discussion pancreatic cancer abstracts 145, lba146, 147, & lba148 philip agop philip, md, phd,...
TRANSCRIPT
DiscussionPancreatic Cancer
Abstracts 145, LBA146, 147, & LBA148
Philip Agop Philip, MD, PhD, FRCP
Karmanos Cancer Center
Wayne State University
Detroit, Michigan
Randomized phase III trial of adjuvant chemotherapy with gemcitabine vs. S-1for resected pancreatic cancer patients
(JASPAC 01 study)
K. Uesaka, et al.Japan Adjuvant Study Group of Pancreatic Cancer (JASPAC)
Abstract #145
#145 2013 ASCO GI
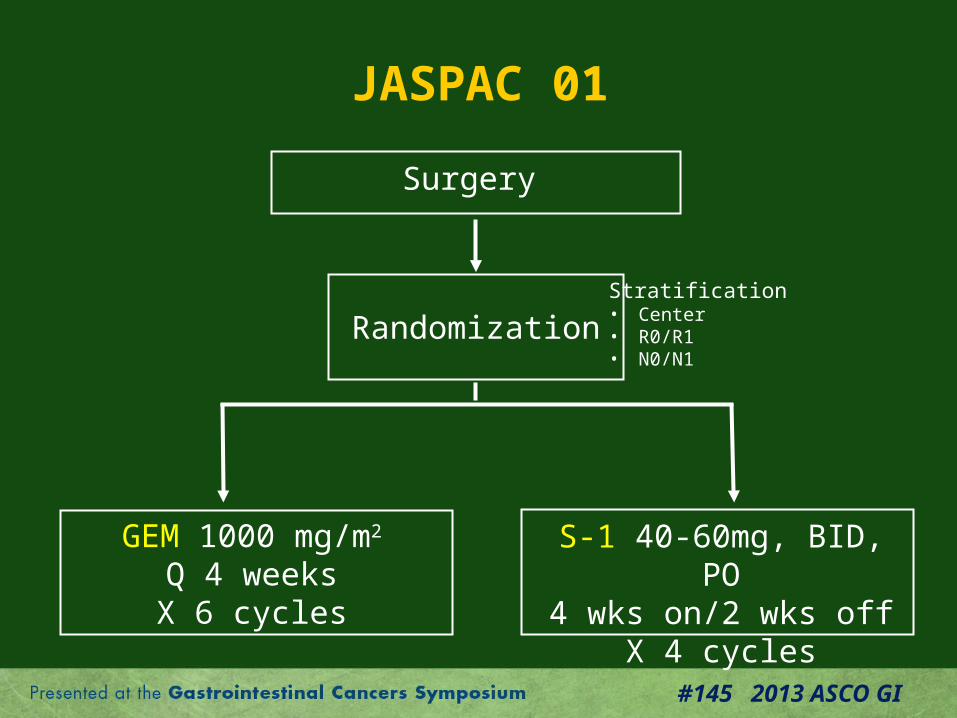
JASPAC 01
Randomization
GEM 1000 mg/m2
Q 4 weeksX 6 cycles
S-1 40-60mg, BID, PO4 wks on/2 wks off
X 4 cycles
Surgery
Stratification• Center• R0/R1• N0/N1
#145 2013 ASCO GI
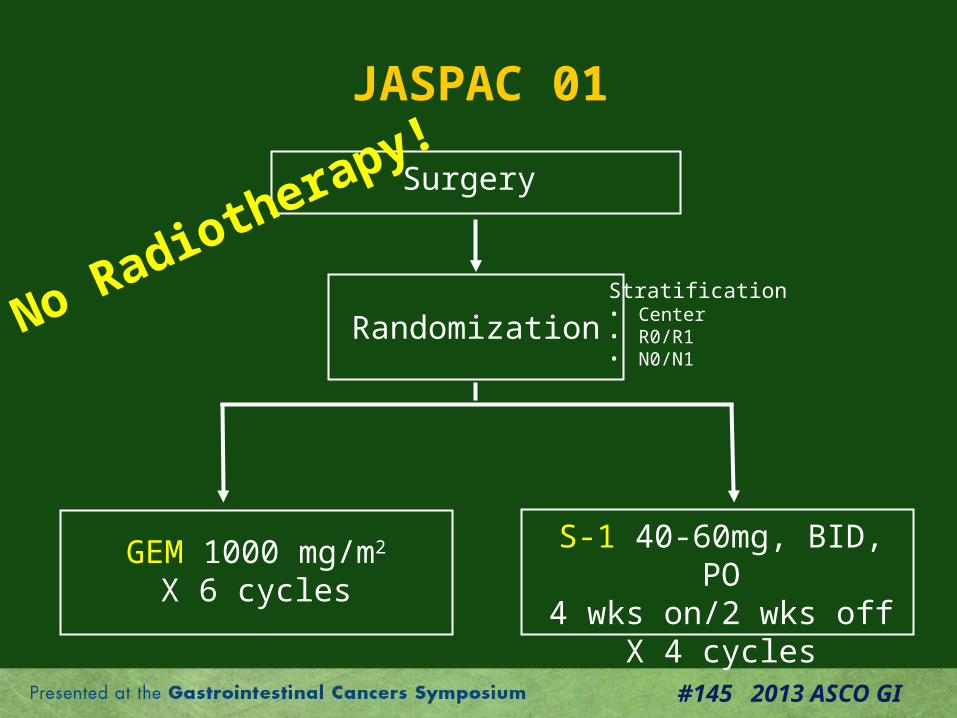
JASPAC 01
Randomization
GEM 1000 mg/m2
X 6 cycles
S-1 40-60mg, BID, PO4 wks on/2 wks off
X 4 cycles
Surgery
Stratification• Center• R0/R1• N0/N1
