design and usability testing of an mhealth application for
TRANSCRIPT

Design and Usability Testing of an mHealth Application for Midwives in Rural Ghana
Olivia Vélez
Submitted in partial fulfillment of the
requirements for the Doctor of Philosophy
under the Executive Committee
of the Graduate School of Arts and Sciences
COLUMBIA UNIVERSITY
2011

© 2011
Olivia Vélez
All rights reserved
ABSTRACT
Design and Usability Testing of a mHealth Application for Midwives in Rural Ghana
Olivia Vélez
Midwives in Ghana provide the majority of rural primary and maternal healthcare
services, but have limited access to data for decision making and knowledge work. Few mobile
health (mHealth) applications have been designed for midwives. The study purpose was to
design and test an mHealth application (mClinic) that can improve data access and reduce the
reporting burden for midwives at the Millennium Villages Project site in Ghana.
From the design science field, the Information Systems Research Framework guided this
study through two research cycles: 1) Relevance, and 2) Design. The first phase of the Relevance
Cycle took a user-centered approach to assess the people, organizations, and technology of the
midwives’ environment through participant observation, contextual inquiry, and interviews. In
the second phase, structured requirements specification was used to categorize the data into
goals, system qualities, and constraints. From the categorized data, use cases were developed for
patient registration, antenatal care, malaria, family planning, and referrals. Use cases then
informed the development of functional requirements. In the Design Cycle, we first used
functional requirements for patient registration and malaria to develop the mClinic prototype as
part of a coded-in-country initiative. Next, we examined usability of the mClinic prototype by
conducting field testing, heuristic evaluation, and usability surveys. Additionally, low-fidelity
prototyping was used to determine applicability of the other use cases to the midwives’
environment.
Midwives reported inability to access critical data, high patient loads, and extensive
reporting requirements. Low technical self-efficacy and inadequate infrastructure were
identified as barriers to implementation. Heuristic evaluation noted issues related to hardware
selection, workflow, and security. Midwives ranked the tool as useful in the usability survey;
however, ease-of-use rankings were neutral. Interviews indicated this was related to low
technical self-efficacy. Applicability checks found support for touch-entry prototypes over those
that included lengthy forms or text-entry.
The study supported the utility of design science and user-centered methods in rural
Ghana for understanding the midwives’ environment, developing functional requirements, and
guiding evaluation. Midwives reported mClinic would facilitate data access and reduce
reporting burdens. Improving midwives data access is essential for clinical decision making and
promoting their knowledge work.
i
TABLE OF CONTENTS
TABLE OF CONTENTS ................................................................................................................. i
LIST OF TABLES ......................................................................................................................... iv
LIST OF FIGURES ........................................................................................................................ v
ABBREVIATIONS ....................................................................................................................... vi
ACKNOWLEDGEMENTS .......................................................................................................... vii
DEDICATION ............................................................................................................................... ix
CHAPTER 1. INTRODUCTION ................................................................................................... 1
Problem Statement ...................................................................................................................... 4
Purpose of Study ......................................................................................................................... 4
Theoretical Framework ............................................................................................................... 5
Relevance cycle ....................................................................................................................... 6
Rigor cycle ............................................................................................................................... 8
Design cycle ............................................................................................................................ 8
Significance of the Study .......................................................................................................... 10
Definition of Concepts .............................................................................................................. 11
Research Questions ................................................................................................................... 12
Conclusion ................................................................................................................................. 14
CHAPTER 2. LITERATURE REVIEW ...................................................................................... 16
Ghana and Health ...................................................................................................................... 16
Maternal Health & Family Planning ..................................................................................... 17
Infectious Disease .................................................................................................................. 17
Non-Communicable Diseases ................................................................................................ 18
Healthcare Workers in Ghana ................................................................................................ 19
Data management and quality ............................................................................................... 19
Training of Rural Midwives .................................................................................................. 20
Information Needs and Practices of Healthcare Workers in Developing Countries ................. 21
Midwives and Nurses as Knowledge Workers Using HIS ....................................................... 23
Health Information Systems in Developing Countries ............................................................. 24
mHealth in Developing Countries ............................................................................................. 25
ii
Emergency services ............................................................................................................... 27
Data collection and disease surveillance ............................................................................... 27
Information resources, diagnostic, and decision support ...................................................... 27
Human-Computer Interaction for Developing Countries (HCI4D) .......................................... 29
Design Science in a Developing Country Context .................................................................... 30
Conclusion ................................................................................................................................. 32
CHAPTER III. METHODOLOGY .............................................................................................. 34
Project Context .......................................................................................................................... 34
Setting........................................................................................................................................ 38
Cycle I. The Relevance Cycle ................................................................................................... 41
Sample ................................................................................................................................... 42
Design .................................................................................................................................... 42
Requirements Analysis .......................................................................................................... 42
Development of Functional Requirements ............................................................................ 44
Cycle II. The Design Cycle ....................................................................................................... 46
Build Phase ............................................................................................................................ 46
Evaluation Phase.................................................................................................................... 47
Summary ................................................................................................................................... 50
CHAPTER IV. RESULTS ............................................................................................................ 51
Cycle 1. Relevance Cycle.......................................................................................................... 51
People .................................................................................................................................... 52
Organizations ......................................................................................................................... 61
Technology ............................................................................................................................ 63
Problems and Opportunities .................................................................................................. 64
Cycle 2. Design Cycle ............................................................................................................... 72
Build Phase ............................................................................................................................ 72
Evaluation Phase.................................................................................................................... 73
Summary ................................................................................................................................... 76
CHAPTER 5. DISCUSSION ........................................................................................................ 78
Summary of Study ..................................................................................................................... 78
Discussion of Results ................................................................................................................ 78
iii
Relevance Cycle .................................................................................................................... 79
Design Cycle.......................................................................................................................... 86
Functional Specifications Revisited ...................................................................................... 88
Contributions ............................................................................................................................. 88
Theory .................................................................................................................................... 88
Methods ................................................................................................................................. 89
mHealth in Developing Countries ......................................................................................... 89
Project Implications................................................................................................................... 90
General Implications ................................................................................................................. 90
Strengths .................................................................................................................................... 91
Limitations ................................................................................................................................ 92
Future Research ......................................................................................................................... 92
Conclusions ............................................................................................................................... 93
REFERENCES ............................................................................................................................. 94
APPENDIX A. Modified Health I-TUES Survey ...................................................................... 105
APPENDIX B. Mobile Devices Used in Study .......................................................................... 107
APPENDIX C. Samples of Low-Fidelity Prototypes ................................................................. 109
iv
LIST OF TABLES
Table 1.1 Summary of Concepts and Definitions 11
Table 1.2 Aims, Research Questions, and ISR Framework Cycle 14
Table 3.1 Outline of Study 40
Table 3.2 Data sources of structured requirements specification 45
Table 3.3 Mobile Usability Heuristics 50
Table 4.1 Classification of Midwives Interviewed 52
Table 4.2 Visit Times and Interruptions 54
Table 4.3 Monthly Reports 56
Table 4.4 Information Sources Used by Midwives 58
Table 4.5 Network and Internet Outages 63
Table 4.6 Use Case for Fever Registration 65
Table 4.7 Use Cases for Patient Registration 66
Table 4.8 List of System Qualities with Rationale 67
Table 4.9 Overview of Planned Forms 69
Table 4.10 Functional Specification and Uses Cases for Patient Registration 70
Table 4.11 Functional Specifications for Fever Registration 71
Table 4.12 Summary of Health I-TUES Survey 74
Table 4.13 Usability Issues and Severity Rankings 75
v
LIST OF FIGURES
Figure 1.1 Design Science Research Cycles 6
Figure 1.2 Temporal System Model 7
Figure 1.3 Study Concepts and Outputs 10
Figure 2.2 General Methodology of Design Science Research 32
Figure 3.1 Typical Road in Rural Ghana 36
Figure 3.2 Data Flow Chart for MGV-Net 37
Figure 3.3 Map of Health Clinic Locations 39
Figure 3.4 Structured Requirements Specification 44
Figure 3.5 Overview of Design Cycle Evaluation Phase 47
Figure 3.6 Sample of Low-Fidelity Prototype 49
Figure 4.1 Typical Clinical Workflow 53
Figure 4.2 Notifiable Disease Report 57
Figure 4.3 Fever Register 62
Figure 4.4 Sample Screen Shots of mClinic Interface 73
Figure 5.1 Paper Medical Records 84
vi
ABBREVIATIONS
ACT Arteminisen Combination Therapy
ANC Antenatal care
CHN Community Health Nurse
CHW Community Health Worker
CPG Clinical Practice Guideline
GHS Ghana Health Service
GPRS General Packet Radio Service
HCI4D Human-Computer Interaction for Development
HEW Health Extension Worker
Health I-TUEM Health Information Technology Usability Evaluation Model
Health I-TUES Health Information Technology Usability Evaluation Scale
HIS Health Information Systems
ICT Information and Communication Technology
IFA Iron Folate (tablets)
ISO International Standards Organization
ITN Insecticide Treated (bed)Nets
ISR Framework Information Systems Research Framework
mHealth Mobile Health
MDGs Millennium Development Goals
MGV-Net Millennium Global Village Network
MVP Millennium Villages Project
NGO Non-Governmental Organization
NHIS National Health Insurance Scheme
ODK Open Data Kit
PDA Personal Digital Assistant
PHR Personal Health Record
PMTCT Prevention of Mother-to-Child Transmission of HIV
RDT Rapid Diagnostic Test
SP Sulfadoxine-Pyrimethamine
TAM Technology Acceptance Model
TBA Traditional Birth Attendant
UN United Nations
UNDP United Nation Development Programme
USAID United States Agency for International Development
USD United States Dollars
WHO World Health Organization
XML eXtensible Markup Language
vii
ACKNOWLEDGEMENTS
Many people touched and influenced this work and I wish to thank them all with my
deepest, heartfelt gratitude. First and foremost, I would like to thank my adviser, Dr. Suzanne
Bakken, who has been a mentor, role model, and friend throughout this process. This work
would never have been accomplished without her belief, support, and encouragement in me.
Second, I would like to thank Dr. Patricia Mechael and Dr. Andrew Kanter for giving me
an opportunity to work on the MGV-Net project; introducing me to the mHealth for development
community; for their encouragement, advice, and support; and, for their inspiring dedication to
improving global health.
I would also like to thank my committee members: Dr. Richard Garfield, Dr. Sarah Cook,
and Dr. Jaqueline Merrill. Their feedback and encouragement was invaluable in tying all the
different pieces of my work together.
I also want to thank all the people who contributed to this project. First, to the midwives
and staff at the MVP site in Bonsaaso, Ghana, for taking time out of their day to talk with me in
length about their work, struggles, and hopes for improving rural health in Ghana. I especially
thank Portia Boakye Okyere for all her help. I would also like to thank the members of the MVP
mHealth team for their work on this project. Finally, thank you to Yaw Anokwa for his advice
on using Open Data Kit (ODK) and all those who have contributed to the development of ODK,
especially the staff at Mindflow for their past and continued work on the development of
mClinic.
Many of the faculty, staff, and students at both the School of Nursing and the Department
of Biomedical Informatics supported me through this project. I would like to give thanks to many
proof readers/editors/advisers: Dr. Yalini Senathirajah and Nicole Gellar, who both read multiple
viii
iterations of my dissertation without bribery; Dr. Robert Lucero, Dr. Sunmoo Yoon, and Dr.
Barbara Sheehan who provided critical advice and support throughout the process; Dr. David
Kaufman who provided advice on HCI and use-case development; my cohort support group,
Shanelle Nelson and Annie Rohan; and many other students and staff who attended my defense
practice and provided last minute editing and feedback.
Many people touched my career along this path. Dr. Sheila Browne, who’s Research
Explorations program started me on this path. Teena Johnson-Smith, who first taught me about
computers. Laurie Wojtusik, who gave me my first clinical informatics job, through neither of
us knew it at the time. Everyone at Hudson River HealthCare, my experiences there, from
summer intern to EHR project manager and strategic planning facilitator, to staff nurse, will
forever influence my career. Dr. Leanne Currie, who introduced me to nursing informatics
research.
My dissertation was supported by a number of different grants and I would like to thank
all the people and organizations who contribute to making funding for this type of research
possible: P30NR010677, 1D11 HP07346, IDRC, Rockefeller Foundation, Novartis Fund for
Sustainable Development, and the OpenROSA Consortium. I would especially like to thank
Donald and Barbara Jonas and everyone at the Jonas Center for Nursing Excellence for their
continuing generosity and recognition of the importance of nursing.
Finally, I would like to thank my family: my parents for their never-ending support; my
mother-in-law for providing me with a quiet place to work in the last few months of writing; my
husband, Sergio, for always having coffee ready, for giving me the opportunity to follow my
dreams while raising a child, and for helping me stay balanced.
ix
DEDICATION
To my daughter Amaya, who was lulled to sleep by journal articles instead of fairy tales,
it is my deepest wish that this work will make the world a little bit better for you.
1
CHAPTER 1. INTRODUCTION
Midwives provide the majority of primary care, maternal care, and emergency obstetric
care in rural Ghana (Prosser, Sonneveldt, Hamilton, Menottie, & Davis, 2006). Though 70% of
Ghana’s population is located in rural areas, the majority of physicians are found in urban areas,
primarily working in tertiary care centers (Prosser, et al., 2006; Taylor, 1992). Evidence has
shown that inadequate distribution of healthcare workers has a negative impact on health
outcomes (Anand & Bärnighausen, 2007; Speybroeck, Kinfu, Dal Poz, & Evans, 2006).
Midwives are considered an essential part of the healthcare workforce in sub-Saharan Africa,
particularly for improving health outcomes in rural settings (Fullerton, Johnson, Thompson, &
Vivio, 2011).
Ghana has made significant strides in reducing its maternal mortality ratio, from 731 per
100,000 live births in 1980 down to 409 per 100,000 live births in 2008 (Hogan et al., 2010).
Improving access to skilled birth attendants, such as formally trained nurse-midwives, has been a
key to this reduction in maternal mortality rates across sub-Saharan Africa (Alvarez, Gil,
Hernandez, & Gil, 2009). Evidence from a recent USAID report indicates that the population of
midwives in Ghana is aging towards retirement; newly graduated midwives have little incentive
to work in rural areas and may be immigrating to other countries for employment; and, midwives
are inadequately distributed throughout the country to meet the healthcare needs of rural
populations (Prosser, et al., 2006). An insufficient midwifery workforce will likely stall or
reverse the reductions that Ghana has made in maternal mortality as well having a negative
impact on other health outcomes (Gerein, Green, & Pearson, 2006; Prosser, et al., 2006).
