hydrogel contact lens-induced corneal warpage
TRANSCRIPT

Contact Lens & Anterior Eye 26 (2003) 153–159
Hydrogel contact lens-induced corneal warpage
Muriel Schornack∗Department of Ophthalmology, Mayo Clinic, 200 First Street SW, Rochester, MN 55905, USA
Abstract
Background: Although contact lens-induced corneal warpage is most frequently associated with PMMA lenses, approximately 27%of reported cases of corneal warpage have been attributed to hydrogel lens wear. The change in corneal contour may be the result ofeither mechanical deformation, chronic metabolic insult, or a combination of mechanical and metabolic challenges. Limited oxygentransmissibility through some hydrogel lenses may lead to chronic hypoxia and acidosis. These metabolic challenges can change cornealphysiology sufficiently to cause clinically significant corneal warpage.Case reports: Three cases of hydrogel contact lens-induced cornealwarpage are presented. In all three cases, cessation of lens wear led to restoration of the normal corneal contour and visual acuity. All patientswere refit with more oxygen-permeable lenses, and have successfully resumed wearing contact lenses.Conclusion: Certain individualswho wear hydrogel contact lenses can experience corneal warpage. Clinical signs of corneal warpage include changes in refractive error,decreased visual acuity with spectacle correction, and changes in corneal topography. Serial topography is useful to monitor the cornea toresolution of the condition. Contact lenses with higher oxygen transmissibility will frequently alleviate the relative hypoxia that may beassociated with corneal warpage.© 2003 British Contact Lens Association. Published by Elsevier Science Ltd. All rights reserved.
Keywords: Corneal warpage; Hydrogel contact lenses; Myopic shift; Corneal hypoxia; PMMA contact lenses; Corneal topography
1. Introduction
Contact lenses have long been recognized as a cause ofchange in corneal contour. In 1965, Hartstein coined theterm “corneal warpage” in his report of 12 cases of in-creased astigmatic refractive error after two to six years ofPMMA contact lens wear[1]. Corneal warpage has beenreported with PMMA, rigid gas permeable, and hydrogelcontact lenses. In 1990, Phillips reported eight cases of con-tact lens-induced corneal warpage from his practice, two ofwhich were associated with hydrogel lens wear[2]. Phillipsalso summarized the published case reports of contactlens-induced corneal warpage between 1965 and 1988. Ofthe 473 cases that had been reported in the literature duringthat time period, 343 (72.5%) were associated with PMMAor rigid gas permeable lenses. The remaining 130 cases(27.5%) were associated with hydrogel lenses[2]. In mostof the cases reviewed by Phillips, corneal changes inducedby hydrogel contact lenses returned to normal contour uponcessation of contact lens wear[2]. In 1990, Wilson et al.[3]described contact lens-induced corneal warpage in 21 eyes,five of which had worn hydrogel contact lenses. Most of theeyes in Wilson’s study stabilized with a normal topographicpattern after discontinuing use of contact lenses. However,
∗ Tel.: +1-507-284-3721; fax:+1-507-284-4612.E-mail address: [email protected] (M. Schornack).
an abnormal pattern persisted in five eyes after ceasing lenswear[3].
Even if patients with corneal warpage are asymptomatic[3,4], signs of corneal warpage, such as changes in refractiveerror and distortion of keratometric mires, can be present[3]. This is a report of three cases of hydrogel contactlens-induced corneal warpage in which the patients’ reportsof blurred vision were associated with reduced acuity withbest spectacle correction and abnormal corneal topographyfindings. Corneal warpage resolved in all three patientsafter discontinuation of contact lens wear. All ultimatelyachieved 20/20 spectacle acuity, and were refit into moreoxygen-permeable contact lenses. No signs of recurrentwarpage have been noted in any of the three patients.
2. Case reports
2.1. Case #1
A 25-year-old man presented with a complaint of con-stantly blurred vision with both his glasses and contact lensesfor the previous two months. His spectacles were nine yearsold and the spectacle refraction from his eye examinationtwo years earlier was−2.50 DS OD and−3.25 DS OS.He wore conventional hydrogel lenses (HydronTM, 8.4 basecurve OU,−2.50 DS OD,−2.75 DS OS, 14.0 diameter OU)
1367-0484/$ – see front matter © 2003 British Contact Lens Association. Published by Elsevier Science Ltd. All rights reserved.doi:10.1016/S1367-0484(03)00026-2

154 M. Schornack / Contact Lens & Anterior Eye 26 (2003) 153–159
all waking hours, and reported that he never wore his con-tact lenses while sleeping. He used a generic multipurposesolution to clean his lenses and he enzymed them weekly.The right contact lens was approximately one year old andthe left lens was one month old. He was in good health butreported an increase in frequency of urination over the pastseveral months with no change in appetite or thirst.
