harnessing regulatory t cells for the therapy of lupus and...
TRANSCRIPT

385ISSN 1750-743XImmunotherapy (2009) 1(3), 385–40110.2217/IMT.09.2 © 2009 Future Medicine Ltd
Review
Harnessing regulatory T cells for the therapy of lupus and other autoimmune diseases
Breakdown of immunologic self-tolerance that usually controls self and nonself discrimination results in the development of autoimmune dis-eases. Therefore, the elucidation of regulatory mechanisms is of great importance for protection against the generation of self-directed immune responses and, consequently, the i nitiation of autoimmune diseases.
Systemic lupus erythematosus (SLE) is an autoimmune disease characterized by increased production of autoantibodies and systemic clinical manifestations. The disease may involve nearly every organ. T and B cells play a role in the development of SLE. Treatment for SLE, as for most autoimmune diseases, relies on the use of corticosteroids and immunosuppressive drugs that are nonspecific and can cause adverse effects [1]. In spite of intensive efforts, no new treatments have been approved for SLE for over 30 years. Thus, there is an unmet need for novel therapeutic means that will be specific, with improved efficacy and lower toxicity than the currently available therapies for SLE.
A central mechanism of peripheral tolerance involves the active suppression of autoimmune responses by T cells with regulatory capacity [2]. Hundreds of publications discussing regulatory
T cells (Tregs) over the past few years have indi-cated the existence of this unique T-cell lineage with the capacity to regulate auto immunity. It is now evident that Tregs consist of heterog-enous populations of CD4+ and CD8+ cells. The subset of Tregs that has generated the highest level of interest among researchers is that of CD4+CD25+ cells. These cells consist of thymus-derived, naturally occurring Tregs and peripherally induced Tregs that are similar phenotypically and functionally. CD4 Tregs are decreased in number and/or function in subjects with an active SLE disease; however, functional regulatory cells were shown to be upregulated following treatment and clini-cal improvement. Similarly, a crucial role has been demonstrated for Tregs in a number of murine models of SLE. Thus, the possibility of therapeutic intervention using Tregs of rel-evant specificity in SLE is very attractive and the induction of antigen-specific functional Tregs utilizing various approaches is achievable. Therefore, a better understanding of the vari-ous developmental pathways and mechanism of action of Tregs is of utmost importance and may lead to the development of novel specific strategies for the treatment of SLE.
Regulatory T cells (Tregs) maintain immunological homeostasis and prevent autoimmunity. The depletion or functional alteration of Tregs may lead to the development of autoimmune diseases. Tregs consist of different subpopulations of cells, of which CD4+CD25+Foxp3+ cells are the most well characterized. However, CD8 Tregs also constitute a major cell population that has been shown to play an important role in autoimmune diseases. This review will discuss the role of Tregs in autoimmune diseases in general and specifically in systemic lupus erythematosus (SLE). SLE is a multisystem autoimmune disease characterized by the production of autoantibodies against nuclear components and by the deposition of immune complexes in the kidneys as well as in other organs. Abnormalities in Tregs were reported in SLE patients and in animal models of the disease. Current treatment of SLE is based on immunosuppressive drugs that are nonspecific and may cause adverse effects. Therefore, the development of novel, specific, side effect-free therapeutic means that will induce functional Tregs is a most desirable goal. Our group and others have designed and utilized tolerogenic peptides that ameliorate SLE manifestations in murine models. Here, we demonstrate the role of CD4 and CD8 Tregs, as well as the interaction between the two subsets of cells and the mechanism of action of the tolerogenic peptides. We also discuss their therapeutic potential for the treatment of SLE.
Keywords: apoptosis n autoimmune disease n autoreactive T cell n peptide-induced regulatory T cell n regulatory T cell n systemic lupus erythematosus n tolerance induction n tolerogenic peptide
Amir Sharabi1 & Edna Mozes1†
†Author for correspondence: 1Department of ImmunologyThe Weizmann Institute of Science, Rehovot 76100, IsraelTel.: +972 8934 3646Fax: +972 8934 [email protected]
For reprint orders, please contact: [email protected]

Immunotherapy (2009) 1(3)386 future science group
Review Sharabi & Mozes
role of T cells in the pathogenesis of lupus & other autoimmune diseasesThe concept that many organ-specific auto-immune diseases are T-cell mediated is well established. Thus, Type 1 diabetes mellitus (DM) in patients and in nonobese diabetic (NOD) mice, which are extensively studied as a spontaneous model of the disease, was reported to be T-cell mediated [3,4]. Similarly, multiple sclerosis (MS) is mainly a T-cell-mediated dis-ease, as is its animal model – experimental auto-immune encephalomyelitis (EAE) – which is an inflammatory demeyelinating disease mediated by myelin-specific CD4+ Th1 lymphocytes [5–7]. Furthermore, in rheumatoid arthritis and in murine collagen-induced arthritis, which is a widely accepted arthritis model, T cells were reported to play a pivotal role [8–10]. Even in myasthenia gravis (MG) and in experimental autoimmune MG (EAMG), where the attack of specific antibodies on the acetylcholine receptor is the accepted cause of disease, there is ample evidence that T cells play a key role in the etio-pathology of the disease in humans and in ani-mals [11–13]. The role of T cells in organ-specific autoimmune diseases has been confirmed and revisited with the discovery of Th17 cells. Th17 cells or their cytokine, IL-17, were demonstrated to be essential in the induction of experimental autoimmune inflammation in animal models of experimental allergic encephalomyelitis [14], collagen-induced arthritis [10], colitis [15] and experimental a utoimmune myocarditis [16].
Systemic lupus erythematosus is an auto-immune disease characterized by the presence of an array of antibodies, including antibodies to DNA, nuclear antigens and ribonucleopro-teins. The progression of the disease is associ-ated with general clinical manifestations and damage to tissue and organs caused by deposi-tion of immune complexes [1]. Besides intrinsic dysfunctions of B lymphocytes that characterize SLE, T cells were shown to play a central role in the pathogenesis of SLE in mouse models and in patients [17,18]. Numerous abnormalities were shown to affect T-cell responses, the production of T-cell cytokines, and the T–B-cell dialog in lupus. Polyclonal CD4+ T-cell activation is a hall-mark of human and murine lupus [19], suggest-ing a global defect in the maintenance of T-cell tolerance to self. Peripheral T cells in lupus-prone mice have a significantly lower threshold for T-cell activation as compared with T cells of normal mice. This intrinsic T-cell abnormality might ultimately lead to enhanced helper func-tion for B-cell autoimmunity [20]. T cells that are
oligoclonal, based upon T-cell receptor (TCR) usage, were shown to infiltrate the kidneys of lupus patients [21]. In addition, expansion of oligoclonal T cells in peripheral blood of SLE patients was demonstrated [22]. In agreement, ablation of CD4 T cells by either thymectomy, genetic deletion of MHC class II molecules or anti-CD4 treatment [23–25] ameliorated disease manifestations in murine disease models. The role of T cells was further demonstrated using a model for the induction of SLE in non-SLE-prone mice. Thus, experimental SLE can be induced in naive BALB/c mice by their immu-nization with a monoclonal anti-DNA antibody that bears a common idiotype (Id), namely 16/6Id [26]. Nevertheless, the disease could not be induced in BALB/c nude mice [27]. Furthermore, experimental SLE could be induced with cells of 16/6Id-specific lines that were administered into syngeneic mice [28]. Moreover, experimental SLE could be induced by inoculating C57BL/6 (H-2b) mice (a strain resistant to the induction of SLE by immunization with the disease-inducing anti-body 16/6Id), with the H-2-matched T-cell line of C3H.SW origin [28], supporting the essential role of T cells in SLE.
The SLE-prone MRL/lpr mice develop a spec-trum of disease manifestations that are similar to fulminant human SLE. MRL/lpr mice with B cells, but no circulating antibodies, still devel-oped interstitial nephritis and vasculitis, as well as a glomerular disease. These nonsecret-ing B cells were discussed to be important as antigen-presenting cells (APCs) that activate T cells, suggesting a direct role for the latter cells in causing the tissue damage observed in SLE [29].
The role of CD8 T cells in the pathogenesis of SLE was also demonstrated. Thus, abnormal CD8+ T-lymphocyte functions, including inap-propriate cytokine production, aberrant cytotox-icity and inhibited suppressor capacity, have been reported in SLE patients [30,31]. Furthermore, depletion of CD8 cells accelerated the develop-ment of SLE in mice with an induced experi-mental SLE by the 16/6Id-bearing anti-DNA monoclonal antibody [32] and in genetically prone (NZB × B × SB)F1 mice [33]. Likewise, CD8-/- mice with a C57BL/6 background, which are resistant to the induction of SLE, were shown to be susceptible to the experimental disease [34]. In addition, CD8 cells specific to the 16/6Id were capable of immunomodulating experimen-tal SLE induced by the 16/6Id [35]. Thus, there is no doubt that T cells play a central role in driving the development of lupus, both in mice and in humans.

www.futuremedicine.com 387future science group
Harnessing regulatory T cells for the therapy of lupus & other autoimmune diseases Review
Tregs in autoimmune diseases & specifically in sLeRegulation of lymphocyte survival is essential for the maintenance of lymphoid homeostasis, thereby preventing the development of autoim-mune diseases. The existence of auto reactive T cells in healthy individuals suggests that peripheral tolerance mechanisms exist to con-trol the response of these cells. Accumulating evidence indicates that not only clonal deletion and anergy but also T-cell-mediated control of self-reactive T cells contributes to the mainte-nance of immunological self-tolerance. Actually, Tregs are now widely regarded as the primary mediators of peripheral tolerance and dendritic cells (DCs) play a role in their development. Several subtypes of Tregs have been described with distinct phenotypes, cytokine production profiles, and modes of action. Most of these Tregs are CD4+; however, CD8+ Tregs with efficient suppressor capacity, as well as natural killer T cells, have also been reported. In the CD4+ regulatory T-cell compartment, IL-10-producing T-regulatory cell type 1 (T
R1),
TGF-b-secreting Th3 cells and CD4+CD25+ cells were reported [2,36]. This review will focus on CD4 and on CD8 Tregs.
n CD4 TregsExtensive work performed both in mice and in humans has documented that CD4+CD25+ T cells are an important subset of Tregs. CD4+CD25+ Tregs (CD4 Tregs) that are natu-rally occurring and expressing Forkhead winged helix protein-3 (Foxp3) are potent inhibitors of a variety of immune responses. Their depletion or functional alteration leads to the develop-ment of autoimmune diseases in otherwise nor-mal animals. Such CD4 Tregs are produced by the normal thymus as a functionally distinct and mature subpopulation of T cells. Genetic defects that affect the development or function of these Tregs may lead to the development of autoimmune and other inflammatory dis-orders in humans. Induced or adaptive CD4 Tregs represent a second subset of CD4+CD25+ functional suppressive cells. Antigen peptides that are given either in a tolerogenic form or by a tolerogenic route (using injection, oral or nasal administration) may selectively induce the appearance of T cells with the regulatory pheno-type and function. These antigen-dependent induced regulatory cells are fully functional following their exposure to antigen tolerogens, as in the case of certain immunomodulatory therapies [37,38].
Reduced levels or function of circulating CD4 Tregs were described in patients with numer-ous autoimmune diseases, such as MS, juvenile idiopathic arthritis, psoriatic arthritis, auto-immune liver disease, MG and Kawasaki dis-ease. Further conflicting data have been reported for r heumatoid arthritis and immune-mediated Type 1 DM [39]. Nevertheless, the status and role of CD4 Tregs in experimental models of autoimmune diseases are much clearer.