There are many factors that contribute job dissatisfaction and high turnover rates among
midwives in rural Ghana. Addressing health workforce issues will require a multifaceted
2
intervention (WHO, 2006b). Poor work environment, high administrative burdens, and work
overload have been identified as key contributing factors (Gerein, et al., 2006; Prosser, et al.,
2006; Snow et al., 2011).
Health information systems (HIS) may be useful in addressing some of the issues and
challenges faced by midwives in rural Ghana. HIS have been shown to improve the quality and
efficiency of healthcare provision (Chaudhry et al., 2006; Tomasi, Facchini, & Santos Maia,
2004). Additionally, effective HIS allow nurses and midwives to function as knowledge
workers, a role in which they gather, use, and build new knowledge (Snyder-Halpern, Corcoran-
Perry, & Narayan, 2001). The knowledge worker role has been found to increase nurses’ feelings
of autonomy and accountability, which has a positive effect on job satisfaction (Finn, 2001;
Pierce, Hazel, & Mion, 1996; Ward & Kozakowski, 1987). However, implementation of HIS in
developing countries has been challenging with many projects failing (Heeks, 2002). Selection
of the appropriate technology and thoughtful design is critical to the success of any
implementation (Braa, Hanseth, Heywood, Woinshet, & Shaw, 2007; Gerber, Olazabal, Brown,
& Pablos-Mendez, 2010; Mechael, 2009a).
An emerging area of HIS is mobile health, or mHealth, which is defined as the use of
mobile technology, such as cellular phones, wireless devices, or radio frequency identification
tags, for healthcare or health services (mHealth Alliance, 2010). Early applications of mHealth
was provided through the use of handheld devices known as personal digital assistants (PDAs)
that provided various information resources such as medication dictionaries or point-of-care
decision support (Istepanian, Laxminarayan, & Pattichis, 2006). The ability to develop
applications on PDAs was limited due to lack of memory, screen space, poor graphical display,
and inability to transfer data wirelessly to and from the device. Over time, however, PDAs have
3
become more powerful, allowing for more memory and data storage, full color graphical
interfaces with video capability, integration of wireless access and integration with cellular
devices into what we now know as smartphones, with the most popular being iPhones,
Blackberry, and Android devices. Designing usable systems on mobile devices faces unique
challenges due to limited screen space, limited processing power, ergonomic considerations, and
security issues (Bertini, Gabrielli, & Kimani, 2006; Jones & Marsden, 2006).
Despite the wide variety of HIS and mHealth applications designed for developing
countries, outcomes related to use of these tools have been mixed and studies assessing the
design and evaluating their outcomes have been limited (Mechael, 2009a; Mechael & Sloninsky,
2008; Tamrat & Kachnowski, 2011; Tomasi, et al., 2004). Challenges of HIS deployments in
developing countries include unstable or unavailable power sources; limited or nonexistent
internet connectivity; largely computer and technology naïve workforces; varying and rapidly
changing legal and governmental regulations; and the need for culturally and locally relevant
information that is not generally found in existing information resources (Braa, et al., 2007;
Gerber, et al., 2010; Heeks, 2006; Mechael & Sloninsky, 2008).
The need to understand the environment for which an application is being designed
cannot be overemphasized. The consequence of poor HIS design can lead to end-user
frustration, decreased productivity, project failure, and medical errors. An analysis of an HIS
deployment in South Africa found that its failure could be attributed to inadequate infrastructure
assessment, insufficient training and support of end-users, and lack of understanding of end-user
needs and the intricacy of healthcare tasks; with an associated monetary loss of $22 million USD
(Littlejohns, Wyatt, & Garvican, 2003). Berg suggests that these failures may occur when HIS
implementations are viewed as a technical project rather than a process of sociotechnical change
4
that requires continual adaptation and development of both the end users and the software
(2001). This begins with a grounded understanding of the end users, their tasks, and the
environment in which the application will be deployed and is cycled through simulations and
prototyping to understand how the application will work in and alter the end users environment
(Gould & Lewis, 1985).
Problem Statement
Midwives in rural Ghana report high levels of job dissatisfaction that results inability of
Ghana Health Services (GHS) to retain and recruit an adequate number of midwives to meet the
populations health needs. The shortage of midwives in rural Ghana will likely stall or reverse
the progress Ghana has made in reducing maternal mortality, providing adequate treatment for
malaria, and other GHS health goals. Key factors contributing to job dissatisfaction have been
poor working environment, professional isolation, and high administrative burden.
Health information system (HIS) technologies, such as mHealth, can provide a
mechanism for streamlining administrative work and decreasing professional isolation while also
giving opportunities for improving point-of-care decision support and knowledge development.
However, implementing such technologies in a developing country is challenging, as
demonstrated by the high failure rates and lack of sustainability of various HIS implementations
attempted in developing settings in the last decade. Appropriately designing systems for
developing countries is especially critical given the limited resources available for improving
healthcare infrastructure in such low resource settings.
Purpose of Study
The purpose of this study was to design and test an mHealth application for use by
midwives working in rural health facilities in Ghana. This study uses the Information Systems
5
Research (ISR) framework to guide our understanding of the environmental context, which
includes people, organization, and technology, for which the artifact is being developed as well
as to gain an understanding of the distinctive problems and opportunities that implementing in
such a setting present.
This study used an action research approach by including active participation and design
input of stakeholders at the study site in Bonsaaso, Ghana. The Millennium Villages Project is a
model community under charter by the United Nations for eliminating extreme poverty, defined
as those who make less than $1.25USD/day, through science-based and sustainable strategies for
addressing healthcare, education, environment, and human rights (Kanter et al., 2009).
Theoretical Framework
The theoretical framework for this study is the ISR Framework in which various design
processes are employed in order to build a product or a design artifact (Hevner, March, Park, &
Ram, 2004). The design and development cycle is repeated iteratively until a desired final
product is achieved. Hevner’s approach proposes that design science research projects using the
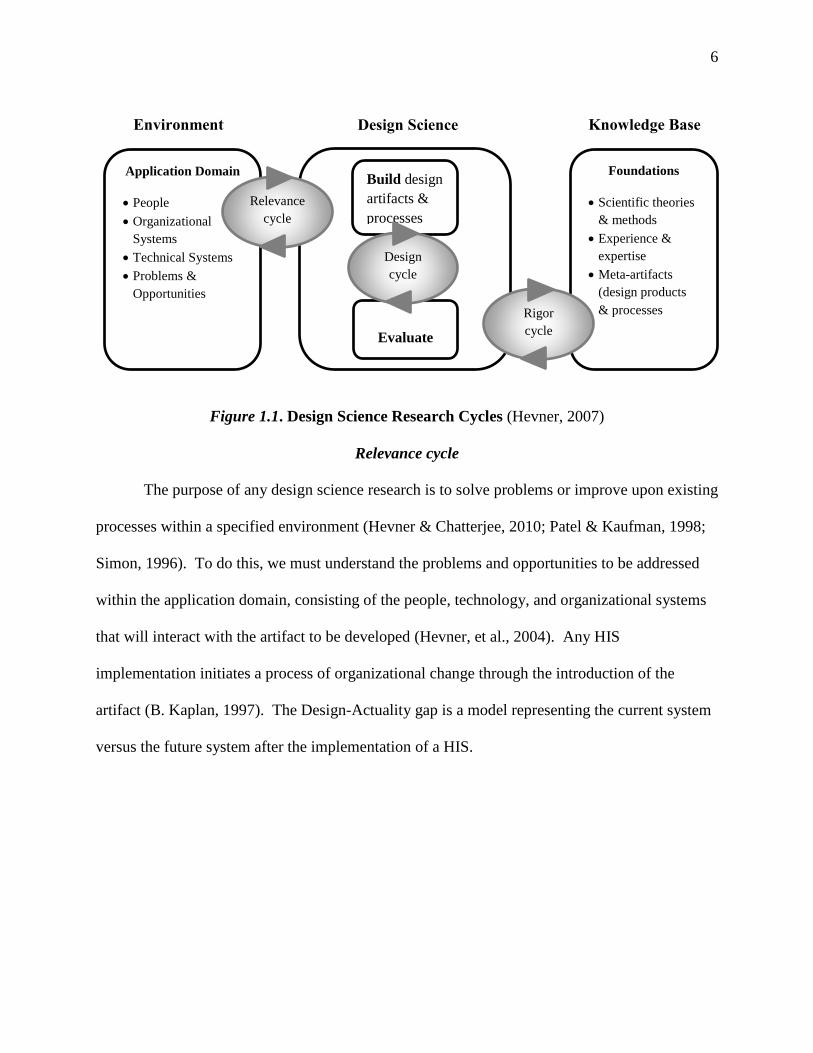
ISR framework should consist of three research cycles, shown in Figure 1.1: the relevance cycle
in which we seek to understand the environment of the research project by determining
requirements and conducting field testing; the design cycle in which artifacts are produced and
evaluated; and, the rigor cycle in which evaluation of artifacts and processes can contribute to the
design science and application domain knowledge base (Hevner, 2007).
6
Figure 1.1. Design Science Research Cycles (Hevner, 2007)
Relevance cycle
The purpose of any design science research is to solve problems or improve upon existing
processes within a specified environment (Hevner & Chatterjee, 2010; Patel & Kaufman, 1998;
Simon, 1996). To do this, we must understand the problems and opportunities to be addressed
within the application domain, consisting of the people, technology, and organizational systems
that will interact with the artifact to be developed (Hevner, et al., 2004). Any HIS
implementation initiates a process of organizational change through the introduction of the
artifact (B. Kaplan, 1997). The Design-Actuality gap is a model representing the current system
versus the future system after the implementation of a HIS.
Design Science
Application Domain
People
Organizational
Systems
Technical Systems
Problems &
Opportunities
Build design
artifacts &
processes
Evaluate
Foundations
Scientific theories
& methods
Experience &
expertise
Meta-artifacts
(design products
& processes
Relevance
cycle
Design
cycle
Rigor
cycle
Environment Knowledge Base
7
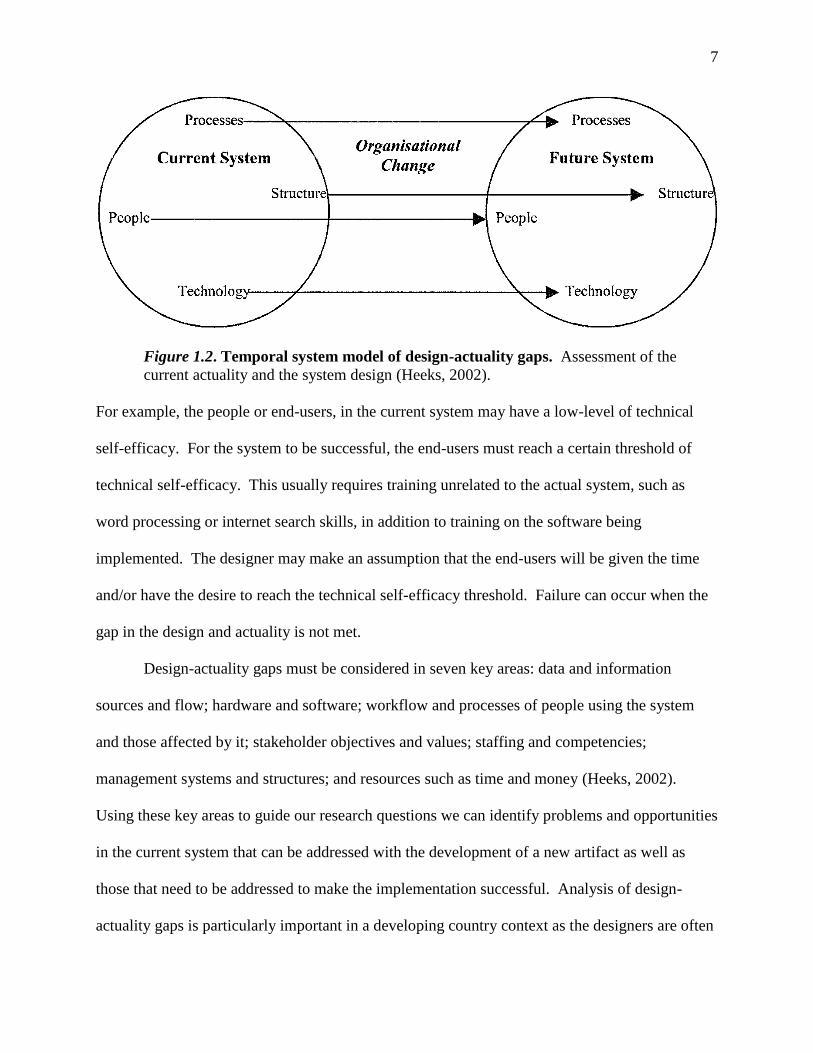
Figure 1.2. Temporal system model of design-actuality gaps. Assessment of the
current actuality and the system design (Heeks, 2002).
For example, the people or end-users, in the current system may have a low-level of technical
self-efficacy. For the system to be successful, the end-users must reach a certain threshold of
technical self-efficacy. This usually requires training unrelated to the actual system, such as
word processing or internet search skills, in addition to training on the software being
implemented. The designer may make an assumption that the end-users will be given the time
and/or have the desire to reach the technical self-efficacy threshold. Failure can occur when the
gap in the design and actuality is not met.
Design-actuality gaps must be considered in seven key areas: data and information
sources and flow; hardware and software; workflow and processes of people using the system
and those affected by it; stakeholder objectives and values; staffing and competencies;
management systems and structures; and resources such as time and money (Heeks, 2002).
Using these key areas to guide our research questions we can identify problems and opportunities
in the current system that can be addressed with the development of a new artifact as well as
those that need to be addressed to make the implementation successful. Analysis of design-
actuality gaps is particularly important in a developing country context as the designers are often
8
from industrialized countries, as is the case in the study, and may make assumptions about the
actuality that are incorrect (Heeks, 2002). The design-actuality gap model has been used in case-
studies for understanding why HIS projects have failed (Best & Kumar, 2008; Gerhan & Mutula,
2007; Hawari & Heeks, 2010). These case studies can highlight common mistakes that can be
avoided during the design of and HIS project to prevent failure.
Rigor cycle
The rigor cycle guided our selection of theories and methods for constructing and
evaluating the artifact (Hevner & Chatterjee, 2010). Our selection of methods came from the
literature review in Chapter 2 as well as the expertise of the research team. Within the literature
review, methods were appraised for potential modification appropriate for use in a developing
country context. Additionally, a search of both peer-reviewed and grey literature was conducted
for existing artifacts that could meet the functional specifications and systems qualities drawn
from the relevance cycle.
Design cycle
The design cycle is sub-divided into two phases: Develop/Build and Evaluate. In the
Develop/Build phase the focus is on the creation of a highly usable artifact. Usability is defined
as the user’s ability to perform the desired task using the artifact in the intended environment
(Bennett, 1984). Usability has been shown to be a predictor of technology acceptance in HIS
implementations (Carayon et al., 2011). The relevance cycle informs the functional
requirements and system qualities of the artifact while the rigor cycle informs the design of the
artifact (Hevner, 2007).
