Relative importance of SBP and DBP as predictors of CHD risk as a function of agepredictors of CHD risk as a function of age
* The difference between SBP and DBP proportional hazard regression coefficients, ie, β(SBP) - β(DBP), was estimated for each age group
SBP, systolic blood pressure; DBP, diastolic blood pressure;CHD, coronary heart disease
25 6545 5535 75
β(SBP) -
β(DBP)*
Age (years)
Favours DBP
Favours SBP
-1.0
-0.5
0.0
0.5
1.0
-1.5
p=0.008
Franklin SS, et al. Circulation 2001;103:1245-1249

9
Impact of highImpact of high --normal BP on CV risknormal BP on CV risk
Optimal BP: <120/80 mmHg; normal BP: 120-129/80-84 mmHg; high-normal BP: 130-139/85-89 mmHg
BP, blood pressure; CV, cardiovascular
Cumulative incidence of CV events
(%)
16
121086420
14
Optimal BP
Normal BP
121086420
0 2 4 6 8 10 12Years
Optimal BP
Normal BP
High-normal BPWomen
Men
Cumulative incidence of CV events
(%)
High-normal BP
Vasan RS, et al. N Engl J Med 2001;345:1291-1297
Implications of small reductions in DBPImplications of small reductions in DBPfor primary preventionfor primary prevention
DBP, diastolic blood pressure; CHD, coronary heart disease
-21
-16
-6
-46
-38
-15
-50
-40
-30
-20
-10
07.5 mmHg 5-6 mmHg 2 mmHg
CHDStroke
Ris
k re
duct
ion
(%)
DBP reduction
Cook NR, et al. Arch Intern Med 1995;155:701-709

10
Hypertension Treatment GuidelinesHypertension Treatment Guidelines
Treatment initiation: JNC VIITreatment initiation: JNC VII
Drug(s) for compelling indications; other antihypertensive drugs
(diuretics, ACE-I, ARB, BB, CCB) as needed
Thiazide-type diuretics for most;
may consider ACE-I, ARB, BB,
CCB, or combination
Yes
Stage 1 hypertension
Drug(s) for compelling indications
No antihypertensive drug indicated
Encourage
Normal
Yes
Pre-hypertension
YesLifestyle modification
With compelling indications
Two-drug combination for most (usually thiazide-type diuretic and
ACE-I or ARB or BB or CCB)
Without compelling indication
Initial drug therapy
Stage 2 hypertension
ACE-I, angiotensin-converting enzyme inhibitor; ARB, angiotensin II receptor blocker; BB, beta-blocker; CCB, calcium-channel blocker JNC VII. JAMA 2003;289:2560-2572

11
Goals of treatment: JNC VIIGoals of treatment: JNC VII
• The SBP and DBP targets are <140/90 mmHg
• The primary focus should be on achieving the SBP goal
• In patients with hypertension and diabetes or renal disease, the BP goal is <130/80 mmHg
JNC VII. JAMA 2003;289:2560-2572SBP, systolic blood pressure; DBP, diastolic blood pressure; BP, blood pressure
Treatment initiation: ESH/ESC 2003Treatment initiation: ESH/ESC 2003Blood pressure
Immediate drug treatment and lifestyle changes
Immediate drug treatment and lifestyle changes
Immediate drug treatment and lifestyle changes
Immediate drug treatment and lifestyle changes
Drug treatment and lifestyle changes
Associated clinical conditions
Immediate drug treatment and lifestyle changes
Drug treatment and lifestyle changes
Drug treatment and lifestyle changes
Drug treatment and lifestyle changes
Lifestyle changes
3 or more risk factors, target organ damage, or diabetes
Immediate drug treatment and lifestyle changes
Lifestyle changes for several months, then drug treatment
Lifestyle changes for several months, then drug treatment
Lifestyle changes
Lifestyle changes
1-2 risk factors
Immediate drug treatment and lifestyle changes
Lifestyle changes for several months, then drug treatment
Lifestyle changes for several months, then drug treatment if preferred by the patient and resources available
No BP intervention
No BP intervention
No other risk factors
Grade 3Grade 2Grade 1High normalNormalOther risk factors and disease history
ESH/ESC Guidelines 2003. J Hypertens 2003;21:1011-1053

