10/27/2014
1
University of New Hampshire Institute on Disability/UCED
Joan B. Beasley, Ph.D.
Integrated Health and Wellness Approaches to Challenging Behavior in Persons with IDD
Joan B. Beasley, Ph.D. Jarrett Barnhill, MD Anne D. Hurley, Ph.D. Beth Marks, RN, Ph.D.
University of New Hampshire Institute on Disability/UCED
Joan B. Beasley, Ph.D.
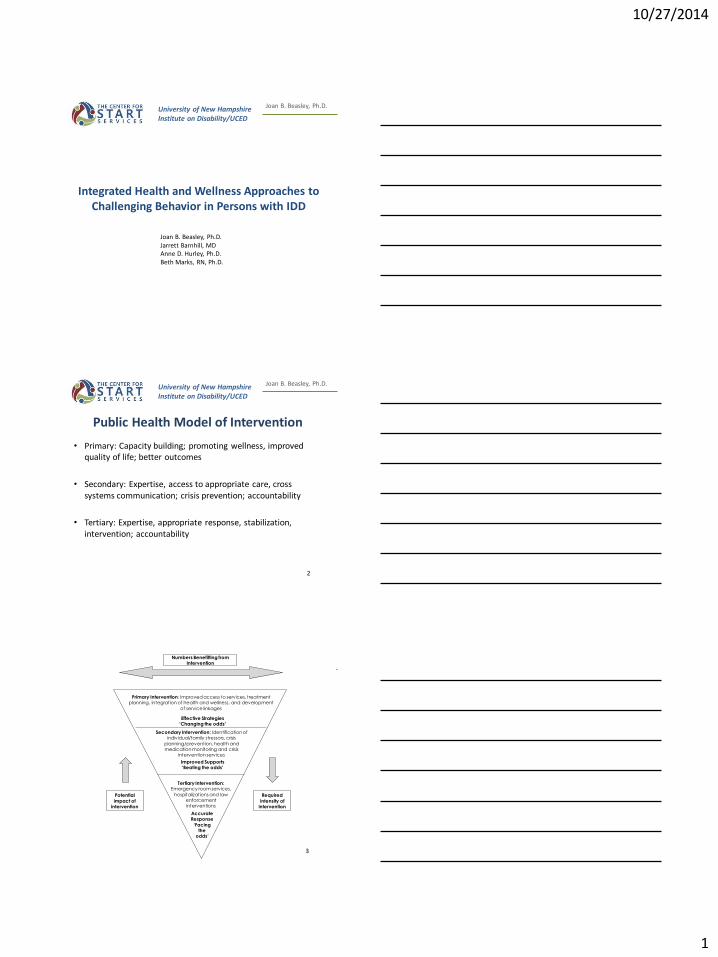
Public Health Model of Intervention
• Primary: Capacity building; promoting wellness, improved quality of life; better outcomes
• Secondary: Expertise, access to appropriate care, cross systems communication; crisis prevention; accountability
• Tertiary: Expertise, appropriate response, stabilization, intervention; accountability
2
University of New Hampshire Institute on Disability/UCED
Joan B. Beasley, Ph.D. Numbers Benefitting from
Intervention
Effective Strategies ‘Changing the odds’
Accurate Response
‘Facing the
odds’
Improved Supports
‘Beating the odds’
Potential
impact of intervention
Required
intensity of intervention
Primary Intervention: Improved access to services, treatment planning, integration of health and wellness, and development
of service linkages
Secondary Intervention: Identification of individual/family stressors, crisis
planning/prevention, health and
medication monitoring and crisis intervention services
Tertiary Intervention: Emergency room services,
hospitalizations and law enforcement interventions
3
10/27/2014
2
University of New Hampshire Institute on Disability/UCED
Joan B. Beasley, Ph.D.
Medical and Genetic Conditions : Key Players for IDD and Mental Health
Assessments
Anne Desnoyers Hurley, Ph.D.
Research Associate Professor
University of New Hampshire- Institute on Disability
4
University of New Hampshire Institute on Disability/UCED
Joan B. Beasley, Ph.D.
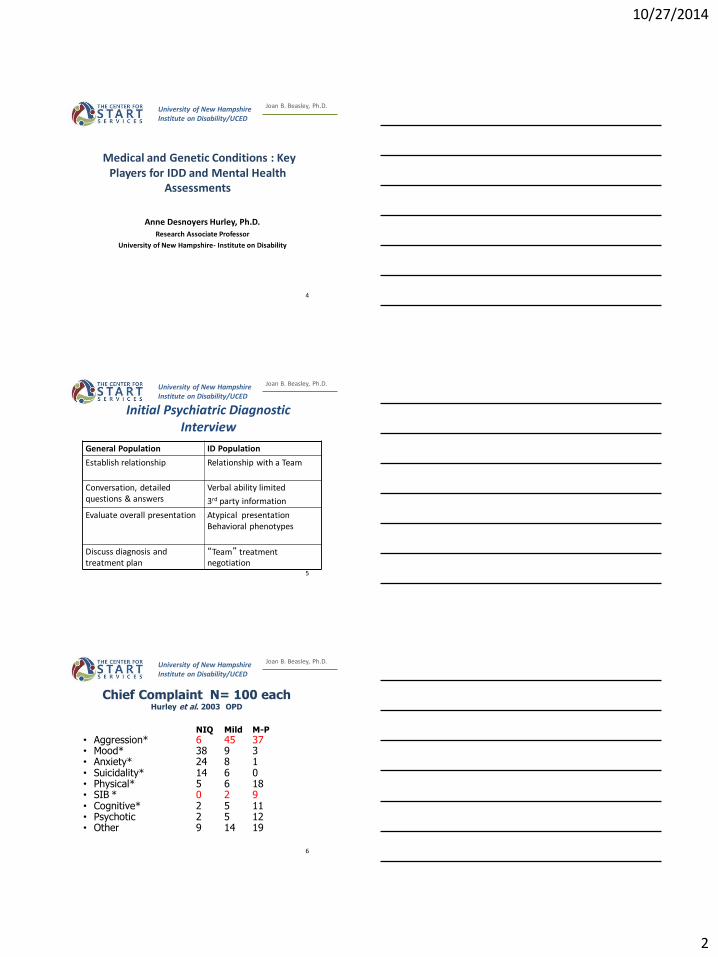
Initial Psychiatric Diagnostic Interview
General Population ID Population
Establish relationship Relationship with a Team
Conversation, detailed questions & answers
Verbal ability limited
3rd party information
Evaluate overall presentation Atypical presentation Behavioral phenotypes
Discuss diagnosis and treatment plan
“Team” treatment negotiation
5
University of New Hampshire Institute on Disability/UCED
Joan B. Beasley, Ph.D.
