effects of atenolol alone, nifedipine alone and their combination on ambulant myocardial ischemia
TRANSCRIPT
Effects of Atenolol Alone, Nifedipine Alone and Their Combination on Ambulant
Myocardial Ischemia James A. Hill, MD, Jose I. Gonzalez, MD, Robert Kolb, RN, and Carl J. Pepine, MD
The effects of atenolol (196 mg/day) and nifedipin6 (20 mg 3 times daily) and their combination on am- bulant myocardial ischemia were investigated using a randomlzed, double-blind, placebo-controlled, crossover trial. Eighteen men with symptomatic coronary artery disease, exercise-induced ischemia and minimal symptoms, underwent 4 blinded treat- ment periods of 2 weeks’ duration (2 placebo, 1 atenolol, 1 nifedlpine). Those that did not have ischemia eliminated by monotherapy received com- blnation therapy with both drugs. Forty-eCght=hour ambulatory electrocardiographic monitoring was used to quantitate ischemic parameters at the end of each period. Both nifedipine and atenolol as monotherapy reduced the number of ischemlc epl- sodes and the average duration of each episode compared with placebo (p <O.OS). Compared with placebo, nlfedipine reduced the total duration of ischemia (p <O.OS) but the effect of atenolol on ischemia duration was of borderline significance (p = 0.099). There were no differences in reduction of ischemic parameters when atenolol was compared with nlfedlplne (difference not significant). In the 9 patients who continued to have lschemia with monotherapy, combination therapy ellmlnated it in 2 and reduced the duration by >50% in the re- maining patients compared with placebo. In conclu- slon, monotherapy wlth nifediplne or atendol is similarly effective In eliminating or reducing ambu- lant ischemla. Combination therapy can provide ad- dltlonal benefit in those wlth continued lschemia.
(Am J Cardlol1991;07:671-675)
From the University of Florida and Gainesville Veterans Administra- tion Medical Center, Gainesville, Florida. This study was supported in part by a grant from ICI Pharmaceuticals Group, Wilmington, Dela- ware. Manuscript received October 25, 1990; revised manuscript re- ceived and accepted November 26,199O.
Address for reprints: James A. Hill, MD, Division of Cardiology, University of Florida College of Medicine, Box J-277, JHMHC, Gainesville, Florida 32610.
valuation E of myocardial ischemia has traditionally been based on determining the threshold of myo- cardial oxygen demand that causes demonstrable
ischemia manifest as angina pectoris. Ambulatory elec- trocardiographic monitoring has enabled the identifica- tion of episodes of myocardial ischemia that are fre- quently not associated with chest pain or its equivalents and often occur at indexes of myocardial oxygen de- mand much lower than those achieved by the same pa- tient during exercise testing. Recent data suggest that when antianginal agents are given to provide what ap pears to be good symptom control, a substantial num- ber of patients continue to have ambulant ischemia,iJ which has been associated with an adverse outcome.3
These findings raise questions about medical therapy and its ability to prevent not only symptoms but also ischemia, and how antiischemic therapy should be used and monitored. We4 previously reported data using dose titration of the P-blocking agent metoprolol in minimal- ly symptomatic patients with modification of ambulant ischemia as the end point of therapy. The purpose of the current study was to extend our observations on the modification of ischemia in minimally symptomatic pa- tients based on ischemia and not on symptoms. Because ambulant ischemia appears to occur by a mechanism not simply related to myocardial oxygen demand, it seems appropriate to examine the effects of medications that have potentially different actions on preventing ischemia. Accordingly, the effects of atenolol and nifed- ipine, alone and in combination, on ambulant myocardi- al ischemia were studied in a double-blind, randomized, placebo-controlled, crossover trial.
METHODS This study was approved by the Institutional Review
Board at the University of Florida and the Research Committee at the Gainesville Veterans Affairs Medical Center. All patients gave informed consent for partici- pation. The protocol design was conceived by the inves- tigators, and data analyses were performed indepen- dently by both ICI Pharmaceuticals and the investi- gators.
