hypertension in pregnancy mojgan vatani staff specialist, wch
TRANSCRIPT

Hypertension in Pregnancy
Mojgan Vatani
Staff Specialist, WCH

• Definition
• Classification
• Investigation
• Management/Treatment

Definition
• Normal pregnancy is characterised by a fall in BP, detectable in the 1st trimester and usually reaching a nadir in the 2nd trimester. BP rises towards pre-conception levels towards the end of the 3rd trimester.

Hypertension in Pregnancy
• Systolic BP greater than or equal to 140 mmHg and/or
• Diastolic BP greater than or equal to 90 mmHg
• Repeated reading over several hours.
• Important as perinatal mortality and morbidity rises with diastolic BP above 90 mmHg.
Recording BP in Pregnancy
• Seated comfortably with her legs resting on a flat surface.
• Left arm
• The standard location is the upper arm, with the stethoscope at the elbow crease over the brachial artery
• In labour, BP can also be measured in lateral recumbency (30 degree). Avoid supine posture.
• Proper size cuff


Cuff size
• Recommendation from American Hearth Association:– Cuff dimension requirements refer to the size
of the compression cavity, NOT the cuff itself.– Cuff width should be equal 40% of the arm
circumference or 1.2 times the diameter of the arm.
– Use the ratio of the arm circumference to the cuff width, not the cuff length.

Cuff size
• A larger cuff with an inflatable bladder covering 80% of the arm circumference should be used if the upper arm circumference is greater than 33 cm.

BP measurement
• The systolic BP is accepted at the first Korotkoff sound (K1) heard
• The diastolic BP is accepted with the disapperance of sounds completely (K5). Where K5 is absent, K4 (muffling) should be accepted.
BP measurement
• Mercury sphygmomanometers remain the gold standard
• Automated BP recorders have been also used. Require regular calibrating at regular intervals.
• 24 hours Ambulatory monitoring is useful in early pregnancy ( <20 weeks). To screen for “white coat” HT.

Classification of hypertensive disorders in pregnancy
• Gestational hypertension
• Chronic hypertension– Essential– Secondary– White coat
• Preeclampsia superimposed on chronic hypertension
• Preeclampsia- eclampsia

Gestational Hypertension
• Hypertension (HTN) which develops at or after 20/40 in women known to be normotensive at booking*, with no previous history of hypertension.
• Must be present on several readings over several hours.• Resolves within 12/52 after delivery• Generally not associated with proteinuria, although the term PIH is
still sometimes mistakenly used to mean pre-eclampsia.• Approximately 20% of women will have a blood pressure reading
above 140/90 at some stage in the second half of pregnancy: not all of them will meet the criteria for Gestational HT or require treatment beyond observation and monitoring.
* In some women with pre-existing hypertension, the normal fall in blood pressure which occurs in the first half of pregnancy may put them into the normotensive range, despite not being on any treatment.
Gestational HT continued….
• In normal pregnancy, blood pressure begins to fall in the first trimester, reaching its lowest levels around 20/40.
• This is due to a decrease in systemic vascular tone, leading to reductions in both preload and afterload.
• There is a compensatory increase in heart rate and activation of the volume-restoring mechanisms, all of which ultimately results in an increase in cardiac output of approx 40%.
• This initial drop in peripheral vascular resistance is probably mediated by oestrogens, prostaglandins, nitric oxide (and others?).
• It appears that prostaglandins reduce the efficacy of angiotensin II, which would normally cause vasoconstriction.

Gestational HT continued…• Both the systolic and diastolic blood pressures slowly rise through
the second half of pregnancy, to return to pre-pregnant levels around term.
• There may be a corresponding reduction in cardiac output.• At least some of this effect is positional, and is influenced by the
action of the gravid uterus on venous return to the heart.• A rise of > 30mmHg systolic or 15mmHg diastolic may also be
abnormal and requires close monitoring.• A systolic bp > 170 and / or diastolic > 110 is always abnormal in
pregnancy: the patient should be admitted for immediate assessment and management.

