diet and kwashiorkor in the democratic republic of congo · diet and kwashiorkor in the democratic...
TRANSCRIPT

Diet and Kwashiorkor in the DemocraticRepublic of Congo
Hallgeir Kismul, Mala Ali Mapatano, and Jean Pierre Banea
AbstractDespite holding a wealth in natural resources, the population of the DemocraticRepublic of Congo (DRC) is among the poorest in the world. Food insecurity andmalnutrition is widespread. While severe child malnutrition in the form ofkwashiorkor has become rare in most other developing countries, thousands forchildren in the DRC are suffering from this disease. Since its early descriptionkwashiorkor among children has been related the consumption of a monotonousdiet low in protein. It has also been postulated that kwashiorkor is caused by anexcess in free radicals and that protective pathways are compromised in kwash-iorkor with these pathways requiring micronutrients in the form of antioxidants.Kwashiorkor typically occurs in areas with severe food insecurity, and in theDRC food insecurity is especially prevalent in the rural areas. The nationalprevalence of children with edema in the DRC has been reported to be as highas 4% with the highest proportion of children with edema living in the rural areas.The diet in most areas of the DRC is monotonous. Cassava is the major and it issevered with different side dishes including cassava leaves. Animal products areconsumed occasionally and wild food constitutes a safety net during periods ofshortage. The relation between diet and kwashiorkor in children in the DRC hasbeen investigated in historical longitudinal study. The diet in the study area is low
H. Kismul (*)Centre for International Health, University of Bergen, Bergen, Norwaye-mail: [email protected]
M.A. MapatanoDepartment of Nutrition, School of Public Health, University of Kinshasa, Kinshasa, Congoe-mail: [email protected]
J.P. BaneaProgramme National de Nutrition (PRONANUT), Kinshasa, Congoe-mail: [email protected]
# Springer International Publishing AG 2017V.R. Preedy, V.B. Patel (eds.), Handbook of Famine, Starvation, and NutrientDeprivation, DOI 10.1007/978-3-319-40007-5_38-1
1

in diversity and the major staples include cassava and maize. Children who didnot develop kwashiorkor had consumed food items that were rich in β-carotenewhile those who did develop kwashiorkor had not.
KeywordsUnderdevelopment • Civil war • Poverty • Agriculture • Food insecurity • Diet •Malnutrition • Marasmus • Kwashiorkor • Antioxidants • β-Carotene
List of AbbreviationsDHS Demographic and health surveyDRC Democratic republic of CongoIPC Integrated food security phase classificationRUTF Ready-to-use therapeutic food
ContentsIntroduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2What is Kwashiorkor? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4The Global Burden of Kwashiorkor . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5The Etiology of Kwashiorkor . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6Food Insecurity in the DRC . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8Malnutrition in the DRC . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9Diet in the DRC . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9Infant Feeding . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10Diet and Kwashiorkor in Northwest DRC: The Bwamanda Study . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10Conclusion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15Policies and Protocols . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15
Protocol . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15Policies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16
Dictionary of Terms . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16Summary Points . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18
Introduction
The Democratic Republic of Congo (DRC), a former Belgian colony, is located incentral Africa. It has a population of 69 million (The World Bank 2013) and isthereby the fourth most populated country in Africa. It is divided into 26 provincesincluding the city province of Kinshasa (see Fig. 1 map). The DRC holds a wealth ofnatural resources including a diversity of mineral and forest resources (The WorldBank 2013). It is classified as the 5th most biodiverse country on the earth (Termoteet al. 2012). The country has an environment that is favorable to agriculture that inmany areas allows for two harvests per year (Rossi et al. 2006). Despite its wealth innatural resources, DRC’s population is among the poorest in the world. Based on itspoor scores with regards to income and health, it is by Human Development Indexranked as the 176, out of 188, poorest countries in the world (UNDP 2015). There isa rural–urban gap in poverty disfavoring rural areas where eight out of ten house-holds are living below the poverty line of 1.25 dollars a day, while in urban areas it is
2 H. Kismul et al.

Fig.1
Map
oftheDem
ocratic
Repub
licof
Con
go(Sou
rce:USAID
2015
,http
://www.ocnus.net/artman2/pu
blish/Africa_8/Kabila%20
-%20
Plan%
20B%20
for
%20
the%
20Con
go.shtml)
Diet and Kwashiorkor in the Democratic Republic of Congo 3

