falling down on warfarin therapyc.ymcdn.com/.../rp_2-slides-falling_down_on_.pdffalling down on...
TRANSCRIPT

Falling Down on Warfarin Therapy
David Andrew Jacob, PharmD
Pharmacy Resident 2013 - 2014
Dayton VA Medical Center
Dayton, Ohio

Objectives • Describe CHADS2 score and the decision to
anticoagulate patients with AFib
• Describe role of HAS-BLED in risk stratification assessment for safety of anticoagulation
• Discuss physician providers view points on warfarin in high fall risk/elderly patients
• Summarize the evidence of risk of hemorrhagic stroke vs. ischemic stroke for high fall risk patients on warfarin
CHADS2 & CHA2DS2-VASc Score
Risk Stratification for AFib Patient’s Risk of Stroke/Embolism

CHA2DS2-VASc Almost same as above, plus…. Vascular Disease History +1 Age < 65 years old +0 | > 65 & < 75 y/o +1 | > 75 y/o +2 Sex Male +0 | Female +1
CHADS2 Score CHADS2 Congestive Heart Failure +1 Hypertension History (controlled or uncontrolled) +1 Age > 75 years old +1 Diabetes Mellitus +1 Stroke History +2
(Lip, 2010, 2011)

Real World Application CHADS2 Score
Stroke Risk % per Year
Score CHADS2 CHA2DS2-VASc
One 2.8% 1.3%
Two 4.0% 2.2%
Three 5.9% 3.2%
Four 8.5% 4.0%
Five 12.5% 6.7%
Six 18.2% 9.8%
Seven 9.6%
Eight 6.7%
Nine 15.2% 2013 CHEST guidelines recommend anticoagulation
with warfarin for patients with CHADS2 score ≥ 1 (Lip, 2010, 2011)

HAS-BLED Score
Risk Stratification for AFib Patient’s Risk of Major Bleed
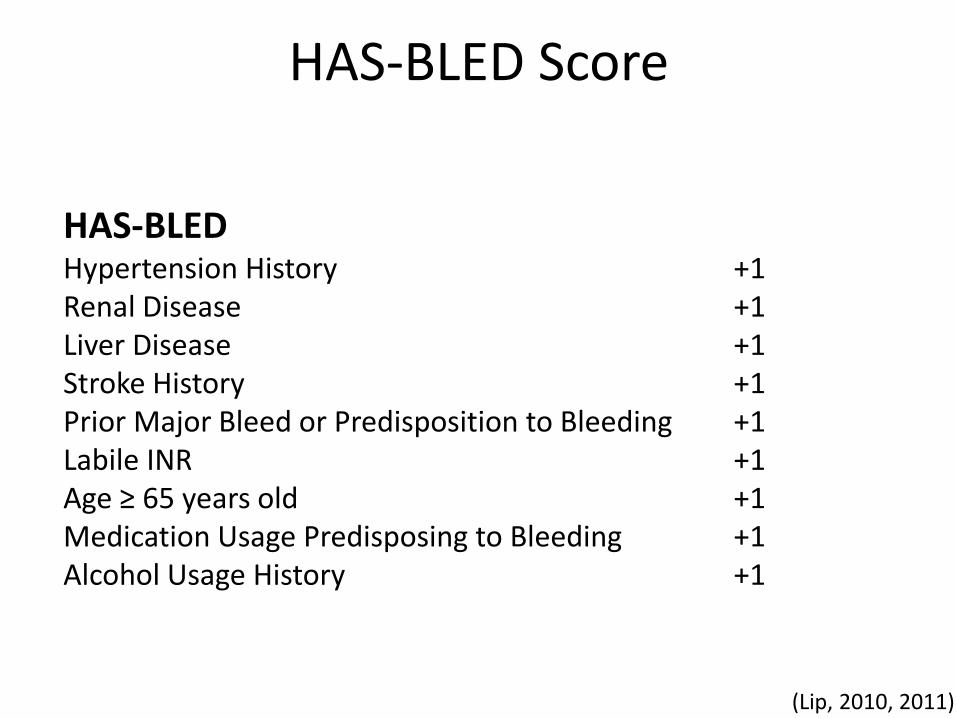
HAS-BLED Score
HAS-BLED Hypertension History +1 Renal Disease +1 Liver Disease +1 Stroke History +1 Prior Major Bleed or Predisposition to Bleeding +1 Labile INR +1 Age ≥ 65 years old +1 Medication Usage Predisposing to Bleeding +1 Alcohol Usage History +1
(Lip, 2010, 2011)

Real World Application HAS-BLED Score
Score HAS-BLED Risk
Zero 0.9%
One 3.4%
Two 4.1%
Three 5.8%
Four 8.9%
Five 9.1%
Six > 5 Too Rare to
Determine Risk
Seven
Eight
Nine
(Lip, 2010, 2011)

Factoring Fall Risk into Clinical Judgment
! ! ! Difficult ! ! !
What is the opinion of our colleagues?