Why worry?
• If blood pressure reaches or exceeds 140/90, there is an increased risk of morbidity and mortality to both mother and fetus.
• Gest HT increases the risk of pre-eclampsia (PE), and hence careful monitoring for the development of this condition is required.
Gestational HT – Management.
• 1. Exclude PE – Ix for mother and fetus.• 2. Monitor to identify early development.• Mild to moderate HTN may not need to be treated: 140-150/90-100
can be managed with observation: treatment will not prevent the development of PE.
• Bp 170/110 is indicative of PE (in the absence of other underlying cause), and must be treated as an emergency, with admission and urgent blood pressure lowering.
• Even in this instance, treatment is aimed at preventing the maternal complications of acute hypertension, and will not prevent progression of PE.
Management
• HYPITAT trial– IOL vs. expectant management for Gest HT or
mild PE after 37 weeks– Multicentre, open-label RCT– 756 women – 377 patients in IOL group and 379 in expectant
management– In IOL group 117(31%) developed poor
maternal outcome compared with 166(44%) allocated to expectant management

HYPITAT trial
IOL(n=377) Expectant(n=379)
RR (95%CI,pvalue)
SVD 273(72%) 253(67%) 1.09(0.99-1.19,0.091)
Instrumental delivery
50(13%) 54(14%) 0.93(0.65-1.33,0.64)
CS 54(14%) 72(19%) 0.75(0.55-1.04,0.085)
No cases of maternal or neonatal death or eclampsia.No difference between the LSCS in the groups. Most LSCS were done for FTP both 1st and 2nd stage and Fetal distress.More use of antihypertensive drugs (oral or IV) in expectant group.ICU care of 6(2%) of IOL and 14(4%) of expectant group.Severe HT recorded more in expectant group (Systolic 15% vs. 23%) (Diastolic 16% vs. 27%).HELLP syndrome recorded more in expectant group(1% vs. 3%)

HYPITAT trial
• IOL is associated with improved maternal outcome and should be advised.

Essential Chronic HT
• HT confirmed before pregnancy or before 20 completed weeks gestation without a known cause.

Chronic Hypertension
• Hypertension which is present either prior to conception or 20/40.• HTN which persists 12/52 after delivery.
• May be primary or secondary: if secondary, the underlying disease process may have implications for the pregnancy (esp renal disease).
• High risk to fetus – uteroplacental insufficiency, IUGR (8-16%) placental abruption (0.7-1.5%) and pre-term delivery (12-34%).
• 20% risk of developing superimposed PE.

Chronic Hypertension
• Primary / essential / idiopathic HTN accounts for the majority of chronic HTN in adults; the causes are unknown.
• Secondary hypertension arises from an identifiable cause, and may have a specific treatment or even cure. Secondary HTN accounts for less than 10% of HTN cases seen.
• Abnormality in one or more of the systems that regulate arterial pressure (vascular, renal, hormonal and central and peripheral adrenergic systems) underlies secondary (and presumably primary) HTN.
Secondary HT
• Important causes in pregnancy– Chronic kidney disease: e.g. reflux
nephropathy, adult polycystic kidney disease– Renal artery stenosis– Systemic disease: with renal involvement
e.g. DM, SLE– Endocrine disorders e.g.
phaechromocytoma, Cushing’s syndrome and primary hyperaldosteronism
– Coarctation of the aorta.