less than seven out of ten (The World Bank 2013). Agriculture makes up about 70%of people’s livelihood and the agricultural sector is dominated by subsistenceagriculture (Ministre du Plan et Révolution de la Modernité de la RDC 2015).Since 1997 and until now, the political situation in the country has been character-ized by civil wars. The death toll of the civil war, 1998–2004, has been estimated to3.9 million (Coghlan et al. 2006). The conflicts have restricted the country’s abilityto promote development and food production and thus improve food security (Weijset al. 2012; Kandala et al. 2011). Hence, DRC is still strongly dependent on foreignaid (République Démocratique du Congo 2014).
Whereas many other countries in sub-Saharan Africa have been able to reduce thenumber of people suffering from malnutrition, prevalence of malnutrition in theforms of stunting, wasting and underweight in the DRC is among the highest insub-Saharan Africa (République Démocratique du Congo 2014). Many children arealso suffering from severe malnutrition.
including marasmus and kwashiorkor. In other parts of the world, kwashiorkorhas become very rare, but in the DRC thousands of children are still suffering fromthis disease.
What is Kwashiorkor?
The earliest description of kwashiorkor can be dated back to biblical times. TheJamaican physician Cecilia Williams, working in what is now Ghana, was in anarticle from 1933 (republished in 1983) the first to describe kwashiorkor in Africa. Ina Lancet article from 1935, she gave the disease its African name kwashiorkor(Williams 1935). The name was given after the notion in the Ga language of thecoastal Ghana, kwa ni oshi korkor, and was translated by Williams as the disease thatthe deposed child gets when the next is born. Williams suggested that the disease wasassociated with a monotonous diet, and given that maize was the main source ofsupplementary food, she suggested that some amino acid or protein deficiency couldnot be excluded as causing the disease.
Kwashiorkor along with marasmus and marasmic kwashiorkor are classified assyndromes of clinical severe childhood malnutrition. Kwashiorkor and marasmickwashiorkor are identified by edema (swelling of body tissues as a result of fluidaccumulation), whereas marasmus is defined as a nonedematous form of extremewasting (Figs. 2 and 3). Edema is the most important and defining feature ofkwashiorkor (Heikens and Manary 2009) (Fig. 4). There are significant variationsof edema severity (Epomedicine 2017). It is classified as mild when it occurs in feetonly, moderate when it occurs in legs and feet and lower arms, and severe when it ispresent on face and arms. Children with kwashiorkor may also develop skin lesionscommon on the extremities (Heilskov et al. 2014) (Fig. 5). Hair abnormalities arestriking when the disease process is of a long duration. Abnormalities includestraight hair, dyspigmentation, and thin hair. Fatty liver resulting in enlargement ofthe liver is also commonly reported as a feature of kwashiorkor (Frenk et al. 1958;Truswell and Miller 1993). The disease has been associated with a high risk of death(Briend et al. 1987; Talbert et al. 2012).
4 H. Kismul et al.

The Global Burden of Kwashiorkor
Kwashiorkor is prevalent in several parts of sub-Saharan Africa and is also found incommunities in Asia and in South and Central America. Very few cases have beenreported from high-income countries. The disease is still an important public healthproblem especially in rural areas where children consume a diet low in dietarydiversity, often consisting of two major staples.
Kwashiorkor is a transitional condition and typically those who suffer from thedisease recover after a few weeks of case management or die from the disease(Williams 1935). This makes it difficult to capture the magnitude of kwashiorkorin cross-sectional surveys that report prevalence of malnutrition (CMAM Forum2015). A report attempting to describe the burden of kwashiorkor in low-incomecountries concluded that prevalence of kwashiorkor in most countries was less than1% (CMAM Forum 2015). Then again some countries reported rates between 1%and 2% including Yemen, Zimbabwe, and the DRC.
HAIR CHANGES
MUSCLEWASTING
DEPIGMENTATIONOF SKIN
GROWT FAILURE
APARTHYIRRITABILITY
ANEMIA
FATTY LIVER
VILLOUSATROPHY OF
SMALL INTESTINE
DERMATOSES
EDEMA
(HYPERALBUMINEMIA)
Fig. 2 Signs of kwashiorkor drawing by Hallgeir Kismul
Diet and Kwashiorkor in the Democratic Republic of Congo 5

The Etiology of Kwashiorkor
The development of kwashiorkor has been linked to diet and metabolism. Until the1980s Kwashiorkor was with marasmus classified as a form of protein-energymalnutrition. Kwashiorkor was seen as a result of children consuming a diet highin energy but low in protein. This consumption pattern leads to pathological abnor-malities such as edema and fatty liver (Whitehead and Alleyne 1972). The hypoth-esis was challenged and studies found that the diet of children who developedkwashiorkor was not characterized by a low intake of protein when compared with
Fig. 4 Child from theDemocratic Republic ofCongo with kwashiorkorshowing pitting oedema photowith permission from BranlyMbunga Kilola
OLD MAN’S FACE
THIN MUSCLE
THIN FAT
NO EDEMA
Fig. 3 Signs of marasmusdrawing by Hallgeir Kismul
6 H. Kismul et al.

the diet of children who developed marasmus (Gopalan 1992). In the early 1980s, itwas postulated that kwashiorkor was caused by an excess of free.
radicals. According to this suggestion, protective pathways were compromised inkwashiorkor. These pathways require the supply of micronutrients in the form ofantioxidants, which could be deficient in kwashiorkor, thus causing a loss of theprotective pathways (Golden and Ramdath 1987). Some population studies havechallenged the free radical hypothesis. As an example a randomized control trial ofchildren aged 1–4 years assessed the efficiency of providing antioxidants to preventkwashiorkor (Ciliberto et al. 2005). This study failed to show that the supplemen-tation of antioxidants prevented the children from developing kwashiorkor. Stillother studies have shown that there is apparently a lack of micronutrition in the dietof children who develop kwashiorkor (Kismul et al. 2014). A child with kwashiorkortypically lives in environments where the diet is restricted to cooked but starchyfoods including cassava and maize. The diet characteristically lacks vegetables andfruits. These are natural sources of micronutrients and dietary antioxidants.
The literature has described relations between breastfeeding and presence ofkwashiorkor. Apparently children who have developed kwashiorkor are less likelyto have been breastfed in comparison with those who have not developed kwashi-orkor (Rytter et al. 2015). Prolonged breastfeeding and supplementation with solidfood have been associated with a substantial reduction of clinical malnutrition in theform of kwashiorkor and marasmus (Cousens et al. 1993).
Although there is an apparent relation between diet and the development ofkwashiorkor, there still exist many uncertainties as to the cause of kwashiorkor. Anumber of hypotheses are put forward and are being tested to better understand theetiology of kwashiorkor. As an example abnormal gut microbiota has beensuggested as a factor contributing to the development of the syndrome. The hypoth-esis has been tested in animal and population studies (Subramanian et al. 2014). Thisliterature suggests that there is a link between the consumption of a nutrient-poordiet, abnormal microbiota, and the development of kwashiorkor (Smith et al. 2013).
Moreover, abnormal gut microbiota has been related to environmental entericdysfunction (Crane et al. 2015).
Fig. 5 Child from theDemocratic Republic ofCongo with kwashiorkorshowing skin lesions, photowith permission from BranlyMbunga Kilola
Diet and Kwashiorkor in the Democratic Republic of Congo 7

