expand the responsibility - va minneapolis · to meet this objective, ... • interviews with...
TRANSCRIPT

1
6/10/16
This document is prepared by the Strategic Planning Committee in response to the charge given by the ACOS of Research Dr. Bloomfield “to develop a 5-year strategic plan to increase research productivity, collaboration and impact at the MVAHCS”. To meet this objective, the strategic planning committee performed:
• Environmental survey of the MVAHCS investigators and research staff • Focus groups held to gain a deeper understanding of the issues raised at the survey • Interviews with medical center leadership, including Mr. Patrick Kelly, Dr. Kent Crossley, Dr.
Kristin Nichol, Dr. Hanna Bloomfield and Dr. Michael Levitt • MVAHCS Bibliometric analysis • Analysis of MVAHCS Research expenditures • Analysis of MVAHCS Funding sources • Analysis of MVAHCS Vital statistics
All of these data, included as an appendix to this document, were reviewed and analyzed in a series of meetings and a two-day retreat. This report is not meant to be a comprehensive list of all challenges or successes in research at MVAHCS, although most of these were discussed at our meetings, but rather an effort to distill the information to few critically important and feasible interventions. The overarching theme in these recommendations is to expand the responsibility of the Research Office.
We are grateful for the support that we received from MVAHCS investigators, medical center leadership and Research Office staff including Julia Christensen, Mallory Lorge and Margaret Bordanea.
We also wish to acknowledge “Good Strategy Bad Strategy,” by Richard Rumelt, and a document cited therein, “Long-Term Competition with the Soviets: A Framework for Strategic Analysis,” by A.W. Marshall, as resources for principles of strategic planning. The Marshall document was used as a template for this strategic plan.
Selcuk Adabag, MD, MS (co-chair) Kristin Chrouser, MD, MPH Philip Dahm, MD (guest member) Apostolos Georgopoulos, PhD Andrew Hansen, PhD Shannon Kehle-Forbes, PhD Mark Klein, MD Kelvin Lim, MD, PhD Tom Rector, PhD (guest member) Yoav Segal, MD, PhD (co-chair) Christine Wendt, MD

2
I. INTRODUCTION
A. The primary objective of this Strategic Plan is to conceive and initiate a new organizational paradigm that will propel the Minneapolis VA Health Care System (MVAHCS) to the forefront of research and development.
B. The Strategic Plan is based on the following understanding: To engender continued support, a VA research program needs to focus on helping the Veterans Health Administration (VHA) achieve its aims. First and foremost, the mission of the VHA and the MVAHCS is to attend to veterans’ health care needs. Research-related aims in the most recent national VA Blueprint for Excellence are “to lead the nation in research and treatment of military service-related conditions, and to conduct research to improve VA health care services and outcomes.”
C. An environmental survey of MVAHCS principal investigators, research staff and leadership found the following, including some challenges:
1. The MVAHCS, a 5-star healthcare facility, employs a cadre of excellent health care providers who have a variety of research interests and expertise. Research is very important to their recruitment and job satisfaction. However, at the current time, most VA health care providers are not hired or evaluated as independent investigators.
2. As VA employees, many researchers struggle to find the time required to develop and maintain cutting-edge skills, knowledge, and interpersonal relationships necessary for a successful research program.
3. The research workforce at the MVAHCS is getting older. We do not attract young, gifted and dynamic investigators on a consistent basis. There are also policy obstacles to hiring foreign nationals.
4. MVAHCS researchers lose hope as they progress from junior to mid-career.
5. While continuing to publish articles, MVAHCS researchers are not applying for funding. Indeed, with $26 million in annual research spending in 2014, MVAHCS ranks 16th in funding nationally among VA medical centers. When asked about the reasons for not submitting grants, MVAHCS researchers cited:
! Insufficient support for grant development, writing and submission
! Insufficient dedicated time for research due to increased clinical and administrative duties
! Regulatory obstacles
D. While the Research Office and the ACOS of Research exercise research duties, which are mostly regulatory, no person or office at the MVAHCS has the overall responsibility for increasing research productivity or advocating for investigators. Furthermore, research productivity is not a consistent factor in the evaluation of service line and section chiefs, and medical center leadership. Such circumstances contribute to a perception that research productivity, while important to the institution, is a secondary priority.

3
E. A full discussion of research productivity at the MVAHCS would, by necessity, address a range of issues. For example, the shrinking recruitment pool for clinician-investigators is not easily separated from prospects for MVAHCS research productivity. Nevertheless, the Strategic Planning Committee felt it appropriate initially to address the roles of the Research Office, because:
1. Within the MVACHS, the Research Office is the entity most closely identified with research.
2. The Research Office already has recognized roles in research administration (accounting, reporting, compliance, etc.).
3. The Research Office has a dedicated and deployable staff.
4. The Research Office can engage MVAHCS investigators to formulate and implement research planning in the short (1-year) and medium (3- to 5-year) terms, and also transcend those terms, to capitalize on institutional strengths and respond to ever-changing externalities including new areas of opportunity. Thus, the Research Office can be a more effective instrument for promoting MVAHCS research.
F. This Strategic Plan examines expansion of the responsibilities of the Research Office in the following areas:
– To improve research productivity
– To coordinate institutional research strategy and planning formally and on an ongoing basis
– To emphasize service and advocacy for investigators
– To create processes for identifying and focusing on areas of MVAHCS competitive advantage
– To create a Research Advisory Panel, to advise the ACOS for Research and share responsibility for advancing the research program consistent with goals of the VHA
II. EXPAND THE RESPONSIBILITY OF THE RESEARCH OFFICE TO INCLUDE RESEARCH PRODUCTIVITY
A. The current roles of the Research Office and ACOS of Research are seen primarily as administrative and include:
! Managing research conduct
! Oversight of regulatory committees such as the Institutional Review Board
! Managing intramural and extramural grant processes for VA employees
! Allocating and managing research space

4
! Promotion of research, e.g. Research Day
! Serving as a resource for guidance and troubleshooting
Lacking in the current framework is a directive to create an environment that will allow MVAHCS researchers to move to the forefront of research.
B. To move to the forefront of research, the MVAHCS will need to increase research productivity. Such productivity is measurable by funding and high-impact publications but other definitions can also be considered. In the current external environment of rapid change, competition for resources, emphasis on team-based research, and societal and agency expectations of research relevance, determinants of institutional research productivity require careful attention, deliberate thinking and coordinated action. Under the leadership of the ACOS for Research, the Research Office can and should assume such a primary emphasis. This shift in emphasis, in effect expanding the roles and responsibilities of the Research Office, is the single abiding theme of the Strategic Plan, meant to set in motion a cascade of favorable outcomes for research productivity.
C. The ACOS for Research and Research Office are accountable to MVAHCS leadership and the Office of Research and Development. At the same time, the ACOS for Research and Research Office are afforded resources, implementation instruments, and mechanisms for determining local policies, procedures and practices consistent with the VHA research mission. Recognizing these parameters, we propose a shift in emphasis whereby the Research Office takes on primary responsibility for research productivity, and engages in formal, ongoing and collaborative strategic planning towards this end. To improve research productivity, such a shift in emphasis will need to be communicated skillfully to the MVAHCS investigator workforce.
D. To increase research productivity, Research Office will need to create a research infrastructure for MVAHCS investigators. CCDOR is a successful example where such an infrastructure and has previously been created. The elements of the infrastructure include but are not limited to:
! Statistical and methodological support
! Support for grant writing and submission
! Programmer services to access nationwide VA data
III. THE RESEARCH OFFICE SHOULD COORDINATE RESEARCH STRATEGY AND PLANNING FORMALLY AND ON AN ONGOING BASIS
A. Emphasis on strategy and planning reinforces processes that are already in place in the Research Office and prompts new questions. Characteristics of such an emphasis include:
– Framing short-, medium- and long-term planning goals consistent with the goals of the VHA

5
– Engaging MVAHCS investigators as formal advisory partners in ongoing strategic planning
– Examining the MVAHCS investigator workforce such as it is, working closely with service line and section chiefs to:
! Recognize and support productive investigators to ensure that they have adequate protected time
! Initiate and oversee recruitments to areas of research strength
o Provide recruitment packages and adequate protected time for promising new recruits
! Match investigators and teams of investigators to emerging funding opportunities
! Facilitate team building with special attention to mentorship for junior investigators
! Counsel struggling investigators especially during times of transition by providing bridge funding
! Plan for succession in areas of aging leadership
! Attend to non-clinician investigators who are brought into full-time positions at the MVAHCS and face competition for VA eligibility from University-based, part-time VA investigators at other institutions
– Defining, on an ongoing basis:
! Areas in which the MVAHCS has accumulated competencies that can serve as the basis for unambiguous, long-term competitive advantage
! Areas in which the MVAHCS must operate to serve the VHA mission, for example spinal cord injury
! Areas in which the MVAHCS should withdraw, for reasons of institutional focus, resource limitations or competitive disadvantage
– Integrating data and judgment to shape a focused, rational and forward-looking research portfolio that serves the VHA mission and is true to the people, priorities and culture of the MVAHCS
B. If carried out effectively, a formal and ongoing strategic planning process will, in the short term, identify one or two achievable objectives that will build momentum for future improvements. Formalization of the strategic planning process itself can and should be the first such objective. Our environmental survey and Strategic Planning Committee deliberations identified several additional areas in which the Research Office could formulate short-term objectives. These include but are not limited to:
! Increasing and improving grant submission support

6
! Strengthening core facilities and services that support essential research areas
! Identifying and mitigating undue regulatory policies and practices that discourage or limit research
! Promoting the success of junior investigators by means including mentorship and milestone planning
C. While unlikely to yield proximate objectives, the relationship between the MVAHCS and the University of Minnesota was identified as an area with important bearing on long-term research productivity, especially as relates to preserving feasibility of NIH funding, as such warranting a part in ongoing strategic planning. Specific issues that were raised included:
! Long-time administrative obstacles to shared University positions for MVAHCS investigators and other key personnel
! Cumbersome contracting processes
! Handling of University of Minnesota indirect costs on research grants to primary MVAHCS investigators
D. While outside the scope of the Strategic Plan, it was noted in our environmental survey and Strategic Planning Committee deliberations that processes determining priorities and policies for VA research at the national level are opaque to most investigators. In principle, a top-tier VA research program would include key investigators who exercise advisory roles at the national level and disseminate practical information accordingly. Working with the ACOS for Research, such individuals could further serve to move the MVAHCS research program, in aggregate, away from predominantly reactive stances towards change.
E. If adopted as a primary recommendation of this Strategic Plan, then the shift in emphasis for the Research Office is expected to affect Research Office personnel, starting with the ACOS for Research. Preliminary ideas for a Research Advisory Panel, to advise the ACOS for Research and share responsibility for strategy and planning, are provided in a forthcoming section. To further free the ACOS for Research to focus on strategy and planning, other changes, subject to approval, may be required, for example entrusting additional administrative oversight responsibilities to the Deputy ACOS for Research.
IV. MODIFIED ROLES FOR THE RESEARCH OFFICE THAT EMPHASIZE SERVICE AND ADVOCACY FOR INVESTIGATORS
A. As a greater emphasis is placed on research productivity, it will become increasingly important to prioritize the morale of investigators and empower investigators to reach new productivity benchmarks.
B. Our environmental survey suggested relatively high levels of investigator satisfaction and found that investigators are motivated to increase their productivity: The majority of investigators surveyed reported a strong desire to serve as Principal Investigator on a funded project.

7
However, a decrease in satisfaction moving from junior to mid-career investigators was noted and the high level of seemingly top-down administrative barriers caused frustration, which in some cases deterred investigators from preparing grant applications.
C. We propose giving investigators a greater voice in policy and planning. One way to achieve this goal is to develop a standing Research Advisory Panel, with representation, service and advocacy as well as advisory responsibilities. Such a panel, described below, would work in concert with the ACOS for Research to facilitate and improve the research environment and productivity.
D. In one of several possible implementations, the Research Advisory Panel would be elected, in part or in whole, from the community of MVAHCS investigators, accounting for diversity in research interests, clinical responsibilities, career stage, gender etc. Topics on which the advisory panel could provide input include:
! Expectations regarding research productivity
! Impact of existing and proposed policies and procedures on investigator satisfaction and productivity
! Creation and allocation of resources, e.g. pilot funding, methodological support, access to programmers to examine national VA data, administrative support for grant preparation and submission, etc.
! Recruitment of new investigators
! Incentives and rewards for research productivity, to include nominating processes for local and national awards and other forms of recognition.
E. As a further affirmation of institutional commitment to investigators, we also propose creating a greater sense of community, facilitated by the Research Office. While investigators as a whole were satisfied with their current collaborations, forums in which they could receive feedback on ideas, grants, or papers, problem-solve barriers to conducting research, and develop camaraderie with other investigators may improve satisfaction and productivity. Specific strategies for meeting these goals may include:
! Brown bag series where researchers present ideas in preliminary stages of development
• Research methods conference series
! Research conferences that accommodate surgeons and others with scheduling constraints
! Mechanisms for grant and paper review
! A lounge for investigators to work, meet and lunch with others
F. In light of findings in the environmental survey, the Research Office should play a greater role in fostering the success of junior investigators and their transition to mid-career. We anticipate that the research community described above would help to improve the environment for junior investigators. We also propose that the Research Office play roles in the following:

8
! Mentoring plans and mentoring committees for junior investigators
! Negotiated agreements for dedicated research time
! Formal orientation on VA research processes including grant submissions, academic resources, and start-up opportunities specific but not limited to junior investigators including MVMREF grants
V. PROCESSES FOR IDENTIFYING AND FOCUSING ON AREAS OF MVAHCS COMPETITIVE ADVANTAGE
A. To improve the environment for research productivity, leaders at the MVAHCS will need to make strategic choices in deployment of resources, initiative, energy and influence. Such choices should be informed by honest assessments of research strengths that offer prospects for long-term institutional competitive advantage, as determined by relevance to veterans and the VHA research mission, impact and innovation, publications and funding, and recognition and prestige.
B. Institutional research strength emanates from many sources, extending beyond research areas and methodologies to include people, culture and infrastructure. Many high-profile success stories in MVAHCS research cross areas but share a common theme: Contributing best-available evidence to answer fundamental clinical questions, in COPD, aortic aneurysm, colon cancer screening, prostate cancer, flu vaccination, and other areas. Such contributions are rooted in the VHA mission, serving veterans and the general population, but also reflect the people, priorities and culture of the MVAHCS that together constitute its major strength.
C. Developing processes for identifying and focusing on areas of MVAHCS competitive advantage will require careful and concerted effort. The ACOS for Research can be joined in these efforts by the Research Advisory Panel, representing a diversity of interests, talents and skills.
D. Insofar as people are the key to building and sustaining research strength, one set of strategic goals is to identify areas that will be targeted for recruitment and retention of principal investigators and other key personnel. These will include, but not be limited to, recruitment and retention packages, protected time and other incentives for investigators at all career stages, and reducing the barriers for hiring promising investigators of foreign national background. A Research Advisory Panel can advise and collaborate in these efforts.
E. An analysis of current research strengths at the MVAHCS identified the following:
1. Historically, investigators and teams of investigators have demonstrated research productivity, as measured by publications in high-impact journals, funding from NIH, VA, DOD, and other agencies, and discoveries that are clinically relevant or important within specialized fields. These investigators have worked in diverse areas of basic, clinical and health services research. Their primary affiliations have included the Research Service itself (chiefly, basic scientists), clinical service lines, and centers such as Brain Sciences, GRECC and CCDOR.

