arterial hypertension epidemiology, pathofysiologie ... van der niepen.pdfclinical management,...
TRANSCRIPT

26/09/2013
1
Arterial Hypertension & Renal disease Pathophysiology, Clinical management,
Therapy prescription and Complications
P. Van der Niepen
Nefrologie & Hypertensie
UZ Brussel
Core Curriculum Course Nephrology
Brussel, 28 september 2013
Hypertension Excellence
centre of the ESH
in Brussel
2
Outline
Introduction - Epidemiology,
Pathophysiology,
Clinical management,
Therapy prescription and Complications
3
Introduction
Hypertension (HT) is a major risk factor for
cardiovascular (CV) and renal disease.
Conversely, chronic kidney disease (CKD) is the
most common form of secondary HT and mounting
evidence suggests it is an independent risk factor
for CV morbidity and mortality.
Renal disease is a consequence as well as a cause of
hypertension

26/09/2013
2
Blood Pressure Predicts Risk of Developing End-
Stage Renal Disease in Men and Women
4
Cumulative incidence of ESRD
in 46 881 men and 51 878
women, according to the 6 BP
categories.
Relative risk (95% CI) of development of
ESRD for BP categories in men and women.
Relative risks, with optimal BP as the reference
category, are adjusted for age and BMI.
Tozawa et al. Hypertension 2003;41:1341-1345
HR of all-cause and CV mortality according to
eGFR/ACR in general population
5 CKD Prognosis Consortium. Lancet 2010; 375: 2073–81
Lower eGFR and higher albuminuria are associated with
mortality and ESRD. A collaborative meta-analysis of KD
population cohorts.
6
Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2012 Clinical
Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney intern,
Suppl. 2013; 3: 1–150.
Green: low risk (if
no other markers of
KD, no CKD);
Yellow: moderately
increased risk;
Orange: high risk;
Red, very high risk

26/09/2013
3
7
Introduction
Effective treatment ameliorates the harmful effects
of uncontrolled hypertension, as has been clearly
demonstrated by a large number of clinical trials [1].
Unfortunately, most trials have excluded patients
with CKD, and those trials that specifically targeted
CKD patients primarily focused on progression of
renal disease as the primary clinical endpoint.
[1]Turnbull F. Lancet 2003; 362:1527-35.
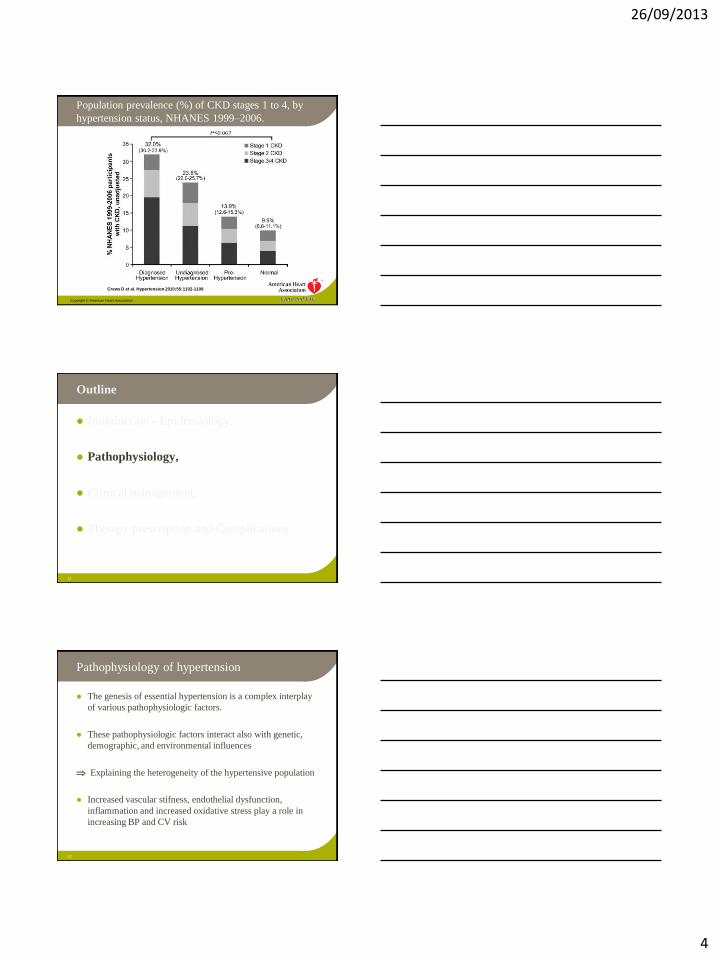
Prevalence of hypertension in CKD
The prevalence of hypertension is higher among
patients with CKD than in individuals without CKD,
progressively increasing with the severity of CKD.
Based on a national survey of a representative
sample of non-institutionalized adults in the USA, it
is estimated that hypertension occurs in
23.3% of individuals without CKD,
35.8% of stage 1,
48.1% of stage 2,
59.9% of stage 3, and
84.1% of stage 4-5 CKD patients
8
U S Renal Data System, USRDS 2010 Annual Data Report: Atlas of Chronic Kidney Disease and
End-Stage Renal Disease in the United States, National Institutes of Health, National Institute of
Diabetes and Digestive and Kidney Diseases. Bethesda, Md, USA, 2010.
