housekeeping - aamc • submit typed ... reduces the amount of paper documentation that must be sent...
TRANSCRIPT

Housekeeping
• Submit typed questions through the Q&A panel. Send to All Panelists.
• If you experience technical issues, Type a message in the Chatpanel to AAMC Meetings.
• You will not hear any audio until the webinar begins.
• To join the audio, select “call me” and enter your phone number or select “I will call in”.
• If you select “I will call in, follow the prompts and be sure to enter the access code and “Attendee ID”.

CY2017 Medicare Outpatient Prospective Payment System (OPPS) Proposed Rule
Contact:Ivy Baer, [email protected] Cox, [email protected] Mullaney, [email protected] Wetzel, [email protected] Xu, [email protected]
August 2, 2016

CY 2017 OPPS Proposed Rule
Published in the Federal Register on July 14, 2016, at page 45604
Available at: https://www.gpo.gov/fdsys/pkg/FR-2016-07-
14/pdf/2016-16098.pdf
Comments due:
September 6, 2016
AAMC OPPS Resources: www.aamc.org/hospitalpaymentandquality

TODAY’S TOPICS
• Section 603
• Packaging Policies
• New comprehensive APCs (C-APCs)
• Transplant & Organ Procurement
• EHR Meaningful Use
• Quality Reporting Program

Payment Update
Payment rate increase by conversion factor adjustment of 1.55%
Based on IPPS market
basket percentage:
+2.8%
Productivity Adjustment:
-0.5%
Statutory Reduction:
-0.75%
• Impact on All
Hospitals: +1.7%
• Impact on Major
Teaching
Hospitals: +1.2%

§603 of Bipartisan Budget Act of 2015

§603 of the Bipartisan Budget Act of 2015
Made significant changes to OPPS payment for remote HOPDs:
• After 1/1/2017, no OPPS payment for items and services furnished by an off campus outpatient department of a hospital if that OPD had not billed under OPPS prior to November 2, 2015, except if furnished by a dedicated ED
• Payment to be made under an “applicable payment system” as of January 1, 2017

§603 of the Bipartisan Budget Act
Dedicated Emergency Department (ED)
On-Campus Location
Within 250 yards of the main campus
Defines “excepted items and services” as those services
furnished on or after January 1, 2017 in:

When Can No Longer Bill Under OPPS
Relocation of Off-Campus PBDsOff-campus PBDs will lose excepted status if move or relocate from physical
address that was listed on hospital enrollment form as of November 1, 2015; possible
exception to be developed for disaster/extraordinary circumstances.
Expansion of Clinical Family of
Services at an Off-Campus PBDIf add new “clinical families” of services after November 2, 2015, wont be paid under
OPPS
Change of Ownership Excepted status transferred to new ownership only if ownership of the main
provider is also transferred and the Medicare provider agreement is accepted
by the new owner
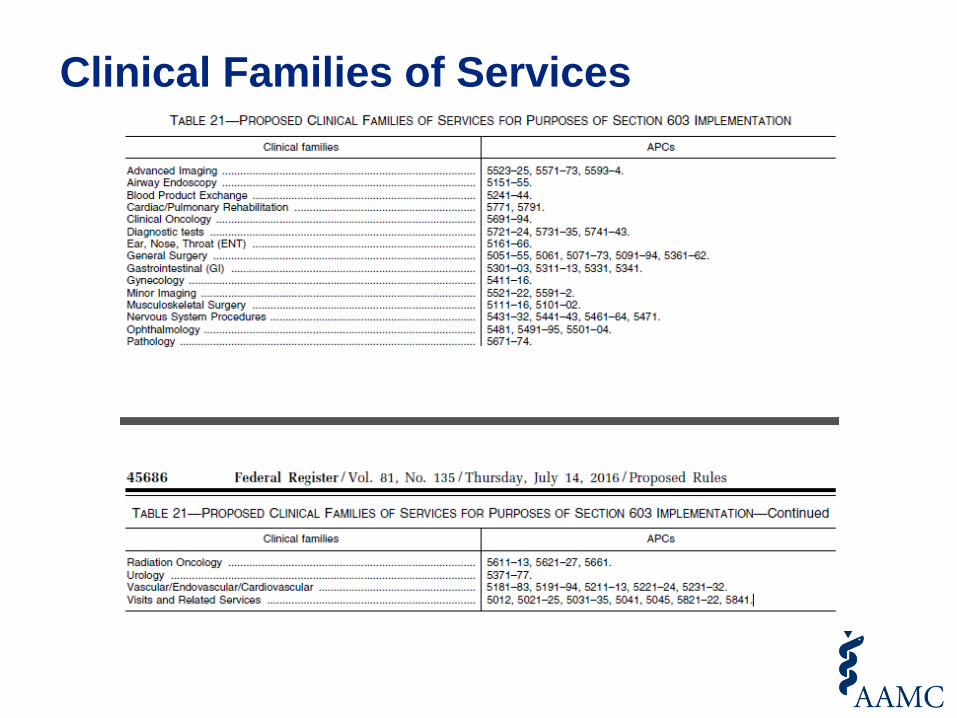
Clinical Families of Services