9
2. Centers such as Brain Sciences, CCDOR and GRECC offer stable infrastructure and other advantages. CCDOR has been funded continuously since 1998 and centralizes operations within the center; for example, statistical and programmer support is provided within the center and not dependent on the Research Office. The basic research laboratories illustrate advantages of centralization outside the center model, including shared equipment and a well-run animal facility. A core group of basic science researchers have steadily maintained requests for core equipment that can be used broadly by many investigators.
3. Funding to the MVAHCS has been relatively stable, with most coming from VA and NIH. Other sources include DOD, foundation grants, and industry trials.
4. CCDOR and Basic Research have been the two most highly funded research entities within the MVAHCS. During the past 4 years, funding to Basic Research has declined significantly, but still accounts for over $6 million annually. In other areas, funding totals can still be influenced significantly – on an absolute or percentage basis – by gain or loss of a single major grant.
5. A preliminary analysis of MVAHCS area strengths positioned for long-term competitive advantage identified CCDOR, GRECC and the Pulmonary Section of the Primary Service Line. By application of the above mentioned principles, these and similarly identified areas of research strength should receive continued institutional support.
F. Notwithstanding pockets of success, the Primary Service Line subspecialties and Specialty Service Line appear to have low publication and funding success on a per capita basis. In part, this is because many VA providers are not hired as investigators. Nevertheless, maintaining research competitiveness within the clinical service lines is clearly one of the major challenges that will need to be addressed in ongoing strategic planning led by the Research Office. We identified several related points:
1. With exceptions, for example the Pulmonary and Infectious Diseases Sections of the Primary Service Line, most clinical sections do not appear to develop research themes or plan accordingly, creating voids in potential areas of research productivity.
2. Clinical demands on MVAHCS clinician-investigators are increasing significantly, in ways that are measured, for example patient enrollment, but also otherwise, relating to non face-to-face care (coordination of care, results reporting, secure messaging, etc.), medical complexity, clinic access requirements, etc. Added and unforeseen clinical demands are a challenge to research productivity, as such warranting attention from service line directors and section chiefs, working with the Research Office.
3. Although our environmental survey did not query the matter directly, there is evidence to suggest that some MVAHCS clinical investigators stop applying for grants, further suggesting that competitiveness for research funding, once lost, is not easily recovered.
4. There are unexploited opportunities to engage clinical providers and non-clinical investigators, such as MD-PhD teams, in new collaborations that are relevant to veterans. Indeed, successful models of such collaborations at the MVAHCS already exist, and several Ph.D. investigators expressed desire to collaborate in such a manner.

10
5. At present, the return on investment for actively facilitating or incentivizing new collaborations cannot be known, but could be explored as part of ongoing strategic planning. If deemed worthwhile, then pilot programs or other mechanisms for promoting team-based, multidisciplinary research may be achievable using MVMREF or VERA funds. Alternatively, a portion of institutional support for centers (Brain Sciences, CCDOR, GRECC) could be set aside for collaborations with center-unaffiliated investigators. There are likely relevant precedents for such or similar arrangements at the MVAHCS.
G. As a routine matter, maintaining research competitiveness requires knowledge of funding opportunities. The Research Office disseminates funding announcements but no one at the MVAHCS appears to research and appraise funding opportunities strategically, from a community-wide perspective. Where realistic, we recommend team building around funding opportunities, looking not just at the VA or NIH but DOD (Team Science Awards), foundations, and industry. The DOD allocates several hundred million dollars to biomedical research annually, likely representing new opportunities for MVAHCS research.
VI. IDEAS FOR A RESEARCH ADVISORY PANEL, TO ADVISE THE ACOS FOR RESEARCH AND SHARE RESPONSIBILITY FOR ADVANCING THE RESEARCH PROGRAM CONSISTENT WITH THE GOALS OF THE VHA
A. We recommend that the ACOS for Research and Research Office assume primary roles in institutional research strategy and planning, with attendant responsibilities for improving the research environment and research productivity. To do so, the Research Office will need to augment its high-quality leadership structure, setting the right tone for the entire MVAHCS research program. New and formal advisory relationships will be required, with investigators who bring knowledge, insight and community-mindedness to the effort.
B. In one possible implementation, we propose a Research Advisory Panel, alternatively a Council, Cabinet, Board or Working Group. Such a body would share responsibility for institutional research productivity with the Research Office and facilitate communication and coordination with MVAHCS investigators:
Others not depicted but clearly figuring into such a scheme include medical center leaders, Research Office personnel, the clinical service lines, regulatory and other administrative committees, MVMREF, non-investigator research staff including study coordinators, technicians, etc., veterans themselves, and others. If accepted as a primary recommendation
ACOS for Research
Research Advisory Panel
Investigators

11
of this Strategic Plan, then the creation and governance of such a Research Advisory Panel would probably, as a first step, need to be chartered.
D. The Research Advisory Panel could number at least 9 members, some appointed and some elected. MVAHCS investigators are expected to constitute the membership, representing a diversity of research interests, service line and center affiliations, career stages, gender and so on. Representatives of medical center leadership, MVMREF, veterans themselves, or others, could also be considered as regular members or, perhaps more appropriately, special liaisons, participating only when their presence is essential. Service on the Research Advisory Panel would entail significant commitment, for example one day per week on average, recognized commensurately in effort mapping.
E. To effect a new organizational paradigm that will propel the MVAHCS to the forefront of research and development, the Research Advisory Panel would need to meet regularly, on a weekly or bi-monthly basis, establishing a productive meeting culture that benefits from continuity in working relationships, planning and follow-up. Meeting minutes will serve as a record of progress, for the panel itself and the broader community.
F. The Research Advisory Panel would take on roles in support of the ACOS for Research and Research Office that are not currently served by the Research and Development Committee, or other leadership or administrative committees at the MVAHCS. Indeed, the Research Advisory Panel could be seen as a vehicle for strengthening collaboration and communication with some or all of these other committees.
G. The Research Advisory Panel would be expected to operate in three highly interrelated domains:
– Awareness, Knowledge and Understanding
! Maintaining a working knowledge of individual investigators comprising the MVAHCS workforce, including background and expertise, publications and funding, service line, center and team affiliations, priorities and work style preferences, and capacity for new research initiatives
! Maintaining knowledge of the MVAHCS research portfolio
! Researching and appraising Program Announcements, Requests for Applications and other funding opportunities, for relevance to the VHA mission and areas of MVAHCS research strength, also recruiting investigators and teams of investigators to such opportunities
! Reviewing secular trends in the external research environment, especially VA and NIH, for their bearing on the MVAHCS research program in the short, medium and long terms
! Remaining apprised of trends and developments in research subject protection, especially those that advance the purpose while reducing the burden of research regulation

12
! Cultivating “insider” knowledge in the areas above, for purposes of practical guidance and productive planning
– Ongoing Strategy and Planning
! Maintaining an adaptable inventory of strategy and planning goals for the short (1-year), medium (3- to 5-year) and long terms, weighted by priority and pursued accordingly
a. Short-term planning goals are, by definition, highly specific and achievable. Examples include: Within one year, to: i) host, at separate meetings of the Research Advisory Panel, six unfunded investigators for discussion of a page of Specific Aims, providing feedback and planning services; ii) conduct “user experience assessments,” shadowing three investigators through the grant submission process, and identifying three new ways in which the Research Office can enhance support and, by extrapolation, the number of MVAHCS grant submissions; and iii) support placement of two additional investigators on NIH or VA Study Sections.
b. Medium-term strategic goals relate to the research portfolio, programmatic directions and infrastructural changes that serve areas of existing and emerging strength. Examples include: To: i) submit, with an MVAHCS principal investigator and MVAHCS and University of Minnesota co-investigators, an institutional NIH training grant application with translational relevance to PTSD and related brain disorders affecting veterans; ii) recruit, in support of the Endocrinology section, a junior clinical investigator, for rigorous development as a site and then lead investigator in multi-center obesity and diabetes trials; and iii) implement a partial sabbatical system for appropriately selected clinical investigators, to be used for submitting grants, acquiring research credentials, or other approved purposes.
c. Long-term strategic goals relate to big questions. Examples include: i) What is the future of basic research at the MVAHCS, and its implications for people, laboratory research space and support services such as the animal facility?; ii) Can the MVAHCS expect to sustain its investigator workforce under current recruitment practices?; and iii) Will the MVAHCS research program be poised to compete in emerging areas of veterans’ health needs?
d. The Strategic Planning Committee concluded that an accountable process for formal and ongoing strategic planning, representing a new paradigm for reasons as outlined, is more important for MVAHCS research productivity than analysis at a single point in time. Such a general-purpose approach is tantamount to a system for generating, evaluating and acting on strategic alternatives, that applies principles such as the VHA mission, and fidelity to the people, priorities and culture of the MVAHCS.

13
– Service and Advocacy for Investigators
! Guaranteeing high-quality lines of communication bidirectionally, from the ACOS for Research to investigators (top-down) and from investigators to the ACOS for Research (bottom-up), perhaps utilizing new formats such as town hall meetings, also identifying and phasing out ineffective lines of communication
! Providing constituent services for investigators and teams of investigators including case and cause advocacy, for example, for methodological support
! Identifying high-quality system elements that facilitate MVAHCS research (policies, procedures, offices, services, etc.) and, conversely, bottlenecks that impede research, for collaborative efforts at quality improvement
! Jointly setting expectations regarding research productivity, allowing for variations by service line and other factors, and negotiating dedicated research time accordingly
! Assessing impact of existing and proposed policies and procedures on investigator satisfaction and productivity
! Routinely approaching MVAHCS investigators and teams of investigators to test for interest in new research opportunities
VII. BARRIERS TO IMPLEMENTATION OF THE STRATEGIC PLAN
A. An environmental survey identified barriers to research productivity at the MVAHCS. Such is not the topic here, rather barriers to the major recommendation in this Strategic Plan, namely that the Research Office take on the major role of improving the research environment and increase research productivity at the MVAHCS, by a formal and ongoing process of strategic planning, using a panel of investigator-advisors, with deliberations to be recorded.
B. The recommendations set forth in the Strategic Plan describe a new paradigm that, in fact, invokes old principles of research leadership, those of generating and implementing institutional research vision, but for a more challenging era. Indeed, this paradigm represents a shift and not wholesale change for the Research Office. Nevertheless, there are potential barriers to be negotiated, including:
! Countermanding language in the current versions of VA policy and procedure documents
! Need for wider VA approval
! Adjustments in roles and responsibilities for Research Office personnel, with acceptance thereof
! Other sources of institutional inertia and/or competing agendas

14
! Strategic communications to introduce and sustain change, especially if there are early failures
C. The most significant barrier to successful implementation of the Strategic Plan may relate to the Research Advisory Panel or other mechanism(s) for formal and ongoing strategic planning. For the case of the Research Advisory Panel: The panel will need to operate at a high level, set up to do so in the all of the usual ways, including appointment/election of appropriate individuals, clear delineation of duties and responsibilities, productive meeting culture, strong emphasis on follow-up, accurate minutes, and so on. A mechanism that operates ineffectively could have significant negative consequences.
VIII. CONCLUSIONS
The MVAHCS is recognized as a 5-star facility for clinical care, however, our ranking in research (16th) lags behind other VA facilities. Matching our research ranking with our success in clinical care requires a paradigm shift making research productivity a priority and a formal criterion for evaluation of individuals, sections and departments. The initial, most important intervention to propel MVAHCS to the forefront of research is to expand the responsibility of the Research Office to include improving research productivity; coordinating institutional research strategy and planning on an ongoing basis; emphasizing service and advocacy for investigators; creating processes for identifying and focusing on areas of MVAHCS competitive advantage and creating a Research Advisory Panel, to advise the ACOS for Research and share responsibility for advancing the research program. These interventions and processes, outlined in more detail in this document, are designed to create a new organizational paradigm that will propel the MVAHCS to the forefront of research and development.

VA Research Strategic Plan Appendix Table of Contents
Meeting Minutes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2 Survey Responses . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15 Gap Analysis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 50 Focus Group Transcripts . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 51 Interview Transcripts . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 60 Supplementary Data . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .73
Bibliometric Analysis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 74 RDIS Expenditures, by Research Unit . . . . . . . . . . . . . . . . . . . . . . . 75 Minneapolis VA Funding Sources, 2014 . . . . . . . . . . . . . . . . . . . . . . 76 Minneapolis VA Vital Statistics, 2014 . . . . . . . . . . . . . . . . . . . . . . . . 77
- 1 -

Meeting Minutes
- 2 -

Strategic Planning Committee Charge Minneapolis VAHCS Research Service 2015
PURPOSE
x To develop a 5 year strategic plan to increase research productivity, collaboration, and impact.
PROCESS (to be determined by committee)
x Environmental scan x Solicit input form board group x Identify key questions, issues, choices x Hold a strategic planning retreat with key stakeholders to develop a draft plan x Solicit board feedback on draft plan x Finalize written strategic plan x Develop an implementation plan
DELIVERABLES
x 5 year Strategic Plan with 3-5 major goals, each with 2-3 specific objectives and associated metrics
x Implementation Plan that specifies timelines, owners and workgroups for each goal PROGRESS UPDATES to ACOS
x Monthly TIMELINE
x Target Due Date: September 30, 2015
- 3 -

Strategic Planning Committee Meeting – April 13, 2015
Meeting called to order at 3:00pm by Hanna Bloomfield Present: Hanna Bloomfield (Introductions only), Yoav Segal, Selcuk Adabag, Mark Klein, Apostolos Georgopoulos, Andrew Hansen, Kelvin Lim, Chris Wendt, Shannon Kehle-Forbes, Kristin Chrouser, Mallory Lorge (Administrative) Absent: (none) Introduction from Dr. Bloomfield x Purpose: To develop a 5-year Strategic Plan to increase research productivity, collaboration,
and impact. Measures of productivity include grant funding and the number and impact of publications. It is time for a broader vision: How can we grow research at MVAHCS?
x The Committee is composed of a diverse group. x Process: As suggested in the handout, steps can include an environmental scan, solicitation
of input from broad groups, identification of key questions, a strategic planning retreat, feedback, finalization of a written strategic plan, development of an implementation plan, etc.
x Deliverables: Five-year Strategic Plan with 3-5 major goals, each with 2-3 specific objectives and associated metrics, and an Implementation Plan specifying timelines, owners and workgroups for each goal, that together will increase excitement, enthusiasm, productivity, and creativity, and increase impact on veteran care, population care, etc.
x Progress: Update ACOS monthly. Introductions from Committee Members x Each member discussed their specialties, involvement with research, and amount of time
with the VA. Where Are We in Research at the VA? x As a basis for a larger discussion, the Committee will need to establish the facts, including
but not limited to funding to Minneapolis VA investigators, publications, local collaborations to be mapped by methods to be determined, and perhaps data on effort mapping.
x To foster collaborations, preliminary ideas also included seminar series and Research Week. x For broader data-gathering, preliminary ideas included surveys and focus groups, perhaps
accompanied by facility-wide announcements of the strategic planning process. What Are the Strengths and Weaknesses of VA Research? x The clinical population is large, accessible and rich. x Most VA staff facilitate rather than hinder research.
- 4 -

x The current environment for junior investigators, especially non-clinicians, is unsustainable, with issues including but not limited to soft-money salaries, VA eligibility and uncertainties surrounding provisions for salary on grants. Mentorship and opportunities to collaborate with senior investigators are lacking.
x “Clinical creep” is impeding clinician-researchers, with increasing demands to manage a growing, more complicated patient population, and significant variability among and within service lines in protecting research time.
x The safety net for funding lapses including bridge funding is inadequate. x Basic research is in decline, and with it the capacity for biological arms in early-phase
clinical trials, among other repercussions. x Administrative support for assembling and submitting grant proposals is inadequate. x The regulatory burden is excessive. x Many aspects of the research infrastructure are opaque. x Core research support in areas such as study design, data management and statistics is
lacking. The effects are not just obvious loss of institutional research productivity but also the converse, namely effort wasted on poorly conceived proposals, etc.
x It is hard to recruit new investigators. There are no provisions for start-up packages in basic science, where such packages are the norm. Significant growth in clinical demands undercuts appeal of the VA and its research opportunities vis-à-vis private practice, where salaries are higher.
x With recent policy changes, effort arrangements with the University of Minnesota are becoming unworkable.
How Important Is the Strategic Planning Process? The Strategic Plan will be important if it merits use, relates to veteran and local populations, and helps to attract and retain good employees. The Committee agreed to continue planning discussions on April 20 and 27. Meeting adjourned at 4:30pm
- 5 -

