fat embolism
TRANSCRIPT

By
Dr. Jitendra Wadhwani
PG ORTHOPAEDICS
PGIMS, ROHTAK
FAT EMBOLISM SYNDROME

Zenker, a pathologist,1st identified fat embolism syndrome at autopsy 1862.
First diagnosed in 1873 by Dr Von Bergmann
1879 Fenger and Salisbury published description of FES
HISTORY

Fat Emboli: Fat particles or droplets that travel through the circulation
Fat Embolism: A process by which fat emboli passes into the bloodstream and lodges within a blood vessel.
Fat Embolism Syndrome (FES): serious manifestation of fat embolism occasionally causes multi system dysfunction, the lungs are always involved and next is brain
DEFINITIONS
FAT EMBOLISM SYNDROME:
Clinical diagnosis, No specific laboratory test is diagnostic
Mostly associated with long bone and pelvic #, and more frequent in closed # then open #
Single long bone fracture 1-5% chance of developing FES, and increases with number of #
Onset is 24-72 hours from initial insult
Mortality: 5-15%
CAUSES
CAUSES CONTD..
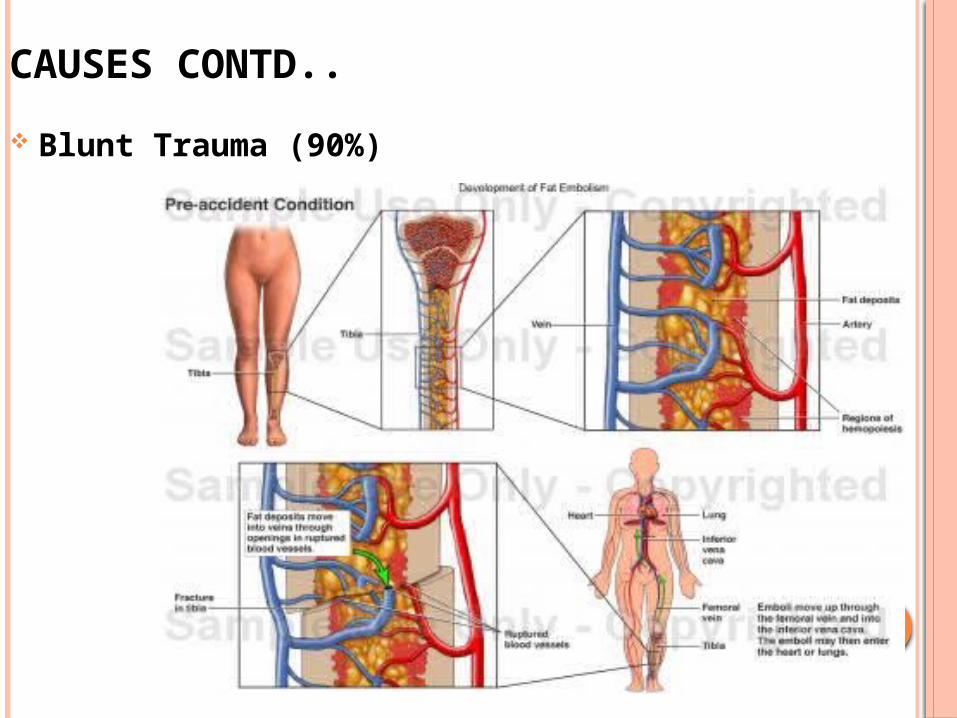
Blunt Trauma (90%)