Involvement of CD4 Tregs in EAE was demon-strated using various approaches. For example, strains of mice that harbor a mono clonal myelin basic protein (MBP)-specific antibody CD4+ T-cell repertoire spontaneously develop EAE. It has been postulated that the latter has been a result of the failure of CD4 Tregs to utilize the endoge-neous TCR a-chain in Rag-2-deficient mice [40]. Furthermore, CD4 Tregs were shown to confer significant protection from the develop ment of myelin oligodendrocyte glycoprtein (MOG)
35–55-
induced EAE [41]. It was demonstrated that myelin proteolipid protein-specific CD4 Tregs confer genetic resistance to the develop ment of EAE [42] and Tregs were also reported to be involved in the resistance of male mice to the development of EAE. By using CD4+ T-cell-driven EAE as a model, it was found that depletion of CD4 Tregs allowed pathology to develop in response to sub-optimal T-cell stimulation, thus demonstrating the role of CD4 Tregs in raising the threshold of triggering autoreactive T-cell responses [43]. Finally, glatiramer acetate, which is used for the treatment of MS patients, was shown to boost the expression of Foxp3 on CD4 Tregs during EAE. Moreover, adoptive transfer of purified Tregs from glatiramer acetate-treated EAE mice resulted in a better effect than the transfer of Tregs from untreated EAE controls [44].
Similar to the case in MG patients, where a deficiency in CD4 Tregs was shown to favor the development of disease, normalization of CD4 Tregs following immunosuppressive ther-apy was demonstrated to be of clinical value. Amelioration of EAMG manifestations was also reported to correlate with the development of functional CD4 Tregs. Thus, an improve-ment in the clinical status of rats with EAMG was reported following treatment with pent-oxifylline, which upregulated CD4 Tregs [45]. Furthermore, EAMG induced in C57BL/6 mice was effectively suppressed by GM-CSF treat-ment that resulted in the expansion of Tregs [46]. In addition, a dual altered peptide ligand (APL), composed of two APLs of two myasthenogenic peptides, was reported to inhibit in vitro and

Immunotherapy (2009) 1(3)388 future science group
Review Sharabi & Mozes
in vivo MG-associated autoreactive responses. The dual APL upregulated functional CD4 Tregs and depletion of CD4 cells diminished the inhibitory effect of the dual APL [47–49]. In addition, an established EAMG, induced in C57BL/6 mice by Torpedo acetylcholine recep-tor, was downregulated following treatment with the dual APL via the upregulation of functional CD4 Tregs [50].
The role of CD4 Tregs in autoimmune-prone NOD mice was extensively studied. Although CD4 Tregs undoubtedly play a role in governing the onset and development of diabetes, the issue of the number of CD4 Tregs in the NOD mouse is controversial. Nevertheless, it was demonstrated that small numbers of antigen-specific CD4 Tregs can reverse diabetes after disease onset [51]. Suppression in the NOD model, especially after anti-CD3 therapy, was shown to depend on active immunoregulation that is TGF-b dependent [52]. Furthermore, DC-expanded, islet-specific CD4 Tregs could block diabetes months after i nitiation of insulitis and restored long-term normo glycemia when given to recent-onset diabetic mice [53]. Thus, the emerging experimental evidence sug-gests that, as in other models of autoimmune diseases, CD4 Tregs are capable of controlling Type 1 DM at various levels.
n CD4 Tregs in SLEMost reports agree that CD4 Tregs are defective in SLE and especially in patients with active dis-ease. Whereas decreased numbers of CD4 Tregs were determined in some studies of SLE patients, especially during the active phase of the disease, others claim a defective activity of the Tregs that is correlated with downregulation of the expres-sion of Foxp3 [54–57]. Although it is still not clear whether the abnormality of SLE is related to a defective number or function of CD4 Tregs, or both, whether Foxp3 is the exclusive marker of functional Tregs, and what conditions lead to the suppressive function of the CD4 Tregs, the accumulating data suggest that strategies to enhance the function of CD4 Tregs might b enefit patients with SLE.
The differences in reports regarding the status of CD4 Tregs in SLE patients may be due to the stage of disease, its activity, various disease manifestations and the influence of therapies. In addition, the use of different surface mark-ers for the definition of Tregs owing to the lack of an absolute specific marker may also account for the differences between observa-tions. Lupus-prone mouse models, which are more homo geneous than SLE patients, allow a
more precise examination of CD4 Tregs with-out the interference of treatment with various immunosuppressive drugs. The involvement of numerical and/or functional modification of Tregs in lupus was demonstrated by the fact that glomerulonephritis accompanied by anti-DNA antibody production was detected in approximately 30% of immunodeficient mice reconstituted with CD25-depleted T cells, indi-cating that systemic autoimmune diseases might be controlled by CD4 Tregs [58]. In addition, depletion of CD4 Treg cells of nonautoimmune mice with anti-CD25 neutralizing antibody and breaking their tolerance resulted in the produc-tion of higher titers of anti-ds/ssDNA-specific antibodies than in the isotype control-treated group, indicating the involvement of CD4 Tregs in the regulatory mechanisms of autoan-tibody production [59]. Furthermore, (NZB × NZW)F1 and (SWR × NZB)F1 mice, which spontaneously develop a lupus-like disease, were reported to display a lower percentage of CD4 Tregs than BALB/c, DBA/1 and (DBA × NZW)F1 non-SLE-prone mice [60]. Reduced numbers of CD4 Tregs were also determined in mice congenic for the NZM2410 sle1 locus [61]. The reduced number of CD4 Tregs was associ-ated with downregulation in the expression of Foxp3. MRL/lpr mice, in which a strong lupus disease develops, were shown to exhibit a nor-mal percentage of CD4 Tregs and the Foxp3 mRNA and protein expression was not altered. Nevertheless, MRL/lpr CD4 Tregs displayed a reduced capacity to suppress proliferation and proinflammatory cytokine secretion from effec-tor cells [62]. Adoptive transfer of exogenously expanded CD4 Tregs reduced the rate at which (NZB × NZW)F1 mice developed renal dis-ease and improved survival, further supporting the role of these cells in disease regulation [63]. Further suggestions for the role of CD4 Tregs in the regulation of SLE manifestations in ani-mal models are based on the observations that treatment with means that ameliorate lupus is associated with the upregulation of functional CD4 Tregs. Thus, induction of mucosal toler-ance by administration of the histone peptide H471
restored the lower numbers of CD4 Tregs
in the SLE-prone (NZB × NZW)F1 mice to levels observed in normal mice [60]. Using low doses (1 µg/mouse) of a nucleosomal histone peptide H4
71–94 for tolerance induction in the
lupus-prone (SWR × NZB)F1 mice was shown to ameliorate disease manifestations, prolong the lifespan of and upregulate CD4 Tregs. The lat-ter suppressed IFN-g production by pathogenic

www.futuremedicine.com 389future science group
Harnessing regulatory T cells for the therapy of lupus & other autoimmune diseases Review
T cells and autoantibody production. The cells were also effective in suppressing lupus-associ-ated responses upon adoptive transfer in vivo [64]. The histone deacetylase inhibitor trichostatin A decreased inflammatory mediator production, autoantibody production, and indices of disease in (NZB × NZW)F1 mice in association with an increase in CD4 Tregs [65]. Finally, (NZB × NZW)F1 mice can be protected from devel-oping SLE when given high intravenous doses (1 mg/mouse) of a synthetic peptide (pCon-sensus [pCons]) based on a shared CDR1/framework 2 epitope encoded within the vari-able heavy chain region of several murine anti-dsDNA immunoglobulins. Treatment with this peptide delays the appearance of autoantibod-ies in the treated mice and prolongs their sur-vival. Administration of the tolerogenic peptide led to the expansion of peptide-reactive CD4 Tregs that inhibited in vitro the production of anti-dsDNA antibody-producing cells [66,67].
n CD8 TregsIn addition to CD4 Tregs, CD8 Tregs have also been demonstrated to play an important role in autoimmune diseases. Some subsets of CD8 Tregs have been suggested to sup-press immunity in a nonspecific manner (e.g., CD8+CD25+, CD8+CD122+, CD45RClow and IL-2/GM-CSF-induced CD8 Tregs). By con-trast, antigen-specific CD8 Tregs are primed to foreign or self-antigens and downregulate spe-cifically the relevant immune responses. These CD8 Tregs include CD8+CD28- Tregs that frequently express Foxp3, CD8+CD75s+ Tregs, CD8+CD45RChigh Tc1 Tregs, and TCR peptide-specific CD8aa Tregs [68,69]. In humans, CD8 dysfunction has been implicated in various auto-immune diseases including inflammatory bowel disease, Type 1 DM, rheumatoid arthritis and MS [70–72]. In MS, it was further demonstrated that the beneficial effects of immunotherapy with glaritamer acetate were at least partially due to the induction of CD8 Tregs [73].
CD8 Tregs have been associated with disease protection and recovery from EAE in rodents. For example, CD8+ T-cell depletion rendered the resistant CD28-deficient mice susceptible to EAE [74]. In the model of MOG
35–55-induced
EAE, the depletion of CD8+ T cells could enhance EAE [75]. Moreover, it was reported that MBP-specific tolerogenic APCs halt the progression of EAE via the induction of CD8 Tregs that suppress MBP-specific autoimmunity [76]. In addition, MHC class Ib-restricted CD8+ T cells downregulated EAE disease activity and
CD8+CD122+ Tregs reduced the signs of EAE, especially in the recovery phase [77]. In a study of a mouse model for inflammatory bowel dis-ease, CD8+CD28- Tregs isolated from the spleen or gut prevented the development of the disease induced by transfer of colitogenic T cells into immunodeficient hosts [78]. In a model of EAMG, it was demonstrated that CD8+CD28- Tregs were involved in the suppression of EAMG-associated responses by a dual APL. The ability of the dual APL to inhibit the proliferation of T cells specific to Torpedo acetylcholine receptor was abrogated in CD8-/- immunized mice. Furthermore, the dual APL did not suppress the production of the pathogenic cytokine IFN-g in CD8-knockout mice that were immunized with the EAMG-inducing Torpedo acetylcholine receptor, sug-gesting that CD8 Tregs play an important role in the mechanism of action by which the dual APL ameliorates EAMG-associated autoreactive responses [79].
n CD8 Tregs in SLEThe information regarding CD8 Tregs in human lupus is limited. In addition to the observation that the functional activity of CD8+ suppressor cells is impaired in SLE patients with active disease and that the defective function could be related to abnormal cytokine secretion of these cells, there is a contrasting report that CD8+CD28- T cells are not quantitatively reduced in patients compared with controls [80,81].
Regarding murine models of lupus, the Hahn group demonstrated that after treatment of (NZB × NZW)F1 mice with their tolerogenic peptide, namely pCons, the number of CD8+ inhibitory cells increased in addition to CD4 Tregs [82]. The CD8 inhibitory cells were of both CD28+ and CD28- phenotypes. Both subsets of CD8 Tregs expressed elevated levels of Foxp3 and their suppressive activity could be fully inhibited by blockade of Foxp3 using the small interfering RNA technology [82]. Nevertheless, the expression of Foxp3 was significantly higher and persistent in the CD8+CD28- cells [82], sug-gesting that a predominant regulatory activity exists for the CD28- cell compartment. Secretion of TGF-b increased in both CD28+ and CD28- subsets of CD8 inhibitory cells as well. CD8 Tregs could directly suppress proliferation of both T and B syngeneic cells, and they were resistant to apoptosis at least partially via the upregulated expression of Bcl-2 [81]. The emer-gence of CD8+ cells was demonstrated to be associated with the downregulation of surface expression of programmed death (PD)-1 [83].

Immunotherapy (2009) 1(3)390 future science group
Review Sharabi & Mozes
Thus, the suppressive capacity of the pCons-induced CD8+ cells depended on the intracellular expression of Foxp3 and on the alteration of PD-1 on the cell surface. Furthermore, induction of tol-erance in the lupus-prone (SWR × NZB)F1 mice by the injection of very low doses (1 µg/mouse) of a nucleosomal histone peptide H4
71–94 induced
CD8 Tregs in addition to CD4 Tregs. The CD8
Tregs required TGF-b for immunosuppression and were effective in suppressing lupus autoim-mune responses upon adoptive transfer in vivo. In vitro, these cells suppressed IFN-g responses of pathogenic lupus T cells to nucleosomal epitopes and reduced autoantibody production by inhibit-ing nucleosome-stimulated T-cell help to nuclear autoantigen-specific B cells [64]. The substantial type of APCs that played a role in the tolerance induction by H4
71–94 was determined to be plas-
macytoid DCs [64]. Thus, the evidence indicated that both CD4 and CD8 Tregs play an important role in the amelioration of SLE manifestations in patients as well as in murine models of the disease.