Research Experience
Coming off CDAHard for junior investigators
Clinicians
Have hard money position
Non clinicians (PhD)
challenge to support salary
hard to qualify for applying
limitations on grant funding
Need for collaborations toprovide other support
streams
Need for safety net
Need more funding sourcesother than VA
Can UMN money be used topay VA salary
Funding
tougher for younger faculty
Under 40 not getting grants(42 yo first R01)
Need for Other fundingprivate
how to support them for drytimes
Lots of Clinical Populations
Staff supportive of research
Can't combine funding fromdifferent services
what are other models offunctioning from other
institutions
Bridge funding
Instability is a major risk
black cloud
structural
lack of bridge funding
institutional agreementslimiting
difficulty assembling salaryfrom multiple sources
contracts - UMN adding28% indirect
no one is stepping this
Basic Science
is dying here
need it support the clinicalwork
theoretical concern -removing of basic labs
cancer research verytranslational now
clinical creep
md visit from 3800-5400 in 6years with increasing acuity
some sections protect MDmore
have hard time hiring
altruism is not the plan
lower salary, no start uppackage
what is the carrot?
hard to recruit someonebecause of no startup
Mentorship
dealing with union
unclear researchinfrastructure - no info
mechanism formethodological rigor
shock about lack ofresearch support
review of research protocols
Academic Affiliation
5/8 issue
nature of affiliation
what do we need to know?
how to relate to VA mission
improved clinical care
attract physicians
hard salary
clinical population
great place to do research
Cliinical Research
Clinical infrastructureavailable for research
- 6 -
Strategic Planning Committee Meeting – April 20, 2015
Meeting called to order at 4:05pm by Yoav Segal Present: Yoav Segal, Selcuk Adabag, Mark Klein, Andrew Hansen, Chris Wendt, Shannon Kehle-Forbes, Kristin Chrouser (conference phone), Mallory Lorge (Administrative) Absent: Apostolos Georgopoulos, Kelvin Lim Updates • A Committee SharePoint is up and running. • Data requested by the Committee are being collected and uploaded to the SharePoint. Research Data • Data provided to the Committee and available on the SharePoint were reviewed and
discussed including nuances. Second-order questions were collected. • The current distribution of RDIS expenditures from funding sources (38% VA, 35% NIH,
27% other) was deemed favorable. • The Committee indicated that data would be used throughout the strategic planning process
to better understand VA research. Topics for the Strategic Planning Process • A preliminary list of possible topics to be addressed by the strategic planning process was
distributed, reviewed, discussed and revised. The revised list is attached. • Among possible topics, a few drew particular attention including protected time and
improving infrastructure for leveraging clinician subject-matter expertise. • The Committee recognized that a key part of the strategic planning process would be to
identify 1 to 3 core topics that if better understood and addressed effectively would improve research, from its current level judged at 6 to 8.
The Committee agreed to move ahead on a means of wider data-gathering (survey, focus groups, etc.) and begin formulating questions. Meeting adjourned at 5:15pm
- 7 -

Topics – If Better Understood, Which Will Have the Highest Impact on Research Productivity?
• Fostering Collaborations • BLRD/CSRD => translation • HSRD/CSRD => implementation, trial design
• Engaging the VA System (patients, clinicians, other facilities, bureaucracy, policy makers) • Establishing and Maintaining Centers of Excellence • Strengthening Connections to Clinical Care (irrefutable needs, implementation, etc.) • Accessing the Clinical Population • Improving the Environment for Junior Investigators, Non-Clinicians
(hard money, mentorship, joint/collaborative grants) • Improving the Environment for Junior Investigators, Clinicians
(clinical demands, mentorship, joint/collaborative grants) • Addressing “Clinical Creep” • Bridge Funding • Understanding the Minneapolis VA HCS Research Portfolio
• Overall size and balance among BLRD-, CSRD-, HSRD- and RRD-type projects • Funding and funding sources among units (CCDOR, GRECC, Brain Sciences, etc.) • Strengths and weaknesses, competitive advantages, etc., factoring into research planning • Funded versus unfunded research
• Basic Research in Decline • Administrative Support • Regulatory Burden • Transparency of the Research Infrastructure • Core Research Support (study design, data management, statistics) • Creating Research Infrastructure to Leverage Clinician Subject-Matter Expertise • Making VA-wide Clinical Data Accessible through Core Infrastructure (programmers,
statisticians, grant writers, etc.) • Understanding the Investigator Workforce
• Size and organization – just right? too big/small? well organized? • Demographics (age, gender, etc.) • Investigator-Intrinsic Factors – skills, priorities, instincts, etc.
• Identifying, selecting and recruiting new investigators in the face of challenges • Within the existing workforce, deploying “the right people in the right places”
• Recruitment of New Investigators • Industry Partnerships (advantages/disadvantages, parameters, etc.), CRADAs • MVMREF – Roles, Responsibilities, Contributions, etc. • University of Minnesota Affiliation • Understanding Institutional (Financial) Resources Vis-à-Vis Research
- 8 -

Strategic Planning Committee Meeting – April 27, 2015 Meeting called to order at 4:00pm by Selcuk Adabag Present: Yoav Segal, Selcuk Adabag, Mark Klein, Andrew Hansen, Christine Wendt, Shannon Kehle-Forbes, Kristin Chrouser, Kelvin Lim, Mallory Lorge (Administrative) Absent: Apostolos Georgopoulos Research Data • Data provided to the Committee, attached to this document, and available on the SharePoint
were reviewed and discussed. • The Committee was surprised to find that – among research units – Basic Research ranked
second only to CCDOR in RDIS expenditures for 2014. The Committee requested further data on trends since 2010.
• The Committee noted that funding for clinical research among investigators in Medicine who are not affiliated with CCDOR was below expectations.
• The Committee noted that – among complexity level 1a VA facilities – the Minneapolis VA was mid-level in funding. By comparison to better funded VA’s, the Minneapolis VA generally fell short in VA as against non-VA funding.
• The Committee requested facility-wide publication data in a form to be determined. Reaching Investigators – What Do We Want to Know? • Shannon Kehle-Forbes led a discussion on options for data-gathering, including surveys and
focus groups, to serve the strategic planning process. She emphasized that any such undertaking would have to start by defining the research question.
• In response to the prompt “What Do We Want to Know?”, the Committee raised several questions: • What are the most important topics related to improving research? How would
investigators rank those topics? Would such rankings be important for the overall strategic plan, individual investigators or both?
• What does research at the Minneapolis VA look and feel like at the ground level? • Which research areas are strengthening? Which are weakening? • What additional trends are important to research at the Minneapolis VA? • What are the barriers to improvement? • What should research look like at the VA? Should it be veteran-centric? • What are the characteristics of successful Minneapolis VA investigators, divisions,
departments and research units? • Why are some investigators attracted to the Minneapolis VA and others not?
• Consensus developed around a survey, to include a request for demographic information and 5 or 6 questions, and to be followed by 3 focus groups of 8 individuals each. The Committee had preliminary discussions on achieving high response and constituting the focus groups.
• The Committee had preliminary discussions on involving stakeholders in the strategic planning process, including the Veterans Council by way of Ralph Heussner, primary care providers, Minneapolis VA and VISN 23 leadership, and perhaps others.
- 9 -

The Committee agreed that each member would submit 3 topics or draft survey questions to Mallory Lorge by Monday, May 4, to serve as the starting point for a survey to be distributed by mid-June. Mallory will investigate options for implementing the survey on-line. The group deferred a follow-up meeting pending further progress. Meeting adjourned at 5:00pm
- 10 -

VA Research Strategic Planning Committee Supplementary Data April 27, 2015
Notes: 1. Source data are from file “RDIS Expenditures – Investigator”, created and last
modified by Margaret Bordanea on April 17, 2015. 2. “Other Units” = Dermatology, Neurology, Pharmacy, Surgery. 3. “Other Sources” = Other Federal, Academic, Corporate, Volunteer Agency. 4. Expenditures are assigned once and, in cases of dual appointment, subjectively. In
general, the hierarchy is: Basic Research = Brain Sciences = CCDOR = Rehab > GRECC > Medicine = Mental Health = Other Units.
5. A significant and unspecified percentage of expenditures, particularly NIH-funded, relate to off-site projects at the University of Minnesota.
2
4
6
8
10
Basic Research
Brain Sciences
CCDOR GRECC Medicine Mental Health
Other Units Rehab
Milli
ons
of D
olla
rs
RDIS Expenditures, 2014
Other SourcesNIHVA
- 11 -

VA R
esea
rch
Stra
tegi
c Pl
anni
ng C
omm
ittee
Su
pple
men
tary
Dat
a Ap
ril 2
7, 2
015
! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! Not
es:!
1. S
ourc
e da
ta a
re fr
om h
ttp://
vaw
w.a
rc.m
ed.v
a.go
v/re
ports
/ver
a/ve
ra20
13/fi
nal_
vera
2013
/ver
a201
3_fin
al_t
able
8.ht
m.
2. S
ome
faci
lity
com
plex
ity le
vels
may
be
date
d.
01020304050607080 San Fran
cisco Palo
AltoSan
Diego
Boston
/Brockto
nWes
t Hav
en Seattle
Los A
ngele
s/Sep
ulved
aPitts
burgh Portlan
d Durham
Minnea
polis Hou
ston Atla
nta Nashv
ille Chicag
oClev
eland Denve
rSan
Antonio
Hines
Albuqu
erque
Gaines
ville
Indian
apolis Memph
isMilw
auke
e Tampa
Birming
ham Dallas
Richmon
d
New Yo
rk/Broo
klyn St. L
ouis Tu
cson
Bay Pine
s FL
San Ju
anBalt
imore Ann
Arbor
Cincinn
ati
Salt La
ke City
Philade
lphia
Washin
gton D
CLit
tle Roc
k Miami Mad
ison
Long
Beach
East O
range
NJLo
ma Lind
a Detroit
Oklaho
ma City
Augus
ta GA Phoen
ixJa
ckson
MS
Iowa C
ity
Charle
ston S
C Bronx Lo
uisvill
e Omaha
Sacram
ento
Columbia
MO
Temple
TX Buffalo
Kansa
s City Le
xingto
nSyra
cuse
Mounta
in Hom
e TN
Northp
ort NY Alba
ny Salem VA
Columbia
SCSalis
bury
NCAsh
eville
NCShre
vepo
rt Dayton Tope
ka
Millions of Dollars
VERA
Res
earc
h Su
ppor
t, Le
vel 1
Fac
ilitie
s, 2
013
Non-
VA P
eer-R
evie
wed
Que
riVA
1a
1
b
1c
- 12 -

Strategic Planning Committee Meeting – August 24, 2015 Meeting called to order at 3:30pm by Selcuk Adabag Present: Apostolos Georgopoulos, Selcuk Adabag, Andrew Hansen, Shannon Kehle-Forbes, Mark Klein, Kelvin Lim, Yoav Segal, Christine Wendt, Mallory Lorge (Administrative) Absent: Kristin Chrouser Survey Results x The e-mail recipient list was not “cleaned up,” including research personnel who are not
Principal Investigators. x Respondents were weighted towards senior-level career stage. x The Committee requested stratification of survey responses on the basis of career stage,
clinician versus non-clinician, and other demographic variables. x The Committee made the following observations:
x Overall, there were pockets of satisfaction and areas for improvement. x “The environment is better than the opportunities.” x Respondents are publishing but not applying for grants. Two hypotheses:
i) Respondents are not Principal Investigators and/or are applying as Co-Investigators; and ii) Clinicians are too busy.
x There is a drop-off in satisfaction between junior- and mid-level career stage. One hypothesis: We are not recruiting junior investigators who will be resilient.
x Committee members commented that there might be a need for deeper understanding regarding mentoring of junior investigators.
x There is satisfaction with collaborations relative to other areas, suggesting that new efforts in this area need not be a top priority.
x Despite satisfaction with collaborations, there is uncertain knowledge of what colleagues are doing.
x Over 50% of the respondents who identified as clinicians spend less than 50% of their time on research. This was not felt to be the profile of a successful clinician-investigator. Additional comments: i) Some sections may stretch access rather than steal research time; ii) Patient but not faculty numbers have increased; and iii) Some clinicians are protected more than others.
Focus Groups x The Committee discussed possible topics:
x i) Low number of grant submissions; ii) Recruitment; iii) Junior investigator environment; iv) Infrastructure; and v) Future of VA research.
x “What does a successful clinician-investigator at the VA look like?” x Creating a research community x “Hidden factors” such as i) VA employment policies regarding visas; and ii) Human
Resources underperformance. x The Committee discussed logistics: i) Separating junior and senior investigators; ii)
Recruitment outside of survey volunteers; and iii) Pairing committee members as mediators.
- 13 -

Looking Ahead x The Committee agreed to start circulating dates for a December retreat lasting a day or two.
The outcome would be a first-draft report. The question as to whether others would be invited was left open.
Meeting adjourned at 4:30pm
- 14 -

Survey Responses
- 15 -

New Summary Report - 21 August 2015
1. When did you complete your training?
30.2%
25.6%
32.6%
11.6%
Before 1990 1990 - 1999 2000 - 2009 2010 - 20150
20
40
60
80
100
Value Percent Count
Before 1990 30.2% 26
1990 - 1999 25.6% 22
2000 - 2009 32.6% 28
2010 - 2015 11.6% 10
Total 86
Statistics
Total Responses 86
Sum 119,880.0
Average 1,394.0
StdDev 7.0
Max 2,010.0
- 16 -

2. What is your perception of your career stage?
23.3%
36.1%
40.7%
Junior Mid Senior0
20
40
60
80
100
Value Percent Count
Junior 23.3% 20
Mid 36.1% 31
Senior 40.7% 35
Total 86
Statistics
Total Responses 86
- 17 -

0 1 - 2 3 - 4 5 or more Responses
Peer-reviewed papers as first/last author 9
10.5%
16
18.6%
24
27.9%
37
43.0%
86
Peer-reviewed papers as middle author 11
12.8%
21
24.4%
18
20.9%
36
41.9%
86
NIH grants as PI 57
66.3%
18
20.9%
4
4.7%
7
8.1%
86
VA grants as PI 39
45.3%
33
38.4%
8
9.3%
6
7.0%
86
Other Federal grants (NSF, DoD, etc.) as PI 67
77.9%
12
14.0%
5
5.8%
2
2.3%
86
Foundation grants as PI 55
64.0%
25
29.1%
3
3.5%
3
3.5%
86
Industry grants as PI 75
87.2%
9
10.5%
2
2.3%
0
0.0%
86
3. What is your gender?
41.9%
57%
1.2%
Female Male I prefer not to answer0
20
40
60
80
100
Value Percent Count
Female 41.9% 36
Male 57.0% 49
I prefer not to answer 1.2% 1
Total 86
Statistics
Total Responses 86
4. In the past 3 years, how many of each of the following did you submit?
- 18 -

5. Have you ever been a Principal Investigator (not Co-Investigator) on a funded VA or NIH grant?
67.4%
32.6%
Yes No0
20
40
60
80
100
Value Percent Count
Yes 67.4% 58
No 32.6% 28
Total 86
Statistics
Total Responses 86
- 19 -

6. Please indicate whether you have VA clinical responsibilities in any of the following areas:
33.7%
10.5% 9.3%
2.3%
44.2%
Primary Care (general internal
medicine, medical
subspecialties)
Specialty Care (surgery,
surgical subspecialties)
Mental Health Extended Care/Rehabilitation I am a non-clinician
investigator at the VA
0
100
25
50
75
Value Percent Count
Primary Care (general internal medicine, medical
subspecialties)
33.7% 29
Specialty Care (surgery, surgical subspecialties) 10.5% 9
Mental Health 9.3% 8
Extended Care/Rehabilitation 2.3% 2
I am a non-clinician investigator at the VA 44.2% 38
Total 86
Statistics
Total Responses 86
- 20 -

7. Please indicate whether you are a core investigator in any of the following:
4.7%
20.9%
4.7%
69.8%
Brain Sciences Center CCDOR GRECC None of the above0
20
40
60
80
100
Value Percent Count
Brain Sciences Center 4.7% 4
CCDOR 20.9% 18
GRECC 4.7% 4
None of the above 69.8% 60
Total 86
Statistics
Total Responses 86
- 21 -