In the build phase, we contracted with a software company in sub-Saharan Africa as part
of a coded-in-country initiative. The coded-in-country initiative supports information and
9
communication technology (ICT) capacity building in Africa by giving project opportunities to
local programmers and entrepreneurs rather than outsourcing the work to ICT teams from highly
developed countries (Dimagi, 2011).
In the evaluation phase of the design cycle, we apply the Health Information Technology
Usability Evaluation Model (Health-ITUEM). Health I-TUEM is a model of usability evaluation
that integrates subjective measures of usability through the technology acceptance model (TAM)
and objective measures of usability through ISO 9241-11 (Yen, 2010). The TAM model posits
that perceived usefulness and perceived ease-of-use predicts a clinician’s intention to use a
particular HIS (Venkatesh, 2003). ISO 9241-11 provides guidelines for objectively evaluating
usability in relation to system effectiveness, user and system performance, and user satisfaction
(UsabilityNet, 1998). Health-ITUEM provides a comprehensive model for assessing usability
using both subjective and objective measures (Yen, 2010).
The research questions for this dissertation fall within the relevance cycle and the
evaluation phase of the design cycle. Figure 1.3 presents the concepts and the expected outputs.

10
Figure 1.3. Study concepts and outputs.
Significance of the Study
The significance of this study is three fold. First, our application will establish the
usefulness of applying the ISR framework in low-resource settings as a means of understanding
the environmental context. Second, we will produce an artifact that has the potential for reducing
data collection and sharing inefficiencies in the application setting, improving the quality of data
collected, to serve as a professional resource, and provide a means for collecting data for patient
management and public health surveillance. This will allow midwives to move from mere data
gathers to true knowledge workers. Third, we will to establish a set of best practices in assessing
Relevance Cycle Design Cycle:
Develop/Build
Design Cycle:
Evaluate ISR
Framework
Concepts Functional
Requirements
Artifact
Produced
(outputs)
Model Design-Actuality
Gaps
Functional
specifications
Use Cases
System
Qualities
mClinic
Prototype
Health I-
TUEM
Usability
Data Sources
Observations of
staff
Interviews with
staff
Investigator field
notes
Literature review
Health I-TUES
Mobile usability heuristic
evaluation
Investigator field notes
Observations of staff during
prototype use
Post-testing interviews
Refined
specifications
11
environmental context in low-resource settings and contribute to the design knowledge base in a
development context.
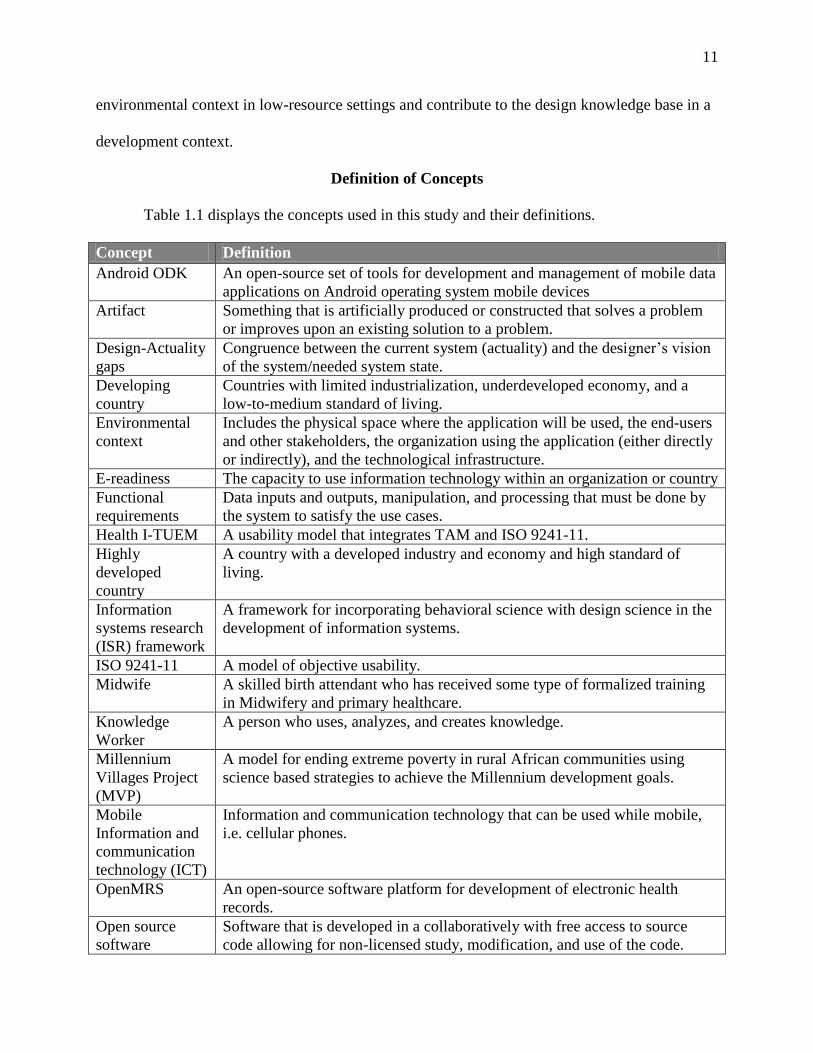
Definition of Concepts
Table 1.1 displays the concepts used in this study and their definitions.
Concept Definition
Android ODK An open-source set of tools for development and management of mobile data
applications on Android operating system mobile devices
Artifact Something that is artificially produced or constructed that solves a problem
or improves upon an existing solution to a problem.
Design-Actuality
gaps
Congruence between the current system (actuality) and the designer’s vision
of the system/needed system state.
Developing
country
Countries with limited industrialization, underdeveloped economy, and a
low-to-medium standard of living.
Environmental
context
Includes the physical space where the application will be used, the end-users
and other stakeholders, the organization using the application (either directly
or indirectly), and the technological infrastructure.
E-readiness The capacity to use information technology within an organization or country
Functional
requirements
Data inputs and outputs, manipulation, and processing that must be done by
the system to satisfy the use cases.
Health I-TUEM A usability model that integrates TAM and ISO 9241-11.
Highly
developed
country
A country with a developed industry and economy and high standard of
living.
Information
systems research
(ISR) framework
A framework for incorporating behavioral science with design science in the
development of information systems.
ISO 9241-11 A model of objective usability.
Midwife A skilled birth attendant who has received some type of formalized training
in Midwifery and primary healthcare.
Knowledge
Worker
A person who uses, analyzes, and creates knowledge.
Millennium
Villages Project
(MVP)
A model for ending extreme poverty in rural African communities using
science based strategies to achieve the Millennium development goals.
Mobile
Information and
communication
technology (ICT)
Information and communication technology that can be used while mobile,
i.e. cellular phones.
OpenMRS An open-source software platform for development of electronic health
records.
Open source
software
Software that is developed in a collaboratively with free access to source
code allowing for non-licensed study, modification, and use of the code.
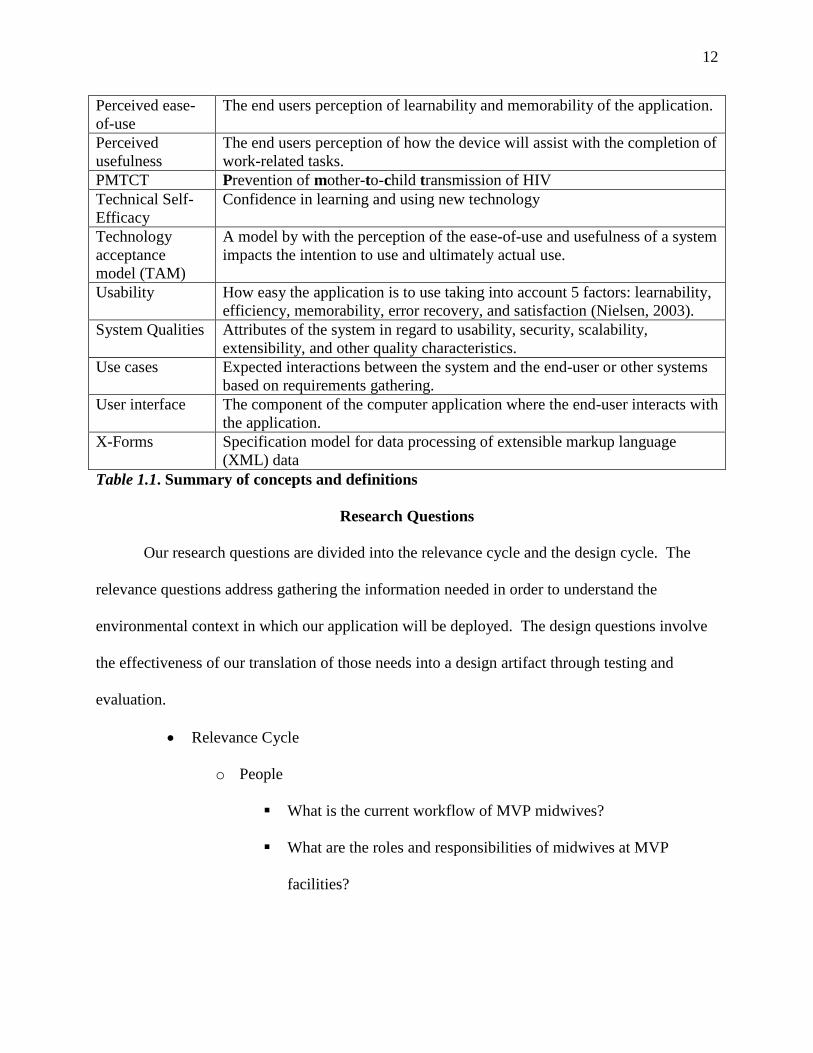
12
Perceived ease-
of-use
The end users perception of learnability and memorability of the application.
Perceived
usefulness
The end users perception of how the device will assist with the completion of
work-related tasks.
PMTCT Prevention of mother-to-child transmission of HIV
Technical Self-
Efficacy
Confidence in learning and using new technology
Technology
acceptance
model (TAM)
A model by with the perception of the ease-of-use and usefulness of a system
impacts the intention to use and ultimately actual use.
Usability How easy the application is to use taking into account 5 factors: learnability,
efficiency, memorability, error recovery, and satisfaction (Nielsen, 2003).
System Qualities Attributes of the system in regard to usability, security, scalability,
extensibility, and other quality characteristics.
Use cases Expected interactions between the system and the end-user or other systems
based on requirements gathering.
User interface The component of the computer application where the end-user interacts with
the application.
X-Forms Specification model for data processing of extensible markup language
(XML) data
Table 1.1. Summary of concepts and definitions
Research Questions
Our research questions are divided into the relevance cycle and the design cycle. The
relevance questions address gathering the information needed in order to understand the
environmental context in which our application will be deployed. The design questions involve
the effectiveness of our translation of those needs into a design artifact through testing and
evaluation.
Relevance Cycle
o People
What is the current workflow of MVP midwives?
What are the roles and responsibilities of midwives at MVP
facilities?
13
What is the current experience of the midwives with technology
and their comfort level in learning new technology?
What are the information needs and information seeking behaviors
of midwives working in MVP facilities in Ghana?
o Organizations
What are the issues in collecting data from the health facilities?
What is the support capacity for and HIS implementation at MVP
Ghana?
o Technology
What is the current technology infrastructure at MVP Ghana?
o Problems & Opportunities
What are the functionality requirements for the application based
on the needs and constraints of the application environment?
Design Cycle
o Justify/Evaluate
What usability issues exist with the artifact?
What are the deficiencies in functionality or qualities of the artifact
that need to be addressed to improve acceptance?
How does the artifact meet heuristic standards?
Table 1.2 organizes the research questions by study aims and ISR cycle.
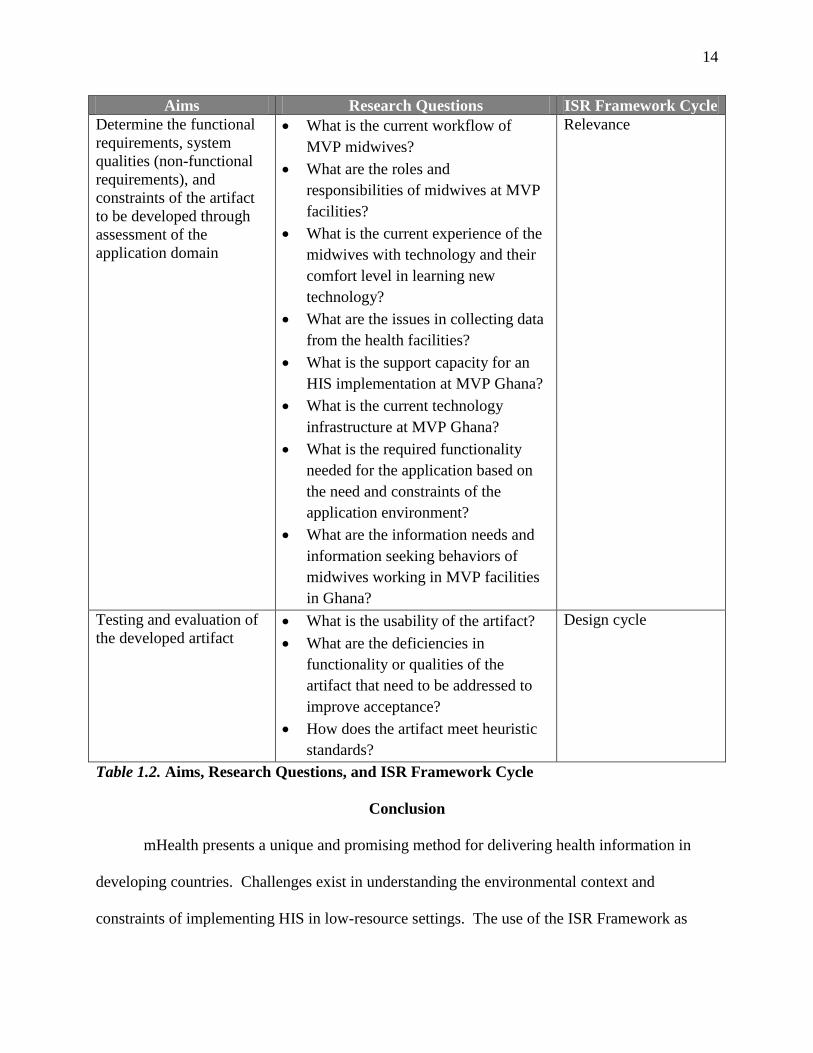
14
Aims Research Questions ISR Framework Cycle
Determine the functional
requirements, system
qualities (non-functional
requirements), and
constraints of the artifact
to be developed through
assessment of the
application domain
What is the current workflow of
MVP midwives?