Food Insecurity in the DRC
Food security is considered an underlying factor with implications for children’s andadults nutritional status and is manifest at the household level. Food insecurity is amajor problem in the DRC, and according to the recent Integrated Food SecurityPhase Classification (IPC) of 2016, over 5 million of the country’s population are inacute food security and livelihood crisis (IPC 2017). In the DRC, malnutrition ismost widespread in the rural areas (The World Bank 2013; Kandala et al. 2011).There are several factors that constraint food production in the rural areas. Themajority of the rural population depends on rainfed subsistence farming cultivatingland less than 2 acres (WFP 2014). The farmers use traditional farming techniquesand all operations are carried out manually. Poor access to seeds both improvedvarieties and traditional is considered a major obstacle to agricultural production(WFP 2014). Furthermore, other agricultural inputs including fertilizers and pesti-cides are more or less unavailable. Poor infrastructure also puts constraints on thepossibility of developing agriculture especially cash cropping. The infrastructure,roads and waterways connecting local communities, agricultural land, and markets,has been described as “in an advanced stage of deterioration” (Mathys andRemancus 2010).
The IPC report subdivides the country with regard to food insecurity in 4 regions(IPC 2017):
1. The regions severely affected by armed conflicts, typically in the Eastern DRC.2. The regions susceptible to climatic and natural changes including floods, El Nino,
outbreaks, etc., in the Eastern and central provinces of the country.3. The regions under the pressure of internal displaced populations and refugees,
these are provinces along the border.4. The regions under chronic food insecurity comprising northern and central
provinces. They are characterized by extreme poverty and ill access to socialservices.
People living in the capital Kinshasa are in comparison with people residing inother provinces food secure. The most food insecure provinces are typically land-locked provinces that are extremely difficult to reach. In such areas, manufacturedgoods including food are sold at very high price, whereas cash cropping is difficult todevelop. In the most food insecure provinces, people rely upon artisanal mining. Inthese provinces, there is a tendency that people neglect food production and theseprovinces have to import much of its food. Provinces affected by war includingSouth Kivu are also food insecure. The land in South Kivu is fertile, but shortage ofland and landlessness are problems closely related to food insecurity. Several foodinsecure provinces face problems due to influx of internal as well as refugees fromneighboring countries (Mathys and Remancus 2010).
8 H. Kismul et al.

Malnutrition in the DRC
The Demographic and Health Survey (DHS) from 2013/14 provides data on theprevalence of malnutrition in children in 2013 in the DRC (RépubliqueDémocratique du Congo 2014). According to the survey, 43% of the childrenbelow 5 years suffered from stunting, 8% from wasting, and 23% from underweight.The DRC thereby had among the highest proportions of children suffering fromstunting in the world.
While the most recent DHS report from 2013/14 (République Démocratique duCongo 2007) does not contain data on kwashiorkor, this information is included inthe DHS from 2007 (République Démocratique du Congo 2007). This reportinforms that 4.1% of the children below 5 years had edema with the largestproportion of children with edema in the age category 9–11 months. There wereno gender differences in the occurrence of edema. On.
the other hand the report demonstrates a rural urban gap and most of the childrenwith edema lived in the rural areas. There were also important regional differences asto occurrence of edema. In particular Orientale and South Kivu provinces had highprevalence of children with edema. The former province is depending on artisanalmining and the latter province has over the last decades been affected by civil war. Itis also reported that children with edema were most likely to live in the pooresthouseholds.
Diet in the DRC
The diet in the DRC depends on regional context and there are also importantdifferences between diet in rural and urban areas (Bervoets and Lassance 1959;Termote et al. 2012). Cassava root is the main staple food crop in most parts of thecountry. In the northern regions, cassava is served with cassava leaves as a side dish.In addition cassava is provided with different vegetables, legumes, and fish. In thewestern part of the country, cassava is typically consumed with vegetables and fish.In the south, maize is the major staple food and is consumed with vegetables andlegumes. Cassava is also a major staple in the eastern part of the country, but foodsuch as sweet potatoes and beans are commonly consumed. In the urban areas,cereals play a more important role in the diet than in the rural parts of the country.Animal products such as meat and egg are only eaten occasionally, whereas dairyproducts are rarely consumed. Wild edible plant and bush meat are components offood production especially in the rural areas and wild food constitutes a safety netduring periods of food shortage. The most import wild plants consumed include wildyam, wild nuts, wild leafy vegetables, and various wild fruits. In addition bush meatand fish are part of the diet in areas located to the vicinity of forests and rivers.However, even in areas characterized by being very rich in biodiversity, wild edibleplants are insufficiently consumed to increase nutrition security or dietary adequacy(Termote et al. 2012).
Diet and Kwashiorkor in the Democratic Republic of Congo 9