Causes of Secondary HTN• Renal disease, both acute and chronic, carries higher risk of complications
to both mother and fetus.• Drugs eg OCP, venlafaxine, NSAIDs, corticosteroids, cyclosporin.• Primary hyperaldosteronism• Renal artery stenosis – both atherosclerotic and due to fibromuscular
dysplasia• Cushings’ syndrome• Hypothyroidism• Hyperthyroidism• Hyperparathyroidism• Phaeochromocytoma – rare, but dangerous to both if occurs.• Obstructive sleep apnoea• Coarctation of the aorta

Factors implicated in Primary HTN• Genetics: HTN about 50% more likely in people with one or both parents
hypertensive. Most likely multiple genes involved, with variations in sodium and chloride channels in renal tubules or calcium channels in smooth muscles being suggested.
• Ethnic background: Aboriginals, Torres St Islanders, Pacific Islanders + Maori more likely.
• Sodium intake: HTN seen mainly in societies where Na intake > 100meq/day (2.3g), seldom seen where it is < 50meq/day (1.2g).
• Alcohol excess
• Caffeine excess - ? In women only.
• Obesity
• Metabolic syndrome (Syndrome X).
• Low birth weight - ? Problems with renal development in utero and in early infancy.
End-organ damage in HTN 1• Acute rises in blood pressure can be associated with end-organ
damage• Malignant hypertension: retinal changes – papilloedema,
haemorrhages and exudates. Malignant nephrosclerosis, resulting in acute renal failure, haematuria and proteinuria.
• Hypertensive encephalopathy: cerebral oedema (sudden hyperperfusion due to loss of autoregulation). Presents as progressive headache, N&V, irritability, confusion, seizures and coma.
• Flash pulmonary oedema in patients with RAS.• Intracranial haemorrhage – either intracerebral or subarachnoid.• Lacunar infarcts.

End-organ damage in HTN 2• Chronic HTN causes debilitating conditions; the risk is greater if
other cardiovascular risk factors are also present.• Cerebrovascular disease: HTN is the main risk factor, and treating
blood pressure will significantly reduce the risk of stroke (both ischaemic and haemorrhagic).
• Coronary artery disease; heart attacks (MI), angina etc.• Heart failure – systolic and diastolic, with LVH, which predisposes to
arrhythmia.• Peripheral vascular disease – limb ischaemia, poor healing etc.• Retinal disease – visual loss• Renal disease – small scarred kidneys due to nephrosclerosis.
HTN also accelerates damage due to any other cause.

Ix of Chronic HTN• CBE, EUC, LFT, TFT’s, Urate and BSL.• 24hr urine collections for protein and catecholamines. If unable, should
have urinary protein:creatinine.• Spun urine for casts and sediment.• Fetal scans for growth including dopplers where relevant.• Other tests frequently done in specialist HTN clinics.
• Monitoring: bloods and urine for development of PE at approximately 4/52 intervals – more frequently if indicated.
• require regular growth scans.• Low threshold for admission (or review in DAU) if bp > 160/100 or develops
signs and symptoms of PE (even with normal blood pressure readings).

Management - Lifestyle
• Reduction in salt intake • Reduction in alcohol intake• Weight loss / maintenance within healthy range • Regular physical activity (30mins at least 5x/wk)• Smoking cessation• Dietary modification• Bed rest (while traditional) has not been shown to be
useful. Reduction in employment hours may be.

Treatment – Gestational HT and Chr HTN
• Methyldopa is the drug of first choice in a non-urgent situation: starts at 250mg daily -> 3g/day.
• Major SE’s: drowsiness / fatigue, oedema, depression / anxiety, headache, fever. Rarely causes SLE-type syndrome, haemolytic anaemia, jaundice and cytopaenias. Hypotension in the neonate may occur.
• Nifedipine, a calcium channel blocker has also been used with good effect and good outcome. Side effects include ankle swelling, facial flushing and constipation. Starts at 30mg daily (SR) -> 120mg daily.
• Labetalol, a non-selective beta blocker can also be used. Starts at 100mg bd up to 2400mg daily. There is a possibility that atenolol, a selective beta blocker, contributes to low weight babies + placentas; it is generally not used.
• Methyldopa, labetalol and nifedipine are safe for use if breast feeding.
• Diuretics, ACE-I’s, AIIRA’s contraindicated in pregnancy / lactation; enalapril has been used safely in lactating women.

