dr mojgan mortazavi associate professor of nephrology acute kidney injury
TRANSCRIPT


Background
• Acute Kidney Injury (AKI) is an abrupt loss of renal function that results in the retention of nitrogenous and other waste products. This can lead to metabolic and organ dysfunction.
• Renal function is most easily monitored by measuring the
serum creatinine level and estimating the glomerular filtration rate (GFR)

What is GFR? How is it Calculated?
• The Glomerular Filtration Rate (GFR) is the volume of fluid filtered from glomerular capillaries into the Bowman’s capsule per unit time

Risk Factors for AKI
• Age > 75 yrs • Chronic kidney disease (CKD, eGFR < 60
mls/min/1.73m2) • Cardiac failure • Diabetes mellitus • Hypovolemia• Nephrotoxic medication • Atherosclerotic peripheral vascular disease • Liver disease • Sepsis

Definition of AKI
As per the Acute Kidney Injury Network:
• An abrupt (within 48hrs) reduction in kidney function defined as an increase in serum creatinine level of 0.3mg/dl
OR
• An increase in serum creatinine ≥ 50% OR
• Urine output is < 0.5ml/kg/hr for >6 consecutive hours

Etiologies of AKI• Prerenal- causes that decrease effective blood flow to the
kidneyso Volume loss (dehydration, bleeding, renal loss, GI loss,
burns, 3rd spacing), decreased cardiac output, systemic vasodilation, renal artery disease, etc.
Etiologies of AKI
• Intrinsic (Renal)- causes due to damage to the kidney itselfo Acute tubular necrosis, glomerulonephritis, acute
interstitial nephritis, vasculitides, autoimmunity, drugs, infection, etc.

Etiologies of AKI
•Postrenal- causes as a result of urinary tract obstruction, can occur anywhere from the renal pelvis to the urethra.o Stone, stricture, tumor, clot, prostate etiology,
bladder neck obstruction, extraluminal compression, etc.

Baseline Set of Laboratories to Consider
• Biochemistryo urea and electrolytes
• Hematologyo CBC
• Urinalysis (+/- microscopy, eosinophils)• Urinary Biochemistry
o electrolytes, urea, osmolality • Microbiology
o urine/blood culture when/if infection suspected• Imaging
o renal ultrasoundo CXR, abdominal x-ray
• ECG

Urine Patterns in Renal Disease
Urinary Pattern Renal Disease
Hematuria with red cell casts, heavy proteinuria, or lipiduria
Glomerular disease or vasculitis
Granular and epithelial casts with free epithelial cells
Acute Tubular Necrosis
Pyuria with white cell and granular casts and no/mild proteinuria
Tubular or interstitial disease or obstruction
Hematuria and pyuria with no or variable casts(excluding red cell casts)
Acute interstitial nephritis, glomerular disease, vasculitis, obstruction, renal infarction
Pyuria alone Usually infections, sterile pyuria suggests TB

ManagementImportantly, manangement of AKI is varied and depends on the cause. Given no effective pharmaceutical options, management of AKI is primarily supportive. However, some general principles can be applied. • Prerenal azotemia is usually responsive to isotonic fluid
repletion • Managament of ATN includes discontinuation of
nephrotoxic agents, optimization of hemodynamics, continued monitoring of renal function (acid/base status, electrolyte abnormalities).
• Postrenal causes warrant removal of the obstruction.

Management Cont.• Things to do for patients with AKI
o Renally dose medicationso Avoid nephrotoxinso Monitor I/Os o Serial assessment of serum creatinine
• Renal Replacement Therapy (i.e dialysis) is the central
component of care for patients with severe AKI • The generally accepted indications for renal replacement
therapy in the setting of AKI include:o Acidosiso Electrolyte disturbanceo Ingestion/Intoxicationo Volume Overloado Overt Uremia

5 Key Steps in Evaluating Acute Renal Failure
1) Obtain a thorough history and physical; review the chart in detail
2) Do everything you can to accurately assess volume status
3) Always order a renal ultrasound
4) Look at the urine
5) Review urinary indices

Acute Renal Failure
Muddy Brown Casts:
Highly suggestive of ATN.
Pigmented granular casts as seen in hyperbilirubinemia can be confused for these.
UpToDate Images.