The patient’s initial visual acuity with his contact lenseswas 20/20− 1 OD and 20/30 OS. The lenses moved ade-quately, covered the cornea completely and centered well.The over-refraction was+0.50 − 0.50 × 110 OD (20/20)and−0.50− 0.50× 085 OS (20/20− 2). The retinoscopyreflex (after removal of the contact lenses) was irregular andvariable, and the refraction was−3.25 − 1.00 × 170 OD(20/20) and−4.00− 0.25× 022 OS (20/20− 2). Cyclo-plegic refraction was performed to eliminate any possiblecontribution of accommodative spasm to the patient’s re-fractive error and yielded−3.00 DS OD (20/20− 1) and−3.50 DS OS (20/25).
The keratometry mires appeared mildly distorted in botheyes, and the measurements were slightly steeper in bothmeridians of both eyes than measurements taken two yearsearlier. The variation may have been within measurementerror for the technique (Table 1).
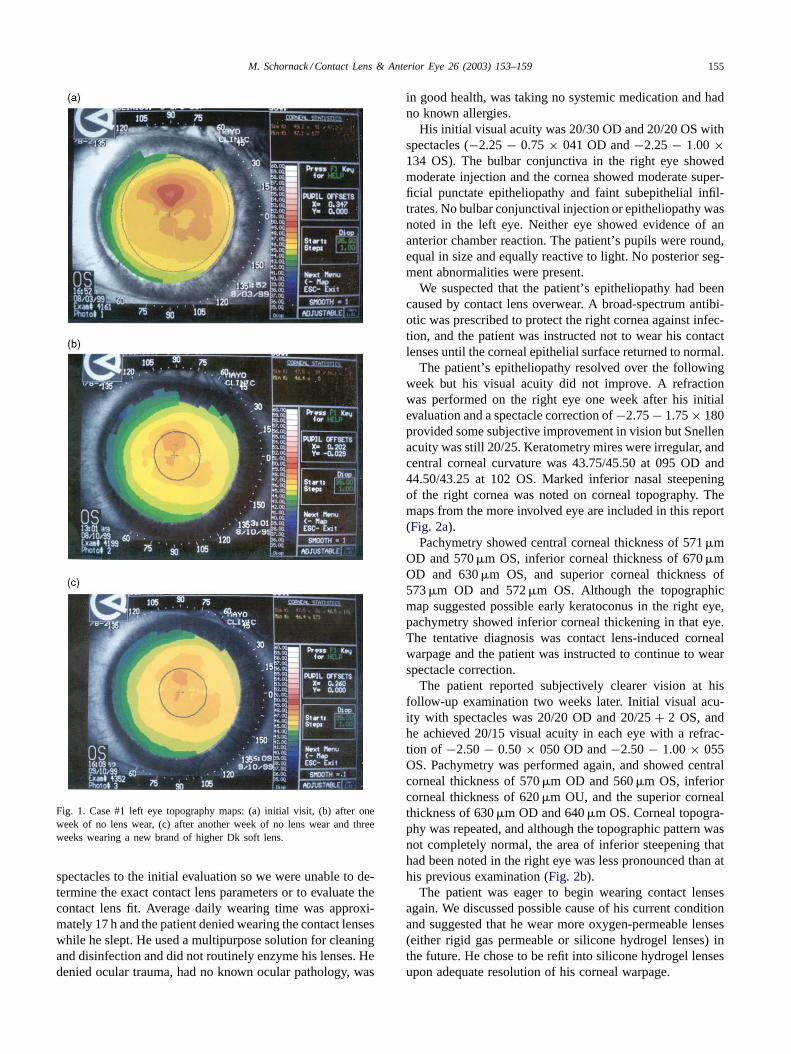
Corneal topography was performed. The results showedsuperior steepening in both eyes with more irregular in theleft eye than the right. The maps from the eye with the moredramatic changes are included in this report (Fig. 1a).
No anterior segment or retinal abnormalities were found.There were no clinical signs of systemic diabetes.
