endoscopy – should everyone be tested?
DESCRIPTION
TRANSCRIPT

Endoscopy – Should Everyone Be Tested?
Primary Care Management
of Dyspepsia Symposium
Roland Valori
Consultant Gastroenterologist
Gloucestershire Royal Hospital
December 2003

What will be covered
· Specific issues
· Health economics of endoscopy

Specific issues
· Iron deficiency
· Positive coeliac serology
· B12 deficiency
· Age threshold for endoscopy
· Barrett’s oesophagus
· Gastric ulcer

Iron deficiencyselecting patients for endoscopy
· All males
· All non-menstruating females
· Selected menstruating females:– positive coeliac serology– GI symptoms– Family history– ? older patient

Positive coeliac serology
· Need for duodenal biopsy depends on– type of serology available– degree of suspicion of coeliac

Duodenal biopsy and coeliac serologywhen to endoscope
Degree of suspicion of coeliac
high medium low
Anti-gliadin+ yes yes yes
- yes +/- no
Anti-endomysial
+ yes yes yes
- yes no no
TT-Glutaminase
+ yes yes +/-
- +/- no no

B12 deficiency
· Always do– intrinsic factor antibodies– coeliac serology
· Follow rules for coeliac serology
· Barium follow through– if there are GI symptoms

· “The challenge for GPs is to maximise detection of serious and treatable disease while minimising cost and adverse effects of investigation”
Logan and Delaney, BMJ 2001;323:695-7

Number of significant symptoms attime of diagnosis
0
2
4
6
8
10
12
14
0 1 2 3
No of Patients =
25Wt loss
14Dysphagia
8Anaemia
7GI Bleed
3Previous surgery
3Mass
3Perforation
1Cerebral mets
1
No of Symptoms
No ofPatients
Christie et al, Gut 1997;41:513-7
The threshold should be 55the evidence
· Christie et al, Gut 1997;41:513-7
· Gillen et al, Am J Gastroenterol 1999;94:75-9
· Effective Health Care bulletin 2000: Volume 6
· Two-week wait rule for upper GI cancer– http://www.doh.gov.uk/cancer
· Draft NICE guidelines 2003
Barrett’s oesophagus
· Two issues– surveillance endoscopy of Barrett's to
identify early cancer– screening patients with GORD to identify
Barrett's suitable for surveillance

BSG Barrett’s oesophagus guidelines
“it is recommended that endoscopic surveillance every 2-3 years should be considered in patients with endoscopically visible CLO, particularly those fit enough to undergo oesophagectomy should HGD or carcinoma be detected”
Draft guidance

BSG Barrett’s oesophagus guidelines
· Surveillance recommendation is based on case series evidence
· Cost-effectiveness is highly sensitive to annual incidence of carcinoma in Barrett's– >1% not too expensive– 0.5-1.0% £62,000/QALY– <0.5% prohibitively expensive
incidence 0.26-0.4%: BMJ 2003; 326:892-4

Endoscopy and bowel cancer
· Using endoscopy as part of a screening strategy, mortality from bowel cancer can be reduced by 15%
endoscopy can prevent bowel cancer

Effect of FOBT screening on incidence of colorectal cancer
New cases of CRC
Odds ratio Confidence interval
control 507
annual screening
417 0.80 0.70 – 0.90
biennial screening
435 0.83 0.73 – 0.94
NEJM 2000;343:1603-07

Bowel cancer screening
· In November 2002 Alan Milburn announced that there would be a bowel cancer screening programme
– £1300 – 2500/QALY– £23 – 42 million/year