Chief Complaint N= 100 each Hurley et al. 2003 OPD
NIQ Mild M-P
• Aggression* 6 45 37 • Mood* 38 9 3 • Anxiety* 24 8 1 • Suicidality* 14 6 0 • Physical* 5 6 18 • SIB * 0 2 9 • Cognitive* 2 5 11 • Psychotic 2 5 12 • Other 9 14 19
6

10/27/2014
3
University of New Hampshire Institute on Disability/UCED
Joan B. Beasley, Ph.D.
7
University of New Hampshire Institute on Disability/UCED
Joan B. Beasley, Ph.D.
How Can We Improve Assessment?
• Send for all medical and educational records • Integrating instrumentation into our
assessment process • Assessment of adaptive skills and
neuropsychological testing and projective testing
• Specific tools to assess symptoms or areas, at initiation and regular follow-up
• Careful integration of psychosocial stressors and medical conditions
8
University of New Hampshire Institute on Disability/UCED
Joan B. Beasley, Ph.D.
START Formal Assessments
• ABC (Aberrant Behavior Checklist)
• RSQ (Recent Stressors Questionnaire)
• MEDS (Matson Evaluation of Medication Side Effects)
• Obtain all medical and educational records
• Case Conference Seminar for select individuals –CET Clinical Education Team
9
10/27/2014
4
University of New Hampshire Institute on Disability/UCED
Joan B. Beasley, Ph.D.
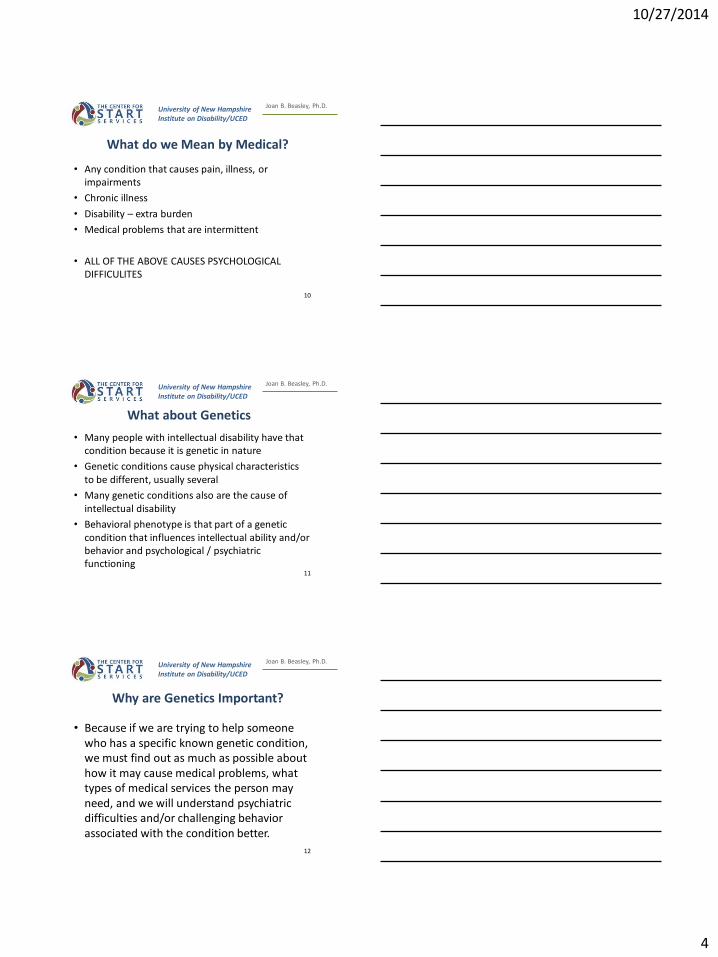
What do we Mean by Medical?
• Any condition that causes pain, illness, or impairments
• Chronic illness
• Disability – extra burden
• Medical problems that are intermittent
• ALL OF THE ABOVE CAUSES PSYCHOLOGICAL DIFFICULITES
10
University of New Hampshire Institute on Disability/UCED
Joan B. Beasley, Ph.D.
What about Genetics
• Many people with intellectual disability have that condition because it is genetic in nature
• Genetic conditions cause physical characteristics to be different, usually several
• Many genetic conditions also are the cause of intellectual disability
• Behavioral phenotype is that part of a genetic condition that influences intellectual ability and/or behavior and psychological / psychiatric functioning
11
University of New Hampshire Institute on Disability/UCED
Joan B. Beasley, Ph.D.
Why are Genetics Important?
• Because if we are trying to help someone who has a specific known genetic condition, we must find out as much as possible about how it may cause medical problems, what types of medical services the person may need, and we will understand psychiatric difficulties and/or challenging behavior associated with the condition better.
12
10/27/2014
5
University of New Hampshire Institute on Disability/UCED
Joan B. Beasley, Ph.D.
Case #1
Down Syndrome
13
University of New Hampshire Institute on Disability/UCED
Joan B. Beasley, Ph.D.
Oscar 17 yo Down syndrome
• Referred due to severe physical aggression
q 2-3 months, female staff or community
members, incontinent, fecal smearing
• 2006 psychiatric eval suggested he was
manipulative
• Axis I current: mental disorder due to
medical problems; r/o autism spectrum
disorder, r/o ODD
14
University of New Hampshire Institute on Disability/UCED
Joan B. Beasley, Ph.D.
Oscar 17 yo Down syndrome
• ADHD –age 5
• Surgical procedure, complications, psychological reactions?
• Hearing impairment
• Vision severe nearsighted, legally blind
• Psychiatric medications with no evidence of response- adverse events documented previously
• Morbid obesity, hyperlipidemia, HTN, sleep apnea, hypothyroidism
15
10/27/2014
6
University of New Hampshire Institute on Disability/UCED
Joan B. Beasley, Ph.D.
Oscar Age 17 Down syndrome
• Prevacid- 30 mg, 1x/day
• Perphenazine- 2 mg, 2 tabs 2x/day
• Levothyroxine- 150 mg 1x/day
• Clonidine- 0.1 mg in AM, 0.05 mg in PM, 0.1mg @ HS
• Abilify- 5 mg @ HS
• Clonazepam- 0.5 mg 1x/day @ HS
• Allegra - 90mg (1/2 tab) @ HS
• Melatonin 3 mg @ HS 16
University of New Hampshire Institute on Disability/UCED
Joan B. Beasley, Ph.D.
