complications of pregnancy and lifetime risk to … · complications of pregnancy and lifetime ......
TRANSCRIPT
Complications of
Pregnancy and Lifetime
Risk to Health Brian McCulloch MD
Advocate Lutheran General Hospital
September 26, 2015
Pregnancy as a window to future health
In 2005 the CDC stated that almost 1 in every 2 adults had at least one
chronic illness
There are three time periods where a women has to enters into health care
on a regular basis : as an infant, for pregnancy and when she develops a
chronic disease.
Health education and prevention of these chronic diseases will be the task as
we move forward.
But first we have to identify those at risk
With pregnancy you have a trapped
population
To not seek prenatal care would be not acceptable by our society
How to use that time to educate, identify problems and direct the patient
and introduce the offspring to the health care system is extremely important
On average there are about 10 prenatal visits routinely covered for global
care
There are usually monthly visits up till 28 weeks and biweekly to 36 weeks
and then weekly till delivery.
Women’s health care
What we’ll be talking about
Definition of gestational diabetes
Screening after gestational diabetes
Long term maternal outcome after gestational diabetes
Fetal / childhood/ adult outcome after gestational diabetes
Gestational hypertension, Chronic hypertension and Preeclampsia Definitions
Long term outcome after preeclampsia
Weight gain and obesity in pregnancy
Maternal long term outcome
I want to start back in the recent past :
1964 with glucose testing
John O’Sullivan published on 752 pregnant women who had 100 gram glucose
screening in 1964
Initially he established the screening guidelines that everyone could agree on
and became our diabetic screening in pregnancy