What are the roles and
responsibilities of midwives at MVP
facilities?
What is the current experience of the
midwives with technology and their
comfort level in learning new
technology?
What are the issues in collecting data
from the health facilities?
What is the support capacity for an
HIS implementation at MVP Ghana?
What is the current technology
infrastructure at MVP Ghana?
What is the required functionality
needed for the application based on
the need and constraints of the
application environment?
What are the information needs and
information seeking behaviors of
midwives working in MVP facilities
in Ghana?
Relevance
Testing and evaluation of
the developed artifact What is the usability of the artifact?
What are the deficiencies in
functionality or qualities of the
artifact that need to be addressed to
improve acceptance?
How does the artifact meet heuristic
standards?
Design cycle
Table 1.2. Aims, Research Questions, and ISR Framework Cycle
Conclusion
mHealth presents a unique and promising method for delivering health information in
developing countries. Challenges exist in understanding the environmental context and
constraints of implementing HIS in low-resource settings. The use of the ISR Framework as

15
proposed in this study will provide a guideline for an action research approach to application
design and evaluation in a developing country. Midwives in rural Ghana need reliable,
accessible, and accurate data to fully apply their domain knowledge to both patient and
population care. Furthermore, this work will result in the development of an artifact that can be
customized for use in similar settings for addressing healthcare workers information needs while
improving clinical decision making with the potential to improve patient outcomes and support
healthcare systems infrastructure.
16
CHAPTER 2. LITERATURE REVIEW
This literature review will first provide a brief profile of Ghana with information on the
country’s key health issues. This is followed by the literature on the information needs of
healthcare workers in developing countries with a focus on the role of midwives in meeting rural
healthcare needs, the use of health information systems in developing countries with a focus on
mHealth, and methods in design science.
Ghana and Health
Ghana, located in Western Africa, was the first sub-Saharan African nation to gain
independence from its colonial rulers in 1957 and has had a stable democracy for the past few
decades. Ghana is a tropical country roughly the size of Oregon with a population of 25 million
(CIA, 2011). It is an ethnically, religiously, and linguistically diverse country. Though English
is the national language and is used in educational settings, less than 36% of the population
speaks it, especially in rural areas, and the adult literacy is approximately 66% (Trudell, 2009;
UNICEF, 2010). Ghana has a gross domestic product per capita of $306 USD (Nguyen,
Rajkotia, & Wang, 2011). The recent discovery of oil deposits in Ghana have brought economic
growth and expansion to the country; the number of Ghanaians living in extreme poverty is
rapidly declining and the country is expected to reach middle income status by 2020 (Ede, Sousa,
Dhaliwal, & Munait, 2011).
The life expectancy at birth for males is 56 years and females is 58 years (WHO, 2011a).
Though the incidence of HIV/AIDS, at 1.8%, is lower than the average incidence of 5.0 % in
other sub-Saharan African nations, the lack of available treatment and the high mortality rate still
make it a pressing issue (HIV InSite, 2011). Other leading causes of death include: malaria,
lower respiratory infections, perinatal conditions, stroke and heart disease, diarrheal diseases and
17
tuberculosis (WHO, 2006a). The WHO estimates the under-five mortality rate for 2005 to be
112 per 1000 live births with malaria (33%), neonatal complications (28%), pneumonia (15%),
diarrheal diseases (12%), and HIV/AIDS (6%) as leading causes (2006a).
Maternal Health & Family Planning
Estimates for maternal mortality rates in Ghana for 2005 range from 378 to 560 per
100,000 live births, and despite discrepancies, remain higher than WHO and government goals
(Asamoah, Moussa, Stafstrom, & Musinguzi, 2011). Maternal mortality is the second leading
cause of death, after infectious disease, among Ghanaian women 12-49 years old, with the most
common cause of maternal death being from post-partum hemorrhage (Andreatta, Gans-Larty,
Debpuur, Ofosu, & Perosky; Ghana Statistical Services, Ghana Health Service, & Macro
International, 2009). In rural areas, lack of skilled attendants, financial resources, and accessible
emergency obstetric care lead to an increased risk of maternal death (Fofie & Baffoe, 2010). The
fertility rate in Ghana is 3.9 births per woman (The World Bank, 2011) with 0.7 births per
woman reported as unintended. Unmet family planning needs are reported by 34% of Ghanaian
women, with a higher rate in rural areas (Johnson & Madise, 2011).
Infectious Disease
Ghana has made great progress towards reducing the transmission of HIV. The
prevalence of HIV decreased from 3.6% in 2003 to 1.8% in 2009 (Ede, et al., 2011). However,
disparities remain between socio-economic groups on access to antiretroviral therapies with only
24% of those needing treatment actually receive it (UNAIDS, 2010). Additionally, condom use
in rural areas and HIV testing in married couples is not widely accepted (Aheto & Gbesemete,
2005).
18
Malaria remains a significant cause of morbidity and mortality in Ghana, particularly
among children under five, and has been associated with an increased risk of stillbirths (Yatich et
al., 2010). Despite the number of malaria prevention initiatives in Ghana, one study found that
less than 40% of pharmacy staff had adequate knowledge about current malaria control
initiatives and only 21% were aware of current malaria treatment guidelines (Buabeng, Matowe,
Smith, Duwiejua, & Enlund, 2010). Even with the introduction of rapid diagnostic tests for
malaria, misdiagnosis and over-diagnosis of malaria remain common, resulting in misallocation
of resources and contributing to medication resistance (Chandler, Whitty, & Ansah, 2010;
Whitty, Chandler, Ansah, Leslie, & Staedke, 2008). This evidence suggests that the information
needs regarding the prevention and management of malaria remain high, even among healthcare
workers.
Non-Communicable Diseases
The prevalence of non-communicable diseases in developing countries has increased
greatly with increasing average lifespans, lifestyle changes, continuing poverty, and urbanization
(de-Graft Aikins et al., 2010). A recent survey found an increasing morbidity for women in
Ghana for diseases more commonly thought of as problems of industrialized nations:
hypertension, diabetes, chronic pain, arthritis, deteriorating visual acuity, and dental problems
(Duda et al., 2011). The WHO describes in the increase in non-communicable disease in
developing countries as a “double burden” for health systems with limited capacity to treat
present problems with infectious disease and a scarcity of healthcare workers with training
and/or experience with chronic disease management (Marshall, 2004). Clinical management of
non-communicable disease often requires long-term data sets and patient histories which are not
currently adequately managed in existing paper records. Increased chronic disease in Ghana has
19
resulted in high rates of disability and premature deaths which have been associated with
inadequate knowledge of health workers of chronic disease management (de-Graft Aikins, 2005;
de-Graft Aikins, Boynton, & Atanga, 2010).
Healthcare Workers in Ghana
Ghana, like many other developing countries, faces a shortage of healthcare workers.
The majority of physicians work in the metropolitan areas of Accra and Kumasi, while rural
areas retention and recruitment to rural areas remains a challenge due to perceived professional
isolation, decreased income, and lack of mentoring and distance learning opportunities (Snow, et
al., 2011).
Nurses, like physicians, are not adequately distributed between rural and urban settings in
Ghana (Donkor & Andrews, 2011). Significant job dissatisfaction and high-turnover rates
among nursing and midwifery staff are common, with considerable “brain drain” to the US and
Great Britain (Talley, 2006). Working conditions and compensation for nurses/midwives are
poor, with job assignments dictated by the government, and virtually no opportunity for
advancement (Donkor & Andrews, 2011). Ghana, like many countries in Sub-Saharan Africa, is
made up of a large number of ethnic groups, sharing their own language, customs, and practices.
Midwives and nurses, who may be serving in an area outside of their own cultural group would
need further information and support about local socio-cultural factors that may affect treatment
seeking behaviors or health risks of patients in the community that they are serving (Apalayine &
Ehikhamenor, 1996).
Data management and quality
Another challenge faced by Ghana’s healthcare system is the management and collection
of data. In many developing countries, cause of death is usually determined through reports
20
from relatives rather than on pathology or autopsy data, as is commonly done in industrialized
countries. These verbal autopsies are often inconsistent in assigning accurate causes to maternal
death making it difficult to determine where and what resources and training should be allocated
(Chandramohan, Rodrigues, Maude, & Hayes, 1998). Certain conditions, such as hypertensive
disorders, tend to be over-diagnosed while death related to malaria and other infectious disease is
underreported (Asamoah, et al., 2011; Ordi et al., 2009). Ghana’s government is in the process
of a rollout of national health insurance (NHIS). Having quality data on use of services and
resources is a key element for appropriate spending, allocation of resources, and ensuring that
NHIS serves in reducing the costs of out-of-pockets expenses and catastrophic health
expenditure for Ghana’s citizens (Debpuur, Welaga, Wak, & Hodgson, 2010; Nguyen, et al.,
2011).
Training of Rural Midwives
For the purpose of this study, we define a midwife as a skilled birth attendant who has
received some type of formalized training in midwifery versus a traditional birth attendant
(TBA) who is primarily trained through apprenticeship. As in the developed world, the pre-
service training of midwives in Ghana vary widely, with technical, baccalaureate and graduate
training available as pathways to entry-to-practice (Fullerton, et al., 2011). This variation means
that midwives may enter practice with three years of previous training as a nurse plus work
experience or with no previous nursing training or clinical work experience (Prosser, et al.,
2006). Furthermore, studies of rural healthcare workers in developing countries have found most
workers to be young and/or inexperienced, with little computer skills and high turnover rates
(Martinez, Villarroel, Seoane, & del Pozo, 2005).
21
Poor road access to rural health facilities may limit opportunities for continuing
education. In Ghana, rural facilities may be several hours away from the nearest population
center due to the lack of paved roads. Additionally, since midwives work independently, leaving
the facility for continuing education means that no or limited services will be provided until she
returns (Martinez, et al., 2005; Prosser, et al., 2006). Evidence suggests that recertification
practices and license maintenance requirements are not consistently applied or monitored in
Ghana. In general, a midwife is licensed to practice for life after completing and passing pre-
service training and certification exams (Fullerton, et al., 2011). Inconsistencies in training and
continuing education practices highlight the need for insuring rural midwives have access to
appropriate information for supplementing their training and clinical knowledge and the need for
a mechanism for continuing training and recertification.
Information Needs and Practices of Healthcare Workers in Developing Countries
Appropriate and timely health information is necessary for providers to give proper care
to their patients, whether this information is lab results, medications, patient history, or
information on the latest standards of care. In developing countries health care providers,
particularly those working in rural areas, often lack access to health information due to a lack of
communication infrastructure as well as lower levels of computer literacy (Pakenham-Walsh,
Priestly, & Smith, 1997).
Providers in developing countries may rely on heavily on colleagues or printed materials
when making health decisions (Kapiriri & Bondy, 2006). This presents challenges as the
information may not be up-to-date or represent current best practices. Furthermore, one study
found that donated textbooks were not appropriate because they did not include culturally or
locally relevant information, such as information about tropical diseases or local health practices
22
or inclusion of treatment modalities that are not locally available (Musoke, 2000). While several
studies found electronic resources useful in developing countries, these studies only looked at
doctors working in urban, tertiary care settings (Aronson, 2004; Burton, Howard, & Beveridge,
2005).
Studies have noted that many midwives feel unprepared to meet the most pressing needs
of the current health crisis in Sub-Saharan Africa, such as treating resistant strains of malaria and
prevention of mother-to-child transmission of HIV (Leshabari, Blystad, de Paoli, & Moland,
2007; Mechael, 2009b; Prosser, et al., 2006). One nurse, with 20 years’ experience in public
health was quoted as saying: "I have only attended one workshop for one week on promoting
exclusive breastfeeding. I'm still using the same knowledge to educate mothers on how to feed
their babies. I feel like I'm not knowledgeable enough to give my clients updates, especially in
this time of AIDS." (Leshabari, et al., 2007, p. 7). This lack of knowledge is exacerbated by the
limited opportunities for continuing education noted in the previous section.
Paper record keeping systems in developing countries may be insufficient for monitoring
of interventions and serve as poor information resources to providers. An analysis of paper
records in Kumasi, Ghana on obstetric complications found deficiencies that made root-cause
analysis of obstetric complications impossible (Danquah et al., 1997). In Ghana, new records are
created based on visit type and patients may use different names based on the type of visit
making record linkage difficult if not impossible (Allotey & Redipath, 2000). Inconsistencies in
record keeping practices present a challenge, particularly in tracking high-risk patients and in
ensuring continuity of care, especially for patients with chronic conditions. While health
information systems (HIS) may assist in record linking, the proper identification and tracking of
patients requires collaboration from local, regional, and governmental health officials.
23
Midwives and Nurses as Knowledge Workers Using HIS
A knowledge worker is defined as “those who are able to critically reflect upon the
explicit knowledge of the organization by adding personal, theoretical, and tacit knowledge”
(Brooks & Scott, 2006, p. 84). Knowledge workers in their role acquire, transmit, and apply
knowledge as well as creating new knowledge (Kelloway & Barling, 2000). Transforming
nurses and midwives into knowledge workers is important for several reasons. First, it promotes
autonomy that may lead to improved job satisfaction (Finn, 2001; Pierce, et al., 1996; Ward &
Kozakowski, 1987). Additionally, nurses and midwives who can effectively use and produce
knowledge can help identify patient needs, affect policy, and play a great role in their healthcare
system (Antrobus, 1997; J Sorrells-Jones & D Weaver, 1999). Nurses and midwives need access
to accurate and complete data regarding their patients in order to function as knowledge workers
(Snyder-Halpern, et al., 2001). Transforming nurses and midwives into effective knowledge
workers may require organizational changes that ensure nurses and midwives have access to
critical information and an organizational culture that allows for diffusion of knowledge to affect
change in individual practice as well as the organization (Brooks & Scott, 2006).
HIS can be useful in promoting knowledge worker role amongst nurses and midwives.
Snyder-Halpern and colleagues (2001) outline the how HIS can aid in knowledge work and the
four roles for nursing and midwifery knowledge workers: data gatherer; information user;
knowledge user; and knowledge builder. In the data gather role, the knowledge worker collects
clinical data (Snyder-Halpern, et al., 2001). HIS can be used to facilitate data collection at the
point-of-care and improve the accuracy of the data collected (Montoya & Carlson, 1996). In the
information user role, the knowledge worker interprets and organizes data for clinical decision
making (Snyder-Halpern, et al., 2001). HIS can support this role by helping to organize relevant
24
data needed for clinical decision making and simplifying access to patient data, providing data in
a timely manner, and fitting into workflow (Bates et al., 2003). The knowledge user role occurs
when domain knowledge is applied to patient information (Snyder-Halpern, et al., 2001). HIS
can facilitate this role with context specific information resources and access to and evidenced-
based clinical knowledge bases (Bates, et al., 2003; Snyder-Halpern, et al., 2001). The
knowledge builder role occurs when domain knowledge is used to interpret and understand
aggregated patient data (Snyder-Halpern, et al., 2001). HIS can support this role by giving
nurses and midwives access to aggregate patient data that allow the nurse or midwife to evaluate
their work and recognize and interpret practice patterns (Ozbolt & Graves, 1993; J. Sorrells-
Jones & D Weaver, 1999).