Patients: To be entered into the study, patients had to have a history of typical angina1 chest pain and coro- nary angiograms demonstrating significant coronary ar- tery disease (coronary stenosis 250% diameter narrow- ing). Alternatively, if coronary angiography was not performed, a redistribution defect on stress thallium- 201 scan in the presence of typical angina and ischemic
THE AMERICAN JOURNAL OF CARDIOLOGY APRIL 1, 1991 671
ST-segment changes were considered criteria for both coronary artery disease and &hernia. In addition, all patients had a treadmill exercise test response consid- ered typical for transient myocardial ischemia (11 mm horizontal ST-segment depression) without symptoms using a modified Bruce protocol within 6 months of study entry. Patients were required to be only minimally symptomatic (Canadian Cardiovascular Society class 1 or 2). Patients were excluded if they had recent myocar- dial infarction (<l month), uncontrolled hypertension, an electrocardiographic abnormality or other conditions (e.g. drugs) that would render the ambulatory electro- cardiogram ST-segment monitor uninterpretable, severe congestive heart failure, known hypersensitivity to ei- ther study medication or standard contraindications to b-blocker therapy, or were taking calcium antagonists or /I blockers.
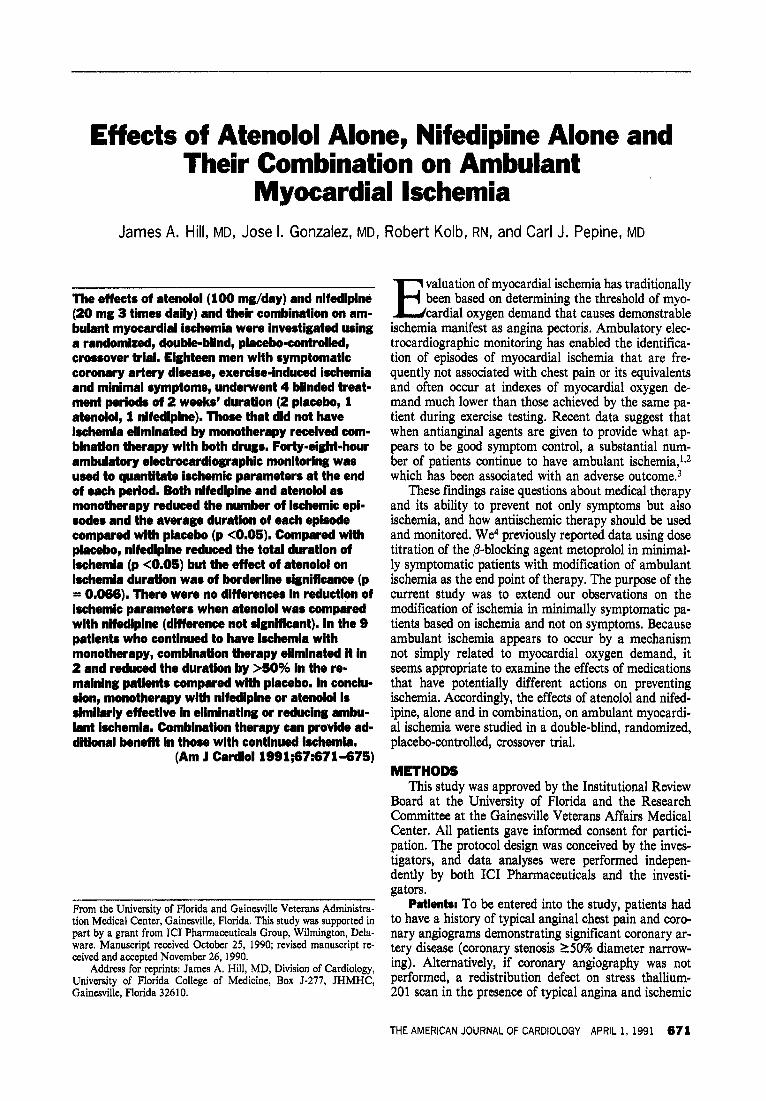
Study design (Figure 1): The study design was a double-blind, crossover, comparison trial of atenolol and nifedipine. In addition, the combination of these 2 drugs was administered in a single blind fashion to patients refractory to monotherapy.
At the beginning of the study, all antianginal medi- cation was discontinued except sublingual nitroglycerin for relief of angina. Patients were then entered into a 2- week, single-blind, placebo run-in period, at the end of which 48-hour ambulatory electrocardiographic moni- toring was performed. To qualify for continuing in the study, patients were required to have either 15 ischemic episodes or a total duration of ischemia of L5 minutes during the 48-hour monitoring period.
