habit reversal vs. negative practice treatment of nervous tics
TRANSCRIPT

BEHAVIOR THERAPY 11, 169--178 (1980)
Habit Reversal vs. Negative Practice Treatment of Nervous Tics
N. H. AZRIN
R. G. NUNN
S. E. FRANTZ
Anna Mental Health and Developmental Center and Rehabilitation Institute, Southern Illinois University
Nervous tics without an apparent physical cause may occur in such forms as jerking of the head, twitching of the eyes, coughing, arm or shoulder jerking, nasal wheezing, facial grimaces, and rapid eyeblinking. The incidence of tics among adults is known primarily from patients whose problem has been sufficiently severe to seek treatment for the problem. For just one type of tic, spasmodic torticollis, Paterson (1945) found an incidence of about 1% among psychiatric admissions and .02% among general hospital admissions.
Controlled experimental evaluations of specific treatments with suffi- cient patients have been rare. Although lacking a control or comparison group, the following descriptive studies indicate that some types of treat- ment of muscular tics have not been notably effective. In psychotherapy with 10 Tourette patients, 40% were found to be slightly or not at all improved (Mahler & Luke, 1946). Garnett and Elbirlik (1953) found that only ½ of nine cases of spasmodic torticollis were "appreciably im- proved" by psychotherapy and other treatments. Patterson and Little (1943) found 73% of the torticollis cases were not "appreciably im- proved." In studies of surgery procedures, 71% were classified as "un- improved" in the study by Meares (1971), 54% by Rynearson and Wolt- man (1932), 39% by Poppen and Martinez-Niochet (1951), and 36% by Patterson and Little (1943).
Grateful acknowledgement is given to R. deVito for providing facilities and assistance, to J. Maedke for statistical assistance, and to P. K. Levison for his general assistance and encouragement. Requests for reprints should be sent to N. H. Azrin, Department of Treat- ment Development, Anna Mental Health and Developmental Center, 1000 N. Main St., Anna, IL 62906, Dr. R. Gregory Nunn is now at Kaiser Permanente, 7060 Claremont Mesa Blvd., San Diego, CA 92111.
169 0005-7894/80/0169-017851.00/0 Copyright 1980 by Association for Advancement of Behavior Therapy
All rights of reproduction in any form reserved.

170 AZRIN, NUNN, AND FRANTZ
Haloperidol has been used in large scale studies and has been found to be relatively effective, reducing tics by 79%, although 51% of the patients showed side effects (Bruun, Shapiro, Shapiro, Sweet, Wayne, & Solo- mon, 1976).
Behavioral studies of tics have been promising but also have been characterized by the lack of a control group and by very small numbers of patients, usually only one or two. The specific treatments have in- cluded feedback (Bernhardt, Hersen, & Barlow, 1972; Raft, 1962; Clee- land, 1973), response contingencies (Barrett, 1962), token economy (Do- leys & Kurtz, 1974), shock punishment (Brierley, 1967), self-monitoring (Hutzell, Platzek, & Logue, 1974), relaxation (McPherson, 1967), and systematic desensitization (Meares, 1973).
Negative practice training (Dunlap, 1932) has been one of the most common behavioral treatments for tics and consists of deliberate acting out of the tic in a massed practice schedule. Negative practice has been found to be at least somewhat effective with Tourette's Syndrome (Sav- icki & Carlin, 1972; Clark, 1966), eyebrow raising (Browning & Stover, 1971), eyeblinking (Costello, 1963; Frederick, 1971; Yates, 1958; Knepler & Sewall, 1974), multiple tics (Walton, 1961, 1964; Yates, 1958), mouth grimacing (Chapel, 1970), and head jerking (Feldman & Werry, 1966; Agras & Marshall, 1965; Turner, Hersen, & Alford, 1974). As was true of the other behavioral treatments, the above studies of negative practice have not included a control group and have not treated more than one or two patients except for Meares' (1973) study of eight patients.