Acute Renal Failure
UpToDate Images.
White Blood Cell Casts:
Raises concern for interstitial nephritis.
Can be seen in other inflammatory disorders.
Also seen in pyelonephritis.

Acute Renal Failure• Hematuria
Nonglomerular hematuria:
Urologic causes.
Bladder/Foley trauma.
Nephrolithiasis.
Urologic malignancy.
May be “crenated” based upon age of urine, osmolality – NOT dysmorphic.

Acute Renal Failure
Red Blood Cell Casts:
Essentially diagnostic of vasculitis or glomerulonephritis.
Dysmorphic Red Cells:
Suggestive of glomerular bleeding as seen with glomerulonephritis.
Blebs, buds, membrane loss.
Rarely reported in other conditions – DM, ATN.

Acute Renal FailureCrystals – Pretty and important.
Uric acid crystals:
Seen in any setting of elevated uric acid and an acidic urine.
Seen with tumor lysis syndrome.
Calcium oxalate crystals:Monohydrate – dumbell shaped, may be needle-like.Dihydrate – envelope shaped.Form independent of urine pH.Seen acutely in ethylene glycol ingestion.
UpToDate Images.

Diagnostic Evaluation Diagnostic Evaluation of Renal Failureof Renal Failure
Cumulative% Correct Diagnosis
Hx, PE, Labs TherapeuticTrials
Renal Biopsy
100-
80-
60-
40-
20-
0-
60%
25%
15%

Renal Biopsy-When?Renal Biopsy-When?
Exclude pre- and post-renal failure, and Exclude pre- and post-renal failure, and clinical findings are not typical for ATNclinical findings are not typical for ATN
Extra-renal manifestations that suggest Extra-renal manifestations that suggest a systemic disordera systemic disorder
Heavy proteinuriaHeavy proteinuria RBC castsRBC casts

Case 1
A 42 year male is admitted to the SICU after sustaining multiple trauma. His course is complicated by Enterobacter sepsis with profound hypotension requiring support with intravenous dopamine. The urine output has gradually decreased to only 300 ml per day. The urine sodium is 78.


Ischemic Acute Renal Failure
• A form of ATN often following a prerenal insult• Severity of renal failure correlates with duration of insult• Treatment is to optimize renal perfusion, avoid
additional nephrotoxic insults and other supportive measures

Conditions that Lead to Pre-renal Acute Renal Failure
Generalizedor Localized Reduction in
Renal Blood Flow
Ischemic Acute Renal Failure
Intravascular Volume Depletion
Decreased Effective Circulating VolumeCHF Cirrhosis Nephrosis
HepatorenalSyndrome
Sepsis

Phases of Ischemic Epithelial Tubular Injury
Time
GFR
Pre-renal
Initiation
Extension
MaintenanceRecovery


Risk Factors for Ischemic Tubular Injury
• Volume depletion• Aminoglycosides• Radiocontrast• NSAIDs, Cox-2 inhibitors• Sepsis• Rhabdomyolysis• Preexisting renal disease• HTN• Diabetes mellitus• Age > 50 • Cirrhosis