Prevalence of hypertension in CKD
The incidence and prevalence of hypertension also
varie with the cause, the type of onset (acute and
chronic KD), and the duration of KD (GN and
vasculitis > interstitial disease);
A strong association with hypertension was
especially reported in patients with renal artery
stenosis (93%), diabetic nephropathy (87%), and
polycystic kidney disease (74%)
9
N. Ridao et al. “Prevalence of hypertension in renal disease,” NDT 2001; 16(1): 70–73.
26/09/2013
4
Crews D et al. Hypertension 2010;55:1102-1109
Copyright © American Heart Association
Population prevalence (%) of CKD stages 1 to 4, by
hypertension status, NHANES 1999–2006.
11
Outline
Introduction - Epidemiology,
Pathophysiology,
Clinical management,
Therapy prescription and Complications
Pathophysiology of hypertension
The genesis of essential hypertension is a complex interplay
of various pathophysiologic factors.
These pathophysiologic factors interact also with genetic,
demographic, and environmental influences
Explaining the heterogeneity of the hypertensive population
Increased vascular stifness, endothelial dysfunction,
inflammation and increased oxidative stress play a role in
increasing BP and CV risk
12

26/09/2013
5
Pathophysiologic factors that play a role in
the development and maintenance of
hypertension
13
Pathophysiologic factors that play a role in the
development and maintenance of hypertension
Pathophysiologic factor Increased or decreased activity
Neurohumoral mechanisms • SNS activity
• RAAS activity
• Production of sodium-retaining hormones
• Production and expression of vasoconstrictors
• Production and expression of vasodilators
• Kallikrein-kinin system activity
Dietary factors • Sodium intake
• Potassium and calcium intake
Vascular factors • Peripheral resistance
• Vascular stifness
• Endothelial dysfunction
Cellular mechanisms • Cellular ion transport
• Adrenergic receptor activity
or
or
Others • Inflammation
• Oxidative stress
• Psychosocial stress
14
Pathophysiology of Hypertension The Sympathetic Nervous System
15
Sympathetic nerve activity in normotensive versus hypertensive persons, showing the resting level
of activity of sympathetic postganglionic neurons that innervate muscle resistance arterioles (B).
The intensity and frequency of muscle sympathetic nerve activity (MSNA) bursts are higher in
hypertensive compared with normotensive persons (B and C). A, The level at which MSNA was
measured. (Guyenet PG. The sympathetic control of BP. Nat Rev Neurosci. 2006;7:335-346.)

26/09/2013
6
The Sympathetic Nervous System: the afferent signals
from peripheral sympathetic and somatic receptors
16
Somatic and sympathetic afferent nerves
The Sympathetic Nervous System: the sympathetic
efferent signals to the periphery
17
Long-term consequences of increased central sympathetic outflow. pCO2, partial pressure of
carbon dioxide.
Pathophysiology of Hypertension The Renin-Angiotensin-Aldosterone System
18

26/09/2013
7
Pathophysiology of Hypertension Salt Sensitivity
19
Mechanisms of salt-induced BP elevation and target organ damage. Increased dietary salt activates
shear forces and stimulates transforming growth factor-β (TGF-β) and nitric oxide (NO)
production. In the setting of increased tonicity and in the presence of aldosterone, NO production
is suppressed, leading to unopposed TGF-β activity. Ultimately, these changes result in increased
BP and TOD. (Redrawn from Sanders PW. Vascular consequences of dietary salt intake. Am J
Physiol Renal Physiol. 2009;297:F237-243.)
Pathophysiology of Hypertension Arterial Stiffness
20
Neurohumoral, mechanical, and genetic factors regulate extracellular matrix protein expression
and result in increased arterial stiffness, peripheral resistance, and BP. MMPs, matrix
metalloproteinases. (Redrawn from Briones AM, Arribas SM, Salaices M. Role of extracellular
matrix in vascular remodeling of hypertension. Curr Opin Nephrol Hypertens. 2010;19:187-194.)
Pathophysiology of Hypertension in Kidney
Disease
The kidneys play a vital role in long-term BP
regulation[]
Virtually all forms of experimental and human HT
exhibit impaired sodium excretion by the kidneys at
normal BP[2]
Sodium loading increases BP only when renal sodium
excretion is constrained (ablation 2/3 renal mass;
administration of angiotensin or aldosteron) Initial BP rise
is mediated by expansion of extracellular fluid volume and
CO(SBP). Over time, ECF volume and CO normalize and
high BP results from elevated peripheral resistance (DBP)[1]
21
[1]C. Guyton et al. “Salt balance and long-term blood pressure control” Ann Rev Med 1980; 31:15–27. [2]J. E. Hall. Hypertension 2003; 41(3):625–633.
