diagnosi e stadiazione del carcinoma prostatico maurizio ... · (2014 eau guidelines) ... 10 pts...
TRANSCRIPT

DIAGNOSI E STADIAZIONE DIAGNOSI E STADIAZIONE DEL CARCINOMA PROSTATICODEL CARCINOMA PROSTATICO
Maurizio BrausiMaurizio BrausiDirettore Urologia Ausl ModenaChairman ESOUDirector Prostate Cancer Unit

DIAGNOSI E STADIAZIONE DEL CARCINOMA PROSTATICODIAGNOSI E STADIAZIONE DEL CARCINOMA PROSTATICO
Maurizio BrausiMaurizio BrausiDirettore Urologia Ausl ModenaChairman ESOUDirector Prostate Cancer UnitDirector Prostate Cancer Unit

Persistently Elevated PSA and Negative y gProstatic Biopsies (multiple sets):
Which Strategy ?Which Strategy ?
* Follow–up with PSA and DRE every 6 months* R t bi (S t ti T l t )* Repeat biopsy (Saturation or Template)* Multiparametric –MRI and targeted biopsies p g p* -2-Pro-PSA, PCA3……

Case I
Patient 59 y-old. No familiarity for Pca. PS= 0 DRE: Prostate of 30cc. No induration or suspicious areap
In 2009 Psa was 6.8 ng/ml. P biopsy (8 cores) : BPH + CPBPH + CP.
In 2011 Psa : 8.05 ng/ml. Biopsy: (12 core) : BPH + g p y ( )CP + HGPIN
What do you suggest ?
a. Re-check PSAb. Re-biopy (Saturation vs Template)c Control patient with PSAc. Control patient with PSAd. others

R t Bi I di tiRepeat Biopsy: Indications (2014 EAU Guidelines)
• Rising or persistently elevated PSA• Suspicious DRE• Atipical Small Acinar Proliferation (ASAP)• Atipical Small Acinar Proliferation (ASAP)• High Grade PIN (at 1-3 years)
N t C id th P i k f ti t• Note: Consider the Pca risk of your patient (familiarity, Psa value, velocity, doubling time, ASAP, HGPIN)

Repeat Biopsies: How
• Saturation biopsy (24-30 cores): the incidence of Pca detected by saturation repeat biopsy is 30% -43% and depends on the N of cores sampled p pduring earlier biopsies
• Template biops : (personal e perience) 1 5 core• Template biopsy: (personal experience) 1.5 core x cc of prostate tissue . Detection rate : 50% Always : before focal therapy, AS and ASAP

Repeat Biopsy
If clinical suspicious Cancer persists (+DRE) with negative prostate biopsy M-MRI should be used to evaluate the anterior part of the glandp g
In case of suspicious or positive finding: targeted biops (US F sion): if negati e follo the patientbiopsy (US Fusion): if negative follow the patient with PSA

The Fate of Patients with Elevated PSA who Received Multiple Sets of Prostate Biopsies:
Long term Follow-up (Brausi et al Eur Urol 2010)Long term Follow-up (Brausi et al Eur Urol 2010)
Material and Methods : 51 i h P l d PSA51 pts. with P. elevated PSAMean PSA = 8.5 ng/ml (3.3-13.6 ng/ml)Mean N Sets of biopsies : 2.6 (8-24 cores)I PSS : (5 14) = 45/51 (>21) = 6/51I-PSS : (5-14) = 45/51. (>21) = 6/51
Hystology: BPH = 31/51BPH + chronic prostatis = 16/51BPH + LGPIN = 4/51
Mean Follow-up = 8.2 years (Psa and biopsy if indicated)

R ltResults
• 65% of patients received a 3rd (18) or 4th (12) sets of biopsie for > psa (> 1ng/ml in 1 year)g y
• Histology: 3 sets BPH : 10 pts BPH + chronic prostatitis : 83 sets . BPH : 10 pts. BPH + chronic prostatitis : 8 4 sets. BPH : 6 pts. BPH + chronic prostatitis : 3 Ad i 3 iAdenocarcinoma : 3 patients
• Conclusions: 3/51 pts. (6%) with a persistent p ( ) pelevated PSA after neg. multiple sets of biopsies developed Pca in timedeveloped Pca in time