No Radiotherapy!
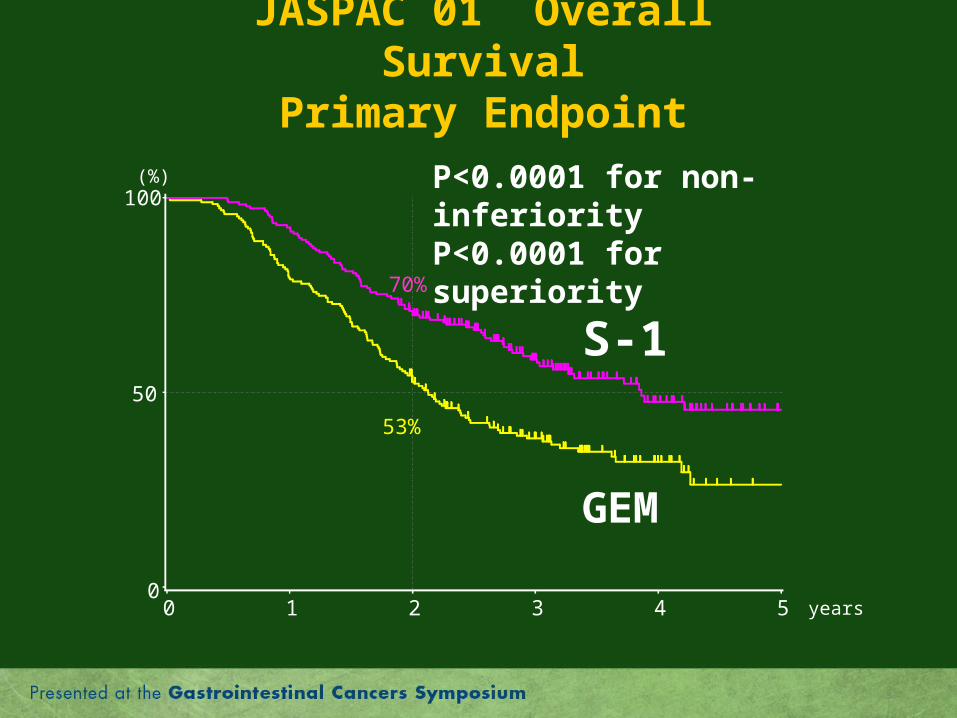
JASPAC 01 Overall SurvivalPrimary Endpoint
0
50
100
0 1 2 3 4 5 years
(%) P<0.0001 for non-inferiorityP<0.0001 for superiority
70%
53%
S-1
GEM
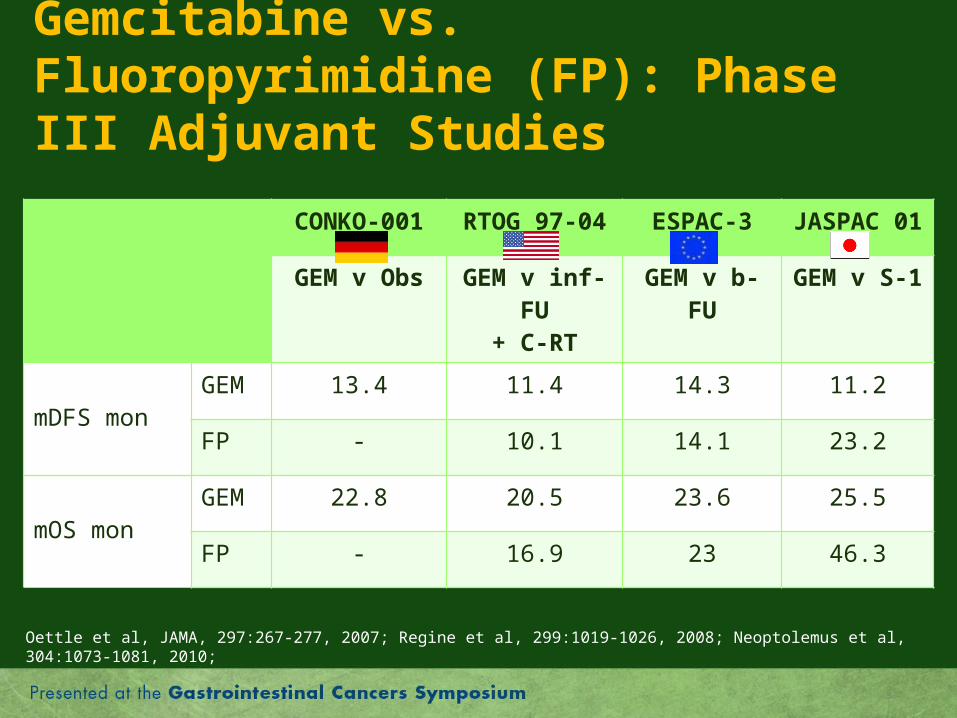
Gemcitabine vs. Fluoropyrimidine (FP): Phase III Adjuvant Studies
CONKO-001 RTOG 97-04 ESPAC-3 JASPAC 01
GEM v Obs GEM v inf-FU+ C-RT
GEM v b-FU GEM v S-1
mDFS monGEM 13.4 11.4 14.3 11.2
FP - 10.1 14.1 23.2
mOS monGEM 22.8 20.5 23.6 25.5
FP - 16.9 23 46.3
Oettle et al, JAMA, 297:267-277, 2007; Regine et al, 299:1019-1026, 2008; Neoptolemus et al, 304:1073-1081, 2010;
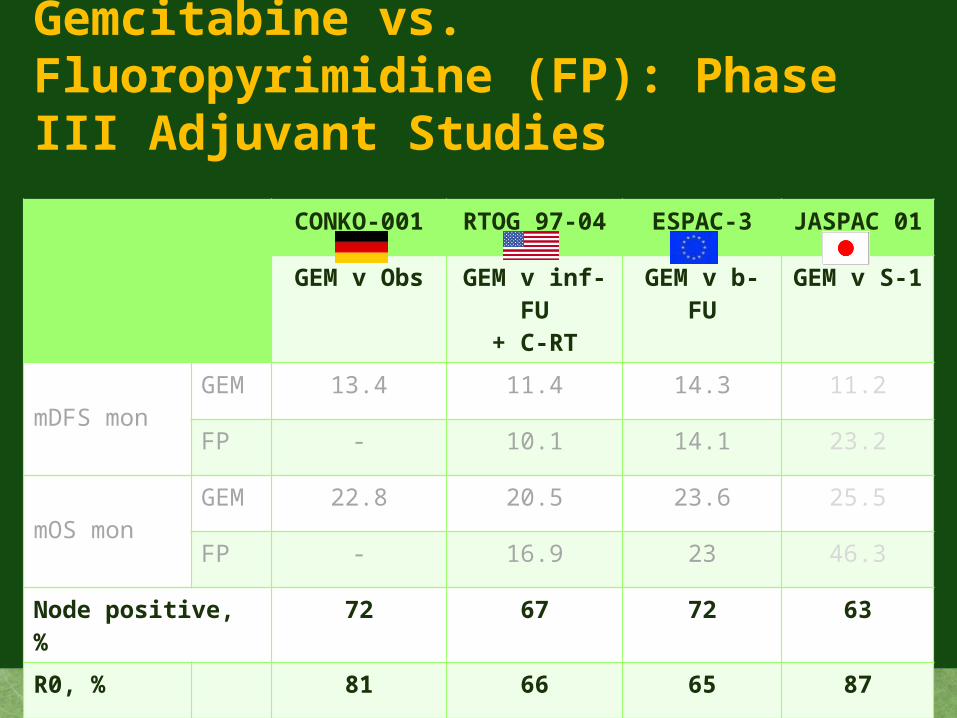
Gemcitabine vs. Fluoropyrimidine (FP): Phase III Adjuvant Studies
CONKO-001 RTOG 97-04 ESPAC-3 JASPAC 01
GEM v Obs GEM v inf-FU+ C-RT
GEM v b-FU GEM v S-1
mDFS monGEM 13.4 11.4 14.3 11.2
FP - 10.1 14.1 23.2
mOS monGEM 22.8 20.5 23.6 25.5