26/09/2013
8
Pathophysiology of Hypertension in Kidney
Disease
Key components of hypertension in KD include:
Inappropriately elevated sympathetic nervous activity
efferent arteriolar vasoconstriction (-receptors) more sodium
retention
Stimulate renin release (-receptors) more AII
efferent arteriolar vc and sodium retention
stimulates PTC to recover filtered sodium (Na+/H+ antiporter)
stimulates aldosteron production and release stimulates distal sodium
reabsorption
Activation of the RAAS
SNS activity
Fall in distal nephron [sodium] is an additional stimulus for renin release
Increased arterial stiffness
Impaired salt and water excretion by the kidneys increase
in extracellular fluid exacerbation of high BP in KD 22
Pathophysiology of Hypertension in Kidney
Disease
Other factors that may explain increased vascular
resistance in CKD include:
Increased production of endothelin and endogenous digitalis-
like substance[1,2]
Reduced generation of vasodilators (NO, Kinins)[3,4]
Imbalance between VD and VC prostaglandins[5]
Oxidative stress[6]
23
[1] D. E. Kohan. AJKD 1997;29(1):2–26. [2] M. P. Blaustein et al. Hypertension 2009; 53, (2):291–
298. [3] N. D. Vaziri. AJKD 2001;38(4):S74–S79, [4] J. A. Mitas, et al. NEJM 1978; 299(4):162–165. [5] M. J. Dunn and V. L. Hood. Am J Physiol 1977; 233(3):169–184. [6] N. D. Vaziri. Curr Opin
Nephrol Hypertens 2004; 13(1):93–99,
Subtle renal defects may underlie the pathogenesis of
essential hypertension
This is supported by
Transplant with kidneys from normotensive donors in
patients with ESRD due to hypertensive nephrosclerosis
results in resolution of their HT[]
NT individuals with family history of HT respond to salt
loading with less natriuresis and higher BP than those with
no family history [2]
HT patients have fewer nephrons than NT counterparts[3]
• The exact nature of renal defect(s) for inappropriate
sodium excretion remains unclear
24
[]J.J. Curtis et al. “Remission of essential HT after renal transplantation” NEJM 1983; 309(17):1009–15. [2]B.R. Widgren et al. “Blunted renal Sodium excretion during acute saline loading in normotensive men
with positive family histories of HT” Am J Hypertens 1991; 4:570–578. [3]G. Keller, et al. “Nephron
number in patients with primary hypertension” NEJM 2003; 348(2):101–108
26/09/2013
9
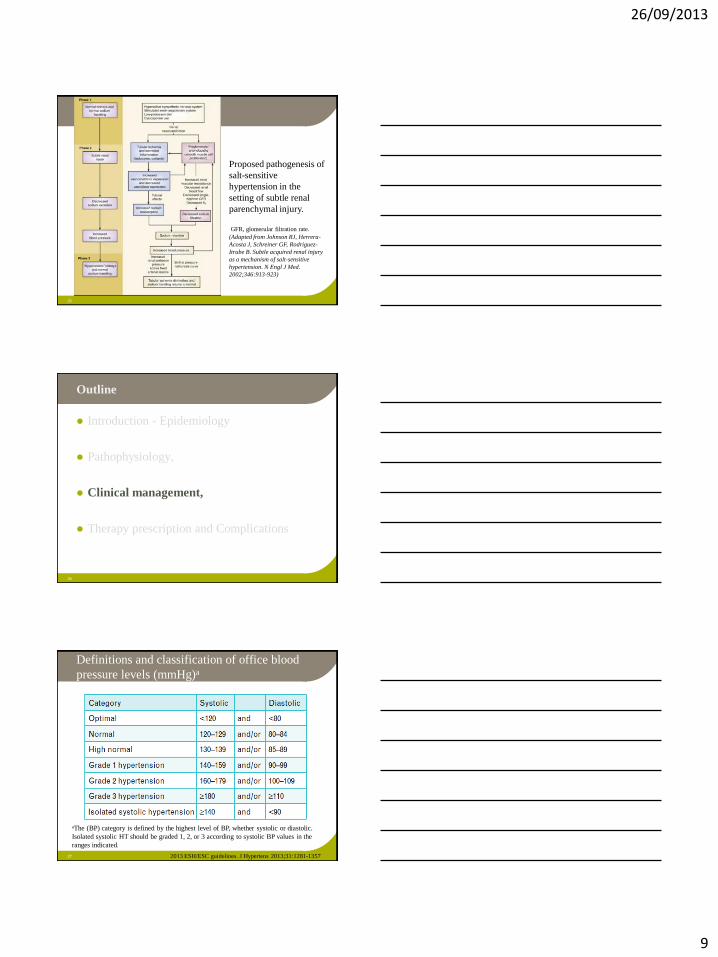
25
Proposed pathogenesis of
salt-sensitive
hypertension in the
setting of subtle renal
parenchymal injury.
GFR, glomerular filtration rate. (Adapted from Johnson RJ, Herrera-
Acosta J, Schreiner GF, Rodriguez-
Itrube B. Subtle acquired renal injury
as a mechanism of salt-sensitive
hypertension. N Engl J Med.
2002;346:913-923)
26
Outline
Introduction - Epidemiology
Pathophysiology,
Clinical management,
Therapy prescription and Complications
Definitions and classification of office blood
pressure levels (mmHg)a
27
aThe (BP) category is defined by the highest level of BP, whether systolic or diastolic.
Isolated systolic HT should be graded 1, 2, or 3 according to systolic BP values in the
ranges indicated.