Case 2
A 56 y.o. male presents with complaints of persistent fever, chills, sore throat, and myalgias for the past 14 days. Ten days ago he started taking amoxicillin he had on hand for dental prophylaxis. His physical exam is remarkable for fever to 38.6oC, an exudative pharyngitis and a diffuse maculopapular rash.
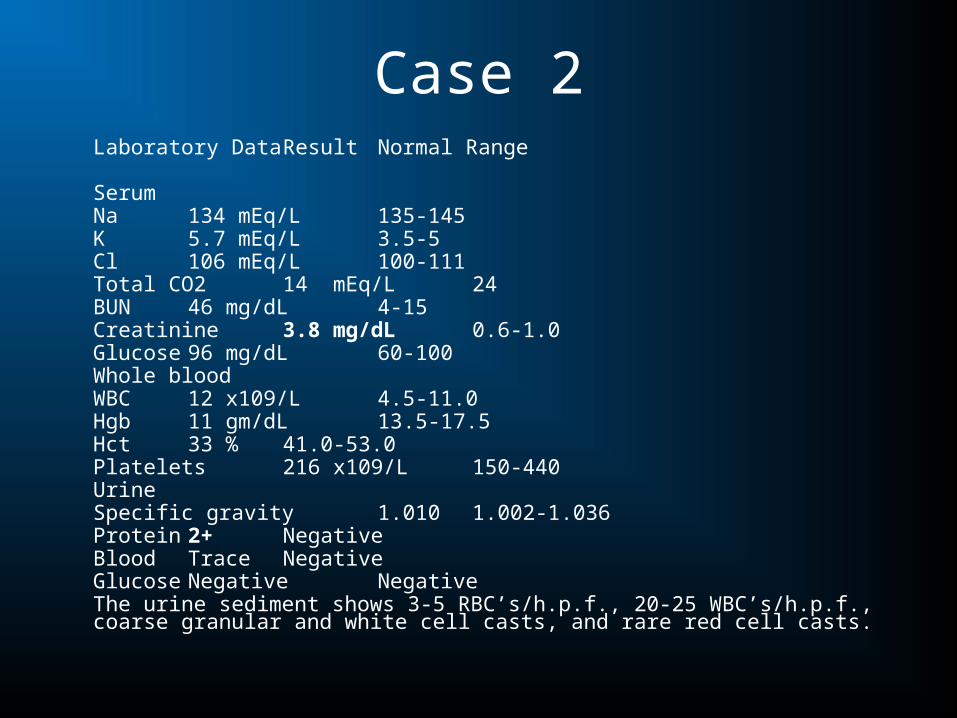
Case 2Laboratory Data Result Normal Range
SerumNa 134 mEq/L 135-145K 5.7 mEq/L 3.5-5Cl 106 mEq/L 100-111Total CO2 14 mEq/L 24BUN 46 mg/dL 4-15Creatinine 3.8 mg/dL 0.6-1.0Glucose 96 mg/dL 60-100Whole bloodWBC 12 x109/L 4.5-11.0Hgb 11 gm/dL 13.5-17.5Hct 33 % 41.0-53.0Platelets 216 x109/L150-440UrineSpecific gravity 1.010 1.002-1.036Protein 2+ NegativeBlood Trace NegativeGlucose Negative Negative
The urine sediment shows 3-5 RBC’s/h.p.f., 20-25 WBC’s/h.p.f., coarse granular and white cell casts, and rare red cell casts.

Case 2
Acute Interstitial Nephritis-Etiology
• Allergic/Drug induced• Autoimmune
– Sarcoid -SLE– Sjogren’s
• Toxins– Chinese herb nephropathy -Heavy metals– Light chain cast nephropathy
• Infiltrative– Leukemia– Lymphoma
• Infections (Legionella, CMV, HIV, Toxoplasma)

Acute Interstitial NephritisClinical Presentation
• Non-oliguric ARF• Fever in allergic and infectious types (except NSAID type)• Rash in allergic type (except NSAID induced)• Eosinophilia• UA: WBC casts
Eosinophiluria (allergic)Hematuria (NSAID related)

Common Causes of Drug Induced AIN
• NSAIDS• Antibiotics
– Penicillins• methacillin• Ampicillin, amoxacillin, carbenacillin, oxacillin• Cephalosporins
– Quinolones (ciprofloxacin)– Anti-tuberculous medications (rifampin, INH, ethambutol)– Sulfonamides (TMP-SMX, furosemide, thiazides)
• Miscellaneous– Allopurinol, cimetidine, dilantin

Acute Kidney Injury: AIN causes
DRUGS• ACEI• Allopurinol• Cephalosporins• Cimetidine• Fluoroquinolones• Loop diuetics• NSAIDS• PCN• Phenytoin• Rifampin• Sulfonamides• Tegretol• Thiazides
INFECTION• Bacterial
– Agents causing pyelonephritis– Legionella– Brucella– Yersinia
• Viral– Hantavirus– HIV– CMV,EBV,HSV

Acute Interstitial NephritisTreatment
• Withdrawal of offending agent
• Treatment of underlying process if infectious/autoimmune etiology
• Trial of corticosteroids, especially in allergic presentations1 mg/kg/day or 2 mg/kg every other day– No randomized trials proving efficacy– Reversal of renal failure usually seen in < 6 weeks

Rhabdomyolysis• Often develops in the setting of crush injury, especially if
superimposed circulatory shock• Hallmarks of diagnosis
– CK > 10,000– (+) dipstick for blood but no RBCs
• Treatment– Volume expansion (judiciously if severe oliguria or
azotemia)– Fasciotomy when indicated for compartment syndrome
(“second wave phenomenon”)• Avoid calcium repletion unless neuromuscular manifestations
present• Rebound hypercalcemia in recovery phase