Types of Down Syndrome
• 95% of people with Down syndrome have trisomy 21– 3 copies of chromosome #21
• 4% have Robertsonian translocation because part of #21 attached to another chromosome, e.g., #14
• 1% have mosaicism because only some cells have 3 copies of #21: they may have milder features
17
University of New Hampshire Institute on Disability/UCED
Joan B. Beasley, Ph.D.
Epidemiology
• >60% spontaneously aborted
• 20% stillborn
• 1983: 9.5 in 10,000 live births
• 2003: 11.8 in 10,000 live births
18
10/27/2014
7
University of New Hampshire Institute on Disability/UCED
Joan B. Beasley, Ph.D.
Down Syndrome Phenotype
• Short stature
• Broad neck
• Small hands
• Epicanthal folds on eyes
• Upslanting palpebral fissures
• Flat nasal bridge
• Small mouth
• Brachicephaly
19
University of New Hampshire Institute on Disability/UCED
Joan B. Beasley, Ph.D.
Down Syndrome Behavioral Phenotype
• Intellectual Disability mild-moderate
• Extroverted, highly social
• Impulsive, insistent
• Ability in reading, math, daily living skills
outstrips predictions based on IQ testing
• More than 10% have Autism
• “Ambitious”
20
University of New Hampshire Institute on Disability/UCED
Joan B. Beasley, Ph.D.
• Scottish award-winning film & TV actress Paula Sage receives award with Brian Cox-- Wikipedia BAFTA Scotland
21
10/27/2014
8
University of New Hampshire Institute on Disability/UCED
Joan B. Beasley, Ph.D.
Anxiety Disorders “Internalizers”
• Panic dx
• Agorophobia
• OCD
• Obsessional slowness
22
University of New Hampshire Institute on Disability/UCED
Joan B. Beasley, Ph.D.
Active/Inattentive-Extroverted “Externalizers”
• ADHD
• May be linked to problems in
expressive-receptive language
frustration and perception of
being “stubborn”
23
University of New Hampshire Institute on Disability/UCED
Joan B. Beasley, Ph.D.
Common Medical Problems
• Hearing impairment ✓
• Visual limitations ✓
• Fine & gross motor ✓
• Congenital heart disease ✓
• Depression
• Anxiety disorders
• Early aging
• Celiac disease
• Hypothyroidism ✓
• Osteoarthritis
• Eczema
• Seizures
• Obesity ✓
• Sleep apnea ✓
• Diabetes
• Alzheimer’s disease
• Constipation
• GERD✓
24
10/27/2014
9
University of New Hampshire Institute on Disability/UCED
Joan B. Beasley, Ph.D.
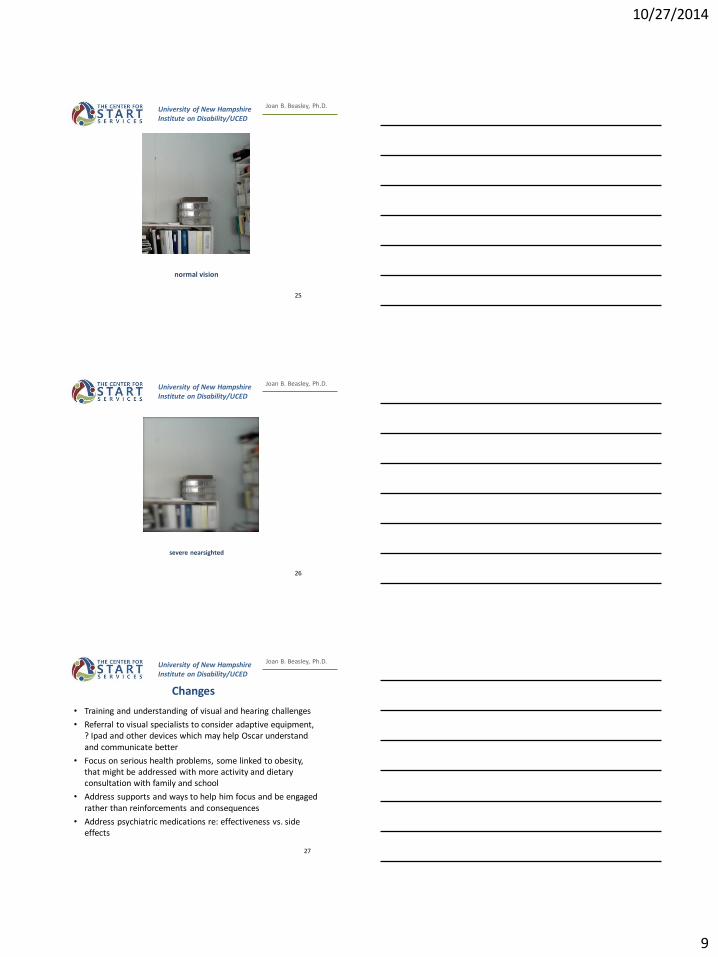
normal vision
25
University of New Hampshire Institute on Disability/UCED
Joan B. Beasley, Ph.D.
severe nearsighted
26
University of New Hampshire Institute on Disability/UCED
Joan B. Beasley, Ph.D.
Changes
• Training and understanding of visual and hearing challenges
• Referral to visual specialists to consider adaptive equipment, ? Ipad and other devices which may help Oscar understand and communicate better
• Focus on serious health problems, some linked to obesity, that might be addressed with more activity and dietary consultation with family and school
• Address supports and ways to help him focus and be engaged rather than reinforcements and consequences
• Address psychiatric medications re: effectiveness vs. side effects
27
10/27/2014
10
University of New Hampshire Institute on Disability/UCED
Joan B. Beasley, Ph.D.
Resources
Guide for Parents of Teens and Young Adults with Down Syndrome Association of West Michigan
616- 956-3488 • 866-665-7451 (toll-free)
http://www.kcdsg.org/files/content/Guide%20for%20Teens%20and%20Adults%20with%20Down%20Syndrome.pdf
European Down Syndrome Association
Health Care Guidelines for People with Down Syndrome
http://www.edsa.eu/files/essentials/edsa_essentials_2_healthcare.pdf
28
University of New Hampshire Institute on Disability/UCED
Joan B. Beasley, Ph.D.