12
Goals of treatment: ESH/ESC 2003Goals of treatment: ESH/ESC 2003
• Achieve maximum reduction in long term total cardiovascular risk
• Treat all reversible risk factors and associated clinical conditions in addition to treating raised blood pressure
• Target blood pressure <140/90 mmHg and to lower values, if tolerated
• For diabetics, target blood pressure is <130/80 mmHg
ESH/ESC Guidelines 2003. J Hypertens 2003;21:1011-1053
Hypertension treatment strategy: Hypertension treatment strategy: ESH/ESC 2003ESH/ESC 2003
Consider:Untreated BP level
Presence or absence of TOD and risk factors
Choose between:
Single agentat low dose
Two-drug combinationat low dose
If goal BP not achieved
Previous agent at full dose
Switch to differentagent at low dose
Previous combination at full dose
Add a third drug at low dose
Three-drug combination at effective doses
Two- to three-drug combination
Full-dosemonotherapy
If goal BP not achieved
BP, blood pressure; TOD, target organ damage ESH/ESC Guidelines 2003. J Hypertens 2003;21:1011-1053
13
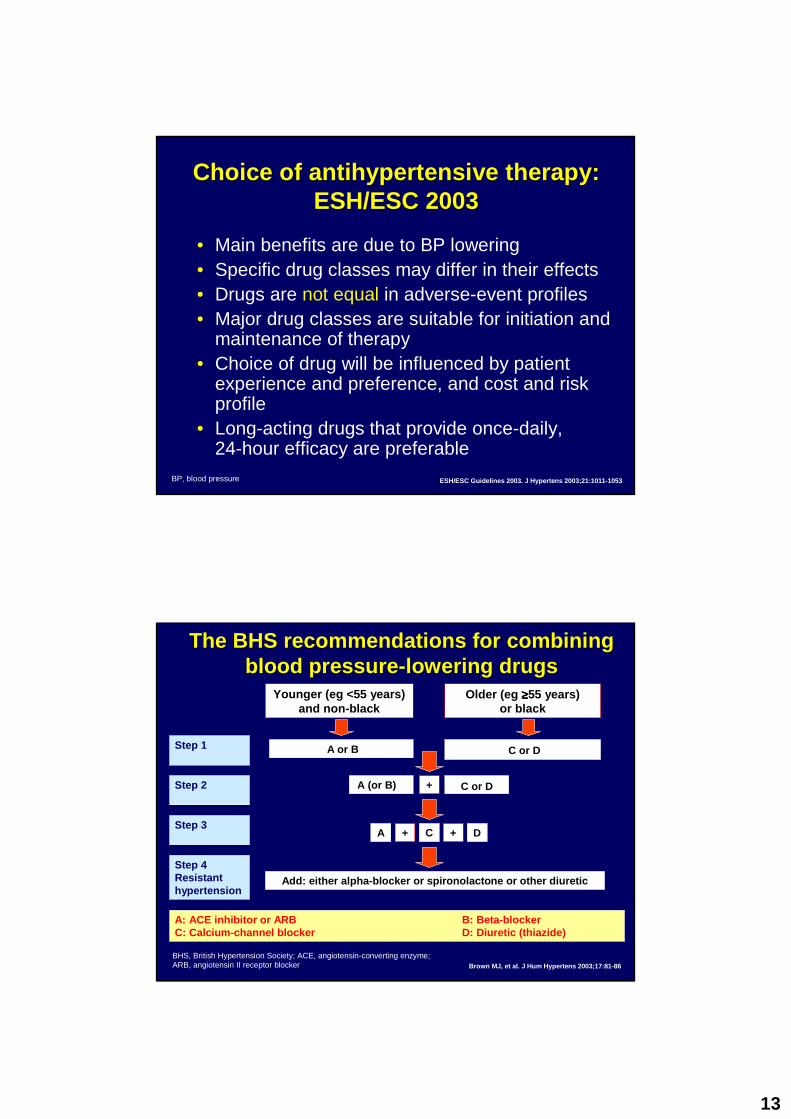
Choice of Choice of antihypertensiveantihypertensive therapy:therapy:ESH/ESC 2003ESH/ESC 2003
• Main benefits are due to BP lowering• Specific drug classes may differ in their effects• Drugs are not equal in adverse-event profiles• Major drug classes are suitable for initiation and
maintenance of therapy• Choice of drug will be influenced by patient
experience and preference, and cost and risk profile
• Long-acting drugs that provide once-daily, 24-hour efficacy are preferable
ESH/ESC Guidelines 2003. J Hypertens 2003;21:1011-1053BP, blood pressure
Younger (eg <55 years)and non-black
Older (eg ≥≥≥≥55 years) or black
Step 1
Step 2
Step 3
Step 4Resistant hypertension
Add: either alpha-blocker or spironolactone or other diuretic
A: ACE inhibitor or ARB B: Beta-blockerC: Calcium-channel blocker D: Diuretic (thiazide)
A (or B)
A
A or B C or D
C or D+
+C D
Brown MJ, et al. J Hum Hypertens 2003;17:81-86
The BHS recommendations for combining The BHS recommendations for combining blood pressureblood pressure --lowering drugslowering drugs
+
BHS, British Hypertension Society; ACE, angiotensin-converting enzyme; ARB, angiotensin II receptor blocker