As frontline workers, the knowledge gathered by midwives and nurses in rural facilities is
critical for identify patterns among patients and identifying need areas for targeted interventions.
HIS implementations that support knowledge work in developing countries have been limited
(W. A. Kaplan, 2006; Mechael & Sloninsky, 2008; United Nations Foundation, 2010).
Health Information Systems in Developing Countries
Several reviews have found that most HIS implementations in developing countries lack
published reports on patient outcomes and/or quality improvements (Blaya, Fraser, & Holt,
2010). This is partially due to complexity in establishing baseline data using paper-records as
well as the rapidly evolving healthcare systems in the developing world due to various,
concurrently occurring local government initiatives in conjunction with the World Health
Organization, the United Nations Development Programme (UNDP), and other non-
governmental organizations (NGOs) (Braa, et al., 2007). Most HIS projects have faced
challenges in establishing long-term sustainability (Gerber, et al., 2010). Projects often require
25
data collection standards to meet the needs of national or international donors that often fail to
address local needs (Gordon & Hinson, 2007). These projects are further challenged by short-
term funding mechanisms and failure to provide adequate training and support once foreign
experts leave (Heeks, 2002).
Sharing of resources and expertise, such as the use of open-source software and
nationally and internationally shared technical expertise have helped to alleviate the costs
associated with HIS implementation while providing a model for sustainable success (Blaya, et
al., 2010; Were et al., 2010). In addition, local human resource capacity building is
recommended for long-term success of any implementation (Heeks, 2002). A key factor to
success of HIS implementations in developing countries is user acceptance (Fraser & Blaya,
2010; United Nations Foundation, 2010; Williamson, Stoops, & Heywood, 2001). Methods for
increasing user acceptance include providing adequate support and training for learning the new
system, encouraging local ownership and data use, cultivating local leadership and project
champions, and sensitivity to local culture (Fraser & Blaya, 2010; Rotich et al., 2003; Waters et
al., 2010). Additional studies have shown that alignment of the HIS intervention with user needs
and provider technical self-efficacy are also significant factors in technology acceptance (Wu,
Wang, & Lin, 2005).
mHealth in Developing Countries
Mobile health technologies are being increasingly used to meet the information needs of
health care workers in sub-Saharan Africa (Fraser & Blaya, 2010). Recent advances in the
mobile telephony technology, as well as significant infrastructure improvements in sub-Saharan
Africa, the low start-up development costs, end-user familiarity, and increased research funding
from both private foundations and industry sources make mobile phones a strong candidate as
26
the tool for health information delivery in developing countries (W. A. Kaplan, 2006; Mechael,
2009a; Mechael & Sloninsky, 2008). The mobile phone market in Africa is the fastest growing
in the world, having increased 58% from 1999 to 2004 (LaFraniere, 2005). Africa was the first
continent where mobile phone use exceeded landline use and the current mobile phone
penetration rate in Africa is 30% and growing (International Telecommunication Union, 2009).
There is growing interest in using the existing and growing mobile phone infrastructure in Africa
as a means of delivering health information solutions, however, systematic reviews on the topic
have found that most published studies have been brief pilot and feasibility studies with limited
evaluation and little mention of project scalability and long-term feasibility (W. A. Kaplan, 2006;
Mechael & Sloninsky, 2008; Tamrat & Kachnowski, 2011). However, mobile technology has
rapidly become faster, smarter, and cheaper; rapidly changing the technological and financial
barriers of studies that are even just a few years old (W. A. Kaplan, 2006).
To date, most mHealth projects in Sub-Saharan Africa have targeted community health
workers (CHWs), who play a vital role in accessing hard-to-reach patients (W. A. Kaplan, 2006;
Tamrat & Kachnowski, 2011). Most CHWs are lay-people with limited education and/or training
to meet the demands of patients burdened with chronic disease or other serious afflictions (Kober
& Van Damme, 2004). Projects targeting other types of providers have been extremely limited
(James & Versteeg, 2007; W. A. Kaplan, 2006; Mechael & Sloninsky, 2008). Applications
using mHealth for healthcare workers have generally been in the following categories:
emergency services, health promotion, data collection and management, monitoring, information
resources for healthcare workers, disease surveillance, and point-of-care decision support
(Mechael, Douglas, Lesh, & Kwan, 2009; Tamrat & Kachnowski, 2011; United Nations
Foundation, 2010).
27
Emergency services
Applications targeted at emergency service support include: Rural Extended Services and
Care for Ultimate Emergency Relief (RESCUER) (Tamrat & Kachnowski, 2011; United
Nations Foundation, 2010). RESCUER combined the use of two-way radios with bicycles and
ambulances in order to respond to obstetric emergencies and resulted in a 50% reduction in
maternal mortality (Musoke, 2002). Similar projects in Bangladesh, the Gambia, and India have
been reported but no published data on the effect of the interventions are available (Cole-Ceesay
et al., 2010; Tamrat & Kachnowski, 2011).
Data collection and disease surveillance
A wide range of tools are available for data collection purposes and disease surveillance.
OpenXData and EpiSurveyor are both used for remote data collection. OpenXData is an open-
source software for data collection that works on inexpensive java based phones and has be used
in several countries in Africa and South East Asia (OpenXData, 2011). EpiSurveyor is similar to
OpenXData though it is available on a wider range of phones and has a cost associated with its
use, though a free version with limited functionality is available (DataDyne, 2011). These tools,
and others like it, allow for faster and higher quality survey data collection (Lang, 2011). A
number of survey tools have also been created for disease surveillance, the most well-known
being FrontlineSMS which was used to monitor water quality in Haiti following the most recent
cholera outbreak (Greenemeier, 2011).
Information resources, diagnostic, and decision support
Several programs have been designed as an information resource for healthcare workers
including: Enhancing nurses access for care quality and knowledge through technology
(ENACQKT); HealthLine; Mobile HIV/AIDS Support; Primary Healthcare Nursing Promotion
28
Program; and, The Uganda Health Information Network (UHIN); diagnostic and decision
support tools such as phone based dosage calculators, medical sensors, and remote diagnostic
support (United Nations Foundation, 2010). The ENACQKT project provided clinical
information resources to nurses and student nurses to nurses in the Caribbean resulting in an 27%
average reduction in time to access clinical information (International Development Research
Center, 2009). HealthLine uses speech recognition to give community health workers with low
literacy levels access to information resources, it is currently in pilot testing (Sherwani et al.,
2007). UHIN allows for sending and receiving data in remote clinics, was developed by
developed by AED-Satellife, who report that the project resulted in quicker and more cost-
effective data collection with improved data quality (Kinkade & Verclas, 2008). AMREF’s
Only summary information was available for Mobile HIV/AIDS support and the Primary
Healthcare nursing promotion program (United Nations Foundation, 2010).
A more advanced example of decision and diagnostic support is e-IMCI. A treatment
algorithm developed by UNICEF known as Integrated Management of Childhood Illness (IMCI)
was integrated in to a PDA (e-IMCI) for use by clinicians in Tanzania. The use of the PDA
based tool found increased adherence to investigation guidelines and a reduction of time spent
documenting care (DeRenzi et al., 2008). Another application, the Aceh Besar midwives
mobile-phone project, supplied midwives with mobile phones to transmit health data and
provides diagnostic support through communication with health coordinators and other
midwives. The study results showed increased confidence in the midwives self-reported ability
to solve difficult clinical problems, though results on medical knowledge scores were mixed
(Chib, 2010).
29
Evaluation of the impact of these applications is still limited. Much of the project data
reported here come from online reports rather than peer-reviewed journals. Most of the reports
were short-term evaluations of pilot testing. Many of these pilots faced common challenges such
as: equipment not being available (Sherwani, et al., 2007); lack of healthcare infrastructure to
support the goals of the project (Cole-Ceesay, et al., 2010; Musoke, 2002); staff morale and
project buy-in (Cole-Ceesay, et al., 2010); and difficulty in distinguishing between borderline
cases in clinical decision making and limiting the development of clinical reasoning (DeRenzi,
et al., 2008).
Human-Computer Interaction for Developing Countries (HCI4D)
In the developing world, it is common for most web users to have only experienced
accessing the internet through a mobile device. Mobile web sites often assume that users have
access to or previous experience with a personal computer and such instructions had a negative
impact on users ability to appropriately navigate a site (Gitau, Mardsen, & Donner, 2010).
Researchers have noted that current participatory design methods rely on users having a base
understanding and knowledge of technology that is often inappropriate in developing settings
(Smith & Dunckley, 2007). Other considerations for HCI4D include inadequate power
infrastructure, low literacy levels or inability to translate technology specific concepts to the
local language, and cultural variations in mental models (Ho, Smyth, Kam, & Dearden, 2009).
Participatory design methods, which often seek design proposal from users, may not be feasible
amongst users whose understanding of technology is limited (Gitau, et al., 2010; Heukleman,
2006; Maunder, Marsden, Gruijters, & Blake, 2007)
Various alterations to user centered design methods for use in developing countries have
been proposed though there is limited data available on the effectiveness of such methods
30
(Maunder, et al., 2007) . Ramachandran et al. (2007) suggests establishing a “technology
baseline”, by exhibiting examples of software with similar functionality to the one to be
implemented. This can also be done through computer literacy and training prior to the design
sessions (Kimaro & Titlestad, 2008). However, these methods may be limited in the case of time
or human resource constraints. The use of low-fidelity prototyping in this context may be
challenging if such prototypes contain concepts that are unfamiliar to the user (Lalji & Good,
2008; Maunder, et al., 2007).
Design Science in a Developing Country Context
As previously noted, many HIS implementations in developing countries have resulted in
failures (Braa, 2004; Heeks, 2002). Heeks (Heeks, 2006) categorizes failures as either total,
when the system is never implemented or is implemented, then abandoned; or partial, when key
goals are not attained or unwanted outcomes occur. Success is defined as most stakeholder
groups attaining key goals without significant unwanted outcomes. Success of an HIS is a
dynamic concept and can be defined in terms of effectiveness, improved efficiency,
organizational acceptance, end-user satisfaction, and patient satisfaction (Berg, 2001).
Design science is the development, implementation, evaluation, and adaptation of
artificial artifacts for problem solving (Hevner, 2007; Simon, 1996). When discussing the
objectives of design science, Patel and Kaufman (1998) have stated:
One of the goals…is to discover what works and then determine why some things
work and others don’t. A working system is an outcome not merely of technology
but of the social and cognitive processes of integrating such a system into the
daily workflow (p. 490).
31
Best practices exist for applying what is known to work in HIS implementations. However, most
pre-design and pre-implementation assessment tools have been developed for use in
industrialized countries. A search of four databases, PubMed, Google Scholar, Google, and
ProQuest, using the search terms “Informatics”, “Information Systems”, “Information
technology”, “*readiness”, “assessment”, “implementation”, “developing countr*”, “low
resource”, and “Africa”, was only able to identify one tool for implementation e-readiness
assessment at the organizational level, the NGO ICT and e-Readiness Self-Assessment Tool
(NGO Connect Africa Network, 2011). This dearth of tools and methods has been noted by
other authors (Dorflinger & Gross, 2010; Toyama & Muneeb, 2009). The lack of existing tools
for assessing needs in developing countries stresses the importance of careful design and
planning in order to close the design-actuality gap.
Design science methods can be useful in closing these gaps. Prescriptive theories on
design will help us determine how to create a system (Gregor & Jones, 2007). Design research
should result in four general outputs: constructs, or concepts and language of the problem; a
model, the proposed problem solutions or representations; methods, which are guidelines,
algorithms, or practices for performing tasks; and, instantiation, or the actual developed artifact
(Hevner & Chatterjee, 2010; March & Smith, 1995).
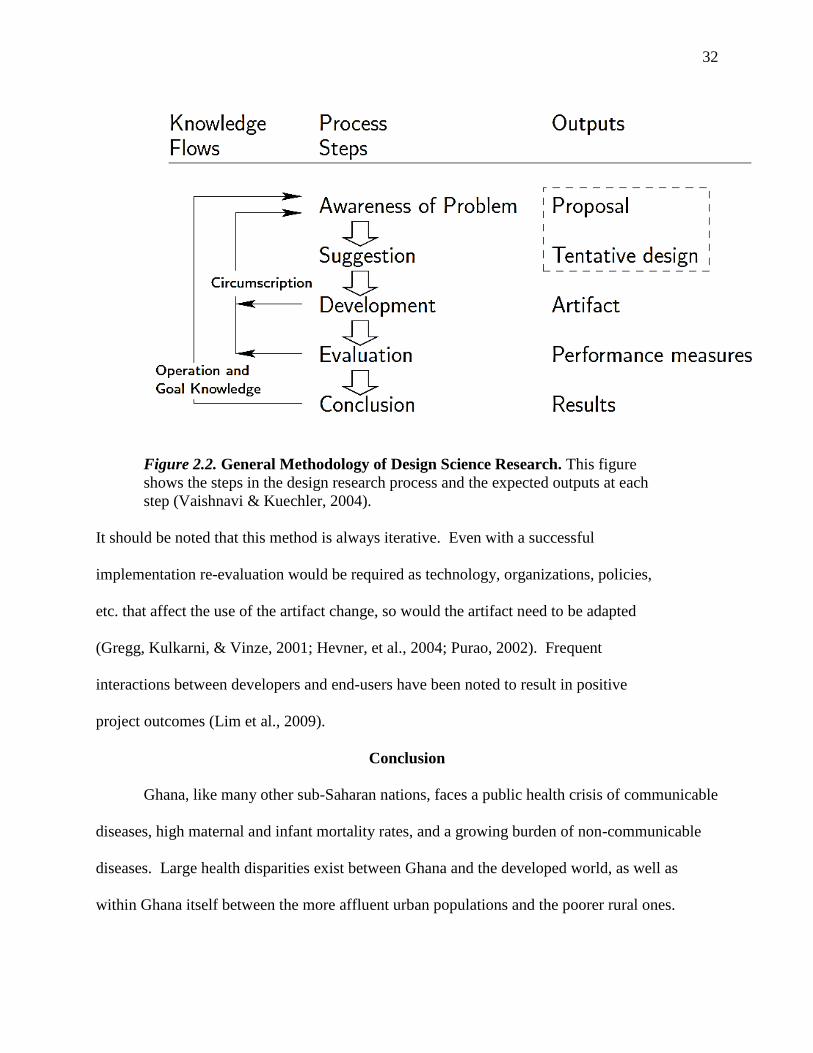
32
Figure 2.2. General Methodology of Design Science Research. This figure
shows the steps in the design research process and the expected outputs at each
step (Vaishnavi & Kuechler, 2004).