D Wh t t d i f i t tl l t dD: What to do in case of peristently elevated PSA and negative biopsy ?
Answer: Evaluate the patient risk (familiarity, ASAP,
HGPIN ER (suspicious/no) N of core biopsiesHGPIN, ER (suspicious/no) N of core biopsies previously performed)
Psa velocity o doubling time is importantMRI + US fusion biospy the best option whe decideMRI US fusion biospy the best option whe decide
to biopsyI L i k ti t t l ith PSA 6In Low risk patients: control with PSA every 6 mos

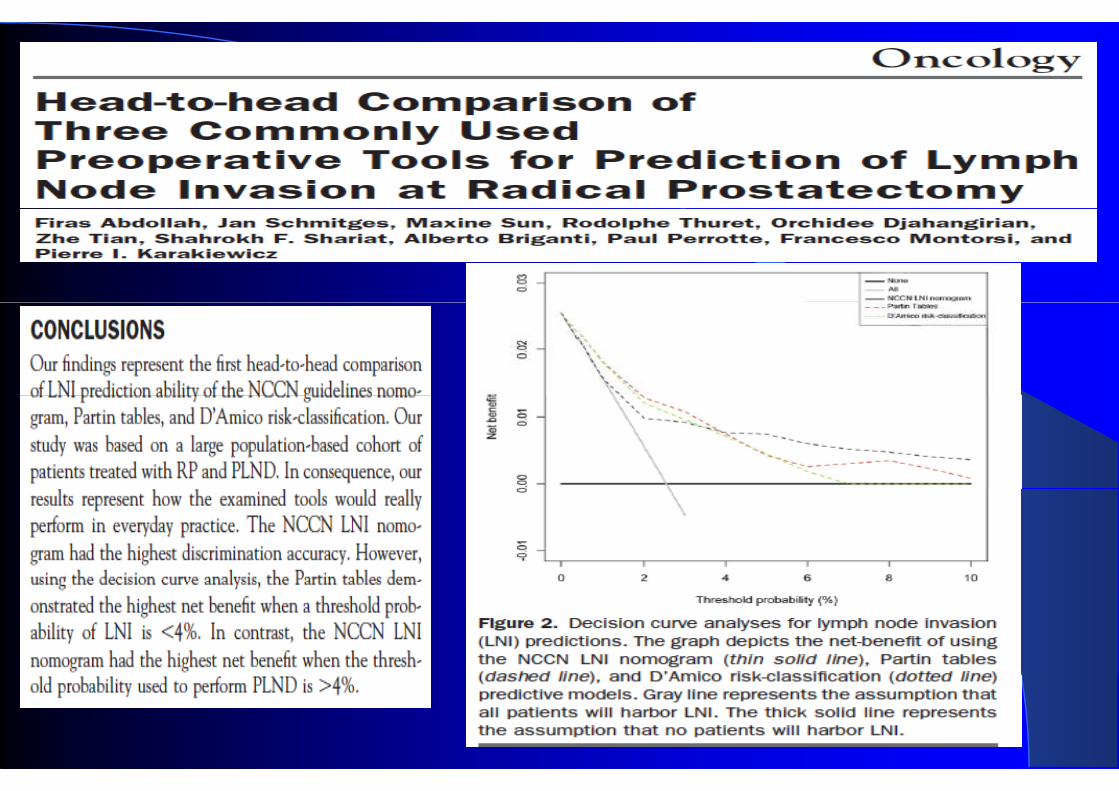
Quale parametri possono essere consideratiQuale parametri possono essere considerati predittivi del N ?p




Qual’e’ il ruolo della linfadenectomia nella RP
Stadiante TerapeuticaStadiante Terapeutica