The working diagnosis was probable contact lens-inducedcorneal warpage. We provided a spectacle prescription(post-dilation refraction) and warned the patient that hisspectacle prescription may fluctuate during the next severalweeks. The patient was advised to discontinue contact lenswear and was scheduled to return in one week for follow-upcorneal topography.
At his follow-up examination, the patient reported mildlyblurred distance vision with his new glasses. With spectacles,his visual acuity was 20/25− 1 OD and 20/50 OS. Althoughhis vision was not perfect, he reported adequate vision toperform necessary daily activities. Corneal topography wasrepeated. Superior steepening was still present, but was lesspronounced than at our prior examination (Fig. 1b).
When the patient returned for a second follow-up exami-nation a week later, his distance visual acuity with spectacles
Table 1Keratometry data, Case #1
OD OS Distortion
Previous exam (1997) 44.50/46.75 at 090 45.62/46.62 at 090 Not recordedInitial exam (1999) 45.12/47.00 at 094 46.00/47.25 at 085 Mild OUFollow-up #1 Not recorded Not recorded Not recordedFollow-up #2 45.37/46.62 at 109 45.86/46.62 at 094 None OUFollow-up #3 45.25/46.50 at 090 45.50/46.75 at 090 None OUFollow-up #4 No change from previous exam No change from previous exam None OU
had improved to 20/20 OD and 20/30 OS. The corneal topog-raphy was performed again, and minimal change was notedin the map since the previous week. Best spectacle correctedvisual acuity was 20/20 with−3.00 DS OD and 20/20− 1with −3.75 DS OS. Keratometry mires were crisp and freefrom distortion in both eyes and central corneal curvature atthis visit had flattened somewhat relative to the initial visitfindings, particularly in the vertical meridian (Table 1).
The patient chose to resume wearing contact lenses. Weselected Proclear CompatiblesTM (8.2 base curve,−3.00 DSOD, −3.50 DS OS, 14.2 diameter) and the trial lenses pro-vided visual acuity of 20/20 OD and 20/20− 1 OS. Thelenses covered the cornea completely, centered well andmoved adequately. We gave the patient an updated prescrip-tion for spectacles and scheduled a follow-up appointment torepeat corneal topography and check his new contact lenses.
The patient returned for a third follow-up examinationthree weeks later at which time he reported good comfortand vision with the contact lenses. We measured acuities of20/20 OD and OS and the lenses continued to move, cover,and center well. Keratometry was performed (Table 1), andthe mires were clear and free of distortion OU. Cornealtopography was repeated and showed continuing resolutionof superior corneal steepening (Fig. 1c).
The patient reported good vision and comfort with hiscontact lenses at his fourth follow-up visit three weeks later.His visual acuity with contact lenses was 20/20 in botheyes and the lenses covered the cornea completely, centeredwell, and moved appropriately. The corneas were clear andkeratometric measurements were unchanged from the pre-vious examination. We prescribed contact lenses identicalto the trial lenses initially dispensed. The patient was in-structed to replace his lenses every two months, limit wear-ing time to 12–14 h daily, remove the lenses before sleepingfor any length of time, and clean and disinfect the lenseswith ReNuTM multipurpose solution.
He returned for a general examination one year later with-out ocular or visual complaints. The refraction remained sta-ble, and his vision remained clear (20/15) in both eyes.
2.2. Case #2
A 14-year-old male presented to the emergency serviceand reported a 4-day history of blurred vision and photo-phobia in his right eye. Although the patient habitually woretoric hydrogel lenses (which he replaced monthly), he wore
M. Schornack / Contact Lens & Anterior Eye 26 (2003) 153–159 155
Fig. 1. Case #1 left eye topography maps: (a) initial visit, (b) after oneweek of no lens wear, (c) after another week of no lens wear and threeweeks wearing a new brand of higher Dk soft lens.
spectacles to the initial evaluation so we were unable to de-termine the exact contact lens parameters or to evaluate thecontact lens fit. Average daily wearing time was approxi-mately 17 h and the patient denied wearing the contact lenseswhile he slept. He used a multipurpose solution for cleaningand disinfection and did not routinely enzyme his lenses. Hedenied ocular trauma, had no known ocular pathology, was
in good health, was taking no systemic medication and hadno known allergies.