Typically the Congolese consume one to two meals per day. The major mealusually consists of a stiff porridge made from cassava or maize flour. The porridge isoften served with a stew made of cassava leaves, spinach, and okra. Typically only aminority enrich the porridge with vegetable, fruits, fish, and meat. Meat is rarelyconsumed. If there are any left-overs, these are consumed for breakfast the next day.In between meals, people drink tea and palm wine and eat various fruits. For thehouseholds that do not produce their own fruits and vegetables, the cost of purchas-ing such food items at the market is often too high.
For the meals, water is collected from deep tube wells or from streams in theforests. During meals, household members are served the same food, but split intogroups; women and young children in one group, older children in another and menin the third.
Infant Feeding
Breastfeeding is universally accepted and practiced in the DRC and 99% of infants0–5 months of age have been breastfed (République Démocratique du Congo 2014).Normally breastfeeding continues up to 2 years and 67% of toddlers 18–23 monthsare breasted. Early complementary feeding is common and more than half (60%) ofthe infants in the DRC experienced mixed feeding by 0–2 months (RépubliqueDémocratique du Congo 2007). In addition to water, early complementary foodconsists of a gruel basically made from porridge and cassava-leaf stew. Women’sworkload is a major obstacle to women practicing exclusively breastfeeding (Burnset al. 2016; Babakazo et al. 2015). In the rural areas women are required to cultivate,gather food, and collect firewood. While the mothers work in the field, their youngchildren are left with relatives and neighbors who provide them with food. At the ageof 7 months, the children are provided with solid food mostly in the form of porridge.As the children grow older, their diet does not change substantially. The childrencontinue to eat porridge and other family food as they grow older.
Diet and Kwashiorkor in Northwest DRC: The Bwamanda Study
Bwamanda is one among the 516 health zones in the DRC and is located in theSouth-Ubangi province in the northwest part of the DRC. Health services areprovided by a central hospital and 10 associated health centers. These healthfacilities serve a population of approximately 200,000. The hospital provides essen-tial health services including some degree of nutritional rehabilitation services. TheNgbaka is the dominant ethnic group in the area and are predominantly subsistencefarmers. The major crops cultivated in the area are cassava and maize. Besides cropproduction, the farmers grow vegetables such as sweet potatoes, taro, green leafyvegetable, and fruits such as papaya and African pear. The Ngbaka are also involvedin gathering wild vegetables and fruits. A number of water bodies and small riverssupport local fishing. The natural resources in the area are widely dispersedrestraining local people’s access to wild food.
10 H. Kismul et al.
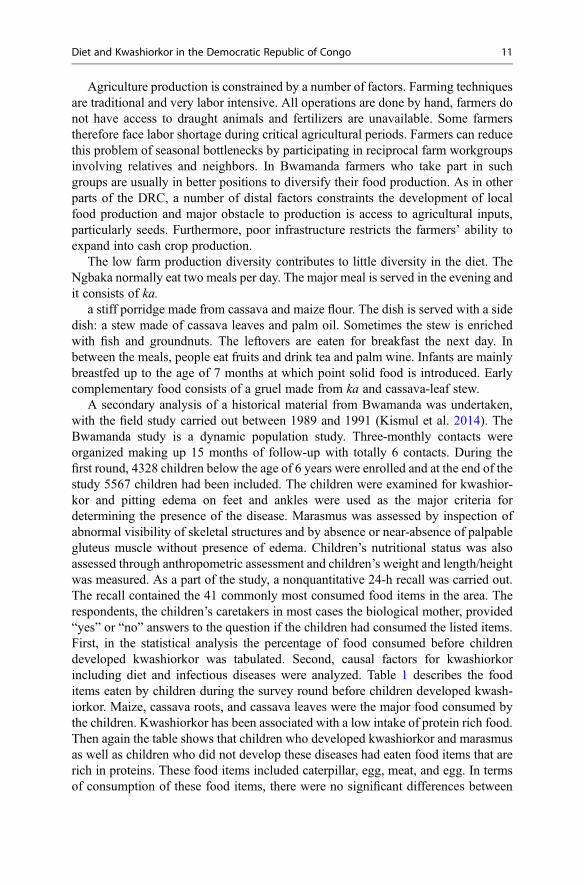
Agriculture production is constrained by a number of factors. Farming techniquesare traditional and very labor intensive. All operations are done by hand, farmers donot have access to draught animals and fertilizers are unavailable. Some farmerstherefore face labor shortage during critical agricultural periods. Farmers can reducethis problem of seasonal bottlenecks by participating in reciprocal farm workgroupsinvolving relatives and neighbors. In Bwamanda farmers who take part in suchgroups are usually in better positions to diversify their food production. As in otherparts of the DRC, a number of distal factors constraints the development of localfood production and major obstacle to production is access to agricultural inputs,particularly seeds. Furthermore, poor infrastructure restricts the farmers’ ability toexpand into cash crop production.
The low farm production diversity contributes to little diversity in the diet. TheNgbaka normally eat two meals per day. The major meal is served in the evening andit consists of ka.
a stiff porridge made from cassava and maize flour. The dish is served with a sidedish: a stew made of cassava leaves and palm oil. Sometimes the stew is enrichedwith fish and groundnuts. The leftovers are eaten for breakfast the next day. Inbetween the meals, people eat fruits and drink tea and palm wine. Infants are mainlybreastfed up to the age of 7 months at which point solid food is introduced. Earlycomplementary food consists of a gruel made from ka and cassava-leaf stew.
A secondary analysis of a historical material from Bwamanda was undertaken,with the field study carried out between 1989 and 1991 (Kismul et al. 2014). TheBwamanda study is a dynamic population study. Three-monthly contacts wereorganized making up 15 months of follow-up with totally 6 contacts. During thefirst round, 4328 children below the age of 6 years were enrolled and at the end of thestudy 5567 children had been included. The children were examined for kwashior-kor and pitting edema on feet and ankles were used as the major criteria fordetermining the presence of the disease. Marasmus was assessed by inspection ofabnormal visibility of skeletal structures and by absence or near-absence of palpablegluteus muscle without presence of edema. Children’s nutritional status was alsoassessed through anthropometric assessment and children’s weight and length/heightwas measured. As a part of the study, a nonquantitative 24-h recall was carried out.The recall contained the 41 commonly most consumed food items in the area. Therespondents, the children’s caretakers in most cases the biological mother, provided“yes” or “no” answers to the question if the children had consumed the listed items.First, in the statistical analysis the percentage of food consumed before childrendeveloped kwashiorkor was tabulated. Second, causal factors for kwashiorkorincluding diet and infectious diseases were analyzed. Table 1 describes the fooditems eaten by children during the survey round before children developed kwash-iorkor. Maize, cassava roots, and cassava leaves were the major food consumed bythe children. Kwashiorkor has been associated with a low intake of protein rich food.Then again the table shows that children who developed kwashiorkor and marasmusas well as children who did not develop these diseases had eaten food items that arerich in proteins. These food items included caterpillar, egg, meat, and egg. In termsof consumption of these food items, there were no significant differences between
Diet and Kwashiorkor in the Democratic Republic of Congo 11