14
Putting Hypertension Guidelines into Putting Hypertension Guidelines into Clinical PracticeClinical Practice
B.Dahlof (Co-chair), P.Sever (Co-chair), N. Poulter (Secr etary) H. Wedel (Statistician), G. Beevers, M. Caulfield, R. Co llins
S. Kjeldsen, A. Kristinsson, J. Mehlsen, G. McInnes, M. Nieminen E. O’Brien, J. Östergren, on behalf of the ASCOT Inv estigators
A randomised controlled trial of the prevention of CHD and other vascular events by BP and
cholesterol lowering in a factorial study design
ASCOT-BPLA, LANCET, vol 366 September 10, 2005

15
AngloAnglo --Scandinavian Cardiac Scandinavian Cardiac Outcome Trial (ASCOT)Outcome Trial (ASCOT)
1. This Trial had to be stopped earlier than expected due to significant reductions in cardiovascular death and all cause mortality in patients taking CCB – based regimen (amlodipine besylate) versus a standard Beta blocker based regimen.
2. In addition, they were less likely to develop diabetes compared to patients taking the Beta blocker-based regimen.
ASCOT-BPLA, LANCET, vol 366 September 10, 2005
Study designStudy design
atenolol ±bendroflumethiazide
amlodipine ±perindopril
19,257hypertensive
patients
PROBE design
ASCOT-BPLA
Investigator-led, multinational randomised controlled trial
placeboatorvastatin 10 mg Double-blind
ASCOT-LLA10,305 patients
TC ≤ 6.5 mmol/L (250 mg/dL)
ASCOT-BPLA, LANCET, vol 366 September 10, 2005

16
Treatment algorithm to BP targets < 140/90 mm Hgor < 130/80 mm Hg in patients with diabetes
amlodipine 5-10 mg atenolol 50-100 mg
perindopril 4-8 mgbendroflumethiazide-K
1.25-2.5 mg
doxazosin GITS 4-8 mg
add
add add
additional drugs, eg, moxonidine/spironolactone
add
ASCOT-BPLA, LANCET, vol 366 September 10, 2005
Mean proportion of time on Mean proportion of time on antihypertensiveantihypertensivemedication by treatment groupmedication by treatment group
Randomised to Atenolol
Randomised to Amlodipine
All Study
54.9Atenolol + bendroflumethiazide (+/- others)
65.7Bendroflumethiazide (+/- others)
79.4Atenolol (+/- others)
49.5Amlodipine + perindopril (+/- others)
58.5Perindopril (+/- others)
82.5Amlodipine (+/- others)
ASCOT-BPLA, LANCET, vol 366 September 10, 2005

17
Systolic and diastolic blood pressureSystolic and diastolic blood pressurem
m H
g
60
80
100
120
140
160
180
Time (years)
Baseline 0.5 1 1.5 2 2.5 3 3.5 4 4.5 5 5.5
atenolol ± thiazideamlodipine ± perindopril
137.7
136.1
79.2
77.4
Mean difference 1.9mmHg
Last visit
Mean difference 2.7mmHg
SBP
DBP
163.9
164.1
94.8
94.5
ASCOT-BPLA, LANCET, vol 366 September 10, 2005
Data safety monitoring board Data safety monitoring board (DSMB)(DSMB)
In October 2004 the DSMB recommended that the BP
arm of ASCOT should be stopped on account of
concerns that those patients receiving atenolol ±thiazide would continue to be disadvantaged compared with the comparator group
The Steering Committee endorsed the
recommendation of the DSMB, and trial closure began Dec, 2004 and ended June 2005.

