endourology and other urologic ancillary procedures department of urosurgery
DESCRIPTION
ENDOUROLOGY AND OTHER UROLOGIC ANCILLARY PROCEDURES Department of Urosurgery. Dellosa, Miguel LeeChuy, Katherine Lee, Sidney Albert Legaspi, Roberto Jose Lerma, Daniel Joseph Li, Henry Winston Jerry Santos, MD Facilitator. Percutaneous Endourology. - PowerPoint PPT PresentationTRANSCRIPT

Dellosa, MiguelLeeChuy, Katherine
Lee, Sidney AlbertLegaspi, Roberto JoseLerma, Daniel Joseph
Li, Henry Winston
Jerry Santos, MDFacilitator
The use of closed procedures via needle and guidewire access to visualize and manipulate the kidneys and upper urinary tract.
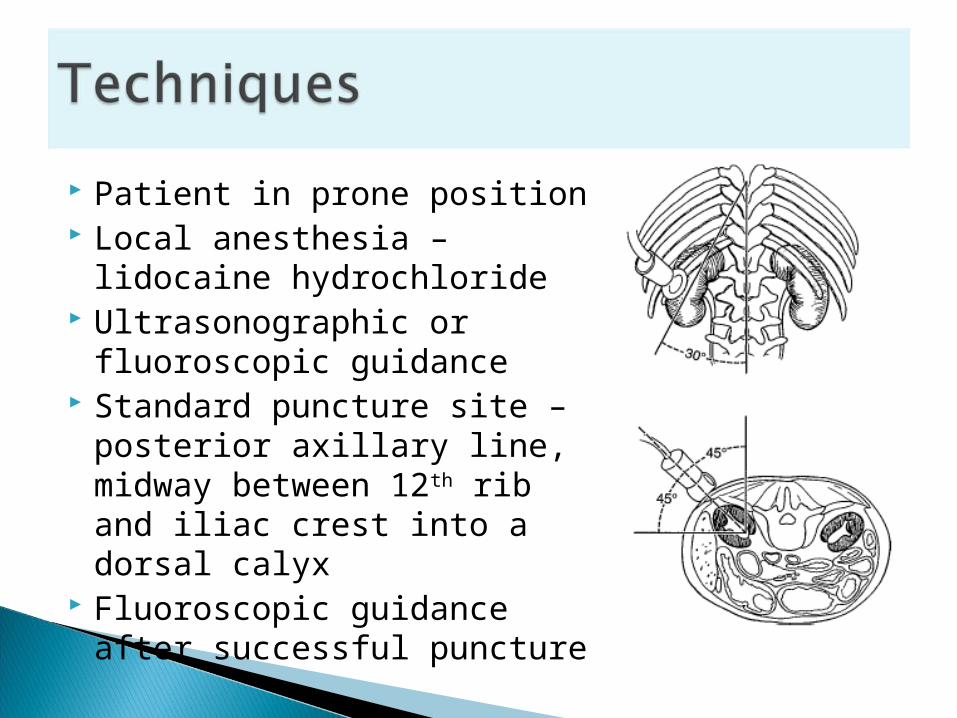
Patient in prone position Local anesthesia – lidocaine
hydrochloride Ultrasonographic or
fluoroscopic guidance Standard puncture site –
posterior axillary line, midway between 12th rib and iliac crest into a dorsal calyx
Fluoroscopic guidance after successful puncture
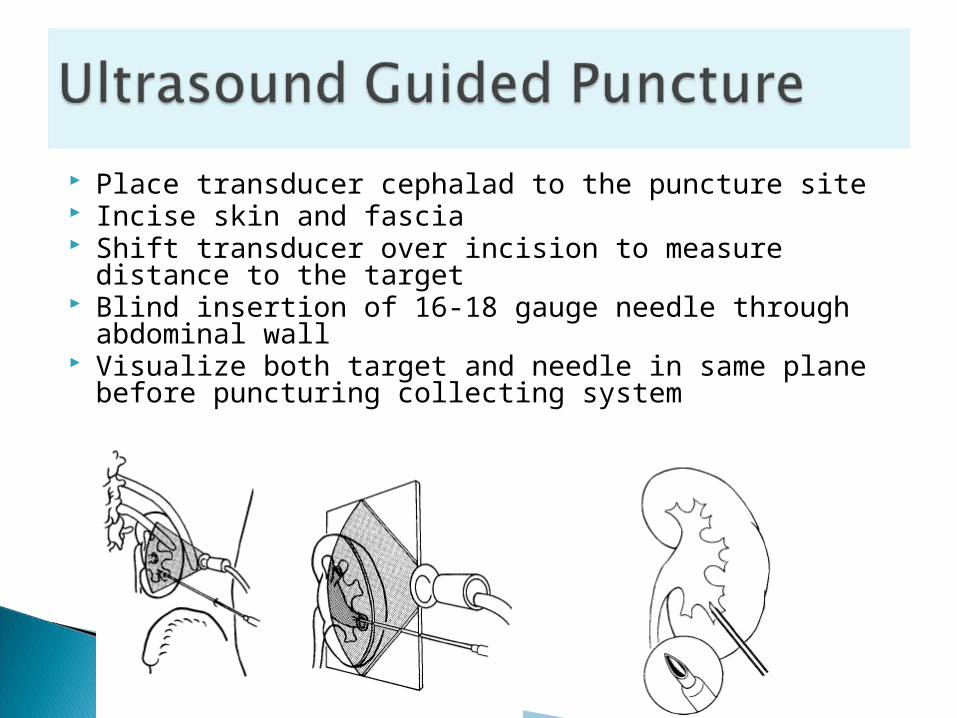