EAU guidelines 2012- 2013: Indications For LNDIndications For LND



Altre Indagini Nella Diagnosi Di N+
• CT• MRI (High resolution- USPIO) • CT PET Colina• CT-PET Colina• Sentinel Node

N Staging : CT and MRIN Staging : CT and MRI





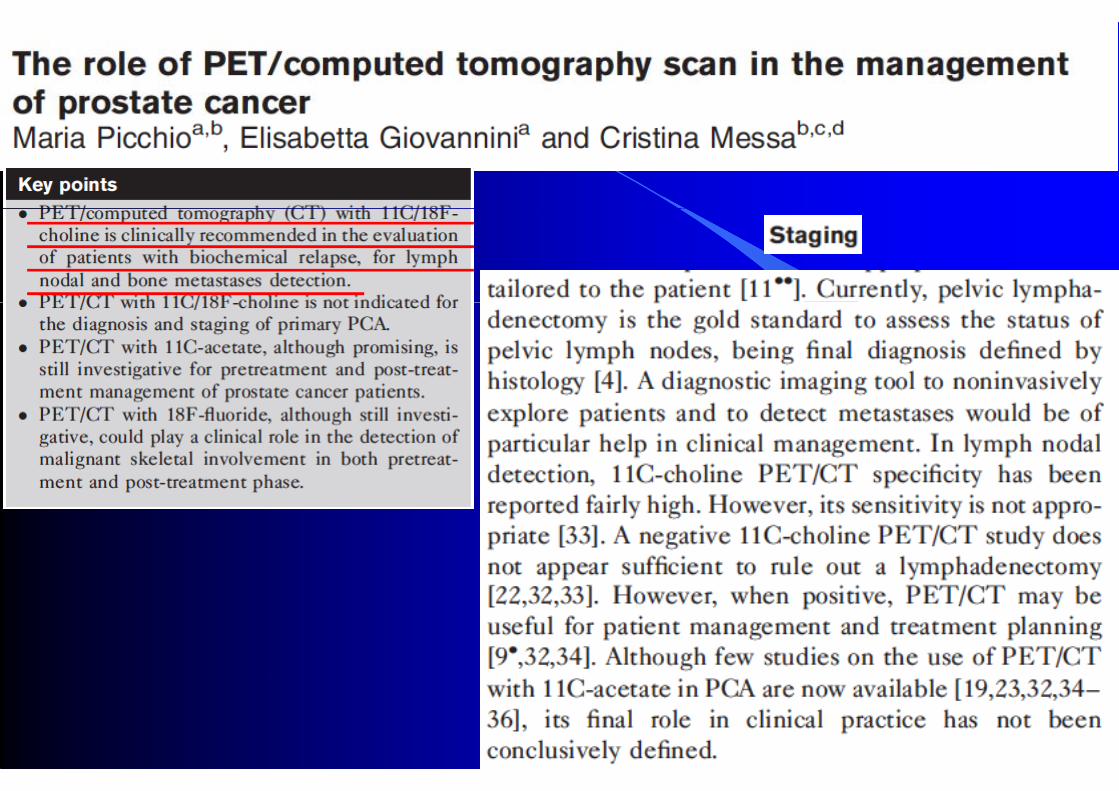
Quale Ruolo ha la Pet/Colina ?

La scintigrafia ossea: Quando dovrebbe essereLa scintigrafia ossea: Quando dovrebbe essere eseguita?g

Quando effettuare la scintigrafia ossea
Quali parametri identificano un significativo rischio di metastasi ossea nello staging pretrattamento ?di metastasi ossea nello staging pretrattamento ?
Quale metodica di imaging identifica meglio unametastasi ossea ?







Q: Bone Scan: Indications
Answer: Bone scan is indicated when PSA is > 20 ng/ml, Gleason score 8 and when patients are psymptomatic with an elevated Alkaline PhosphatasePhosphatase

GRAZIE, per ora…….