The theoretical basis of the present behavior approach derived from behavioral studies with profoundly retarded and autistic persons who exhibited stereotyped, repetitive, nonfunctional movements such as body rocking, head shaking, and hand gazing. Such behavioral stereotypy has been found in about 2~ of profoundly retarded persons (Berkson & Dav- enport, 1962). An effective method of eliminating behavioral stereotypy was developed (Azrin, Kaplan, & Foxx, 1973; Foxx & Azrin, 1973) based in part on a competing response rationale in which the patients were required to practice movements which were topographically incompatible with the stereotypic response. The similarity of the head-jerking move- ments of spasmodic torticollis to the head shaking of the profoundly re- tarded persons suggested that a similar treatment might be effective for muscle tics of nonretarded persons. Accordingly, the method was mod- ified and tested with 11 nonretarded outpatients, 4 of whom suffered from tics such as head shaking, head jerking, arm jerking, tongue thrusting, and shoulder jerking, the others suffering from other nervous habits (Azrin & Nunn, 1973). The method, termed habit reversal, resulted in a mean decrease of 90% of the habit or tic on the first day, 95% after 1 month, and 99% after 3 months. No control group was used.
The success of the habit reversal method with the four tiqueurs in Azrin and Nunn (1973) suggested further and more extensive evaluation. The present study, therefore, used a larger number of patients, a longer follow-up, a greater variety of tics, and an experimental comparison of the habit reversal method with the negative practice method.

HABIT REVERSAL AND NEGATIVE PRACTICE 171
TABLE 1 COMPARISON OF THE CLIENTS IN THE TWO GROUPS WITH RESPECT TO SEVERAL
DIMENSIONS OF POSSIBLE RELEVANCE TO THEIR TIC PROBLEM AND ITS TREATMENT
Habit Negative reversal practice All patients patients patients
Number of patients 10 12 22 Female 2 3 5 Male 8 9 17 Average age 30 yrs 31 yrs 30 yrs Range of ages 12-62 yrs 11-57 yrs 11-62 yrs Age at onset of tic 11 yrs 13 yrs 12 yrs Average duration of tic 20 yrs 17 yrs 19 yrs Median daily frequency of tic 425/day 450/day 450/day Mean daily frequency of tic 1,130/day 1,572/day 1,360/day Range of frequency of tic 50-5,500/day 6-9,000/day 6-9,000/day No. of patients seeking
other treatments* 8 12 20 Currently receiving drugs
for tic 1 3 4 Received drugs for tic in past 6 10 16
* All saw neurologists.
METHOD Subjects and Experimental Design
A newspaper advertisement in a large city was used to obtain patients. All patients were required to be examined by a neurologist and all 22 were included whose tics were not judged to have a medical etiology. A coin flip was used to assign patients to the two treatment conditions, resulting in 10 patients in the habit reversal and 12 patients in the negative practice treatment.
Table 1 compares the clients in the two groups with respect to several dimensions of possible relevance to their tic problem and its treatment. All patients had been examined and/or treated by a neurologist as re- quired by the criterion for inclusion in the study; in addition, 20 of the 22 patients had been treated by other kinds of therapists, such as psy- chologists and psychiatrists. Of the 22 patients, 16 had been treated in the past by drugs, primarily Valium, Haloperidol, and Librium; 4 were receiving these drugs at the start of the study. For all of these dimensions of age, sex, tic frequency, etc. shown in Table 1, analysis by Chi Square or t test showed no statistically significant difference between the two groups for any of these dimensions.