18
CV mortalityCV mortality
Number at riskAmlodipine ± perindopril 9639 9544 9441 9322 9167 8078Atenolol ± thiazide 9618 9532 9415 9261 9085 7975
0.0 1.0 2.0 3.0 4.0 5.0 Years0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
Amlodipine ±±±± perindopril(No. of events 263)
Atenolol ±±±± thiazide(No. of events 342)
HR = 0.76 (0.65-0.90)p = 0.0010
%
AllAll --cause mortality cause mortality
Number at riskAmlodipine ± perindopril 9639 9544 9441 9332 9167 8078Atenolol ± thiazide 9618 9532 9415 9261 9085 7975
%
0.0 1.0 2.0 3.0 4.0 5.0 Years0.0
2.0
4.0
6.0
8.0
10.0
HR = 0.89 (0.81-0.99)p = 0.0247
Amlodipine ±±±± perindopril(No. of events 738)
Atenolol ±±±± thiazide(No. of events 820)

19
NewNew--onset diabetes mellitus onset diabetes mellitus
Number at riskAmlodipine ± perindopril 9639 9383 9165 8966 8726 7618Atenolol ± thiazide 9618 9295 9014 8735 8455 7319
0.0 1.0 2.0 3.0 4.0 5.0 Years0.0
2.0
4.0
6.0
8.0
10.0
Amlodipine ±±±± perindopril(No. of events = 567)
Atenolol ±±±± thiazide(No. of events = 799)
HR = 0.70 (0.63-0.78)p < 0.0001
%
Primary end point + coronaryrevascularisation procedures
Number at riskAmlodipine ± perindopril 9639 9458 9288 9086 8857 7732Atenolol ± thiazide 9618 9447 9236 8986 8719 7590
%
0.0 1.0 2.0 3.0 4.0 5.0 Years
0.0
1.0
2.0
3.0
4.0
5.0
6.0
7.0
HR = 0.86 (0.77-0.96)p = 0.0058
Atenolol ±±±± thiazide(No. of events 688)
Amlodipine ±±±± perindopril(No. of events 596)
8.0