His initial visual acuity was 20/30 OD and 20/20 OS withspectacles (−2.25− 0.75× 041 OD and−2.25− 1.00×134 OS). The bulbar conjunctiva in the right eye showedmoderate injection and the cornea showed moderate super-ficial punctate epitheliopathy and faint subepithelial infil-trates. No bulbar conjunctival injection or epitheliopathy wasnoted in the left eye. Neither eye showed evidence of ananterior chamber reaction. The patient’s pupils were round,equal in size and equally reactive to light. No posterior seg-ment abnormalities were present.
We suspected that the patient’s epitheliopathy had beencaused by contact lens overwear. A broad-spectrum antibi-otic was prescribed to protect the right cornea against infec-tion, and the patient was instructed not to wear his contactlenses until the corneal epithelial surface returned to normal.
The patient’s epitheliopathy resolved over the followingweek but his visual acuity did not improve. A refractionwas performed on the right eye one week after his initialevaluation and a spectacle correction of−2.75− 1.75× 180provided some subjective improvement in vision but Snellenacuity was still 20/25. Keratometry mires were irregular, andcentral corneal curvature was 43.75/45.50 at 095 OD and44.50/43.25 at 102 OS. Marked inferior nasal steepeningof the right cornea was noted on corneal topography. Themaps from the more involved eye are included in this report(Fig. 2a).
Pachymetry showed central corneal thickness of 571�mOD and 570�m OS, inferior corneal thickness of 670�mOD and 630�m OS, and superior corneal thickness of573�m OD and 572�m OS. Although the topographicmap suggested possible early keratoconus in the right eye,pachymetry showed inferior corneal thickening in that eye.The tentative diagnosis was contact lens-induced cornealwarpage and the patient was instructed to continue to wearspectacle correction.
The patient reported subjectively clearer vision at hisfollow-up examination two weeks later. Initial visual acu-ity with spectacles was 20/20 OD and 20/25+ 2 OS, andhe achieved 20/15 visual acuity in each eye with a refrac-tion of −2.50− 0.50× 050 OD and−2.50− 1.00× 055OS. Pachymetry was performed again, and showed centralcorneal thickness of 570�m OD and 560�m OS, inferiorcorneal thickness of 620�m OU, and the superior cornealthickness of 630�m OD and 640�m OS. Corneal topogra-phy was repeated, and although the topographic pattern wasnot completely normal, the area of inferior steepening thathad been noted in the right eye was less pronounced than athis previous examination (Fig. 2b).
The patient was eager to begin wearing contact lensesagain. We discussed possible cause of his current conditionand suggested that he wear more oxygen-permeable lenses(either rigid gas permeable or silicone hydrogel lenses) inthe future. He chose to be refit into silicone hydrogel lensesupon adequate resolution of his corneal warpage.

156 M. Schornack / Contact Lens & Anterior Eye 26 (2003) 153–159
Fig. 2. Case #2 right eye topography maps: (a) one week after initial visit,(b) after two weeks of not lens wear, (c) after five weeks of no lens wear.
When he returned for examination three weeks later,he reported consistently good vision with his new spec-tacles (20/15 OD and OS). Central corneal curvature was43.50/44.25 at 090 OD and 44.25/43.25 at 130 OS on
keratometry. Corneal topography was repeated, and the to-pography of the right eye was improved (Fig. 2c) with botheyes showing comparable levels of mild inferior steepening.PureVisionTM (balafilcon A) contact lenses were fitted (8.6base curve,−2.75 DS OU, 14.0 diameter) and they moved,covered and centered well, providing 20/20 visual acuity ODand OS. Wearing time was limited to a maximum of 5–6 hper day and to avoid sleeping while wearing contact lenses.
At his follow-up examination one month later, he reportedgood vision and comfort with the lenses. His visual acuitywas 20/20 OD and OS with the contact lenses and the lensesmoved, covered, and centered well. Wearing time was in-creased to 10 h per day and he was encouraged to scheduleregular follow-up examinations.
2.3. Case #3
A 46-year-old woman presented with decreased distanceand near visual acuity with her current contact lenses andspectacles along with decreasing contact lens tolerance. Hercurrent contact lenses and spectacles (−9.00 DS OD,−9.50DS OS with+1.50 add OU) were two years old. She habit-ually wore her conventional hydrogel lenses (AquaflexTM,Vault I, −7.00 DS, 13.8 diameter OU) 16–18 h daily. Sheused a multipurpose solution and did not enzyme her lenses.Her ocular history was unremarkable and she reported goodgeneral health.