Tic
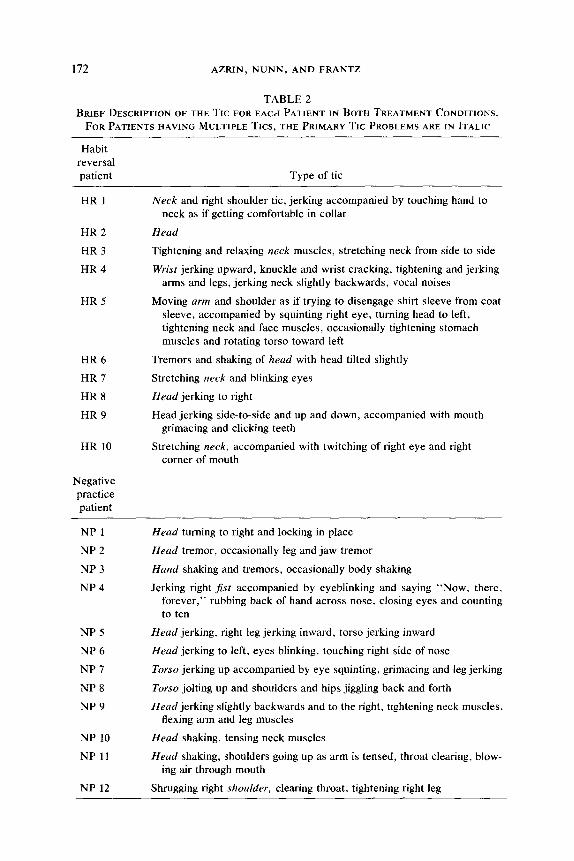
Table 2 provides a brief description of the tics for each patient in both treatment conditions. Many patients had multiple tics, in which case the
172 AZRIN, NUNN, AND FRANTZ
TABLE 2 BRIEF DESCRIPTION OF THE TIC FOR EACH PATIENT IN BOTH TREATMENT CONDITIONS.
FOR PATIENTS HAVING MULTIPLE TICS, THE PRIMARY TIC PROBLEMS ARE IN ITALIC
Habit reversal patient Type of tic
HR 1
HR 2
HR 3
HR 4
HR 5
HR 6
HR 7
HR 8
HR 9
HR 10
Negative practice patient
Neck and right shoulder tic, jerking accompanied by touching hand to neck as if getting comfortable in collar
Head
Tightening and relaxing neck muscles, stretching neck from side to side
Wrist jerking upward, knuckle and wrist cracking, tightening and jerking arms and legs, jerking neck slightly backwards, vocal noises
Moving arm and shoulder as if trying to disengage shirt sleeve from coat sleeve, accompanied by squinting right eye, turning head to left, tightening neck and face muscles, occasionally tightening stomach muscles and rotating torso toward left
Tremors and shaking of head with head tilted slightly
Stretching neck and blinking eyes
Head jerking to right
Head jerking side-to-side and up and down, accompanied with mouth grimacing and clicking teeth
Stretching neck, accompanied with twitching of right eye and right corner of mouth
NP i
NP 2
NP 3
NP 4
NP 5
NP 6
NP 7
NP 8
NP 9
NP 10
NP 11
NP 12
Head turning to right and locking in place
Head tremor, occasionally leg and jaw tremor
Hand shaking and tremors, occasionally body shaking
Jerking right fist accompanied by eyeblinking and saying "Now, there, forever," rubbing back of hand across nose, closing eyes and counting to ten
Head jerking, right leg jerking inward, torso jerking inward
Head jerking to left, eyes blinking, touching right side of nose
Torso jerking up accompanied by eye squinting, grimacing and leg jerking
Torso jolting up and shoulders and hips jiggling back and forth
Head jerking slightly backwards and to the right, tightening neck muscles, flexing arm and leg muscles
Head shaking, tensing neck muscles
Head shaking, shoulders going up as arm is tensed, throat clearing, blow- ing air through mouth
Shrugging right shoulder, clearing throat, tightening right leg
H A B I T REVERSAL A N D N E G A T I V E PRACTICE 173
primary and most frequent tic(s) are indicated in Table 2 by italic. Most of the tics involved the head, neck, or shoulders, but some patients also had eyeblinking, hand jerking, vocalization, torso jerking, grimacing and throat clearing, or leg movements. Treatment was given primarily for the primary tic movements, and all the daily response rec- ords were also for the primary tics.