Place transducer cephalad to the puncture site Incise skin and fascia Shift transducer over incision to measure distance to the
target Blind insertion of 16-18 gauge needle through abdominal
wall Visualize both target and needle in same plane before
puncturing collecting system
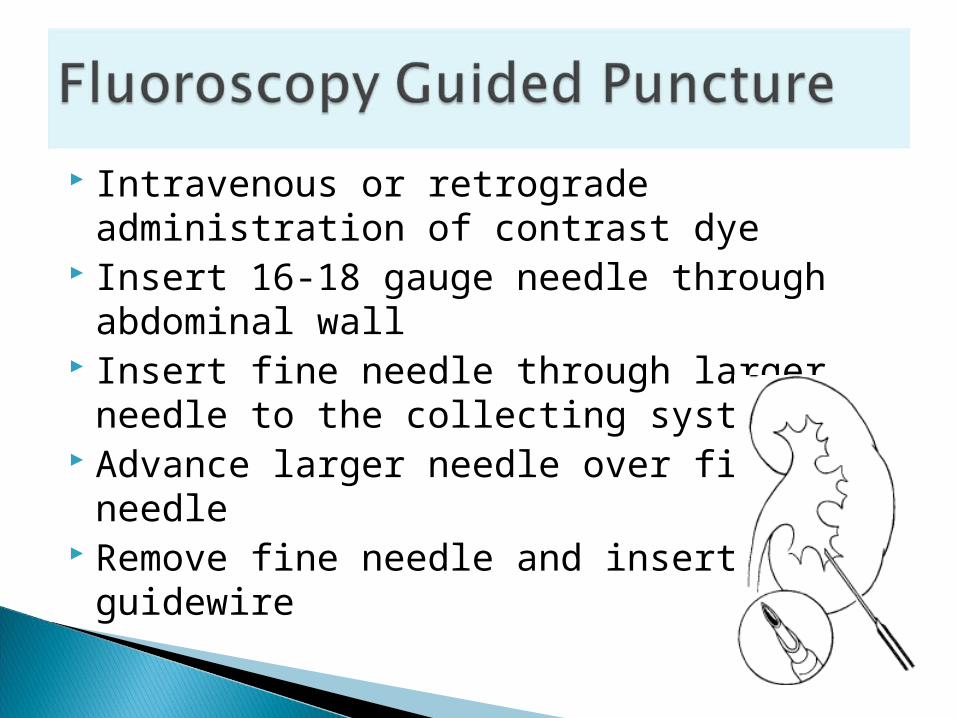
Intravenous or retrograde administration of contrast dye
Insert 16-18 gauge needle through abdominal wall
Insert fine needle through larger needle to the collecting system
Advance larger needle over fine needle Remove fine needle and insert guidewire
Diagnostic Antegrade pyelography Pressure/perfusion study (Whitaker test)Therapeutic Nephrostomy catheter drainage Antegrade ureteral stenting Dilation of ureteral strictures Perfusion chemolysis of renal stones Percutaneous nephrolithotomy Percutaneous resection and coagulation of
urothelial tumors
Blood clotting anomalies
Obtaining radiograph after antegrade injection of contrast dye (20-30% diluted)
Simultaneously done with Whitaker’s test