Her initial visual acuity with contact lenses was 20/40 ODand 20/30 OS. An over-refraction of−1.00 DS improved theacuity of her right eye to 20/25 and spherical over-refractiondid not improve the left eye’s vision. The contact lensescovered the cornea completely and centered adequately butmoved minimally, even with manual manipulation, and milddeposits were present on both lenses. Her acuity in eacheye was 20/20 with a spectacle refraction (−8.75 − 1.00× 157 OD and−8.25 − 1.00 × 180 OS). Keratometricmeasurement of central corneal curvature was 44.50/46.50at 090 OD and 44.00/45.75 at 090 OS and the mires weremildly distorted for both eyes. Significant inferior steepeningwas identified in both eyes with topography (Fig. 3a and b).
Well-perfused corneal neovascularization extended1.5–2.0 mm centrally from the limbus in both eyes. No ep-itheliopathy was present in either eye and no other anterioror posterior abnormalities were found.
The shift in refractive error and the inferior corneal steep-ening noted on topography were consistent with contactlens-induced corneal warpage. The patient was given herspectacle prescription and was instructed to avoid contactlens wear until her next examination.
The patient reported acceptable vision with her currentspectacles and visual acuity was 20/30 OD and 20/20 OSupon her return one month later. Corneal topography stillshowed significant inferior steepening, however the areasof inferior steepening had narrowed and there was someimprovement in symmetry between inferior and superiorcorneal contour of both eyes. The patient was advised to

M. Schornack / Contact Lens & Anterior Eye 26 (2003) 153–159 157
Fig. 3. Case #3 right (a) and left (b) eye topography maps at initial visit.
continue to wear her spectacles until her next examination(one month later).
At her second follow-up visit (two months after her initialvisit) her refraction was−7.50− 0.50× 005 OD and−8.25DS OS, giving acuity of 20/20 in each eye (Fig. 4a and b).Keratometry mires were clear and free from distortion, andcentral corneal curvature was 43.00/45.50 at 090 OD and43.50/45.50 at 090 OS. Corneal topography showed markedflattening of the inferior quadrant in both eyes compared toher previous examination and the contour of each corneawas more symmetrical in the vertical meridian.
The patient was eager to begin wearing contact lensesagain. We fit her with Focus Night and DayTM (lotrafilcon)lenses (8.6 base curve,−7.00 OD,−7.50 OS, 13.8 diameter)and these provided visual acuity of 20/20 in each eye. Thelenses covered the cornea completely, centered well, andmoved well. She was instructed to wear the lenses no morethan 10 h per day and to use ReNuTM multipurpose solutionfor her lens care.
She returned two weeks later for a contact lens evaluation.Her distance visual acuity with contact lenses was 20/20OD and OS and she was content to wear reading glasses
Fig. 4. Case #3 right (a) and left (b) eye topography maps after twomonths of spectacle lens wear.
over her contact lenses as needed. The contact lenses con-tinued to move, cover, and center well. The corneal neo-vascularization that had been noted at her initial visit wasstill present, but was minimally perfused. Corneal topogra-phy was repeated and showed no change from her previousvisit. The lenses were prescribed and biennial evaluation wasrecommended.
3. Discussion
The cases described above demonstrate contact lens-induced corneal warpage. Most abnormalities in cornealcontour noted upon initial evaluation abated with cessationof lens wear, i.e. mild corneal inequality may have remained.Unfortunately, pre-contact lens topography is not availablefor these patients so we cannot determine whether theircorneas truly returned to baseline contour. In addition toimprovements in corneal topography noted upon cessationof lens wear, clinical observations and patient symptoms

158 M. Schornack / Contact Lens & Anterior Eye 26 (2003) 153–159
were suggestive of contact lens-induced corneal warpage.In Case #1, the keratometry measurements were less than0.50 D steeper in 1999 than in 1997, but the mires were dis-torted. The patient’s inability to achieve clear 20/20 visionthrough any form of correction, in addition to the distortionof the mires of the keratometer, led us to suspect cornealdistortion. In the second case, persistently decreased visionin the right eye after the resolution of epitheliopathy andanterior stromal infiltrates led us to suspect corneal distor-tion. The myopic and astigmatic shift of refractive errorand mildly distorted keratometric mires in Case #3 weresuggestive of corneal warpage. In all three cases, cornealtopography findings assisted in making the diagnosis ofcorneal warpage and allowed us to monitor corneal changesduring the resolution of the warpage.