Habit Reversal Treatment
The habit reversal treatment consisted of two sets of procedures, the first of which was specific to the immediate control of the tic, whereas the second set was general behavior therapy procedures. The primary corrective procedure was the competing reaction in which the patient learned to exert isometric pressure of the muscles that were opposed to the tic movement. Table 3 briefly describes the competing response used for the primary tics exhibited by the patients in the habit reversal treat- ment. The patient was taught to perform this competing reaction in such a manner that it was not apparent to an observer, this being done by practicing in front of a mirror and the therapist. The amount of tension exerted was that amount just sufficient to " lock" the body part in place and to prevent even deliberate attempts to perform the tic movement. The competing reaction was to be performed for 3 minutes whenever a tic movement occurred, or was likely to occur, as well as being practiced daily at home in front of a mirror. In those few instances in which the isometric competing reaction was not sufficient to block the tic, the pa- tient was taught to use other bodily assist measures even though they were obtrusive, but to discontinue them as the simpler isometric con- traction proved sufficient. These temporary assist measures are listed parenthetically in Table 3. The general behavior therapy procedures in- cluded a review of the inconveniences caused by the tic, identification of the situations and persons associated with either a high or low probability of tic episodes, heightening awareness of the tic by deliberately perform- ing and describing it in front of a mirror, relaxation training, daily self- recording of the tic episodes, social support by the presence of a family member during treatment, behavior rehearsal of the competing reaction, relaxation exercises, and deliberate immediate display of the improve- ment to provide reinforcement for treatment adherence. The general pro- cedure has been described in detail elsewhere (Azrin & Nunn, 1973, 1977).
Treatment was given during one or two sessions of about 2½ hours duration per session. Thereafter the therapist maintained telephone con- tact during the first few days with the patient and family member, in- creasing the interval between calls as the patient gained control.
Negative Practice Treatment
The patients receiving the negative practice treatment completed the same intake questionnaires and discussion concerning difficulties caused by the tics, origin of the habits, previous treatments, and so forth, as did the habit reversal patients. They also received three pages of written

174 AZRIN, NUNN, AND FRANTZ
TABLE 3 DESCRIPTION OF THE COMPETING REACTION FOR VARIOUS TICS
Tic Competing reaction
Backwards head jerking
Sideways head jerking
Shoulder jerking
Head shaking
Wrist tics
Neck stretching
Moving shoulder and arm as if disengaging sleeve from jacket
With the head in a centered position, contract neck flexors so that head tilts slightly downward. Neck appears shortened and bulged. (If this reaction is inadequate, push the chin into the sternum. Gradually decrease the contraction so that the head is raised off the stenum in the more natural head-upright position.)
Keep head in center position and contract neck flexors so that head tilts slightly downward. (If this reaction cannot be maintained for 3 minutes, is inadequate, put hand on side of face and push the head in the direction opposite to the tic.) After strenghtening of opposing neck muscles, change to the isometric neck flexor reaction without the hand assist.
Contract shoulders by depressing the shoulders down as far as they will go while keeping the arms close to the body.
Shift head posture from very erect or angled to drooping or tilting the head slightly forward. Slightly contract neck muscles that oppose shaking movements.
Push hands on arms of chairs, desk, leg, etc. and contract the muscles so that hands are pushing opposite the tic movement (i.e., contract hands down if the wrist jerks upward).
Contract neck flexors and depress head so that neck appears shortened.