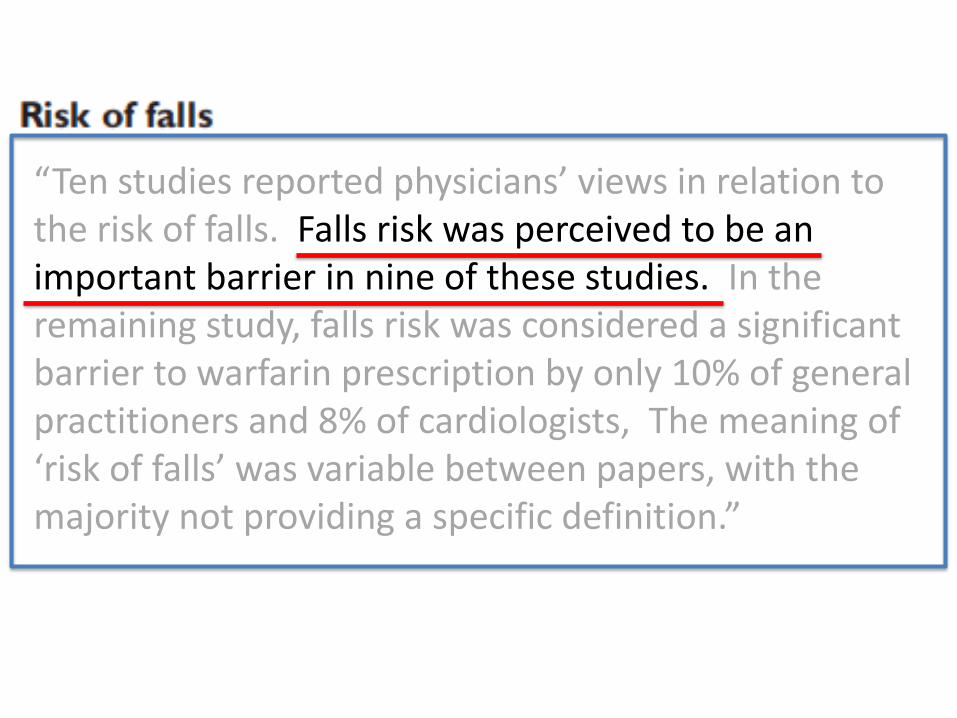
“Ten studies reported physicians’ views in relation to the risk of falls. Falls risk was perceived to be an important barrier in nine of these studies. In the remaining study, falls risk was considered a significant barrier to warfarin prescription by only 10% of general practitioners and 8% of cardiologists, The meaning of ‘risk of falls’ was variable between papers, with the majority not providing a specific definition.”


P I C O
P > 65 y/o, AFib, at risk for falling, but no other contraindications to antithrombotic therapy used to model outcomes
I Long-term warfarin use
C Long-term aspirin use No antithrombotic therapy
O Composite of possible outcomes (stroke, ICH, death) expressed in terms of QALYs
(Man-Son-Hing, 1999)

Methods
• Markov decision analytic model
• Systemic review of MEDLINE studies
– 190 relevant studies
• 49 met inclusion criteria
• Assumed event rates from meta-analyses of Atrial Fibrillation Investigators (2000 patient-years of f/u)
– Annual stroke risk 6%, RRR= 21% ASA, 68% warfarin
– SDH and ICH too few to get precise estimate for groups
• SHD rate in elderly = 0.0004 for every patient-year
– Rate of falls 33% of people, 1 fall within 1 year of f/u
(Man-Son-Hing, 1999)