Case #2
F-G syndrome
Opitz–Kaveggia syndrome
29
University of New Hampshire Institute on Disability/UCED
Joan B. Beasley, Ph.D.
George 30’s Mild ID
• Lives in 24-hr staffed apartment, gets upset easily, bangs on walls, pulls staff into debate with no end
• Speaks well, but often too quickly
• Can be “manipulative”
• Had 3 psychiatric hospitalizations, talks about spirits that calm him
• Short attention span, obsessive compulsive behaviors that must be repeated
30
10/27/2014
11
University of New Hampshire Institute on Disability/UCED
Joan B. Beasley, Ph.D.
Strengths - Challenges
• Can speak well verbally
• Has interests such as sports, fishing, shopping, wrestling
• Likes to dress as a “gangster”
• Trouble with constipation, bedwetting, complains of heartburn
• Still upset about girlfriend who died 4 years ago
• Has 2 part time jobs
31
University of New Hampshire Institute on Disability/UCED
Joan B. Beasley, Ph.D.
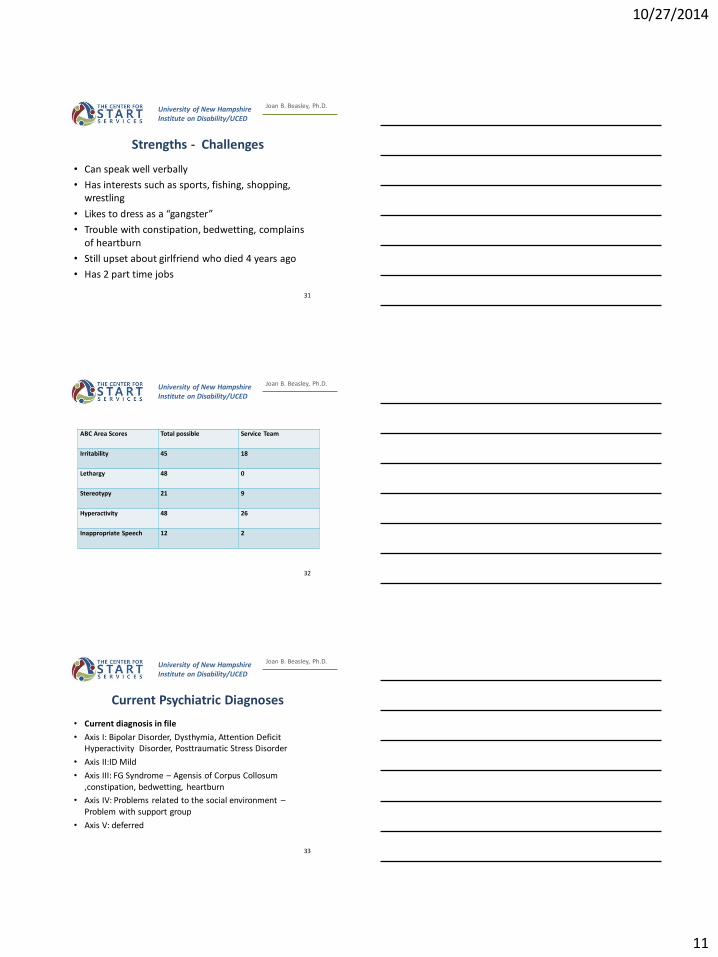
ABC Area Scores Total possible Service Team
Irritability 45 18
Lethargy 48 0
Stereotypy 21 9
Hyperactivity 48 26
Inappropriate Speech 12 2
32
University of New Hampshire Institute on Disability/UCED
Joan B. Beasley, Ph.D.
Current Psychiatric Diagnoses
• Current diagnosis in file
• Axis I: Bipolar Disorder, Dysthymia, Attention Deficit Hyperactivity Disorder, Posttraumatic Stress Disorder
• Axis II:ID Mild
• Axis III: FG Syndrome – Agensis of Corpus Collosum ,constipation, bedwetting, heartburn
• Axis IV: Problems related to the social environment – Problem with support group
• Axis V: deferred
33
10/27/2014
12
University of New Hampshire Institute on Disability/UCED
Joan B. Beasley, Ph.D.
• Ranitidine HCL 1 50mg BID, GERD
• Colace/Doc-Q-Lace 100mg Daily constipation
• Ditropan XL/ 10mg QHS incontinence
• Levothyroxine sodium 50mcg Daily hypothyroid
• Lamictal/Lamotrigine 300mg QHS
• Risperdal/risperidone 1mg BID
• Risperdal/risperidone 1 mg Q 24 PRN agitation
• Risperdal 3mg HS
• Propanolol HCL 10mg TID
• Tenex/Guanfacine 1mg TID ry
• Simethicone 125mg Q 8 hr PRN bloating
34
University of New Hampshire Institute on Disability/UCED
Joan B. Beasley, Ph.D.
Genetics Home Reference page Rare Diseases Information NIH
• 5 regions of the X chromosome are involved
• The condition is called FGS1 when it is caused by a change (mutation) in a gene MED12
• FGS2 is caused by mutations in the FLNA gene. The genes responsible for FGS3, FGS4, and FGS5 remain unknown. FGS is inherited in an X-linked recessive pattern
35
University of New Hampshire Institute on Disability/UCED
Joan B. Beasley, Ph.D.
autosomal recessive inheritance wikipedia
36
10/27/2014
13
University of New Hampshire Institute on Disability/UCED
Joan B. Beasley, Ph.D.
FG Syndrome- Physical Problems
• Feature of facial configuration
• Macrocephaly
• Undescended testicles
• Broad thumbs and large great toes
• Cardiac defects
• Low muscle tone or hypotonia
• Intestinal and anal abnormalities and severe constipation
• Often die in infancy
• Inguinal hernia
• Reflux
• Limb defects
37
University of New Hampshire Institute on Disability/UCED
Joan B. Beasley, Ph.D.
FG Syndrome - Behavioral Phenotype-Neurological Problems
Intellectual disability, mild to severe
Outgoing personality
Extreme hyperactivity
Abnormalities in corpus collosom
Seizure disorder
Low muscle tone – hypotonia
Self-absorption and fascinations with mechanical toys and objects, Autism Spectrum Disorder
Demanding of attention
Becomes “unglued” by little changes 38
University of New Hampshire Institute on Disability/UCED
Joan B. Beasley, Ph.D.