They did this to improve perinatal outcome and lower the rate of macrosomia
(large fetus) and thereby improve perinatal morbidity and mortality.
He had a stable population in his area in Boston and he did long term follow
up
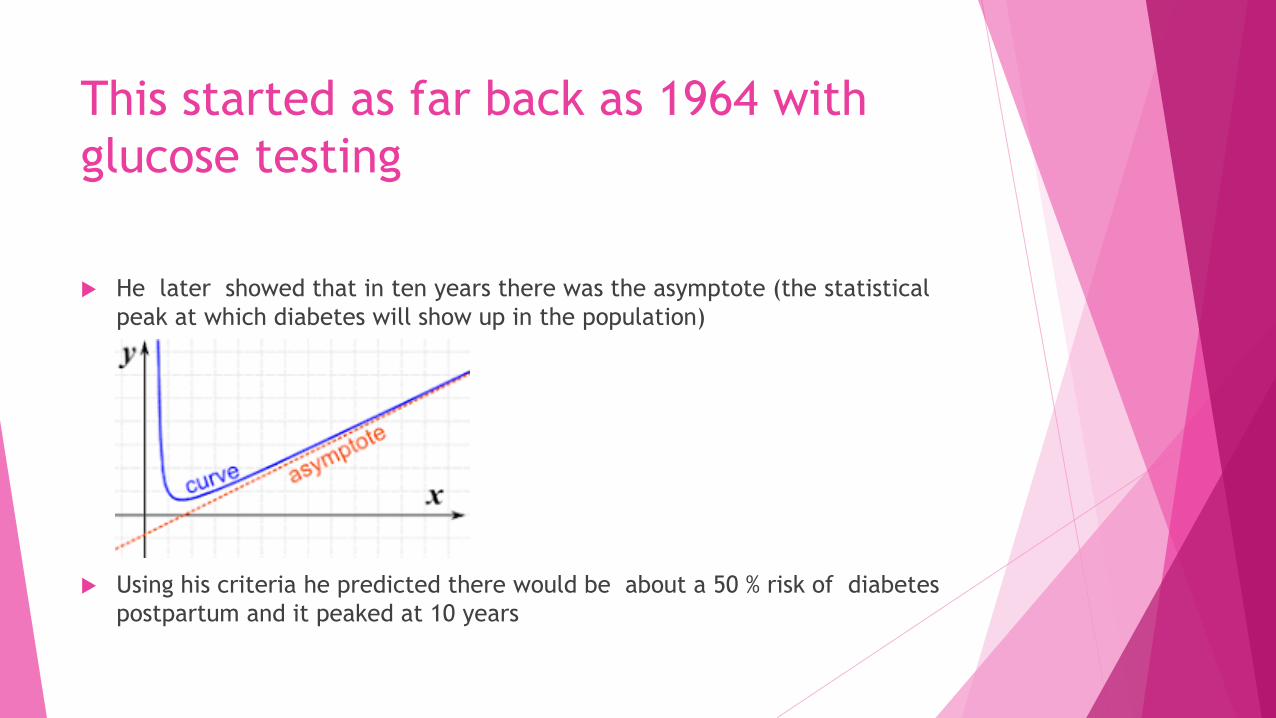
This started as far back as 1964 with
glucose testing
He later showed that in ten years there was the asymptote (the statistical
peak at which diabetes will show up in the population)
Using his criteria he predicted there would be about a 50 % risk of diabetes
postpartum and it peaked at 10 years

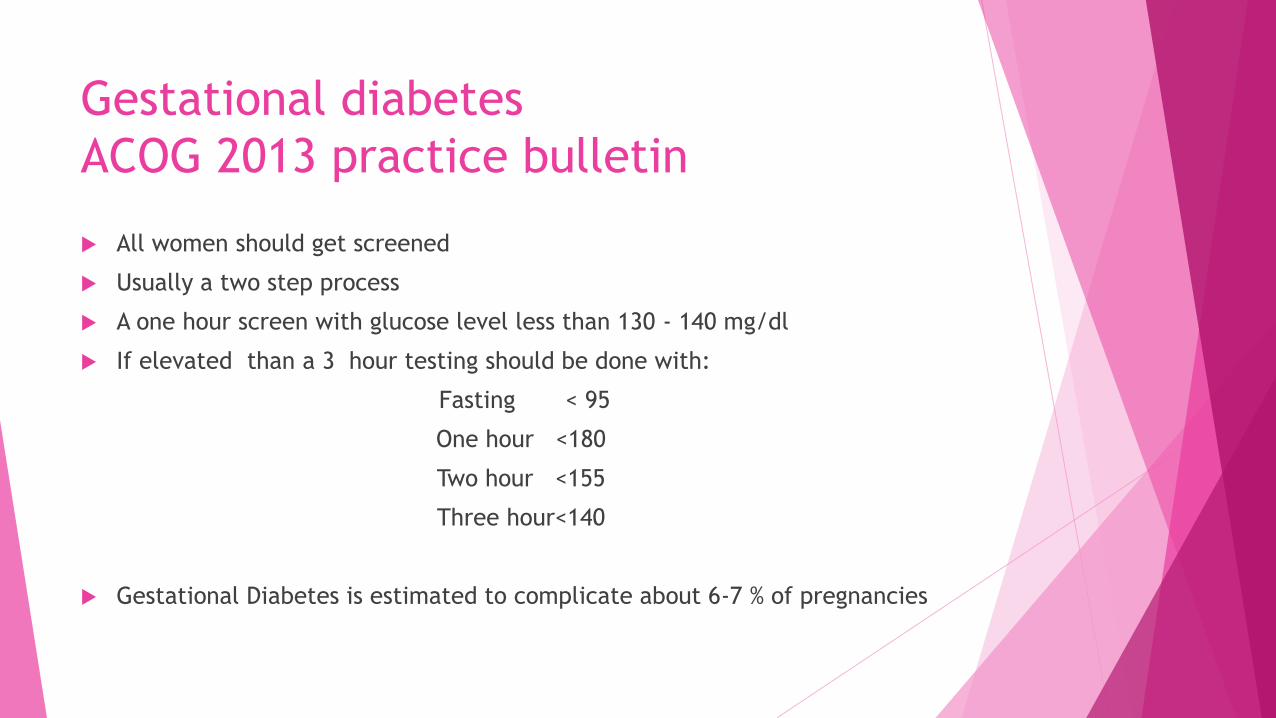
Gestational diabetes
ACOG 2013 practice bulletin
All women should get screened
Usually a two step process
A one hour screen with glucose level less than 130 - 140 mg/dl
If elevated than a 3 hour testing should be done with:
Fasting < 95
One hour <180
Two hour <155
Three hour<140
Gestational Diabetes is estimated to complicate about 6-7 % of pregnancies
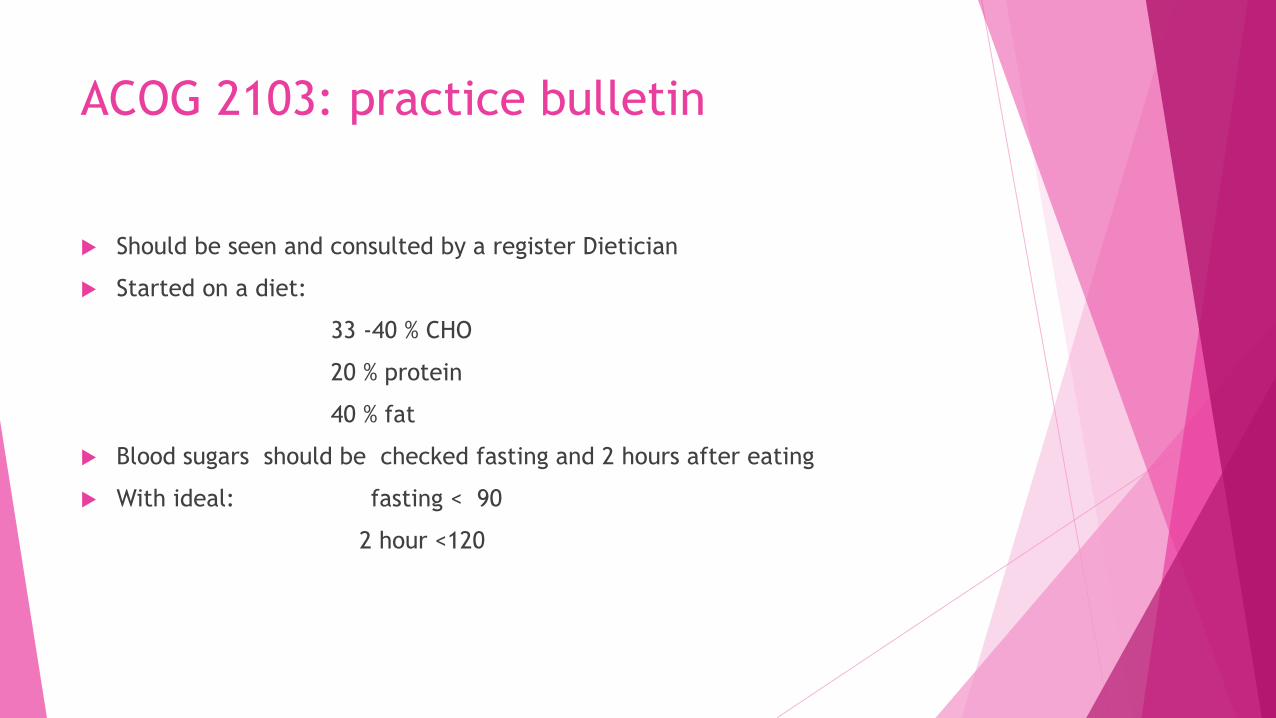
ACOG 2103: practice bulletin
Should be seen and consulted by a register Dietician
Started on a diet:
33 -40 % CHO
20 % protein
40 % fat
Blood sugars should be checked fasting and 2 hours after eating
With ideal: fasting < 90
2 hour <120
One step screening
Fasting serum blood sugar then 75 gram load
And if one value elevated then label it diabetes
Cut off values : Fasting< 92
One hour <180
Two hour <153
Very high failure rate 18 %
So not universally accepted
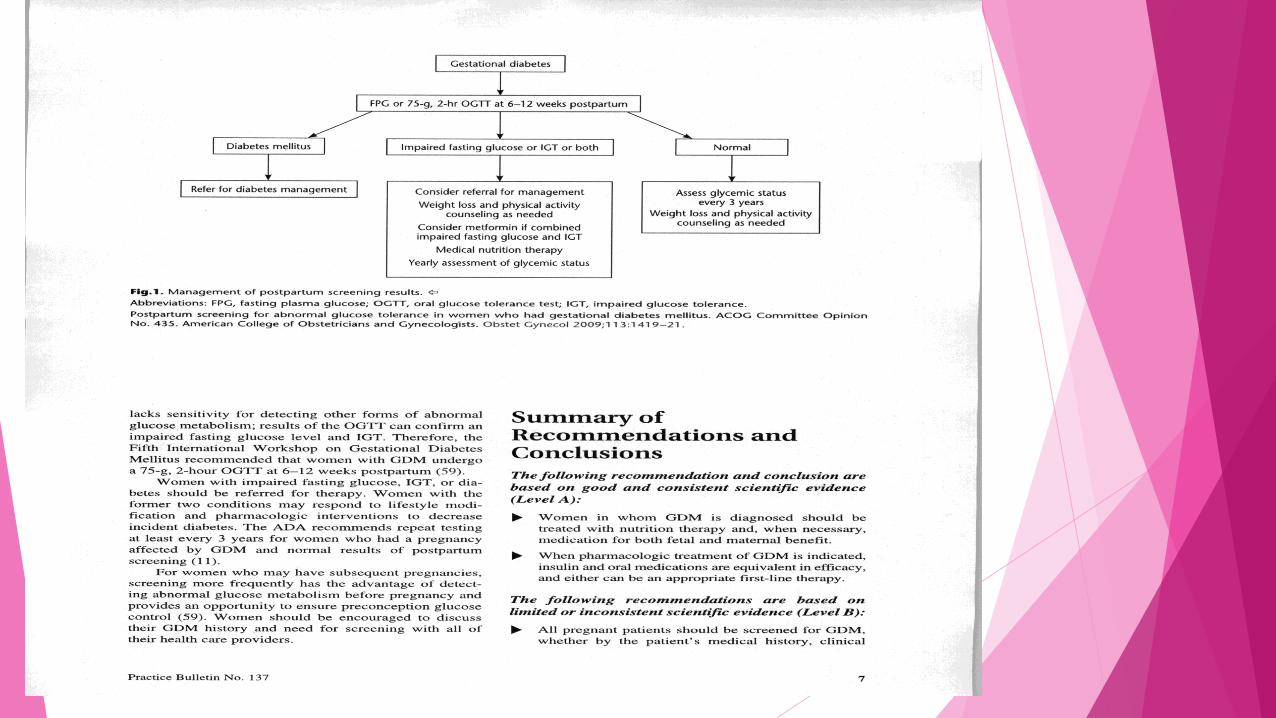
Post partum follow up
Screening should be at 6-12 weeks
Fasting blood sugar (easier to perform)
or 75 gram glucose with 2 hour (higher sensitivity)
Up to one third of GDM’s will have impaired glucose metabolism
15 to 50% will develop type 2 diabetes later in life
ADA recommends screening every 3 years
90% of women with a history of
Gestational diabetes recognize it