Assess pyeloureteral resistance by differentiating an obstructed from non-obstructed dilated system
Simultaneous measurements of intrapelvic and intravesical pressures during antegrade perfusion at 5, 10, 15, and 20mL/min flow rates via a manometer
Differential pressure = renal pelvic – bladder pressure◦ Flow rate 10mL/min: normal < 13 cmH2O; mild
obstruction 14-22 cmH2O; moderate to severe obstruction > 22 cmH2O
◦ Flow rate 15mL/min: normal < 18 cmH2O◦ Flow rate 20mL/min: normal < 21 cmH2O

Drainage and decompression of upper urinary tract if retrograde ureteral catheterization cannot be done
Insertion of guidewire, dilator, then nephrostomy catheter
Can do antegrade ureteral stenting and balloon dilation through catheter
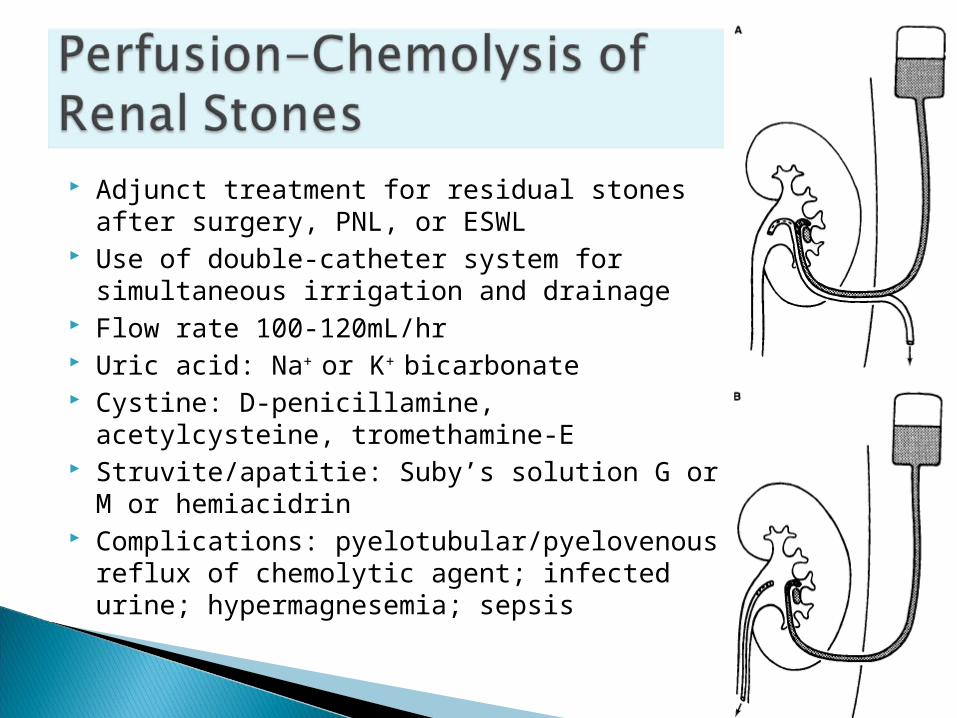
Adjunct treatment for residual stones after surgery, PNL, or ESWL
Use of double-catheter system for simultaneous irrigation and drainage
Flow rate 100-120mL/hr Uric acid: Na+ or K+ bicarbonate Cystine: D-penicillamine, acetylcysteine,
tromethamine-E Struvite/apatitie: Suby’s solution G or M or
hemiacidrin
Complications: pyelotubular/pyelovenous reflux of chemolytic agent; infected urine; hypermagnesemia; sepsis