8. What is your primary area of research?
30.2%
37.2%
22.1%
5.8% 4.7%
Basic laboratory research Clinical research Health services research Rehabilitation Other0
20
40
60
80
100
Value Percent Count
Basic laboratory research 30.2% 26
Clinical research 37.2% 32
Health services research 22.1% 19
Rehabilitation 5.8% 5
Other 4.7% 4
Total 86
Statistics
Total Responses 86
- 22 -
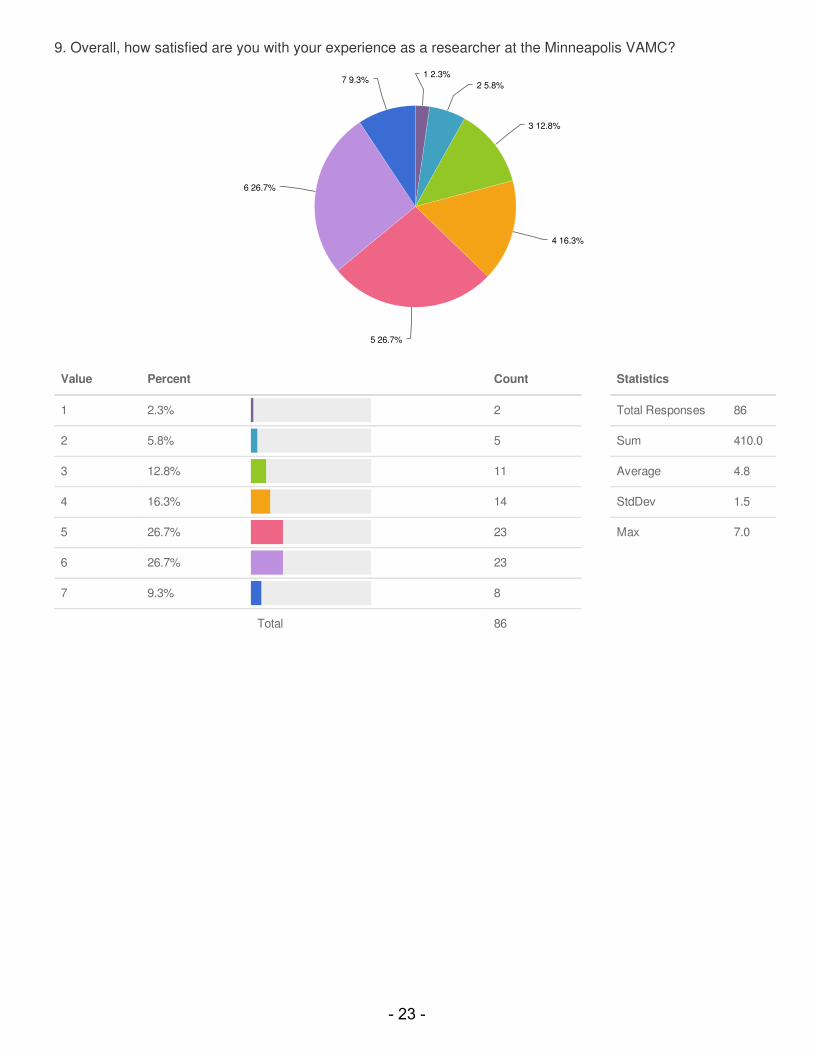
9. Overall, how satisfied are you with your experience as a researcher at the Minneapolis VAMC?
1 2.3%
2 5.8%
3 12.8%
4 16.3%
5 26.7%
6 26.7%
7 9.3%
Value Percent Count
1 2.3% 2
2 5.8% 5
3 12.8% 11
4 16.3% 14
5 26.7% 23
6 26.7% 23
7 9.3% 8
Total 86
Statistics
Total Responses 86
Sum 410.0
Average 4.8
StdDev 1.5
Max 7.0
- 23 -
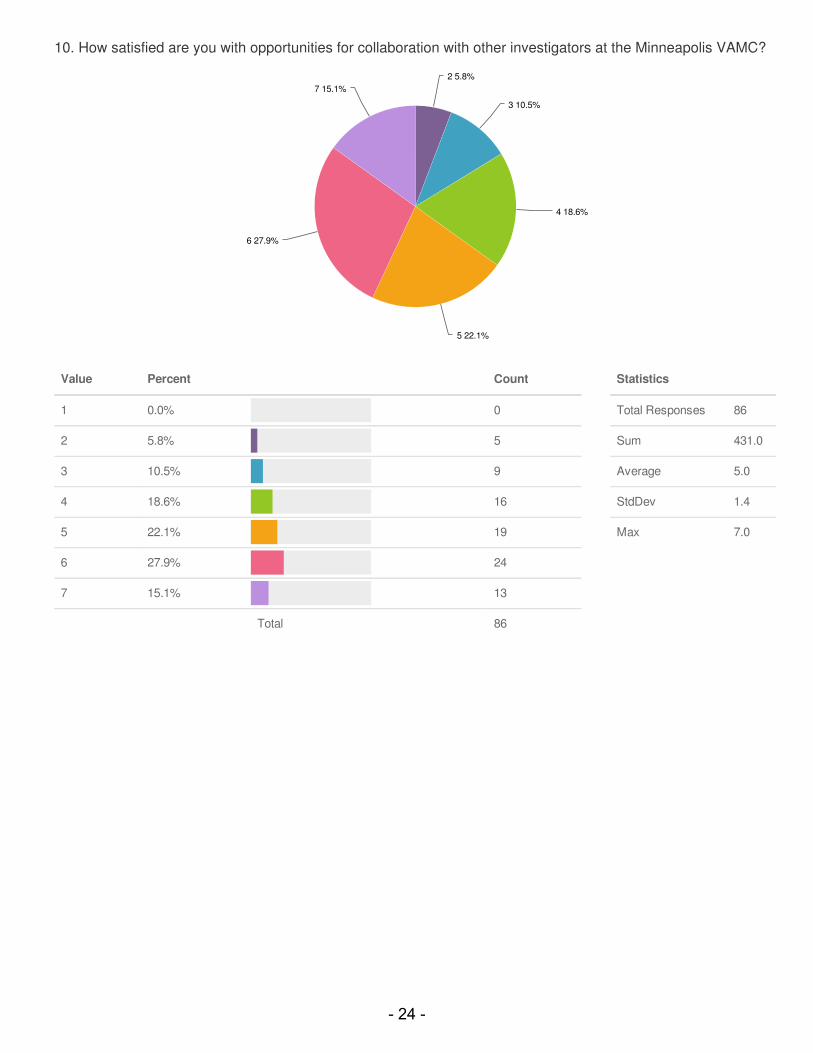
10. How satisfied are you with opportunities for collaboration with other investigators at the Minneapolis VAMC?
2 5.8%
3 10.5%
4 18.6%
5 22.1%
6 27.9%
7 15.1%
Value Percent Count
1 0.0% 0
2 5.8% 5
3 10.5% 9
4 18.6% 16
5 22.1% 19
6 27.9% 24
7 15.1% 13
Total 86
Statistics
Total Responses 86
Sum 431.0
Average 5.0
StdDev 1.4
Max 7.0
- 24 -

11. How important is it that the environment at the Minneapolis VAMC foster collaborations among investigators?
1 1.2%
2 1.2%
3 3.5%
4 3.5%
5 7%
6 27.9%
7 55.8%
Value Percent Count
1 1.2% 1
2 1.2% 1
3 3.5% 3
4 3.5% 3
5 7.0% 6
6 27.9% 24
7 55.8% 48
Total 86
Statistics
Total Responses 86
Sum 534.0
Average 6.2
StdDev 1.2
Max 7.0
- 25 -

12. Are you currently collaborating with other investigators?
Yes 93%
No 7%
Value Percent Count
Yes 93.0% 80
No 7.0% 6
Total 86
Statistics
Total Responses 86
- 26 -

Check all that apply.
77.5%
61.3%
41.3%
62.5%
45%
Yes, I am collaborating with
Minneapolis VAMC
investigators within my
department or division
Yes, I am collaborating with
Minneapolis VAMC
investigators outside my
department or division
Yes, I am collaborating with
investigators at other VA
facilities
Yes, I am collaborating with
investigators at the University
of Minnesota
Yes, I am collaborating with
investigators at other
academic sites
0
100
25
50
75
Value Percent Count
Yes, I am collaborating with Minneapolis VAMC
investigators within my department or division
77.5% 62
Yes, I am collaborating with Minneapolis VAMC
investigators outside my department or division
61.3% 49
Yes, I am collaborating with investigators at other VA
facilities
41.3% 33
Yes, I am collaborating with investigators at the
University of Minnesota
62.5% 50
Yes, I am collaborating with investigators at other
academic sites
45.0% 36
Total 80
Statistics
Total Responses 80
- 27 -

Strongly
Disagree1 2 3
NeitherAgree
nor Disagree4 5 6
Strongly
Agree7 Responses
There is a culture of collaboration at the
Minneapolis VAMC.
0
0.0%
7
8.1%
7
8.1%
20
23.3%
25
29.1%
18
20.9%
9
10.5%
86
The research environment at the
Minneapolis VAMC is collegial.
2
2.3%
5
5.8%
6
7.0%
13
15.1%
20
23.3%
25
29.1%
15
17.4%
86
I have talented colleagues at the
Minneapolis VAMC with whom I can
collaborate.
0
0.0%
2
2.3%
3
3.5%
8
9.3%
14
16.3%
26
30.2%
33
38.4%
86
Investigators at the Minneapolis VAMC
share information and ideas with each
other.
0
0.0%
7
8.1%
5
5.8%
18
20.9%
24
27.9%
16
18.6%
16
18.6%
86
Investigators at the Minneapolis VAMC
work well together.
0
0.0%
3
3.5%
4
4.7%
16
18.6%
31
36.0%
16
18.6%
16
18.6%
86
I know what my colleagues at the
Minneapolis VAMC are working on.
1
1.2%
8
9.3%
18
20.9%
23
26.7%
16
18.6%
14
16.3%
6
7.0%
86
I have time to collaborate. 1
1.2%
9
10.5%
9
10.5%
17
19.8%
20
23.3%
19
22.1%
11
12.8%
86
Not at all Helpful1 2 3 4 5 6 Very Helpful7 Responses
Additional seminar series 12
14.0%
7
8.1%
7
8.1%
27
31.4%
15
17.4%
12
14.0%
6
7.0%
86
Up-to-date, on-line investigator profiles 2
2.3%
5
5.8%
11
12.8%
12
14.0%
29
33.7%
13
15.1%
14
16.3%
86
Collaborative grant opportunities 1
1.2%
2
2.3%
0
0.0%
8
9.3%
21
24.4%
32
37.2%
22
25.6%
86
New forums to incubate ideas 1
1.2%
1
1.2%
3
3.5%
13
15.1%
19
22.1%
31
36.0%
18
20.9%
86
13. Specify the degree to which you agree with the following statements:
14. How helpful would the following be to improving collaborations at the Minneapolis VAMC?
- 28 -

15. How satisfied are you with the environment for junior investigators at the Minneapolis VAMC?
1 2.3%
2 22.1%
3 17.4%
4 22.1%
5 24.4%
6 9.3%
7 2.3%
Value Percent Count
1 2.3% 2
2 22.1% 19
3 17.4% 15
4 22.1% 19
5 24.4% 21
6 9.3% 8
7 2.3% 2
Total 86
Statistics
Total Responses 86
Sum 328.0
Average 3.8
StdDev 1.4
Max 7.0
- 29 -

16. How important is it that the environment at the Minneapolis VAMC foster the development of junior
investigators?
3 1.2%
4 5.8%
5 5.8%
6 16.3%
7 70.9%
Value Percent Count
1 0.0% 0
2 0.0% 0
3 1.2% 1
4 5.8% 5
5 5.8% 5
6 16.3% 14
7 70.9% 61
Total 86
Statistics
Total Responses 86
Sum 559.0
Average 6.5
StdDev 0.9
Max 7.0
- 30 -

17. Have you received research mentorship at the Minneapolis VAMC?
Yes 53.5%
No 46.5%
Value Percent Count
Yes 53.5% 46
No 46.5% 40
Total 86
Statistics
Total Responses 86
- 31 -

Not at all Helpful1 2 3 4 5 6 Very Helpful7 Responses
Research strategy and planning 0
0.0%
1
2.2%
2
4.3%
3
6.5%
15
32.6%
9
19.6%
16
34.8%
46
Applying for independent funding 0
0.0%
3
6.5%
3
6.5%
7
15.2%
10
21.7%
7
15.2%
16
34.8%
46
Identifying Co-Investigator roles 1
2.2%
6
13.0%
2
4.3%
10
21.7%
10
21.7%
8
17.4%
9
19.6%
46
Publishing papers 0
0.0%
3
6.5%
3
6.5%
4
8.7%
13
28.3%
11
23.9%
12
26.1%
46
Professional networking 0
0.0%
6
13.0%
5
10.9%
4
8.7%
12
26.1%
7
15.2%
12
26.1%
46
Check all that apply.
58.7%
67.4%
21.7%23.9%
21.7%
Yes, I had/have a formal
Minneapolis VAMC mentor
Yes, I had/have an informal
Minneapolis VAMC mentor
Yes, I had/have a mentoring
committee
Yes, I had/have a University of
Minnesota mentor
Yes, I had/have a mentor from
another academic site
0
100
25
50
75
Value Percent Count
Yes, I had/have a formal Minneapolis VAMC mentor 58.7% 27
Yes, I had/have an informal Minneapolis VAMC mentor 67.4% 31
Yes, I had/have a mentoring committee 21.7% 10
Yes, I had/have a University of Minnesota mentor 23.9% 11
Yes, I had/have a mentor from another academic site 21.7% 10
Total 46
Statistics
Total Responses 46
How helpful have your mentors been to you in the following areas?
- 32 -

Strongly
Disagree1 2 3
Neither Agree
nor Disagree4 5 6
Strongly
Agree7 Responses
The amount of funding that I am
expected to find is reasonable.
2
10.0%
2
10.0%
2
10.0%
3
15.0%
5
25.0%
3
15.0%
3
15.0%
20
The time that I have to secure
external funding is reasonable.
2
10.0%
3
15.0%
3
15.0%
4
20.0%
3
15.0%
4
20.0%
1
5.0%
20
Senior investigators care about my
professional development.
0
0.0%
2
10.0%
3
15.0%
2
10.0%
3
15.0%
5
25.0%
5
25.0%
20
The Research Office has helped me
progress in my career.
1
5.0%
3
15.0%
2
10.0%
7
35.0%
1
5.0%
4
20.0%
2
10.0%
20
I will be successful as an independent
investigator.
1
5.0%
0
0.0%
0
0.0%
5
25.0%
4
20.0%
6
30.0%
4
20.0%
20
25 - 50% 50 - 75% >75% Responses
Administration 39
83.0%
7
14.9%
1
2.1%
0
0.0%
47
Research 11
22.9%
20
41.7%
14
29.2%
3
6.3%
48
Teaching 34
70.8%
14
29.2%
0
0.0%
0
0.0%
48
Clinical Duties 13
27.1%
20
41.7%
14
29.2%
1
2.1%
48
18. You previously indicated that you are a junior investigator. Specify the degree to which you agree with the
following statements:
19. You previously indicated that you have VA clinical responsibilities. On average, what percent of your work
time do you spend on each of these activities?
- 33 -

20. How satisfied are you with your time available for research and scholarship?
1 4.2%
2 10.4%
3 18.8%
4 10.4%
5 22.9%
6 14.6%
7 18.8%
Value Percent Count
1 4.2% 2
2 10.4% 5
3 18.8% 9
4 10.4% 5
5 22.9% 11
6 14.6% 7
7 18.8% 9
Total 48
Statistics
Total Responses 48
Sum 219.0
Average 4.6
StdDev 1.8
Max 7.0
- 34 -

21. How important is it that you have protected time for research and scholarship?
4 2.1%
5 4.2%
6 20.8%
7 72.9%
Value Percent Count
1 0.0% 0
2 0.0% 0
3 0.0% 0
4 2.1% 1
5 4.2% 2
6 20.8% 10
7 72.9% 35
Total 48
Statistics
Total Responses 48
Sum 319.0
Average 6.6
StdDev 0.7
Max 7.0
- 35 -

Strongly
Disagree1 2 3
Neither
Agree nor
Disagree4 5 6
Strongly
Agree7 Responses
My clinical responsibilities are increasing
over time.
7
14.6%
4
8.3%
5
10.4%
4
8.3%
6
12.5%
8
16.7%
14
29.2%
48
Clinical demands prevent me from
performing research.
10
20.8%
6
12.5%
2
4.2%
9
18.8%
10
20.8%
5
10.4%
6
12.5%
48
Clinical duties should be divided equally
among investigators and non-investigators.
20
41.7%
12
25.0%
6
12.5%
3
6.3%
3
6.3%
0
0.0%
4
8.3%
48
Junior investigators should receive
protected time.
0
0.0%
1
2.1%
1
2.1%
2
4.2%
4
8.3%
16
33.3%
24
50.0%
48
Protected time should be tied to research
productivity.
2
4.3%
0
0.0%
1
2.1%
7
14.9%
9
19.1%
16
34.0%
12
25.5%
47
I would want to work as a clinician at the
Minneapolis VAMC even if I could not
conduct research.
10
20.8%
5
10.4%
8
16.7%
5
10.4%
8
16.7%
7
14.6%
5
10.4%
48
22. Specify the degree to which you agree with the following statements?
- 36 -