Contract shoulder by depressing the shoulder downward and pressing arm to side of body.
i n s t ruc t ions regarding nega t ive prac t ice t r e a t m e n t adap ted f rom Smith (1957), and the therapis t d i scussed the ra t iona le with them. The bas ic p rocedu re i nvo lved pa t ien ts pu rpose ly pe r fo rming the tic in f ront of a mirror for 30-sec periods over a 1-hour per iod in terspersed by br ief rests, and saying to themse lves , " th i s is what I ' m supposed n o t to d o . " T h e y were to c o n t i n u e the exerc ises each day unt i l 4 days after the habi t was b roken , after which they would gradual ly d i s c on t i nue the pract ice for an addi t iona l 2 weeks , bu t to r e s u m e pract ice if a re lapse occurred . Af ter t r ea tmen t , they were ins t ruc ted to prac t ice the nega t ive prac t ice tech- n iques in f ront of a mir ror for the 30-sec per iods a bou t eve ry hour. These pa t ien ts were g iven the same record ing sheets and record ing ins t ruc t ions as the habi t reversa l pa t ien ts and also rece ived one t r e a t me n t sess ion of abou t 2½ hours dura t ion .

H A B I T R E V E R S A L A N D N E G A T I V E P R A C T I C E 175
Recording The recording was the same for both treatment conditions. At the time
of the initial phone contact, the patients were instructed to attend to the number of tic episodes they were having, and their reports of that number were taken at the initial office visit as the baseline frequency. After the initial office visit, the patients recorded each episode on a recording card that they carried with them and totaled the number each day on a chart that was mailed in at regular intervals or reported by phone. Follow-up data were obtained for 4 weeks for patients in both treatments and up to 18 months for the habit reversal patients. No quantitative reliability or validity data were available. Qualitative checks were available in that all patients who reported at the office session that their tics were occurring every few seconds or minutes did actually exhibit the tics and at a rate roughly in accord with their reports. A posttreatment source of qualitative confirmation of the patients' reports were the reports of the family mem- bers of the eight patients who were contacted as part of the social support component of the habit reversal treatment. Their reports were also in rough agreement with the quantitative reports of the patients; for seven of the eight patients, the patients' reports of zero tic episodes were con- firmed by the family contacts' reports that the patients no longer exhibited the tic at that time.
RESULTS Fig. 1 shows the mean percentage reduction of the tic episodes. Neg-
ative practice reduced the tic episodes by about 1/3 during the 4-week follow-up that was obtained. Positive practice reduced the tic episodes by 84% on the first day. The tics decreased progressively thereafter by 92% by the fourth week, by 97% during the second month, 99% during the fourth, fifth, and sixth months and at the 18-month follow-up showed a 97% reduction. These follow-up data were obtainable for all 10 habit reversal patients during the first 4 weeks, from 7 patients up to the fourth month, and from 5 patients after the fourth month.
Analysis of variance of repeated measures yielded F(1,20) = 16.43, p < .001 for the difference between treatments, but no significant difference between time periods or for the interaction between time and treatment. Separate t tests showed that the reduction in the tics was significantly greater for the habit reversal treatment for each of the 10 time periods (p < .01).
The individual data showed that during the fourth week, 2 of the 12 (17%) negative practice patients were virtually free of their tics (one or less tic episodes per day) vs. 8 of the 10 (80%) habit reversal patients. During the third month, 86% of the habit reversal patients were virtually free of their tics and 80% at the 18-month follow-up. All five of the habit reversal clients who were unavailable for the 18-month follow-up had less than one tic episode per day at their last available follow-up dates.
Of the 10 habit reversal patients, 8 reported at their last follow-up that their secondary tics, which had not been treated directly, disappeared along with the primary tic or were not a significant problem.

176 A Z R I N , N U N N , A N D F R A N T Z
PRE TREATMENT
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
POST TREATMENT
NEGATIVE PRACTICE TREATMENT
N = 22
J ~ ~ W ~ ~ ~ ERLTREATMENT
, , , , i , , , , i i , T T 1 2 3 4 5 6 7 2 3 t~ 2 3 i+
DAYS WEEKS MOtQTHS
TIME SINCE TREATMENT
A
I !