Characterization & mechanisms of action of Cd4 TregsMany of the cell markers that can be determined for CD4 Tregs are associated with the activation status of the cells in both mice and humans and therefore cannot be used solely to differentiate between activated CD4 cells and CD4 Tregs. In the mouse, the IL-2 receptor a-chain (CD25), which is upregulated in T cells following activa-tion, is a typical marker of CD4 Tregs [84]. The expression of cytotoxic T-lymphocyte-associated antigen (CTLA)-4 is another example of a typi-cal regulatory molecule that is upregulated in non regulatory cells following their activation. Attempts to improve the definition of T cells with regulatory activity resulted in their allocation within subsets of cells that express memory-related markers such as CD45RBlow and CD62Lhigh. The discovery of Foxp3 to be expressed specifically in CD4 Tregs enabled a most reliable differentiation between activated T cells and cells that function as suppressors/regulators [85,86]. Neuropilin-1 is a coreceptor to a tyrosine kinase receptor that is constitutively expressed on the surface of CD4 Tregs independently of their activation status, in contrast to nonregulatory T cells whose expres-sion is downregulated following activation of the cell [87]. In addition, in this case, only CD4 cells that highly expressed neuropilin-1 exhibited high levels of expression of Foxp3. Those molecules that mostly participate in the immune regulation mediated by inducible (adaptive) CD4 Tregs are discussed below.
Foxp3 is a key transcription factor that is required for the development, maintenance and function of Tregs, and is sufficient to confer regu-latory activity on naive T cells [85,86]. Foxp3 is con-sidered to be a master gene because it controls the expression of multiple genes that mediate the reg-ulatory activity of Tregs [88]. Furthermore, Foxp3 plays a major role in the regulation of immune responses only when it is expressed in T cells [89].
The best defined inhibitory receptor is CTLA-4 [90]. It is expressed constitutively in Tregs, but it is further upregulated by cell stimulation, thus contributing to the function of Tregs [91,92]. CTLA-4 in Tregs leads to the down-regulation of CD80 and CD86 on DCs, which in turn attenuates the activation of effector T cells [93–96]. Mechanisms that explain the suppressed activity of effector cells by CTLA-4 involve an increase in the activation threshold of T cells [97], and the induction of indoleamine 2,3-dioxygen-ase [98]. Deficiency in CTLA-4 [99,100] or defi-ciency in B7 molecules (CD80 or CD86) [101] was shown to interrupt this suppressive process. Although Tregs from CTLA-4-deficient mice were reported to develop and function normally through compensatory upregulated production of TGF-b [102], it has been recently shown that CTLA-4-deficient Tregs have diminished sup-pressive capacity that could not be overcome even when compensatory suppressive mecha-nisms became more active [103]. Furthermore, the ability of Tregs to control the differentiation of activated T cells into IFN-g-producing effec-tor cells [104] was abrogated by Tregs lacking the expression of CTLA-4 [103]. Hence, CTLA-4 is a critically required molecule for Tregs activity.
TGF-b is an additional essential molecule that is important for maintaining the expression of Foxp3 in Tregs and is central for the suppressive capabilities of these cells [105–107]. However, the downstream signaling through which TGF-b mediates the expression of Foxp3 is unclear. The suppressive effects of TGF-b can be transferred to effector T cells through soluble forms of this cytokine, or through direct contact with Tregs, which display TGF-b on their surface [108]. When cell-to-cell contact takes place, TGF-b molecules on the surface of Tregs are triggered to aggregate through signals originating from CTLA-4 [108]. T cells that cannot respond to TGF-b thus escape control by Tregs [107] and, as a consequence, generalized autoimmunity is developed in vivo [109].
PD-1 is a cell-surface inhibitory receptor [90]. It is upregulated on activated T cells (and B cells), and the concurrent engagement of PD-1 and

www.futuremedicine.com 391future science group
Harnessing regulatory T cells for the therapy of lupus & other autoimmune diseases Review
TCR with the same APC causes the termina-tion of TCR signaling [110]. The PD-1 molecule is therefore essential for protecting against auto-immunity [111]. The interactions per se between PD-1 and its ligand were not required for Tregs to enable the induction of tolerance and pre-vention of autoimmune diabetes [112]. Indeed, normal ranges of expression of Foxp3 could be determined even in PD-1-knockout mice, although Tregs from these mice lacked func-tional suppression [113]. Rather, the inhibition of PD-1 signaling in naive T cells was shown to increase the expression of Foxp3 [84]. By contrast, the expression of PD-1 was reported to induce characteristics of regulatory cells in a spleen-derived subpopulation of CD4+CD25- cells. These cells were determined to constitutively express Foxp3 and CTLA-4, and to inhibit the development of colitis, although to a lesser extent than Tregs [114].
IL-35 is a new inhibitory cytokine that belongs to the IL-12 cytokine family. It is com-posed of the IL-12a and IL-27b chains; the lat-ter is encoded by Epstein–Barr virus-induced-gene 3 (Ebi3), which appears to be a downstream target of Foxp3. IL-35 is expressed preferentially in Tregs, and it was found to confer regulatory activity on naive T cells and to suppress T-cell proliferation in vitro as well [115].
Most of the above markers are used for the definition of human CD4 Tregs as well. However, since CD25 is not as useful in humans as in the mouse in defining Tregs, and the cor-relation between expression of Foxp3 and regula-tory function is controversial in humans as well, other markers such as the cell surface a-chain of IL-7 receptor (e.g., CD127) are recommended for proper definition of Tregs [116].
n Specificity of CD4 Tregs in autoimmune diseasesCD4 Tregs possess TCRs of an increased avidity for self-peptides in comparison with CD4+CD25- cells [117]. The ana lysis of the TCRs of Tregs revealed a massive diversity of repertoires [118,119], and it has been suggested that Tregs selectively affect effector T cells whose TCRs are for the same antigen [120]. The specific activity of Tregs was demonstrated in different animal models for autoimmune dis-eases. For instance, CD4 cells originating from thyroid-ablated rats were i ncapable of protecting against the induction of autoimmune thyroiditis in the recipient mice, hence, exemplifying the significance of organ-derived antigens for potent antigen-specific CD4 Tregs [121]. Furthermore,
Tregs expressing TCR that is specific for an islet antigen were shown to be efficient in suppressing and reversing early onset of diabetes in NOD mice, whereas polyclonal Tregs were consider-ably less effective [51,122,123]. Similar effects were determined in mice that develop EAE spontane-ously, in which the development of the disease was prevented following the adoptive transfer of CD4 Tregs whose TCRs were specific for MBP, in contrast to nonspecific Tregs that were inef-fective [124]. Similarly, CD4 Tregs from healthy, prediseased NZM mice were not capable of improving glomerulonephritis and sialoadeni-tis developed spontaneously in the mice [125]. More recently, the notion that CD4 Tregs are disease specific was also demonstrated in mice that were thymectomized on day 3 by showing that the development of autoimmune ovarian disease could be suppressed by CD4 Tregs from the ovarian lymph nodes, but not by CD4 Tregs from nonovarian lymph nodes [126]. The results of these studies suggest that Tregs are antigen specific, and therefore therapeutic manipula-tions aimed at inducing functional suppressive Tregs should be carried out in the context of an antigen-specific driven process in order to enable the application of a controlled and an efficient function of the newly generated suppressive cells.
requirements for peripheral generation of antigen-specific Tregs n Antigen dosing & mode
of administrationPeripheral generation of Tregs occurs in response to an exposure to antigens peptides that are not necessarily presented in the thymus [127]. The antigen-specific Tregs are critical for prevailing organ-specific tolerance [121]. They can be found in the draining lymphoid tissues of the affected organ where self-antigens originating from that organ can constantly be presented to the Tregs [104,128]. The antigen that would be recognized specifically by an appropriate TCR determines the specificity of the target cells in the periphery. However, the amount of the antigen and its mode of administration are both important determi-nants. Thus, the development of Tregs can be carried out following the administration of small amounts of an antigen, under tolerogenic and not immunogenic conditions [129–132].
n Antigen-presenting cells The administration of an antigen under tolero-genic regimens should be followed by its pre-sentation by APCs during the induction process of antigen-specific Tregs. Indeed, the ability of

Immunotherapy (2009) 1(3)392 future science group
Review Sharabi & Mozes
APCs to promote the induction of Foxp3 in T cells is based essentially on the interactions between cognate T cells and APCs, and not on the production of soluble factors [132]. Among the types of APCs that possess properties of antigen presentation, B cells and DCs are the most stud-ied candidates in association with the induction of antigen-specific Tregs [132,133]. The type of APC to be involved in the induction process of CD4 Tregs is suggested to be determined by the antigen dosing. Thus, DCs are the main APCs to mediate the induction of CD4 Tregs when very small amounts of the tolerogenic peptide are used [133], whereas the usage of increased amounts of antigen would favor the participation of B cells as the main APCs [132,133].
n CostimulationWhereas B7:CD28 costimulation was reported as essential for the development of Tregs in the thymus [134–137], costimulation is not required, and in fact, might hinder the induction of Tregs in the periphery [131,132,138]. Thus, tolerogenic administration of an antigen under repressed expression of CD28 resulted in upregulated expression of Foxp3, unlike the case of enhanced expression of B7 that led to inhibited expression of Foxp3 [139]. The inhibition of CD28 costimu-lation may favor the induction of Tregs, at least in part because it leads to downregulated lev-els of activator protein-1, a molecule interact-ing with the nuclear factor of activated T cells (NFAT) [140]. Moreover, the reduced expression of activator protein-1 may result in NFAT being more available for interaction and complex for-mation with Foxp3. As previously reported, such Foxp3–NFAT complexes are required for the induction of Tregs [141]. Costimulation through CTLA-4 was demonstrated to be essen-tial for the induction of Tregs both in the peri-phery [138,142] and in the thymus [103], at least partly owing to its upregulating effects on the p roduction of TGF-b [143].
n CytokinesThe peripheral induction of Tregs [106,144], as opposed to the development of naturally occur-ring Tregs [145], depends on the presence of TGF-b. TGF-b signaling is required for de novo expression of Foxp3 [131]. However, it is not clear whether TGF-b affects the induction of Foxp3 directly through a Smad-signaling pathway or indirectly by its ability to impair the proliferation of T cells, which then might facilitate the expres-sion of Foxp3 by peripheral T cells. TGF-b sig-naling is required for the suppressive capacity of
Tregs, and for the in vivo expansion of Tregs [146]. Recently, it has been shown that TGF-b increases the amounts of acetylated Foxp3 protein binding to active chromatin sites, suggesting that TGF-b may be involved in the prolongation of the half-life of Foxp3 RNA species, and/or the phosphory-lation of the chromatin-bound Foxp3, which may enable cellular compartment transitions for other transcription factors [147]. IL-2, in addition to TGF-b, is required for the peri pheral induction of Tregs [148,149]. Nevertheless, in certain settings of CD4 Tregs induction, it was demonstrated that the levels of IL-2 were already satisfactory without requiring an exogenous addition of IL-2 [133,150]. It is noteworthy that the development of natu-rally occurring Tregs in the thymus was shown to be IL-2 independent, although IL-2 signaling was required for the homeostasis maintenance of Tregs [151,152].
n Effector T lymphocytesEffector T cells were recently suggested to play a role in the suppression induced by Tregs because their presence might potentiate Tregs for inhibitory capacity. This concept was con-sidered after demonstrating differences in the molecular signature of Tregs, depending on the presence or absence of effector cells [153]. Thus, it was demonstrated that regulatory mediators (e.g., IL-35) could be upregulated by Tregs only in the p resence of effector T cells [154].
role of Tregs in the mechanism of action of the tolerogenic peptide hCdr1, which ameliorates sLeIn an attempt to develop specific therapeutic means for SLE, our group designed and syn-thesized a tolerogenic 19-amino acid peptide, namely hCDR1 [155], based on the sequence of the heavy chain complementarity determining region (CDR)1 of the human anti-DNA mono-clonal antibody that bears the major idiotype, 16/6Id [156]. hCDR1 was tested for its ability to ameliorate established SLE manifestations in spontaneous and induced models of SLE in mice. Administration of small doses of hCDR1 (25–50 µg/mouse) subcutaneously [157], once a week for 10–14 weeks resulted in a significant amelioration of the serological (e.g., reduced autoantibody production) and renal (e.g., dimin-ished proteinuria levels and decreased immune complex depositions in the glomeruli) manifes-tations that developed either in the SLE-prone (NZB × NZW)F1 mice or in BALB/c mice that were induced with experimental SLE with the disease-inducing anti-DNA antibody that

www.futuremedicine.com 393future science group
Harnessing regulatory T cells for the therapy of lupus & other autoimmune diseases Review
bears the 16/6Id [157]. Furthermore, hCDR1 downregulated disease manifestations asso-ciated with CNS lupus, as evidenced by reduced brain pathology and improved behavior param-eters (e.g., anxiety and memory) [Lapter S et al.,
Unpublished Observations]. Similarly, severe com-bined immunodeficient (SCID) mice that were engrafted with peripheral blood lymphocytes from SLE patients and developed a SLE-like disease benefited from treatment with the tolero-genic peptide hCDR1 [158]. The beneficial effects of hCDR1 were associated with downregulated expression and secretion of the proinflammatory and pathogenic cytokines (i.e., IL-1b, TNF-a, IFN-g and IL-10) and with upregulation of the immunosuppressive cytokine TGF-b [157]. Note that the weekly tolerogenic administrations of hCDR1 did not result in the production of p eptide-specific antibodies.