What’s the “Applicable Payment System”?
• If not excepted, no payment under OPPS in 2017
• Could qualify as an ASC or a CMHC, but then no 340B and time lag to qualify
• For 2017: non-facility rate under physician fee schedule
• Will be paid to physicians—no payment to hospitals
• Hospital can bill for services not paid under OPPS, such as labs that are not packaged

2018
When CMS hopes to be ready to with an “applicable payment system”

Impact on 340B
• Under 340B HRSA requires that the clinic be reported as a reimbursable cost center on the hospital’s cost report
• ASCs and CMCHs wouldn’t qualify
• Must ask CMS to confirm that PBDs will still be reported as reimbursable cost centers
• Remember: legislation only changes payment

If the rule is finalized as proposed
What to do:
• Submit an amended Medicare provider enrollment form for these locations; submit voluntary attestation to MAC that PBDs meet the provider-based requirements
• Keep track of costs
• Submit bills (they will not be paid; you want to build the case for the costs you incurred)

§603: AAMC Concerns
AAMC Concerns
• Untenable to not pay hospitals for services in PBDs in 2017
• Very narrow reading of statute: can’t relocate or expand services without losing HOPD status
• Same outpatient department may be paid under OPPS for some services, “alternative payment system” for others
• Impact on 340B Drug Pricing Program

Packaging Policies

Proposed New Packaging Policy
CMS continues to expand packaging policy:
• Lab tests: package all lab tests on the same claim, even when a lab test is ordered for a different purpose by a different practitioner (vs. current policy that allows separate payment for unrelated lab tests)
• Services with Conditional Packaging Status Indicator Q1 or Q2: expand conditional packaging policy from same date of service to same claim.

Expanded Lab Packaging
No separate payment for unrelated lab tests on the same claim
Discontinue reporting “L1” code
Expanded exemptions: All advanced diagnostic lab tests (vs. current policy of excluding all molecular pathology tests and preventive lab tests)
TBD as defined in section 1834A(d)(5)(A))

Q1/Q2 Conditional Packaging Services
Expand Q1 and Q2 conditional package policy from on the same date of service to on the same claim
> 800 codes with status indicator Q1 or Q2
e.g. various X-ray exams, certain ultrasound exams, and various pathology tests
Package Q1 services when on the same claim with S, T, or V procedures; Q2 with T procedures
For details of codes with status indicator Q1/Q2, please refer to the Addendum B table on the CMS 2017 OPPS website

New Comprehensive APCs

Comprehensive-APCs
Package payment for all
adjunctive services and
procedures into the most costly
primary procedure (J1 status
indicator code)
• When more than 1
primary procedure, pay
only the most expensive
procedure
• Complexity adjustment for
certain pairs of primary
procedures
Primary Care
Service
Adjunctive services
Adjunctive Procedures
Secondary Services
Secondary Items