20
Number at riskAmlodipine ± perindopril 9639 9400 9204 8984 8744 7614Atenolol ± thiazide 9618 9373 9136 8864 8591 7470
Total coronary end point Total coronary end point
Years0.0 1.0 2.0 3.0 4.0 5.0
0.0
2.0
4.0
6.0
8.0
10.0
Amlodipine ±±±± perindopril(No. of events 753)
Atenolol ±±±± thiazide(No. of events 852)
HR = 0.87 (0.79-0.96)p = 0.0070
%
Fatal and nonFatal and non --fatal stroke fatal stroke
Number at riskAmlodipine ± perindopril 9639 9483 9331 9156 8972 7863Atenolol ± thiazide 9618 9461 9274 9059 8843 7720
0.0 1.0 2.0 3.0 4.0 5.0 Years0.0
1.0
2.0
3.0
4.0
5.0
Amlodipine ±±±± perindopril(No. of events 327)
Atenolol ±±±± thiazide(No. of events 422)
HR = 0.77 (0.66-0.89)p = 0.0003
%
21
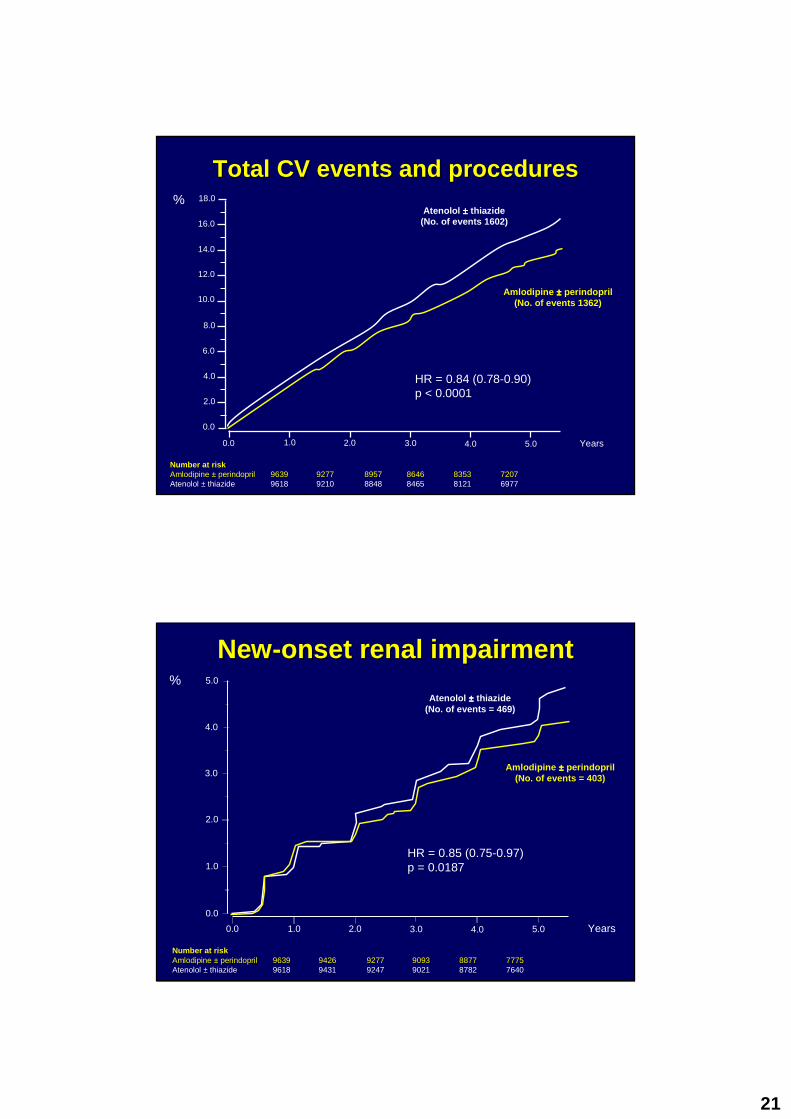
Total CV events and proceduresTotal CV events and procedures
Number at riskAmlodipine ± perindopril 9639 9277 8957 8646 8353 7207Atenolol ± thiazide 9618 9210 8848 8465 8121 6977
0.0 1.0 2.0 3.0 4.0 5.0 Years
0.0
2.0
4.0
6.0
8.0
10.0
12.0
14.0
16.0
18.0
Amlodipine ±±±± perindopril(No. of events 1362)
Atenolol ±±±± thiazide(No. of events 1602)
HR = 0.84 (0.78-0.90)p < 0.0001
%
NewNew--onset renal impairmentonset renal impairment
Number at riskAmlodipine ± perindopril 9639 9426 9277 9093 8877 7775Atenolol ± thiazide 9618 9431 9247 9021 8782 7640
HR = 0.85 (0.75-0.97)p = 0.0187
0.0 1.0 2.0 3.0 4.0 5.0 Years
0.0
1.0
3.0
4.0
5.0%
2.0
Amlodipine ±±±± perindopril(No. of events = 403)
Atenolol ±±±± thiazide(No. of events = 469)