CAUSES CONTD..
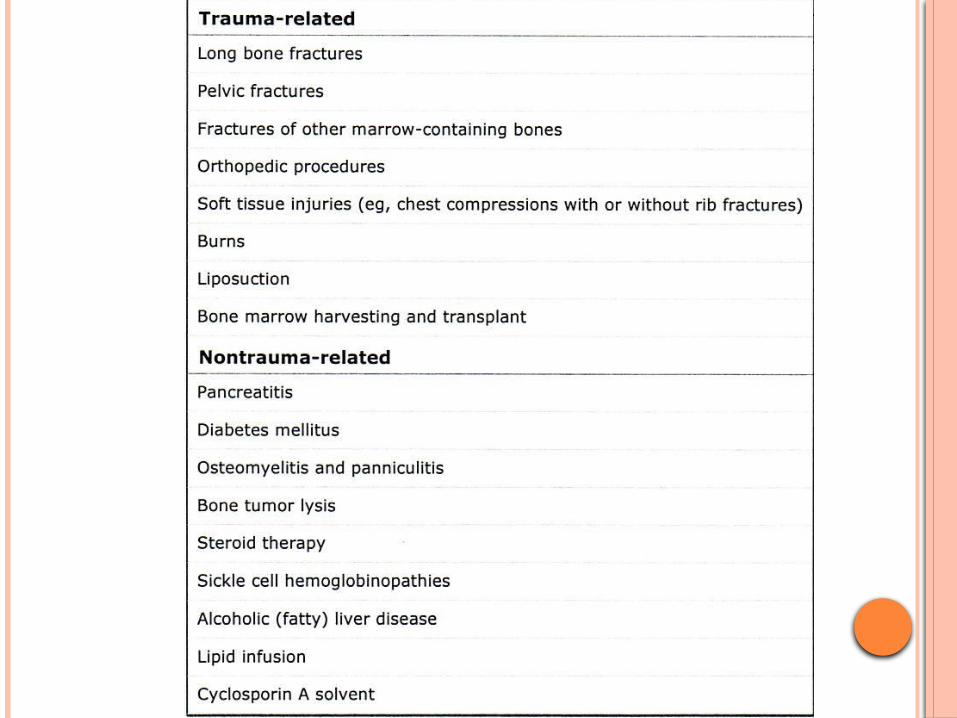
Non Trauma: agglutination of chylomicrons and VLDL by high levels of plasma CRP.
– disease-related• Diabetes, acute pancreatitis, burns, SLE, sickle cell crisis
– drug-related• parenteral lipid infusion
– procedure-related• Orthopedic surgery, liposuction

Pathophysiology Exact mechanism unknown, but two main
hypothesis
• Mechanical vs. Biochemical
• MECHANICAL – Fat globules from disrupted bone marrow or adipose tissue are forced into torn venules in areas of trauma.
• BIOCHEMICAL – Hormonal changes caused by trauma and/or sepsis induce systemic release of free fatty acids (FFA) as chylomicrons which cause the systemic FES.

MECHANICAL HYPOTHESIS-
– Fractures of marrow-containing bone (Femur,
Pelvis) have the highest incidence of FES and
cause the largest volume of fat emboli, because
the disrupted venules in the marrow remain
tethered open by their osseous attachments.
– The marrow contents enter the venous
circulation with little difficulty.
CONT..
This theory is supported by research on
Orthopaedic long bone (IM reaming) and
spinal surgeries which cause fat globules to
enter the blood circulation when vigorous
reaming/fixation is done.
Increased Pressure + Volume Extravasation
Measuring fat globules pre and post reaming
shows significant difference in concentration
CONT..
Fat droplets are deposited in the pulmonary
capillary beds and travel through arteriovenous
shunts to the brain. Systems affected include
LUNG, BRAIN and CIRCULATION.
Microvascular lodging of droplets produces local
ischemia and inflammation, with concomitant
release
of inflammatory mediators, platelet aggregation,
and vasoactive amines

BIOCHEMICAL :
FES is dependent upon degradation of the embolized fat
into free fatty acids.
Neutral fat does not cause an acute lung injury, it is
hydrolyzed over the course of hours to several products,
including FFA, which cause ARDS in animal models.
CRP (acute phase reactant), which is elevated in
trauma patients, appears to be responsible in lipid
agglutination (FES) for both traumatic and non-
traumatic FES.
CONT..
The process of Neutral fat cells -> FFA ->
Agglutination with CRP may explain the time
sequence of clinical findings in FES.
Onset of symptoms may coincide with
Agglutination.
This theory is animal model based and
circumstantial at best.