FP - 16.9 23 46.3
Node positive, % 72 67 72 63
R0, % 81 66 65 87

JASPAC 01
• Superiority of adjuvant S-1 over GEM in Japanese patients with resected panc. ca.
• “Non-Japanese” studies must be considered to define the role of S-1 in early and late stage disease in conjunction with biomarkers studies (e.g., S-1 metabolism)
• The role of adjuvant radiation therapy in panc. ca will be determined by the ongoing RTOG/SWOG/EORTC study
Randomized Phase III Study of Weekly nab-Paclitaxel plus Gemcitabine vs Gemcitabine Alone in Patients with Metastatic Adenocarcinoma of the
Pancreas (MPACT)
Daniel D. Von Hoff, et al.
Abstract #148
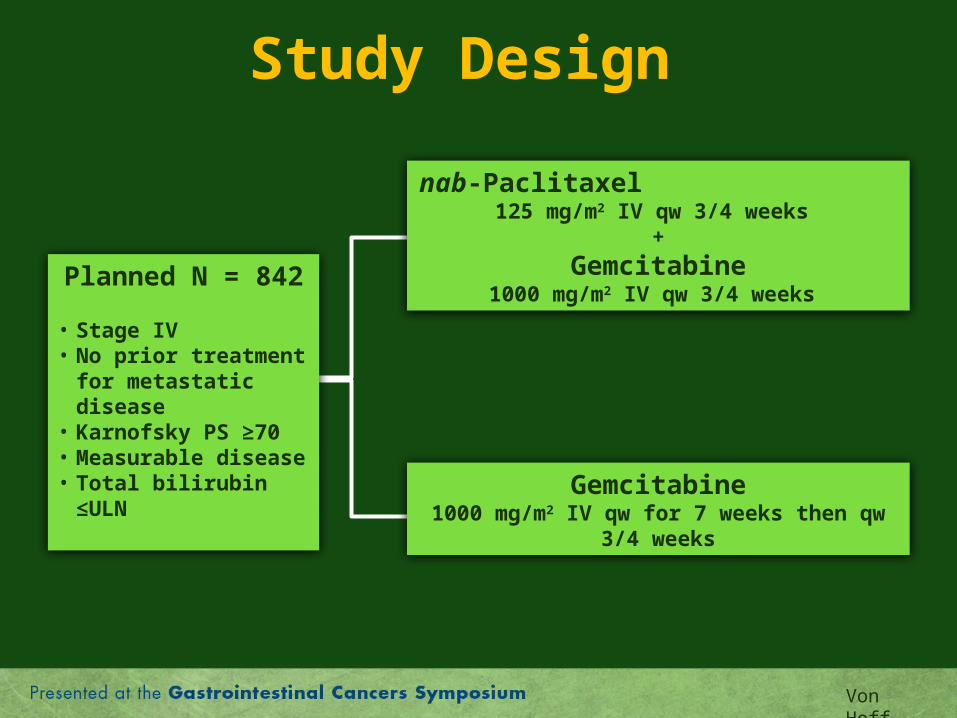
Study Design
Planned N = 842
• Stage IV• No prior treatment for
metastatic disease• Karnofsky PS ≥70 • Measurable disease• Total bilirubin ≤ULN
nab-Paclitaxel 125 mg/m2 IV qw 3/4 weeks
+
Gemcitabine1000 mg/m2 IV qw 3/4 weeks