(Man-Son-Hing, 1999)
(Garwood, 2008)
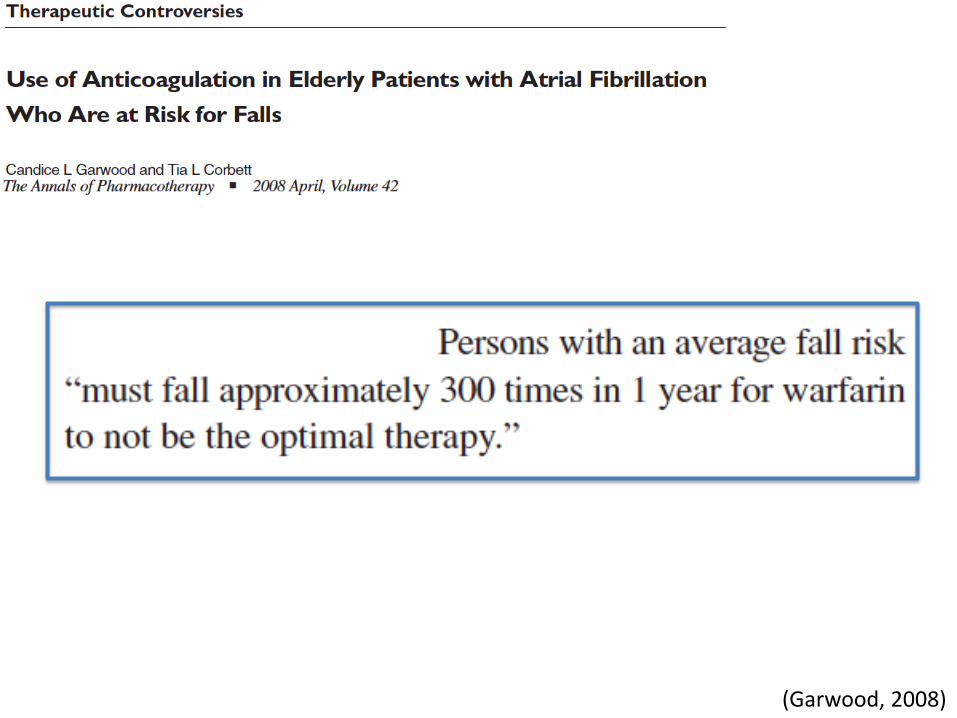
(Garwood, 2008)
Non-Model Data
Analysis of Real Patients


P I C O
P Medicare beneficiaries (x ̄= 80 y/o) w/ AFib. 48% of cohort on warfarin at hospital D/C.
I High Risk for falls (n=1245)
C Other patients with AFib (n=18,261)
O Subsequent hospitalization for ICH based on ICD-9 codes
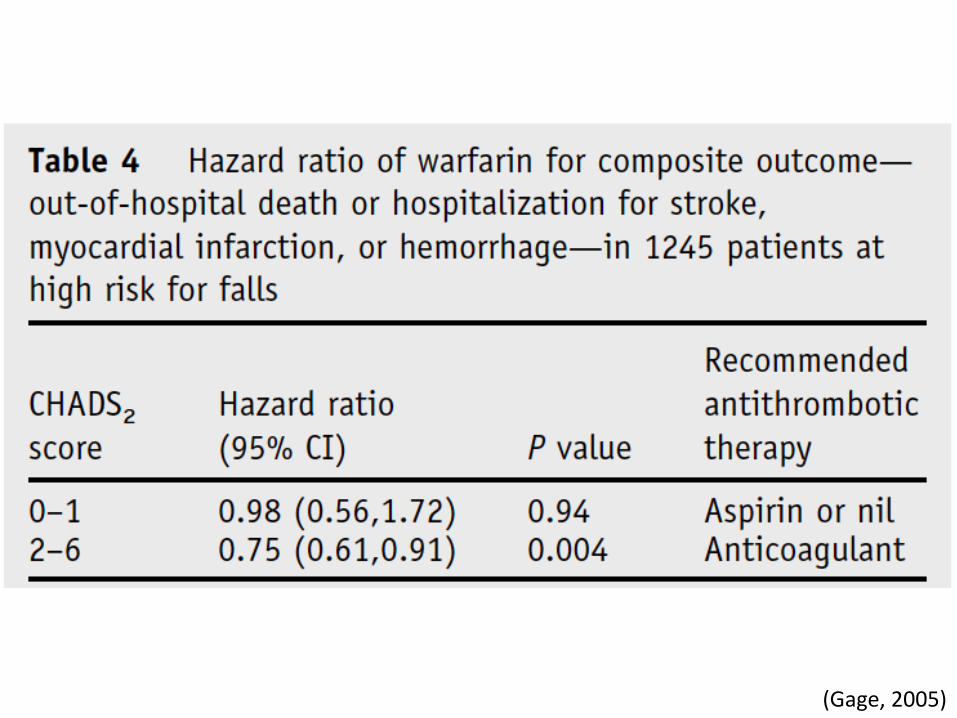
(Gage, 2005)