5 6 18
FIG. 1. Reduction of tics by two treatment methods. The tic frequency is expressed as the average percentage reduction relative to the pretreatment frequency which is 0% re- duction by definition. The vertical dotted line designates the time when treatment was given. Time since treatment is expressed in days for the first week, in weeks for the first month, and in months thereafter plus an 18-month follow-up. The day designated "0" is when treatment was given. The upper curve is for the patients receiving negative practice and the lower curve is for those receiving habit reversal treatment.
DISCUSSION The habit reversal treatment appears to be an effective approach to
treating diverse nervous tics. The tics decreased by 84% on the first day and decreased further to a 99% reduction at 4-6 months. The 18-month follow-up still showed a 97% reduction. The treatment required one or two training sessions plus follow-up telephone calls. The habit reversal treatment was more effective than the negative practice treatment which reduced tics by about ½. The use of the control group, larger sample size, and longer follow-up in the present study extends the findings of the previous study of this method (Azrin & Nunn, 1973) and indicates that the habit reversal method reduces diverse nervous tics for an extended duration and is more effective than the alternative negative practice meth- od. Evaluation of its effectiveness relative to other treatments for tics must await controlled studies. Such controlled studies for other types of habits have found that the habit reversal method was more effective than desensitization in treating stuttering (Azrin, Nunn, & Frantz, 1979) and wait list control for treating nailbiting (Nunn & Azrin, 1976).

HABIT REVERSAL AND NEGATIVE PRACTICE 177
REFERENCES Agras, S., & Marshall, C. The application of negative practice to spasmodic torticollis.
American Journal of Psychiatry. 1965, 122, 579-582. Azrin, N. H., Kaplan, S. J., & Foxx, R, M. Autism reversal: Eliminating stereotyped
self-stimulation of retarded individuals. American Journal of MentalDeficiency, t973, 78, 241-248.
Azrin, N. H., & Nunn, R .G. Habit reversal: A method of eliminating nervous habits and tics. Behaviour Research and Therapy, 1973, 11,619-628.
Azrin, N. H., & Nunn, R. G. Habit control: (Stuttering, nail biting, and other nervous habits). New York: Simon & Schuster, 1977.
Azrin, N. H., Nunn, R. G., & Frantz, S, E. Comparison of regulated-breathing vs. ab- breviated desensitization on reported stuttering. Journal of Speech and Hearing Dis- orders, 1979, 44, 331-339.
Barrett, B. H. Reduction in rate of multiple tics by free operant conditioning methods. Journal of Nervous and Mental Disease, 1962, 135, 187-195.
Berkson, G., & Davenport, R. J., Jr. Stereotyped movements of mental defectives. I. Initial survey. American Journal of Mental Deficiency, 1962, 66, 849-852.
Bernhardt, A. J., Hersen, M., & Barlow, D . H . Measurement and modification of spas- modic torticollis: An experimental analysis. Behavior Therapy. 1972, 3, 294-297.
Brierley, H. The treatment of hysterical spasmodic torticollis by behavior therapy. Be- haviour Research and Therapy, 1967, 5, 139-142.
Browning, R. M., & Stover, D. O. Behavior modification in child treatment. Chicago: Aldine/Atherton, 1971.
Bruun, R. D., Shapiro, A. K., Shapiro, E., Sweet, R., Wayne, H., & Solomon, G . E . A follow-up of 78 patients with Gilles de la Tourette 's syndrome. American Journal of Psychiatry, 1976, 133, 944-947.
Chapel, J . L . Behavior modification techniques with children and adolescents. Canadian Psychiatric Association Journal, 1970, 15, 315-318.
Clark, D. F. Behavior therapy of Gilles de la Tourette 's syndrome. British Journal of Psychiatry, 1966, 112, 771-778.
Cleeland, C .S . Behavioral technics in the modification of spasmodic torticollis. Neurol- ogy, 1973, 23, 1241-1247.
Costello, C. G. The essentials of behavior therapy. Canadian Psychiatric Association Journal, 1963, 8, 162-166.
Doleys, D. M., & Kurtz, P.S. A behavioral treatment program for the Gilles de la Tourette syndrome. Psychological Reports, 1974, 35, 43-48.