23. How satisfied are you with the research infrastructure at the Minneapolis VAMC?
1 3.5%
2 19.8%
3 14%
4 12.8%
5 30.2%
6 15.1%
7 4.7%
Value Percent Count
1 3.5% 3
2 19.8% 17
3 14.0% 12
4 12.8% 11
5 30.2% 26
6 15.1% 13
7 4.7% 4
Total 86
Statistics
Total Responses 86
Sum 353.0
Average 4.1
StdDev 1.6
Max 7.0
- 37 -

24. How important is it to have a supportive research infrastructure for your success as an investigator?
2 1.2%
4 2.3%
5 4.7%
6 18.6%
7 73.3%
Value Percent Count
1 0.0% 0
2 1.2% 1
3 0.0% 0
4 2.3% 2
5 4.7% 4
6 18.6% 16
7 73.3% 63
Total 86
Statistics
Total Responses 86
Sum 567.0
Average 6.6
StdDev 0.8
Max 7.0
- 38 -

Not at all
Helpful1 2 3 4 5 6
Very
Helpful7 Responses
Support for study design and methods 2
2.3%
3
3.5%
7
8.1%
13
15.1%
21
24.4%
20
23.3%
20
23.3%
86
Support for statistical needs 2
2.3%
1
1.2%
4
4.7%
8
9.3%
16
18.6%
8
9.3%
47
54.7%
86
Support for access to national VA data 4
4.7%
2
2.3%
5
5.8%
15
17.4%
11
12.8%
13
15.1%
36
41.9%
86
Support for data management including
collaborative data sharing
3
3.5%
6
7.0%
6
7.0%
12
14.0%
17
19.8%
14
16.3%
28
32.6%
86
General IT support 1
1.2%
4
4.7%
1
1.2%
14
16.3%
8
9.3%
25
29.1%
33
38.4%
86
Support for grant submissions 1
1.2%
2
2.3%
4
4.7%
6
7.0%
7
8.1%
28
32.6%
38
44.2%
86
Access to research coordinators 1
1.2%
4
4.7%
2
2.3%
16
18.6%
9
10.5%
23
26.7%
31
36.0%
86
Clerical/secretarial support 2
2.3%
6
7.0%
7
8.1%
6
7.0%
11
12.8%
17
19.8%
37
43.0%
86
Access to high-quality research and technical
staff
0
0.0%
3
3.5%
3
3.5%
9
10.5%
10
11.6%
27
31.4%
34
39.5%
86
Figure and illustration services 5
5.8%
16
18.6%
6
7.0%
16
18.6%
14
16.3%
11
12.8%
18
20.9%
86
New investigator orientation to available research
support services
5
5.8%
9
10.5%
6
7.0%
15
17.4%
14
16.3%
16
18.6%
21
24.4%
86
Mid-career planning and development services 1
1.2%
7
8.1%
6
7.0%
13
15.1%
19
22.1%
15
17.4%
25
29.1%
86
Professional grant writing services 6
7.0%
11
12.8%
4
4.7%
9
10.5%
16
18.6%
16
18.6%
24
27.9%
86
Strongly
Disagree1 2 3
Neither Agree
nor Disagree4 5 6
Strongly
Agree7 Responses
The Research Office fulfills its roles in
providing research support services.
5
5.8%
16
18.6%
4
4.7%
11
12.8%
24
27.9%
21
24.4%
5
5.8%
86
The Research Office fulfills its roles in
recruitment and retention.
8
9.3%
13
15.1%
12
14.0%
27
31.4%
17
19.8%
8
9.3%
1
1.2%
86
The Research Office fulfills its roles in
strategy and planning.
4
4.7%
15
17.4%
7
8.1%
24
27.9%
22
25.6%
13
15.1%
1
1.2%
86
25. How helpful would providing the following research support services be to increasing your research
productivity?
26. Specify the degree to which you agree with the following statements?
- 39 -

27. How satisfied are you with the performance of the Research Office in advancing research at the Minneapolis
VAMC?
1 9.3%
2 9.3%
3 10.5%
4 18.6%5 26.7%
6 20.9%
7 4.7%
Value Percent Count
1 9.3% 8
2 9.3% 8
3 10.5% 9
4 18.6% 16
5 26.7% 23
6 20.9% 18
7 4.7% 4
Total 86
Statistics
Total Responses 86
Sum 366.0
Average 4.3
StdDev 1.7
Max 7.0
- 40 -
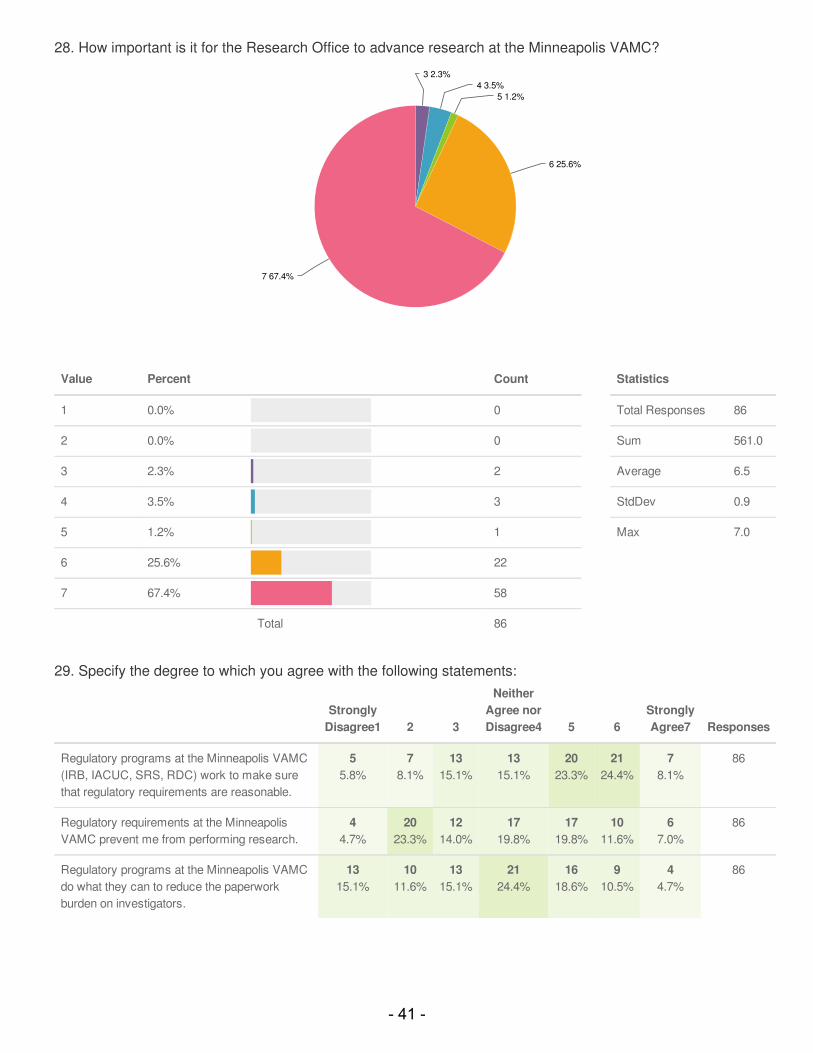
Strongly
Disagree1 2 3
Neither
Agree nor
Disagree4 5 6
Strongly
Agree7 Responses
Regulatory programs at the Minneapolis VAMC
(IRB, IACUC, SRS, RDC) work to make sure
that regulatory requirements are reasonable.
5
5.8%
7
8.1%
13
15.1%
13
15.1%
20
23.3%
21
24.4%
7
8.1%
86
Regulatory requirements at the Minneapolis
VAMC prevent me from performing research.
4
4.7%
20
23.3%
12
14.0%
17
19.8%
17
19.8%
10
11.6%
6
7.0%
86
Regulatory programs at the Minneapolis VAMC
do what they can to reduce the paperwork
burden on investigators.
13
15.1%
10
11.6%
13
15.1%
21
24.4%
16
18.6%
9
10.5%
4
4.7%
86
28. How important is it for the Research Office to advance research at the Minneapolis VAMC?
3 2.3%
4 3.5%
5 1.2%
6 25.6%
7 67.4%
Value Percent Count
1 0.0% 0
2 0.0% 0
3 2.3% 2
4 3.5% 3
5 1.2% 1
6 25.6% 22
7 67.4% 58
Total 86
Statistics
Total Responses 86
Sum 561.0
Average 6.5
StdDev 0.9
Max 7.0
29. Specify the degree to which you agree with the following statements:
- 41 -

30. How satisfied are you with recruitment of new investigators to the Minneapolis VAMC?
1 3.5%
2 17.4%
3 23.3%
4 39.5%
5 9.3%
6 7%
Value Percent Count
1 3.5% 3
2 17.4% 15
3 23.3% 20
4 39.5% 34
5 9.3% 8
6 7.0% 6
7 0.0% 0
Total 86
Statistics
Total Responses 86
Sum 305.0
Average 3.5
StdDev 1.2
Max 6.0
- 42 -

Strongly
Disagree1 2 3
Neither Agree
nor Disagree4 5 6
Strongly
Agree7 Responses
The Minneapolis VAMC recruits new
investigators effectively.
6
7.0%
13
15.1%
18
20.9%
29
33.7%
16
18.6%
4
4.7%
0
0.0%
86
The Minneapolis VAMC is well served by
its current recruitment practices.
6
7.0%
16
18.6%
17
19.8%
37
43.0%
9
10.5%
1
1.2%
0
0.0%
86
The Minneapolis VAMC offers
competitive recruitment packages.
10
11.6%
13
15.1%
21
24.4%
30
34.9%
10
11.6%
2
2.3%
0
0.0%
86
Investigator searches at the Minneapolis
VAMC attract high-quality candidates.
3
3.5%
16
18.6%
12
14.0%
36
41.9%
10
11.6%
9
10.5%
0
0.0%
86
31. How important is it that the Minneapolis VAMC recruit new investigators to maintain the research workforce?
3 3.5%
4 4.7%
5 12.8%
6 19.8%7 59.3%
Value Percent Count
1 0.0% 0
2 0.0% 0
3 3.5% 3
4 4.7% 4
5 12.8% 11
6 19.8% 17
7 59.3% 51
Total 86
Statistics
Total Responses 86
Sum 539.0
Average 6.3
StdDev 1.1
Max 7.0
32. Specify the degree to which you agree with the following statements:
- 43 -

33. Since you have been at the Minneapolis VAMC, have you received and then declined a formal job offer(s)
from another institution?
Yes 41.9%
No 58.1%
Value Percent Count
Yes 41.9% 36
No 58.1% 50
Total 86
Statistics
Total Responses 86
- 44 -

34. How satisfied are you with cooperation at the institutional level between the Minneapolis VAMC and the
University of Minnesota to enhance research?
1 5.8%
2 22.1%
3 22.1%4 20.9%
5 16.3%
6 11.6%
7 1.2%
Value Percent Count
1 5.8% 5
2 22.1% 19
3 22.1% 19
4 20.9% 18
5 16.3% 14
6 11.6% 10
7 1.2% 1
Total 86
Statistics
Total Responses 86
Sum 309.0
Average 3.6
StdDev 1.5
Max 7.0
- 45 -

35. How important is it that the Minneapolis VAMC and University of Minnesota cooperate at the institutional level
to enhance research?
2 1.2%
4 4.7%
5 17.4%
6 29.1%
7 47.7%
Value Percent Count
1 0.0% 0
2 1.2% 1
3 0.0% 0
4 4.7% 4
5 17.4% 15
6 29.1% 25
7 47.7% 41
Total 86
Statistics
Total Responses 86
Sum 530.0
Average 6.2
StdDev 1.0
Max 7.0
- 46 -

Strongly
Disagree1 2 3
Neither
Agree nor
Disagree4 5 6
Strongly
Agree7 Responses
Minnesota Veterans Medical Research and
Education Foundation (MVMREF) plays an
important role in the success of my research
program.
5
5.8%
11
12.8%
8
9.3%
19
22.1%
13
15.1%
16
18.6%
14
16.3%
86
It is important that the Minneapolis VAMC’s
research program engage industry partners.
3
3.5%
9
10.5%
4
4.7%
15
17.4%
26
30.2%
17
19.8%
12
14.0%
86
It is important that research leaders at the
Minneapolis VAMC be well-networked with VA
Central Office.
1
1.2%
1
1.2%
2
2.3%
6
7.0%
18
20.9%
28
32.6%
30
34.9%
86
Leaders at the Minneapolis VAMC and VISN 23
are dedicated to the research mission.
6
7.0%
7
8.1%
12
14.0%
18
20.9%
19
22.1%
16
18.6%
8
9.3%
86
I am rewarded by the Minneapolis VAMC for my
research productivity.
5
5.8%
18
20.9%
8
9.3%
17
19.8%
15
17.4%
16
18.6%
7
8.1%
86
My research program is directed to service-
related issues, e.g. TBI, PTSD, Gulf War illness.
25
29.1%
10
11.6%
7
8.1%
13
15.1%
5
5.8%
10
11.6%
16
18.6%
86
I have the resources that I need to obtain a grant
as a PI in the next five years.
5
5.8%
13
15.1%
9
10.5%
13
15.1%
17
19.8%
21
24.4%
8
9.3%
86
Conducting research is important to my job
satisfaction.
1
1.2%
0
0.0%
0
0.0%
2
2.3%
8
9.3%
21
24.4%
54
62.8%
86
Heading a research program as a PI is my top
priority at work.
2
2.3%
0
0.0%
3
3.5%
8
9.3%
17
19.8%
17
19.8%
39
45.3%
86
I want to be involved in research but not as a PI. 31
36.0%
12
14.0%
13
15.1%
18
20.9%
4
4.7%
4
4.7%
4
4.7%
86
The Research Service at the Minneapolis
VAMC should focus resources on areas of
strength, e.g. HSRD and service-related
conditions, versus other areas.
16
18.6%
15
17.4%
12
14.0%
21
24.4%
11
12.8%
8
9.3%
3
3.5%
86
Count Response
1 - IT related issues, such as the ability to procure, install, and use research related software.
1 Mechanisms are needed to provide temporary support to investigators who are between grants.
1 Nice survey
1 support facilities are critical for getting grants and collaboration.
36. Specify the degree to which you agree with the following statements:
37. We will be conducting a series of focus groups to gather more in-depth information about what you think the
Research Service can do to enhance and improve your research productivity. Lunch will be provided!
Please click here or e-mail [email protected] to indicate your willingness to participate. Please
provide any additional thoughts you have about the topics queried above or other areas that are important for us
to consider in developing the Research Service Strategic Plan.
- 47 -