It should be noted that this method is always iterative. Even with a successful
implementation re-evaluation would be required as technology, organizations, policies,
etc. that affect the use of the artifact change, so would the artifact need to be adapted
(Gregg, Kulkarni, & Vinze, 2001; Hevner, et al., 2004; Purao, 2002). Frequent
interactions between developers and end-users have been noted to result in positive
project outcomes (Lim et al., 2009).
Conclusion
Ghana, like many other sub-Saharan nations, faces a public health crisis of communicable
diseases, high maternal and infant mortality rates, and a growing burden of non-communicable
diseases. Large health disparities exist between Ghana and the developed world, as well as
within Ghana itself between the more affluent urban populations and the poorer rural ones.
33
These challenges are exacerbated by a lack of trained healthcare workers to meet the needs of the
population.
In rural areas, primary care is provided primarily by midwives. These midwives are
responsible for a wide scope of practice, from neonates up to the elderly. They have little
opportunity for continuing education and rely heavily on pre-service training as their knowledge-
base. This is concerning due to the inconsistency in pre-service training as well as the inability
of midwives to keep abreast of best evidence and current clinical practice guidelines (Prosser, et
al., 2006). Pre-service training programs may not prepare novice midwives for the challenges of
rural health care as many students have reported having limited access to current textbooks or
scholarly journals (Khalil, 2006). These gaps in training and continuing education should be
taken into consideration in the design of an information support tool.
An HIS implementation must be designed for the midwives’ current actuality in order to
be successful. It has been noted that up to 25% of HIS implementations in developing countries
have failed, and those that persist often proves to be unsustainable or unscalable (Heeks, 2002,
2008; Walsham & Sahay, 2006; Were, et al., 2010). Friedman (1995) noted:
Installing an information system in a functioning health care setting requires in-
depth understanding of the organization and ecology of the workplace: how the
system affects the structure of work and how, in return, some unchangeable
features of the work create constraints on a system (p. 66).
Design science provides a structure for understanding the ecology of the application
environment. By using the Information Systems Research Framework to guide our system
design and testing we can improve our understanding of the current system actuality in order to
close the design-actuality gap.
34
CHAPTER III. METHODOLOGY
This study was composed of two research cycles as guided by the ISR framework (Table
3.1). The first, the relevance cycle, was intended to increase our understanding of the application
domain to determine the functional requirements of the artifact. This was done through
characterizing the information seeking behavior and information needs of nurses and midwives
currently working at Millennium Village Project (MVP) facilities in Ghana. Second, we did an
analysis of current workflow, documentation procedures, and documentation practices in regard
to quality and completeness needed for proper follow-up and reporting. Additionally, we looked
at barriers to the implementation of a mobile-phone based application. In the second cycle, the
design cycle, we evaluated the usability of our artifact using field testing and post-testing
interviews and surveys.
Project Context
In September of 2000, world leaders gathered and adopted the United Nations (UN)
Millennium Declaration which was a commitment to a global partnership for ending extreme
poverty (defined as people earning less than $1.25 USD/day) by 2015. The goals of this
partnership, known collectively as the Millennium Development goals (MDGs) are the
following: eradicate extreme hunger and poverty; achieve universal primary education; promote
gender equality and empower women; reduce child mortality; improve maternal health; combat
HIV/AIDs, Malaria and other diseases; ensure environmental sustainability; and develop a global
partnership for development (United Nations, 2000).
In 2002, the UN Millennium project was commissioned by the UN Secretary General to
develop a concrete plan of action for meeting the MDGs. MVP is based on those findings and
instituted in collaboration with the Earth Institute at Columbia University, The Millennium
35
Promise Organization, and the United Nations Development Program. MVP sites are located
throughout sub-Saharan Africa and work in collaboration with local governments to achieve a
sustainable end to extreme poverty by targeting the MDGs (Kanter, et al., 2009). The MVP
Bonsaaso Ghana Cluster consists of six villages encompassing a population of 30,000. The
villagers are primarily employed in small-scale, open-pit mining operations or through family
and cooperative farms.
To meet the healthcare needs of this community, MVP has built or enhanced seven rural
clinics, increased collaboration with the local district hospital, and provided two emergency
transport vehicles. Three of the MDGs specifically target healthcare issues: reduce child
mortality (MDG4); improve maternal health (MDG5); and combat HIV/AIDs, Malaria, and other
diseases (MDG6). Strategies for MDG4 have included improving immunization coverage for
children under five and increasing screening rates for malnutrition and childhood illnesses. For
MDG5, MVP has responded by constructing new health facilities or improving existing clinics,
ensuring clinics are adequately equipped with medical supplies, and training community health
workers to recognize the need for emergency obstetrics, and increasing access to family planning
(Kanter, et al., 2009). MDG6 has been addressed through teaching prevention methods,
supplying of prophylactics (bed nets for malaria; condoms for HIV) and supplying medicine and
strategies for the treatment of HIV, Malaria and TB.
The villages are primarily connected by a network of unpaved roads, shown in Figure
3.1, and transportation to each village can take over an hour, though most of the villagers do not
have access to transportation. Villages are serviced by seven community health facilities
spread throughout the region as well as a district hospital. However, many villagers may have to
walk a considerable distance to reach the facility.
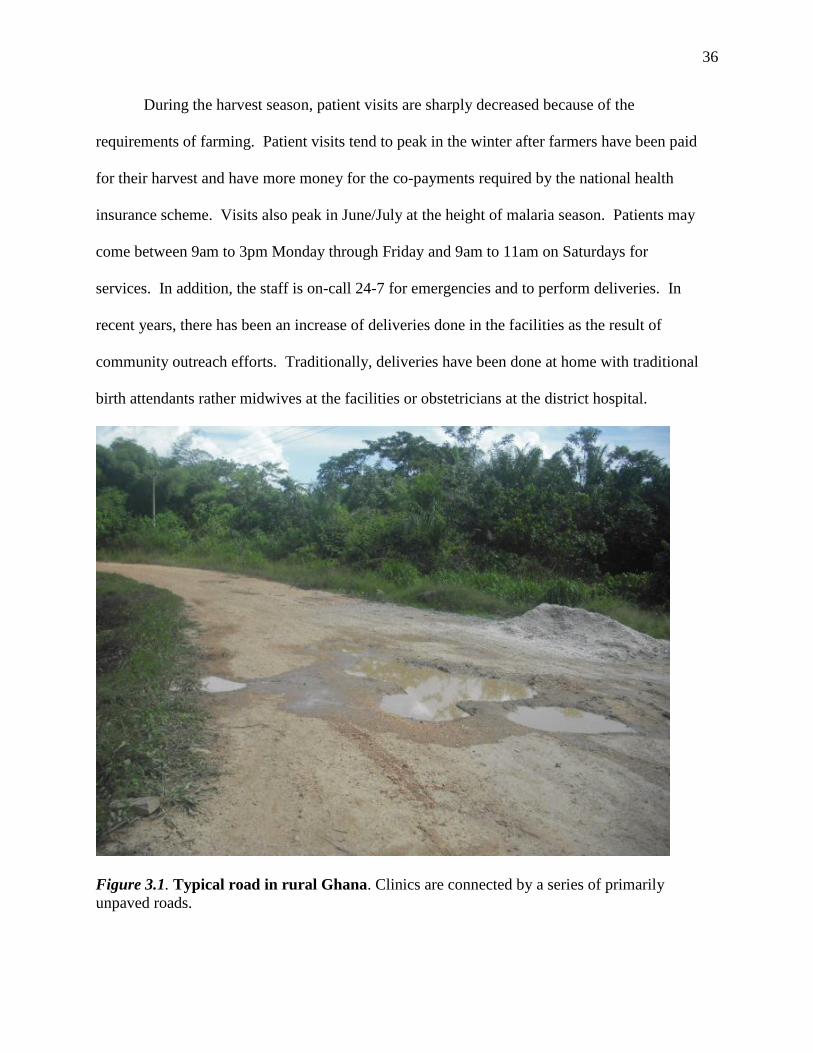
36
During the harvest season, patient visits are sharply decreased because of the
requirements of farming. Patient visits tend to peak in the winter after farmers have been paid
for their harvest and have more money for the co-payments required by the national health
insurance scheme. Visits also peak in June/July at the height of malaria season. Patients may
come between 9am to 3pm Monday through Friday and 9am to 11am on Saturdays for
services. In addition, the staff is on-call 24-7 for emergencies and to perform deliveries. In
recent years, there has been an increase of deliveries done in the facilities as the result of
community outreach efforts. Traditionally, deliveries have been done at home with traditional
birth attendants rather midwives at the facilities or obstetricians at the district hospital.
Figure 3.1. Typical road in rural Ghana. Clinics are connected by a series of primarily
unpaved roads.
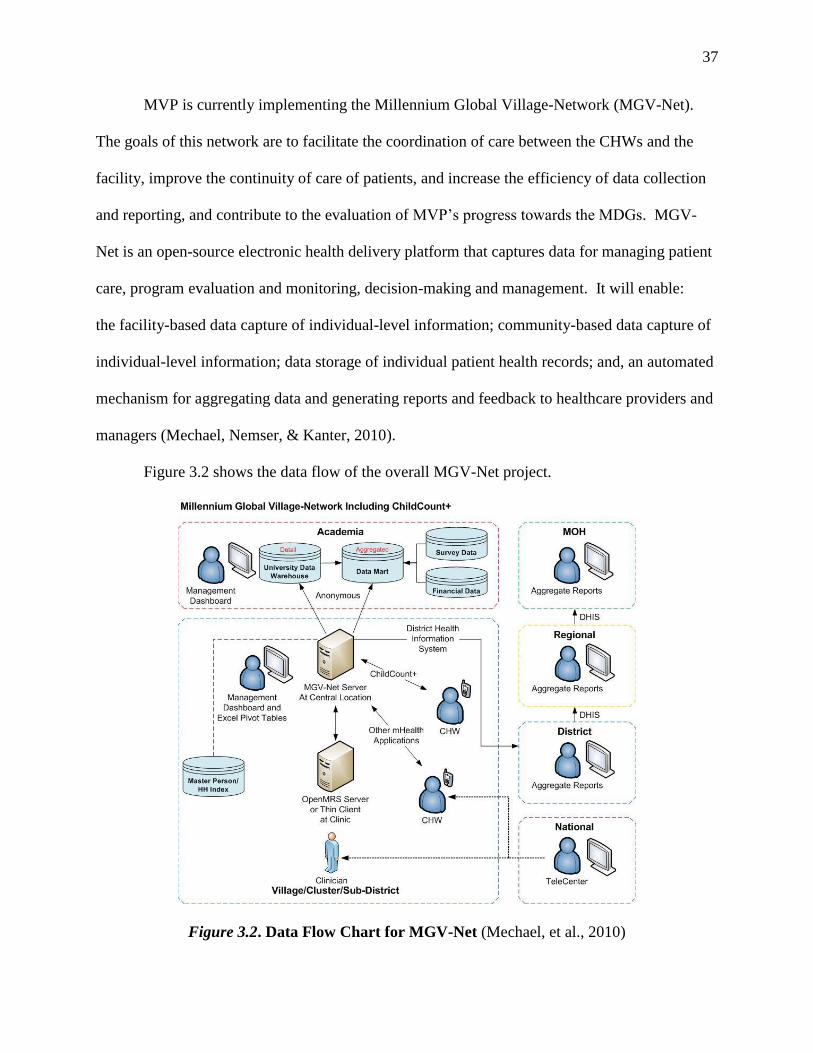
37
MVP is currently implementing the Millennium Global Village-Network (MGV-Net).
The goals of this network are to facilitate the coordination of care between the CHWs and the
facility, improve the continuity of care of patients, and increase the efficiency of data collection
and reporting, and contribute to the evaluation of MVP’s progress towards the MDGs. MGV-
Net is an open-source electronic health delivery platform that captures data for managing patient
care, program evaluation and monitoring, decision-making and management. It will enable:
the facility-based data capture of individual-level information; community-based data capture of
individual-level information; data storage of individual patient health records; and, an automated
mechanism for aggregating data and generating reports and feedback to healthcare providers and
managers (Mechael, Nemser, & Kanter, 2010).
Figure 3.2 shows the data flow of the overall MGV-Net project.
Figure 3.2. Data Flow Chart for MGV-Net (Mechael, et al., 2010)
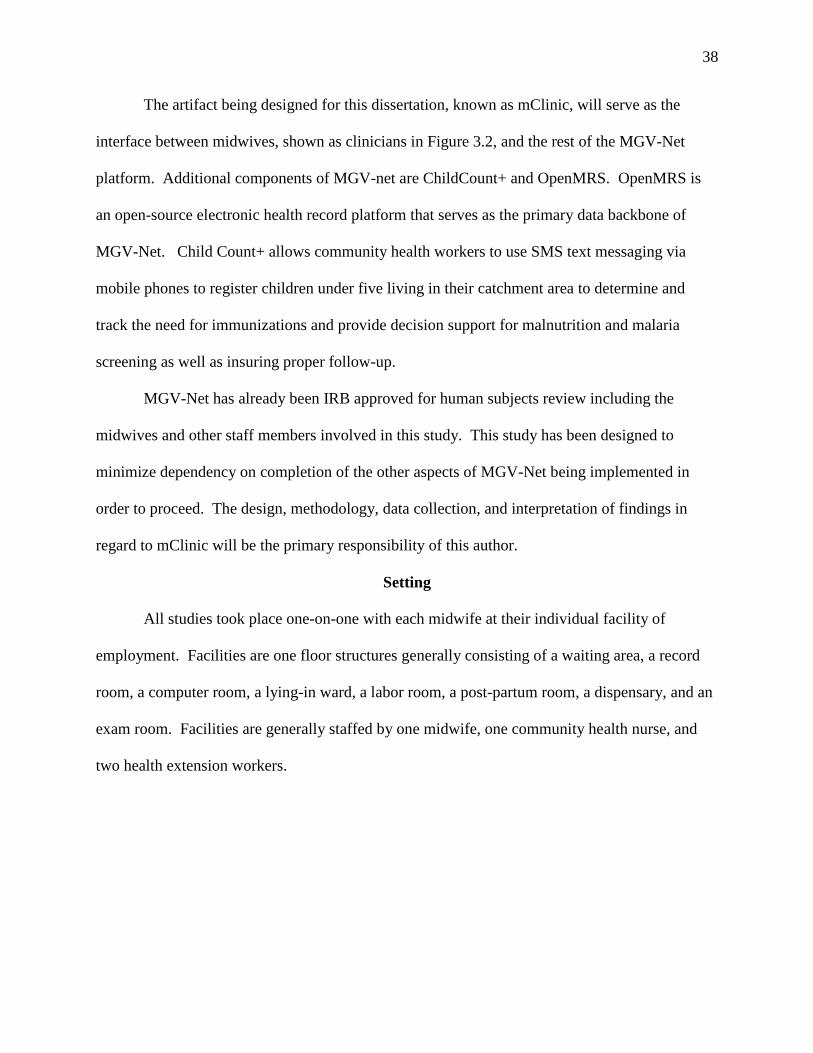
38
The artifact being designed for this dissertation, known as mClinic, will serve as the
interface between midwives, shown as clinicians in Figure 3.2, and the rest of the MGV-Net
platform. Additional components of MGV-net are ChildCount+ and OpenMRS. OpenMRS is
an open-source electronic health record platform that serves as the primary data backbone of
MGV-Net. Child Count+ allows community health workers to use SMS text messaging via
mobile phones to register children under five living in their catchment area to determine and
track the need for immunizations and provide decision support for malnutrition and malaria
screening as well as insuring proper follow-up.