After the placebo run-in period, qualifying patients entered the first 2-week, double-blind, active treatment period. Patients were randomly assigned to receive ei- ther atenolol, 100 mg once each day, or nifedipine, 20 mg 3 times daily, and the corresponding placebo. If lim- iting side effects occurred after active treatment was ini- tiated, the dosage could be decreased to 50 and 30 mg/ day, respectively. After the first active treatment period, patients entered a second 2-week, single-blind, placebo period. This second placebo treatment period was per-
formed to assess for possible spontaneous improvement or worsening of the ischemic variables as a confounding factor. After this second placebo period, patients were crossed over to the alternate active therapy and corre- sponding placebo and this therapy was continued for 2 weeks. If asymptomatic ischemia was not eliminated during therapy with either active treatment, patients re ceived combination therapy with both agents at the same dose used during the monotherapy treatment peri- ods for an additional 2 weeks.
Ambulatory electrocardiographic monitoring was performed during the last 2 days of each study period. These days were chosen to eliminate any possible carry- over effect from the prior treatment period. Total study duration was 8 to 10 weeks,
Ambulatory monitoring: Ambulatory electrocardio- graphic monitoring was performed using Oxford FM ambulatory monitors (model 3500). A 2-lead system was used that reflected a modified lead V5 and lead III. At the time of hook-up, patients were tested using vari- ous maneuvers to assess postural and hyperventilation- induced electrocardiographic abnormalities that would affect the specificity of any ST changes noted. Patients were asked to keep a diary detailing occurrence of angi- na, nitroglycerin consumption, various daily activities and emotional changes. Angina was scored on a scale of l/z to 4 (mild tightness to worst pain ever experienced).
