dr suganthi singaravelu spr5 anaesthetics journal club presentation - arrowe park hospital
DESCRIPTION
Risk factors for unplanned transfer to Intensive care within 24 hours of admission from the emergency department. Dr Suganthi Singaravelu SpR5 Anaesthetics Journal Club presentation - Arrowe park Hospital. Introduction. 5% of ED admissions undergo unplanned transfer to ICU 1 - PowerPoint PPT PresentationTRANSCRIPT
Risk factors for unplanned transfer to
Intensive care within 24 hours of admission from
the emergency department
Dr Suganthi SingaraveluSpR5 Anaesthetics
Journal Club presentation -Arrowe park Hospital
Introduction
5% of ED admissions undergo unplanned transfer to ICU1
Unplanned admission has a higher mortality than direct admission from ED to ICU
Better recognition and interventions in ED are needed.

Aim of the study
To describe the risk factors associated with unplanned transfer to ICU within 24hours of admission to the ward from ED
Methods- Patients identification
All adult patients admitted in ED between 2007 and 2009
Data obtained from Kaiser Permanente North California -13 hospitals with similar patient populations.
Exclusion: Direct transfer to theatre or ICU, pregnant patients
Methods- Patient characteristics
Patient: Age, gender, admitting diagnosis, chronic illness burden, acute physiological derangement in the ED and hospital length of stay
Chronic illness: Comorbidity Point Score (COPS)
Acute: Laboratory Acute Physiological Score (LAPS)
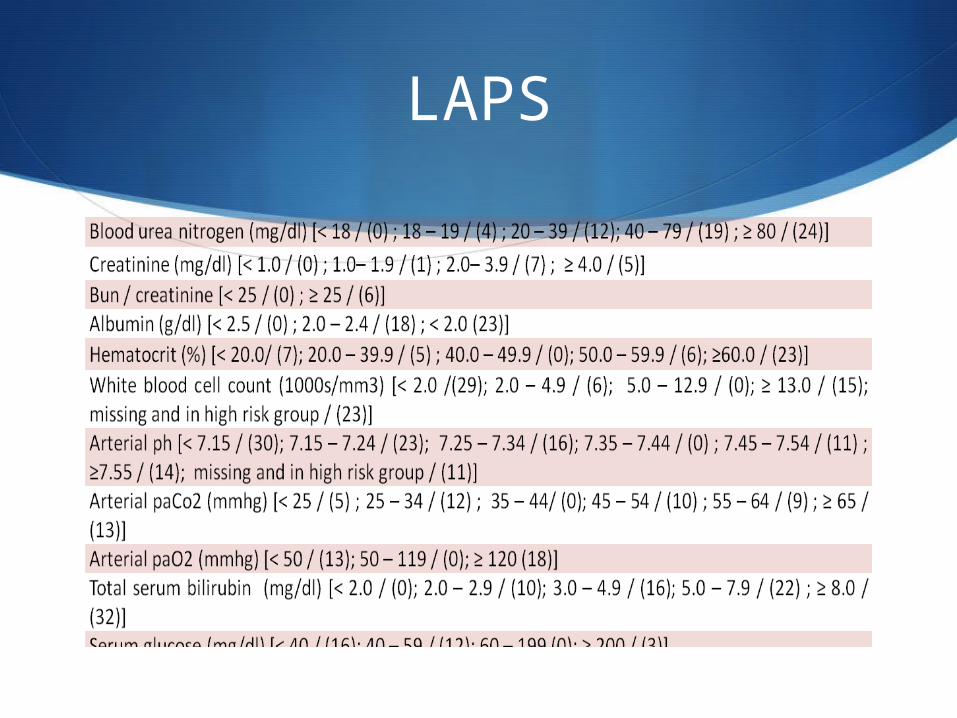
LAPS
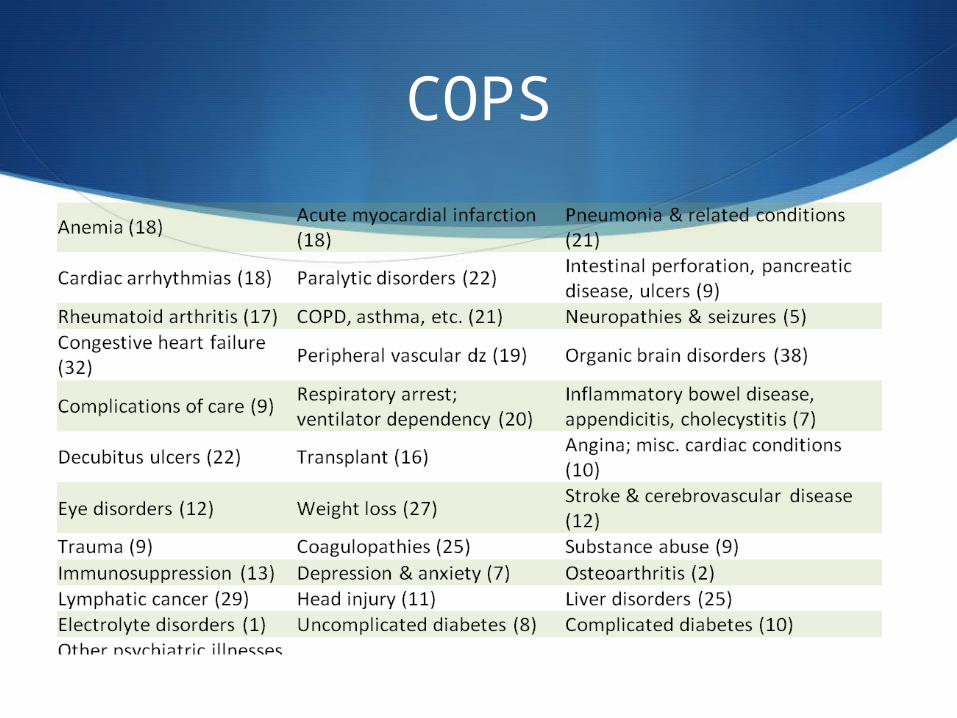
COPS
Statistics
Univariate analysis:
ANOVA and
chi square test
Multivariate logistic regression
Results
Total: 178,315 non ICU admission from ED
4,252 (2.4%) – admitted to ICU within 24 hours of leaving ED
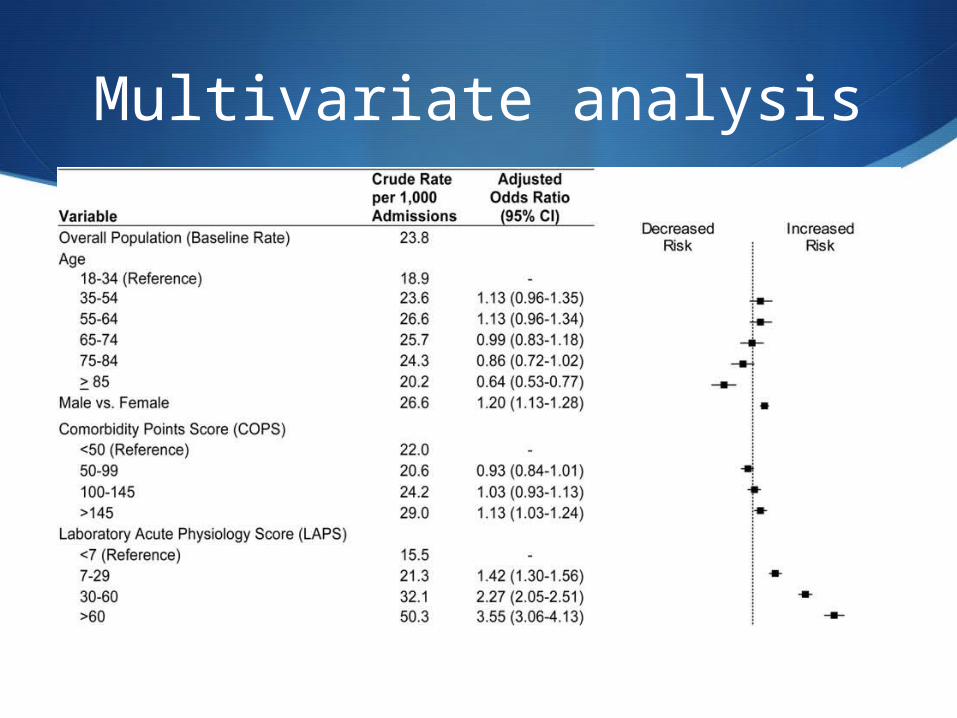
Multivariate analysis
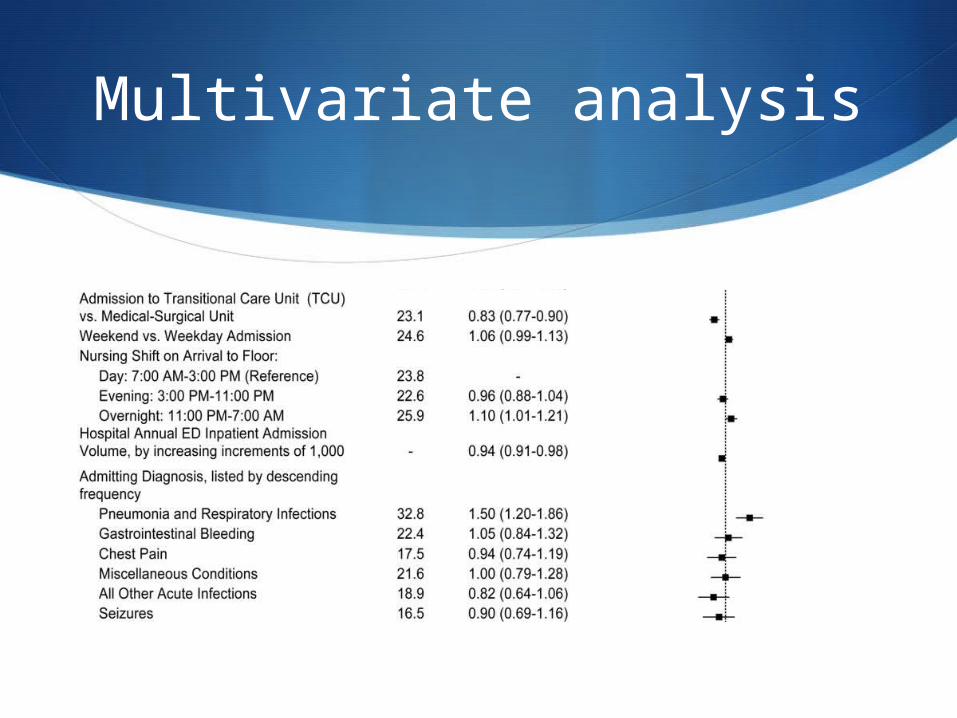
Multivariate analysis
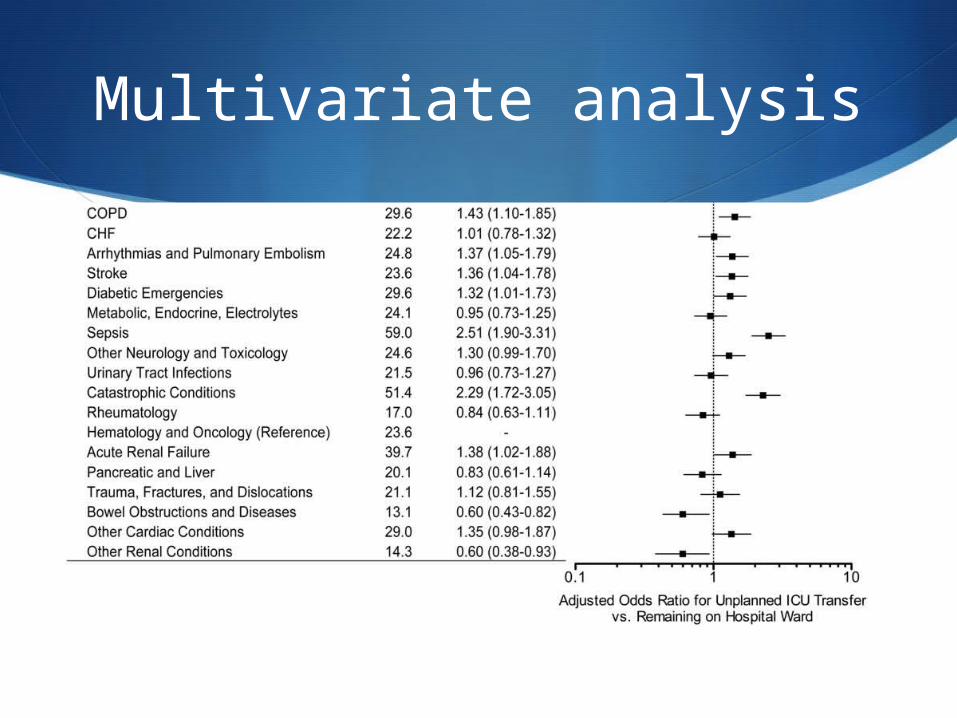
Multivariate analysis
Significant Risk factors
Higher co-morbidity
More deranged physiology
Arrived overnight in the ward
More frequent in lower volume hospitals
Results
Respiratory conditions (COPD/ pneumonia/acute RTI) comprised nearly half (47%) of all conditions.
1 in 30 pneumonia and 1 in 33 COPD were transferred to ICU from ward
Overall 1 in 42 with respiratory condition – worse mortality
Respiratory problems
Tendency for rapid deterioration
ICU may accept in early stage
Applying prediction rules to identify the patients who may need ventilation
Intermediate (HDU) care for these patients
Discussion- Hospital size
Unplanned transfers X 2 higher in low volume centers- Reasons???
- Less resources
- lower ICU capacity
- less on –call intensivists
- less experience with certain critical care conditions
Dark hours 11pm to 7 am?
Unclear why arriving overnight has higher risk
Possibilities are
ED overcrowding in the evening
Decreased staffing
longer delays in critical diagnostic
tests and interventions
Lesser risk of ICU admission
TCU (HDU)
Age >85 – advanced directives or patient preferences

Limitation of the study
Not designed to distinguish the underlying cause i.e. under recognition of illness or delays in interventions
vital signs and mental status that were not included could improve the risk adjustment.
Study conclusions
Unplanned admission to ICU is more likely in patients with respiratory conditions, sepsis and MI, higher co morbidity burden and grossly abnormal lab results.
Better inpatient triage, earlier interventions or closer monitoring may prevent unplanned ICU admissions.

How to apply in our hospital
Prediction rules can be considered for better triage
Organisational changes for night shift, more HDU beds or A&E resources
Compare data with high volume centers and regular monitoring