Dunlap, K. Habits: Their making and unmaking. New York: Liveright, 1932. Feldman, R. B., & Werry, J. S. An unsuccessful attempt to treat a tiqueur by massed
practice. Behaviour Research and Therapy, 1966, 4, 111-117. Foxx, R. M., & Azrin, N. H. The elimination of autistic self-stimulatory behavior by
overcorrection. Journal of Applied Behavior Analysis, 1973, 6, 1-14. Frederick, C . J . Treatment of a tic by systematic desensitization and massed response
evocation. Journal of Behavior Therapy and Experimental Psychiatry, 1971, 2, 281- 283.
Garnett, R. W., Jr., & Elbirlik, K. Torticollis. Southern Medical Journal, 1953, 46, 892- 898.
Hutzell, R. R., Platzek, D., & Logue, P .E . Control of symptoms of Gilles de la Tourette's syndrome by self-monitoring. Journal of Behavior Therapy and Experimental Psy- chiatry, 1974, 5, 71-76.
Knepler, K. N., & Sewall, S. Negative practice paired with smelling salts in the treatment of a tic. Journal of Behavior Therapy and Experimental Psychiatry. 1974, 5, 189-192.

178 AZRIN, NUNN, AND FRANTZ
Mahler, M. S., & Luke, J. A. Outcome of the tic syndrome. Journal of Nervous and Mental Disease, 1946, 103, 433-445.
McPherson, E. L . R . Control of involuntary movement. Behaviour Research and Ther- apy, 1967, 5, 143-145.
Meares, R.A. Natural history of spasmodic torticollis and effect of surgery. Lancet, 1971, 2, 149.
Meares, R .A . Behavior therapy and spasmodic torticollis. Archives of General Psychia- try, 1973, 28, 104-107.
Nunn, R. G., & Azrin, N. H. Eliminating nailbiting by the habit reversal procedure. Behaviour Research and Therapy, 1976, 14, 339-348.
Paterson, M.T. Spasmodic torticollis: Results of psychotherapy in 21 cases. The Lancet, 1945, 249, 556-559.
Patterson, R. M., & Little, S .C . Spasmodic torticollis. Journal of Nervous and Mental Disease, 1943, 98, 571-599.
Poppen, J. L., & Martinez-Niochet, A. Spasmodic torticollis. Surgical Clinics of North America, 1951, 31, 883-890.
Raft, A. A. Learning theory and the treatment of tics. Journal of Psychosomatic Re- search. 1962, 6, 71-76.
Rynearson, E. H., & Woltman, H . W . Spasmodic torticollis: Results of removal of foci of infection and treatment with specific vaccine. American Journal of the Medical Sciences, 1932, 183, 559-562.
Savicki, V., & Carlin, A . S . Behavioral treatment of Gilles de la Tourette's syndrome. International Journal of Child Psychotherapy, 1972, 1, 97-109.
Smith, M. Effectiveness of symptomatic treatment of nailbiting in college students. Psy- chological Newsletter, 1957, 8, 219-231.
Turner, S. M., Hersen, M., & Alford, H. Effects of massed practice and meprobamate on spasmodic torticollis: An experimental analysis. Behaviour Research and Therapy, 1974, 12, 259-260.
Walton, D. Experimental psychology and the treatment of a tiqueur. Journal of Child Psychology and Psychiatry, 1961, 2, 148-155.
Walton, D. Massed practice and simultaneous reduction in drive level---Further evidence of the efficacy of this approach to the treatment of tics. In H. J. Eysenck (Ed.), Experiments in behavior therapy. London: Pergamon Press, 1964.
Yates, A . J . The application of learning theory to the treatment of tics. Journal of Ab- normal and Social Psychology. 1958, 56, 175-182.
RECEIVED" July 9, 1979; REVISED: August 7, 1979 FINAL ACCEPTANCE: August 21, 1979