Treatment continued
• In mild hypertension (BP < 150 / 100), conservative management is recommended.
• Meta-analysis has suggested that treating mild HTN does reduce the risk of severe HTN in women by 30 – 50%, and may avoid the need for additional antihypertensives.
• It provides no benefit in terms of preventing PE, pre-term delivery, SGA babies, abruption or perinatal mortality.
• There appears to be a link between treatment of mild HTN and fetal growth restriction: a 10mmHg fall in MAP was associated with an average reduction of 176g in birth weight.
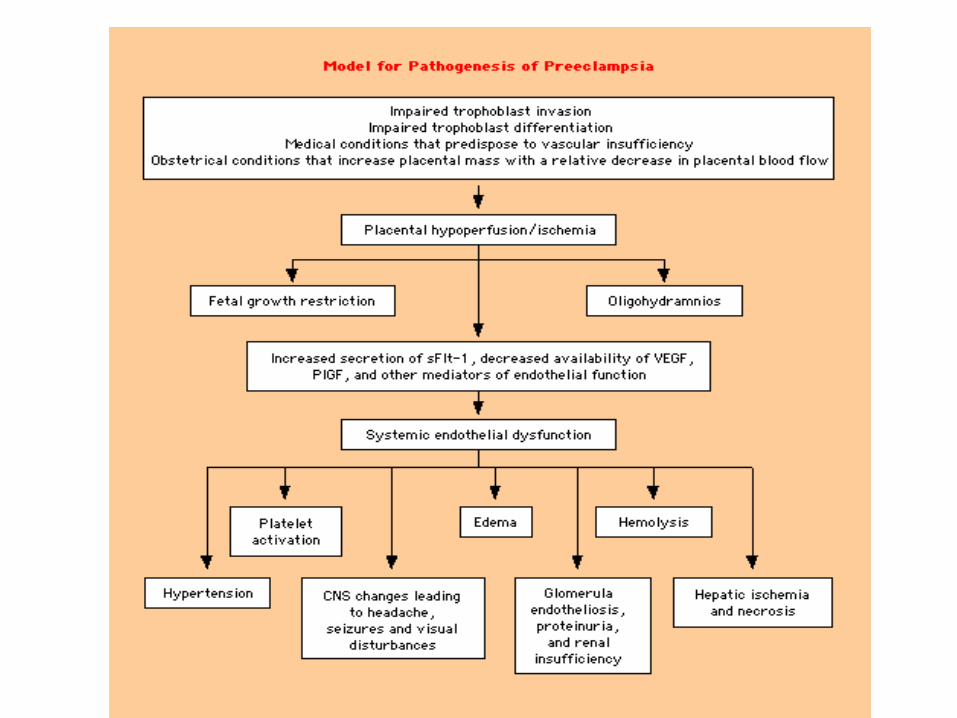
Pre-eclampsia / Eclampsia• PE is sometimes still referred to as toxaemia – a term that covers
HTN or proteinuria in pregnancy from any cause. • The exact cause or causes are unknown: PE is a disease of the
placenta (a viable fetus may not be present), and appears to be based in inadequate maternal or uteroplacental circulation.
• This leads to placental hypoxia, oxidative stress and infarction, which in turn leads to damage of the endothelium and release of multiple inflammatory and pro-coagulant factors.
• This endothelial dysfunction becomes widespread within the maternal vasculature, and leads to the varied presentation of PE.