as a risk factor for type 2
diabetes, but only 16% felt they
themselves were at risk


Swedish study
18 year old males
Registration data for the military
Had info on brothers

Association of maternal diabetes mellitus in
pregnancy with offspring adiposity into early
adulthood Circulation 2011 Results :
Maternal early pregnancy BMI was weakly positively associated with birth
weight and moderately associated with offspring BMI at age 18.
Maternal early pregnancy BMI was positively associate with odds of Diabetes
mellitus in pregnancy.
There is evidence that greater amniotic fluid and cord blood insulin levels are
related to later offspring adiposity.
The does appear to be an inutero mechanism to explain elevated BMI beyond
the familial cofounding mechanism.
There has been many more medical
relationships identified in pregnancy
over the next 40+ years
There was a big interest with the 2011 update Guidelines from the
American heart association published in the journal Circulation.
Effectiveness-Based Guidelines
for the Prevention of
Cardiovascular Disease in
Women—2011 Update
A Guideline From the American
Heart Association
Published OnLine Feb 16, 2011
Cardiovascular disease
Cardiovascular disease has been identified as a women's disease also not just
a man’s disease.
There was a downward trend in female cardiovascular disease till 2008 but
now that is rising again paralleling the obesity epidemic
Obesity
Facts from the WHO (updated March 2013)
Obesity has almost doubled since 1980 worldwide
2008: 1.4 billion adults were overweight (35%), 500 million were obese (11%) (age 20 and over)
300 million women were obese
More than 40 million children under the age of five were overweight in 2011
Care Implications in the Setting of
Obesity in Pregnancy
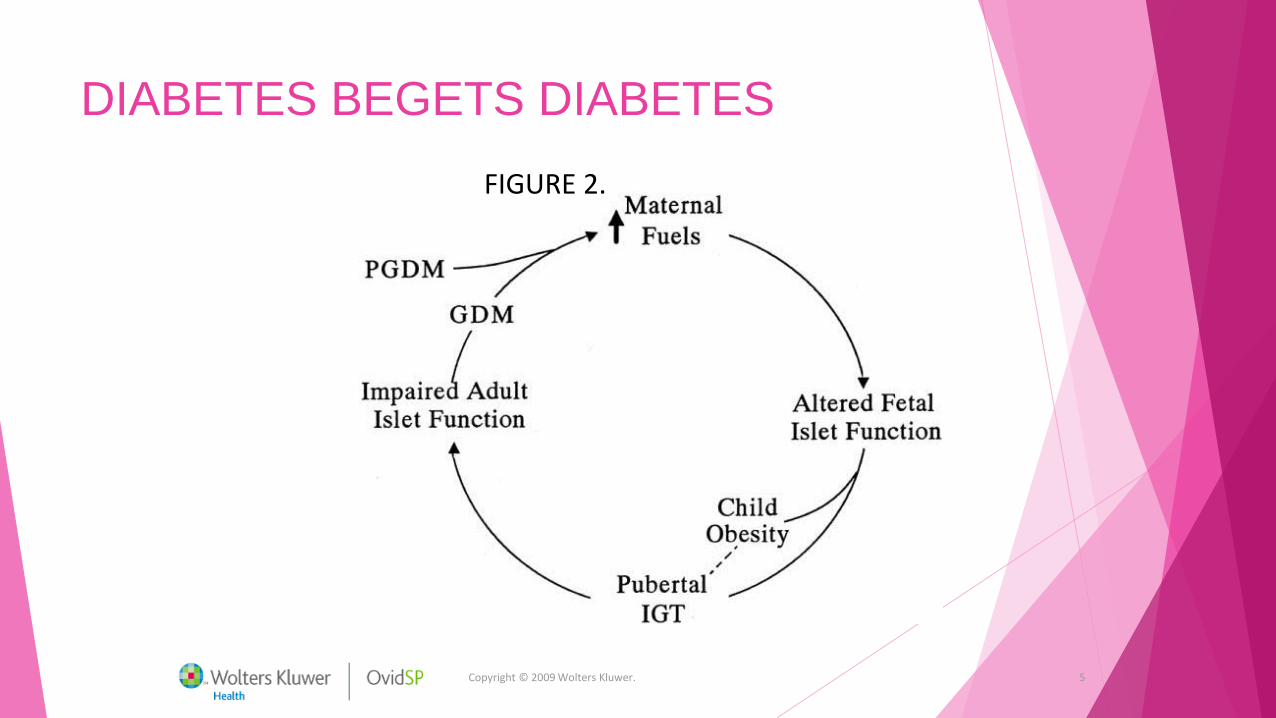
Copyright © 2009 Wolters Kluwer. 5
FIGURE 2.