Endoscopic Intrarenal Endoscopic Intrarenal InstrumentationInstrumentation Nephroscopes – endoscopic instruments,
15-26F sheaths, inserted percutaneously◦ Standard rigid instruments available in sizes 24-
26F, have telescopes with offset eyepieces Smaller working channel allows insertion of
flexible intruments Instrumentation through flexile
nephroscopes is limited by size and flexibility of working instruments
NephroscopyNephroscopy Rarely indicated for diagnostic purpose Mostly performed for percutaneous
lithotripsy ESWL has gradually replaced PNL for renal
stone treatment PNL used in:
◦ Urinary obstruction not caused by stone itself◦ Large volume stones◦ Stones that cannot be positioned within SW focus

Renal StonesRenal Stones PNL is limited to specific stone diseases Large stones must be disintegrated using
mechanical, ultrasonic, electrohydraulic, or laser energy
For soft stones - continuous disintegration and evacuation of fragments
Hard stones – broken up into largest possible fragments that can be extracted
Ureteropelvic StenosisUreteropelvic Stenosis Direct-vision internal incision (pyelolysis,
endopyelotomy, endopyeloplasty)◦ Offers advantage of an incision under direct vision
Renal Pelvis TumorRenal Pelvis Tumor Electroresection, electrocoagulation,
electrovaporization, neodymium:YAG laser coagulation
Percutaneous management may be an alternative to nephroureterectomy for patients with grade I disease, and for palliative tratment
Percutaneous Aspiration & Percutaneous Aspiration & BiopsyBiopsy Usually perfomed for diagnostic purposes In combination with therapeutic intentions Ultrasound and CT are imaging techniques
of choice
Renal CystsRenal Cysts Indications of diagnostic puncture of cystic
lesion:◦ Irregular, thick wall, internal echoes on ultrasound
exam◦ Density numbers on CT higher than serous fluid◦ Hematuria
Indications of puncture for therapy:◦ Cyst causes compression
Renal BiopsyRenal Biopsy Performed percutaneously or open surgery Bleeding is expected due to vascularity of
parenchyma Open surgical biopsy rather than
percutaneous biopsy is indicated in patients with solitary kidneys or uncontrolled hypertension


• The normal kidneys are bean-shaped• Located between the upper border of T11
and lower border of L3• The right kidney lies approximately 2 cm
lower than the left.• The normal range of renal length in adults is
11 to 15 cm.• The increased radiolucency of the fat makes
the outline of the kidney standout from the soft tissues


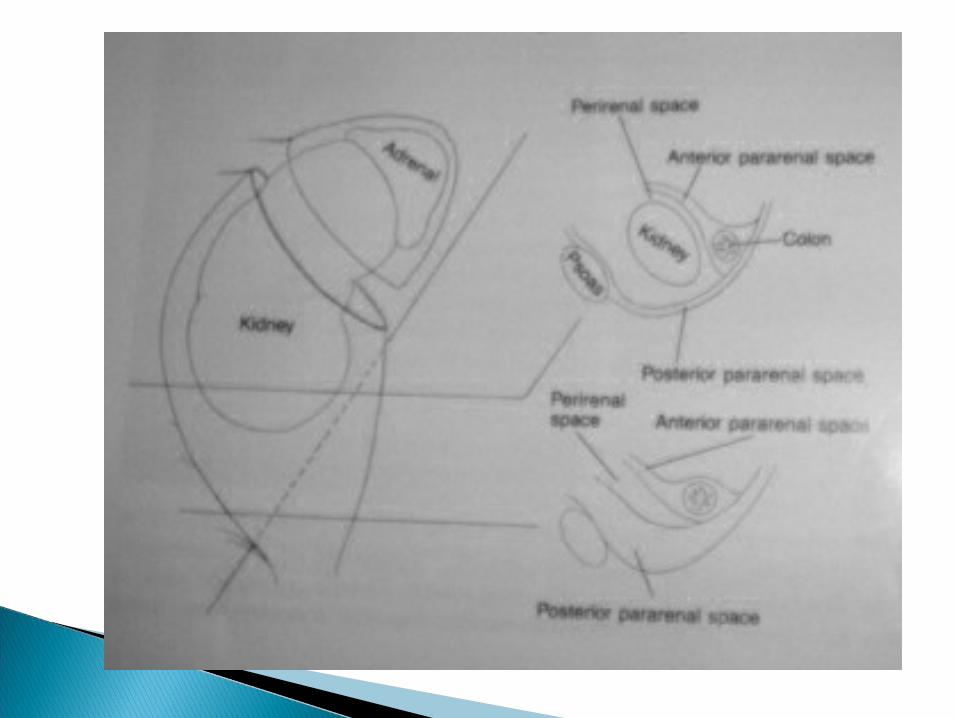
• The kidneys are contained within the renal capsule and surrounded perirenal fat, which is enclosed within Gerota’s fascia.
• There are 3 anatomic spaces around each kidney:
1. Perirenal2. Anterior pararenal3. Posterior pararenal

