final report the stroke rehabilitation pilot project of seo this project was funded by the ontario...
TRANSCRIPT

Final Final ReportReportFinal Final
ReportReportThe Stroke The Stroke Rehabilitation Pilot Rehabilitation Pilot
Project of SEOProject of SEOThis project was funded by the This project was funded by the
Ontario Ministry of Health, Long Ontario Ministry of Health, Long Term CareTerm Care
Cally Martin BScPT, MSc (Rehab)Cally Martin BScPT, MSc (Rehab)
John Paterson BEd, MSc (Rehab)John Paterson BEd, MSc (Rehab)
Patient and FamilyPatient and FamilyContinuum of careContinuum of care
The Ontario Stroke StrategyThe Ontario Stroke Strategy
Stroke recognition
Prevention
Pre-hospital
Emergency Acute
REHAB
Community
Transition
VISIONVISIONTo ensure that all Ontarians have access to To ensure that all Ontarians have access to the best possible quality stroke care, from the best possible quality stroke care, from prevention, through treatment and prevention, through treatment and rehabilitation, to community re-integration.rehabilitation, to community re-integration.

NORTHU
MBERLA
ND
Southeastern Ontario Region
Population 565,50012,500 miles2
20,000 km2
H
H
HH
H
HHH
H
H
H

The Discharge Link Project (DLP)The Discharge Link Project (DLP)
GoalTo investigate best practice related to stroke client transition from inpatient rehabilitation to the community by:
enhancing therapy augmenting provider
communication

The DLP ProcessThe DLP Process
Participants included: – Adults with new stroke– Recently discharged from inpatient rehab– Require home care– Going home or to residential setting
Excluded:– Those going to LTC

The DLP ProcessThe DLP Process
The Enhanced Therapy (first 2 mths) – Pre-Discharge Link Meeting (OT to OT) – Post-Discharge OT & PSW meeting– Month 1
up to 2 extra visits/wk OT, PT and/or SLP +5 hours extra PSW/wk
– Month 2 up to 1 extra visit/wk OT, PT and/or SLP
Allocation to group: ability of CCAC to provide enhanced service

The DLP ProcessThe DLP ProcessEvaluation Function:
– FIM (CIHI-NRS) at Rehab Admission and Discharge, 3, 6 & 12 mos after discharge
RNL and Health Status at 3mos Client satisfaction survey Key Informant Interviews & focus groups CCAC workload Hospital readmissions
Qualitative and quantitative analysis

DLP Distribution of Participants DLP Distribution of Participants
Total of 61 (24 U + 37 E)
Groups were well matchedCommunity Care Access Centre
Usual care
group
Enhanced
therapy group
Totals
Hastings and Prince Edward (HPE)
6 12 18
Kingston, Frontenac, Lennox & Addington Counties (KFL&A)
8 13 21
Lanark, Leeds and Grenville (LLG)
10 12 22
Totals 24 37 61

DLP Severity of StrokeDLP Severity of Stroke FRG = Functionally Related Group (at
Admission) Based on ratio of motor and cognitive sub-
scores on the FIM
0123456789
participants
1 2 3 4 5 6 7 8 9
FRG Category
NormalEnhanced

Stroke FRGs Organized into Upper, Middle & Lower Bands
Stroke FRGs Organized into Upper, Middle & Lower Bands
Motor
Motor
Motor
Motor
Motor
Cognitive
CognitiveAge
FRGMedianLOS
>48
13-48
>62
49-62
38-48
13-37
16-74
>74
>30
5-30
74-91
63-73
56-62
49-55
18-35
5-17
9
8
7
6
5
4
3
2
1
9.0
13.0
15.0
18.0
21.0
27.0
32.0
28.0
36.0
Upper Band
Middle Band
Lower Band
Functional Task Benchmarks for Stroke Rehabilitation. Margaret G. Stineman, MD, Roger C. Fiedler, PhD,Carl V. Granger, MD, Greg Maislin, MS, MA. Arch Phys Med Rehabil Vol. 79, May 1998 Pg. 499

DLP: LOS and Wait Times DLP: LOS and Wait Times
Total time post onset U=106.5U=106.5 E=96.7E=96.7
23.0
7.635.3
28.1
53.8
56.6Usual Care
Enhanced
Days
Acute LOS
Rehab LOS
Wait time forCCAC

