encyclopedia of cognitive behavior therapy || anger control problems
TRANSCRIPT

Anger Control Problems
as visual imagery and metaphors to assist with the restructur-ing of irrational beliefs or dysfunctional schemas associatedwith anger. Social skills interventions would benefit from thedevelopment of more systematic approaches to modulatingnonverbal and paralinguistic behaviors in individuals withanger problems.
Finally, advances in cognitive neuroscience are con-tributing to the development of a better understanding of therole of biological factors in a variety of behavioral disorders,including anger problems. These advances neither mandatethe use of pharmacological interventions nor preclude theuse of cognitive–behavioral therapy. However, they do indi-cate that some people with anger problems may benefit frompharmacological interventions. Cognitive–behavioral thera-pists have developed treatment protocols that are designedto facilitate compliance with pharmacological interventionand/or the termination of pharmacological intervention inmood disorders and anxiety disorders. Cognitive–behavioraltherapists interested in anger disorders would do well to alsoinnovate in this area.
See also: Adolescent aggression and anger management, Angercontrol problems, Anger management therapy with adolescents,Disruptive anger
REFERENCES
American Psychiatric Association. (1994). Diagnostic and statistical manual of mental disorders (4th ed.). Washington, DC: Author.
Awalt, R. M., Reilly, P. M., & Shopshire, M. S. (1997). The angry patient:An intervention for managing anger in substance abuse treatment.Journal of Psychoactive Drugs, 29, 353–358.
Deffenbacher, J. L. (1999). Cognitive–behavioral conceptualization andtreatment of anger. Journal of Clinical Psychology, 55, 295–309.
Deffenbacher, J. L., Filetti, L. B., Lynch, R. S., Dahlen, E. R., & Oetting, E.R. (2002). Cognitive–behavioral treatment of high anger drivers.Behaviour Research and Therapy, 40, 895–910.
Deffenbacher, J. L., Oetting, E. R., & DiGiuseppe, R. A. (2002). Principlesof empirically supported interventions applied to anger management.Counseling Psychologist, 30, 262–280.
Eckhardt, C. I., & Deffenbacher, J. L. (1995). Diagnosis of anger disorders.In H. Kassinove (Ed.), Anger disorders (pp. 27–47). Bristol, PA:Taylor & Francis.
Fava, M., & Rosenbaum, J. F. (1999). Anger attacks in patients with depression. Journal of Clinical Psychiatry, 60, 21–24.
Grodnitzky, G. R., & Tafrate, R. C. (2000). Imaginal exposure for angerreduction in adult outpatients: A pilot study. Journal of BehaviourTherapy and Experimental Psychiatry, 31, 259–279.
Haaga, D. A. (1999). Treating options for depression and anger. Cognitiveand Behavioral Practice, 6, 289–292.
Novaco, R. W., & Chemtob, C. M. (1998). Anger and trauma:Conceptualization, assessment and treatment. In V. M. Follette & J. I. Ruzek (Eds.), Cognitive–behavioral therapies for trauma.New York: Guilford Press.
World Health Organization. (2002). Composite International DiagnosticInterview reference and training manual. Geneva: Author.
RECOMMENDED READINGS
Cognitive Behavioral Case Conference section of Cognitive and BehavioralPractice, 6, 271–292.
Deffenbacher, J. L. (1999). Cognitive–behavioral conceptualization andtreatment of anger. Journal of Clinical Psychology, 55, 295–309.
Anger Control Problems
Donald MeichenbaumKeywords: anger, exposure-based therapies, self-instructional train-ing, self-monitoring procedures, stress inoculation training
Anger-control problems are an often-overlooked disorderand they have received limited attention in the treatment literature. An examination of the American PsychiatricAssociation DSM-IV reveals nine diagnostic categories forAnxiety Disorders and ten diagnostic categories ofDepressive Disorders, but only three diagnostic categoriesfor anger-related problems, namely, Intermittent ExplosiveDisorders, and two Adjustment Disorders with Conduct-Disorder features. The dearth of research on anger is furtherhighlighted by DiGiuseppe and Tafrate (2001) who notedthat for every article on anger over the past 15 years, thereare ten articles in the area of depression and seven articles inthe area of anxiety. The absence of research activity onanger is somewhat surprising given that anger-relatedbehaviors are one of the most common psychiatric symp-toms that cut across some 19 different psychiatric condi-tions. Anger, hostility, and accompanying violence are oftencomorbid with other disorders. For example, veterans withPTSD have been found to be at increased risk for domesticabuse with as many as one-third of combat veterans withPTSD having assaulted their partners in the past year.Vietnam veterans with PTSD are six times more likely toabuse drugs compared to Vietnam veterans without PTSD,with anger being a significant relapse cue for substanceabuse. PTSD, substance abuse, mood disorders, anger, andaccompanying hostility and aggression go hand in hand andprovide clinicians with major challenges.