New Comprehensive-APCs
2015
• Implemented 25 C-APCs
2016
• Finalized 10 additional C-APCs
2017
• Proposing 25 additional new C-APCs
• https://www.gpo.gov/fdsys/pkg/FR-2016-07-14/pdf/2016-16098.pdf(p. 45621-45622)

Comprehensive-APCs
• For 2017, CMS not proposing extensive changes to the already established methodology used for C-APCs
C-APC methodology made effective in CY 2015 No
Change
Defining the services assigned to C-APCs as primary
services or a specific combination of services performed in
combination with each other
No
Change
Following the C-APC payment policy methodology of packaging all
covered OPD services on a hospital outpatient claim reporting a
primary service that is assigned to status indicator “J1” or reporting
the specific combination of services assigned to status indicator
“J2”, excluding services that are not covered OPD services or that
cannot by statute be paid under the OPPS
No
Change

Transplant & Organ Procurement

Organ Transplant
CMS proposes to change performance thresholds in order to decrease the number of unused, recovered organs.
• Increases the observed to expected (O/E) ratio of patient deaths and graft failures to 1.85 (up from 1.5) for solid organ transplant programs
CMS may explore other approaches in the future and focus on optimizing effective use of available organs instead of adjusting CMS outcomes thresholds

Organ Procurement
CMS makes several proposals in order to ensure more consistent requirements with Organ Procurement Organizations
Revises the definition of “eligible death” to include donors up to age 75 and changes clinical criteria for donors with multi-system organ failure
Aligns regulations on aggregate donor yield for OPO outcome performance measures to align with Scientific Registry of Transplant Recipients
Reduces the amount of paper documentation that must be sent to a receiving transplant center

EHR Meaningful Use

EHR Meaningful Use
• CMS proposal: In 2016, EHR reporting period is any continuous 90-day period in CY 2016 for EPs, eligible hospitals, and CAHs that have not successfully demonstrated meaningful use in a prior year (new participants) and the full CY 2016 for EPs, eligible hospitals, and CAHs that have successfully demonstrated meaningful use in a prior year (returning participants).
• EPs and eligible hospitals
90-Day Reporting Period
**Does not apply to state Medicaid EHR Incentive Program
New Participants
• Continuous 90-day period in CY2016 and applies for 2017 and 2018 payment adjustment years
Returning Participants
• Reporting period is full CY 2016 and applies for the 2018 adjustment year

EHR Meaningful Use
• CMS proposes to reduce a subset of thresholds for eligible hospitals attesting under the Medicare EHR Incentive Program
• In 2017 for Modified Stage 2
• View Download Transmit (VDT): from 5% to at least one patient
• In 2017 and 2018 for Stage 3
• Patient Electronic Access to Health Information
• Patient Access: from more than 80% to more than 50%
• Patient-Specific Education: from more than 35% to more than 10%
• Coordination of Care
• VDT: from more than 5% to at least one patient
• Secure Messaging: from more than 25% to more than 5%
• Health Information Exchange
• Patient Care Record Exchange: from more than 50% to more than 10%
• Request/Accept Patient Care Record: from more than 40% to more than 10%
• Clinical Information Reconciliation: from more than 80% to more than 50%
• Public Health and Clinical Data Registry Reporting
• Any combination of six measures to any combination of three measures
Reduced Thresholds
**Does not apply to state Medicaid EHR Incentive Program
Questions?
Submit typed questions
through the Q&A panel.
Send to All Panelists.