1 Minneapolis VA Research Service needs to be evaluated by the number and amount of grants that the Minneapolis VA
investigators have obtained. Creating a supportive research infrastructure with the services outlined in this survey is critical for
success. The leadership needs to be truly dedicated to research for success.
1 I am concerned about the usefulness of the results of this survey. The link was distributed to a broad range of research
employees yet most of the questions pertained to core/senior investigators. There are many questions that I would have like to
have skipped or been able to answer "Not applicable" but that wasn't an option.
1 Have to acknowledge that IRB has made great efforts to be more research-friendly while maintaining a high standard. This is
MUCH appreciated. However, navigating IRB can still be extremely time consuming - this remains an area for development.
1 Focus should be on areas of strength but also on areas that are rising to the level of critical mass for R&D. Groups that have
eligible numbers of PIs for centers should be supported to obtain center funding when opportunities exist.
1 The regulatory burden has become unbearable. The research office tries to help but needs at least triple the staff. Please hire
more research office staff.
1 In my opinion two major areas that influence research environment are: (1) Ease of acquiring new technologies (equipment) in
the Common Service. (2) Fostering of collegiality among the investigators (not clear how it can be achieved in practice!).
1 Assistance from u of m ahc for federal local and intramural grants is lacking. Difficult to collaborate w colleagues at the u or
avail research resources such as ctsi
1 The Research Office should take control of paperwork requirements, streamlining and offering a clear vision to the PI of what
has to happen to collaborate with other researchers, to begin and then maintain research projects (including how to do
something as simple as onboard a new employee!) and ultimately to secure additional funding.
1 If you go back and read your questions, you will not this survey is not geared at all towards, which I think is telling. We are not
all PI's! Experienced staff help keep get projects completed on time and in a high quality manner. I would suggest you have a
focus group (or two) geared to staff (coordinators, RA's, data managers) as well as PIs.
1 While research is important, clinical service should remain our main mission and should be the cornerstone for reimbursement
of our employees.
1 Some of the questions were not applicable to my situation but the survey forces one to complete all questions...this may result
in misleading data
1 It is apparent that the VA support is focused on clinical and outcome based patient related research. Unless the leadership
really wants to commit i.e. funding, clerical and other assistance to basic laboratory research they should not recruit individuals
who want to do basic research as it is unfair to those individuals.
1 I think it is important to address some national regulatory and Central IRB issues that hinder research such as: easy payment
to subjects, ability to pay VA employees as subjects, and lack of resources at the Central IRB that delay research. We have
also had problem with media services (e.g., getting things printed in a timely manner). I find my area (CCDOR) very well
staffed and fabulous, but run into problems when dealing with areas outside CCDOR and outside research. Travel constraints
are one of the main problems hindering my research career as it makes it difficult to attend professional meetings.
1 The main barrier to my research has been lack of adequate clinical research space (i.e., areas where research patients can be
seen and research interventions with patients can be conducted). This is the main reason for any "less than fully satisfied"
answers regarding the environment for research here.
1 The leaders of the research office are not sufficiently engaged and that needs to change. Other than forwarding e-mails from
central office it is not clear what else they do to support the mission of fostering research. The administrative support is terrible
and the ancillary services (i.e. travel) are fragmented and not user friendly. The IRB is painfully slow and often times lacks the
subject matter expertise to judge many of the research proposals that are sent to them.
1 I would welcome greater cohesiveness and less silos between researchers from different lines of service
Count Response
- 48 -

1 Some other things to consider include: - Allowing researchers the flexibility to work off-site, say 1 day a week, to increase
productivity (e.g., work on publications, catch up on relevant literature) - Working with IT to provide each department (e.g.,
HSR&D) with a designated IT specialist to troubleshoot problems, install software, etc. If there is not enough IT staff to go
around, one compromise may be to have the person designated for say 2 or 3 days a week to a specific department. -
Increasing recruitment of promising investigators and research staff (e.g., research associates, RAs) of different racial/ethnic
backgrounds - Moving IRB Continuing Review dates so that the paperwork is not due 4 months in advance but more like 2
months in advance.
1 Would be great to have online IRB submissions. As a junior person, would be nice to get oriented about resources for research
as well as career-planning about future options/goals.
1 My comments reflect my perception that the Research Office has become inundated with regulatory issues and therefore no
longer provides support for research, but rather, engages in ensuring compliance. I think this shift has been detrimental to the
fundamental mission of research.
1 Research is actually crucial to maintaining an adequate number of clinicians who specialize. The VA will never be able to
compete on salary alone, since in many specialties, one could go to private practice and get 2 or 3 times the salary for a full-
time clinical position. The opportunity for research is unique. If this is lost, then it would be surprising not to struggle in
maintaining an adequate number of specialists. So, the administration needs to make research a priority and can justify it to
maintain clinical specialty services. Along with that, the VA is falling far behind in recruiting translational researchers and
researchers with exerience in genomics. A significant number of specialities have this research at the forefront. The VA is in
danger of falling so far behind, that it will be very difficult to catch up.
1 Some of these questions were difficult to answer, since they were in absolute terms (e.g., "prevent me from doing research",
when maybe "interfere" would be more applicable). Some asked about whether provision of certain resources, which I've
managed to scrounge up on my own, would increase my productivity--they wouldn't, at this point, but certainly could have
previously, and could now for others. I answered questions about Research Office with the IRB, IACUC, and Safety Committee
in mind, but maybe they weren't intended. It would be nice to have free text options here, to provide specifics for some of these
questions.
1 My productivity is greatly hampered by lack of adminstrative and project support. I spend a large portion of my work week
completing tasks that I could delegate to others if there was administrative support (e.g., travel planning) or if I had access to
stable and well-trained project coordinators/research assitants. For example, as project coordinators have to seek new
sources of support before their grant ends, I lost my project coordinator 6 months before the end of the grant. While I was able
to find a replacement, this replacement is untrained and I am essentially doing a lot of project coordination. If I was capable of
increasing the continuity of my staff and had better access to administrative support, then I could be more productive.
Additionally, managing ongoing grants, seeking new funding, and publishing are pressures that are in constant tension. It is
difficult to be successful in all 3.
1 A researcher incubation environment does not exist and one ought to be fostered and developed in order to encourage
"research curious staff". It is possible that some investigators with potential for research, but who are less savvy with the
networking that it takes to be successful are being left behind. It might help if the research office fostered within its ranks
successful basic scientists as role models. Outcomes research is great, but it is over-represented at the Minneapolis VAMC.
At an elemental level, supporting basic science research would be helpful, but developing a programmatic effort to building a
strong basic science research group ought to be the aspiration. Thanks!
Count Response
- 49 -

!
- 50 -

Focus Group Transcripts
- 51 -

Research Focus Group – September 30, 2015
Where should research at the Minneapolis be in 5-10 years?
P1 - Less siloed. More cross-over between different services (HSR&D, CSR&D, RR&D). Collaborative grant submissions
P7 – Challenge with how competitive science is getting. Need to be top of the game to stay in the picture. Devote time and effort to things that really count. Find a way to decrease the administrative burden (BS) to be able to do the science. Too much time doing forms, avoiding trouble, meeting requirements, etc. Less time is left for doing the science. It also detracts from the fun of the work and limits the productivity. Productivity is key to surviving. We have some local control and we tend to outdo what we think is needed. Killing the research enterprise. Sense is that we may be more handicapped by the burden of these things compared to other places.
M – Can you tell one?
P7 – There are so many things at once.
P6 – Institutions like CCDOR have dealt with some of the issues. Centralized some of the regulatory and bookkeeping tasks. Have their own admin team to help with this stuff. Need more time to work on grant writing and less on the other paperwork. Can research office reduce the burden in some way. Solutions have been found for Centers. Can these be generalized.
P2 – Been here one year but still feel new here. Do not know what everyone else is doing. Nice to meet people in this focus group. Having some sort of orientation or other ways of meeting other researchers. We can get equipment fixed! Did not know how to do that. Have resources but they do not work. Lots of money going into things but not far enough to get the research accomplished. Need to have a way for new people to learn about resources available to research. Potential to be really great, but it’s not there. I’m hopeful.
P6 – Agree that orientation for new people would be useful. Don’t know what is expected and typical for what to include in grants, etc. Comments suggest the need for mentoring.
P4 – Similar comment about PDF software. Did not know it was available.
P3 – Part of a multi-site study. Lack of consistency between multiple VA s. Nice that the medical records are electronic. Different things go through different VA s at different speeds. Space it at a premium. Not encouraged to find funding if there is no space to put staff that would be hired. Consent forms could be easier to fill out electronically. IRB does not have Adobe Pro? If they did the consent forms could be easier to use.
- 52 -
How important is it to rebuild the cadre of NIH grant holders? Why? How would you do that?
P4 – How can we make current investigators more competitive for NIH grants. Affiliation with the UMN helps to be competitive.
M – What type of collaboration would be helpful?
P4 – Senior person as UMN that has been helpful in my research
P2 – Core facilities that look very good at the University of Minnesota. Helps to make grants competitive. I work with people at the U and the VA. Hard to get the two systems to work together. VMU here is great and their place is great but they do not speak the same language. Having an initiative to make seamless transition. My lab has VA grant money, but hard to spend this money at core facilities at the University. Should not take a year to use money that you have been awarded to do your work. Not all of the VA’s fault. U also have problems.
P6 – Had money for a contract to use resources at the University. Should not be treated as if we are trying to spend the money somewhere else.
P2 – Had trouble with MRI when it was down. Were doing MRIs to Fairview. Can’t stop the studies when things broke down. Took an incredible amount of time to get that working.
M – Help young investigators submit to NIH. Problems with collaboration at the U.
P7 – Some investigators may have been always funded by VA or other non-NIH grants. Recruiting people that are viable investigators to try and get them to consider trying submitting an NIH grant. VA and NIH grants are all weird in their own way. Hard to figure this all out just from the directions. Need someone who knows. De-mystifying the process would be good. Grease the skids for someone using only non-VA to also try with NIH.
P6 – Mentorship. There are a lot of young investigators who are in mentored awards (K-awards or similar). Some are in less formal mentorship opportunities. Perhaps there are opportunities for those with NIH or those who have been successful to share that knowledge with other investigators. You don’t know what you don’t know. Implement something that make mentorship more formalized. Best way to pass on the information is to have this passed down from successful to junior investigator.
M – What about basic science? Should we work to keep this strong?
P1 – Problems with gaining eligibility to go for CSR&D studies. Need to bring in clinician investigators that can pass eligibility threshold. Lots of things could cross over with fundamental and applied aspects. Conversations have started but did not lead anywhere. Use feedback from Veterans to also drive basic research
P7 – Lab based physician scientist is a dying breed. No one has an interest in doing lab-based research (trainees). Even if we should get people doing basic research, who will do it?
P4 – Little interest in clinicians moving into basic science.
P7 – Physicians would like to partner with people who can do the basic lab work, samples. Not that many people want to learn how to do the lab procedures. Sometimes commercial tests are available. When new techniques are developed, that requires more effort.
- 53 -

P2 – Basic science is still very important. Doing animal research allows for things you cannot do in human subject testing. The investigator is a clinician and I run the lab.
P7 – Does your PI have a lab background such that she did this at one time?
P2 – No. I explain procedures to her that we are doing. She assists with surgeries and also keeps the work clinically relevant.
Why are grant submissions low? What can be done to increase the number of grant submissions?
P4 – Can you have more than one at a time?
P7 – Certain types of grants you cannot. Others you can.
P1 – Rehab R&D only allows for payment of effort on grants. Other grants cover full salary.
M – Assume people want to. What gets in the way?
P3 – I’ve been overwhelmed by other researchers who already have huge data. Where would I put a research team if I could get grants to cover them? Would rather Co-I sometimes unless I knew I could execute the way I want to.
P5 – Too many studies that build off of other studies. New studies start over. Too many PIs and not enough recycling. Get 4 year studies. Would be nice to use large data sets to go forward instead of starting over. We just get going and then have to design or start some other study. Centers feel like they have limited admin resources. Perhaps it is less than what others have. Coming up with bigger teams, bigger groups that can put together larger core group and admin people type projects. Can we pull in more people and put big things together.
M - What could research office do to support this idea?
P5 – Not sure what mechanisms are out there. Need to find the funding mechanisms to shoot for. Admin support is helpful.
P7 – Everything we do has barriers. More questions, more admin burden, blocks us. Easy to say “na” too much effort to do this. Any improvement on all of these issues can increase the chances for going for grants.
How much should the Minneapolis VA support unfunded research? What kind of support should it provide?
P7 – Unfunded research is wonderful. The goal is to generate knowledge. If it can be done with no funding, this is the best! Idea of having high funding with little output being terrible. If people are doing unfunded research and not publishing, that is a problem because they are using resources.
P5 – Seeking clarification about the question. If projects are supported by the research office, they are not actually “unfunded”. Using funding to support the project. Gave examples of LIPs in the CCDOR group.
- 54 -

M – There is a finite amount of support. Some is being used for unfunded research.
P1 – Have a couple unfunded projects that later led to funded projects. The idea is usually to do unfunded research to get pilot data to lead to funded work later. Dangerous to cut out unfunded research entirely.
P3 – Does not need to always use the infrastructure of the research office. There are interesting databases in clinical settings that can be used. Need research time to review, but it is a byproduct of what they are doing clinically. Agree with P7 that these things need to be leading to something (publications, grants, etc).
Why does satisfaction drop off between junior and mid-career?
P2 – Frustration that builds up. From conversations, people are fed up with infrastructure. I am new and have energy to tackle. Maybe later I’ll have a poor attitude if these things do not change. They want us to do our research and be successful, but we do not have the tools. Biggest problems with basic science is the IT situation. We have great equipment (very modern) but require networking and we cannot take the data off of these machines because we cannot put these data on a VA computer to analyze it and publish it.
M - Over time you get beat down by the system.
P2 – Some rules of IT should not apply to research because we do not deal with patients.
P3 – ISO just stopped us from using something that had a slightly different version of some software and the tool does not have any identifiable data. Frozen project until this issue is resolved.
P1 – Actionable thing if we could have an IT liaison who can help get everything done within the regulations. Someone who works with IT to make things happen rather than stops us.
P7 – Changing from “no you can’t” to “let’s figure out how to make this happen”. We are going to move this forward.
P2 – Any time you come into something the first answer is “no”. The first approach is to say “no” rather than help problem solve.
P6 – Attitude of researchers are presented with a problem and find a solution. We are told no and we find a way to get things done. When confronted with research office telling us “no” that is not possible. We want to work with them to get things accomplished. Here is the problem, let’s find a solution to the problem. Lot of incentive to do nothing and not a lot to do something and potentially make a mistake.
- 55 -

ResearchFocusGroup–October1,2015
WhereshouldresearchattheMinneapolisbein5-10years?
P1–Frustrationwiththesystem.It’shardtogetintotheVAgrantsystemevenwithasecondR01.CannotgeteligibilitytoBLR&D.Describesthisasamysteriousbarrier.
P4–NeedmorevisibilityinwhatresearchwehavehereatMinneapolisVA.
P2–AgreeswithP4.Requestsmoreleadership.Wantsleadershiptorecognizeresearch.
P3–Newhereinthelast2years.Doesnotknowwhatotherresearchisgoingon.ResearchDayhelpedbuttookplaceoneyearafterarrivalattheVA.Wantsmoreresearchpresentationsandopportunitiestogettoknoweachother.
P1–VAneedsmoreandbetterpublicity.
P3–VAwebsiteishelpful.
P1–RecommendsbuildingResearchTeams(forexample,P1workswithanimalmodelsandcoulddosoaspartofateam)andapplyingtogetherasteamsforgrants.InP1’spersonalexperience,preliminarydatahasbeenmostpredictiveofsuccess.Suggestssomehowapplyingfororobtainingpoolsofmoneythatcouldbeusedtogetpreliminarydataandthenapplyforlargergrants.Didnotknowhowmuchwouldbeneededorwouldcostforsuccess.
P3-Concernedthatmostmembersofalabarefundedbysoftmoney.MostlyfundedbyVAgrantsandneverhavesecurity.Wantsroomformorenon-VAgrants(difficultyinfundingoffVAandnon-VAgrants).Wouldliketoseeapotofmoneyforbridgingbetweengrants.
HowimportantisittorebuildthecadreofNIHgrantholders?Why?Howwouldyoudothat?
P3–WhynotgettingNIHgrants?Aretheyhardertoget?Arepeoplenotapplying?IstheVAnotappealingfornewresearchers?
P1–GoodforVAtoretainbasicresearch.NIHresearchbuildsbridgewithUMN.MostvibrantresearchiswithNIHdollars.Withoutbasicresearchers,theVAresearchwouldbesmallerinscope.Preventsintellectualisolation.Doesn’tknowhowtogetmoreresearchers.IfrecruitingforresearchthentheVAneedstoshowthatresearcherscanhavesecurityattheVA.ThelackofsecurityhasanegativeimpactonVAresearch.IstheMinneapolisVArecruitingbasicresearchers?
P4–IfIcouldbeeligibleforaVAgrantthingswouldbebetter.RightnowIwouldtellotherresearchersinterestedinworkingattheVAthatthisisaproblemworkingattheVA.
- 56 -