Diagnosis is made CLINICALLY NOT
CHEMICALLY. It does not matter how
much fat globules are in your circulation, it
just matters if you have their side effects.
FES typically manifests 24 to 72 hours after
the initial insult. Rarely <12 hrs or >72 hrs.
CLINICAL PRESENTATION-
TRIAD OF FES
Hypoxemia
Neurological abnormalities
Petechial rash
EARLY SIGNS
Dyspnea
Tachypnea
hypoxemia
PULMONARY:
Hypoxia, rales, pleural friction rub
Breath sounds: Loud harsh, Crepts & wheeze
ARDS may develop(fat emboli obstructs lung vessel
(20microns) platelets and fibrin adhere.)
½ of pts with FES require mechanical ventilation (Bulger,
Archives of Surgery 1997; 132: 435-9)
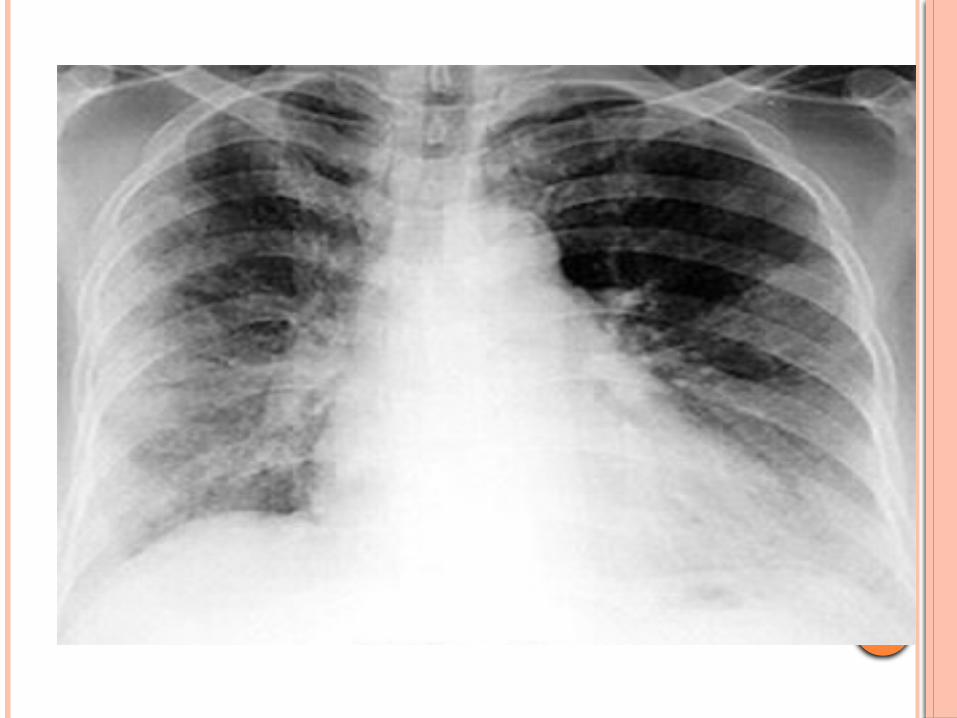
CXR usually normal early on, later may show
‘snowstorm’ pattern- diffuse bilateral infiltrates
CT chest: ground glass opacification with
interlobular septal thickening
NEUROLOGICAL FINDINGS:
Usually occur after respiratory symptoms.
Incidence 80% patients with FES
Minor global dysfunction most common, but ranges
from mild delirium to coma.
Seizures/focal deficits not common but can occur
Transient and reversible in most cases
CT Head: general edema, usually nonspecific
MRI brain: Low density on T1, and high intensity T2
signal, correlates to degree of impairment
RASH:
Petechial
Usually on conjuntiva , neck, axillae
Results from occlusion of dermal capillaries
by fat globules and then extravasations of
RBC
Fleeting & last short.Resolves in 5-7 days
PATHOGNOMONIC, but only present in 20-
50% of patients