MGV-Net has already been IRB approved for human subjects review including the
midwives and other staff members involved in this study. This study has been designed to
minimize dependency on completion of the other aspects of MGV-Net being implemented in
order to proceed. The design, methodology, data collection, and interpretation of findings in
regard to mClinic will be the primary responsibility of this author.
Setting
All studies took place one-on-one with each midwife at their individual facility of
employment. Facilities are one floor structures generally consisting of a waiting area, a record
room, a computer room, a lying-in ward, a labor room, a post-partum room, a dispensary, and an
exam room. Facilities are generally staffed by one midwife, one community health nurse, and
two health extension workers.
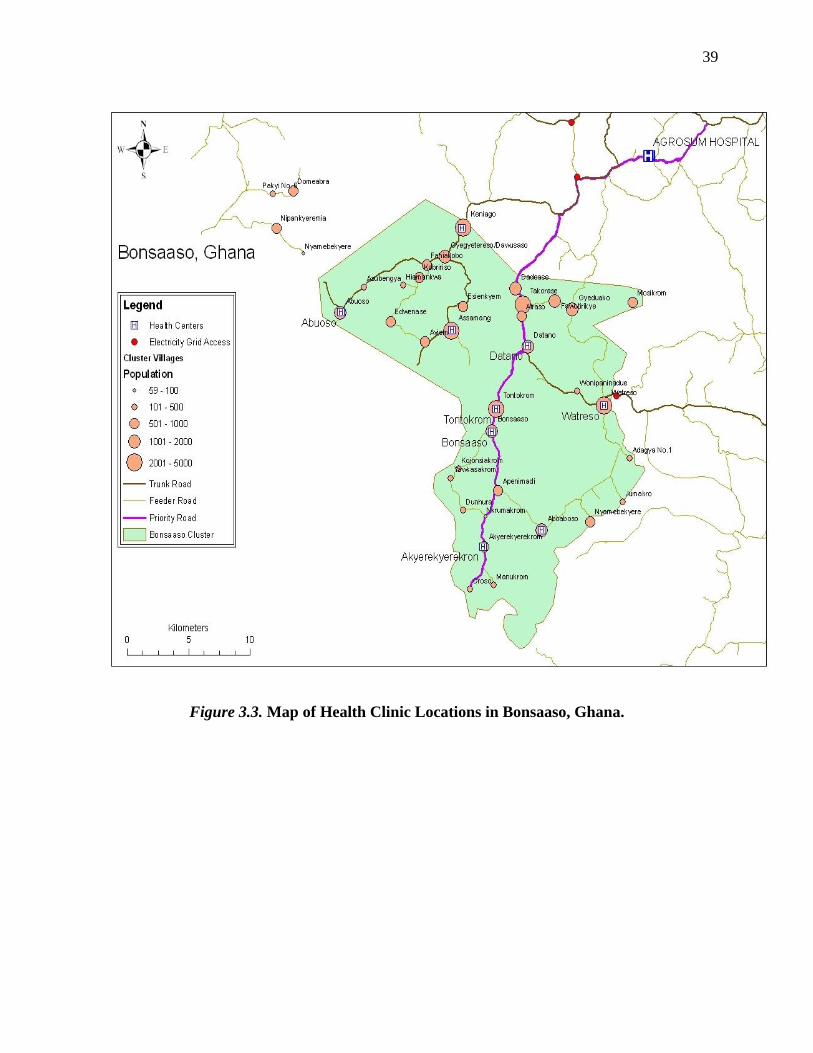
39
Figure 3.3. Map of Health Clinic Locations in Bonsaaso, Ghana.
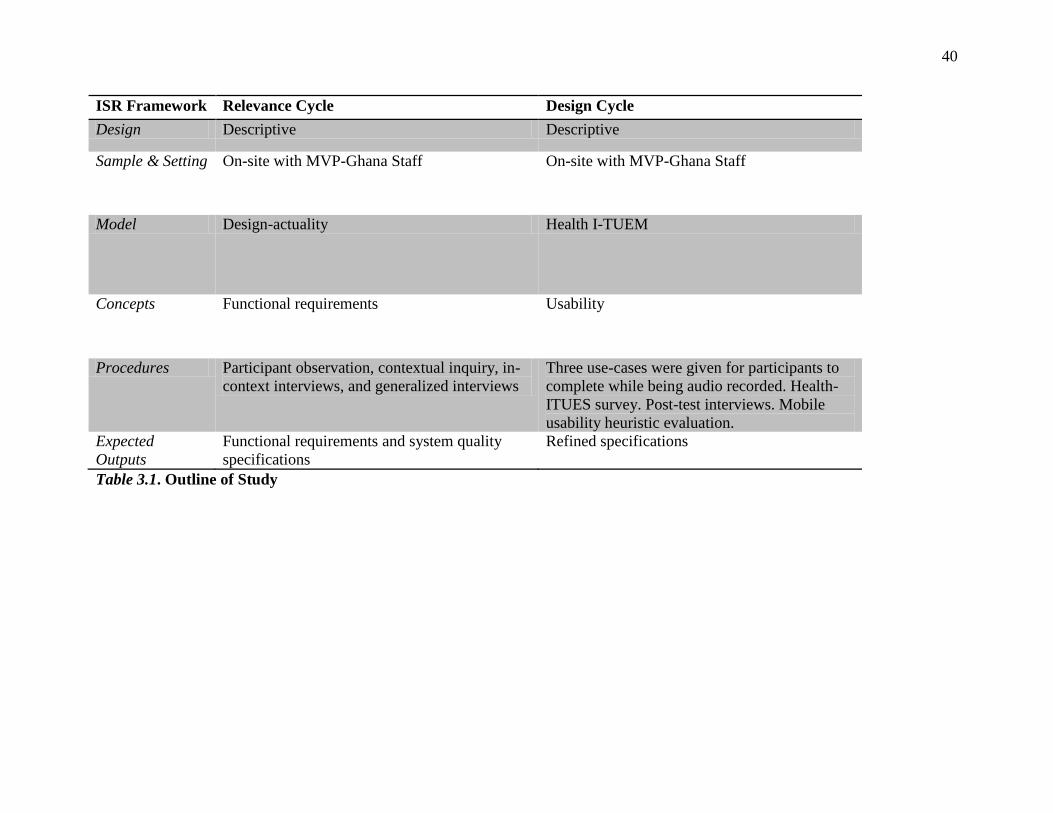
40
ISR Framework Relevance Cycle Design Cycle
Design Descriptive Descriptive
Sample & Setting On-site with MVP-Ghana Staff On-site with MVP-Ghana Staff
Model Design-actuality Health I-TUEM
Concepts Functional requirements Usability
Procedures Participant observation, contextual inquiry, in-
context interviews, and generalized interviews
Three use-cases were given for participants to
complete while being audio recorded. Health-
ITUES survey. Post-test interviews. Mobile
usability heuristic evaluation.
Expected
Outputs
Functional requirements and system quality
specifications
Refined specifications
Table 3.1. Outline of Study
41
Cycle I. The Relevance Cycle
In this cycle, we seek to understand the people, organizations, and technology that make
up the application domain. The purpose is to identify the problems and opportunities that can be
addressed with HIS. The goal of this cycle was to create a functional and non-functional
requirements specification and to develop use cases for building our prototype. The research
questions for this cycle as guided by the ISR framework are as follows:
People
o What is the current workflow of MVP midwives?
o What are the roles and responsibilities of midwives at MVP facilities?
o What is the current experience of the midwives with technology and their
comfort level in learning new technology?
o What are the information needs and information seeking behaviors of
midwives working in MVP facilities in Ghana?
Organizations
o What are the issues in collecting data from the health facilities?
o What is the support capacity for an HIS implementation at MVP Ghana?
Technology
o What is the current technology infrastructure at MVP Ghana?
Problems & Opportunities
o What is the required functionality needed for the application based on the
need and constraints of the application environment?
42
Sample
Six out of seven midwives that had been working at MVP-Ghana were interviewed in
their facility in September 2010. Other staff members were interviewed at the MVP-Ghana
administrative site included: the data manager, a data analyst, the information systems (IS)
manager, and the health team manager.
Design
This was a descriptive study using participant observation and user-centered design
techniques. This part of the study was done in two phases; first, we did a requirements analysis
followed by development of functional requirements based on the results of the first phase.
Requirements Analysis
Procedures
This study used a combination of participant observation, contextual inquiry, in-context
interviews, and generalized interviews to establish a rich data set with iterative, descriptive
coding for analysis. Contextual inquiry is a user-centered method for design that involves
participation observation during which the participant describes the tasks they are performing or
the researcher asks for further clarification (Coble, Maffitt, Orland, & Kahn, 1995). Each
midwife was observed for one morning of clinic hours (approximately 9am to 2pm).
Community health nurses were observed for the duration of specialty clinic hours (either
antenatal care or child well care) for the same time period. Field notes and memoing were used
to record participant observation. Contextual inquiry conducted with midwives after
observations for 30-60 minutes (Coble, et al., 1995). Part of the contextual inquiry process was
spent review the paper tools that the midwives used to document care and for reporting to GHS
and MVP. Additional open-ended interviews were conducted using the design-actuality gaps
43
model to guide questions to refine our understanding of midwives and other staff members’
roles, understand midwives perceptions of organization goals, and discover existing barriers to
an mHealth implementation.
Interviews of other staff were also conducted at the MVP-Ghana administrative site using
Non-Governmental Organization (NGO) ICT eReadiness Self-Assessment Readiness Tool as a
guide. This tool was developed for NGOs to assess their eReadiness and is specifically targeted
toward the assessment of African organizations that may be limited in terms of infrastructure,
resources and technical skills (Van Belle, 2009). The tool goes through a series of questions on
technical infrastructure resources to assess current technology use and readiness for the
introduction of additional technology (NGO Connect Africa Network, 2011).
The paper tools collected during interviews were reviewed by the research team and a
US-based midwife to assess for completeness of needed elements. Brainstorming with MVP
leadership, a US-based midwife with expertise on global health practices and midwifery training,
software developers and an HCI expert were used to refine the functional requirements and use
cases.
Data Analysis
Analysis of current documentation tools was done by comparing data captured by existing tools
to national and international standards of care. Midwives’ statements were captured using memoing
and then sorted into the following categories of interest derived from the ISR Framework:
midwife characteristics, roles, and capabilities. Additional data analysis was done using
descriptive methods. Open coding was used to develop initial data categories from both field notes,
analysis of current paper tools, and contextual inquiry. Codes were then categorized into goals, functional
requirements, constraints, and system qualities and used to develop use cases.
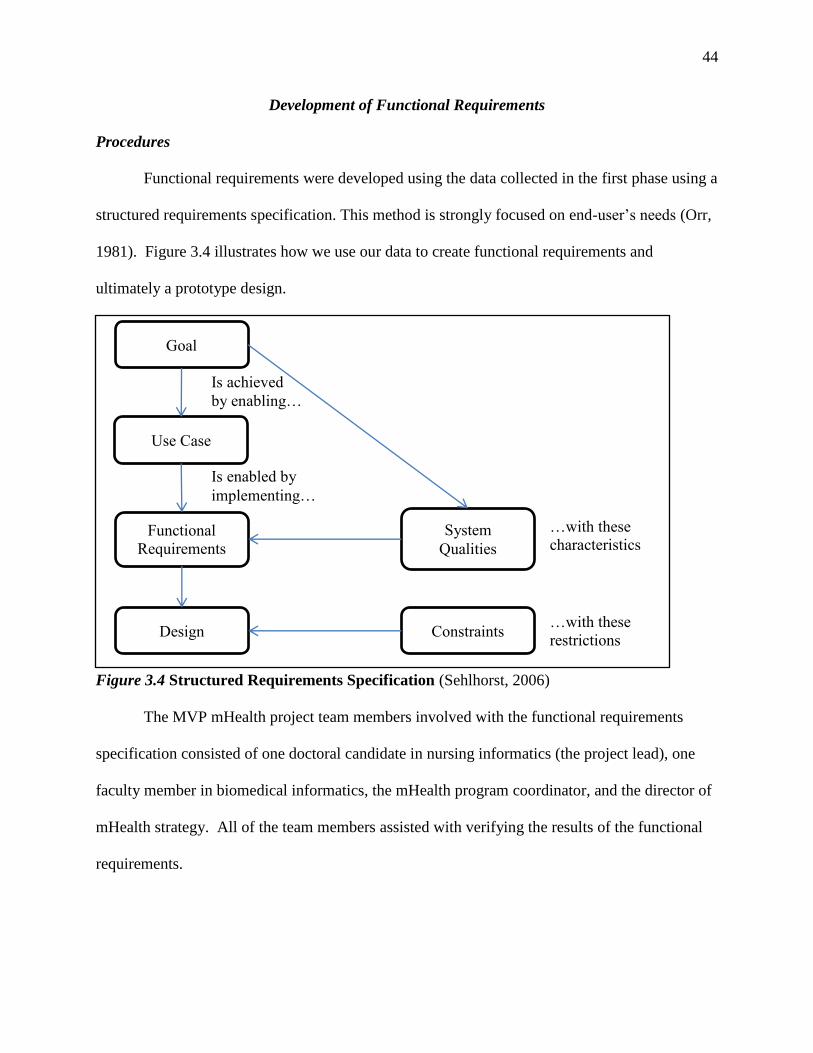
44
Development of Functional Requirements
Procedures
Functional requirements were developed using the data collected in the first phase using a
structured requirements specification. This method is strongly focused on end-user’s needs (Orr,
1981). Figure 3.4 illustrates how we use our data to create functional requirements and
ultimately a prototype design.