DLP: Community Provider
Service (First 2 months, incl. 12 Link
Meetings)
DLP: Community Provider
Service (First 2 months, incl. 12 Link
Meetings)
16.1
22.4
3.5
11.3
0 5 10 15 20 25
Usual CareEnhanced
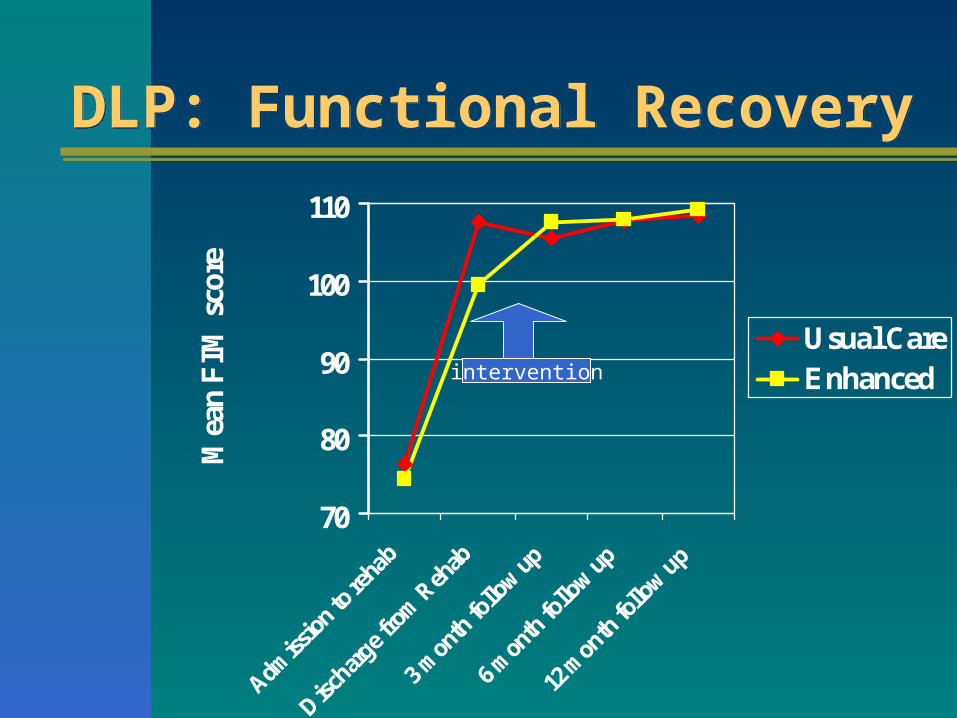
DLP: Functional Recovery DLP: Functional Recovery
70
80
90
100
110
Admiss
ion t
o reh
ab
Discha
rge f
rom Reh
ab
3 mon
th fo
llow up
6 mon
th fo
llow up
12 m
onth fo
llow up
Mea
n FIM
sco
re
Usual CareEnhancedintervention

DLP: Functional Recoverybetween Discharge and
3 mths
DLP: Functional Recoverybetween Discharge and
3 mths
76.3
107.5105.5
74.4
99.4
108.3107.7
109.2107.9107.5
70
80
90
100
110
Admissionto rehab
Dischargefrom
Rehab
3 monthfollow up
6 monthfollow up
12 monthfollow up
Mean
FIM
score N
E

DLP: Change in Recovery DLP: Change in Recovery
25
7.311.5 11
31.3
-2.1
0.2
-2-5
0
5
10
15
20
25
30
35
ADM - DIS DIS - 3mths
DIS - 6mths
DIS - 12mths
Mean c
hange in
FIM
sco
re
Usual CareEnhanced

Regression AnalysisRegression Analysis
The most significant predictors of the improved change in function were:1. FIM score at Discharge p = 0.004*
2. Rehab Care Professional Visits p = 0.169#
* significant at p<0.05
# evidence of contribution to the model

DLP: Hospital ReadmissionsDLP: Hospital Readmissions
U(24)U(24) E (37)E (37)
Re-hospitalizations 11(46%) 9(24%)
Total bed-days 133 73Ave days per stay 8.3
6.1

DLP: Reasons for ReadmissionsDLP: Reasons for Readmissions
Usual Care Group
Fall, multiple fracturesFall, Pelvic fracture
TIA, SeizurePneumoniaInfectionHeart Condition
Enhanced Care Group
Knee replacementHip replacementBypass Surgery
TIA, SeizurePneumoniaInfectionHeart Condition

DLP: Hospital Readmissions - CostsDLP: Hospital Readmissions - Costs
$87,514
$3646
$0
$20,000
$40,000
$60,000
$80,000
$100,000
Overall Cost Cost perperson
Cost of Re-Hospitalizations
Enhanced (37)
Usual Care (24)

DLP: Cost ComparisonsDLP: Cost Comparisons
1,298
2,146
3,4443,646
509
4,155
$0$500
$1,000$1,500$2,000$2,500$3,000$3,500$4,000$4,500
ave. re-admission
cost
ave. cost ofcommunity
therapy
net cost
cost
per pers
on
Usual CareEnhanced

““A cycle of discontinuity”A cycle of discontinuity”
“You get so used to working within a system that you … you forget that there might be something better out there...”
“I finally get to do real OT!”
Key informant interviews:Voices of Providers….Key informant interviews:Voices of Providers….

Key informant interviews:Voices of clients….Key informant interviews:Voices of clients….
“I am totally overwhelmed”
““Horrific”Horrific”““Hell on earth”Hell on earth”
“It was hard. It was tough”
“if spouses become therapists… it really degrades and demises the personal
relationship.”
“What do you do?”

DLP RecommendationsDLP Recommendations
1. Provide enhanced & timely professional therapy for stroke clients
2. Consider priority setting for those recovering from new stroke
3. Increase system responsiveness and flexibility
4. Establish a formal process for coordination of care
5. Promote models of care that promote client recovery

DLP Recommendations, p2DLP Recommendations, p2
6. Investigate strategies to recruit and retain professional services and promote stable provider workforce
7. Provide stroke rehab education to CCAC, professional staff and PSWs
8. Explore role of OT, PT communication assistants
9. Support caregivers
10.Regional planning

Thank you!Thank you!
The Ontario Ministry of Health, Long-Term Care for funding the project
The Rehab subcommitteeCCACs and Hospitals of SEOCare providersClients, Caregivers/Family