An episode of ischemia was defined as horizontal or downsloping ST-segment depression of 21. mm lasting for at least 1 minute in either lead. Each episode of &hernia was separated from other episodes of &hernia by a period when the ST segment returned to baseline for at least 1 minute. All recordings were analyzed at the study site by an experienced technician and at least 1 physician investigator.
As a simple measure of variability during a 24-hour period, ischemic parameters were summed into four 6- hour periods, 0600 to 1200,120O to 1800,180O to 2400, and 2400 to 0600 hours.
Statlstical analysis: Only patients who had data available from both active treatment phases were in-
1 ATENOLOL 1 / NIFEDIPINE 1
SINGLE DOUBLE SINGLE DOUBLE SINGLE BLIND BLIND BLIND BLIND BLIND
WEE
FIGURE 1. Study de- sign. AECG = ambula- tory electrocardiogra- QhY.
672 THE AMERICAN JOURNAL OF CARDIOLOGY VOLUME 67
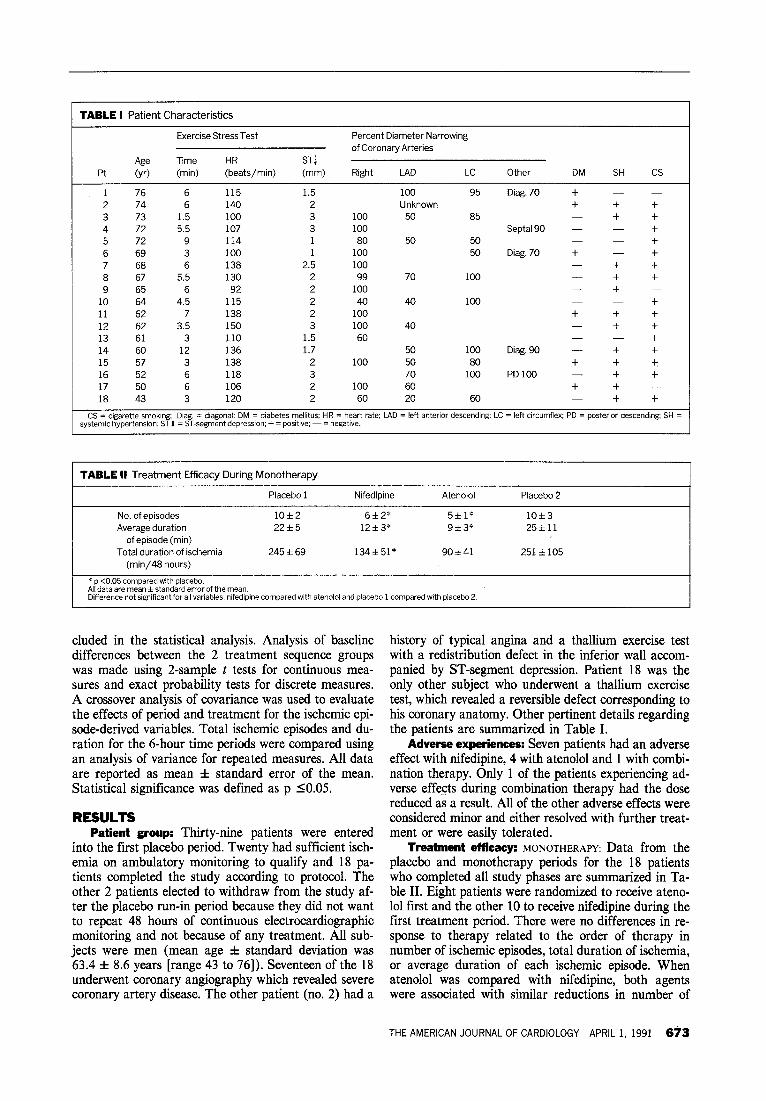
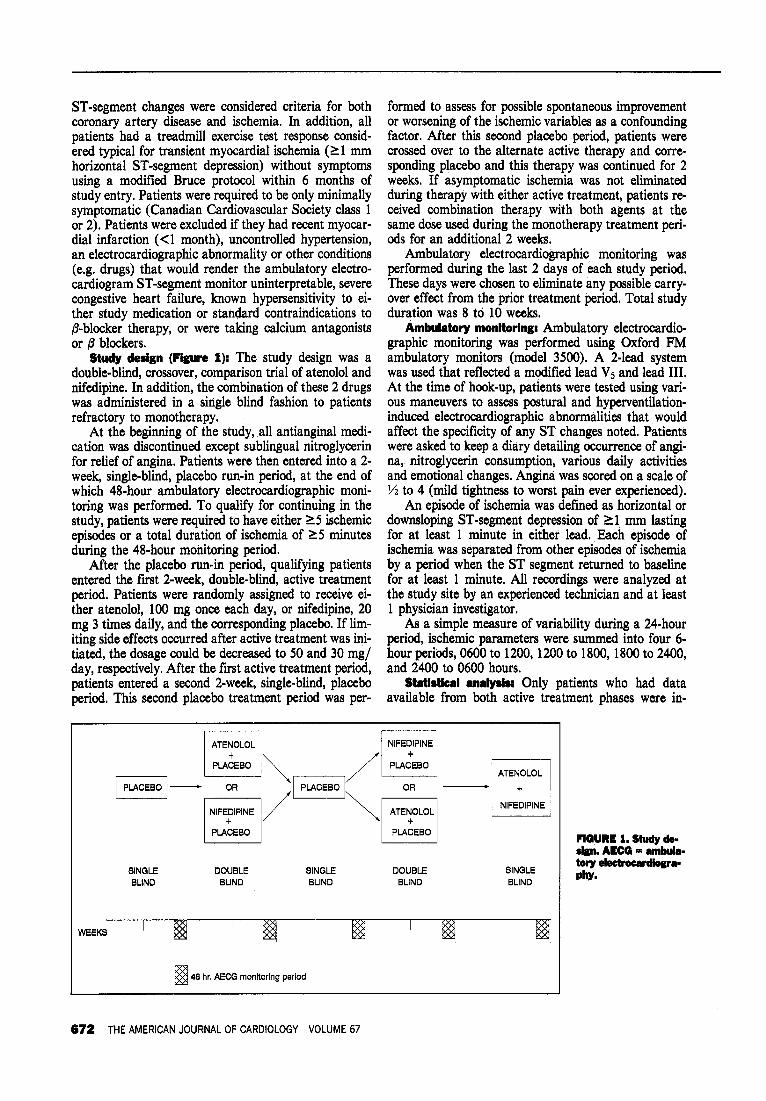
TABLE I Patient Characteristics
Pt Age (yr)
Exercise Stress Test
Time HR
(min) (beats/min) ST1 (mm)
Percent Diameter Narrowing of Coronary Arteries
Right LAD LC Other DM SH CS
1 76 6 115 1.5 100 95 Diag. 70 + -
2 74 6 140 2 Unknown + + + 3 73 1.5 100 3 100 50 85 + + 4 72 5.5 107 3 100 Septal90 - + 5 72 9 114 1 80 50 50 - t 6 69 3 100 1 100 50 Diag. 70 + t 7 68 6 138 2.5 100 t t 8 67 5.5 130 2 99 70 100 - t t 9 65 6 92 2 100 - t
10 64 4.5 115 2 40 40 100 - t 11 62 7 138 2 100 t t + 12 62 3.5 150 3 100 40 - t t
13 61 3 110 1.5 60 - - t 14 60 12 136 1.7 50 100 Diag. 90 - + t
15 57 3 138 2 100 50 80 + t +, 16 52 6 118 3 70 100 PDlOO - + t 17 50 6 106 2 100 60 + + - 18 43 3 120 2 60 20 60 t t
CS = cigarette smoking; Diag. = diagonal: DM = diabetes mellltus; HR = heart rate; LAD = left anterior descending; LC = left circumflex; pD = posterior descendLng; SH = systemic hypertension: ST U = ST-segment depression; + = positive; - = negative.