DIABETES BEGETS DIABETES
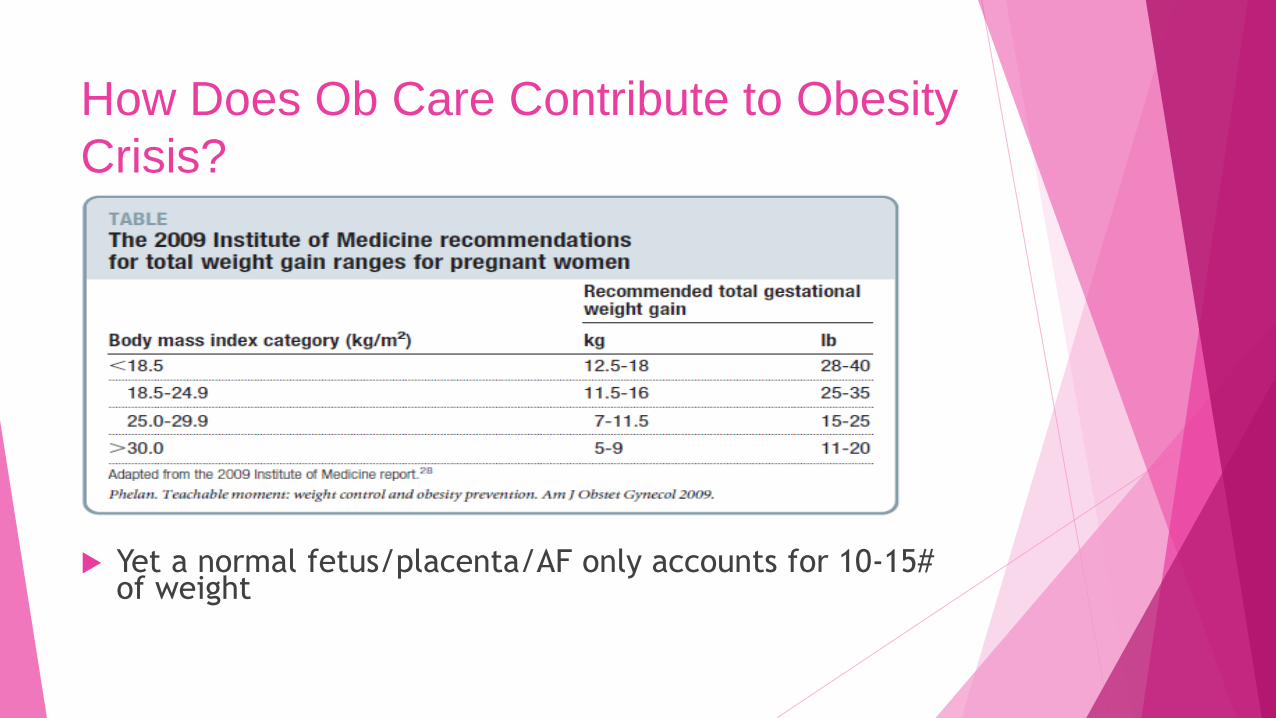
How Does Ob Care Contribute to Obesity
Crisis?
Yet a normal fetus/placenta/AF only accounts for 10-15# of weight
Implications of IOM Recommendations
Decreases incidence of SGA infants
Does not look at excessive LGA rates
Does not look at weight retention by mothers
Recommend increased weight gain for teens and Blacks
due to risk of SGA – BUT these groups at increase risk of
significant obesity
Obesity in the reproductive age
From 1980 to 1999 – increases in:
Mean maternal weight increased by 20% (144 to 172lbs)
Saw increases in:
Percentage of women ≥200lb (7.3 24.4%)
Percentage of women ≥250lb (1.9 10.7%)
Percentage of women ≥300lb (0.5 4.9%)
Percentage with a BMI >29 (16.3 36.4%)
Lu GC et al, Gray Journal (American Journal of Obstetrics and Gynecology), 2001, in
Birmingham, Alabama
Definition of obesity based on BMI
(kg/m2)
<18.5 Underweight
18.5 – 24.9 Normal Weight
25 – 29.9 Overweight
≥ 30 Obese
–30 – 34.9 Class I
–35 – 39.9 Class II
–≥ 40 Class III
Correlates well with fat mass
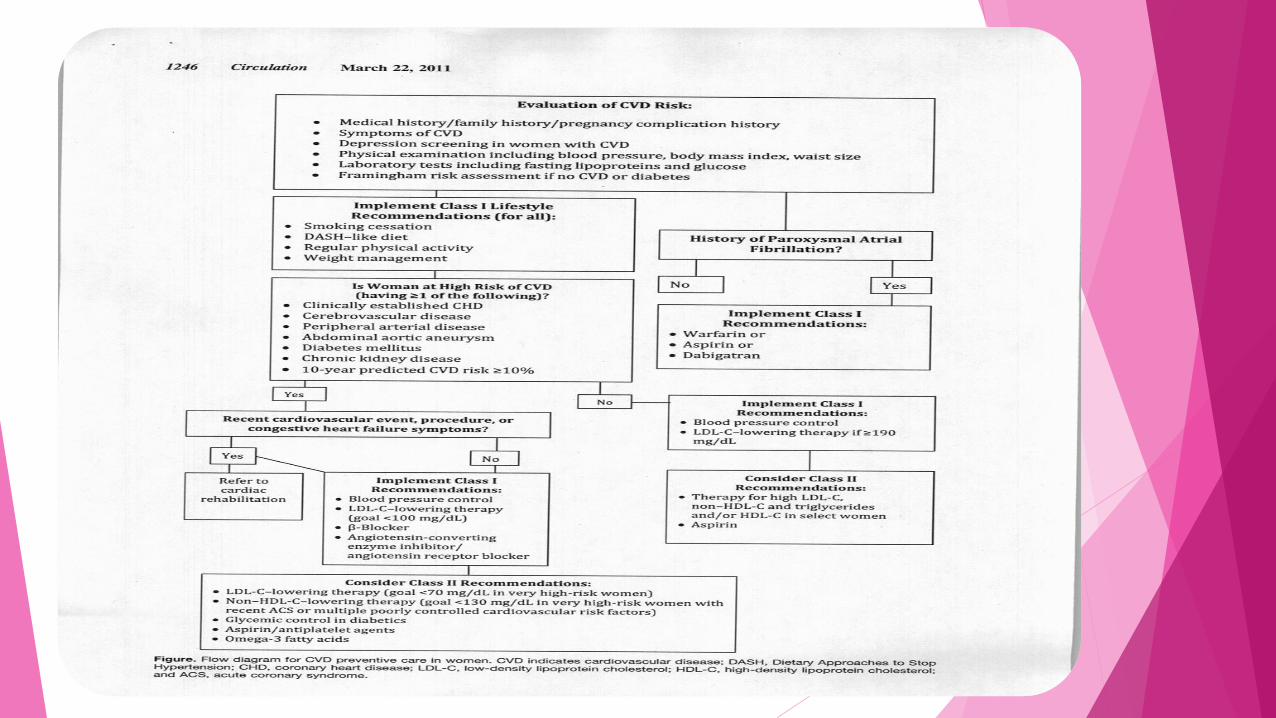
Healthcare professionals who meet women for the first time later in their lives
should take a careful and detailed history of pregnancy complications with
focused questions about a history of gestational diabetes mellitus,
preeclampsia, preterm birth, or birth of an infant small for gestational age
Appropriate referral postpartum by the obstetrician to a primary care physician
or cardiologist should occur so that in the years after pregnancy risk factors can
be carefully monitored and controlled
Nutrition is important for both