Gemcitabine1000 mg/m2 IV qw for 7 weeks then qw 3/4
weeks
Von Hoff

IMPACT: Efficacy
nab-Pacli + GEM
GEM Hazard ratiop value
Med OS, mos 8.5 6.7 0.72/0.000015
Med PFS, mos 5.5 3.7 0.69/0.000024
12-mon alive, % 35 22 0.0002Objective response, %
23 7 1.1x10-10

Major Treatment Options for Metastatic Pancreatic Cancer
• Gemcitabine +/- erlotinib• FOLFIRINOX• Nab-paclitaxel plus gemcitabine• Others (e.g., GemCape, GTX) • Clinical trial
Major Treatment Options for Metastatic Pancreatic Cancer
• Gemcitabine +/- erlotinib• FOLFIRINOX• Nab-paclitaxel plus gemcitabine• Others (e.g., GemCape, GTX) • Clinical trials

Tolerability:Selected Grade 3+ Toxicities, %
nab-pacli + GEM
FOLFIRINOX
Fatigue 17 23.6Diahhrea 6 12.7Neuropathy 17 9Neutropenia 38 45.7Neutropenic fever 3 5.4Thrombocytopenia 13 9.1
Conroy et al, NEJM, 364:1817-1825, 2011

Efficacy
nab-pacli + GEM
FOLFIRINOX