Left Kidney
Anterior Layer of the renal fascia
Posterior Layer of the renal fascia
Fibrous capsule of the kidney
Perirenal fat

The leaves of the Gerota’s fascia fuse superiorly, medially and laterally, enclosing the kidney, adrenal gland, renal vasculature and emerging portion of the proximal ureter.
In theory fluid collections are more likely to collect in spaces between tissue planes rather than in the perirenal and pararenal spaces.

The ureters cannot be defined on plain KUB film however radioopaque calculi may be detected along the course of the ureter.

3 areas of normal narrowinga. Ureteropelvic junctionb. Ureterovesical junctionc. Bifurcation of the iliac vessels
These are sites where calculi often lodge in the course of passage

The shadow of the urinary bladder can often be identified.
The urinary bladder is a muscular hollow viscus which lies in the pelvis but balloons upward when distended.
The psoas muscle shadows are usually well outlined.
Assymmetry or other abnormalities are noted.
In perirenal abscess, the psoas muscle shadow is enlarged and its margin is indistinct adjacent to the area of infection.
Psoas abscess may displace the kidney and ureter


Vesical calculi can be outlined. Vascular calcifications, including phleboliths
and arterial plaques are frequently seen.


• Assessment of GUT requiring IV injection of contrast to visualize renal collecting systems, ureters and UB
• Indications:– Urinary stones– Neoplasia– Urinary inflammations– Urinary trauma and obstruction– Miscellaneous: congenital anomalies, GUT fistula
formation, patent urachus, etc.

◦ NPO◦ Bowel cleansing◦ Some cases: adequate hydration (MM, IDDM and
renal failure)


Contrast material◦ Organic iodides: radiopacity depends on its iodine
content◦ 2 types:
Ionic Non-ionic: lower osmolality
Advantages: less toxicity and less reactions Disadvantage: more expensive
◦ Mechanism of exretion: Almost entirely by glomerular filtration little or no
tubular resorption

• hypersensitivity to contrast• combined hepatic and renal disease• oliguria• serum creatinine >2.5-3.0 mg/dl• IDD with renal insufficiency (serum crea > 1.5
mg/dl)• Multiple myeloma• Hx of severe allergy• Use of metformin (within previous 48hrs)• ++ value of INFORMATION obtained must be
weighed against the risk
◦Adverse contrast reactions Minor: urticaria, sweating , nausea, vomiting
Major: laryngeal edema, hypotension, bradycardia, shock, seizure, anaphylactoid rxn, such as cardio-respi arrest

-minimally invasive procedure that requires cystoscopy and the placement of catheters in the ureters
-radiopaque contrast medium is introduced into the ureters or renal collecting structures through the ureteral catheters, and radiographs of the abdomen are taken.

Retrograde Urogram
INDICATIONS: a.)excretory urograms or CT urogram
(CTU) are unsatisfactoryb.) history of adverse reaction to
intravenouscontrast media

Nephrogram• Diffuse opacification of the renal parenchyma• Reflects the ability of proximal tubules to reabsorb
water and concentrate the contrast • Visualize renal outline
Pyelogram• Visualization of the pelvocalyceal complex and ureters• Contrast has reached the collecting tubules and
excretory passages• Information on architecture and function of kidney
Cystogram-Visualization of the lower part of ureters and
UB
• Visualization of the UB wherein a urethral catheter is inserted and the UB is filled with contrast
usually instilled via a transurethral catheter, but when necessary can be administered via percutaneous suprapubic bladder puncture

suspected UB rupture in trauma patients suspected UB tumors diverticula calculi

imaged radiographically by retrograde injection of radiopaque fluid or in antegrade fashion with voiding cystourethrography, or with voiding following EU.
antegrade technique is required when lesions of the posterior urethra, for example, posterior urethral valves, are suspected.
retrograde technique is more useful for examining the anterior (penile) urethra

A wave frequency of 1 cycle/s (cps) is called a hertz (Hz). Sound frequencies greater than 20 kHz are beyond the range of human hearing and are called ultrasound.
Medical sonography uses ultrasound to produce images. The frequencies commonly used in medical sonography are between 3.5and 15 MHz.