2013 ESH/ESC guidelines. J Hypertens 2013;31:1281-1357
26/09/2013
10
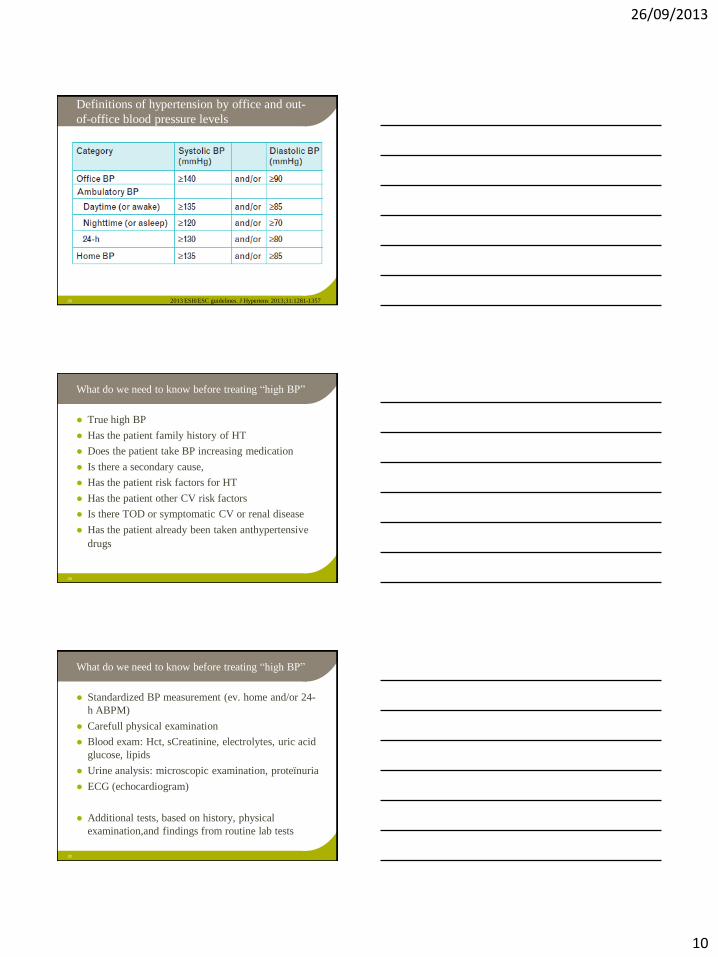
Definitions of hypertension by office and out-
of-office blood pressure levels
28 2013 ESH/ESC guidelines. J Hypertens 2013;31:1281-1357
What do we need to know before treating “high BP”
True high BP
Has the patient family history of HT
Does the patient take BP increasing medication
Is there a secondary cause,
Has the patient risk factors for HT
Has the patient other CV risk factors
Is there TOD or symptomatic CV or renal disease
Has the patient already been taken anthypertensive
drugs
29
What do we need to know before treating “high BP”
Standardized BP measurement (ev. home and/or 24-
h ABPM)
Carefull physical examination
Blood exam: Hct, sCreatinine, electrolytes, uric acid
glucose, lipids
Urine analysis: microscopic examination, proteïnuria
ECG (echocardiogram)
Additional tests, based on history, physical
examination,and findings from routine lab tests
30

26/09/2013
11
Clinical indications for out-of-office BP
measurement for diagnostic purposes
31
ABPM, ambulatory
blood pressure
monitoring;
BP, blood pressure;
CKD, chronic kidney
disease;
CV, cardiovascular;
HBPM, home blood
pressure monitoring.
2013 ESH/ESC guidelines. J Hypertens 2013;31:1281-1357
32
The relationship between BP and CV morbidity and mortality is
modified by the concomitance of other CV risk factors.
The relationship between BP and CV morbidity and mortality
is modified by the concomitance of other CV risk factors.
Metabolic risk factors are more common when BP is high
than when it is low[1,2,3].
1Lewington S et al. Lancet 2002; 360:1903–1913. 2Kannel WB et al. Am J Hypertens 2000;
13:3S-10S. 3Thomas F et al. Hypertension 2001; 37:1256-61.
Survival probability for CVD mortality in younger (left) and older (right) men according to the
presence of HTN and associated RFs.
Nt = normotensive subjects; Ht 0, HT subjects without RFs; Ht 1-2, HT subjects with 1 or 2 RFs; ...
Assessment of total cardiovascular risk
33
Stratification of total CV risk in categories of low, moderate, high and very high risk according to SBP
and DBP and prevalence of RFs, asymptomatic OD, diabetes, CKD stage or symptomatic CVD. Subjects
with a high normal office but a raised out-of-office BP (masked HT) have a CV risk in the HT range.
Subjects with a high office BP but normal out-of-office BP (white-coat HT), particularly if there is no
diabetes, OD, CVD or CKD, have lower risk than sustained HT for the same office BP.
2013 ESH/ESC guidelines. J Hypertens 2013;31:1281-1357

26/09/2013
12
When to initiate antihypertensive drug
treatment
34
Initiation of lifestyle changes & antihypertensive drug treatment. Targets of treatment are also indicated.
The optimal DBP target in patients with diabetes is between 80 and 85 mmHg. In the high normal BP
range, drug treatment should be considered in the presence of a raised out-of-office BP (masked HT).
Lack of evidence in favour of drug treatment in young individuals with isolated systolic HT. 2013 ESH/ESC guidelines. J Hypertens 2013;31:1281-1357
BP goals in hypertensive patients
35
CHD, coronary heart disease; CKD, chronic kidney disease; CV, cardiovascular; DBP, diastolic
blood pressure; SBP, systolic blood pressure; TIA, transient ischaemic attack.
aClass of recommendation. bLevel of evidence.
2013 ESH/ESC guidelines. J Hypertens 2013;31:1281-1357
TREATMENT STRATEGIES
Lifestyle changes
36 Based on the effect on BP and/or CV risk profile
Based on outcome studies

26/09/2013
13
TREATMENT STRATEGIES
Pharmacological therapy
Choice of antihypertensive drugs
The main benefits of antihypertensive treatment
are due to lowering of BP per se and are largely
independent of the drugs employed as has been
shown by large meta-analysis[,2,3]
Diuretics, BB, CCB, ACEI and ARBs are all
suitable for the initiation and maintenance of
antihypertensive treatment, either as monotherapy
or in some combinations[1]
37
[] 2013 ESH guidelines. J Hypertens 2013; 31:1281-1357. [2] Law MR et al. BMJ 2009;
338:b1665. [3] BPLTTC. Lancet 2003; 362:1527-35. Arch Intern Med 2005; 165:1410-19.