OTHER FINDINGS
Retinopathy (exudates, cotton wool spots, hemorrhage)
Lipiduria
Fever (to 39-40ºC)
DIC
Myocardial depression (prominent S, T depression,
RBBB, arrythmia)
Thrombocytopenia/Anemia
Hypocalcemia
DIAGNOSIS
FES is CLINICAL diagnosis, not biochemical. A high degree of suspicion is needed to make diagnosis . -Common misconception that the presence of fat
globules, either in sputum, urine, or a wedged PA catheter, is necessary to confirm the diagnosis of FES
In 50% of fracture patients, fat globules was demonstrated in the serum, without symptoms of FES.
HOWEVER Growing literature on the use of bronchoscopy with
bronchoalveolar lavage to detect fat droplets in alveolar macrophages as a means to diagnose fat embolism. Sensitivity and specificity are unknown, being studied in Trauma patients
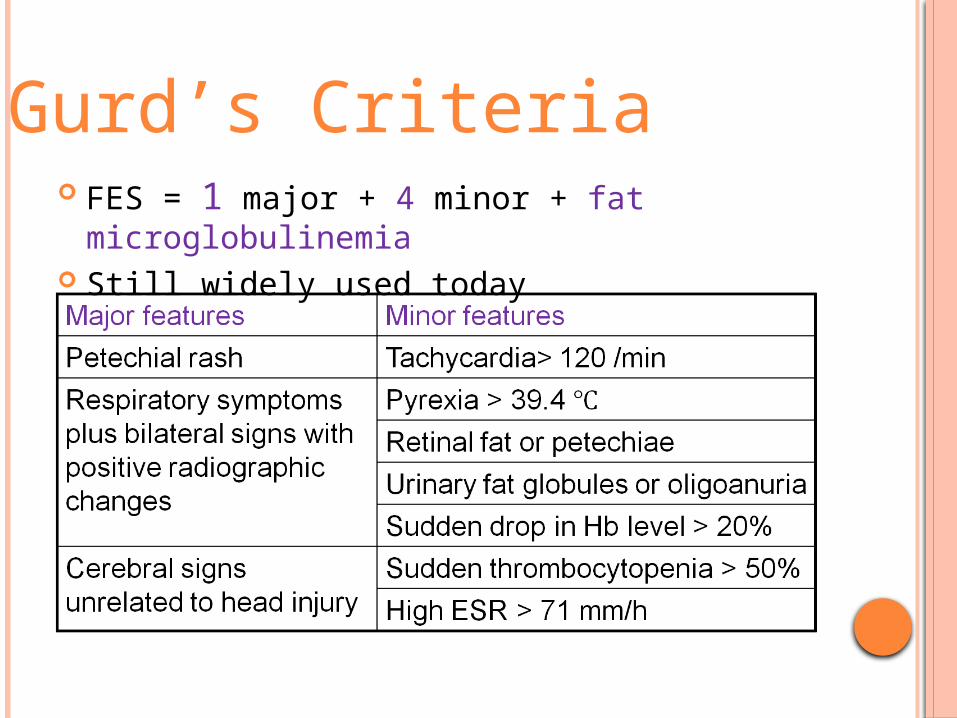
FES = 1 major + 4 minor + fat microglobulinemia
Still widely used today
Gurd’s Criteria
FES = femur fracture ± tibia fracture + 1 feature
Based on respiratory parameters
Lindeque’s Criteria
3 TYPES- In 1962
SUBCLINICAL FES
NON FULMINANT FES
FULMINANT FES
SEVITT’S CLASSIFICATION-

SUBCLINICAL FES:
Around 3 days post trauma
Probably occurs in almost all long bone
fractures of the lower extremity and
fractures of the pelvis
Characterised by decreased PaO2, decreased
Hb% and decreased platelets. No clinical
signs and symptoms of respiratory
insufficiency.
NONFULMINANT FES:
- Any time ,upto 6 days post trauma
-Clinical signs and symptoms are clearly evident.
Petechiae, tachycardia, respiratory failure, and signs
of CNS embolism.
Thrombocytopaenia, anaemia, and coagulation
abnormalities can be found, as can pulmonary
alveolar and interstitial opacities on chest x ray
There is no definitive test for this version of
the syndrome, as most of the changes
described can occur as a result of trauma as
well as a result of fat
embolism, the diagnosis remains a clinical
one, and the significance is uncertain

FULMINANT FES:
Occurs very suddenly and rapidly after injury,
and progresses very quickly, often resulting in
death within a few hours of the initial trauma.
Clinical features are acute respiratory failure, acute
cor pulmonale and embolic neurological changes.
These occur shortly after injury and often result in
the death of the patient.
Pats. with multiple fractures are particularly
susceptible to this form of the syndrome,
which, although it is relatively rare, is of
immense clinical significance because of its
high mortality.