Analyses of the cell populations obtained from mice with SLE manifestations revealed that in the T-cell compartment, most of the cells were characterized by activated/memory cells with only a small fraction of cells having the naive phenotype [159]. The rates of apoptosis in the activated T cells were significantly higher in comparison with those of the healthy con-trols. The downregulated expression of Bcl-xL, together with upregulated expression and func-tion of Fas ligand (FasL), caspase 8 and cas-pase 3 suggested that activation-induced cell death (AICD) was dominant in the T cells of the SLE-afflicted mice [160,161].
The beneficial effects of treatment with hCDR1 on SLE manifestations could be adop-tively transferred. Thus, spleen-derived cells from hCDR1-treated, young, free-of-disease (NZB × NZW)F1 donors efficiently down-regulated lupus manifestations in the old, SLE-afflicted recipients [162]. Studies performed in our laboratory showed that the transferred cells con-tained subsets of cells with inhibitory capabili-ties, with CD4 Tregs being the major constituent of this population. Treatment of SLE-afflicted mice with hCDR1 upregulated CD4 Tregs by 30–40% in comparison with cells of either vehicle or control peptide-treated mice [163]. The hCDR1-induced CD4 Tregs were found to express CD45RBlow, CTLA-4, TGF-b and Foxp3. Furthermore, we showed that the trans-fer of non-hCDR1-induced Tregs (i.e., Tregs that were enriched from healthy, vehicle-treated mice) into SLE-afflicted (NZB × NZW)F1 mice did not beneficially affect the disease manifestations. By contrast, the adoptive transfer of enriched hCDR1-induced CD4
Tregs into the diseased mice resulted in sig-nificant beneficial responses. The latter effects were equivalent to those achieved following the transfer of 20-fold higher numbers of whole spleen-derived cells from hCDR1-treated mice [163]. Assessment of the in vitro suppressive effects of hCDR1-induced Tregs on effector T cells from the lupus-prone mice confirmed that the Tregs were highly potent even at a 1:100 Treg:T-effector-cell ratio [163]. It is notewor-thy that hCDR1-induced CD4 Tregs express higher levels of TGF-b, CTLA-4 and Bcl-xL, in addition to intensified Foxp3. The efficient inhibitory activity of hCDR1-induced CD4 Tregs, together with the demonstration that Tregs originating from a control peptide, the vehicle-treated mice, or from unmanipulated mice, did not have a significant clinical effect on mice with established lupus, suggest that the hCDR1-induced CD4 Tregs were specific to SLE. This notion was further supported by experiments showing that the proliferation of cells from mice with experimental SLE could be inhibited following the transfer of cells from mice that were pretreated with hCDR1, but not from mice that were pre-treated with the dual APL, which was shown to inhibit MG-associated manifestations [47–50].
Development of hCDR1-induced CD4 Tregs in the diseased mice involves inter action with an additional kind of Treg, namely CD8 Tregs. Treatment with hCDR1 led to an upregula-tion of CD8 cells in association with repressed expression of the CD28 costimulatory molecule, an effect shown to be mediated by CTLA-4 [159,164]. The expression of Foxp3 was confined mainly to the CD8+CD28- subset of cells [164]. The induced CD8 Tregs from hCDR1-treated mice inhibited in vitro antigen-specific cell proliferation and the secretion of pathogenic cytokines [164]. However, the in vivo effects of hCDR1-induced CD8 Tregs were quite limited and significantly less prominent than those of hCDR1-induced CD4 Tregs. Nevertheless, in vivo depletion of CD8+ cells diminished the clinical improvement following treatment with hCDR1. It was demonstrated that in the absence of CD8 Tregs, CD4 Tregs were unable to expand in the hCDR1-treated mice, and the expres-sion of Foxp3 was reduced, thereby interfering further with the suppressive function of CD4 Tregs. However, CD8 cells from hCDR1-treated mice that were adoptively transferred into SLE-afflicted mice led to upregulation of CD4 Tregs with intensified Foxp3 expression in the recipi-ent mice. Therefore, our data suggest that CD8
Immunotherapy (2009) 1(3)394 future science group
Review Sharabi & Mozes
Tregs are required for the optimal expansion and f unction of hCDR1-induced CD4 Tregs that ameliorate lupus manifestations [164].
As previously mentioned, T cells of the SLE-afflicted mice exhibited increased rates of apop tosis; however, treatment with hCDR1 reduced the rates of apoptosis in the effec-tor T cells [160,161]. Several signaling path-ways for apoptosis were affected by hCDR1.
The c-Jun NH2-terminal kinase (JNK) of
the p21Ras/MAP kinase pathway was highly expressed in T cells of the diseased mice and treatment with hCDR1 downregulated its acti-vation [165]. Previous reports indicated that high activity of JNK kinase promotes Th1 effector cell maturation [166,167]; therefore, its reduced activity following treatment with hCDR1 may contribute to the downregulation of the patho-genic cytokine IFN-g. The Fas signaling path-way was also affected by treatment with hCDR1. We found that cells originating from mice with established manifestations of SLE expressed high levels of FasL [161]. The ligation of FasL to its receptor on the affected cells is known to initiate a program of apoptosis that would be mediated via the activation of caspases 8 and 3 [168]. We found that CD4 Tregs from hCDR1-treated mice repressed Fas signaling via the downregulation of the expression of FasL in a CTLA-4-dependent manner, and diminished the activity of caspases 8 and 3 and upregu-lated the expression of the survival molecule Bcl-xL [159–161]. The suppressive effect on the expression of FasL played a role in restoring the normal profile of the pathogenic cytokines of the diseased mice [161]. It was further demonstrated that the expression of FasL in SLE-afflicted mice had a pathogenic role in kidney disease, which could be controlled following neutralization of FasL [169]. Moreover, inhibition of the activity of caspases in the hCDR1-treated mice could by itself lead to the clinical amelioration observed in our experiments because the mere inhibi-tion of pan-caspase activity (using ZVAD-fmk) in a murine model of lupus was shown to be c linically e ffective [170].
Bcl-xL was shown to play several roles in lym-phocytes from mice with established lupus. As a molecule with an antiapoptotic effect, the low expression of Bcl-xL in T cells of the diseased mice contributed to the increased rates of apop-tosis combined with the enhanced activity of the proapoptotic Fas and p21Ras signaling pathways [160,161,165]. Following the administration of hCDR1 to the SLE-afflicted mice, the expression of Bcl-xL in T cells was upregulated. Moreover, the expression of Bcl-xL was enhanced in both the effector T cells and the CD4 Tregs of the tolerized mice. As a result, the rate of apoptosis was downregulated. It is hypothesized that intra-cellular material of apoptotic cells whose levels are frequent and sustained, may be the source of the self-antigens that provoked the autoimmune-associated responses in SLE [171,172]. Hence, the ability of hCDR1 to downregulate the rate of
T-cell apoptosis
T-cell apoptosis
T-cell activation
T-cell activation
pJNKFasLCaspases
CD69CD45RBhigh CD28
Tolerogenic treatment with hCDR1
SLE-afflictedmice
CD8 cells CD4+25+ cells
CD28
Foxp3 CTLA-4
Bcl-xL
Foxp3
TGF-βEffector CD25- T cells
TGF-β CTLA-4 Bcl-xL
Amelioration of SLE-relatedserological and clinical manifestations
IFN-γ
IL-10
CD69
CD28
pJNK
FasL
Caspase 8
Caspase 3
Immunotherapy © Future Science Group (2009)
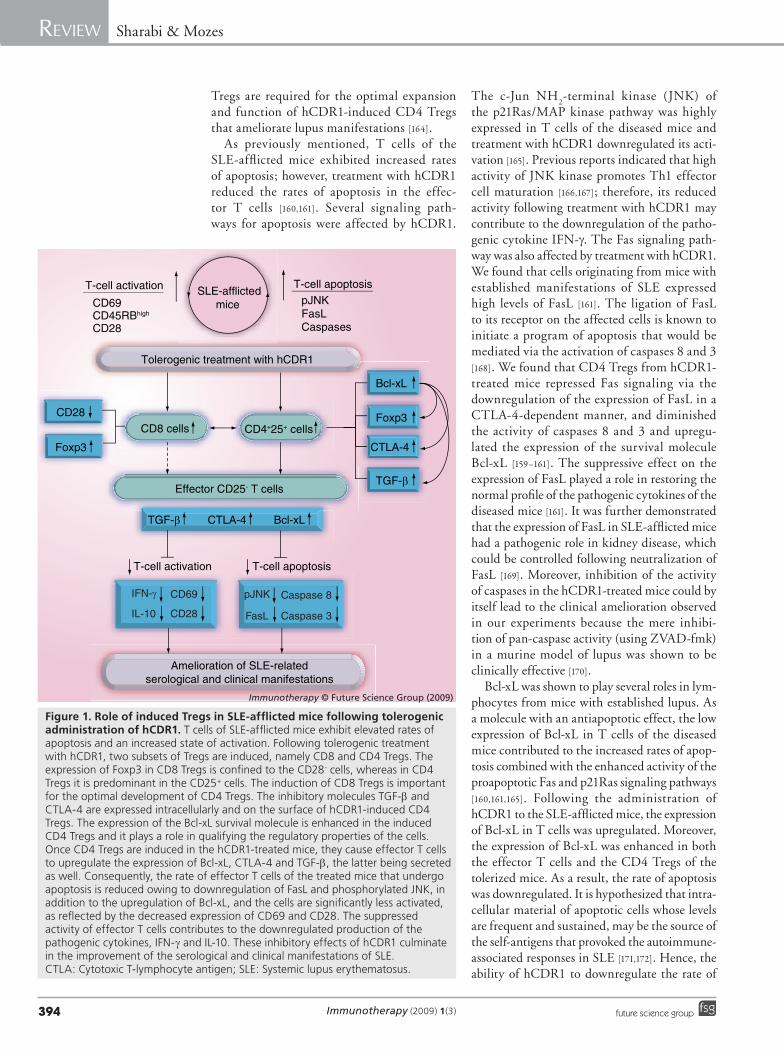
Figure 1. role of induced Tregs in sLe-afflicted mice following tolerogenic administration of hCdr1. T cells of SLE-afflicted mice exhibit elevated rates of apoptosis and an increased state of activation. Following tolerogenic treatment with hCDR1, two subsets of Tregs are induced, namely CD8 and CD4 Tregs. The expression of Foxp3 in CD8 Tregs is confined to the CD28- cells, whereas in CD4 Tregs it is predominant in the CD25+ cells. The induction of CD8 Tregs is important for the optimal development of CD4 Tregs. The inhibitory molecules TGF-b and CTLA-4 are expressed intracellularly and on the surface of hCDR1-induced CD4 Tregs. The expression of the Bcl-xL survival molecule is enhanced in the induced CD4 Tregs and it plays a role in qualifying the regulatory properties of the cells. Once CD4 Tregs are induced in the hCDR1-treated mice, they cause effector T cells to upregulate the expression of Bcl-xL, CTLA-4 and TGF-b, the latter being secreted as well. Consequently, the rate of effector T cells of the treated mice that undergo apoptosis is reduced owing to downregulation of FasL and phosphorylated JNK, in addition to the upregulation of Bcl-xL, and the cells are significantly less activated, as reflected by the decreased expression of CD69 and CD28. The suppressed activity of effector T cells contributes to the downregulated production of the pathogenic cytokines, IFN-g and IL-10. These inhibitory effects of hCDR1 culminate in the improvement of the serological and clinical manifestations of SLE. CTLA: Cytotoxic T-lymphocyte antigen; SLE: Systemic lupus erythematosus.
www.futuremedicine.com 395future science group
Harnessing regulatory T cells for the therapy of lupus & other autoimmune diseases Review
apoptosis contributes to diminishing at least some of the provoking antigens that drive the immune response and possibly also to a better clearance of apoptotic debris [173]. Furthermore, the induced expression of Bcl-xL led to reducing the activation state of T cells and to downregu-lated secretion of IFN-g and IL-10. Importantly, the hCDR1-induced CD4 Tregs elicited the e xpression of Bcl-xL in the effector T cells [160].