Median OS, mos 8.7 11.1Median PFS, mos
5.5 6.4
ORR (%) 23.0 31.6
Conroy et al, NEJM, 364:1817-1825, 2011
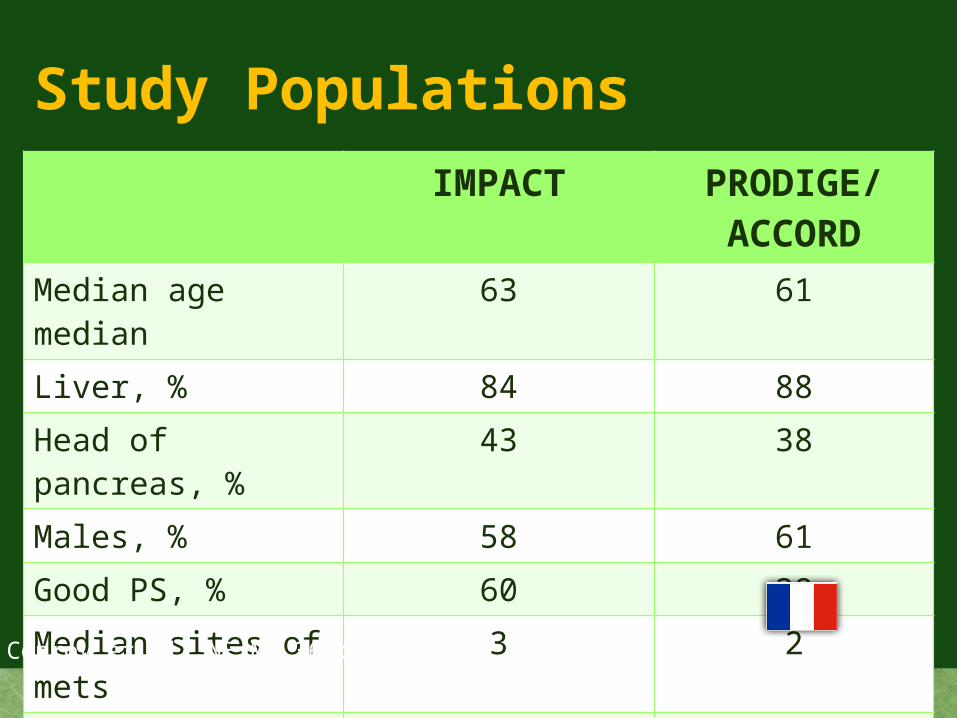
Study PopulationsIMPACT PRODIGE/
ACCORDMedian age median 63 61
Liver, % 84 88
Head of pancreas, % 43 38
Males, % 58 61
Good PS, % 60 38
Median sites of mets 3 2
Number of patients 861 342
Treatment centers Multiple countries
Conroy et al, NEJM, 364:1817-1825, 2011

IMPACT• Is an example of pre-clinical to pilot testing to
Phase III drug stepwise developmental program• Nab-paclitaxel plus GEM is a new frontline
regimen in patients with metastatic panc. ca. and favorable performance status
• Nab-paclitaxel +/- GEM (or other drugs) must be investigated in earlier stage disease and in combinations with biologicals
• The molecular basis of nab-paclitaxel’s activity and its association with a biomarker(s) must be determined (going back to the lab!)