Besides the challenge of comorbidity, Novaco (1996)has highlighted several additional challenges to the treat-ment of patients with anger and aggressive behaviors. Thesechallenges include:
1. Angry patients may become angry during therapyand direct their aggression toward their therapist.
23

Anger Control Problems
2. Angry patients need to be continually reassessed forthe risk of violence toward themselves and towardothers (according to the Tarasoff decision).
3. Angry patients are often resistant to treatment,highly impatient, easily frustrated, and unrealistic in their treatment goals and, moreover, are oftennoncompliant with treatment.
As DiGiuseppe and Tafrate (2001) observe, “angryclients do not come for therapy; they come for supervision” onhow to fix people in their lives (bosses, co-workers, partners,children) whom they have failed to change or they come tovent on how unfairly and disrespectfully they have beentreated.
Finally, the need for effective treatment approaches foraggressive behavior has been underscored by Slep andO’Leary (2001) who reported that in the United States eachyear 1.6 million women are severely assaulted by their part-ners and over 900,000 children are maltreated. In 6% of allU.S. households, partner and child physical abuse co-occurin families. The need is urgent and the question is: what dotherapists have to offer to effectively treat individuals withangry and aggressive behaviors?
COGNITIVE–BEHAVIORAL TREATMENT (CBT)
Five meta-analytic reviews of anger treatment haveappeared that have examined the relative efficacy of CBTwith adults, adolescents, and children (Beck & Fernandez,1998; Bowman-Edmondson & Cohen-Conger, 1996;DiGiuseppe & Tafrate, 2001; Sukhodolsky & Kassinove,1997). The populations treated included college studentsselected for high anger, aggressive drivers, angry outpa-tients, batterers, prison inmates, students with learning dis-abilities, individuals with developmental delays, and peoplewith medical problems such as hypertension and Type Apersonalities. The results of the meta-analyses indicate that“the anger treatments seem to work equally for all agegroups and all types of populations and are equally effectivefor men and women. … The average effect sizes across alloutcome measures ranged from .67 to .99, with a mean of.70” (DiGiuseppe & Tafrate, 2001, p. 263).
The results of these meta-analyses revealed that CBTfor anger reduction was moderately successful. Patients inCBT were better off than 76% of control untreated patients,and 83% of the CBT patients improved in comparison totheir pretest scores. This level of improvement was main-tained at a follow-up period that ranged from 2 to 64 weeks.
While these initial results are encouraging, the effectsizes for CBT of anxiety disorders have been found to bearound 1.00 and for depression it has reached 2.00.
Meichenbaum (2001) has reviewed the intervention litera-ture on spouse abusers and provides a cautionary note that25% to 50% of men who batter who attend treatment programs repeat their violence during the period from 6 months to 2 years following treatment. While a review ofthe literature on intimate partner violence is beyond thescope of this brief article, there is increasing evidence thatfurther development of effective treatments for aggressivebehavior is required. The research by Holtzworth-Munroe(2000) is most promising, as she has identified different pat-terns of aggressive behavior (family-only versus generalizedaggression versus aggression that accompanies comorbiddisorders). Given the complexity and altered developmentalpatterns of aggressive behaviors (childhood onset versusadolescent onset) and the important role of gender differ-ences, differential treatments of angry and aggressive behaviors are indicated (Reid, Patterson, & Snyder, 2002).Even with these caveats in mind, the initial results of cogni-tive–behavioral interventions with angry and aggressiveindividuals are encouraging.