Corneal topography may also allow us to identify abnor-malities in corneal curvature before patients become visu-ally symptomatic. Ruiz-Montenegro et al.[4] studied alter-ations in corneal topography in asymptomatic persons withnormal vision and found that PMMA, rigid gas permeableor hydrogel lenses can induce topographic abnormalities.Differences in the surface asymmetry index and surface reg-ularity index in the daily wear hydrogel contact lens andcontrol groups were not statistically significant. However,Ruiz-Montenegro reported that contact lens wearers weremore likely than controls to have abnormal corneal topog-raphy (irregular astigmatism, lack of central radial symme-try, or progressive steepening of the curvature from centralto peripheral cornea)[4]. Collection of topographic imagesprior to the initiation of contact lens wear would give thecontact lens practitioner baseline data on corneal contour.Regular topographic evaluation of contact lens wearers mayallow the practitioner to detect early signs of corneal stressand identify patients at risk of developing visually signifi-cant corneal warpage. This would allow for earlier and ap-propriate intervention and management.
Hypoxia associated with hydrogel lens wear may be afactor in the development of corneal warpage. If the lensdoes not allow for delivery of oxygen to the cornea andthe diffusion of carbon dioxide away from the cornea, thecornea may become acidotic. Acidosis has been associatedwith endothelial polymegathism, epithelial microcysts, com-promised epithelial junctional integrity, increased epithelialfragility, corneal edema, striate lines, and infiltrative ker-atitis [5]. In 1984, Holden and Mertz[6] reported that adaily wear hydrogel lens needed a Dk/L of at least 20–24to avoid inducing edema. Sweeney[7] described “cornealexhaustion syndrome” in 1992 when she presented severalcases in which patients that had worn PMMA or thick hy-drogel lenses developed corneal edema and contact lens in-tolerance. She theorized that contact lenses with low oxygentransmissibility led to reduction in endothelial cell functionas well as accumulation of carbon dioxide in the corneal ep-ithelium and anterior stroma. The resultant hypoxic and aci-dotic corneal environment led to mild edema and disruptionof normal stromal architecture.
We cannot determine with certainty the etiology ofcorneal warpage in the series of patients presented here,however several aspects of each case lead us to suspectmetabolic challenge. Patient #1 was originally wearinglow-minus HydronTM lenses, which have a Dk of 8.4 anda Dk/L of 14, well below the minimum recommended byHolden and Mertz. The center thickness of the lens is just0.06 mm, so it is unlikely that the lens would mechanicallycause significant corneal deformation. The exact param-eters of the lenses worn by Patient #2 are unknown, butthe patient did report that he wore toric lenses. The in-creased inferior thickness of prism ballasted toric lensescan lead to relative inferior hypoxia[8]. If our patient’slenses were a prism ballast design, relative inferior hypoxiacould potentially account for the inferior edema measuredby pachymetry. The epitheliopathy noted on initial exam-ination could have been due to mechanical stress on thecornea, however the epithelial compromise and mild infil-trative keratitis could have also been a result of hypoxia[5].The corneal neovascularization of Patient #3 suggests somedegree of chronic hypoxia was present. She originally woreAquaflexTM lenses, which had a Dk/L of 15.5 and a centerthickness of 0.06 mm. The combination of low Dk/L lensmaterial, thin lens design and presence of neovasculariza-tion allow for metabolic challenge to be a likely explanationfor the changes noted in her corneal topography.
Given the presumed metabolic etiology of these casesof hydrogel-induced corneal warpage, our managementconsisted of refitting patients to lenses with higher oxygentransmissibility upon resolution of topographic abnormal-ities. In Case #1, the patient was refit from a low water(38%) nonionic lens with a center thickness of 0.06 and aDk value of 8.4 into a high water (62%) nonionic lens witha center thickness of 0.065 and a Dk value of 34.0. Siliconehydrogel lenses, which have Dk values of 110 (balafilconA) or 175 (lotrafilcon) were not available at the time ofPatient #1’s presentation, but have since proven to be veryuseful in similar cases. In Case #2, the patient was refit intobalafilcon lenses. Lotrafilcon lenses were prescribed forPatient #3. Silicone hydrogel lenses are slightly stiffer thanother disposable lenses, so if the original cause of cornealwarpage was mechanical rather than metabolic insult, sili-cone hydrogels may actually cause more deformation thanregular hydrogel lenses. As a positive factor related to in-creased modulus of elasticity, the increased modulus mayhave allowed Patient #2 to achieve clear 20/20 vision withspherical lenses in spite of mild astigmatic refractive error.We will follow these patients closely to monitor for anysigns of recurrent topographic abnormalities.