Aminoglycoside Nephrotoxicity
• Generally presents 1 week after exposure• Non-oliguric • Low trough levels do not guard against nephrotoxicity• Incidence of ATN
– 10% after 1 week– 40% after 2 weeks
• Risk factors for ATN– Advanced age - Superimposed sepsis– Liver disease - Hypotension

Radiocontrast-Induced Acute Renal Failure
• Induces renal vasoconstriction and direct cytotoxicity via oxygen free radical formation
• Risk factors:– Renal insufficiency - Diabetes– Advanced age - > 125 ml contrast– Hypotension
• Usually non-oliguric ARF; irreversible ARF rare

Contrast Induced Nephropathy
• Assess CIN risk– eGFR <30 – Hospital admission, Nephrology consult, Dialysis planning, renal protection– eGFR 30-59 – Discontinue NSAIDs, IV volume expansion, Intra-arterial: isoosmolar, Intra-
venous: iso-osmolar or low osmolar contrast; limit contrast volume– eGFR >60, Discontinue metformin
• Optimal Volume Status• Low-osmolality contrast media• F/U Creatinine 24 – 72hr after contrast exposure• Adequate IV volume expansion with isotonic crystalloid for 3 – 12hr
before the procedure and continue for 6 – 24hr afterward. Oral fluid data is insufficient
• No adjunctive medical or mechanical treatment has been proved to be efficacious
• Prophylactic hemodialysis and hemofiltration not validated

Acute Renal Failure due toIntratubular Obstruction
• Crystalluria– Ethylene glycol: Calcium oxalate– Tumor lysis: Urate and Calcium phosphate – Medications
• Acyclovir• Methotrexate• Sulfonamides• Anti-retroviral agents
• Myeloma cast nephropathy



Case 3A 35-year-old Hispanic female presents with a one
month history of periorbital and lower extremity edema. Over two days prior to presentation she has experienced arthralgias in her wrists and elbows. On physical examination she is in no acute distress. Blood pressure is 162/94, temperature 37.4 . Her skin exam is significant for a malar erythematous rash. The heart and lungs are normal. There is 3+ edema to the thighs bilaterally.

Case 3Laboratory Data Result Normal Range
SerumNa 138 mEq/L 135-145K 4.2 mEq/L 3.5-5Cl 108 mEq/L 100-111Total CO2 17 mEq/L 24BUN 75 mg/dL 4-15Creatinine 3.5 mg/dL 0.6-1.0Glucose 83 mg/dL 60-100Anti-neutrophil antibody 1:160 NegativeWhole bloodWBC 5.9 x109/L 4.5-11.0Hgb 11.9 gm/dL 13.5-17.5Hct 34 % 41.0-53.0Platelets 153 x109/L 150-440UrineSpecific gravity 1.015 1.002-1.036Protein 3+ NegativeBlood 3+ NegativeRBC >50/h.p.f. 0-4Sodium 10 mEq/L VariableCreatinine 35 mg/dL Variable

Case 3

AKI: Glomerulonephritis (RPGN)/Systemic Vasculitis
• Immune-Complex Mediated• SLE• Cryoglobulinemic vasculitis• Henoch-Schönlein purpura
• Post-strep GN
• Direct Ab attack• Anti-GBM disease• Goodpasture’s syndrome
• Pauci-immune vasculitis• Microscopic polyangiitis• Wegener’s granulomatosis• Churg-Strauss syndrome
• Thrombotic Microangiopathy
• TTP• HUS• Scleroderma renal crisis• Preeclampsia• Malignant hypertension

AKI: Summary
• Small changes in creatinine can have grave clinical consequences
• ABCDE assessment and careful management of fluid status is mainstay of treatment
• Get help early

Future fixes…• Neutrophil Gelatinase-
Assoc. Lipocalin (NGAL)– Levels in blood and urine rise
within a few hours after injury
• Cystatin C– Absorbed by kidney, but not
secreted– Rises one day before Cr
• Interleukin 18– Produced by caspase-I which
is implicted in pathogenesis of ARF
Have been shown to predict AKI severity in post-op hearts