• Kim Peek (1951-2009) was a “savant” of exceptional ability
• Exceptional memory (could memorize an entire book at an early age) and social difficulties
• He had agenesis of the corpus collosom and FG syndrome
• Screen writer for Rain Man met him
• http://www.youtube.com/watch?v=k2T45r5G3kA Kim Peek video
39
10/27/2014
14
University of New Hampshire Institute on Disability/UCED
Joan B. Beasley, Ph.D.
Kim Peek basis of Rain Man wikipedia
40
University of New Hampshire Institute on Disability/UCED
Joan B. Beasley, Ph.D.
Changes
• GI specialist re: underlying conditions contributing to his problems in this area + other medical recommendations
• Discuss reducing d/c risperidone
• Provide more consistency in choices & activities
• Staff to be coached in dealing with “arguments” and rigid thinking
• Alter expectations re: his independence
• Counseling re: loss and past difficulties
41
University of New Hampshire Institute on Disability/UCED
Joan B. Beasley, Ph.D.
Final Points
• All people that we help are not able to speak for/ or advocate for themselves as well as typical people
• Not only are their wishes and dreams often inaccessible, they are unable to relate information and symptoms in psychiatric settings and also in medical settings
42

10/27/2014
15
University of New Hampshire Institute on Disability/UCED
Joan B. Beasley, Ph.D.
Final Points
• Often medical problems are a source of “challenging behavior” and/or “psychiatric problems”
• Behavioral phenotypes explain many difficulties and must be considered
43
University of New Hampshire Institute on Disability/UCED
Joan B. Beasley, Ph.D.
Final Points
• A thorough medical evaluation must be initiated for people with ID and challenging behavior and/or psychiatric symptoms
• We must help everyone to see the individuals we help through a personal understanding of their lives… how would it be if I were born legally blind? How do we help someone who is neurologically different in a way that causes him to be just as he is and accept his inability to be as we wish?
44
University of New Hampshire Institute on Disability/UCED
Joan B. Beasley, Ph.D.
Resilience: A Complex Neurodevelopmental Phenomenon
Jarrett Barnhill MD, DLFAPA, FAACAP, NADD-CC University of North Carolina
Chapel Hill, NC Medical Director, National Center fore START Services
UNH/IOD
45
10/27/2014
16
University of New Hampshire Institute on Disability/UCED
Joan B. Beasley, Ph.D.
Goals
• Basic differences between risk/vulnerability/predisposed and resilience
• Concept of developmental windows for vulnerability, resilience and emerging cognitive, emotional and practical skills
• Complex traits have complex genetics, understanding of gene-environment interactions - an ecological model
• What can we do about building resilience - treat v. state
46
University of New Hampshire Institute on Disability/UCED
Joan B. Beasley, Ph.D.
What is Resilience?
• A dynamic process that contributes to a positive adaptation to significant adversity
• Why don’t monozygotic twins have a 100% concordance for psychiatric disorders - shared/non-shared environments, long-term v. short-term differences; probabilistic not deterministic
• A fluid-dynamic process, nodal points in the risk/predisposing- protective/perpetuating processes
• Begins in infancy - synchrony, attunement, attachment, movement towards autonomy
• How does ID affect to this developmental trajectory
47
University of New Hampshire Institute on Disability/UCED
Joan B. Beasley, Ph.D.
Many Faces of Resilience
• Immunity to many disease states - HIV/AIDS resistant noted with Chemokine-5 receptor prevents the virus from entering the cell
• Dementia - APOE e2/4 ratio; cognitive reserve; exercise, dietary health - relationship to aging (Trisomy 21)
• Trauma and Stress Related disorders - early parenting/attachment/temperament; relationship to gene X environment interaction; capacity to elicit protective responses from others; early intervention - 10-15% develop PTSD
• Individuals with genetic risks for severe mental disorders but who never develop the syndrome
• Intellectual Disabilities - cognitive, emotional, practical skills v. deficits
48

10/27/2014
17
University of New Hampshire Institute on Disability/UCED
Joan B. Beasley, Ph.D.
Complex Developmental Trajectory of Resilience
• Trajectory of vulnerability/mastery development - phase specific stressors challenged and help organize adaptive skills
• The evolution of parent-infant attachment, synchrony, reciprocity and temperament play key roles in the organization of CNS, stress response systems and development of late emerging executive and fluid intelligence
• Relationship to neuroplasticity, critical periods, turning points
• Events that disrupt this trajectory can be biological, psychological, and social but need to be specified - if we do not adapt our thinking to integrate new information the bio-psycho-social model can become a cliché
49
University of New Hampshire Institute on Disability/UCED
Joan B. Beasley, Ph.D.
Resilience as a Complex Behavioral Trait
• Brain development - top down regulation of perception, emotion, language, memory and executive function
• Polygenic/ pleiotropic - complex gene environment interactions
• Brain as an organ of social adaptability developing in a social context - stress response system, neuroendocrine regulation
• Temperament: beh. inhibition, extroversion/introversion, novelty
• Attachment - secure, ambivalent, disorganized/avoidant
50
University of New Hampshire Institute on Disability/UCED
Joan B. Beasley, Ph.D.
Social-Cultural Issues
• Ecological model - developmental changes in levels of socialization, expectations, expansion of basic attachment to social and cultural factors
• Synchrony, oxytocin/vasopressin and belonging
• Access to material resources; relationships, identity, cohesion, power and control, cultural adherence, social justice
• Level of environmental “enrichment”
• Impact of changing demands, culture change and loss of effective rituals
51
10/27/2014
18
University of New Hampshire Institute on Disability/UCED
Joan B. Beasley, Ph.D.
What Can We Do - Enhancing Resilience?
• Design program in ecological and developmental contexts
• Identify most at risk children and intervene early, safety needs
• Adapt programs to developmental age, temperamental matching the changing trajectory of attachment needs
• Adapt therapy to pulsed interventions that concentrate of maximizing critical periods
• Shift from a pathology focus to an adaptive one - flexibility of programs
• Modification of the developmental process, alter gene effects
52
University of New Hampshire Institute on Disability/UCED
Joan B. Beasley, Ph.D.
Reference:
Carrey N Ungar M (Eds). Resilience. Child and Adolescent Psychiatric Clinics of North America, 2007, Philadelphia: Elsevier Saunders. 16(2).
53
HealthMatters Program: Turning Evidence into Sustainable Practice for People with
Developmental Disabilities
Beth Marks, PhD, RN
NADD Pre-conference Integrated Health and Wellness Approaches to Challenging Behavior in Persons with IDD
San Antonio, Texas November 12, 2014 54
10/27/2014
19
Getting the Memo
Real People – Health
promotion for people with intellectual and
developmental disabilities (I/DD) and psychiatric disabilities
Practical Solutions – Evidence based practice for community services
Real Changes – Support for long-term
lifestyle changes
Copyright ©2014 HealthMattersProgram.org
55
Real People
• People with I/DD are more overweight and obese compared to the general population.