short- and long-term health
Barker hypothesis – fetal origins (Twenty years ago, he showed for the first time- that people who had low birth weight are at greater risk of developing coronary heart disease.)
“thrifty phenotype” The thrifty phenotype hypothesis
suggests that early-life metabolic adaptations help in survival of the organism by selecting an appropriate trajectory of growth in response to environmental cues. Recently, some scientists have proposed that the thrifty phenotype prepares the organism for its likely adult environment in long term.

Healthcare professionals who meet women for the first time later in their lives
should take a careful and detailed history of pregnancy complications with
focused questions about a history of gestational diabetes mellitus, preeclampsia,
preterm birth, or birth of an infant small for gestational age
Appropriate referral postpartum by the obstetrician to a primary care physician or
cardiologist should occur so that in the years after pregnancy risk factors can be
carefully monitored and controlled
What is preeclampsia ?
In 2013 ACOG put out a booklet about 40 pages and cited 124
reference articles : Hypertension in pregnancy
They defined preeclampsia as a pregnancy –specific hypertensive
disease with multisystem involvement
Most often at term
Can be superimposed on another hypertensive disorder like CHTN

Preeclampsia
New onset hypertension
New onset of proteinuria
However There can be multisystem organ involvement
Defined as platelet count less than 100,000
Elevated LFT’s ( 2 times the normal )
Renal insufficiency serum creatinine of >1.1
Pulmonary edema
Headache with visual disturbances