Table
1Con
sumptionof
differentfoo
ditemsin
thesurvey
roun
dprecedingthedevelopm
ento
fkw
ashiorko
r(n
=37
)andno
n-developm
ento
fkw
ashiorko
r(n
=81
08)anddevelopm
entof
marasmus
(n=
374)
inchild
renbetween6and50
mon
thsof
age.(K
ismul
etal.2
014).
Foo
ditems
Childrenwith
Kwashiorko
r%
(95CI)
Childrenwith
out
kwashiorko
r%
(95CI)
Childrenwith
marasmus
%(95CI)
Foo
ditems
Childrenwith
kwashiorko
r%
(95CI)
Childrenwith
out
kwashiorko
r%
(95CI)
Childrenwith
marasmus
%(95CI)
African
pears
0.0(0.0,
8.2)
0.0(0.0,1.1)
0.0(0.0,1.3)
Okra
2.3(0.4,12.1)
4.5(4.2,4.8)
5.2(3.2,8.4)
Amaran
th7.0(2.4,18
.6)
1.8(1.7,2.1)
3.1(1.6,5.8)
Pam
oil
86.0
(72.0,93
.4)
88.8
(88.3,89
.3)
80.3
(75.4,84
.5)
Aubergine
0.0(0.0,8.2)
0.8(0.7,0.9)
0.0(0.0,
1.3)
Papaya
2.3(0.4,12.1)
15.5(15.0,16
.1)a
11.8(8.5,16.0)
a
Avo
cado
0.0(0.0,8.2)
0.2(0.1,0.2)
0.0(0.0,
1.3)
Pineapp
le4.7(1.3,15
.5)
1.4(1.2,1.6)
1.7(0.7,4.0)
Ban
ana
9.3(3.7,21
.6)
19.1(18.5,19
.7)
16.3
(12.5,21
.0)
Pow
der
milk
0.0(0.0,8.2)
0.0(0.0,0.1)
0.0(0.0,
1.3)
Beans
31.1(30.4,31
.8)
0.4(0.3,0.5)
0.0(0.0,
1.3)
Rice
2.3(0.4,12.1)
0.6(0.5,0.8)
0.0(0.0,
1.3)
Bread
fruit
0.0(0.0,8.2)
1.1(0.9,1.2)
1.7(0.7,4.0)
Sesam
e0.0(0.0,8.2)
0.1(0.1,0.2)
0.3(0.1,0.9)
Cassava
leav
es76
.7(62.3,
86.8)
79.2
(78.6,79
.9)
70.7
(65.2,
75.6)
Shrim
p0.0(0.0,8.2)
0.1(0.1,0.2)
0.0(0.0,
1.3)
Caterpillars
2.0(1.8,2.2)
2.0(1.8,2.2)
1.0(1.4,3.0)
Snails
2.3(0.4,12.1)
1.4(1.3,1.6)
1.4(0.5,3.5)
Cassava
roots
77.7
(62,3,86
.8)
72.6(71.9,73
.3)
72.3
(66.9,77
.2)
Soy
a4.7(1.3,15
.5)
5.2(4.9,5.5)
5.9(3.7,9.2)
12 H. Kismul et al.