• Paid caregivers experience stress and burnout
• poor health
• emotional problems
• unhealthy lifestyles
• poor quality of life
Copyright ©2014 HealthMattersProgram.org
Did you know that 36% of all
American adults are obese?
56
Mental Health, Morbidity & Mortality
CVD, acute & chronic pulmonary disease, accidents, suicide, cancer,
diabetes, liver disease, and septicemia
Smoking, obesity, & sedentary lifestyles
Die on average between 13.5 and 32.2 years earlier than general population
Biological pathways & chronic stress with mental illness
increased pituitary activity, cortisone levels, & proinflammatory factors
strokes and heart attacks, and abnormalities of the autonomic nervous system that might lead to more heart disease and sudden death issues.
1. Medical evaluation of psychiatric patients. Results in a state mental health system.Arch Gen Psychiatry1989; 46:733–740. 2. Wayne Katon, MD, Department of Psychiatry and Behavioral Sciences at the University of Washington School of Medicine
57
10/27/2014
20
Main Causes of Obesity
• Medications that cause weight gain
• Less physical activity
• Genetics – lower muscle tone
• Environment – having the opportunity to eat and move
o Controlling food choices
o Choosing activity or exercise
Handout 2: Genetics, Lifestyle and Obesity 58
Primary Care is Reactive
Difficult for people who are reluctant, or unable, to seek help
Short consultation times
Physical exams are difficult for people who may be vague or suspicious
Emphasis often on psychological and social issues if mental health providers are present
Preventive and promotive health services often absent
1. Medical evaluation of psychiatric patients. Results in a state mental health system.Arch Gen Psychiatry1989; 46:733–740. 2. Wayne Katon, MD, Department of Psychiatry and Behavioral Sciences at the University of Washington School of Medicine
59
It’s Everyone’s Job
Lifelong culture of interdependency
Expectations and the tyranny of none
Power to impact health status and determine health practices
60

10/27/2014
21
Community Engagement Matters
• Developing and implementing evidence-based community-based health promotion programs.
• Sustaining evidence- based programs across community sectors.
• Parity in health status and equity in health care services for people with I/DD.
61
9
Where People Live Matters
American Heart Association and American Stroke Association. (2009). Cardiovascular Diseases in the United States: 2009, retrieved from www.americanheart.org/downloadable/heart/1238516653013CVD_Stats_09_final%20single%20pages%20%282%29.pdf
Copyright ©2014 HealthMattersProgram.org
Total Cardiovascular Disease Deaths, 2005/100,000 population
62
Health Promotion
• Enable people to take control over and to improve their health.
• Build capacity within CBOs and communities:
Access to affordable and available health care.
Acceptable culturally relevant and satisfactory health care.
63
10/27/2014
22
Disability and Health Status
While a large proportion of persons
who are in bad health end up with a disability,
a large number
of people with
disabilities end up with bad health.
65
Knowledge Lost in Translation
• Information gap
oSlow or no reach to people receiving services
oGood questions are asked – but not reaching academia.
• Gaps for groups:
owomen oracial/ethnic minorities oother high-risk groups in the
US healthcare system – people with disabilities
Lenfant C. Clinical Research to Clinical Practice - Lost in Translation? N Engl J Med 2003;349:868-74.
Dispelling Myths…
Myths
People with I/DD are sick.
Chronic conditions (e.g., obesity, hypertension, diabetes) are disability related.
Lifestyle habits are impossible to change.
Facts
People with I/DD see themselves as healthy.
Chronic conditions are lifestyle related (e.g., sedentary, poor diets, lack of opportunity).
Health promotion strategies work!
...…Changing Attitudes
66
10/27/2014
23
Determining Health Needs and Interests
• Biological factors – syndrome and gender- related conditions
• Behavioral practices
• Access to health care services and programs
– Physical, attitudinal, programmatic, and communication/literacy
• Socio-economic and environmental issues
67
Beyond Personal Health Practices
• Sustainable health promotion programs
o “Point of View” for Health
o Behaviors most often influenced by broader socio-environmental and economic factors
o “Where the people are…”
• Community Coalitions
o Social capital – sense of trust and long-term reciprocity
68
Health and Equity
Translating Evidence-Based Health Promotion Practice to Policy
There has been a lack of bi-directionality (sort of) because your research is yours (rightly so) and our comments may be helpful to you or not, but may not have significant influence on your process in the end.
~ Leslie Hoelzel, Grant Manager, ARCA
Translating Evidence-Based Health Promotion Research to Practice
There has been a lack of bi-directionality (sort of) because your research is yours (rightly so) and our comments may be helpful to you or not, but may not have significant influence on your process in the end.
~ Leslie Hoelzel, ARCA
69
10/27/2014
24
1.Community ignored
2.Community placed
3.Community informed
4.Community as partners
Community Partnerships: “Won’t-Take-Failure-for-an-answer”
70
Aging, Disability, and Aging with a Disability
Currently 641,000 adults age 60 and older.
Projected increase of 90% to 1.2 million age 60+ by 2030.
Individuals with I/DD who have lived 30-50 years with a disability are experiencing new health concerns.
Copyright ©2014 HealthMattersProgram.org
71
Adults living in community settings have the
highest CVD risk of all
adults with I/DD.
CVD is strongly associated
with health behaviors –
specifically poor nutrition
and lack of physical activity.
CVD and People with I/DD
Cardiovascular disease (CVD) is one of the most common causes of death.