Ultrasound images are reflection images formed when part of the sound that was emitted by the transducer bounces back from tissue interfaces to the transducer.
A more sensitive method of detecting flow, called power mode Doppler, is available on modern equipment. This technique displays the integrated power of the Doppler signal rather than the mean Doppler frequency shift

Sonography of the kidney. Upper: Normalkidney. Renal cortex (C), normal renal sinus echoes(S). Middle: Moderate hydronephrosis and hydroureter;dilated renal pelvis (P). Dilated proximal ureter (proxure). Lower: Severe hydronephrosis of the transplantedkidney, compound sagittal scans, dilated clubbed calices(C), dilated renal pelvis (P).
Ultrasound is commonly used for the evaluation of the kidney, urinary bladder, prostate, testis, and penis.
Assessment of renal size and growth.
Triaging patients with renal failure, e.g. small echogenic kidneys suggest renal parenchymal(medical) disease, whereas a dilated pelvocaliceal system indicates an obstructive, and potentially reversible, cause of renal failure. Useful in detection and characterization of renal masses. It provides an effective method of distinguishing benign cortical cysts from potentially malignant solid renal lesions.
Ultrasound may also be used to follow up mildly complicated cysts detected on CT, e.g. hyperdense cysts or cysts with thin septations.
The differential diagnosis for echogenic renal masses includes renal stones, angiomyolipomas, renal cortical neoplasms (including carcinoma), and, less commonly,abscesses and hematomas.
All echogenic renal masses should be correlated with clinical history and, if necessary, confirmed with another imaging modality or follow-up ultrasound.
Echogenic lesions smaller than 1 cm are more difficult to characterize by CT owing
to partial volume averaging; in the correct clinical setting, follow-up ultrasound rather than repeat CT may be more useful.
Doppler sonography is useful for the evaluation of renal vessels, vascularity of renal masses, and complications following renal transplant. It can detect renal vein thrombosis, renal artery stenosis, and ureteral obstruction prior to the development of hydronephrosis, arteriovenous fistulas, and pseudoaneurysms.

Perinephric fluid collections following renal transplantation, extracorporeal shockwave lithotripsy, or acute obstructions are reliably detected by ultrasound.
Developments in other imaging modalities have decreased the use of ultrasound in several clinical scenarios.
Most patients with suspected renovascular hypertension are evaluated with CTA or MRA rather than Doppler sonography

ease of use, High patient tolerance noninvasiveness lack of ionizing radiation low relative cost wide availability. include a relatively low signal-to-noise level,
tissue nonspecificity, limited field of view, and dependence

relatively low signal-to-noise level tissue nonspecificity, limited field of view Dependence on the operator’s skill and the
patient’s habitus.




Acute flank pain Hematuria Renal infection
(search for abscess) Renal trauma Staging renal
neoplasm Solid or cystic mass

Contrast scans◦ IV iodinated contrast media◦ Anatomy and pathology
Noncontrast scans◦ Renal or perirenal calcification◦ Hemorrhage◦ Urine extravasation
• Contrast media • rapid intravenous bolus for assessment of renal anatomy
or measurement of aortorenal transit time. • Using a bolus injection and rapid sequence scanning,
renal arterial opacification is followed immediately by enhancement of the cortex.
• Nephrogram phase with medullary enhancement is reached within 60 seconds.
• Excretion of contrast material into the collecting structures can be expected within 2–3 minutes after initiation of contrast administration.
Detect ureteral tumors◦ Tumor staging and evaluation of the cause and
level of obstruction. intravenous contrast is the preferred imaging modality
• Helical CT without oral or intravenous contrast is the preferred imaging modality for patients with renal colic or suspected urolithiasis

Primarily in staging bladder tumors Bladder rupture following trauma Increased sensitivity in bladder filled with
dilute contrast medium (CT cystography)
Prostatic CT◦ Lymphadenopathy◦ Prostatic abscessess
Testis◦ Undescended testis◦ Testicular tumors◦ Nodal distant metastases