Bowel cancer screening· Endoscopic workload expressed as procedures
or sessions per year per million population:
Screening method
FOBT FS
flexible sigmoidoscopy
0 6000
colonoscopy (at steady state)
1500 450
‘endoscopy sessions’
300 690
10%increase
20%increase
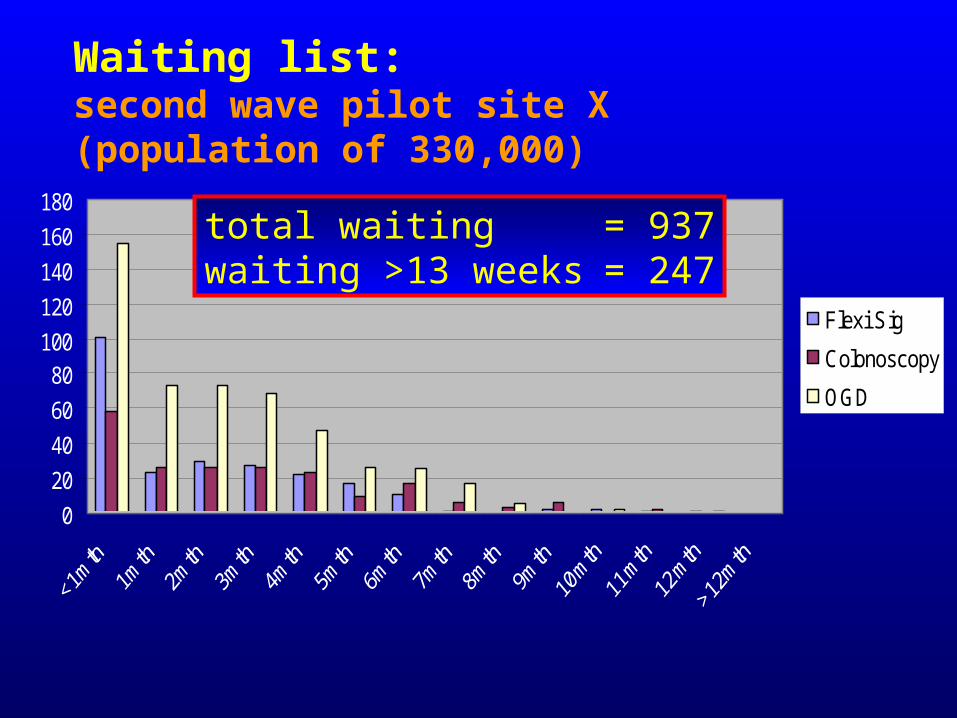
Waiting list: second wave pilot site X (population of 330,000)
0
20
40
60
80100
120
140
160
180
Flexi Sig
Colonoscopy
OGD
total waiting = 937waiting >13 weeks = 247

Implementing screening
· Not until the symptomatic service is ‘sorted’:– modernisation of endoscopy services– more and better trained endoscopists– quality assurance process
@

Modernisation
· Is all about– getting it right for the patient– using capacity efficiently– controlling demand using cost/benefit
evidence– resourcing the demand capacity gap
properly

Modernisation
· Is all about– getting it right for the patient– using capacity efficiently– controlling demand using cost/benefit
evidence– resourcing the demand capacity gap
properly

Annual open access endoscopy referral rate for West Gloucestershire GP practices (1996-7)
0
2
4
6
8
10
12
14
16
18
20
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23
Endoscopy referrals per 1000 patients per year
Practices
(Intervention arm of serology RCT)
2x
4x0.65%/year
1x

Endoscopic findings in a random adult population
· Sweden
· Random sample invited for OGD*
· 1001/1363 accepted
· Age range 20-81
· Mean age 53.5
· 51.3% women
* Independent of symptomsAro P et al, DDW 2002

Endoscopic diagnosisStroud (344) Sweden (1001) Forest of Dean (391)
0
10
20
30
40
50
60
Normal HH O'it is CLO GU DU Ga Ca
StroudSwedenFOD
Waldon, Aro and Wilkinson
Stroud and FOD - symptom-based selectionSwedish study - random selection
Problems with nihilistic approach· Dealing with people· Dealing with GPs who are dealing with
people· Endoscoping influences behaviour, it may
lead to:– reduced worry– fewer symptoms– reduced consultation– reduced medication use

Alternative strategies to manage dyspepsia
· Early endoscopy
· Empirical treatment
· Test and treat
· Test and ‘scope

Alternative strategies to manage dyspepsia
· Early endoscopy
· Empirical treatment
· Test and treat
· Test and ‘scope
Choices
Health economics

Choices(decisions)
Efficacy
Cost
Resource
Beliefs
Willingness to pay
Perspectives

Cost
Efficacy
LOSER
WINNER
x

Cost £
EfficacyPatient
Sx-free at 12/12
BMJ 2002;324:1012-6
T/T vs treat
Endo vs treat>50
T/T vs Endo
Endo vs treat<50
x
x

Conclusions
· Do not ignore iron deficiency

Conclusions
· Beware of Barrett's propaganda– surveillance can do harm as well as good– we do not know the balance of good and
harm– cost-effectiveness depends on the
incidence of cancer in the population surveyed
• Whatever, it is hugely expensive compared with other interventions

Conclusions
· Early endoscopy for patients with dyspepsia aged >55– it appears to be ‘cost-effective’– cancer is much more likely to be found

Conclusions
· For younger patients:– if typical reflux symptoms treat empirically– if non-specific dyspepsia test for Hp and
treat– endoscope if
• patient or doctor has concerns about cancer• patient needs to take regular NSAIDs

Conclusions
· If you want to save the life of a patient with dyspepsia arrange a flexible sigmoidoscopy

Hp and reflux disease
· The net effect is to reduce the number of subjects with milder GORD symptoms, but to increase the (smaller) number with more severe symptoms
Richard Harvey, DDW/SWGG 2002