(Gage, 2005)

Warfarin Effect on ICH RISK
Hazard Ratio Confidence Interval
Warfarin 1.0 0.8 – 1.4
Aspirin 1.1 0.8 – 1.4
“Prescription of warfarin or aspirin at baseline did not significantly affect RISK of intracranial hemorrhage”
(Gage, 2005)
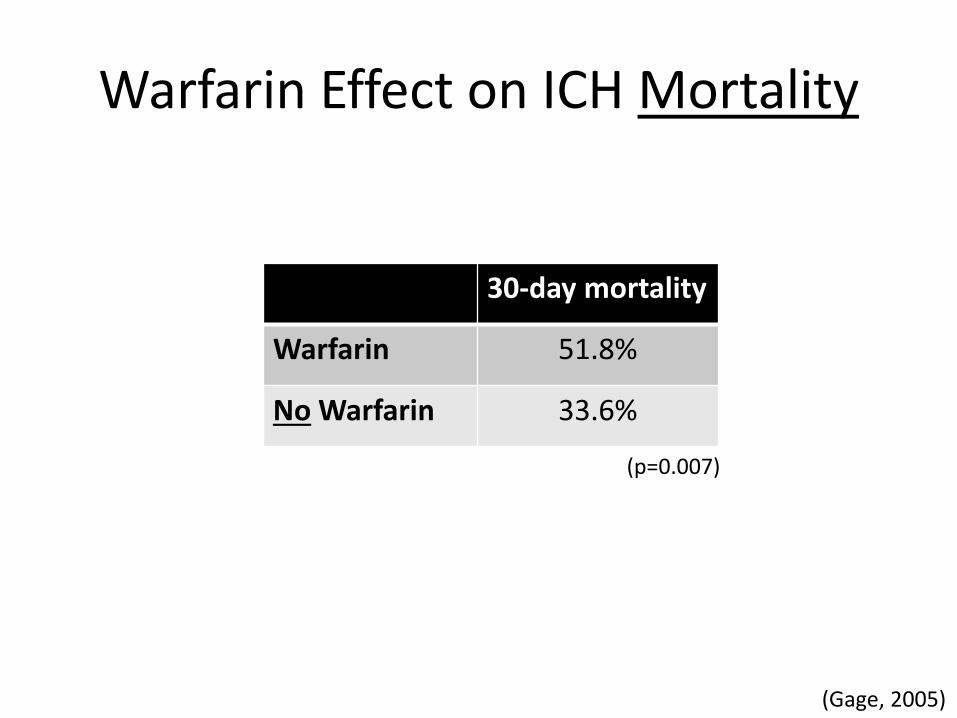
Warfarin Effect on ICH Mortality
30-day mortality
Warfarin 51.8%
No Warfarin 33.6%
(p=0.007)
(Gage, 2005)
(Gage, 2005)

How will this effect my practice?
Fall risk will not be the end all justification for holding anticoagulation
I will recommend consideration of other risk factors for ICH more to providers balancing clinical decision to continue anticoagulation.
Prior stroke, prior bleed, neuropsychiatric impairment (schizophrenia, dementia, & PD)

Reference Man-Son-Hing M. Choosing Antithrombotic Therapy for Elderly Patients
With Atrial Fibrillation Who Are at Risk for Falls. Arch Intern Med. 1999;159(7):677-685.
Garwood CL, Corbett TL. Use of anticoagulation in elderly patients with atrial fibrillation who are at risk for falls. Ann Pharmacother. 2008;42(4):523-32.
Gage BF, Birman-deych E, Kerzner R, Radford MJ, Nilasena DS, Rich MW. Incidence of intracranial hemorrhage in patients with atrial fibrillation who are prone to fall. Am J Med. 2005;118(6):612-7.
Lip GY, Frison L, Halperin JL, Lane DA. Comparative validation of a novel risk score for predicting bleeding risk in anticoagulated patients with atrial fibrillation: the HAS-BLED (Hypertension, Abnormal Renal/Liver Function, Stroke, Bleeding History or Predisposition, Labile INR, Elderly, Drugs/Alcohol Concomitantly) score. J Am Coll Cardiol. 2011;57(2):173-80.
Lip GY, Nieuwlaat R, Pisters R, Lane DA, Crijns HJ. Refining clinical risk stratification for predicting stroke and thromboembolism in atrial fibrillation using a novel risk factor-based approach: the euro heart survey on atrial fibrillation. Chest. 2010;137(2):263-72.