Wide field of view, Detect subtle differences in the x-ray
attenuation properties of various tissues, good spatial resolution, anatomical cross-sectional images, and operator independence.
Reformatted planes in 3D

Limitations to the transaxial plane for direct imaging
Tissue nonspecificity Low soft-tissue contrast resolution, Need for contrast media (both oral and
intravenous). Radiation exposure


Clinical Applications:• Congenital anomalies
• Diagnosis of renal vein thrombosis
• Diagnosis and staging of renal cell carcinoma

MR angiography◦ renal transplant vessels◦ renal vein tumor thrombosis◦ renal artery stenosis
Gadolinium
◦ obstruction (renal artery stenosis)

T1-weighted conventional spin-echo image -Higher signal intensity cortex (C) -lower signal intensity medulla (M)-Left renal vein (arrow) -Inferior vena cava (I)

LEFT- large renal cell carcinoma (T) arising from the inferior pole of the right kidney
RIGHT- Coronal image of a large renal cell carcinoma (T) replacing almost entire parenchyma of the left kidney (K). Superior displacement of the pancreas (arrows).

Gadolinium-enhanced renal magnetic resonance angiography
LEFT- renal arteries are normal
RIGHT- atrophic left kidney with an occluded left renal artery
severely stenotic right renal artery
Advantages-Direct imaging in any plane desired-Choice of large or small field of view- Excellent soft-tissue contrast- No exposure to ionizing radiation- Less operator dependence
Disadvantages◦ scanning time is relatively slow

Absolute contraindications◦ intracranial aneurysm clips◦ intraorbital metal fragments◦ any electrically,magnetically, or mechanically
activated implants Eg. Cardiac pacemakers, biostimulators,
neurostimulators, cochlear implants, and hearing aids

Most useful in:
Evaluation renal masses in pxs with contraindication to IV contrast
Contrast enhanced CT has been inadequate for diagnosis and staging
Detection renal vascular disorder
• ++appearance of specific structures varies with the IMAGING SEQUENCE

Endoscopic Intrarenal Endoscopic Intrarenal InstrumentationInstrumentation Nephroscopes – endoscopic instruments,
15-26F sheaths, inserted percutaneously◦ Standard rigid instruments available in sizes 24-
26F, have telescopes with offset eyepieces Smaller working channel allows insertion of
flexible intruments Instrumentation through flexile
nephroscopes is limited by size and flexibility of working instruments
NephroscopyNephroscopy Rarely indicated for diagnostic purpose Mostly performed for percutaneous
lithotripsy ESWL has gradually replaced PNL for renal
stone treatment PNL used in:
◦ Urinary obstruction not caused by stone itself◦ Large volume stones◦ Stones that cannot be positioned within SW focus

Renal StonesRenal Stones PNL is limited to specific stone diseases Large stones must be disintegrated using
mechanical, ultrasonic, electrohydraulic, or laser energy
For soft stones - continuous disintegration and evacuation of fragments
Hard stones – broken up into largest possible fragments that can be extracted
Ureteropelvic StenosisUreteropelvic Stenosis Direct-vision internal incision (pyelolysis,
endopyelotomy, endopyeloplasty)◦ Offers advantage of an incision under direct vision

Renal Pelvis TumorRenal Pelvis Tumor Electroresection, electrocoagulation,
electrovaporization, neodymium:YAG laser coagulation
Percutaneous management may be an alternative to nephroureterectomy for patients with grade I disease, and for palliative tratment
Percutaneous Aspiration & Percutaneous Aspiration & BiopsyBiopsy Usually perfomed for diagnostic purposes In combination with therapeutic intentions Ultrasound and CT are imaging techniques
of choice

Renal CystsRenal Cysts Indications of diagnostic puncture of cystic
lesion:◦ Irregular, thick wall, internal echoes on ultrasound
exam◦ Density numbers on CT higher than serous fluid◦ Hematuria
Indications of puncture for therapy:◦ Cyst causes compression

Renal BiopsyRenal Biopsy Performed percutaneously or open surgery Bleeding is expected due to vascularity of
parenchyma Open surgical biopsy rather than
percutaneous biopsy is indicated in patients with solitary kidneys or uncontrolled hypertension

THANK YOU FOR LISTENING!
HAVE A NICE DAY