Preeclampsia:
Hypertension definitions
Hypertension is defined as greater than 140 systolic and or
a diastolic blood pressure of greater than 90.
Proteinuria is defined as 300 mg/dl protein in a 24 hour
collection or a protein to creatinine ratio on a urine
specimen exceeding 3.0 mg/dl
Hypertension in pregnancy taskforce
2013 terminology recommendations
Use the term preeclampsia without severe features or
Preeclampsia with severe features
We should not use the terms mild preeclampsia or severe
preeclampsia
Hypertension in pregnancy taskforce
2013 recommendations
Chronic hypertension elevated BP’s before pregnancy or before 20 weeks
gestation
Chronic hypertension with superimposed preeclampsia
(preeclampsia occurs 4-5 times higher in this patient group )
Gestational hypertension – new onset BP elevation after 20 weeks
Postpartum hypertension
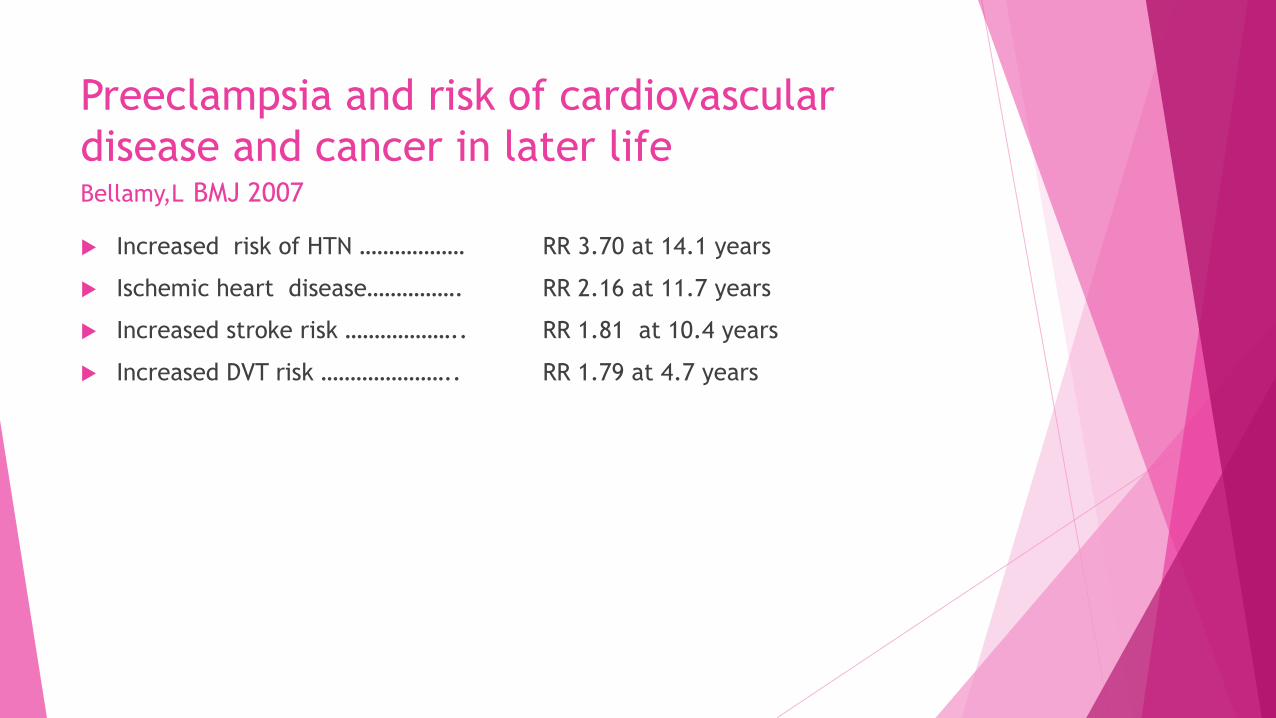
Preeclampsia and risk of cardiovascular
disease and cancer in later life Bellamy,L BMJ 2007
Increased risk of HTN ………………
Ischemic heart disease…………….
Increased stroke risk ………………..
Increased DVT risk …………………..
RR 3.70 at 14.1 years
RR 2.16 at 11.7 years
RR 1.81 at 10.4 years
RR 1.79 at 4.7 years
What Is Relative Risk
The probability of an event occurring
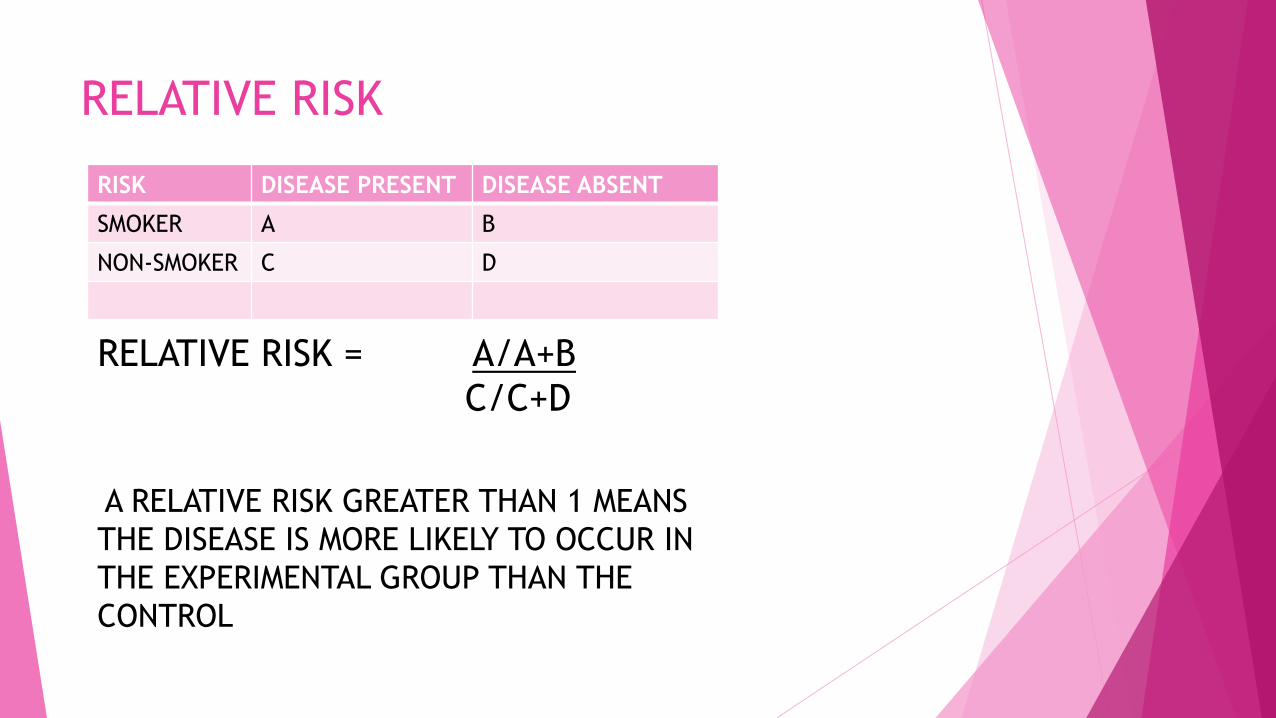
RELATIVE RISK
RISK DISEASE PRESENT DISEASE ABSENT
SMOKER A B
NON-SMOKER C D
RELATIVE RISK = A/A+B
C/C+D
A RELATIVE RISK GREATER THAN 1 MEANS
THE DISEASE IS MORE LIKELY TO OCCUR IN
THE EXPERIMENTAL GROUP THAN THE
CONTROL
PREECLAMPSIA AND CANCER RISK
Overall there was no increased risk of
cancer including breast cancer
17 years after preeclampsia.