Complications of PE
• CNS – eclamptic convulsions, cerebral haemorrhage, cerebral oedema, cortical blindness, retinal oedema, retinal detachment
• Renal – renal cortical necrosis, renal tubular necrosis, nephrotic syndrome
• Respiratory – laryngeal oedema, pulmonary oedema• Liver – jaundice, hepatic infarction, hepatic rupture,
HELLP syndrome• Coagulation system – DIC, microangiopathic
haemolysis, HELLP• Placenta – infarction and bleeding, abruption

Increased risk of PE
• Primigravida, primipaternity, increasing maternal age• Previous PE, family Hx of PE• Obesity, Metabolic syndrome, PCOS• Diabetes, HTN, chronic renal disease, antiphospholipid
syndrome and other thrombophilias, migraine, asthma• Stressful job• Advanced gestational age• Multiple pregnancy, hydatidiform mole, Trisomies.
Diagnosis of PE• New-onset of proteinuria and HTN after 20/40.• Proteinuria on dipstick has high false positive rate – need to confirm
on 24hr collection or urinary PCR.
• Symptoms include: headache, visual disturbances, nausea and vomiting, upper abdominal pain, excessive weight gain and generalised oedema (>0.5kg/wk), acute dyspnoea. There may be no symptoms.
• Signs include: IUGR, reduced urine output, pulmonary oedema, peripheral oedema, confusion, hyperreflexia and clonus.
• PE can be diagnosed in the absence of hypertension or proteinuria.
Investigations in PE
• CBE – Thrombocytopaenia, microangiopathic haemolysis, reduced plasma volume (high haematocrit)
• Urate, creatinine, urinary PCR – renal impairment• LDH, AST, ALT – liver dysfunction (HELLP)• US for fetal growth, doppler studies, amniotic fluid index.
CTG.• Ix to exclude other causes may be appropriate
Treatment
• In preeclamptic women with a gestational age > 30 weeks, significant organ dysfunction indicates the need to deliver the baby
• Before 30 week's gestation aim to prolong the pregnancy• Steroids should be given once diagnosis of PE is established if <
34/40• Progressive organ dysfunction (eg worsening LFT’s despite
treatment) is an indication for delivery• Close monitoring for variables such as blood pressure, urine output
etc.• Invasive monitoring may be required eg arterial lines, CVC’s.

Treatment
• Admission• For severe HTN (>170/110): acute blood pressure lowering
required.• Nifedipine tablets - 20 mg every 30 minutes - not > 80 mg in first 2
hours. Watch for hypotension. • Intravenous labetalol – 20mg increments up to 300mg or infusion at
1 -2 mg/min. Effective in 5 – 10 mins, lasts 3 – 6 hours. • Intravenous hydralazine – bolus or infusion• Reducing systolic BP initially by only 20-30 mm Hg and diastolic by
10-15 mm Hg should protect the mother from cerebral haemorrhage without jeopardising the fetus
• Oral nifedipine is frequently first choice, IV treatment is generally reserved for true hypertensive crisis

Treatment continued• Continuous electronic fetal monitoring during acute treatment • The risk of sudden hypotension with vasodilators such as nifedipine
can be minimised by the use of concomitant plasma expansion • Appropriate fluid replacement also required for management of
kidney and liver involvement• After initial stabilization, the following drugs could be used for
maintenance treatment: – Nifedipine - maximum daily maintenance dose 160 mg – Labetalol - maximum daily maintenance dose 3,000 mg – Methyldopa - maximum daily maintenance dose 3,000 mg
Treatment
• Neurological• Terminate ongoing convulsions with intravenous magnesium
sulphate 4 - 6 g (MgSO4) Treat blood pressure • Prophylaxis of further convulsions with magnesium sulphate, initially
intravenous 4 g loading dose followed by 1-3 g / hr for 24 hrs after birth
• The decision to start prophylactic treatment should be based on a thorough assessment of the individual's risk to develop eclamptic seizures. All women with severe hypertension should receive MgS04 during the initial stabilization

Treatment• If PE is non-threatening and stable, or < 30/40 – aim to prolong pregnancy. • PE bloods done at least 2x/wk, alternate daily or daily.• Fetal monitoring:• Ultrasound and umbilical artery Doppler velocimetry • Ultrasound estimation of fetal growth rate every 2 weeks • Doppler studies • Estimation of amniotic fluid volume • Cardiotocography (CTG) • Daily CTG • In the preterm fetus a non-reactive CTG tracing indicates the need for more
detailed biophysical monitoring • In the mature fetus a non-reactive CTG tracing may be an indication for
delivery