Copyright ©2014 HealthMattersProgram.org
72
10/27/2014
25
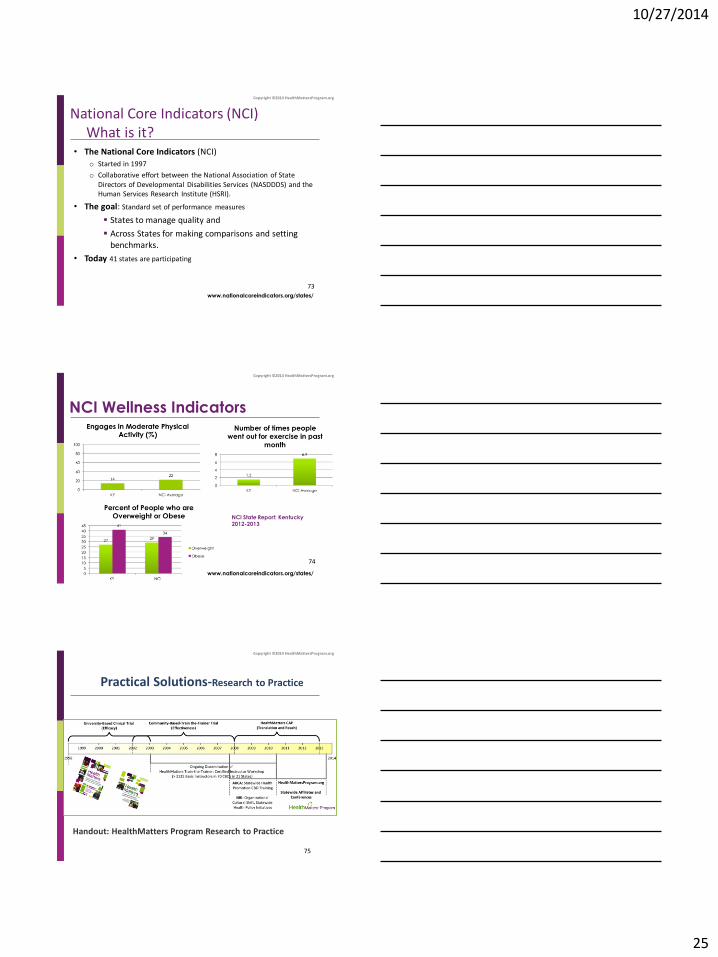
National Core Indicators (NCI) What is it?
• The National Core Indicators (NCI)
o Started in 1997
o Collaborative effort between the National Association of State Directors of Developmental Disabilities Services (NASDDDS) and the Human Services Research Institute (HSRI).
• The goal: Standard set of performance measures
States to manage quality and
Across States for making comparisons and setting benchmarks.
• Today 41 states are participating
Copyright ©2014 HealthMattersProgram.org
www.nationalcoreindicators.org/states/
73
NCI Wellness Indicators
www.nationalcoreindicators.org/states/
Copyright ©2014 HealthMattersProgram.org
NCI State Report: Kentucky 2012-2013
74
Practical Solutions-Research to Practice
Copyright ©2014 HealthMattersProgram.org
Handout: HealthMatters Program Research to Practice
75

10/27/2014
26
HealthMatters Program: Research Trials
University-Based Program
Professional Led
Community-Based
Program Train-the-Trainer
Adults with I/DD
exercise attitudes
exercise self-efficacy
exercise outcome expectations
life satisfaction
cardiovascular fitness, strength and
endurance
cognitive–emotional barriers
Heller, et al., (2004); Rimmer, et al., (2004)
Adults with I/DD
perceived health behaviors
exercise self-efficacy
nutrition/activity knowledge
cholesterol & glucose
fitness (flexibility)
exercise & nutrition socio-
environmental supports
Marks, Sisirak, Chang (2013)
Copyright ©2014 HealthMattersProgram.org
76
Health and Exercise – What can HealthMatters Do?
Example Goal
Increase the overall
percentage of recipients who
engage in moderate
physical activity for
30 minutes a day at
least three times per week by at least 5%.
Strategies to Meet Goal
* Structured activities within day services (12-week
HealthMatters Program) * Partnership with community recreation centers
* Targeted health education programs
Copyright ©2014 HealthMattersProgram.org
77
HealthMatters Train the Trainer Workshop: Becoming a Certified Instructor
• Theoretically-driven Workshop
• Strategies to teach exercise and nutrition classes and motivate people to achieve wellness goals
• Tools to evaluate changes in health
Handout: Workshop Brochure
Copyright ©2014 HealthMattersProgram.org
CEUs are provided for Advance Practice Nurses,
Registered Nurses, Licensed Practical Nurses, Social
Workers (LCSW, LSW, LPC, LCPC), Nursing Home
Administrators, Speech Language Pathologists, Physical
Therapists, Occupational Therapists, Recreational
Therapists, and Qualified ID Professionals (QIDP).
78
78
10/27/2014
27
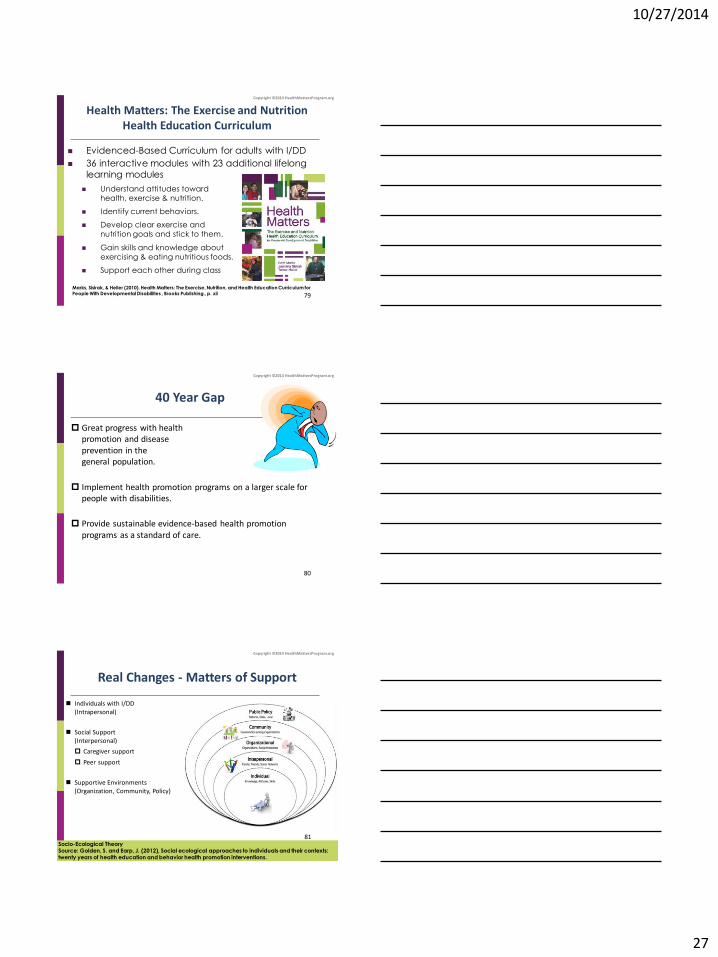
Health Matters: The Exercise and Nutrition Health Education Curriculum
Evidenced-Based Curriculum for adults with I/DD
36 interactive modules with 23 additional lifelong
learning modules
Understand attitudes toward health, exercise & nutrition.