31
Proposed Quality Metrics for OQR and VBP

Quality Measures/Programs in the CY 2017 Proposed Rule
Outpatient Quality Reporting (OQR) Program CY 2020:
• Seven new measures proposed:
Two measures assessing hospital visits following outpatient chemotherapy treatment and surgery
5 Outpatient and Ambulatory Surgery (OAS) Consumer Assessment of Healthcare Providers and Systems (CAHPS) survey questions
• No measures proposed for removal
Hospital Value Based Purchasing (VBP) Program FY 2018
• Change to HCAHPS pain management related questions for VBP
32

Hospital Outpatient Quality
Reporting (OQR) Program
33

Admissions and ED Visits Following Outpatient Chemotherapy (OP-35)
• Calculates rates of inpatient admissions and ED visits within 30 days following chemotherapy.
• Performance period = CY 2018; Payment determination = CY 2020
• Claims based measure
• Includes chemotherapy for all cancers, except Leukemia
• Patients attributed to HOPD that administered Chemotherapy
• Not NQF adjusted; Not SES adjusted; MAP conditionally supported (based on NQF endorsement and SES trial period review).
34

Admissions and ED Visits Following Outpatient Chemotherapy (OP-35), Cont.
Hospitals will have two separate rates calculated for patient visits following chemotherapy
35
Inpatient
admissions
ED visits*
Hospital Score OP-35
*ED visits involve: anemia, dehydration, diarrhea, emesis,
fever, nausea, neutropenia, pain, pneumonia, sepsis

Hospital Visits After Outpatient Surgery (OP-36)
• Calculates single rate of inpatient admissions, ED visits, and observation stays within 7 days of outpatient surgery
• Performance period = CY 2018; Payment determination = CY 2020
• Claims based measure
• NQF endorsed; Not SES adjusted; MAP approved (but noted that SES should be considered)
36

Hospital Visits After Outpatient Surgery (OP-36), Cont.
Hospitals will have a single rate calculated for patient visits following outpatient surgery
37
Inpatient
admissions
ED visits
Hospital Score OP-36
Observation
stays

Outpatient Patient Experience Survey
Outpatient and Ambulatory Surgery Consumer Assessment of Healthcare Providers and Systems (OAS CAHPS) Survey proposed for CY 2020
38
OAS CAHPS contains 37 questions
5 of these questions proposed for OQR
These 5 include 3 composite measures:
Each composite contains at least 6 additional
questions, and 2 global rating questions

Outpatient Patient Experience Survey, Cont.
OAS Question Topics:
39
Pain Related Questions [Communications Domain]
HOPD’s not
scored on this
question

Outpatient Patient Experience Survey, Cont.
• Performance period = CY 2018; payment determination = CY 2020
• Demographic information is collected on survey
• Not NQF endorsed
• OAS CAHPS Survey (and all OQR program measures) are pay-for-reporting
• CMS requests feedback on pain related questions
• CMS started voluntary national submission of OAS CAHPS Survey in January, 2016
40

Additional OQR Related Information
• CMS seeks feedback on eCQM opioid measure (not proposed)
• Extension of extraordinary circumstances deadline from 45 to 90 days
• Clarification regarding appeals: hospitals that fail to submit a timely reconsideration request will not be eligible to appeal with Provider Reimbursement Review Board
41

Hospital Value Based
Purchasing (VBP) Program
42

Proposed Removal of HCAHPS Pain Management Questions from VBP
• Starting FY 2018, CMS proposes to exclude three HCAHPS pain management related questions from VBP performance
• Change is a response to opioid epidemic
• Pain management questions would remain on HCAHPS and would continue to be publicly reported
• CMS currently working on alternative pain management question language
• AAMC previously supported legislation that would achieve this goal
43

AAMC Quality Resources Individual Institution Reports
• AAMC Hospital Compare Benchmark Report ([email protected])
• AAMC Quality Report ([email protected])
• AAMC Impact Report ([email protected])
General Resources
• AAMC IPPS & OPPS Regulatory Page -Contains previous OPPS webinars and comment letters (www.AAMC.org/hospitalpaymentandquality)
• AAMC Quality Spreadsheet – Updated (https://www.aamc.org/download/412838/data/aamcqualitymeasuresspreadsheet.xlsx)
44

Questions?
Submit typed questions
through the Q&A panel.
Send to All Panelists.