• In preeclampsia close to term, the fetus will usually tolerate labour and vaginal birth
• Intrapartum continuous electronic fetal monitoring is recommended
• When delivery is indicated pre-term because of severe preeclampsia, particularly when the indication for birth is fetal, delivery by caesarean section will usually be in the best interests of both baby and mother
Anaesthetic review before labour / birth

Postpartum• All of the features of preeclampsia will eventually resolve • New maternal complications may occur up to a week after birth • Women who require delivery for maternal indications usually need
monitoring in a high dependency area and laboratory tests may need repeating 4-6 hourly
• Careful monitoring of fluid balance • Oliguria should alert concern for developing post partum renal
failure • In the woman who is showing clinical improvement, blood tests are
not routinely indicated post partum • Antihypertensive drugs are usually continued but can be weaned as
the blood pressure continues to settle

And finally…..
• Recurrence is likely in up to half of women with preeclampsia or gestational hypertension, especially if this occurred early in pregnancy. Recurrent gestational hypertension may herald future essential hypertension
• Investigations for an underlying thrombophilic state, renal disease or auto-immune disease are not routinely indicated but should be undertaken in women with recurrent or early onset severe preeclampsia or if there is evidence of significant placental vasculopathy
• Future pregnancies should be managed in conjunction with a high risk pregnancy service.
• Aspirin may be of benefit in preventing recurrence.

Case 1
• 28 yo, G2P1
• First pregnancy IOL at 38 weeks for gestational HT. Forceps delivery of 2.9 kg baby girl. BP settled quickly postpartum. No medication required.
• 1st visit at 10 weeks at the hospital and BP is 170/110.

• Checked BP multiple times over the next few days.
• Started on Methyl-Dopa 250 mg TDS
• Bloods all normal. PCR normal.

• 1st Trimester maternal serum screening: low risk.
• Again seen at hospital at 15 weeks: BP 140/80
• Morphology normal
• Seen at 21 weeks and BP 180/120

• Admitted for 3 days.
• Methyldopa increased to 500 mg TDS
• BP settled to 140/80
• Bloods all normal. PCR normal
• BP in ANC at 23 weeks 170/110.
• Bloods again normal. PCR 15.
• Methyldopa increased to 500 mg QID

Review at 25 weeks.
• BP 220/120
• Mild headache. No other symptoms.
• Nifedipne 20 mg and repeated again. BP 150/100
• Bloods: Plts 130, crea 80, urate 0.40, LFT normal. PCR 2000!

• Admitted to HDU
• Ultrasound: EFW 530 gm ( <5%), AEDF, abnormal MCA doppler and DV abnormal but not reversed. AFI 8 cm.
• What to do now!

Case 2
• 27 yo• G3P0, x2 early m/c• Type I DM diagnosed age 12. On Lantus and
Novorapid. • HbA1C 5.6% at booking• Multiple Sclerosis diagnosed 18 months prior
to pregnancy• Has been on Interferon treatment for 14
months
• Folate prepregnancy• GP shared care ( country patient)• Poorly controlled diabetes during pregnancy!• Admitted at 32+6 days with headache, feeling
unwell and proteinuria. T/F to WCH.• BP 130-140/90-95• Plts normal, Crea 76, Urate 0.42, LDH 340, PCR
98.

• u/s: fetal macrosomia: EFW 1.95 Kg ( around 98%), Liquor 25 cm and dopplers normal. Breech.
• BP settled. Stable.• D/C. Stay in Adelaide• PE monitoring as outpatient. • PE remained stable. • Diabetes poorly controlled. U/S at 35+4 weeks
baby 4 Kg! AFI 30 cm. Umbilical artery doppler raised.
• BSLs high
• Decided for elective LSCS at 36 weeks.
• Baby 4260g
• Postop BP and bloods stable.
• Good recovery.