22
Summary of all end pointsSummary of all end points
The area of the blue square is proportional to the amount of statistical information
Amlodipine ±±±± perindopril better Atenolol ±±±± thiazide better0.50 0.70 1.00 1.45
PrimaryNon-fatal MI (incl silent) + fatal CHD
SecondaryNon-fatal MI (exc. Silent) +fatal CHDTotal coronary end pointTotal CV event and proceduresAll-cause mortalityCardiovascular mortalityFatal and non-fatal strokeFatal and non-fatal heart failure
TertiarySilent MIUnstable anginaChronic stable anginaPeripheral arterial diseaseLife-threatening arrhythmiasNew-onset diabetes mellitusNew-onset renal impairment
Post hocPrimary end point + coronary revasc procsCV death + MI + stroke
2.00
Unadjusted Hazard ratio (95% CI)
0.90 (0.79-1.02)
0.87 (0.76-1.00)0.87 (0.79-0.96)0.84 (0.78-0.90)0.89 (0.81-0.99)0.76 (0.65-0.90)0.77 (0.66-0.89)0.84 (0.66-1.05)
1.27 (0.80-2.00)0.68 (0.51-0.92)0.98 (0.81-1.19)0.65 (0.52-0.81)1.07 (0.62-1.85)0.70 (0.63-.078)0.85 (0.75-0.97)
0.86 (0.77-0.96)0.84 (0.76-0.92)
ASCOT-BPLA, LANCET, vol 366 September 10, 2005
ConclusionsConclusions• Amlodipine ± perindopril based therapy confers an advantage
over atenolol ± thiazide based therapy on all major CV end points, all-cause mortality and new-onset diabetes
• Irrespective of the reasons for benefit, the amlodipine ±perindopril regimen should be preferred to the standard regimen of atenolol ± thiazide for most patients with hypertension
• Compared with standard antihypertensive therapy without statintherapy, the amlodipine ± perindopril regimen plus atorvastatinreduced coronary and stroke events by almost 50%
ASCOT-BPLA, LANCET, vol 366 September 10, 2005

23
ASCOTASCOT--BPLABPLA
Implications on Hypertension Implications on Hypertension GuidelinesGuidelines
NICE Guideline 2006NICE Guideline 2006

24
Pharmacological interventionsPharmacological interventions• Drug therapy reduces the risk of cardiovascular disease
and death. Offer drug therapy to: – patients with persistent high blood pressure of 160/100
mmHg or more– patients at raised cardiovascular risk (10-year risk of
CVD of 20% or more or existing CVD or target organ damage) with persistent blood pressure of more than 140/90 mmHg.
Pharmacological interventionsPharmacological interventions
• In hypertensive patients aged 55 or older or black patients of any age, the first choice for initial therapy should be either a calcium-channel blocker or a thiazide-type diuretic . For this recommendation, black patients are considered to be those of African or Caribbean descent, not mixed-race, Asian or Chinese.

25
Pharmacological interventionsPharmacological interventions
• In hypertensive patients younger than 55 , the first choice for initial therapy should be an angiotensin-converting enzyme (ACE) inhibitor (or an angiotensin-II recept or antagonist if an ACE inhibitor is not tolerated).
General issues when prescribing
• Offer patients with isolated systolic hypertension (systolic blood pressure more than 160 mmHg) the same treatment as patients with both raised systolic and diastolic blood pressure.
• Offer patients older than 80 years the same treatment as other patients aged 55 or older – take account of any co-morbidity and other drugs they are taking.
26
General issues when prescribing
• Prescribe drugs taken only once a day if possible.
• Prescribe non-proprietary drugs if these are appropriate and minimise cost.
• Give information about the benefits and side effects of drugs so that patients can make informed choices.
Drug treatmentDrug treatment
Key issues in updating the recommendations
• Beta-blockers : In head-to-head trials, beta-blockers were usually less effective than a comparator drug at reducing major cardiovascular events, particularly stroke. Beta-blockers were also less effective than an ACE inhibitor or a calcium channel blocker at reducing the risk of diabetes, particularly in patients taking a beta-blocker and a thiazide-type diuretic.
• Calcium-channel blockers or thiazide-type diuretics : These are the most likely drugs to confer benefit as first-line treatment for most patients aged 55 or older.

27
Drug treatmentDrug treatmentKey issues in updating the recommendations
• People younger than 55 years : The evidence suggests that initial therapy with an ACE inhibitor may be better than initial therapy with a calcium-channel blocker or a thiazide-type diuretic.
• Using more than one drug : Adding an ACE inhibitor to a calcium-channel blocker or a diuretic (or vice versa) is a logical combination, and has been commonly done in trials. There is little evidence on using three drugs so the recommendation is based on the most straightforward option.