Chili
pepper
4.7(1.3,
15.5)
8.9(8.4,9.3)
4.5(2.6,7.5)
Spinach
2.3(0.4,12.1)
2.8(2.6,3.1)
2.1(1.0,4.5)
Egg
4.7(1.3,15
.5)
0.7(0.5,0.8)
1.0(0.4,3.0)
Squ
ash
0.0(0.0,8.2)
4.9(4.6,5.2)
5.2(3.2,8.4)
Fish
18.6
(9.7,32.6)
31.1(30.4,31
.8)
25.3(20.6,30
.6)
Sug
arcane
0.0(0.0,8.2)
0.7(0.6,0.9)
0.3(0.1,1
.9)
Fruit
(other)
0.0(0.0,8.2)
1.8(16,2.0)
1.0(0.4,3.0)
Sweet
potato
0.0(0.0,8.2)
6.8(6.4,7.2)
4.5(2.6,7.5)
Ground
nuts
18.6
(9.7,32.6)
28.6
(27.9,29
.3)
23.9(19.3,29
.1)
Termites
0.0(0.0,8.2)
0.3(0.3,0.4)
0.0(0.0,
1.3)
Maize
97.7
(87.9,99
.6)
93.5(93.1,93
.8)
91,7
(88.0,94
.4)
Tom
atoes
0.0(0.0,8.2)
1.3(1.1,1.5)
0.0(0.0,
1.3)
Man
go0.0(0.0,8.2)
0.9(0.7,1.0)
0.7(0.2,2.5)
Wheat
0.0(0.0,8.2)
0.6(0.5,0.7)
0.3(0.1,1.9)
Meat
0.0(0.0,8.2)
4.7(4.4,5.0)
5.5(3.4,8.8)
Other
vegetables
2.3(0.4,12.1)
15.1(14.6,15
.7)a
17.6(13.7,22
.5)b
Milk
0.0(0.0,8.2)
0.1(0.1,0.1)
0.0(0.0,1.3)
Yam
2.3(0.4,12.1)
1.3(1.1,1.4)
0.7(0.2,2.5)
Mushroom
0.0(0.0,8.2)
2.3(2.1,2.5)
1.7(0.7,4.0)
a p<
0.05
bp<
0.01
with
values
estim
ated
using2-sampletestforequalityof
prop
ortio
nswith
continuity
correctio
nsas
implem
entedin
prop
testin
R
Diet and Kwashiorkor in the Democratic Republic of Congo 13

children with kwashiorkor and children with marasmus and children without any ofthese diseases. On the other hand a significant higher proportion of children who didnot develop kwashiorkor had consumed papaya, sweet potatoes, and “other vegeta-bles,” with the latter term comprising taro leaves, wild vegetables, and fruits. Thesefood items are characterized by their high content of β-carotene. The statisticalanalysis demonstrated that the risk of developing kwashiorkor in children whowere chronically malnourished increased the longer the children did not consumefood that contained β-carotene Fig. 6 illustrates how the risk of developing kwash-iorkor is reduced by eating food that is rich in β-carotene.
To summarize the Ngbaka live in environment characterized by food insecurityand in particular farmers who are not able to overcome labor constraints are
Fig. 6 Risk reduction for developing kwashiorkor showing reduction of consuming β-carotene richproducts according to age in months. The dotted line is risk reduction after 2 months, dashed lineafter 4 months, and solid line after 6 months, (a) shows risk reduction for a child with a height-for-age Z-score (HAZ) of minus five, (b) for a child with HAZ of minus three, and (c) a child with HAZof zero. HAZ-scores are based on the WHO-2006 Child Growth Standards (Kismul et al. 2014)
14 H. Kismul et al.

susceptible to food and nutrition insecurity. In addition distal factors limit farmers’ability to develop a more diverse food production. The diet in the area is monotonousand cassava and maize are the major food items consumed by young children. In thisfood and nutritional unsecure environment, children are at high risk of developingdifferent forms of malnutrition. The consumption of a monotonous diet that does notinclude vegetable and fruits increase the risk of chronically malnourished children todevelop severe forms of malnutrition such as kwashiorkor.
Conclusion
Kwashiorkor in Africa has been related to diet since its first description. Kwashior-kor occurs in situations characterized by food insecurity and famine. Furthermore,kwashiorkor has been related to the consumption of a monotonous diet oftencharacterized by the absence of.
consumption of fruit and vegetables. Thousands of children in the DRC are livingin this type of environment and they are at high risk of developing kwashiorkor.Nutritional programs in the DRC need in particular to focus on rural areas withparticular attention to provinces with high prevalence of malnutrition. It is especiallyimportant to assist ongoing efforts that aim at stimulating the consumption of avaried diet through improved agricultural and horticultural production.
Policies and Protocols
Protocol
Children with kwashiorkor can be treated with ready-to-use therapeutic food(RUTF), a home-based treatment carried out within a model for community-basedmanagement of acute malnutrition (Trehan and Manary 2015). RUTF is a high-energy, lipid-based spread. The powder ingredients are embedded in lipid-rich paste.The result is an energy dense food that resists microbial contamination (Briend2001). Treatment with RUTF is provided for children with uncomplicated kwashi-orkor (Manary et al. 2009), as it is also applied by PRONANUT, the nationalnutrition program which further recommends association with an antibiotic, and,where needed, vitamin A and an antimalarial (Manary et al. 2009). These arechildren who are treated in their early stage of illness. Children who are treatedlater in the stage of the illness may have a number of complications. These childrenshould receive individual treatment. For these children, extended nutritional supple-mentation as well as enrolment in nutritional program can be insufficient.
Diet and Kwashiorkor in the Democratic Republic of Congo 15