Identify current behaviors.
Develop clear exercise and nutrition goals and stick to them.
Gain skills and knowledge about exercising & eating nutritious foods.
Support each other during class
Marks, Sisirak, & Heller (2010). Health Matters: The Exercise, Nutrition, and Health Education Curriculum for
People With Developmental Disabilities , Brooks Publishing., p. xii
Copyright ©2014 HealthMattersProgram.org
79
40 Year Gap
Great progress with health promotion and disease prevention in the general population.
Implement health promotion programs on a larger scale for people with disabilities.
Provide sustainable evidence-based health promotion programs as a standard of care.
Copyright ©2014 HealthMattersProgram.org
80
Real Changes - Matters of Support
Individuals with I/DD (Intrapersonal)
Social Support (Interpersonal)
Caregiver support
Peer support
Supportive Environments (Organization, Community, Policy)
Socio-Ecological Theory Source: Golden, S. and Earp, J. (2012), Social ecological approaches to individuals and their contexts: twenty years of health education and behavior health promotion interventions.
Copyright ©2014 HealthMattersProgram.org
81
10/27/2014
28
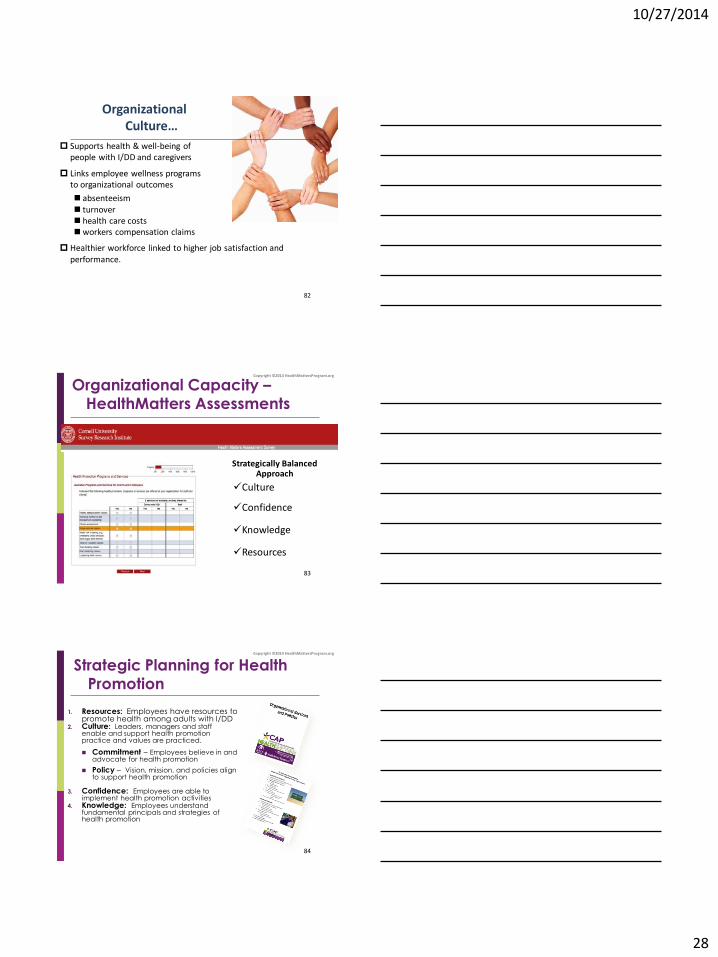
Organizational Culture…
Supports health & well-being of people with I/DD and caregivers
Links employee wellness programs to organizational outcomes
absenteeism turnover health care costs workers compensation claims
Healthier workforce linked to higher job satisfaction and performance.
82
Strategically Balanced Approach
Culture
Confidence
Knowledge
Resources
Organizational Capacity – HealthMatters Assessments
Copyright ©2014 HealthMattersProgram.org
83
1. Resources: Employees have resources to
promote health among adults with I/DD 2. Culture: Leaders, managers and staff
enable and support health promotion practice and values are practiced.
Commitment – Employees believe in and advocate for health promotion
Policy – Vision, mission, and policies align to support health promotion
3. Confidence: Employees are able to
implement health promotion activities 4. Knowledge: Employees understand
fundamental principals and strategies of health promotion
Strategic Planning for Health Promotion
Copyright ©2014 HealthMattersProgram.org
84
10/27/2014
29
Signs&Symptoms Program: Early Recognition of Health Problems
Increase continuity of care within day/residential CBOs.
Instruct caregivers to observe early signs and symptoms of new or changing health concerns among people with I/DD.
85
HealthAdvocacy for Providers, Families, and People with I/DD
Increase understanding of health care experiences and needs among adolescents and adults with I/DD
Improve culturally relevant care
86
Peer to Peer HealthMessages Program
Teach people with I/DD to become Healthy Lifestyle Coaches (HLCs)
Mentors support HLCs to implement a 12-week HealthMessages Program for peers.
12 week program
87
10/27/2014
30
HealthMatters 4Kids: Today Counts
Diabetes Prevention Workshop
Introduces health promotion and health advocacy for children and adolescents with I/DD
Developed by Northpointe Resources in collaboration with HealthMatters Program at UIC.
Audience
Parents/Caregivers, Educators, and Healthcare Providers who support children with I/DD.
88
Scaling-Up Evidence-Based Programs
• Facilitate buy-in, fiscal accountability, and policy support from stakeholders
• Understand facilitators and barriers for scale-up
• Achieve widespread translation in CBOs for reach, effectiveness, adoption, implementation and maintenance of program
89 89
HealthMatters: Scale-Up Research Project
A 5year research study evaluating the usefulness of an interactive webinar (Health Matters Program: Train the Trainer online course).
Aimed at staff working in community-based organizations providing services to people I/DD.
90
10/27/2014
31
Study Objectives
This study will help us learn how we can best deliver webinar training
to give staff in community-based organizations the necessary skills to:
Assist individuals with I/DD to develop their health promotion goal.
Develop and teach a physical activity, nutrition, and health education program for individuals with I/DD to reach their health promotion goal.
Support individuals with I/DD to make long-term lifestyle changes
Copyright ©2014 HealthMattersProgram.org
91
Contact
Beth Marks
312-413-4097
www.HealthMattersProgram.org
92