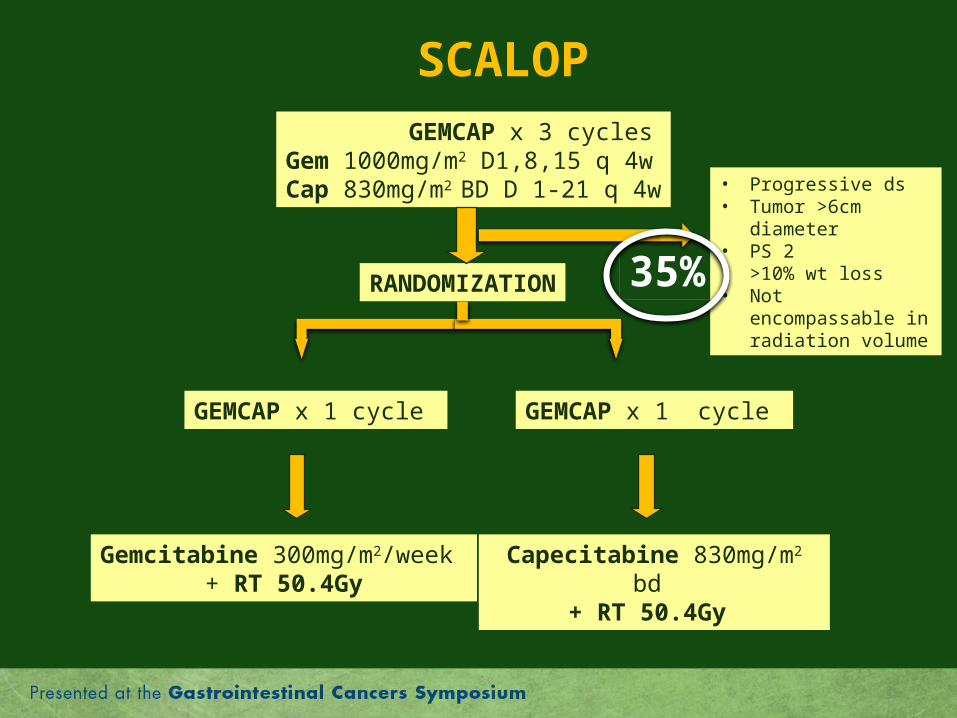
Induction GEMCAP Chemotherapy followed by Gemcitabine (Gem) or
Capecitabine (Cap)-based Chemoradiation (CRT) for Locally
Advanced Pancreatic Cancer (LAPC): the Final Results of the SCALOP Trial
S Mukherjee, et al.SCALOP Investigators
Abstract LBA146

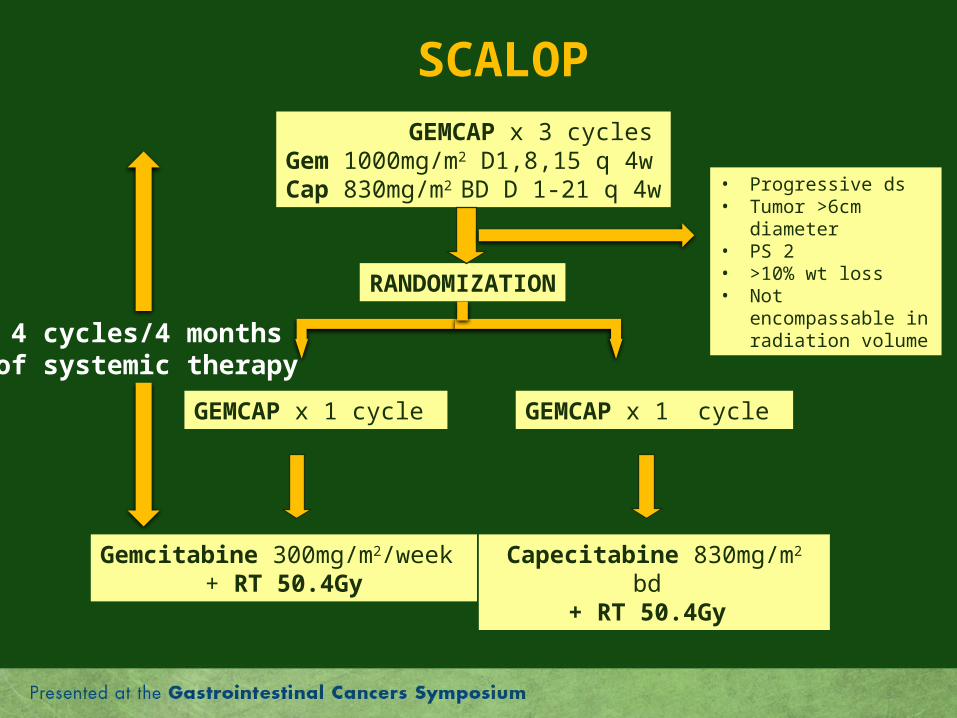
GEMCAP x 3 cyclesGem 1000mg/m2 D1,8,15 q 4wCap 830mg/m2 BD D 1-21 q 4w
RANDOMIZATION
GEMCAP x 1 cycle GEMCAP x 1 cycle
Gemcitabine 300mg/m2/week + RT 50.4Gy
Capecitabine 830mg/m2 bd + RT 50.4Gy
• Progressive dx• Tumor >6cm diameter• PS 2• >10% wt loss• Not encompassable
in radiation volume
SCALOP
GEMCAP x 3 cyclesGem 1000mg/m2 D1,8,15 q 4wCap 830mg/m2 BD D 1-21 q 4w
RANDOMIZATION
GEMCAP x 1 cycle GEMCAP x 1 cycle
Gemcitabine 300mg/m2/week + RT 50.4Gy
Capecitabine 830mg/m2 bd + RT 50.4Gy
• Progressive ds• Tumor >6cm diameter• PS 2• >10% wt loss• Not encompassable
in radiation volume
SCALOP
35%
GEMCAP x 3 cyclesGem 1000mg/m2 D1,8,15 q 4wCap 830mg/m2 BD D 1-21 q 4w
RANDOMIZATION
GEMCAP x 1 cycle GEMCAP x 1 cycle
Gemcitabine 300mg/m2/week + RT 50.4Gy
Capecitabine 830mg/m2 bd + RT 50.4Gy
• Progressive ds• Tumor >6cm diameter• PS 2• >10% wt loss• Not encompassable
in radiation volume
SCALOP
4 cycles/4 monthsof systemic therapy

Summary of Efficacy DataCAPE-RT GEM-RT p
PFS at 9 mos, % 62.9 51.4 NSMedian PFS, mos 12.0 10.4 NSMed OS, mos 15.2 13.4 0.025
All Randomized Taken offN 114 74 40Med OS, mos 12.7 14.6 8.1
What do we learn from SCALOP?