Antigen-presenting cells such as DCs and B cells are candidates for the presentation of hCDR1 to T cells. However, we found that B cells of hCDR1-treated mice exhibited increas-ing rates of apoptosis, possibly owing to down-regulation of the survival molecule Bcl-xL [160]. Furthermore, treatment with hCDR1 led to reduced numbers of DCs, favoring an immature phenotype of the remaining DCs, as manifested by the reduced expression of MHC class II and B7 molecules [174]. Indeed, immature DCs were
previously reported to play a role in the induc-tion of tolerance via their potent ability to induce CD4 Tregs [133]. The effects of hCDR1 on DCs were mediated at least partially by the immu-nosuppressive cytokine TGF-b [174], which was shown to be upregulated in T cells following treatment with hCDR1 [163].
In summary, mice with established manifesta-tions of lupus that are treated with the tolerogenic peptide hCDR1 were shown to clinically improve in many aspects of the disease. As illustrated in Figure 1, a multistep process leading to better regu-lation of the immune response is initiated and orchestrated after the induction of functional Tregs. Once hCDR1-induced CD8 and CD4 Tregs develop, the increased state of activation and the elevated rates of apoptosis that typically char-acterize lupus-derived lymphocytes are ultimately downregulated. Hence, treatment with hCDR1 enables breaking a vicious cycle that occurred
executive summary
Role of T cells in the pathogenesis of lupus & other autoimmune diseases � T cells play key roles in the etiopathology of T-cell-mediated autoimmune diseases and in diseases that are driven by B cells that produce
pathogenic autoantibodies. � In systemic lupus erythematosus (SLE), numerous abnormalities were shown to affect T-cell responses, the production of T-cell cytokines
and the T–B-cell dialog in lupus, leading to a global defect in the maintenance of T-cell tolerance to self. Tregs in autoimmune diseases & specifically in SLE � Tregs are widely regarded as the primary mediators of peripheral tolerance. � In a large number of autoimmune diseases, the levels and function of circulating CD4 and CD8 regulatory T cells (Tregs) were
determined to be reduced. � Clinical amelioration of some autoimmune diseases by various therapeutic means was shown to be associated with upregulated CD4
and CD8 Tregs. � Experimental evidence suggests that tolerogenic approaches may control the autoreactive-related clinical manifestations via the
induction of antigen-specific Tregs. � In SLE, the number and function of Tregs were reported to inversely correlate with the disease activity status in patients and in animal
models of lupus. � Administration of tolerogenic peptides to lupus-prone mice resulted in the clinical improvement of SLE manifestations via the
peptide-specific induction of CD8 and CD4 Tregs. Characterization & mechanism of action of CD4 Tregs � CD4 Tregs highly express CD25. Foxp3 is essential for the optimal function of the Tregs. In addition, inhibitory molecules such as
cytotoxic T-lymphocyte antigen (CTLA)-4 and TGF-b execute the suppressive effects of the cells.Specificity of CD4 Tregs in autoimmune diseases � CD4 Tregs have increased avidity for self-peptides, as demonstrated in a variety of murine models for autoimmune diseases. � CD4 Tregs with specificities that were irrelevant to the studied autoimmune diseases were inefficient in ameliorating the
disease-associated autoreactive responses.Requirement for peripheral generation of antigen-specific Tregs � The dose of an antigen peptide and its tolerogenic mode of administration. � Antigen-presenting cells (either B cells or dendritic cells) that would present the tolerizing antigen peptide. � Repressing CD28 expression while costimulating through CTLA-4. � TGF-b and IL-2 for expanding the newly generated CD4 Tregs. � Effector T cells to potentiate the inhibitory capacity of the cells.
Role of Tregs in the mechanism of action of the tolerogenic peptide hCDR1, which ameliorates SLE � Tolerogenic administration of low doses of hCDR1 ameliorated the serological, renal and neurological manifestations of SLE in murine models. � Treatment with hCDR1 induced functional CD4 Tregs that specifically downregulated SLE-associated manifestations. � hCDR1-induced CD8 Tregs are required for the development of functional CD4 Tregs. � hCDR1-induced CD4 Tregs diminished the rates of apoptosis and suppressed the activation state of effector T cells, resulting in
downregulated production of pathogenic cytokines and upregulated production of TGF-b.

Immunotherapy (2009) 1(3)396 future science group
Review Sharabi & Mozes
during the progression of the disease, where the decreased rates of apoptosis contribute to dimin-ishing the perpetuating antigen inoculum and, as a result, the cells are less activated.
Conclusions & future perspectiveThe emerging data from multiple studies that were performed in SLE patients and especially in murine models of lupus are consistent with the view that decreased numbers and/or func-tion of Tregs contribute to the pathogenesis of SLE. Therefore, therapeutic means that will induce functional Tregs of relevant specificities are likely to restore normal immune homeo-stasis in patients and to protect them from further development of pathogenic responses and tissue destruction. The coexistence of sev-eral subpopulations of Tregs has been reported and, as discussed above, an interaction between some of these subsets of Tregs (e.g., CD8+ and CD4+ Tregs) might be required for the opti-mal immunoregulatory function of the Tregs. Therefore, novel, specific therapeutic means that ‘chronically’ upregulate functional Tregs of the required subsets might be more effective
in ameliorating the autoimmune disease than the administration of an expanded specific pop-ulation of Tregs. Tolerogenic peptides, such as those described in this review that ameliorate the clinical manifestations in murine models of lupus via upregulation of CD4+ and CD8+ Tregs, are potential candidates for more specific and safer therapies that are needed for SLE. It is hoped that the encouraging information gained from numerous experiments performed in various animal models will serve as the basis for well-designed clinical trials aimed at har-nessing Tregs for treatment of lupus and other autoimmune diseases.
Financial & competing interests disclosureThe authors have no relevant affiliations or financial involvement with any organization or entity with a finan-cial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or p ending, or royalties.
No writing assistance was utilized in the production of this manuscript.
BibliographyPapers of special note have been highlighted as:n of interest
1 Hahn BH: An overview of the pathogenesis of systemic lupus erythematosus. In: Dubis’ Lupus Erythomatosus. Wallace D, Hahn BH (Eds), Lippincott Williams & Wilkins, PA, USA 87–92 (2002).
2 Sakaguchi S, Yamaguchi T, Nomura T, Ono M: Regulatory T cells and immune tolerance. Cell 133, 775–787 (2008).
n Review article with updated information on the role of regulatory T cells (Tregs) in health and disease.
3 Chatenoud L, Primo J, Bach JF: CD3 antibody-induced dominant self tolerance in overtly diabetic NOD mice. J. Immunol. 158, 2947–2954 (1997).
4 Saudek F, Havrdova T, Boucek P, Karasova L, Novota P, Skibova J: Polyclonal anti-T-cell therapy for Type 1 diabetes mellitus of recent onset. Rev. Diabet. Stud. 1, 80–88 (2004).
5 Zamvil SS, Steinman L: The T lymphocyte in experimental allergic encephalomyelitis. Annu. Rev. Immunol. 8, 579–621 (1990).
6 Gocke AR, Cravens PD, Ben LH et al.: T-bet regulates the fate of Th1 and Th17 lymphocytes in autoimmunity. J. Immunol. 178, 1341–1348 (2007).
7 Stinissen P, Hellings N: Activation of myelin reactive T cells in multiple sclerosis: a possible role for T cell degeneracy? Eur. J. Immunol. 38, 1190–1193 (2008).
8 Mauri C, Williams RO, Walmsley M, Feldmann M: Relationship between Th1/Th2 cytokine patterns and the arthritogenic response in collagen-induced arthritis. Eur. J. Immunol. 26, 1511–1518 (1996).
9 Chabaud M, Durand JM, Buchs N et al.: Human interleukin-17: a T cell-derived proinflammatory cytokine produced by the rheumatoid synovium. Arthritis Rheum. 42, 963–970 (1999).
10 Lubberts E, Joosten LA, Oppers B et al.: IL-1-independent role of IL-17 in synovial inflammation and joint destruction during collagen-induced arthritis. J. Immunol. 167, 1004–1013 (2001).
11 Lindstrom J, Shelton D, Fujii Y: Myasthenia gravis. Adv. Immunol. 42, 233–284 (1988).
12 Drachman DB: Myasthenia gravis. N. Engl. J. Med. 330, 1797–1810 (1994).
13 Ahlberg R, Yi Q, Pirskanen R et al.: Treatment of myasthenia gravis with anti-CD4 antibody: improvement correlates to decreased T-cell autoreactivity. Neurology 44, 1732–1737 (1994).
14 Korn T, Anderson AC, Bettelli E, Oukka M: The dynamics of effector T cells and Foxp3+ regulatory T cells in the promotion and regulation of autoimmune encephalomyelitis. J. Neuroimmunol. 191, 51–60 (2007).
15 Zhang Z, Zheng M, Bindas J, Schwarzenberger P, Kolls JK: Critical role of IL-17 receptor signaling in acute TNBS-induced colitis. Inflamm. Bowel Dis. 12, 382–388 (2006).
16 Sonderegger I, Röhn TA, Kurrer MO et al.: Neutralization of IL-17 by active vaccination inhibits IL-23-dependent autoimmune myocarditis. Eur. J. Immunol. 36, 2849–2856 (2006).
17 Hahn BH, Datta SK: Characteristics of T cells that participate in the pathogenesis of SLE. Lupus 6, 330–332 (1997).
18 Craft J, Peng S, Fujii T, Okada M, Fatenejad S: Autoreactive T cells in murine lupus: origins and roles in autoantibody production. Immunol. Res. 19, 245–257 (1999).
19 Rozzo SJ, Drake CG, Chiang BL, Gershwin ME, Kotzin BL: Evidence for polyclonal T cell activation in murine models of systemic lupus erythematosus. J. Immunol. 153, 1340–1351 (1994).
20 Vratsanos GS, Jung S, Park YM, Craft J: CD4+ T cells from lupus-prone mice are hyperresponsive to T cell receptor engagement with low and high affinity peptide antigens: a model to explain spontaneous T cell activation in lupus. J. Exp. Med. 193, 329–337 (2001).

www.futuremedicine.com 397future science group
Harnessing regulatory T cells for the therapy of lupus & other autoimmune diseases Review
21 Murata H, Matsumura R, Koyama A et al.: T cell receptor repertoire of T cells in the kidneys of patients with lupus nephritis. Arthritis Rheum. 46, 2141–2147 (2002).