MANAGEMENT
TREATMENT IS LARGELY SUPPORTIVE
Constant Positive Airway pressure(CPAP)
Mechanical Ventilation
Antibiotics
Nutritional support
Corticosteroids
Heparins
Have all been used
INITIAL TREATMENT
Adequate airway
Start IV line – correct fluid deficit
Basic investigation – including baseline chest X-ray
and ABG assay (v. imp).
Nasogastric tube – should be inserted in patient
with severe trauma and gastric contents suctioned
to prevent aspiration and ARDS
MONITORING
TPR, BP
I/O chart – maintain output 50-100cc/hr
CVP – to correct fluid deficit
If overload pulmn. Edema (4-8cm H2O)
Pulmonary haemodynamics– PCWP for accurate mean
of deficit correction (5-12mm of Hg)
Arterial blood gas monitoring
SPECIFIC DRUG THERAPY:
Many drugs have tried, most without demonstrable
benefit in established ARDS except Corticosteroids
but with some prophylactic benefit.
Drugs which may be tried in Fat embolism associated
ARDS are:
1.Ethanol : Lipase inhibitor, low incidence when level
>20mg.
2.Heparin : PL aggregation useful in DIC assoc ARDS
also.Controversial in trials.10000-15000 iu stat & 10000
iu 4-6hly with PTT at 1.5-2.5 INR.
3.Hypertonic glucose: block post traumatic
mobilization of FFA – may improve oxygenation.
4.Corticosteroids – stabilize cell member, PMN
adhesion, prevent surfactant reduction, protect
capillary endothelium, compliment activation and
minimize transudation.
CORTICOSTEROIDS –
ØValue in ARDS of Fat embolism, aspiration, sepsis,
shock and cerebral edema.
ØHelpful in late stage in recovering patients in
reducing fibrotic change.
ØImprove and preserve arterial oxygenation and
stimulate proliferation and maturation of Type II
pneumocyte.
CORTICOSTEROIDS -
Prophylactic dose 10mg/Kg Q8H
Or
80mg/kg bolus
Or
1-2gm IV over 24 hrs. & maintain for 48-96 hrs by
gradual reduction

ATLS Protocol :
1. Early immobilization of fracture and early
definitive reduction (open or closed).
2. Maintain intravascular volume to maintain
cardiovascular stability (hypovolemic shock
resuscitation), may use colloids (albumin) as it
can expand fluid and bind FFA.
3. Mechanical ventilation with PEEP
4. IV Ethanol has been used in Russia, Europe and some American centres to decrease rate of FES.
J Bone Joint Surg Am. 1977 Oct;59(7):878-80
“A raised level of alcohol in the blood was associated with a lower incidence of fat embolism” all other variables controlled.
- Other studies
- Can J Surg. 1970 Jan;13(1):41-9
- Br Med J. 1978 May 13;1(6122):1232-4
ROLE OF FRACTURE STABILIZATION
Highly debated issue
- Accumulated evidence over past decade support
early fixation within 24 hours of injury.

Early IF – decompress # hematoma as ongoing
source of fat emboli and retained necrotic debris,
eliminate pain and physiologic stress with continued
# motion, optimize pulmn function, contributes to
reduced ventilatory dependence and improve
survival.
But transient increasing pulmn Ar pressure and
worsening pulmn gas exchange observed during
reaming of medullary canal. So undreamed nailing
is suggested for femoral fixation in multiple #
patients.
PROGNOSIS
Mild -undetected
Mod -low mortality
Severe -fatal unless if treatement
instituted early. Survivors have pulmonary sequele.