TABLE II Treatment Efficacy During Monotherapy
Placebo 1 Nifedipine Atenolol Placebo 2
No. of episodes Average duration
of episode (min) Total duration of ischemia
(min/48 hours)
lOf2 22f5
245 f 69
6f2’ 12+3*
134451*
5f 1” 9*3*
90*41
lOf3 25fll
251 f 105
* p <0.05 compared with placebo. All data are mean f standard error of the mean. Difference not significant for all variables, nifedipine compared with atenolol and placebo 1 compared with placebo 2.
eluded in the statistical analysis. Analysis of baseline differences between the 2 treatment sequence groups was made using 2-sample t tests for continuous mea- sures and exact probability tests for discrete measures. A crossover analysis of covariance was used to evaluate the effects of period and treatment for the ischemic epi- sode-derived variables. Total ischemic episodes and du- ration for the 6-hour time periods were compared using an analysis of variance for repeated measures. All data are reported as mean f standard error of the mean. Statistical significance was defined as p 10.05.
RESULTS Patient group: Thirty-nine patients were entered
into the first placebo period. Twenty had sufficient isch- emia on ambulatory monitoring to qualify and 18 pa- tients completed the study according to protocol. The other 2 patients elected to withdraw from the study af- ter the placebo run-in period because they did not want to repeat 48 hours of continuous electrocardiographic monitoring and not because of any treatment. All sub- jects were men (mean age f standard deviation was 63.4 f 8.6 years [range 43 to 761). Seventeen of the 18 underwent coronary angiography which revealed severe coronary artery disease. The other patient (no. 2) had a
history of typical angina and a thallium exercise test with a redistribution defect in the inferior wall accom- panied by ST-segment depression. Patient 18 was the only other subject who underwent a thallium exercise test, which revealed a reversible defect corresponding to his coronary anatomy. Other pertinent details regarding the patients are summarized in Table I.
Adverse experiences: Seven patients had an adverse effect with nifedipine, 4 with atenolol and 1 with combi- nation therapy. Only 1 of the patients experiencing ad- verse effects during combination therapy had the dose reduced as a result. All of the other adverse effects were considered minor and either resolved with further treat- ment or were easily tolerated.