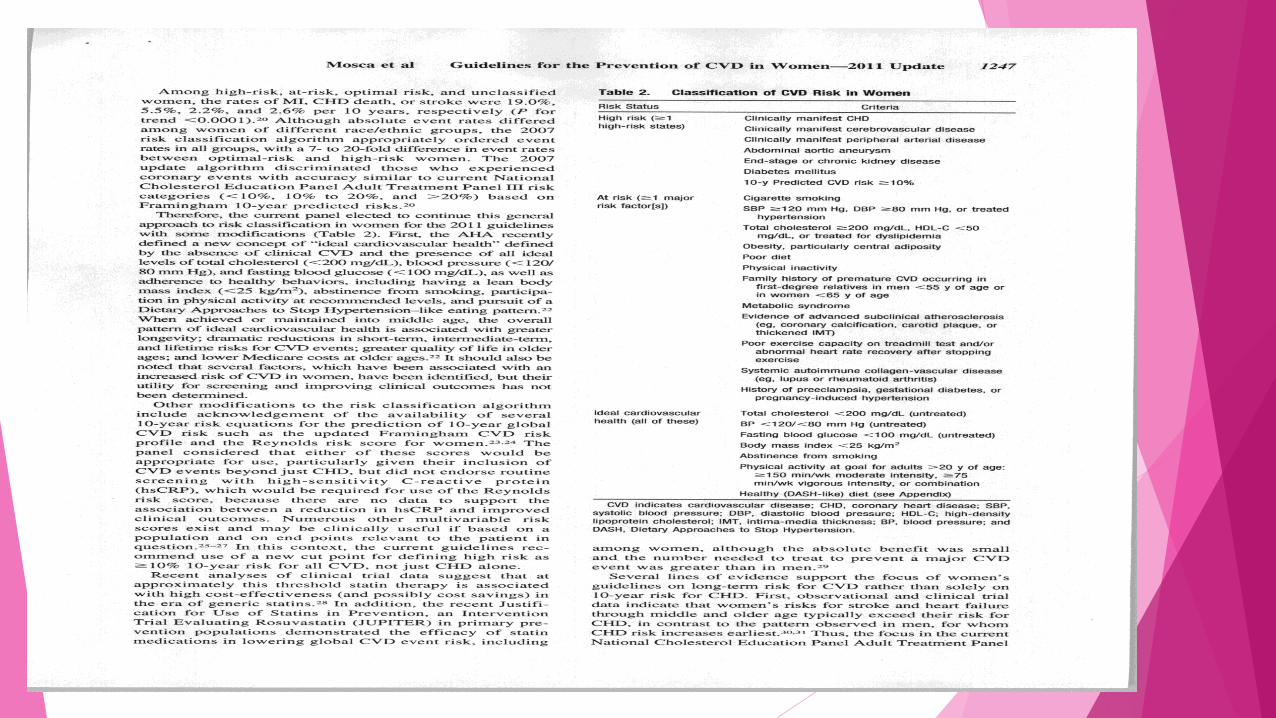
METABOLIC SYNDROME

Metabolic syndrome (aka Syndrome X - dyslipidemia, hypertension,
hyperglycemia commonly cluster together.
This clustering he called Syndrome X)
*ATP III1 identified 6 components of the metabolic syndrome that relate to
CVD:
Abdominal obesity
Atherogenic dyslipidemia
Raised blood pressure
Insulin resistance ± glucose intolerance
Proinflammatory state
Prothrombotic state
*The National Cholesterol Education Program’s Adult Treatment Panel III
report (ATP III)
METABOLIC SYNDROME
35% of woman
Native Americans highest risk at 60% of woman between
45-49
Less than 10% in France, until 60 years of age when risk
hits 18%
Those with the syndrome have the highest risk of heart
disease
Effectiveness-Based Guidelines
for the Prevention of
Cardiovascular Disease in
Women—2011 Update
A Guideline From the American
Heart Association
Published OnLine Feb 16, 2011
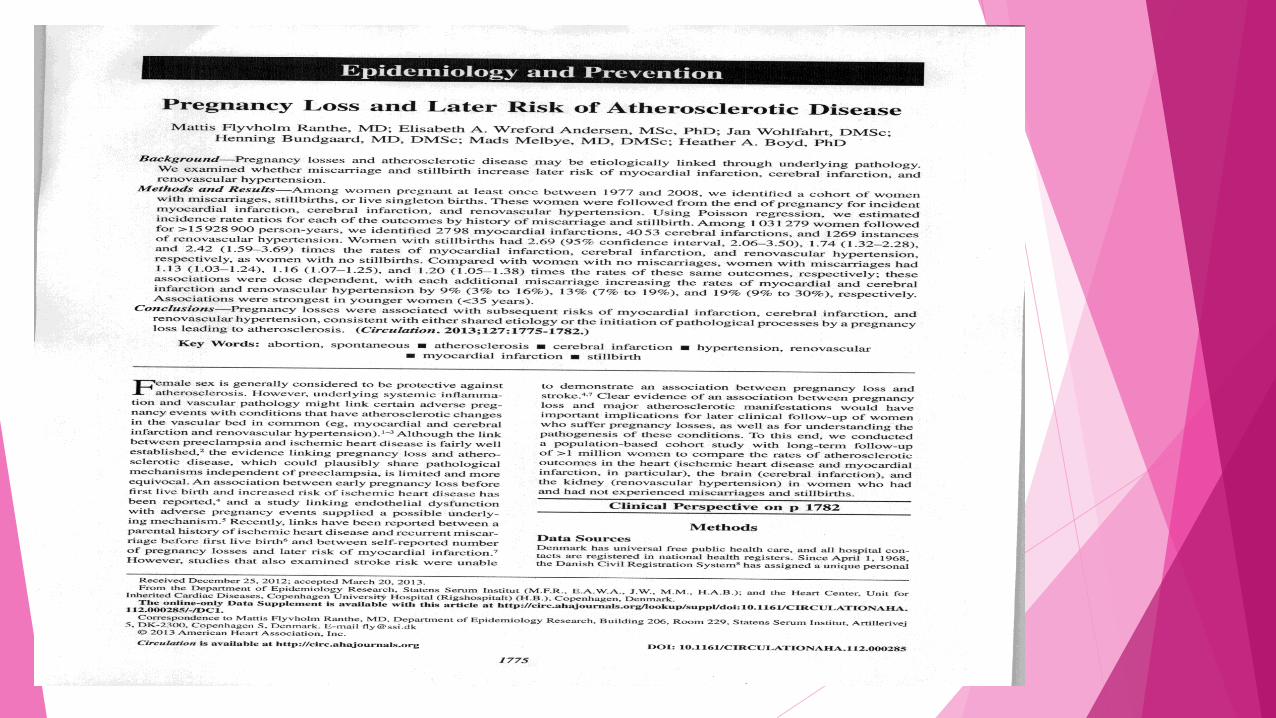
Pregnancy loss and later risk of
atherosclerotic disease circulation 2013
Population based cohort study with long term follow up in Denmark
1997 to 2008 greater than 1 million women studied
> 1 Stillborn then IRR was 2.69 for MI,
1.74 for cerebral infarct ,and
2.42 for renovascular hypertension
> 1 Miscarriage then IRR was 1.13 for MI
1.16 cerebral infarcts
1.20renovascular hypertension
IRR( incidence rate ratios)
Brisbane England 1981 - 1984
8456 Mothers Interviewed 4 times: first prenatal visit
3-5 days after birth
6 months after birth
5 years after birth
Physical exam of the child at 5 years of age
47 % loss to follow up
Results :Smoking ,paternal weight /BMI ,shorter breast fed children all had
higher blood pressure but only 0.92 mmHg
Women's Health
Cardiovascular sequelae of
preeclampsia/eclampsia:
A systematic review and meta-analyses Sarah D. McDonald, MD,
Women's Health
Cardiovascular sequelae of
preeclampsia/eclampsia:
A systematic review and meta-analyses Sarah D. McDonald, MD, MSc,a Ann Malinowski, MSc, MD,b Qi Zhou, PhD,c Salim Yusuf, MD, PhD,d,e
and Philip J. Devereaux, MD, PhDc,d Hamilton, Ontario, Canada am Heart J 2008
Five case-control and 10 cohort studies met eligibility criteria, with
a total of 116,175 women with and
2,259,576 women without preeclampsia/eclampsia.