Policies
The strategy to reduce severe child malnutrition in the form of kwashiorkor shouldbuild on an approach that acknowledges how underlying, immediate, and basicfactors determine the development of kwashiorkor. It is important to tackle factorsat all three levels and recognize that addressing factors at only one level will haverestricted effect on the development of kwashiorkor.
The development of kwashiorkor in the DRC occurs in situations characterizedby severe poverty and food insecurity. To reduce severe malnutrition, there is a needfor significant changes at the macro level. Policies that aim at reducing malnutritionshould therefore be directly related to policies that put emphasis on economic growthand poverty reduction.
At the immediate level, it is important to address the problem of food insecurity. Itis essential to target children living poor food insecure households in rural areas.These children are especially at high risk of developing kwashiorkor. People livingin rural areas of the DRC are predominantly semisubsistence farmers. Food securitypolicies should attend to causes leading to low production and little diversity in foodproduction among small-scale farmers. Policies should especially improve betteraccess to agricultural extension and agricultural inputs such as seeds, fertilizers, andcredit. In terms of diversity in agricultural production, it is important to promote thecultivation of crops and fruits that are rich in β-carotene. Furthermore, improvementsin food production and consumption rely on infrastructure development and farmersin particular need better access to markets for sale of their agricultural produce.Strategies that aim at reducing malnutrition through strengthening small-scale agri-cultural production should in particular target households with few resources in formof land, labor, and capital.
At the basic level, policies should promote nutrition-specific interventions. Suchinterventions could be effective ways of reducing the incidence of kwashiorkor. Thediet in many areas of the DRC is to a large extent based on cassava and maize.Children are therefore at high risk of developing vitamin A deficiency. Vitamin Asupplementation might be an effective way of reducing malnutrition includingsevere malnutrition.
Dictionary of Terms
Clinical severe childhood malnutrition a term used for the three clinical syn-dromes of clinical severe malnutritionincluding marasmus, kwashiorkor, andmarasmic kwashiorkor.
Complementary feeding a process that start when breast milk nolonger is enough to meet the nutritionalneeds of the infant other foods and liq-uids are needed, along with breast milk.
16 H. Kismul et al.

Diet a term that is commonly defined as thefood that a person eats every day. It canbe portrayed with regards to chemicalcomposition in terms of nutrient contentor described as food and food groups.
Free radical is an atom or groups of atoms with anunpaired number of electrons. It can beformed when oxygen interacts with cer-tain molecules.
Kwashiorkor a form of severe malnutrition where thepresence of edema is the most significantfeature.
Marasmus nonedematous severe child malnutritionand characterized by extreme wasting
Edema swelling of body tissues as a result offluid accumulation.
Summary Points
• Kwashiorkor typically occurs among children in areas that are characterized bysevere food and nutrition insecurity.
• Kwashiorkor has since its early description among children in Africa been relatedto the consumption of a monotonous diet.
• Earlier kwashiorkor was considered as a result of children consuming a diet highin energy but low in protein.
• Scholars have postulated that kwashiorkor is caused by an excess of free radicals.According to this suggestion, protective pathways are compromised in kwashi-orkor. The pathways require the supply of micronutrients in the form ofantioxidants.
• Food insecurity is a major problem in the DRC with food insecurity and childmalnutrition being most widespread in the rural areas.
• Cassava root is the main staple food crop in most parts of the DRC and it is ofteneaten with a side dish such as stew made of cassava leaves.
• Animal products such as meat and egg are only eaten occasionally, whereas dairyproducts are rarely consumed.
• A longitudinal study examining the relation between diet and kwashiorkor hasbeen carried out using material from Bwamanda an area in northwest Congo.
• The study demonstrated that the risk of developing kwashiorkor in children whowere chronically malnourished increased the longer the children did not consumefood that contained β-carotene.
Diet and Kwashiorkor in the Democratic Republic of Congo 17
References
Babakazo P, Donnen P, Akilimali P, Ali NM, Okitolonda E (2015) Predictors of discontinuingexclusive breastfeeding before six months among mothers in Kinshasa: a prospective study. IntBreastfeed J 10(19):2–9
Bervoets W, Lassance M (1959) Modes et coutumes alimentaires des Congolais en milieu rural:Résultats d’une enquête portant sur le Congo belgeet le Ruanda-Urundi à l’exclusion duKatanga 1955–1957. Académie royale des Sciences coloniales, Brussels
Briend A (2001) Highly nutrient-dense spreads: a new approach to delivering multiple micro-nutrients to high-risk groups. Br J Nutr 85:S175
Briend A, Wojtyniak B, Rowland MGM (1987) Arm circumference and other factors in children athigh-risk of death in rural Bangladesh. Lancet 2(8561):725–728
Burns J, Emerson JA, Amundson K, Doocy S, Caulfield LE, Klemm RD (2016) A qualitativeanalysis of barriers and facilitators to optimal breastfeeding and complementary feeding prac-tices in south Kivu, Democratic Republic of Congo. Food Nutr Bull 37(2):119–131
Ciliberto H, Ciliberto M, Briend A, Ashorn P, Bier D, Manary M (2005) Antioxidant supplemen-tation for the prevention of kwashiorkor in Malawian children: randomised, double blind,placebo controlled trial. Br Med J 330(7500):1109–1111
CMAM Forum (2015) Putting kwashiorkor on the map, Community-based Management of AcuteMalnutrition (CMAM), New York
Coghlan B, Brennan R, Ngoy P, Dofara D, Otto B, Clements M, Stewart T (2006) Mortality in theDemocratic Republic of Congo: a nationwide survey. Lancet 367(9504):44–51
Cousens S, Nacro B, Curtis V, Kanki B, Tall F, Traore E, Diallo I, Mertens T (1993) Prolongedbreast-feeding – no association with increased risk of clinical malnutrition in young-children inBurkina-Faso. Bull World Health Organ 71(6):713–722
Crane RJ, Jones KDJ, Berkley JA (2015) Environmental enteric dysfunction: an overview. FoodNutr Bull 36:S76–S87
Epomedicine (2017) Edema: physical examination [Online]. 18.1. Available: http://epomedicine.com/clinical-medicine/physical-examination-edema/. Accessed 7 Mar 2017
Frenk S, Gomez F, Ramos-Galvan R, Cravioto J (1958) Fatty liver in children; kwashiorkor. Am JClin Nutr 6(3):298–309
Golden MHN, Ramdath D (1987) Free-radicals in the pathogenesis of kwashiorkor. Proc Nutr Soc46(1):53–68
Gopalan C (1992) Kwashiorkor and marasmus: evolution and distinguishing features. Natl Med JIndia 5(3):145–151
Heikens GT, Manary M (2009) 75 years of kwashiorkor in Africa. Malawi Med J 21(3):96–98Heilskov S, Rytter MJH, Vestergaard C, Briend A, Babirekere E, Deleuran MS (2014) Dermatosis
in children with oedematous malnutrition (kwashiorkor): a review of the literature. J Eur AcadDermatol Venereol 28(8):995–1001
IPC (2017) Democratic Republic of the Congo (DRC): current acute food insecurity overview June2016 – January 2017 [Online]. Integrated Food Security Phase Classification (IPC). Available:http://www.ipcinfo.org/ipcinfo-detail-forms/ipcinfo-map-detail/en/c/446422/. Accessed 7 Feb2017
Kandala NB, Madungu TP, Emina JBO, Nzita KPD, Cappuccio FP (2011) Malnutrition amongchildren under the age of five in the Democratic Republic of Congo (DRC): does geographiclocation matter? BMC Public Health 11(261):2–15
Kismul H, Van den Broeck J, Lunde TM (2014) Diet and kwashiorkor: a prospective study fromrural DR Congo. Peerj 2:e350
Manary MJ, Heikens GT, Golden M (2009) Kwashiorkor: more hypothesis testing is needed tounderstand the aetiology of oedema. Malawi Med J 21(3):106–107
Mathys E, Remancus S (2010) Food security country framework for the Democratic Republic ofCongo FY 2011–FY 2015, New York
18 H. Kismul et al.