Relative risk estimates of coronary heart disease
events and stroke (Law meta-analysis; BMJ 2009)
38
Relative risk estimates of coronary heart disease (CHD) events and stroke in 46 drug
comparison trials comparing each of the five classes of BP lowering drug with any other class
of drug (excluding CHD events in trials of β blockers in people with a history of CHD)
Drugs to be preferred in specific conditions
39 2013 ESH/ESC guidelines. J Hypertens 2013;31:1281-1357

26/09/2013
14
Compelling and possible contra-indications to the use
of antihypertensive drugs
40 2013 ESH/ESC guidelines. J Hypertens 2013;31:1281-1357
Monotherapy vs. drug combination strategies to achieve target
BP. Moving from a less intensive to a more intensive therapeutic
strategy should be done whenever BP target is not achieved.
41 2013 ESH/ESC guidelines. J Hypertens 2013;31:1281-1357
Possible combinations of classes of antihypertensive
drugs
42
Green continuous lines: preferred combinations; green dashed line: useful combination (with
some limitations); black dashed lines: possible but less well tested combinations; red continuous
line: not recommended combination. Although verapamil and diltiazem are sometimes used with a
beta-blocker to improve ventricular rate control in permanent atrial fibrillation, only dihydropyridine
calcium antagonists should normally be combined with beta-blockers.
26/09/2013
15
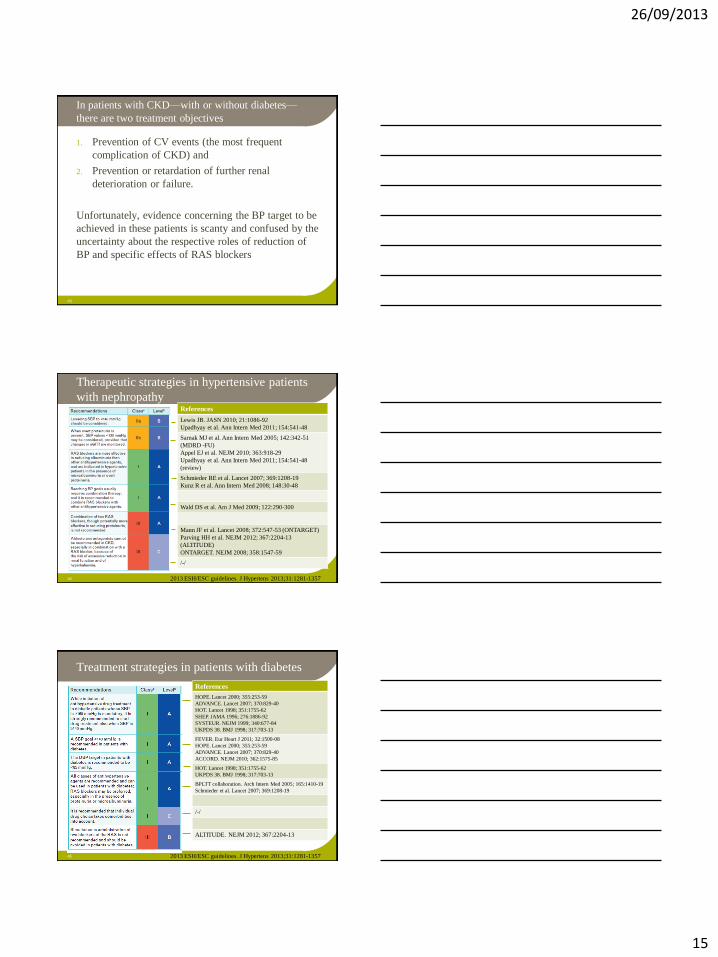
In patients with CKD—with or without diabetes—
there are two treatment objectives
1. Prevention of CV events (the most frequent
complication of CKD) and
2. Prevention or retardation of further renal
deterioration or failure.