22 Talken BL, Schäfermeyer KR, Bailey CW, Lee DR, Hoffman RW: T cell epitope mapping of the Smith antigen reveals that highly conserved Smith antigen motifs are the dominant target of T cell immunity in systemic lupus erythematosus. J. Immunol. 167, 562–568 (2001).
23 Steinberg AD, Roths JB, Murphy ED, Steinberg RT, Raveche ES: Effects of thymectomy or androgen administration upon the autoimmune disease of MRL/Mp-lpr/lpr mice. J. Immunol. 125, 871–873 (1980).
24 Jevnikar AM, Grusby MJ, Glimcher LH: Prevention of nephritis in major histocompatibility complex class II- deficient MRL-lpr mice. J. Exp. Med. 179, 1137–1143 (1994).
25 Wofsy D, Ledbetter JA, Hendler PL, Seaman WE: Treatment of murine lupus with monoclonal anti-T cell antibody. J. Immunol. 134, 852–857 (1985).
26 Mendlovic S, Brocke S, Shoenfeld Y et al.: Induction of a systemic lupus erythematosus-like disease in mice by a common human anti-DNA idiotype. Proc. Natl Acad. Sci. USA 85, 2260–2264 (1988).
27 Mozes E, Mendlovic S, Kalush F, Waisman A, Shoenfeld Y, Fricke H: Immunoregulation of autoimmune diseases. Isr. J. Med. Sci. 26, 688–690 (1990).
28 Fricke H, Mendlovic S, Blank M, Shoenfeld Y, Ben-Bassat M, Mozes E: Idiotype specific T-cell lines inducing experimental systemic lupus erythematosus in mice. Immunology 73, 421–427 (1991).
29 Chan OT, Hannum LG, Haberman AM, Madaio MP, Shlomchik MJ: A novel mouse with B cells but lacking serum antibody reveals an antibody-independent role for B cells in murine lupus. J. Exp. Med. 189, 1639–1648 (1999).
30 Ohtsuka K, Gray JD, Stimmler MM, Toro B, Horwitz DA: Decreased production of TGF-b by lymphocytes from patients with systemic lupus erythematosus. J. Immunol. 160, 2539–2545 (1998).
31 Filaci G, Bacilieri S, Fravega M et al.: Impairment of CD8+ T suppressor cell function in patients with active systemic lupus erythematosus. J. Immunol. 166, 6452–7645 (2001).
32 Ruiz PJ, Zinger H, Mozes E: Effect of injection of anti-CD4 and anti-CD8 monoclonal antibodies on the development of experimental systemic lupus erythematosus in mice. Cell Immunol. 167, 30–37 (1996).
33 Adachi Y, Inaba M, Sugihara A et al.: Effects of administration of monoclonal antibodies (anti-CD4 or anti-CD8) on the development of autoimmune diseases in (NZW × BXSB)F1 mice. Immunobiology 198, 451–464 (1998).
34 Singer DS, Zinger H, Kohn LD, Mozes E: Differing MHC class I requirements for induction and propagation of experimental systemic lupus erythematosus. Eur. J. Immunol. 29, 2259–2268 (1999).
35 Blank M, Ben-Bassat M, Shoenfeld Y: Modulation of SLE induction in naive mice by specific T cells with suppressor activity to pathogenic anti-DNA idiotype. Cell Immunol. 137, 474–486 (1991).
36 Sakaguchi S: Naturally arising CD4+ regulatory T cells for immunologic self-tolerance and negative control of immune responses. Annu. Rev. Immunol. 22, 531–562 (2004).
37 Bluestone JA, Abbas AK: Natural versus adaptive regulatory T cells. Nat. Rev. Immunol. 3, 253–257 (2003).
38 von Herrath MG, Harrison LC: Antigen-induced regulatory T cells in autoimmunity. Nat. Rev. Immunol. 3, 223–232 (2003).
39 Dejaco C, Duftner C, Grubeck-Loebenstein B, Schirmer M: Imbalance of regulatory T cells in human autoimmune diseases. Immunology 117, 289–300 (2006).
40 Furtado GC, Olivares-Villagómez D, Curotto de Lafaille MA, Wensky AK, Latkowski JA, Lafaille JJ: Regulatory T cells in spontaneous autoimmune encephalomyelitis. Immunol. Rev. 182, 122–134 (2001).
41 Kohm AP, Carpentier PA, Anger HA, Miller SD: Cutting edge: CD4+CD25+ regulatory T cells suppress antigen-specific autoreactive immune responses and central nervous system inflammation during active experimental autoimmune encephalomyelitis. J. Immunol. 169, 4712–4716 (2002).
42 Reddy J, Illes Z, Zhang X et al.: Myelin proteolipid protein-specific CD4+CD25+ regulatory cells mediate genetic resistance to experimental autoimmune encephalomyelitis. Proc. Natl Acad. Sci. USA 101, 15434–15439 (2004).
43 O’Connor RA, Anderton SM: Foxp3+ regulatory T cells in the control of experimental CNS autoimmune disease. J. Neuroimmunol. 193, 1–11 (2008).
44 Jee Y, Piao WH, Liu R et al.: CD4+CD25+ regulatory T cells contribute to the therapeutic effects of glatiramer acetate in experimental autoimmune encephalomyelitis. Clin. Immunol. 125, 34–42 (2007).
45 Aricha R, Feferman T, Souroujon MC, Fuchs S: Overexpression of phosphodiesterases in experimental autoimmune myasthenia gravis: suppression of disease by a phosphodiesterase inhibitor. FASEB J. 20, 374–376 (2006).
46 Sheng JR, Li LC, Ganesh BB, Prabhakar BS, Meriggioli MN: Regulatory T cells induced by GM-CSF suppress ongoing experimental myasthenia gravis. Clin. Immunol. 128, 172–180 (2008).
47 Ben-David H, Sela M, Mozes E: Downregulation of myasthenogenic T cell responses by a dual altered peptide ligand via CD4+CD25+-regulated events leading to apoptosis. Proc. Natl Acad Sci. USA 102, 2028–2033 (2005).
48 Aruna BV, Sela M, Mozes E: Suppression of myasthenogenic responses of a T cell line by a dual altered peptide ligand by induction of CD4+CD25+ regulatory cells. Proc. Natl Acad. Sci. USA 102, 10285–10290 (2005).
49 Ben-David H, Venkata Aruna B, Sela M, Mozes E: A dual altered peptide ligand inhibits myasthenia gravis associated responses by inducing phosphorylated extracellular-regulated kinase 1,2 that upregulates CD4+CD25+Foxp3+ cells. Scand. J. Immunol. 65, 567–576 (2007).
50 Aruna BV, Sela M, Mozes E: Downregulation of T cell responses to AChR and reversal of EAMG manifestations in mice by a dual altered peptide ligand via induction of CD4+ CD25+ regulatory cells. J. Neuroimmunol. 177, 63–75 (2006).
51 Tang Q, Henriksen KJ, Bi M et al.: In vitro-expanded antigen-specific regulatory T cells suppress autoimmune diabetes. J. Exp. Med. 199, 1455–1465 (2004).
52 Belghith M, Bluestone JA, Barriot S, Mégret J, Bach JF, Chatenoud L: TGF-b-dependent mechanisms mediate restoration of self-tolerance induced by antibodies to CD3 in overt autoimmune diabetes. Nat. Med. 9, 1202–1208 (2003).
53 Tarbell KV, Petit L, Zuo X et al.: Dendritic cell-expanded, islet-specific CD4+ CD25+ CD62L+ regulatory T cells restore normoglycemia in diabetic NOD mice. J. Exp. Med. 204, 191–201 (2007).
54 Crispin JC, Martínez A, Alcocer-Varela J: Quantification of regulatory T cells in patients with systemic lupus erythematosus. J. Autoimmun. 21, 273–276 (2003).
55 Liu MF, Wang CR, Fung LL, Wu CR: Decreased CD4+CD25+ T cells in peripheral blood of patients with systemic lupus erythematosus. Scand. J. Immunol. 59, 198–202 (2004).

Immunotherapy (2009) 1(3)398 future science group
Review Sharabi & Mozes
56 Valencia X, Yarboro C, Illei G, Lipsky PE: Deficient CD4+CD25high T regulatory cell function in patients with active systemic lupus erythematosus. J. Immunol. 178, 2579–2588 (2007).
57 Hahn BH, Anderson M, Le E, La Cava A: Anti-DNA Ig peptides promote Treg cell activity in systemic lupus erythematosus patients. Arthritis Rheum. 58, 2488–2497 (2008).
58 Bagavant H, Tung KS: Failure of CD25+ T cells from lupus-prone mice to suppress lupus glomerulonephritis and sialoadenitis. J. Immunol. 175, 944–950 (2005).
59 Hsu WT, Suen JL, Chiang BL: The role of CD4CD25 T cells in autoantibody production in murine lupus. Clin. Exp.Immunol. 145, 513–519 (2006).
60 Wu HY, Staines NA: A deficiency of CD4+CD25+ T cells permits the development of spontaneous lupus-like disease in mice, and can be reversed by induction of mucosal tolerance to histone peptide autoantigen. Lupus 13, 192–200 (2004).
61 Chen Y, Cuda C, Morel L: Genetic determination of T cell help in loss of tolerance to nuclear antigens. J. Immunol. 174, 7692–7702 (2005).
62 Parietti V, Monneaux F, Décossas M, Muller S: Function of CD4+, CD25+ Treg cells in MRL/lpr mice is compromised by intrinsic defects in antigen-presenting cells and effector T cells. Arthritis Rheum. 58, 1751–1761 (2008).
63 Scalapino KJ, Tang Q, Bluestone JA, Bonyhadi ML, Daikh DI: Suppression of disease in New Zealand Black/New Zealand White lupus-prone mice by adoptive transfer of ex vivo expanded regulatory T cells. J. Immunol. 177, 1451–1459 (2006).
64 Kang HK, Michaels MA, Berner BR, Datta SK: Very low-dose tolerance with nucleosomal peptides controls lupus and induces potent regulatory T cell subsets. J. Immunol. 174, 3247–3255 (2005).
65 Reilly CM, Thomas M, Gogal R Jr et al.: The histone deacetylase inhibitor trichostatin A upregulates regulatory T cells and modulates autoimmunity in NZB/W F1 mice. J. Autoimmun. 31, 123–130 (2008).
66 Hahn BH, Singh RR, Wong WK, Tsao BP, Bulpitt K, Ebling FM: Treatment with a consensus peptide based on amino acid sequences in autoantibodies prevents T cell activation by autoantigens and delays disease onset in murine lupus. Arthritis Rheum. 44, 432–441 (2001).
67 La Cava A, Ebling FM, Hahn BH: Ig-reactive CD4+CD25+ T cells from tolerized (New Zealand Black × New Zealand White)F1 mice suppress in vitro production of antibodies to DNA. J. Immunol. 173, 3542–3548 (2004).
68 Tang XL, Smith TR, Kumar V: Specific control of immunity by regulatory CD8 T cells. Cell. Mol. Immunol. 2, 11–19 (2005).
69 Skaggs BJ, Singh RP, Hahn BH: Induction of immune tolerance by activation of CD8+ T suppressor/regulatory cells in lupus-prone mice. Hum. Immunol. 69, 790–796 (2008).
n Review article on the induction and function of CD8 Tregs in systemic lupus erythematosus (SLE)-prone mice.
70 Brimnes J, Allez M, Dotan I, Shao L, Nakazawa A, Mayer L: Defects in CD8+ regulatory T cells in the lamina propria of patients with inflammatory bowel disease. J. Immunol. 174, 5814–5822 (2005).
71 Zozulya AL, Wiendl H: The role of CD8 suppressors versus destructors in autoimmune central nervous system inflammation. Hum. Immunol. 69, 797–804 (2008).
72 Suzuki M, Konya C, Goronzy JJ, Weyand CM: Inhibitory CD8+ T cells in autoimmune disease. Hum. Immunol. 69, 781–789 (2008).