Ministre du Plan et Révolution de la Modernité de la RDC (2015) Rapport OMD Evaluation desprogrès accomplis par la République Démocratique du Congo dans la réalisation des Objectifsdu Millénaire pour le développement, Kinshasa
République Démocratique du Congo (2007) Enquête Démographique et de Santé RépubliqueDémocratique du Congo 2007, Kinshasa
République Démocratique du Congo (2014) Enquête Démographique et de Santé RépubliqueDémocratique du Congo 2013/14, Kinshasa
Rossi L, Hoerz T, Thouvenot V, Pastore G, Michael M (2006) Evaluation of health, nutrition andfood security programmes in a complex emergency: the case of Congo as an example of achronic post-conflict situation. Public Health Nutr 9(5):551–556
Rytter MJH, Namusoke H, Babirekere-Iriso E, Kaestel P, Girma T, Christensen VB, Michaelsen KF,Friis H (2015) Social, dietary and clinical correlates of oedema in children with severe acutemalnutrition: a cross-sectional study. BMC Pediatr 15(25):2–9
Smith MI, Yatsunenko T, Manary MJ, Trehan I, Mkakosya R, Cheng JY, Kau AL, Rich SS,Concannon P, Mychaleckyj JC, Liu J, Houpt E, Li JV, Holmes E, Nicholson J, Knights D,Ursell LK, Knight R, Gordon JI (2013) Gut microbiomes of Malawian twin pairs discordant forkwashiorkor. Science 339(6119):548–554
Subramanian S, Huq S, Yatsunenko T, Haque R, Mahfuz M, Alam MA, Benezra A, DeStefano J,Meier MF, Muegge BD, Barratt MJ, VanArendonk LG, Zhang Q, Province MA, Petri WA Jr,Ahmed T, Gordon JI (2014) Persistent gut microbiota immaturity in malnourished Bangladeshichildren. Nature 510(7505):417–421
Talbert A, Thuo N, Karisa J, Chesaro C, Ohuma E, Ignas J, Berkley JA, Toromo C, Atkinson S,Maitland K (2012) Diarrhoea complicating severe acute malnutrition in Kenyan children: aprospective descriptive study of risk factors and outcome. PLoS One 7(6):e38321
Termote C, Meyi MB, Djailo BD, Huybregts L, Lachat C, Kolsteren P, Van Damme P (2012) Abiodiverse rich environment does not contribute to a better diet: a case study from DR Congo.PLoS One 7(1):e30533
The World Bank (2013) The Democratic Republic of the Congo: poverty reduction strategy paper,Washington, DC
Trehan I, Manary MJ (2015) Management of severe acute malnutrition in low-income and middle-income countries. Arch Dis Child 100(3):283–287
Truswell AS, Miller JC (1993) Pathogenesis of the fatty liver in protein-energy malnutrition. Am JClin Nutr 57(5):695–696
UNDP (2015) Human development index and its components 2014, United Nations DevelopmentProgramme (UNDP), New York
Weijs B, Hilhorst D, Fer A (2012) Livelihoods, basic services and social protection in DemocraticRepublic of the Congo, Wageningen University, Wageningen
WFP (2014) Comprehensive food security and vulnerability analysis (CFSVA) Democratic Repub-lic of Congo, World Food Programme (WFP), Rome
Whitehead RG, Alleyne GAO (1972) Pathophysiological factors of importance in protein-caloriemalnutrition. Br Med Bull 28(1):72–79
Williams CD (1935) Kwashiorkor: a nutritional disease of children associated with a maize diet.Lancet 226(5855):1151–1152
Diet and Kwashiorkor in the Democratic Republic of Congo 19