Unfortunately, evidence concerning the BP target to be
achieved in these patients is scanty and confused by the
uncertainty about the respective roles of reduction of
BP and specific effects of RAS blockers
43
Therapeutic strategies in hypertensive patients
with nephropathy
44
References
Lewis JB. JASN 2010; 21:1086-92
Upadhyay et al. Ann Intern Med 2011; 154:541-48
Sarnak MJ et al. Ann Intern Med 2005; 142:342-51
(MDRD -FU)
Appel EJ et al. NEJM 2010; 363:918-29
Upadhyay et al. Ann Intern Med 2011; 154:541-48
(review)
Schmieder RE et al. Lancet 2007; 369:1208-19
Kunz R et al. Ann Intern Med 2008; 148:30-48
Wald DS et al. Am J Med 2009; 122:290-300
Mann JF et al. Lancet 2008; 372:547-53 (ONTARGET)
Parving HH et al. NEJM 2012; 367:2204-13
(ALTITUDE)
ONTARGET. NEJM 2008; 358:1547-59
/-/
2013 ESH/ESC guidelines. J Hypertens 2013;31:1281-1357
Treatment strategies in patients with diabetes
45
References
HOPE. Lancet 2000; 355:253-59
ADVANCE. Lancet 2007; 370:829-40
HOT. Lancet 1998; 351:1755-62
SHEP. JAMA 1996; 276:1886-92
SYSTEUR. NEJM 1999; 340:677-84
UKPDS 38. BMJ 1998; 317:703-13
FEVER. Eur Heart J 2011; 32:1500-08
HOPE. Lancet 2000; 355:253-59
ADVANCE. Lancet 2007; 370:829-40
ACCORD. NEJM 2010; 362:1575-85
HOT. Lancet 1998; 351:1755-62
UKPDS 38. BMJ 1998; 317:703-13
BPLTT collaboration. Arch Intern Med 2005; 165:1410-19
Schmieder et al. Lancet 2007; 369:1208-19
/-/
ALTITUDE. NEJM 2012; 367:2204-13
2013 ESH/ESC guidelines. J Hypertens 2013;31:1281-1357
26/09/2013
16
Complications of hypertension
Subclinical target organ damage
Left ventricle hypertrophy
Retinopathy
Microalbuminuria
Carotid intima-media thickness, generalised atheromatosis
Binswanger lesions (asymptomatic white-matter lacunar infarcts)
Cardiovascular and renal events
Coronary heart disease, Heart failure
Stroke
Renal failure
Peripheral artery disease, aortic dissection, aortic aneurysm
Vascular dementia
CV death
46
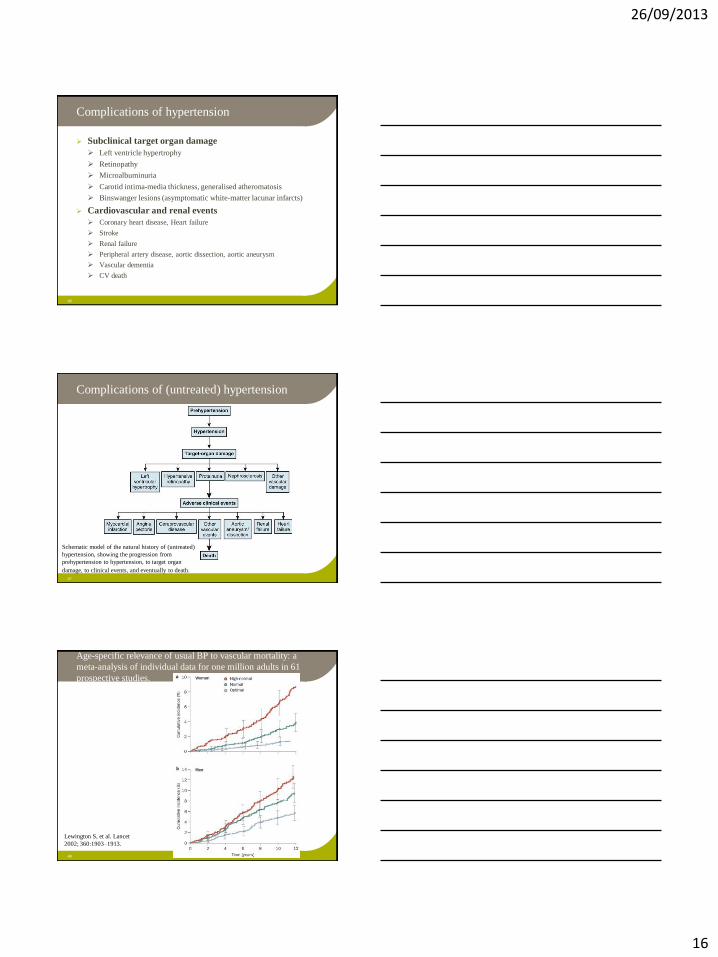
Complications of (untreated) hypertension
47
Schematic model of the natural history of (untreated)
hypertension, showing the progression from
prehypertension to hypertension, to target organ
damage, to clinical events, and eventually to death.
48
Age-specific relevance of usual BP to vascular mortality: a
meta-analysis of individual data for one million adults in 61
prospective studies.
Lewington S, et al. Lancet
2002; 360:1903–1913.
26/09/2013
17
49
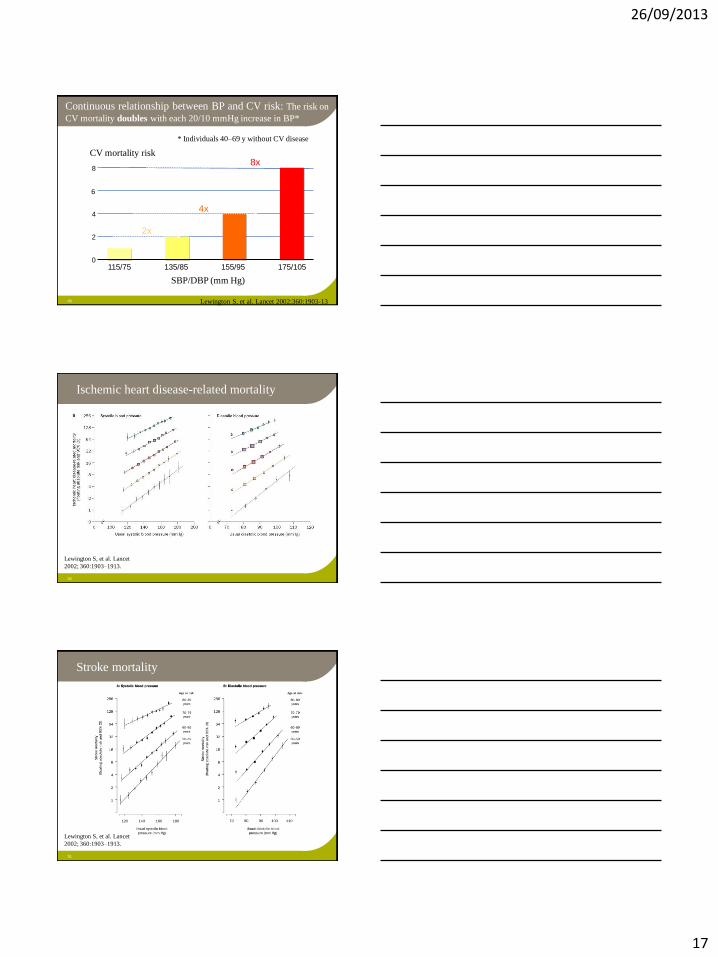
CV mortality risk
0
2
4
8
115/75 135/85 155/95 175/105
6
2x
4x
8x
SBP/DBP (mm Hg)
* Individuals 40–69 y without CV disease
Lewington S, et al. Lancet 2002;360:1903-13
Continuous relationship between BP and CV risk: The risk on
CV mortality doubles with each 20/10 mmHg increase in BP*
Ischemic heart disease-related mortality
50
Lewington S, et al. Lancet
2002; 360:1903–1913.