P4–Needscriticalmass.Likeinthe“goodolddays”whentheyhadtechnologysupportandlabmanagers.Thatmadeequipmentworkokay.Researchstaffarenotconnectedtoactualresearch.Equipmentsupportismissing.
Whyaregrantsubmissionslow?Whatcanbedonetoincreasethenumberofgrantsubmissions?P4–PhD’sarestymiedanddependentonotherstokeepyourjob.IcansendinanNIHgrantthatonlysupportsafractionofmysalary.Can’tuseMVMREF.
P1–DroptheeffortrequirementtoapplyforNIH.
P4–VAeligibilityisthecruxofthematter.
P1–5/8effort,isitagamestopper?Ifthatisthecasethemaxthatyoucanaskon3/8NIH.
P3–5/8stillnoteligibleforbenefits–forbenefitseligibilityyouneed75%
P4–Inprecariouspositionbecauseyouaredependentonothers,lackofsupport
P2–Pressureofcontinuousfunding,hardtofindcollaborations,thereisnovisiblenetworkinmentalhealth,betterforthosetrainedinVA,hardfromoutsidetheVA,
P2–Duringthelast2yearsIhavebeenpartofanewresearchteam.Ihavebenefittedfromformingnewcollaborations.Mentalhealthleadershaveincreasedvisibilityofresearchrecently.
P3–Howareothersmakingitwork?Whatareoptions?Whatistheoutlookofsuccessfulpeople?Istheresuchathingastenure?
P1–Mid-careerresearcherslikelyrememberbettertimes.Thingsarealothardernow.
NetworkingwithCentralOffice
P4–DoesnotunderstandwhyPhD’sherearenotgettingVAeligibilityfortheabilitytoapplyforresearchgrants.
P1–WantsVACOtoclarifyexpectationsonhowtogetVAeligibilitytoapplyforgrants.RecommendspushingbackonVACOrulesandgivingfeedbacktoVACOresearchoffice.JustwantsarighttocompeteforVAgrants.
P3–Hadaquestionaboutthesurveyitself–dopeoplefeelthattheycancallVACOdirectly(individualinvestigators)?
P4–RepliedtoP3above–states“donotcallVACO.”HestateshegotintroubleforcallingVACOandthatitisperceivedasinappropriateforaninvestigatortocallVACOresearchofficedirectly.
- 57 -
P3–P3repliedtoP4thatshehadgonetoagrant-writingworkshopandwastoldbyVAR&DstafftocontactVACOresearchofficedirectly,butlocallywastoldnottodoso.
M–Doeschainofcommandhurttheoverallresearchprocess?
P1,3,and4–No.
OpenDiscussion
P1–FeelsthatwehavegoodanimalsupportandagoodIACUC–verygood,infact.IACUCisnotanoppositionalcommittee.BrainScienceCenterinfrastructureworksfastandassistshisresearchinmakingahigherimpact.Thiscenterisoutstanding.
P4–Wantsagoodinfrastructureforbasicscience–ifwehadthatitwouldbe“HUGE!!!”HasheardgoodthingsaboutCCDORandGRECC.Feelsverymuchthatbasicresearchisnotsupported.FeelsthatVAshouldfundpositionswith“hard”moneylikeothercentershave.ThereisnosuchthingasaVA-funded(hardmoney)labmanagerthatcanhandlemanytasks.Ifso,itwouldbe“worthitsweightingold.”
P3–IRBisphenomenal.Getsimmediatefeedbackandcan’tsayenoughabouttheIRBthatispositive.(NotesthattheJesseBrownVAIRBreliedonpaper,snailmail,andhadroutinedelaysof1-2months).
P1–Researchofficeishelpful.
P2-IRBhasimprovedoverthelast8years.
Again:Whyaregrantsubmissionslow?Whatcanbedonetoincreasethenumberofgrantsubmissions?P4–Grant-writingisahugetimecommitment.Thistakesawayfromgettingpapersdone.
P1–Duringgrant-writing,shutsdowneverythingelse.Inaperpetualchasefordollars.Notesthatresearchersarediscouragedandgivingupinthelargerresearchworld.Competitionforgrantdollarshashitanextremelevel.
P3–Sendinggrantsallthetime.Feelslikeotherworkisnotgettingdone.Difficultfindingbalance.
M–Whatcantheresearchofficedo?
P4–Coordination.AttheU,thereisbettercoordinationforgrantsubmissions.AttheVA,thePIisonhis/herown.RecommendsonepersonwhoseentirejobfocusisguidingaPIthroughthegrantsubmissionprocess.
- 58 -

P1–Agrantcoordinatorisreallyimportant.
P1–Seedmoneywouldstimulateteam-building.Alsotheofficecoulddomatch-making.RecommendfacilitatingpairingVA-ineligiblePhD’switheligiblePI’s.HadaquestionastowhethertheCo-Investigatormechanismwasaroutetoeligibility.Goodteamsarebetterthangoodindividuals.
P4–Recommendsagrantcoordinatorwithinsight.
P1–Hasnotedthatmulti-PIoptionsaredoingbetterwithobtainingNIHgrants.
P2–TheResearchOfficeneedstoadvocateforPI’s.Recentlyhadan18-monthcontractdisputeaffectresearch.ThiswasacontractwiththeUthatwasahorribleandunfriendlyprocess.Alsorecentlytriedtohireanewemployeeinaprocessthattook9monthsfrompositiondescriptiontohire.
P1–ContractswiththeUofMarehard.RecommendsstreamliningalinkwiththeU.RecommendsspecificpeopleattheVAwhoworkoncontractswiththeU.
P4–ContractingattheVISNlevelresultedinahangupwithanimalcareintherecentpastrequiring18monthstoresolve.
- 59 -

Interview Transcripts
- 60 -

VA Research Strategic Planning Committee Dr. Michael Levitt Interview Interviewers: Adabag, Segal October 20, 2015 1. What do you see when you look out on the research program at the Minneapolis VA? (Prompts: What do you think is going well? What do you think could improve?)
CCDOR is doing well. Dr. Bloomfield is doing a good job. Morale is up in the Research Office. Laboratory research is having problems, played out over 28 years, where at the outset “every internist had a lab.” The number of funded PhDs has declined and most have retired out. Decline in available funding may have set off a cycle in which there has been decline in interest and now very few trainees. It is not clear that the problems are local to Minneapolis as VA’s around the country are closing lab space. There may not be room for improvement in this situation.
2. What would you like the Minneapolis VA research program to look like in 5 to 10
years?
“I would love it if there were internists doing funded lab research,” generating their own data. CSRD/ HSRD-type research is that which will need to be mined but “not my thing.” CCDOR is excellent, especially its organization in moving from research question to methods, statistics, grant-writing, etc., but this may not apply to laboratory research.
3. How important is it to you and the Minneapolis VA that we have a top-ranked research
program? Why? (Prompt: Name several VAs ranking higher and lower in research funding.) Prestige of the research program was Dr. Levitt’s job as ACOS for Research.
4. What are the considerations for recruiting and sustaining researchers at the
Minneapolis VA?
Effective leadership, for example at the Division Chief level, is important in making the case and mobilizing resources for recruiting and sustaining new investigators. CCDOR support has been crucial in some recent examples. It is not clear whether geography is a limiting factor. It is not clear whether researchers who might be recruited are being trained any more effectively elsewhere.
- 61 -
5. Are there practical ways in which the Minneapolis VA can provide more support for research? (Prompt: How have you worked to advance research at the Minneapolis VA?)
“Support CCDOR.” For laboratory research, financial support has not been limiting. During Dr. Levitt’s tenure, Medical Center leadership supported research in many important ways.
6. In your opinion, is research leadership at the Minneapolis VA well networked
nationally? Is this important and, if so, why?
Dr. Levitt doesn’t know whether being well networked makes a difference. He did not feel himself to be well networked.
7. How does leadership consider research in assessing performance of the service
lines?
“I have no idea.” 8. Research capacity varies greatly among service lines. Is this an issue that needs to
be addressed? What do you think could be done to address it?
“I don’t think that there’s a problem.”
- 62 -

VA Research Strategic Planning Committee Dr. Kristin Nichol Interview Interviewers: Hansen, Klein October 27, 2015 1. What do you see when you look out on the research program at the Minneapolis VA? (Prompts: What do you think is going well? What do you think could improve?)
Research in VA in Medicine is going well. Engaged faculty, more established faculty, new hires with skills for research. Different PSLs have different strengths. Would like to see growth across areas. PSLs could bring on more faculty and grow research. Institution has a problem supporting young faculty, bridging faculty. Streamlining regulatory procedures would be desirable. Need to be creative about ways to support research.
2. What would you like the Minneapolis VA research program to look like in 5 to 10
years?
Would like to see at least 50% of providers and lots of PhDs asking scholarly questions and many getting funded for research. Would like to see more providers engaged in scholarship. See more people getting funded and would like to see the support they need for success.
3. How important is it to you and the Minneapolis VA that we have a top-ranked research
program? Why? (Prompt: Name several VAs ranking higher and lower in research funding.) Don’t care about “top-ranked”, but should be a successful program. How many people have time/resources to do research is more important.
4. What are the considerations for recruiting and sustaining researchers at the
Minneapolis VA?
Making sure people have skills, credentials, support, experience, and funding opportunities. Could be more structured for support of young faculty. Small grants should be used to jump start junior faculty, start-up packages. Time-explicit tracks for clinic/research positions. Time is currency.
5. Are there practical ways in which the Minneapolis VA can provide more support for
research? (Prompt: How have you worked to advance research at the Minneapolis VA?)
Looking at new recruits. Time. Repurpose medical care funds to support continuous improvement that can also support research. Exploring opportunities to pay for training –
- 63 -
tuition support for clinical research certificates. Provide support for faculty here. Streamline the regulatory burden (research service). Challenge on basic science side. Can research service help pay for basic science training? Sabbatical options – paid salary to learn new skills – medical center covers 6 months salary, Central Office cover the other six months.
6. In your opinion, is research leadership at the Minneapolis VA well networked
nationally? Is this important and, if so, why?
Really important. We are well connected within the VA (Drs. Bloomfield and Fu). Some investigators are well connected in other areas (e.g. NIH). Important to advocate for our programs.
7. How does leadership consider research in assessing performance of the service
lines?
Chief of Staff is supportive of the education mission. Research doesn’t factor into evaluations in any significant way. Not big on bean counting. Should not have strict criteria for assessment, but needs to be assessed. Leadership here values research. It is a big component for medicine.
8. Research capacity varies greatly among service lines. Is this an issue that needs to
be addressed? What do you think could be done to address it?
Different SLs have different roles to play. Medicine should be most active in the research role. Hard for surgeons, for example. A model for some disciplines would be hiring PhD scientists to help drive the research with clinician input. All PSLs should know they have a mission for research. Variable but should try to grow. PSL leadership should care about research. Expectations of having faculty in research.
Last statement: Institution needs to provide resources to support the clinical enterprise to give more time for research.
- 64 -

VA Research Strategic Planning Committee Mr. Patrick Kelly Interview Interviewers: Adabag, Hansen October 29, 2015 1. What do you see when you look out on the research program at the Minneapolis VA? (Prompts: What do you think is going well? What do you think could improve?)
I’m proud of the research program. Great research findings contribute to good standing of the VA. Pleased to talk about research here. There were some compliance issues early on when I started to work here. I’m pleased that there are very few compliance issues now. Oversight of human and animal subjects is strong. I’m pleased where we have brought the program. The research program helps us to bring good people to our center. I think it is important to ask how research we are doing relates to Veteran’s health. Need to know how bench research will lead to practical effects – how will this make a different in the lives of Veterans. VA is a place for both basic science and applied science. Important to make sure it is improving our knowledge and that we are getting bang for our buck.
2. What would you like the Minneapolis VA research program to look like in 5 to 10
years?
Our foundation (MVMREF) is not as strong as it could be. Could assist new investigators with start-up funding. MVMREF could be better at getting people started. Research building could potentially draw things together. I hope our program grows. Would like to see GRECC do more education and outreach to smaller sites.
3. How important is it to you and the Minneapolis VA that we have a top-ranked research
program? Why? (Prompt: Name several VAs ranking higher and lower in research funding.) Would like for us to be on par with our peers. Great clinical staff and potential to do more. If we could secure more grants, we could grow the research. Like it when staff have opportunities for research.
4. What are the considerations for recruiting and sustaining researchers at the
Minneapolis VA?
We try to bring in people with career development awards. Aggressive at bringing people in and protecting their time for research. We can give administrative support. Could be a good resource provided by the foundation. Try to raise more money in the foundation.
5. Are there practical ways in which the Minneapolis VA can provide more support for
research?
- 65 -

(Prompt: How have you worked to advance research at the Minneapolis VA?)
Dr. Bloomfield requested more support staff and we have provided that support. These activities may identify further needs for research. Funding has been OK. Things can be done through the medical center. We are willing to respond to needs of research service. VISN 23 has no research presence. Research money passes through the VISN level. Could talk to VISN about support for research.
6. In your opinion, is research leadership at the Minneapolis VA well networked
nationally? Is this important and, if so, why?
We have a lot of investigators that are plugged in. Dr. Nichol and Dr. Crossley are well connected and are working with Dr. Bloomfield to get more connected with Central Office.
7. How does leadership consider research in assessing performance of the service
lines?
Probably not much. Most is centered around clinical work and day-to-day work. WE started featuring researchers during executive leadership meetings. Research Day is a great event. No research components in evaluations. We should consider these in the future, particularly for those with protected time for research.
8. Research capacity varies greatly among service lines. Is this an issue that needs to
be addressed? What do you think could be done to address it?
Should be driven by interest. We should support those with interest in research. We should also carve out areas of strength. Support the staff that want to be involved in research. Last comments – Research should be part of evaluations for those with protected time. We need to invest resources where we are getting return on our investments.
- 66 -

VA Research Strategic Planning Committee Dr. Hanna Bloomfield Interview Interviewers: Chrouser, Klein November 10, 2015 1. What do you see when you look out on the research program at the Minneapolis VA? (Prompts: What do you think is going well? What do you think could improve?)
Dr. Bloomfield sees a vibrant program. It could grow more. It could be more collaborative both within the VA and with the University. We could leverage more funding from the University. We are in the top 15 VAs but we could be higher. Growing means more VERA dollars, which weigh VA more than non-VA funding.
Dr. Bloomfield sees her role as to grow VA and NIH grant funding. She currently does not have a good sense of the productivity of investigators at the VA or of what that productivity ought to be.
2. What would you like the Minneapolis VA research program to look like in 5 to 10 years?
A goal is to be in the top 10 VA's rather than the top 15 in terms of funding. A goal is that we have a less paper-based system for oversight.
Dr. Bloomfield wants more physical space for clinical research. There's currently unused physical space at the VA. There are 4 wings with 10,000 ft.² each and each has extra space. Renovation for clinical research space is already being planned. This fiscal year is the design phase and next fiscal year will be a remodel. Her hope for clinical research in 5 to 10 years is that once there's physical space available staffing could be developed for these clinical research units.
Dr. Bloomfield’s view of basic science research at the VA in the next 5 to 10 years is that there would be 3 to 5 (or maybe even 5-10) strong well-funded groups studying different topics such as obesity, cancer or hepatology. She does not envision "service lines" which link basic and clinical research by topic areas – at least in her short-term agenda.
3. How important is it to you and the Minneapolis VA that we have a top-ranked research program? Why? (Prompt: Name several VAs ranking higher and lower in research funding.)
A top-ranked research program attracts outstanding clinicians. It creates positive press. It's important "because it's my job."
Dr. Bloomfield aspires to be like the San Francisco VA because they administer their own NIH grants and get the indirect funds. She also admires the Boston VA where they were able to get the freestanding research building for their MRI projects and are now
- 67 -

collaborating broadly with both Boston University and Harvard. She does not see a stand-alone research building at the Minneapolis VA as a top current priority.
4. What are the considerations for recruiting and sustaining researchers at the Minneapolis VA? Research doesn't recruit. It’s Dr. Bloomfield’s job to encourage Dr. Crossley to allow clinical searches that encourage academic types to apply, who are interested in research. They have put together a one million-dollar fund with 500 K from the VA and 500 K from the University (left over from old studies) that can be used for recruitment purposes. The funding is under control of the Chief of Staff. In terms of bridge funding it tends to be rarely needed and when it is needed it is usually for PhD's or the staff of successful PI’s who happen to be in between grants. Currently she is the one responsible for these decisions but thinks it might be better if it were done by committee. There's no recruitment of basic science faculty to the VA. They come through their mentor’s funding stream. PhD's have eligibility criteria which is set by Central Office and to a certain extent it discourages non-MDs from doing research at the VA. There is no plan to change this policy. Dr. Bloomfield feels that this policy keeps the focus on clinically relevant topics.
5. Are there practical ways in which the Minneapolis VA can provide more support for research? (Prompt: How have you worked to advance research at the Minneapolis VA?) Dr. Bloomfield is interested in what others have to say about this question. A less paper- based system could help. There could also be help in other ways – for example to provide some data analysis services, for VA national data. CCDOR already does some of their own data analysis and she would like to provide this for non-CCDOR investigators.
6. In your opinion, is research leadership at the Minneapolis VA well networked
nationally? Is this important and, if so, why?
Yes, there is a great ACOS listserv. Dr. Bloomfield knows a lot of people who know the system well. She finds it's especially important to know what is going on elsewhere, especially when meeting with local non-research leadership because they want to know what other VAs are doing.
7. How does leadership consider research in assessing performance of the service lines? It all comes down to how much protected time that you give people. The criteria for
- 68 -

maintaining protected time is likely a combination of grants and papers although there are not formal metrics for that.
There is an Academic Excellence Council which is designed to support and represent the research and educational missions of the VA. Their latest accomplishment is to get the VA to agree to pay for research training for clinicians (certificate in clinical research) from medical care funds.
8. Research capacity varies greatly among service lines. Is this an issue that needs to be addressed? What do you think could be done to address it? Yes. The Chief of Staff wants each service line to have a research presence. The answer to what that looks like will be different for each service line. Dr Santilli is talking about developing more infrastructure to encourage surgical research. Rehab research is growing due to the presence of biomedical engineers.
Parting Thoughts: Dr. Bloomfield will try to get more VISN support for research, once VISN leadership is sorted out. Sometimes a VISN will give money to a medical center to support human resources for research. She is going to go to the VISN and pitch options to them, including Dr. Hansen’s Rehab work, etc.
- 69 -