73 Tennakoon DK, Mehta RS, Ortega SB, Bhoj V, Racke MK, Karandikar NJ: Therapeutic induction of regulatory, cytotoxic CD8+ T cells in multiple sclerosis. J. Immunol. 176, 7119–7129 (2006).
74 Najafian N, Chitnis T, Salama AD et al.: Regulatory functions of CD8+CD28- T cells in an autoimmune disease model. J. Clin. Invest. 112, 1037–1048 (2003).
75 Montero E, Nussbaum G, Kaye JF et al.: Regulation of experimental autoimmune encephalomyelitis by CD4+, CD25+ and CD8+ T cells: ana lysis using depleting antibodies. J. Autoimmun. 23, 1–7 (2004).
76 Faunce DE, Terajewicz A, Stein-Streilein J: Cutting edge: in vitro-generated tolerogenic APC induce CD8+ T regulatory cells that can suppress ongoing experimental autoimmune encephalomyelitis. J. Immunol. 172, 1991–1995 (2004).
77 Lee YH, Ishida Y, Rifa’i M, Shi Z, Isobe K, Suzuki H: Essential role of CD8+CD122+ regulatory T cells in the recovery from experimental autoimmune encephalomyelitis. J. Immunol. 180, 825–832 (2008).
78 Ménager-Marcq I, Pomié C, Romagnoli P, van Meerwijk JP: CD8+CD28- regulatory T lymphocytes prevent experimental inflammatory bowel disease in mice. Gastroenterology 131, 1775–1785 (2006).
79 Ben-David H, Sharabi A, Dayan M, Sela M, Mozes E: The role of CD8+CD28 regulatory cells in suppressing myasthenia gravis-associated responses by a dual altered peptide ligand. Proc. Natl Acad. Sci. USA 104, 17459–17464 (2007).
80 Alvarado-Sánchez B, Hernández-Castro B, Portales-Pérez D et al.: Regulatory T cells in patients with systemic lupus erythematosus. J. Autoimmun. 27, 110–118 (2006).
81 Hahn BH, Singh RP, La Cava A, Ebling FM: Tolerogenic treatment of lupus mice with consensus peptide induces Foxp3-expressing, apoptosis-resistant, TGFb-secreting CD8+ T cell suppressors. J. Immunol. 175, 7728–7737 (2005).
82 Singh RP, La Cava A, Wong M, Ebling F, Hahn BH: CD8+ T cell-mediated suppression of autoimmunity in a murine lupus model of peptide-induced immune tolerance depends on Foxp3 expression. J. Immunol. 178, 7649–7657 (2007).
83 Singh RP, La Cava A, Hahn BH: pConsensus peptide induces tolerogenic CD8+ T cells in lupus-prone (NZB × NZW)F1 mice by differentially regulating Foxp3 and PD1 molecules. J. Immunol. 180, 2069–2080 (2008).
84 Chatenoud L, Salomon B, Bluestone JA: Suppressor T cells – they’re back and critical for regulation of autoimmunity. Immunol. Rev. 182, 149–163 (2001).
85 Hori S, Nomura T, Sakaguchi S: Control of regulatory T cell development by the transcription factor Foxp3. Science 299, 1057–1061 (2003).
86 Fontenot JD, Gavin MA, Rudensky AY: Foxp3 programs the development and function of CD4+CD25+ regulatory T cells. Nat. Immunol. 4, 330–336 (2003).
87 Bruder D, Probst-Kepper M, Westendorf AM et al.: Neuropilin-1: a surface marker of regulatory T cells. Eur. J. Immunol. 34, 623–630 (2004).
88 Ramsdell F: Foxp3 and natural regulatory T cells: key to a cell lineage? Immunity 19, 165–168 (2003).
89 Liston A, Farr AG, Chen Z, Benoist C, Mathis D, Manley NR, Rudensky AY: Lack of Foxp3 function and expression in the thymic epithelium. J. Exp. Med. 204, 475–480 (2007).
90 Sharpe AH, Freeman GJ: The B7–CD28 superfamily. Nat. Rev. Immunol. 2, 116–126 (2002).
91 Read S, Malmström V, Powrie F: Cytotoxic T lymphocyte-associated antigen 4 plays an essential role in the function of CD25+CD4+ regulatory cells that control intestinal inflammation. J. Exp. Med. 192, 295–302 (2000).
92 Takahashi T, Tagami T, Yamazaki S et al.: Immunologic self-tolerance maintained by CD25+CD4+ regulatory T cells constitutively expressing cytotoxic T lymphocyte-associated antigen 4. J. Exp. Med. 192, 303–310 (2000).

www.futuremedicine.com 399future science group
Harnessing regulatory T cells for the therapy of lupus & other autoimmune diseases Review
93 Tadokoro CE, Shakhar G, Shen S et al.: Regulatory T cells inhibit stable contacts between CD4+ T cells and dendritic cells in vivo. J. Exp. Med. 203, 505–511 (2006).
94 Miller MJ, Safrina O, Parker I, Cahalan MD: Imaging the single cell dynamics of CD4+ T cell activation by dendritic cells in lymph nodes. J. Exp. Med. 200, 847–856 (2004).
95 Stoll S, Delon J, Brotz TM, Germain RN: Dynamic imaging of T cell-dendritic cell interactions in lymph nodes. Science 296, 1873–1876 (2002).
96 Bousso P, Robey E: Dynamics of CD8+ T cell priming by dendritic cells in intact lymph nodes. Nat. Immunol. 4, 579–585 (2003).
97 Lohr J, Knoechel B, Nagabhushanam V, Abbas AK: T-cell tolerance and autoimmunity to systemic and tissue-restricted self-antigens. Immunol. Rev. 204, 116–127 (2005).
98 Fallarino F, Grohmann U, Hwang KW et al.: Modulation of tryptophan catabolism by regulatory T cells. Nat. Immunol. 4, 1206–1212 (2003).
99 Oderup C, Cederbom L, Makowska A, Cilio CM, Ivars F: Cytotoxic T lymphocyte antigen-4-dependent down-modulation of costimulatory molecules on dendritic cells in CD4+ CD25+ regulatory T-cell-mediated suppression. Immunology 118, 240–249 (2006).
100 Serra P, Amrani A, Yamanouchi J et al.: CD40 ligation releases immature dendritic cells from the control of regulatory CD4+CD25+ T cells. Immunity 19, 877–889 (2003).
101 Paust S, Lu L, McCarty N, Cantor H: Engagement of B7 on effector T cells by regulatory T cells prevents autoimmune disease. Proc. Natl Acad. Sci USA 101, 10398–10403 (2004).
102 Tang Q, Boden EK, Henriksen KJ, Bour-Jordan H, Bi M, Bluestone JA: Distinct roles of CTLA-4 and TGF-b in CD4+CD25+ regulatory T cell function. Eur. J. Immunol. 34, 2996–3005 (2004).
103 Wing K, Onishi Y, Prieto-Martin P et al.: CTLA-4 control over Foxp3+ regulatory T cell function. Science 322, 271–275 (2008).
n Recent article demonstrating the crucial role of cytotoxic T-lymphocyte antigen-4 in the function of CD4 Tregs.
104 Walker LS, Chodos A, Eggena M, Dooms H, Abbas AK: Antigen-dependent proliferation of CD4+ CD25+ regulatory T cells in vivo. J. Exp. Med. 198, 249–258 (2003).
105 Marie JC, Letterio JJ, Gavin M, Rudensky AY: TGF-b1 maintains suppressor function and Foxp3 expression in CD4+CD25+ regulatory T cells. J. Exp. Med. 201, 1061–1067 (2005).
nn Reports the essential link between TGF-b and maintenance and function of peripheral CD4 Tregs.
106 Yamagiwa S, Gray JD, Hashimoto S, Horwitz DA: A role for TGF-b in the generation and expansion of CD4+CD25+ regulatory T cells from human peripheral blood. J. Immunol. 166, 7282–7289 (2001).
107 Fahlén L, Read S, Gorelik L et al.: T cells that cannot respond to TGF-b escape control by CD4+CD25+ regulatory T cells. J. Exp. Med. 201, 737–746 (2005).
108 Oida T, Xu L, Weiner HL, Kitani A, Strober W: TGF-b-mediated suppression by CD4+CD25+ T cells is facilitated by CTLA-4 signaling. J. Immunol. 177, 2331–2339 (2006).
109 von Boehmer H: Mechanisms of suppression by suppressor T cells. Nat. Immunol. 6, 338–344 (2005).
110 Bennett F, Luxenberg D, Ling V et al.: Program death-1 engagement upon TCR activation has distinct effects on costimulation and cytokine-driven proliferation: attenuation of ICOS, IL-4, and IL-21, but not CD28, IL-7, and IL-15 responses. J. Immunol. 170, 711–718 (2003).
111 Keir ME, Butte MJ, Freeman GJ, Sharpe AH: PD-1 and its ligands in tolerance and immunity. Annu. Rev. Immunol. 26, 677–704 (2008).
112 Fife BT, Guleria I, Gubbels Bupp M et al.: Insulin-induced remission in new-onset NOD mice is maintained by the PD-1-PD-L1 pathway. J. Exp. Med. 203, 2737–2747 (2006).
113 Polanczyk MJ, Hopke C, Vandenbark AA, Offner H: Treg suppressive activity involves estrogen-dependent expression of programmed death-1 (PD-1). Int. Immunol. 19, 337–343 (2007).
114 Totsuka T, Kanai T, Makita S et al.: Regulation of murine chronic colitis by CD4+CD25- programmed death-1+ T cells. Eur. J. Immunol. 35, 1773–1785 (2005).
115 Collison LW, Workman CJ, Kuo TT et al.: The inhibitory cytokine IL-35 contributes to regulatory T-cell function. Nature 450, 566–569 (2007).
116 Liu W, Putnam AL, Xu-Yu Z et al.: CD127 expression inversely correlates with FoxP3 and suppressive function of human CD4+ T reg cells. J. Exp. Med. 203, 1701–1711 (2006).
117 Hsieh CS, Liang Y, Tyznik AJ, Self SG, Liggitt D, Rudensky AY: Recognition of the peripheral self by naturally arising CD25+ CD4+ T cell receptors. Immunity 21, 267–277 (2004).
118 Kasow KA, Chen X, Knowles J, Wichlan D, Handgretinger R, Riberdy JM: Human CD4+CD25+ regulatory T cells share equally complex and comparable repertoires with CD4+CD25- counterparts. J. Immunol. 172, 6123–6128 (2004).
119 Pacholczyk R, Ignatowicz H, Kraj P, Ignatowicz L: Origin and T cell receptor diversity of Foxp3+CD4+CD25+ T cells. Immunity 25, 249–259 (2006).
120 Tanchot C, Vasseur F, Pontoux C, Garcia C, Sarukhan A: Immune regulation by self-reactive T cells is antigen specific. J. Immunol. 172, 4285–4291 (2004).
121 Seddon B, Mason D: Peripheral autoantigen induces regulatory T cells that prevent autoimmunity. J. Exp. Med. 189, 877–882 (1999).
122 Tarbell KV, Yamazaki S, Olson K, Toy P, Steinman RM: CD25+ CD4+ T cells, expanded with dendritic cells presenting a single autoantigenic peptide, suppress autoimmune diabetes. J. Exp. Med. 199, 1467–1477 (2004).
123 Masteller EL, Warner MR, Tang Q, Tarbell KV, McDevitt H, Bluestone JA: Expansion of functional endogenous antigen-specific CD4+CD25+ regulatory T cells from nonobese diabetic mice. J. Immunol. 175, 3053–3059 (2005).
124 Hori S, Haury M, Coutinho A, Demengeot J: Specificity requirements for selection and effector functions of CD25+4+ regulatory T cells in anti-myelin basic protein T cell receptor transgenic mice. Proc. Natl Acad. Sci. USA 99, 8213–8218 (2002).
125 Bagavant H, Tung KS: Failure of CD25+ T cells from lupus-prone mice to suppress lupus glomerulonephritis and sialoadenitis. J. Immunol. 175, 944–950 (2005).