Stroke mortality
51
Lewington S, et al. Lancet
2002; 360:1903–1913.
26/09/2013
18
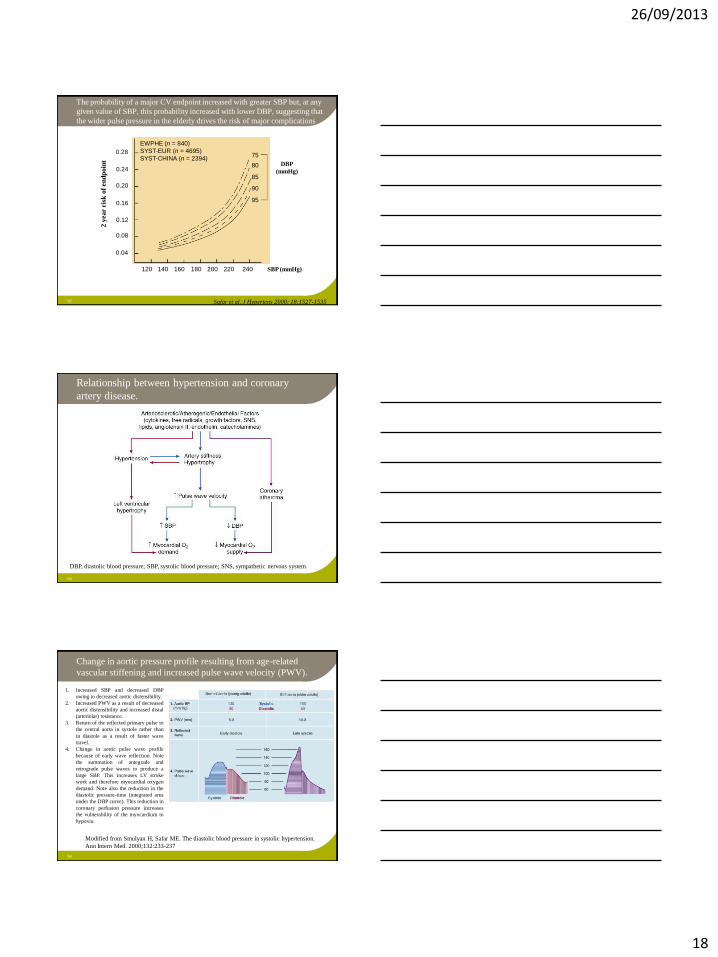
52 Safar et al. J Hypertens 2000; 18:1527-1535
75
80
85
90
95
DBP
(mmHg)
120 140 160 180 200 220 240 SBP (mmHg)
0.28
0.24
0.20
0.16
0.12
0.08
0.04
EWPHE (n = 840)
SYST-EUR (n = 4695)
SYST-CHINA (n = 2394)
2 y
ea
r ris
k o
f en
dp
oin
t The probability of a major CV endpoint increased with greater SBP but, at any
given value of SBP, this probability increased with lower DBP, suggesting that
the wider pulse pressure in the elderly drives the risk of major complications
Relationship between hypertension and coronary
artery disease.
53
DBP, diastolic blood pressure; SBP, systolic blood pressure; SNS, sympathetic nervous system.
Change in aortic pressure profile resulting from age-related
vascular stiffening and increased pulse wave velocity (PWV).
54
1. Increased SBP and decreased DBP
owing to decreased aortic distensibility.
2. Increased PWV as a result of decreased
aortic distensibility and increased distal
(arteriolar) resistance.
3. Return of the reflected primary pulse to
the central aorta in systole rather than
in diastole as a result of faster wave
travel.
4. Change in aortic pulse wave profile
because of early wave reflection. Note
the summation of antegrade and
retrograde pulse waves to produce a
large SBP. This increases LV stroke
work and therefore myocardial oxygen
demand. Note also the reduction in the
diastolic pressure-time (integrated area
under the DBP curve). This reduction in
coronary perfusion pressure increases
the vulnerability of the myocardium to
hypoxia.
Modified from Smulyan H, Safar ME. The diastolic blood pressure in systolic hypertension.