28
BetaBeta --blockerblocker• Beta-blockers are no longer preferred as a routine initial therapy for
hypertension
• But consider them for younger people, particularly:– women of childbearing potential– patients with evidence of increased sympathetic drive– patients with intolerance of or contraindications to ACE
inhibitors and angiotensin-II receptor antagonists
• If a patient taking a beta-blocker needs a second drug, add a calcium-channel blocker rather than a thiazide-type diuretic, to reduce the patient’s risk of developing diabetes.
BetaBeta --blockerblocker• If a patient’s blood pressure is not controlled by a regimen that includes
a beta-blocker (that is, it is still above 140/90 mmHg), change their treatment by following the flow chart above.
• If a patient’s blood pressure is well controlled (that is,140/90 mmHg or less) by a regimen that includes a beta-blocker, consider long-term management at their routine review. There is no absolute need toreplace the beta-blocker in this case.
• When withdrawing a beta-blocker, step down the dose gradually.
• Beta-blockers should not usually be withdrawn if a patient has a compelling indication for being treated with one, such as symptomatic angina or a previous myocardial infarction.

29
PharmcoPharmco --economic Analysis economic Analysis
For 1st line treatment of essential hypertension (people at low risk of heart failure)
• Calcium Channel Blockers are the most cost effective option because they are associated with a low risk of diabetes and they also have a good effectiveness profile across the range of other cardiovascular disease risks.
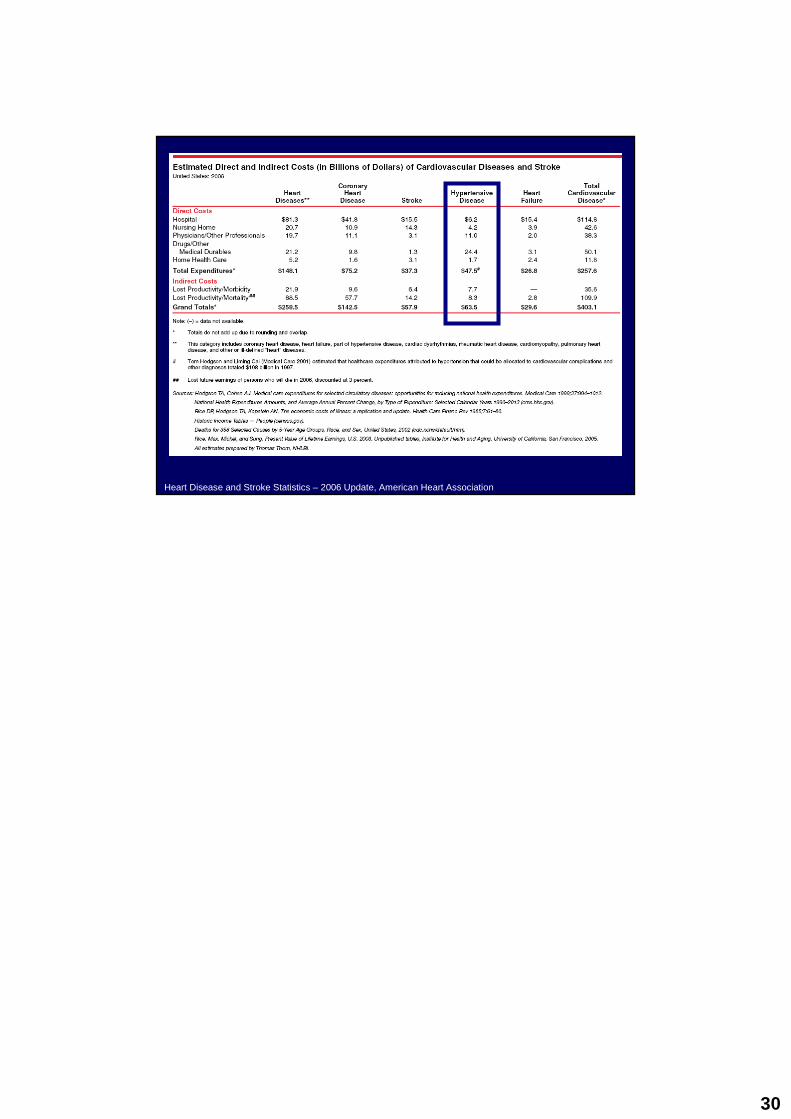
The cost of cardiovascular diseases The cost of cardiovascular diseases and strokeand stroke
Heart Disease and Stroke Statistics – 2006 Update, American Heart Association
30
Heart Disease and Stroke Statistics – 2006 Update, American Heart Association