Cardiovascular sequelae of
preeclampsia/eclampsia:
A systematic review and meta-analyses
Sarah D. McDonald, MD, Hamilton, Ontario
Am Heart J.2008 Relative to women with uncomplicated pregnancies, women with a history of
preeclampsia/eclampsia had an increased risk of:
cardiac disease in both the case-control studies (odds ratio 2.47, 95% CI 1.22-5.01)
and the cohort studies (relative risk [RR]2.33, 1.95-2.78)
increased risk of cerebrovascular disease (RR 2.03, 1.54-2.67)
peripheral arterial disease(RR 1.87, 0.94-3.73),
cardiovascular mortality (RR 2.29, 1.73-3.04).
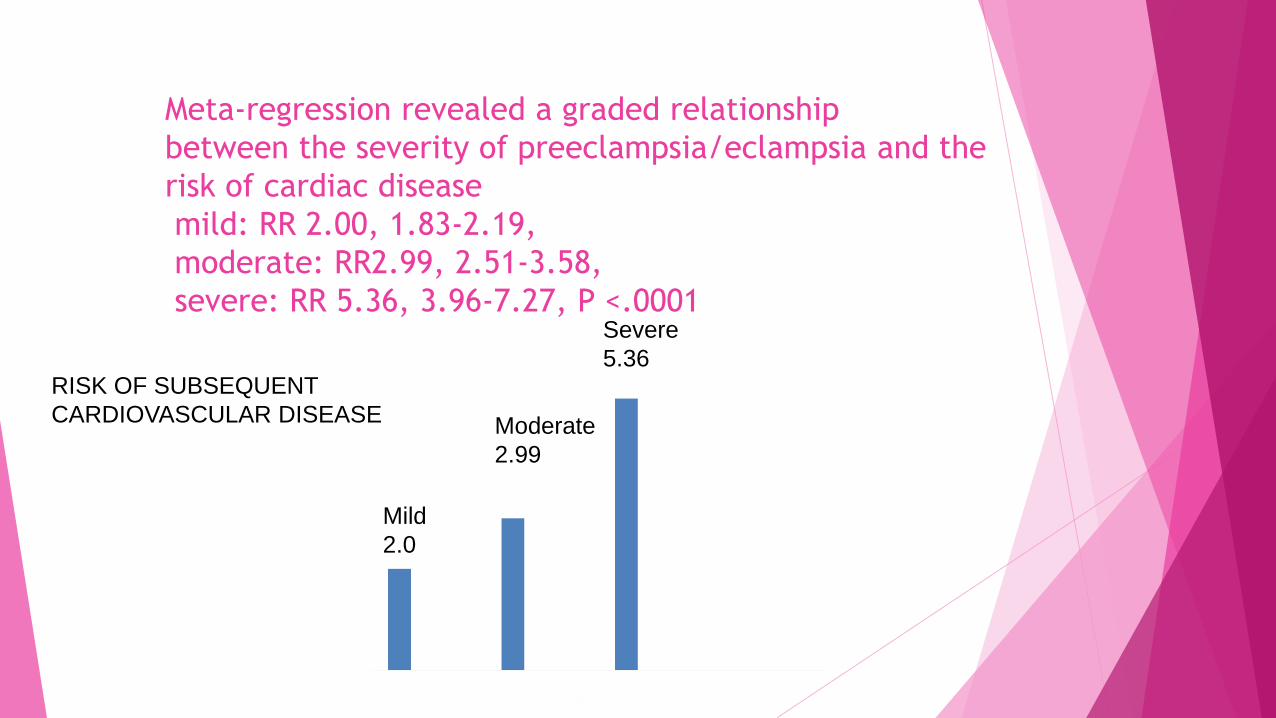
Meta-regression revealed a graded relationship
between the severity of preeclampsia/eclampsia and the
risk of cardiac disease
mild: RR 2.00, 1.83-2.19,
moderate: RR2.99, 2.51-3.58,
severe: RR 5.36, 3.96-7.27, P <.0001
RISK OF SUBSEQUENT
CARDIOVASCULAR DISEASE
Mild
2.0
Moderate
2.99
Severe
5.36
Cardiovascular sequelae of
preeclampsia/eclampsia:
A systematic review and meta-analyses
Sarah D. McDonald, MD, Hamilton, Ontario
Am Heart J.2008
Conclusions
Women with a history of preeclampsia/eclampsia
have approximately double the risk of early cardiac,
cerebrovascular, and peripheral arterial disease, and
cardiovascular mortality. (Am Heart J 2008;156:918-30.)