THE NATURE OF COGNITIVE–BEHAVIORAL INTERVENTIONS
A number of varied interventions have been employedwith individuals with anger-control problems including relaxation-based interventions, systematic desensitization,behavioral skills training, adjudicated psychoeducationalcounseling programs, rational–emotive behavioral therapy,and cognitive–behavioral programs, such as self-instructionaltraining, stress inoculation training, problem-solving inter-ventions, and exposure-based procedures. The CBT inter-ventions are usually short-term (8 to 22 sessions) and maybe conducted on an individual and/or group basis. The average length of treatment in various outcome studies was12 sessions. The research indicates that on average individ-ual treatment is more effective than group treatment. Butthis conclusion should be treated as preliminary given thelimited number of such comparative outcome studies. A major finding of the meta-analyses was that programs thatused standardized treatment manuals and that conductedtreatment fidelity checks were the most effective. To quoteDiGiuseppe and Tafrate (2001),
Practitioners working with aggressive clients should choosestructured interventions, delivered in an individualized format and employ safeguards to ensure that the treatment isdelivered in a manner consistent with the manuals. (p. 264)
With this proviso in mind, the remainder of this articleprovides an outline of the content of the multicomponentcognitive–behavioral interventions with patients with
24
Anger Control Problems
anger-control problems. For more detailed accounts seeMeichenbaum (2001) and the Recommended Readings.
Stress inoculation training (SIT) (Meichenbaum, 1985,2001; Novaco, 1975) has provided the major conceptual andprocedural framework for the cognitive–behavioral inter-ventions of anger control. SIT is a broad-based multi-component training that is arranged in flexible interlockingphases. The three phases are
● A conceptual educational phase● A skills acquisition and consolidation phase● An application (graduated exposure and practice)
phase
SIT provides a set of procedural guidelines to be indi-vidually tailored to the needs of each patient. The treatmentgoal of SIT is to bolster the patients’ coping repertoires andtheir confidence in being able to apply their coping skills ina flexible effective fashion. A central concept underlyingSIT is that of “inoculation” and like the medical metaphor,the treatment involves exposing the patient to graduateddoses of stressors that challenge, but do not overwhelm
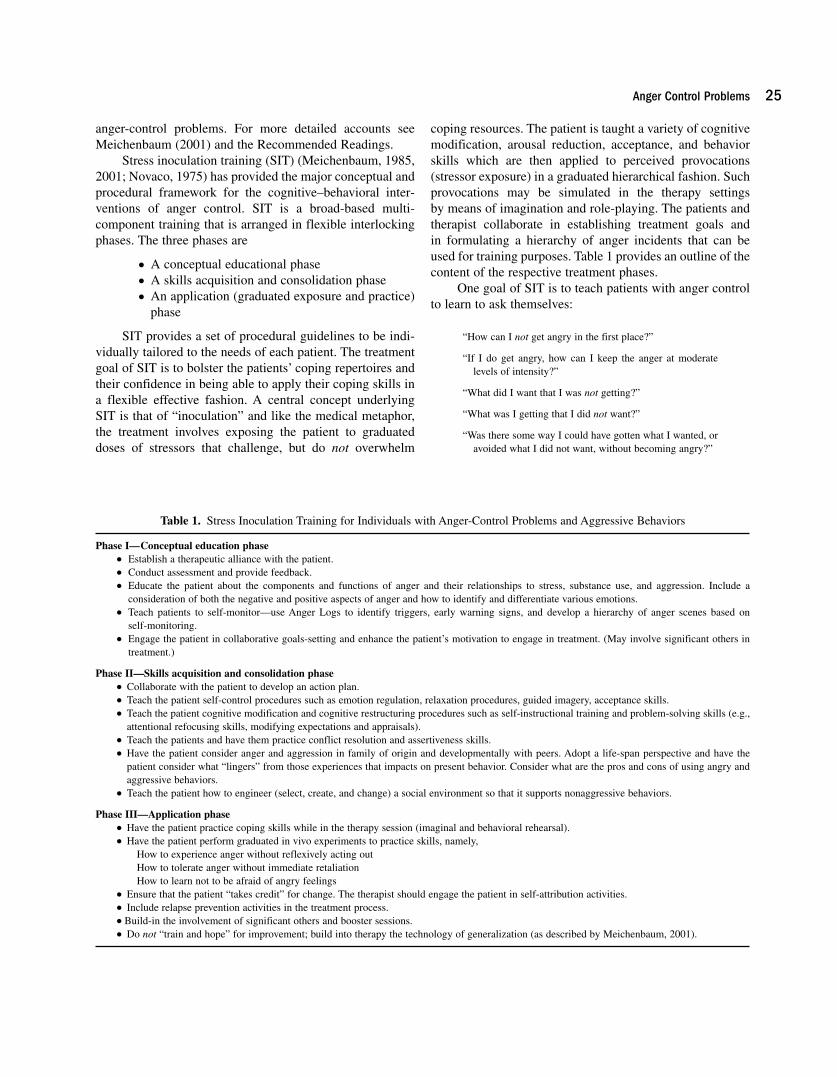
coping resources. The patient is taught a variety of cognitivemodification, arousal reduction, acceptance, and behaviorskills which are then applied to perceived provocations(stressor exposure) in a graduated hierarchical fashion. Suchprovocations may be simulated in the therapy settings by means of imagination and role-playing. The patients andtherapist collaborate in establishing treatment goals and in formulating a hierarchy of anger incidents that can beused for training purposes. Table 1 provides an outline of thecontent of the respective treatment phases.