• Cape-RT is the current preferred standard and will continue as such
• Ongoing research questions– The contribution of chemo-RT (GERCOR, Dr P. Hammel;
ALLIANCE, Dr A. Ko)– Molecular selection for chemo-RT (RTOG, Dr E. Ben
Josef) – More effective systemic therapies
• Develop study designs and endpoints that are appropriate to each question
M. J. Pishvaian, et al.
A Phase I/II Study of ABT-888, 5-Fluorouracil and Oxaliplatin in Patients
with Metastatic Pancreatic Cancer
Abstract #147
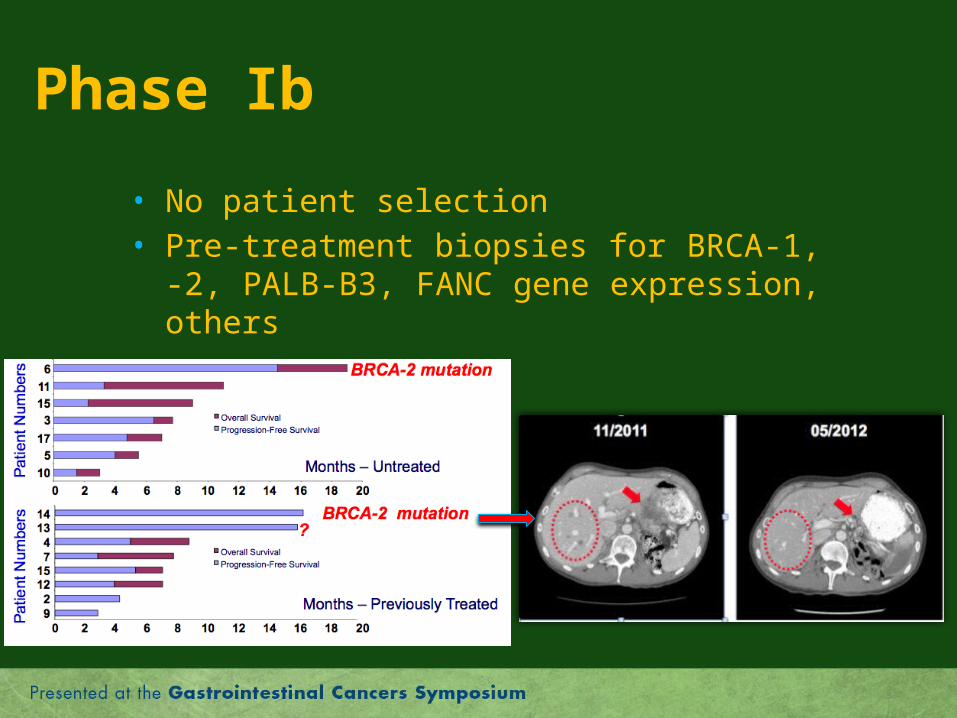
Phase Ib
• No patient selection• Pre-treatment biopsies for BRCA-1, -2, PALB-
B3, FANC gene expression, others
PARPi and Pancreatic Cancer
• A platinum +/- PARPi strategy is worth pursuing in patients with BRCA-2 mutations
• Explore biologic combinations with PARPi • Need to determine relative contributions of
platinum vs. PARPi to anti-tumor activity• National or “preferably” international
collaborative effort is necessary for a timely completion of clinical trials (e.g., ARCAD)

Thank you
backup

Take Home Messages
• Adjuvant S-1 is a new standard for resected pancreas ca. with a potential for its development outside of Japan
• nab-Paclitaxel/GEM is a new treatment standard for patients with metastatic pancreas ca. warranting further development in conjunction with a biomarker discovery strategy

Take Home Messages (2)
• Capecitabine 1.66 grams/m2/day will continue to be our radisoenstizer of choice in pancreas ca.
• A treatment strategy of a platinum compound +/- PARPi needs pre-clinical/pilot clinical evaluations in BRCA-2 mutated panc. ca.
• More tissue-based research and stronger collaborative efforts are necessary for successful studies in pancreatic cancer!

Gemcitabine vs. Fluoropyrimidine (FP): Phase III Adjuvant Studies
CONKO-001 RTOG 97-04 ESPAC-3 JASPAC 01
GEM v Obs GEM v inf-FU+ C-RT
GEM v b-FU GEM v S-1
mDFS monGEM 13.4 11.4 14.3 12
FP - 10.1 14.1 24
mOS monGEM 22.8 20.5 23.6 23
FP - 16.9 23 46
Hazard ratio for overall survival 0.80 0.94 0.56
Oettle et al, JAMA, 297:267-277, 2007; Regine et al, 299:1019-1026, 2008; Neoptolemus et al, 304:1073-1081, 2010;