126 Samy ET, Wheeler KM, Roper RJ, Teuscher C, Tung KS: Cutting edge: Autoimmune disease in day 3 thymectomized mice is actively controlled by endogenous disease-specific regulatory T cells. J. Immunol. 180, 4366–4370 (2008).
127 Karim M, Kingsley CI, Bushell AR, Sawitzki BS, Wood KJ: Alloantigen-induced CD25+CD4+ regulatory T cells can develop in vivo from CD25-CD4+ precursors in a thymus-independent process. J. Immunol. 172, 923–928 (2004).
128 Klein L, Khazaie K, von Boehmer H: In vivo dynamics of antigen-specific regulatory T cells not predicted from behavior in vitro. Proc. Natl Acad. Sci. USA 100, 8886–8891 (2003).
129 Apostolou I, von Boehmer H: In vivo instruction of suppressor commitment in naive T cells. J. Exp. Med. 199, 1401–1408 (2004).
130 Thorstenson KM, Khoruts A: Generation of anergic and potentially immunoregulatory CD25+CD4 T cells in vivo after induction of peripheral tolerance with intravenous or oral antigen. J. Immunol. 167, 188–195 (2001).
Immunotherapy (2009) 1(3)400 future science group
Review Sharabi & Mozes
131 Kretschmer K, Apostolou I, Hawiger D, Khazaie K, Nussenzweig MC, von Boehmer H: Inducing and expanding regulatory T cell populations by foreign antigen. Nat. Immunol. 6, 1219–1227 (2005).
n Optimal conditions for the induction of functional antigen-specific CD4 Tregs.
132 Kim JM, Rudensky A: The role of the transcription factor Foxp3 in the development of regulatory T cells. Immunol. Rev. 212, 86–98 (2006).
133 Yamazaki S, Bonito AJ, Spisek R, Dhodapkar M, Inaba K, Steinman RM: Dendritic cells are specialized accessory cells along with TGF-b for the differentiation of Foxp3+ CD4+ regulatory T cells from peripheral Foxp3 precursors. Blood 110, 4293–4302 (2007).
134 Tai X, Cowan M, Feigenbaum L, Singer A: CD28 costimulation of developing thymocytes induces Foxp3 expression and regulatory T cell differentiation independently of interleukin 2. Nat. Immunol. 6, 152–162 (2005).
135 Salomon B, Lenschow DJ, Rhee L et al.: B7/CD28 costimulation is essential for the homeostasis of the CD4+CD25+ immunoregulatory T cells that control autoimmune diabetes. Immunity 12, 431–440 (2000).
136 Tang Q, Henriksen KJ, Boden EK et al.: Cutting edge: CD28 controls peripheral homeostasis of CD4+CD25+ regulatory T cells. J. Immunol. 171, 3348–3352 (2003).
137 Lohr J, Knoechel B, Jiang S, Sharpe AH, Abbas AK: The inhibitory function of B7 costimulators in T cell responses to foreign and self-antigens. Nat. Immunol. 4, 664–669 (2003).
138 Zheng SG, Wang JH, Stohl W, Kim KS, Gray JD, Horwitz DA: TGF-b requires CTLA-4 early after T cell activation to induce FoxP3 and generate adaptive CD4+CD25+ regulatory cells. J. Immunol. 176, 3321–3329 (2006).
139 Lyddane C, Gajewska BU, Santos E, King PD, Furtado GC, Sadelain M: Cutting edge: CD28 controls dominant regulatory T cell activity during active immunization. J. Immunol. 176, 3306–3310 (2006).
140 Fraser JH, Rincón M, McCoy KD, Le Gros G: CTLA4 ligation attenuates AP-1, NFAT and NF-kB activity in activatedT cells. Eur. J. Immunol. 29, 838–844 (1999).
141 Wu Y, Borde M, Heissmeyer V et al.: FOXP3 controls regulatory T cell function through cooperation with NFAT. Cell 126, 375–387 (2006).
142 Razmara M, Hilliard B, Ziarani AK, Chen YH, Tykocinski ML: CTLA-4 x Ig converts naive CD4+CD25- T cells into CD4+CD25+ regulatory T cells. Int. Immunol. 20, 471–483 (2008).
143 Wahl SM, Swisher J, McCartney-Francis N, Chen W: TGF-b: the perpetrator of immune suppression by regulatory T cells and suicidal T cells. J. Leukoc. Biol. 76, 15–24 (2004).
144 Yamagiwa S, Gray JD, Hashimoto S, Horwitz DA: A role for TGF-b in the generation and expansion of CD4+CD25+ regulatory T cells from human peripheral blood. J. Immunol. 166, 7282–7289 (2001).
145 Piccirillo CA, Letterio JJ, Thornton AM et al.: CD4+CD25+ regulatory T cells can mediate suppressor function in the absence of transforming growth factor b1 production and responsiveness. J. Exp. Med. 196, 237–246 (2002).
146 Huber S, Schramm C, Lehr HA et al.: Cutting edge: TGF-b signaling is required for the in vivo expansion and immunosuppressive capacity of regulatory CD4+CD25+ T cells. J. Immunol. 173, 6526–6531 (2004).
147 Samanta A, Li B, Song X et al.: TGF-b and IL-6 signals modulate chromatin binding and promoter occupancy by acetylated FOXP3. Proc. Natl Acad. Sci. USA 105, 14023–14027 (2008).
148 Zheng SG, Wang J, Wang P, Gray JD, Horwitz DA: IL-2 is essential for TGF-b to convert naive CD4+CD25- cells to CD25+Foxp3+ regulatory T cells and for expansion of these cells. J. Immunol. 178, 2018–2027 (2007).
149 Knoechel B, Lohr J, Kahn E, Bluestone JA, Abbas AK: Sequential development of interleukin 2-dependent effector and regulatory T cells in response to endogenous systemic antigen. J. Exp. Med. 202, 1375–1386 (2005).
150 Kang HK, Liu M, Datta SK: Low-dose peptide tolerance therapy of lupus generates plasmacytoid dendritic cells that cause expansion of autoantigen-specific regulatory T cells and contraction of inflammatory Th17 cells. J. Immunol. 178, 7849–7858 (2007).
151 Fontenot JD, Rasmussen JP, Gavin MA, Rudensky AY: A function for interleukin 2 in Foxp3-expressing regulatory T cells. Nat. Immunol. 6, 1142–1151 (2005).
152 D’Cruz LM, Klein L: Development and function of agonist-induced CD25+Foxp3+ regulatory T cells in the absence of interleukin 2 signaling. Nat. Immunol. 6, 1152–1159 (2005).
153 Vignali DA, Collison LW, Workman CJ: How regulatory T cells work. Nat. Rev. Immunol. 8, 523–532 (2008).
154 Collison LW, Workman CJ, Kuo TT et al.: The inhibitory cytokine IL-35 contributes to regulatory T-cell function. Nature 450, 566–569 (2007).
155 Sthoeger ZM, Dayan M, Tcherniack A et al.: Modulation of autoreactive responses of peripheral blood lymphocytes of patients with systemic lupus erythematosus by peptides based on human and murine anti-DNA autoantibodies. Clin. Exp. Immunol. 131, 385–392 (2003).
156 Waisman A, Shoenfeld Y, Blank M, Ruiz PJ, Mozes E: The pathogenic human monoclonal anti-DNA that induces experimental systemic lupus erythematosus in mice is encoded by a VH4 gene segment. Int. Immunol 7, 689–696 (1995).
157 Luger D, Dayan M, Zinger H, Liu JP, Mozes E: A peptide based on the complementarity determining region 1 of a human monoclonal autoantibody ameliorates spontaneous and induced lupus manifestations in correlation with cytokine immunomodulation. J. Clin. Immunol. 24, 579–590 (2004).
158 Mauermann N, Sthoeger ZM, Zinger H, Mozes E: Amelioration of lupus manifestations by a peptide based on the complementarity determining region 1 of an autoantibody in severe combined immunodeficient (SCID) mice engrafted with peripheral blood lymphocytes of systemic lupus erythematosus (SLE) patients. Clin. Exp. Immunol. 137, 513–520 (2004).
159 Sharabi A, Azulai H, Sthoeger ZM, Mozes E: Clinical amelioration of murine lupus by a peptide based on the complementarity determining region-1 of an autoantibody and by cyclophosphamide: similarities and differences in the mechanisms of action. Immunology 121, 248–257 (2007).
160 Sharabi A, Luger D, Ben-David H, Dayan M, Zinger H, Mozes E: The role of apoptosis in the ameliorating effects of a CDR1-based peptide on lupus manifestations in a mouse model. J. Immunol. 179, 4979–4987 (2007).
161 Sharabi A, Haviv A, Zinger H, Dayan M, Mozes E: Amelioration of murine lupus by a peptide, based on the complementarity determining region-1 of an autoantibody as compared with dexamethasone: different effects on cytokines and apoptosis. Clin. Immunol. 119, 146–155 (2006).
162 Zinger H, Eilat E, Meshorer A, Mozes E: Peptides based on the complementarity-determining regions of a pathogenic autoantibody mitigate lupus manifestations of (NZB × NZW)F1 mice via active suppression. Int. Immunol. 15, 205–214 (2003).
www.futuremedicine.com 401future science group
Harnessing regulatory T cells for the therapy of lupus & other autoimmune diseases Review
163 Sharabi A, Zinger H, Zborowsky M, Sthoeger ZM, Mozes E: A peptide based on the complementarity-determining region 1 of an autoantibody ameliorates lupus by upregulating CD4+CD25+ cells and TGF-b. Proc. Natl Acad. Sci. USA 103, 8810–8815 (2006).
164 Sharabi A, Mozes E: The suppression of murine lupus by a tolerogenic peptide involves Foxp3-expressing CD8 cells that are required for the optimal induction and function of Foxp3-expressing CD4 cells. J. Immunol. 181, 3243–3251 (2008).
n Requirement of CD8 Tregs for the induction of functional CD4 Tregs.
165 Rapoport MJ, Sharabi A, Aharoni D et al.: Amelioration of SLE-like manifestations in (NZB × NZW)F1 mice following treatment with a peptide based on the complementarity determining region 1 of an autoantibody is associated with a downregulation of apoptosis and of the pro-apoptotic factor JNK kinase. Clin. Immunol. 117, 262–270 (2005).
166 Rincon M, Enslen H, Raingeaud J et al.: Interferon-g expression by Th1 effector T cells mediated by the p38 MAP kinase signaling pathway. EMBO J. 17, 2817–2829 (1998).
167 Constant SL, Dong C, Yang DD, Wysk M, Davis RJ, Flavell RA: JNK1 is required for T cell-mediated immunity against Leishmania major infection. J. Immunol. 165, 2671–2676 (2000).
168 Green DR, Droin N, Pinkoski M: Activation-induced cell death in T cells. Immunol. Rev. 193, 70–81 (2003).
169 Nakajimab A, Hiraia H, Kayagakib N et al.: Treatment of lupus in NZB/W F1 mice with monoclonal antibody against Fas ligand. J. Autoimm. 14, 151–157 (2000).
170 Seery JP, Cattell V, Watt FM: Cutting edge: amelioration of kidney disease in a transgenic mouse model of lupus nephritis by administration of the caspase inhibitor carbobenzoxy-valyl-alanyl-aspartyl-(b-O-methyl)-fluoromethylketone. J. Immunol. 167, 2452–2455 (2001).
171 Riemekasten G, Hahn BH: Key autoantigens in SLE. Rheumatology (Oxford) 44, 975–982 (2005).
172 Munoz LE, van Bavel C, Franz S, Berden J, Herrmann M, van der Vlag J: Apoptosis in the pathogenesis of systemic lupus erythematosus. Lupus 17, 371–375 (2008).
173 Janko C, Schorn C, Grossmayer GE et al.: Inflammatory clearance of apoptotic remnants in systemic lupus erythematosus (SLE). Autoimmun. Rev. 8, 9–12 (2008).
174 Sela U, Sharabi A, Dayan M, Hershkoviz R, Mozes E: The role of dendritic cells in the mechanism of action of a peptide that ameliorates lupus in murine models. Immunology (2008) DOI: 10.1111/j.1365-2567.2008.02988.x (In press).