One goal of SIT is to teach patients with anger controlto learn to ask themselves:
“How can I not get angry in the first place?”
“If I do get angry, how can I keep the anger at moderatelevels of intensity?”
“What did I want that I was not getting?”
“What was I getting that I did not want?”
“Was there some way I could have gotten what I wanted, or avoided what I did not want, without becoming angry?”
25
Table 1. Stress Inoculation Training for Individuals with Anger-Control Problems and Aggressive Behaviors
Phase I—Conceptual education phase● Establish a therapeutic alliance with the patient.● Conduct assessment and provide feedback.● Educate the patient about the components and functions of anger and their relationships to stress, substance use, and aggression. Include a
consideration of both the negative and positive aspects of anger and how to identify and differentiate various emotions.● Teach patients to self-monitor—use Anger Logs to identify triggers, early warning signs, and develop a hierarchy of anger scenes based on
self-monitoring.● Engage the patient in collaborative goals-setting and enhance the patient’s motivation to engage in treatment. (May involve significant others in
treatment.)
Phase II—Skills acquisition and consolidation phase● Collaborate with the patient to develop an action plan.● Teach the patient self-control procedures such as emotion regulation, relaxation procedures, guided imagery, acceptance skills.● Teach the patient cognitive modification and cognitive restructuring procedures such as self-instructional training and problem-solving skills (e.g.,
attentional refocusing skills, modifying expectations and appraisals).● Teach the patients and have them practice conflict resolution and assertiveness skills.● Have the patient consider anger and aggression in family of origin and developmentally with peers. Adopt a life-span perspective and have the
patient consider what “lingers” from those experiences that impacts on present behavior. Consider what are the pros and cons of using angry andaggressive behaviors.
● Teach the patient how to engineer (select, create, and change) a social environment so that it supports nonaggressive behaviors.
Phase III—Application phase● Have the patient practice coping skills while in the therapy session (imaginal and behavioral rehearsal).● Have the patient perform graduated in vivo experiments to practice skills, namely,
How to experience anger without reflexively acting outHow to tolerate anger without immediate retaliationHow to learn not to be afraid of angry feelings
● Ensure that the patient “takes credit” for change. The therapist should engage the patient in self-attribution activities.● Include relapse prevention activities in the treatment process.● Build-in the involvement of significant others and booster sessions.● Do not “train and hope” for improvement; build into therapy the technology of generalization (as described by Meichenbaum, 2001).

Anger Control Problems
In this manner, patients can learn how to:
1. “Deautomatize” the usual manner in which theyrespond to perceived provocations by developingcognitive, emotion-regulation, and behavioral skills.
2. Control anger by developing more appropriate inter-personal coping techniques.
3. Select, change, and create social environments thatsupport assertive, but not aggressive, interpersonalrepertoires.
There is much promise that effective interventions can bedeveloped to prevent such violence. To learn more aboutempirically based treatment approaches that have been appliedeffectively along the entire life span, the interested reader can go to the following websites: www.colorado.edu/cspv/blueprints and www.melissainstitute.org.