These cases also clearly illustrate the value of cornealtopography in contact lens practice. Most contact lens prac-titioners routinely assess central corneal curvature withkeratometry on their patients. In addition to providing ameasurement of the cornea’s radius of curvature, keratom-etry allows the practitioner to detect any central cornealdistortion but one of the limitations of keratometric corneal

M. Schornack / Contact Lens & Anterior Eye 26 (2003) 153–159 159
assessment is that curvature is only measured in fourparacentral points. Consequently, peripheral distortion andirregular astigmatism are difficult to detect with a keratome-ter alone. Corneal topography gives the practitioner a muchmore complete picture of the entire cornea’s contour. Astopographers become more widely available, they may beused more routinely in the care and management of contactlens patients. Clinical studies to define the range and typesof normal topographic variation in patients who do not wearcontact lenses and in asymptomatic contact lens wearerswould be helpful as the use of topographers becomes morecommonplace in contact lens practice.
4. Conclusion
The overall visual prognosis for patients who experi-ence contact lens-induced corneal warpage is excellent.Although cases of permanently decreased spectacle acuitywith PMMA or rigid gas permeable contact lens-inducedcorneal warpage have been reported[2,3], there has beenno report of permanently reduced spectacle acuity follow-ing hydrogel-induced warpage. All three of the patientsdescribed above attained 20/20 or better visual acuity uponstabilization of corneal topographic patterns.
Patients who have experienced contact lens-inducedcorneal warpage should be monitored closely. Any changesin refractive error and corneal curvature (measured by bothkeratometry and corneal topography) should be noted. Iffurther signs of corneal stress are noted, patients shouldeither be refit into more oxygen-permeable lenses, limitcontact lens wear or possibly even discontinue contact lensuse in extreme cases.
5. Clinical implications
Hydrogel induced corneal warpage is a real phenomenonseen in an everyday contact lens practice. Severe forms aresuspected and detected when a significant shift in refrac-
tive error occurs, or when best corrected spectacle acuityis reduced. The early detection of soft lens-induced cornealwarpage will be easily accomplished with the use of rou-tine corneal topography which many practices have alreadyincorporated into the everyday management of contact lenspatients. I predict the regular use of corneal topographyfor average contact lens patients will continue to increaseas these instruments become the gold standard in the mea-surement of the corneal surface. Slit-scanning instruments,such as Bausch & Lomb’s Orbscan II, can take this assess-ment one step further, by immediately differentiating contactlens-induced corneal warpage from a corneal ectasia withthe incorporation of pachometry measurements.
Loretta B. Szczotka, OD, MS, FAAODepartment of Ophthalmology
University Hospitals of Cleveland andCase Western Reserve University
Cleveland, OH
References
[1] Hartstein J. Corneal warping due to wearing of corneal contact lenses:a report of 12 cases. Am J Ophthalmol 1965;60:1103–4.
[2] Phillips CI. Contact lenses and corneal deformation: cause, correlate,or coincidence? Acta Ophthalmol 1990;68:661–8.
[3] Wilson SE, Lin DTC, Klyce SD, Reidy JJ, Insler MS. Topographicchanges in contact lens-induced corneal warpage. Ophthalmology1990;97:734–44.
[4] Ruiz-Montenegro J, Mafra CH, Wilson SE, Jumper JM, Klyce SD,Mendelson EN. Corneal topographic alterations in normal contactlens wearers. Ophthalmology 1993;100(1):128–34.
[5] Liesegang TJ. Physiologic changes of the cornea with contact lenswear. CLAO J 2002;28(1):12–27.
[6] Holden BA, Mertz GW. Critical oxygen levels to avoid corneal edemafor daily and extended wear contact lenses. Invest Ophthalmol VisSci 1984;25:1161–7.
[7] Sweeney DF. Corneal exhaustion syndrome with long-term wear ofcontact lenses. Optom Vis Sci 1992;69(8):601–8.
[8] Westin EJ, McDavid K, Benjamin WJ. Inferior cornealvascularization associated with extended wear of prism-ballasted torichydrogel lenses. Int Contact Lens Clin 1989;16(1):20–3.