Ann Intern Med. 2000;132:233-237
26/09/2013
19
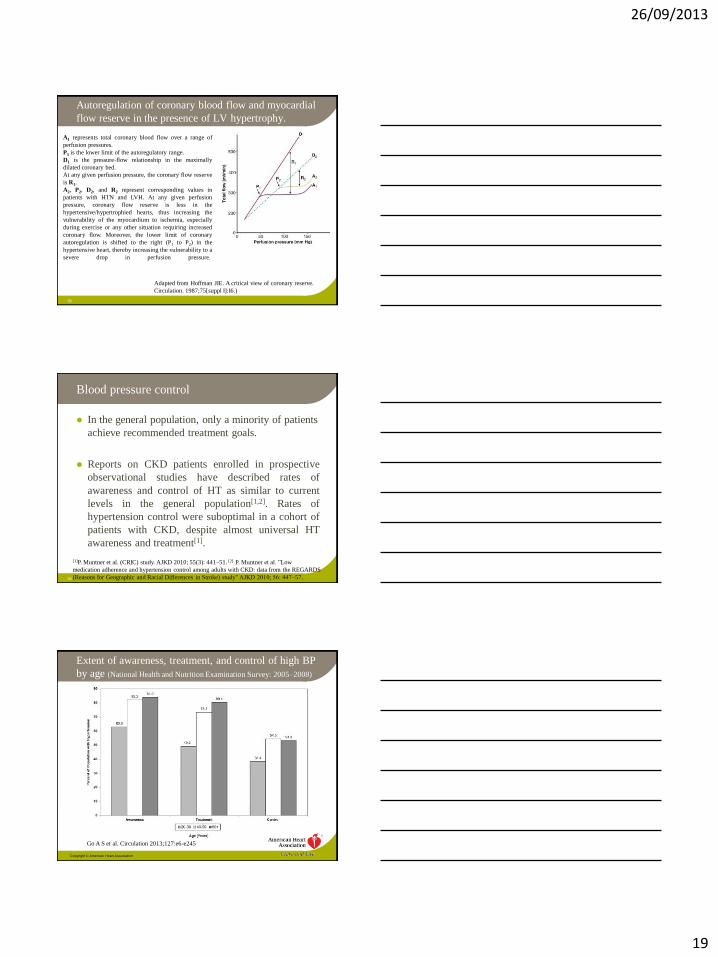
Autoregulation of coronary blood flow and myocardial
flow reserve in the presence of LV hypertrophy.
55
A1 represents total coronary blood flow over a range of
perfusion pressures.
P1 is the lower limit of the autoregulatory range.
D1 is the pressure-flow relationship in the maximally
dilated coronary bed.
At any given perfusion pressure, the coronary flow reserve
is R1.
A2, P2, D2, and R2 represent corresponding values in
patients with HTN and LVH. At any given perfusion
pressure, coronary flow reserve is less in the
hypertensive/hypertrophied hearts, thus increasing the
vulnerability of the myocardium to ischemia, especially
during exercise or any other situation requiring increased
coronary flow. Moreover, the lower limit of coronary
autoregulation is shifted to the right (P1 to P2) in the
hypertensive heart, thereby increasing the vulnerability to a
severe drop in perfusion pressure.
Adapted from Hoffman JIE. A critical view of coronary reserve.
Circulation. 1987;75[suppl I]:I6.)
Blood pressure control
In the general population, only a minority of patients
achieve recommended treatment goals.
Reports on CKD patients enrolled in prospective
observational studies have described rates of
awareness and control of HT as similar to current
levels in the general population[1,2]. Rates of
hypertension control were suboptimal in a cohort of
patients with CKD, despite almost universal HT
awareness and treatment[1].
56
[1]P. Muntner et al. (CRIC) study. AJKD 2010; 55(3): 441–51. [2] P. Muntner et al. ”Low
medication adherence and hypertension control among adults with CKD: data from the REGARDS
(Reasons for Geographic and Racial Differences in Stroke) study” AJKD 2010; 56: 447–57.
Go A S et al. Circulation 2013;127:e6-e245
Copyright © American Heart Association
Extent of awareness, treatment, and control of high BP
by age (National Health and Nutrition Examination Survey: 2005–2008)

26/09/2013
20
58
I-inSyst: Blood pressure control (0-6/2004)
SBP (mmHg)
60 80 100 120 140 160 180 200 220 240 260
DB
P (
mm
Hg
)
20
40
60
80
100
120
140
160
21.5%
2.3%
28.5%
47.8%
23.7% 76.3%
50.1%
49.9%
n=11,562 (49%V); 18% DM; 63 yrs; 150 (12)/88 (6) mm Hg
Van der Niepen et al, J Hypertens 2008; 26(10):2057-63
78,5%
NOT at goal
# : 1.6; 50% monotherapy
21.5 %
HT prevalence, awareness, treatment and control in
adults with CKD (CRIC study. AJKD 2010; 55: 441-51)
59
SBP & DBP distribution among participants
in the CRIC study (n=3612).
Overall rates of HT prevalence, awareness,
treatment and control among participants
of the Chronic Renal Insufficiency Cohort
(CRIC) study. HTN Prevalence among all
CRIC participants; Aware and Treated are
the percent among all participants with HT.
HT control rates are calculated for all
CRIC participants with HT.
Conclusions
Hypertension is a frequent CVRF
Hypertension is a cause and a consequence of CKD
The pathophysiology is complex
Total CV risk should be calculated
Treatment and BP control can be ameliorated
60