VA Research Strategic Planning Committee Dr. Kent Crossley Interview Interviewers: Adabag, Wendt December 2, 2015 1. What do you see when you look out on the research program at the Minneapolis VA? (Prompts: What do you think is going well? What do you think could improve?)
The majority of research is within the Department of Medicine. It could improve in other areas. There is not a lot of research activity in Lab Medicine. There is an effort in Imaging to attract an investigator. Biomechanics have done some research but could do more. Research is spotty in Surgery. I would like to appoint a Vice Chair of Research in Surgery. MVMREF is not working well. We are looking for a new director. There is no active fundraising. No funds are available to be contributed for start-up funds. There is not much activity in education, compared to the San Francisco VA Foundation. The Research Service is doing well. Hanna has done a good job. Dr. Crossley is not hearing complaints regarding research. The informal mentoring program is working well.
2. What would you like the Minneapolis VA research program to look like in 5 to 10
years?
I would like to see a larger program with more extramural funding covering a broader array of specialties, e.g. surgical specialties. I’d like to see more skilled investigators hired. I would like the MVMREF to take a bigger role in fundraising and develop robust connections within the community and within the medical school. It is challenging to recruit community members for the foundation. People with serious interest in Veterans’ issues are necessary. In the eyes of national VA leadership, research takes a back seat to clinical care. In general, they see that it is more important to hire physicians to do the work but less important that they do research. However, in Minneapolis it is different. Mr. Kelly is generally supportive of research. Dr. Crossley thinks that it is more important to hire physician-scientists to maintain a high standing and for physician contentment and retention. Ties with the University are extremely important. We are different than other VAs in that we have very few shared positions. Dr. Crossley views that as a major problem. The medical school recently reviewed the possibility of shared positions (e.g. 80/20) and decided that it isn’t feasible. Q: How can we make the ties with UMN stronger if we cannot have shared positions? We need to replicate the model that Dr. Georgopoulos started by creating a center with some investigators based at the U and some at the VA. i.e. 2 centers meshed. For example, the open position for chief of GRECC could be a hire that has research synergistic for both the U and the VA, e.g. the UMN’s emphasis is on aging and metabolism. There are challenges in this hire. A recent candidate met this requirement, but he was not an acting clinician so VA central would not approve the hire.
- 70 -

3. How important is it to you and the Minneapolis VA that we have a top-ranked research
program? Why? (Prompt: Name several VAs ranking higher and lower in research funding.)
We are currently no. 18 in research. It’s very important that we are in the top 10. Q: How would we get there? We need to hire more investigators. We need to identify more money for start-ups and possibly interim funding. Q: Can we get there if we don’t have shared positions with the U? Yes. We have some 80/20 positions such as Kris Chrouser and Dr. Ramaswamy. We can do that. There are ways to have closer ties without work division.
4. What are the considerations for recruiting and sustaining researchers at the
Minneapolis VA?
Sustaining investigators is person-dependent. Mr. Kelly is supportive of research and education. Q: What about increasing clinical work? People don’t come to me and say that we don’t have enough time for research. Our goal for new hires is to identify start-up funds, assign a mentor and give appropriate time for research for 2-3 years. After the 2-3 years of support we expect the investigator to be independent in funding. Recently we were able to identify some ‘leftover’ money in MVMREF for start-up funds. There is no identified ongoing source for start-up funds. Q: How about lapses in grants? Time can be allocated for research in the absence of funding for some after the initial 2-3 years if there is promise of future funding. This is decided on an individual basis by the Section and Service Line Chief. It is a problem for non-MD investigators since there salaries are all based on external funding. For non-MD investigators with lapses in funding, the Research Service (i.e. Hannah Bloomfield) can possibly supply gap funds. Ideally in this situation the foundation would help. Q: Any resources outside the Foundation? The VISN? There is no current mechanism in VISN 23. Iowa City and perhaps the Omaha VA might be interested in working with us to approach VISN leadership regarding research support. VISN leadership is in a flux right now. Currently, VISN support is person-dependent.
5. Are there practical ways in which the Minneapolis VA can provide more support for
research? (Prompt: How have you worked to advance research at the Minneapolis VA?)
- 71 -

The infrastructure needs improvement. Mental Health Service has put together a good support infrastructure. Support is low outside Mental Health. It is service-specific. Hanna has hired Tom Rector to support investigators. We need more grant-writing support. The University has a grant-writing program with high success rate. Anne Joseph is leading it.
6. In your opinion, is research leadership at the Minneapolis VA well networked
nationally? Is this important and, if so, why?
Yes, we are well connected. Hanna is very persuasive. 7. How does leadership consider research in assessing performance of the service
lines?
This is not well defined or well done. Research success is not part of the performance evaluation.
8. Research capacity varies greatly among service lines. Is this an issue that needs to
be addressed? What do you think could be done to address it?
See previous responses.
- 72 -

Supplementary Data
- 73 -

VA Research Strategic Planning Committee Bibiometric Analysis December 11, 2015
Notes 1. Bibliometric indexes were determined for VA investigators identified by RDIS expenditures
in 2014. 2. Bibliometric indexes were determined using Harzing’s Publish or Perish. 3. For each investigator, the h-index “h” is defined as the number of published papers “h” that
have been cited at least “h” times. 4. The hc-index, or contemporary h-index, is a modified h-index that gives weight to recent
citations. 5. The g-index is a modified h-index that gives weight to highly cited publications. 6. Graphs to the left are frequency distributions of bibliometric indexes for VA investigators. 7. Graphs to the right are box-and-whisker plots for bibliometric indexes across Research
Units.
!
20
40
60
80
100
120
140
160
180
200
h-in
dex
20
40
60
80
100
120
140
160
180
200
g-in
dex
Basic Brain CCDOR GRECC Medicine Mental Other Rehab Research Sciences Health
20
40
60
80
100
120
140
160
180
200
hc-in
dex
10
20
30
0 20 40 60 80 100 120 140 160 180 200
No. I
nves
tigat
ors h-index
10
20
30
0 20 40 60 80 100 120 140 160 180 200
g-index
10
20
30
hc-index
- 74 -

VA Research Strategic Planning Comm
ittee Supplem
entary Data M
ay 11, 2015
2 4 6 8 10 12
Millions of DollarsR
DIS Expenditures, 2010, 2012, 2014
Other Sources
NIH
VA
!!!!!!!!!!!!!!!!!!!!!!!!! Notes: 1. Source data are from
file “RDIS Expenditures – Investigator”, last modified by M
argaret Bordanea on May 5, 2015.
2. “Other Units” = Adm
inistration, Dermatology, Neurology, Pharm
acy, Radiation Oncology, Surgery.
3. “Other Sources” = O
ther Federal, Academic, Corporate, Volunteer Agency.
4. Expenditures are assigned once and, in cases of dual appointment, subjectively. In general, the hierarchy is: Basic
Research = Brain Sciences = CCDOR = Rehab > G
RECC > Medicine = M
ental Health = Other Units.
5. A significant percentage of expenditures, particularly NIH-funded, relate to off-site projects at the University.
Basic Research
Brain Sciences
CCDOR
GRECC
Medicine
Mental
Health O
ther Rehab
- 75 -

Minneapolis VA M
edical Center Funding, RDIS Expenditures 2014
Cod
e Fu
nd
ing
Sou
rce P
ct Total
D
epartment of V
eterans Affairs (V
ACO
)
9003 M
erit Review
(CC 103)
4.9 1,321,287
9022 Rehabilitation R
&D
(Prog 822) 7.9
2,120,303 9024
Health S
ervices R&
D (Prog 824)
15.8 4,242,738
9025 Cooperative S
tudies (Prog 825) 4
1,065,654 9050
Clinical S
cience R&
D
5.5 1,480,441
TO
TAL D
epartment of V
eterans Affairs (V
ACO
) 38.2
10,230,423
National Institutes of H
ealth (NIH
)
9103 N
ational Cancer Institute
1.6 418,319
9107 N
ational Heart, Lung &
Blood Inst
14.9 3,985,029
9109 N
atl Inst of Allergy &
Infectious Dis
1 276,147
9113 N
atl Inst of Dental and C
raniofacial Research
1 274,644
9115 N
atl Inst of Diabetes, D
igest. & K
idney 5.1
1,363,623 9121
Natl Inst of N
eurological Disor &
Stroke
1.9 519,319
9125 N
ational Institute on Aging
4.4 1,185,755
9129 N
atl Inst on Arth, M
usculo & S
kin Dis
0.6 168,435
9133 N
atl Inst on Drug A
buse 1.8
473,269 9135
Natl Inst on M
ental Health
0.5 145,240
9138 N
atl Inst of Biom
edical Imaging and B
ioengineering 0.5
124,079 9143
Natl Inst of H
ealth (Inst not known)
1.4 371,446
TO
TAL N
ational Institutes of Health (N
IH)
34.8 9,305,305
O
ther U.S
. Federal Agency
9203
Dept of D
efense 1.3
335,275 9209
Dept of H
ealth & H
uman S
ervices 2
524,468 9227
National S
cience Foundation 0.1
36,499 9299
Other Federal G
overnment A
gency 3.1
840,558
TOTA
L Other U
.S. Federal A
gency 6.5
1,736,800
- 76 -

Academ
ic Institution, Donor, or G
overnment
9301
Affiliated U
niversity 1.3
359,483 9360
VA M
edical Care S
upported Mgm
t. Studies
8.3 2,224,142
TO
TAL Academ
ic Institution, Donor, or G
overnment
9.6 2,583,625
Private Proprietary C
ompany
9710
Am
gen 0.3
74,523 9731
Eli Lilly 0
13,255 9738
Glaxo
3.7 987,553
9742 H
offman-La R
oche 0
4,550 9760
Merck &
Co.
0.3 80,124
9765 N
ovartis 0.5
125,716 9778
Roche
0 11,665
9787 Sanofi-A
ventis 0
11,665 9798
Zeneca
0.1 23,330
9799 O
ther Private Proprietary Com
pany 3
790,327
TOTA
L Private Proprietary Com
pany 7.9
2,122,708
Voluntary A
gency or Foundation
9805 Am
erican Cancer S
ociety 0
8,745 9871
National K
idney Foundation 0.1
23,652 9879
Paralyzed Veterans of A
merica
0.3 81,782
9895 Va Private R
esearch Corporation
0.1 31,501
9899 O
ther Voluntary A
gency\Foundation 2.4
649,347
TOTA
L Voluntary Agency or Foundation
3 795,027
TO
TAL EX
PEND
ITURE
100 26,773,888
- 77 -

Departm
ent of Veterans Affairs (VAC
O),
10,230,423 (38%)
National Institutes of
Health (N
IH), 9,305,305
(35%)
Other U
.S. Federal Agency, 1,736,800
(6%)
Academic Institution,
Donor, or G
overnment,
2,583,625 (10%
)
Private Proprietary C
ompany,
2,122,708 (8%
)
Voluntary Agency or Foundation, 795,027
(3%)
- 78 -

Research Workload 2009 2010 2011 2012 2013 2014
Investigators (VA Funded) 48 45 61 43 67 75
Research Proj-ects 550 522 635 653 511
Merit Reviews 47 51 56 46 92
VA Cooperative Studies 14 10 15 16 22 17
Rese
arch
Education Affiliations 2009 2010 2011 2012 2013 2014Agreements 171 193 280 234 253 235
Trainees 617 600 589 593 596 594
Medical / Surgical Residents 519
653 505 503 533 529
Medical Students 319 300 278 327 395 398
Uni
que
Pa
tient
s by
Era
Educ
atio
n
8
Age
and
Gen
der
World War IIUnknownPre-Korean War
Post-Korean War
Vietnam Era
Post Vietnam
OEF/OIF/ONDDesert Storm
Korean War
Other (Peacetime)
Minneapolis VA: Vital Statistics
<25
25-34
35-44
45-54
55-64
65-74
75-84
85+
1179
6706
4847
8951
21321
28793
16103
8738
Female, 6,203
Male, 90,410
Population Age Gender
Male, 90,410
Female - 6,203
World War II - 7,233
Pre-Korean War - 345
Korean War - 10,901
Post-Korean War - 5,704
Vietnam Era - 43,355
Post-Vietnam - 7,950
OEF/OIF/OND Desert Storm - 16,049
Other (Peacetime) - 3,030
Unknown - 2,072
Post-Korean War
Vietnam Era
Post Vietnam
OEF/OIF/ONDDesert Storm
Korean War
- 79 -

Inpatients 2009 2010 2011 2012 2013 2014
Operating Beds 199 199 199 199 199 199
Average Daily Census 126 134 133 137 138 135
% Occupancy 63.2% 67.2% 66.8% 69.1% 69.3% 67.6%
Average Length of Stay (days) 5.96 6.30 6.22 6.29 5.98 5.91
Discharges 7697 7747 7801 8035 8431 8353
Community Living Center (CLC) Operating Beds 88 88 88 80 88 88
Average Daily Census 58.24 62 55 64 70 63
% Occupancy 66.2% 63.6% 62.5% 80.0% 79.5% 71.8%
Average Length of Stay (days) 30.8 34.1 29.7 28.7 31.2 31.5
Discharges 691 663 675 821 815 744
Outpatient Visits 2009 2010 2011 2012 2013 2014
Minneapolis VA Medical Center 603,169 609,653 638,426 673,903 700,968 702,787Chippewa Valley WI 9,883 10,284 10,680 12,008 13,456 14,744Hibbing 7,182 7,863 7,055 6,124 9,257 14,754South Central (Mankato and St. James) 5,523 6,588 7,572 11,573 14,727 14,138Maplewood 9,272 9,412 10,462 10,522 10,538 15,963Rochester 9,676 11,341 11,530 12,680 13,044 13,977Twin Ports (Superior WI) 32,287 33,734 32,983 31,430 29,958 40,259Hayward and Rice Lake WI 8,834 10,358 10,872 10,918 12,718 13,698Northwest Metro 0 0 0 18,487 28,952 32,916Shakopee (opened 2014) 2,180Albert Lea (opened 2014) 2,765
Total 685,826 699,233 729,580 787,645 833,618 868,111
Unique Patients 2009 2010 2011 2012 2013 2014
Minneapolis VA Health Care System 82,481 86,254 89,768 91,807 93,073 96,489Chippewa Valley WI 3,403 3,446 3,648 3,938 4,059 4,267Hibbing 3,035 3,197 3,154 3,015 3,458 3,552South Central (Mankato, St. James) 1,705 1,781 2,472 3,169 3,673 3,747Maplewood 2,778 3,182 3,656 3,654 3,861 5,198Rochester 3,024 3,473 3,680 3,889 4,129 4,318Twin Ports (Superior WI) 5,672 5,891 6,096 6,291 6,371 7,434Hayward and Rice Lake WI 2,303 2,700 2,889 2,936 3,527 3,361Northwest Metro 7,443 7,753
Shakopee (opened 2014) 1,110
Albert lea (opened 2014) 1,146Total 84,936 89,087 92,361 94,594 96,638 100,777 99
Minneapolis VA: Vital Statistics
- 80 -