Treatment efkacy: MONOTHERAPY: Data from the placebo and monotherapy periods for the 18 patients who completed all study phases are summarized in Ta- ble II. Eight patients were randomized to receive ateno- 101 first and the other 10 to receive nifedipine during the first treatment period. There were no differences in re- sponse to therapy related to the order of therapy in number of ischemic episodes, total duration of ischemia, or average duration of each ischemic episode. When atenolol was compared with nifedipine, both agents were associated with similar reductions in number of
THE AMERICAN JOURNAL OF CARDIOLOGY APRIL 1, 1991 673
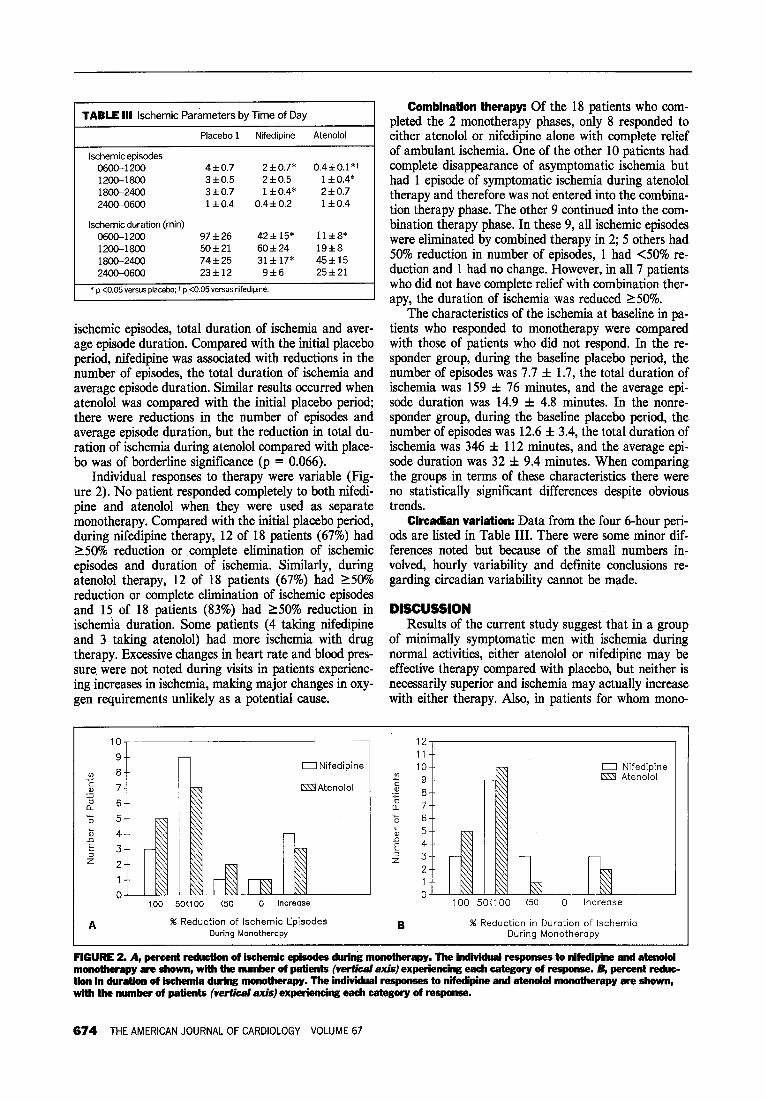
TABLE III lschemic Parameters by Time of Day
Placebo 1 Nifedipine Atenolol
lschemicepisodes 0600-l 200 4f0.7 2f0.7’ 0.4z!r0.1’~ 1200-1800 3Fto.5 2f0.5 1 rt 0.4* 18Oc24OO 3dco.7 1 f 0.4* 2 f 0.7
240&0600 1 f0.4 0.4 h 0.2 1 f0.4
lschemic duration (min)
0600-1200 97f26 42f 15’ llf8’
12OC1800 50f21 60f24 19f8 1800-2400 741k25 31 f 17’ 45*15
2400-0600 23f12 9f6 25f21
* p <0.05 YBWS placebo: 7 p <0.05 versus nifedipine.
ischemic episodes, total duration of ischemia and aver- age episode duration. Compared with the initial placebo period, nifedipine was associated with reductions in the number of episodes, the total duration of ischemia and average episode duration. Similar results occurred when atenolol was compared with the initial placebo period; there were reductions in the number of episodes and average episode duration, but the reduction in total du- ration of ischemia during atenolol compared with place- bo was of borderline significance (p = 0.066).
Individual responses to therapy were variable (Fig- ure 2). No patient responded completely to both nifedi- pine and atenolol when they were used as separate monotherapy. Compared with the initial placebo period, during nifedipine therapy, 12 of 18 patients (67%) had 150% reduction or complete elimination of ischemic episodes and duration of ischemia. Similarly, during atenolol therapy, 12 of 18 patients (67%) had 150% reduction or complete elimination of ischemic episodes and 15 of 18 patients (83%) had 150% reduction in ischemia duration. Some patients (4 taking nifedipine and 3 taking atenolol) had more ischemia with drug therapy. Excessive changes in heart rate and blood pres- sure were not noted during visits in patients experienc- ing increases in ischemia, making major changes in oxy- gen requirements unlikely as a potential cause.