See also: Adolescent aggression and anger management, Aggressiveand antisocial behavior in youth, Anger—adult, Anger managementtherapy with adolescents, Disruptive anger
REFERENCES
Beck, R., & Fernandez, E. (1998). Cognitive–behavioral therapy in thetreatment of anger: A meta-analysis. Cognitive Therapy and Research,22, 63–75.
Bowman-Edmondson, C. B., & Cohen-Conger, J. C. (1996). A review oftreatment efficacy for individuals with anger problems: Conceptual,assessment and methodological issues. Clinical Psychological Review,16, 251–275.
Chemtob, C. M., Novaco, R. W., Hamada, R. S., & Gross, D. M. (1997).Cognitive–behavioral treatment for severe anger in post-traumaticstress disorder. Journal of Consulting and Clinical Psychology, 65,184–189.
DiGiuseppe, R., & Tafrate, R. C. (2001). A comprehensive treatment modelof anger disorders. Psychotherapy: Theory, Research, Practice andTraining, 36, 262–271.
Gerlock, A. S. (1996). An anger management intervention model for veter-ans with PTSD. NC-PTSD Clinical Quarterly, 6, 61–64.
Holtzworth-Munroe, A. (2000). A typology of men who are violent towardtheir female partners: Making sense of the heterogeneity of husbandviolence. Current Directions in Psychological Science, 9, 160–170.
Meichenbaum, D. (1985). Stress inoculation training: A practitioner’sguidebook. New York: Pergamon Press.
Meichenbaum, D. (2001). Treatment of individuals with anger-controlproblems and aggressive behaviors: A clinical handbook. Clearwater,FL: Institute Press.
Novaco, R. W. (1975). Anger control: The development and evaluation ofexperimental treatment. Lexington, MA: D. C. Heath.
Novaco, R. W. (1996). Anger treatment and its special challenges. NC-PTSD Clinical Quarterly, 6, 56–60
Reid, J. B., Patterson, G. R., & Snyder, J. (2002). Antisocial behavior inchildren and adolescents. Washington, DC: American PsychologicalAssociation.
Slep, A. M., & O’Leary, S. G. (2001). Examining partner and child abuse:Are we ready for a more integrated approach to family violence?Clinical Child and Family Psychology Review, 4, 87–107.
Sukhodolsky, D. G., & Kassinove, H. (1997). Cognitive behavioral thera-pies for anger and aggression in youth: A meta-analytic review. Posterpresented at the 105th annual convention of the AmericanPsychological Association, Chicago.
RECOMMENDED READINGS
Deffenbacher, J. L., & McKay, M. (2000). Overcoming situational and general anger: Therapist protocol. Oakland, CA: New HarbingerPublications.
Kassinove, H., & Tafrate, R. (2003). Practitioner’s guidebook to angermanagement. Atascadero, CA: Impact Publishers.
Meichenbaum, D. (2001). Treatment of individuals with anger-controlproblems and aggressive behaviors: A clinical handbook. Clearwater,FL: Institute Press.
Anger Management Therapy withAdolescents
W. Rodney Hammond and Jennifer M. WyattKeywords: anger management, anger control, adolescence, aggression,violence
Anger-control problems in adolescence are characterized byintense emotional reactions that, combined with cognitive distortions, high impulsivity, poor social skills, and a history of experience with aggression, often culminate in verbally orphysically aggressive outbursts (Nelson & Finch, 2000). Pooranger management not only contributes to the likelihood ofaggressive behavior, but also puts adolescents at increased riskfor problems in school (e.g., failing classes, being expelled, ordropping out) and in the community (e.g., contact with juve-nile or adult courts, and incarceration). In and of itself, angergenerally does not necessitate treatment. The acting-outepisodes are usually what draw the attention of parents andteachers, prompting a referral for some form of angermanagement therapy.
Characteristics of some adolescents and their environ-ments make them more likely to experience intense anger,more likely to attend to anger feelings and cognitions, andmore likely to act out as a result of anger (Feindler &Scalley, 1998). External risk factors include a history of wit-nessing or being victimized by aggression and a social envi-ronment that reinforces aggression, both of which imbue theadolescent with a schema of aggression as a viable and
26