Combination therapy: Of the 18 patients who com- pleted the 2 monotherapy phases, only 8 responded to either atenolol or nifedipine alone with complete relief of ambulant ischemia. One of the other 10 patients had complete disappearance of asymptomatic ischemia but had 1 episode of symptomatic ischemia during atenolol therapy and therefore was not entered into the combina- tion therapy phase. The other 9 continued into the com- bination therapy phase. In these 9, all ischemic episodes were eliminated by combined therapy in 2; 5 others had 50% reduction in number of episodes, 1 had <50% re- duction and 1 had no change. However, in all 7 patients who did not have complete relief with combination ther- apy, the duration of ischemia was reduced 150%.
The characteristics of the ischemia at baseline in pa- tients who responded to monotherapy were compared with those of patients who did not respond. In the re- sponder group, during the baseline placebo period, the number of episodes was 7.7 f 1.7, the total duration of ischemia was 159 f 76 minutes, and the average epi- sode duration was 14.9 f 4.8 minutes. In the nonre- sponder group, during the baseline placebo period, the number of episodes was 12.6 f 3.4, the total duration of ischemia was 346 f 112 minutes, and the average epi- sode duration was 32 f 9.4 minutes. When comparing the groups in terms of these characteristics there were no statistically significant differences despite obvious trends.
Circadian variation: Data from the four 6-hour peri- ods are listed in Table III. There were some minor dif- ferences noted but because of the small numbers in- volved, hourly variability and definite conclusions re- garding circadian variability cannot be made.
DISCUSSION Results of the current study suggest that in a group
of minimally symptomatic men with ischemia during normal activities, either atenolol or nifedipine may be effective therapy compared with placebo, but neither is necessarily superior and ischemia may actually increase with either therapy. Also, in patients for whom mono-
10,
m 8 7 .$ 7
CT 6
0 Nifedipine
LFlAtenolol
100 50(100 (50 0 Increase
A % Reduction of lschemic Episodes During Monotherapy
12,
U Nifedipine KII Atenolol
100 50(100 (50 0 Increase
% Reduction in Duration of lschemio During Monotheropy
FIGURE 2. A, percent reduction of itiic episodes during monotherapy. The individual responses to nifedipine and atenolol monotherapy are ehown, with the rmmber of patients (vertical axis) experiencing each category of response. G, percent reduc- tion in duration of iechemia during monotherapy. The individual responses to nifedipine and atendol monotherapy are shown, wlth the mnnhor of patlsnts (vertical axis) experiencing each category of responee.
674 THE AMERICAN JOURNAL OF CARDIOLOGY VOLUME 67

therapy is ineffective in eliminating ambulant ischemia, combination therapy may prove useful. Despite a trend toward more ischemia in the nonresponders, there were no characteristics of the ischemia at baseline that pre- dicted a good response to either monotherapy or the need for combination therapy. Although this has not been previously reported, definitive determination of such characteristics would require a larger sample size.
Other investigators have evaluated the use of both p blockers and calcium antagonists alone for the treat- ment of myocardial ischemia. Quyyumi et al2 evaluated the response to atenolol and nifedipine in 9 patients with ischemic ST depression on the ambulatory electrocar- diogram. They administered the same doses of nifedi- pine and atenolol as in the current study but their pa- tient population was very symptomatic both during ex- ercise and angina at rest. During atenolol treatment, 3 patients had no ischemia and the group as a whole had significantly less ischemia with atenolol than with nifed- ipine. Contrary to the current study results, no patient’s condition was worse with monotherapy than with no therapy. Mulcahy et ak5 extending these observations and including some of the data of Quyyumi, reported the responses of 53 patients to treatment with nifedi- pine, atenolol or the combination on transient ischemia. Atenolol was associated with a significant reduction in both frequency and duration of ischemia, whereas ni- fedipine had little effect. In this report, other than group data, few comparisons can be made because the specific circumstances of therapy, patient population studied and other details are not clear.
Others have reported the effects of combination therapy on ischemic parameters. Egstrup6 evaluated the response of ischemic parameters in 42 patients with chronic stable angina to nifedipine, metoprolol and their combination in a parallel design. Metoprolol was found to decrease total ischemic episodes 55% and duration of ischemia 51%, whereas nifedipine showed no change in either parameter. Combination therapy also reduced the number of ischemic episodes as well as the duration of ischemia significantly better than nifedipine but no bet- ter than metoprolol monotherapy. Moreover, there was a small (17%) increase in asymptomatic ischemic epi- sodes with nifedipine.
We found that with both therapies ambulant isch- emia may increase, which has been reported previously but not emphasized. Dihydropyridine calcium antago- nists have been previously reported to provoke transient myocardial ischemia,7 but whether an actual “proisch- emit effect” occurs with either drug cannot be deter- mined. Cohn et al8 investigated the effect of added ni- fedipine, and found that a 23% reduction in ischemic
episodes occurred in the group as a whole but 43 of 136 (32%) had more episodes, whereas 75 of 136 (55%) had a reduction. This again suggests that the general trend is for improvement in ischemia with nifedipine but that there is considerable individual variability.
Study limitations: There are several important limi- tations in the current study that deserve comment. First, a small number of highly selected patients were studied over a relatively short time period. The crossover design makes conclusions more valid in a small group but long- term effects cannot be determined. Second, all the sub- jects were men. Third, there was considerable variabili- ty among patients in terms of amount and duration of ischemia. However, this does reflect the characteristics of the population with ambulatory ischemia and those at risk for adverse events.‘y9 Fourth, to simplify the study design, only fiied doses of the study drugs were given and no attempt was made to titrate to maximal effect. Finally, we cannot be sure that spontaneous vari- ability in ambulant ischemia did not contribute to some of the presumed treatment effect. However, the similar- ity of the 2 placebo periods and the lack of order effect on ischemia make this possibility less likely.
Acknowledgment: We would like to thank Elizabeth France, RN, for her help in organizing the initial phases of this study, Howard Hait from ICI Pharmaceuticals for statistical support and Paul Blake, MD, from ICI Pharmaceuticals for his kind support throughout the study.
REFERENCES 1. Deedwania PC, Carbajal EV. Prevalence and patterns of silent myocardial ischemia during daily life in stable angina patients receiving conventional antian- ginal drug therapy. Am J Cardiol 1990;65:1090-1096. 2. Quyyumi AA, Crake T, Wright CM, Mockus LJ, Fox KM. Medical treatment of patients with severe exertional and rest angina: double blind comparison of /3 blocker, calcium antagonist, and nitrate. Br Heart J 1987;57:505-511. 3. Gottlieb SO, Weisfeldt ML, Ouyang P, Mellits ED, Gerstenblith G. Silent ischemia as a marker for early unfavorable outcomes in patients with unstable angina. N Engl J Med 1986;314:1214-1219. 4. Imperi GA, Lambert CR, Coy K, Lopez L, Pepine CJ. Effects of titrated beta blockade (metoprolol) on silent myocardial ischemia in ambulatory patients with coronary artery disease. Am J Cardiol 1987;60:519-524. 5. Mulcahy D, Cunningham D, Crean P, Wright C, Keegan J, Quyyumi A, Park A, Fox K. Circadian variation of total ischemic burden and its alteration with anti- angina1 agents. Lmcet 1988;2:755-759. 6. Egstrup K. Randomized double-blind comparison of metoprolol, nifedipine, and their combination in chronic stable angina: effects on total ischemic activity and heart rate at onset of ischemia. Am Heart J 1988;116:971-978. 7. Lambert CR, Hill JA, Feldman RL, Pepine CJ. Myocardial ischemia during intravenous nicardipine administration. Am J Cardiol 1985;55:844-845. 8. Cohn PF, Vetrovec GW, Nesto R, Gerber FR. The Nifedipine-Total Ischemia Awareness Program: a national survey of painful and painless myocardial isch- emia including results of antiischemic therapy. Am J Cnrdioi 1989;63:534-539. 9. Rocco MB, Nabel EG, Campbell S, Goldman L, Barry J, Mead K, Selwyn A. Prognostic importance of myocardial ischemia detected by ambulatory monitor- ing in patients with stable coronary artery disease. Circulation 1988;78:877-884.
THE AMERICAN JOURNAL OF CARDIOLOGY APRIL 1, 1991 675