Figure 3.4 Structured Requirements Specification (Sehlhorst, 2006)
The MVP mHealth project team members involved with the functional requirements
specification consisted of one doctoral candidate in nursing informatics (the project lead), one
faculty member in biomedical informatics, the mHealth program coordinator, and the director of
mHealth strategy. All of the team members assisted with verifying the results of the functional
requirements.
Goal
Use Case
Functional
Requirements
Design
Is achieved
by enabling…
Is enabled by
implementing…
System
Qualities
…with these
characteristics
Constraints …with these
restrictions
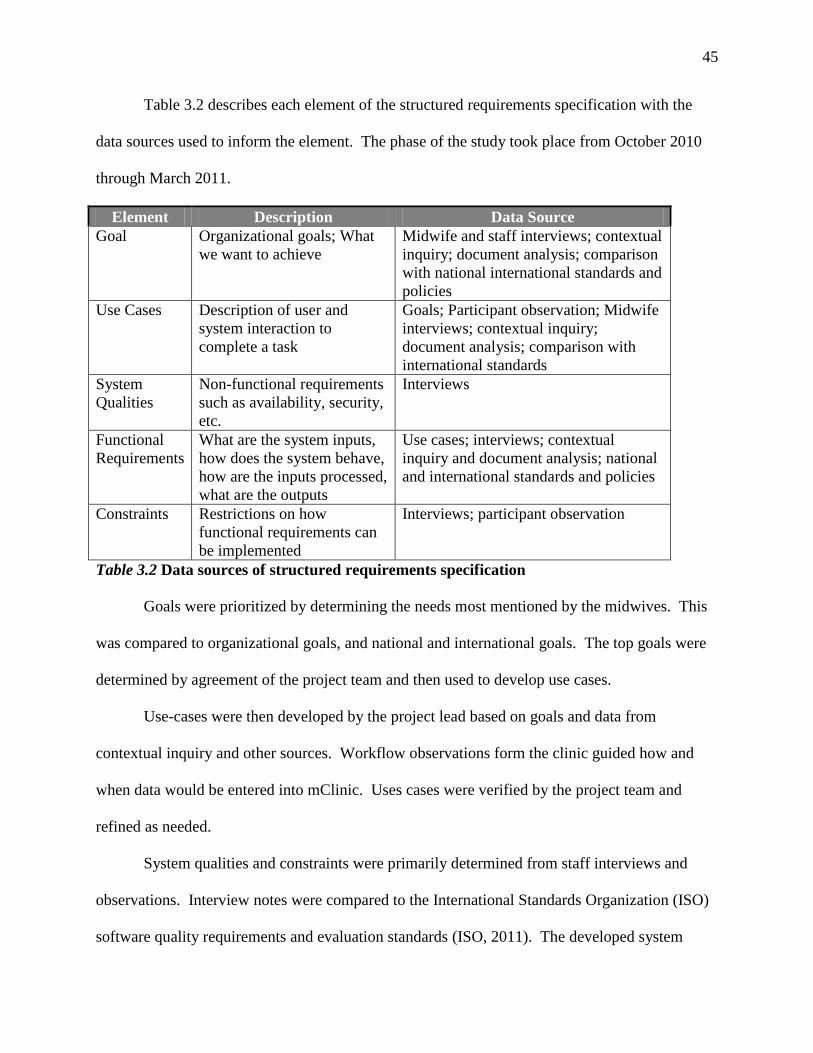
45
Table 3.2 describes each element of the structured requirements specification with the
data sources used to inform the element. The phase of the study took place from October 2010
through March 2011.
Element Description Data Source
Goal Organizational goals; What
we want to achieve
Midwife and staff interviews; contextual
inquiry; document analysis; comparison
with national international standards and
policies
Use Cases Description of user and
system interaction to
complete a task
Goals; Participant observation; Midwife
interviews; contextual inquiry;
document analysis; comparison with
international standards
System
Qualities
Non-functional requirements
such as availability, security,
etc.
Interviews
Functional
Requirements
What are the system inputs,
how does the system behave,
how are the inputs processed,
what are the outputs
Use cases; interviews; contextual
inquiry and document analysis; national
and international standards and policies
Constraints Restrictions on how
functional requirements can
be implemented
Interviews; participant observation
Table 3.2 Data sources of structured requirements specification
Goals were prioritized by determining the needs most mentioned by the midwives. This
was compared to organizational goals, and national and international goals. The top goals were
determined by agreement of the project team and then used to develop use cases.
Use-cases were then developed by the project lead based on goals and data from
contextual inquiry and other sources. Workflow observations form the clinic guided how and
when data would be entered into mClinic. Uses cases were verified by the project team and
refined as needed.
System qualities and constraints were primarily determined from staff interviews and
observations. Interview notes were compared to the International Standards Organization (ISO)
software quality requirements and evaluation standards (ISO, 2011). The developed system
46
qualities and constraints were then reviewed and refined by the project team. Use cases and
system qualities were used to inform the functional specification while the constraints placed
restriction on the software selected for the project.
Cycle II. The Design Cycle
The purpose of this cycle was to have targeted end-users identify issues related to the
usability of the artifact and to verify the applicability of proposed functional specifications and
use cases. The goal is to evaluate the proposed artifact, to obtain data to improve the design, and
to increase the likelihood of technology acceptance. The research questions for this cycle are the
following:
What usability issues exist with the artifact?
What are the deficiencies in functionality or qualities of the artifact that need to be
addressed to improve acceptance?
How does the artifact meet heuristic standards?
This cycle is divided into two phases, the build phase and the evaluation phase.
Build Phase
Various mHealth applications were reviewed by the project lead and the mHealth
coordinator and Open Data Kit (ODK) was selected for the development of mClinic. ODK
allows forms based data to be sent and received by OpenMRS on Android phones. A
development team was selected based on previous experience ODK and OpenMRS and regional
location in Sub-Saharan Africa.
Software was selected based on the constraints determined during the relevance cycle and
approved by the project team. We contracted with the development team in January 2011 and
development took place from January through May. Use cases and functional specifications
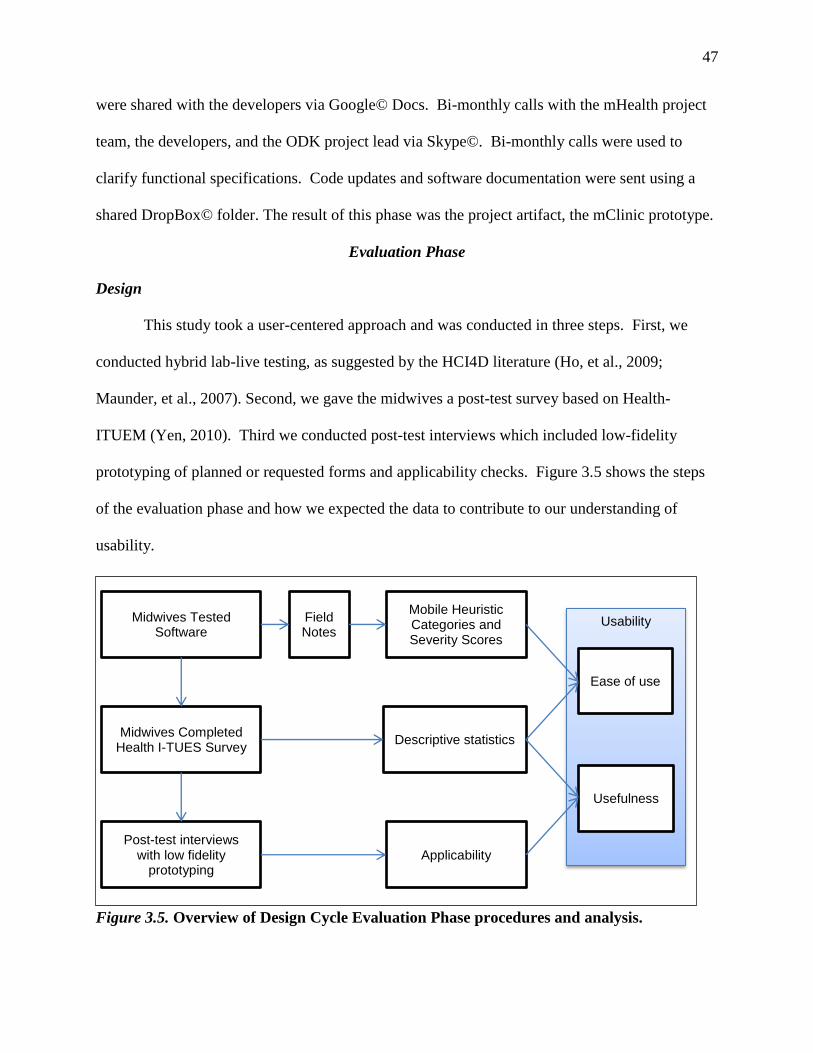
47
were shared with the developers via Google© Docs. Bi-monthly calls with the mHealth project
team, the developers, and the ODK project lead via Skype©. Bi-monthly calls were used to
clarify functional specifications. Code updates and software documentation were sent using a
shared DropBox© folder. The result of this phase was the project artifact, the mClinic prototype.
Evaluation Phase
Design
This study took a user-centered approach and was conducted in three steps. First, we
conducted hybrid lab-live testing, as suggested by the HCI4D literature (Ho, et al., 2009;
Maunder, et al., 2007). Second, we gave the midwives a post-test survey based on Health-
ITUEM (Yen, 2010). Third we conducted post-test interviews which included low-fidelity
prototyping of planned or requested forms and applicability checks. Figure 3.5 shows the steps
of the evaluation phase and how we expected the data to contribute to our understanding of
usability.
Figure 3.5. Overview of Design Cycle Evaluation Phase procedures and analysis.
Usability Midwives Tested Software
Midwives Completed Health I-TUES Survey
Post-test interviews with low fidelity
prototyping
Field Notes
Mobile Heuristic Categories and Severity Scores
Descriptive statistics
Applicability
Usefulness
Ease of use
48
Sample
All seven midwives currently working at MVP-Ghana were interviewed in their
individual facilities in May of 2011. Additional interviews were conducted with the data analyst
and the IS manager at the MVP administrative site.
Procedures
Testing of mClinic was be conducted outside of regular clinic hours, however, in some
instances there were patients being seen in the facilities at the same time. Participants were
given three scenarios based on goals and developed use cases. The first was to register a new
patient into the mClinic, the second and third were to record patients who had come into the
clinic with a fever and were suspected of having malaria. Real data collected in the clinic was
used for the testing and deleted afterwards. The participants were asked to provide feedback
while using mClinic. This testing was voice recorded as well as the researcher recording field
notes.
Post-testing, participants completed a survey using a modified version of the Health-
ITUES scale (Appendix A), which assesses perceived usability. Exploratory factor analysis
extracted a four factor solution with Cronbach’s alphas ranged from .81 to .95 for subscales in a
sample of registered nurses rating a shift scheduling system (Yen, Wantland, & Bakken, 2010).
A confirmatory factor analysis showed that the explained variances were: 78.1% for quality of
work life, 93.4% for perceived usefulness, 51.0% for perceived ease-of-use, and 39.9% for user
control (Yen, 2010).
Finally, we conducted post-testing interviews. Midwives were asked their thoughts about
the usability and usefulness of mClinic. Applicability checks on functional requirements and use
cases were conducted with the MVP midwives and MVP staff. Midwives were shown low-
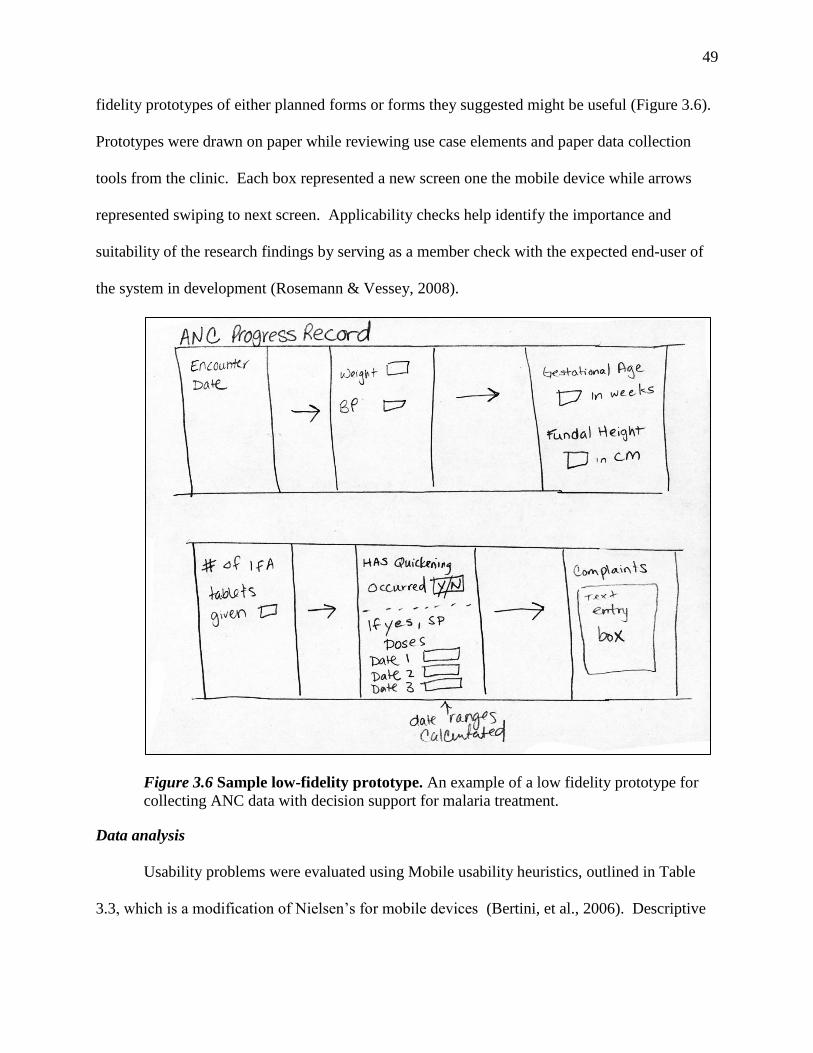
49
fidelity prototypes of either planned forms or forms they suggested might be useful (Figure 3.6).
Prototypes were drawn on paper while reviewing use case elements and paper data collection
tools from the clinic. Each box represented a new screen one the mobile device while arrows
represented swiping to next screen. Applicability checks help identify the importance and
suitability of the research findings by serving as a member check with the expected end-user of
the system in development (Rosemann & Vessey, 2008).
Figure 3.6 Sample low-fidelity prototype. An example of a low fidelity prototype for
collecting ANC data with decision support for malaria treatment.
Data analysis
Usability problems were evaluated using Mobile usability heuristics, outlined in Table
3.3, which is a modification of Nielsen’s for mobile devices (Bertini, et al., 2006). Descriptive
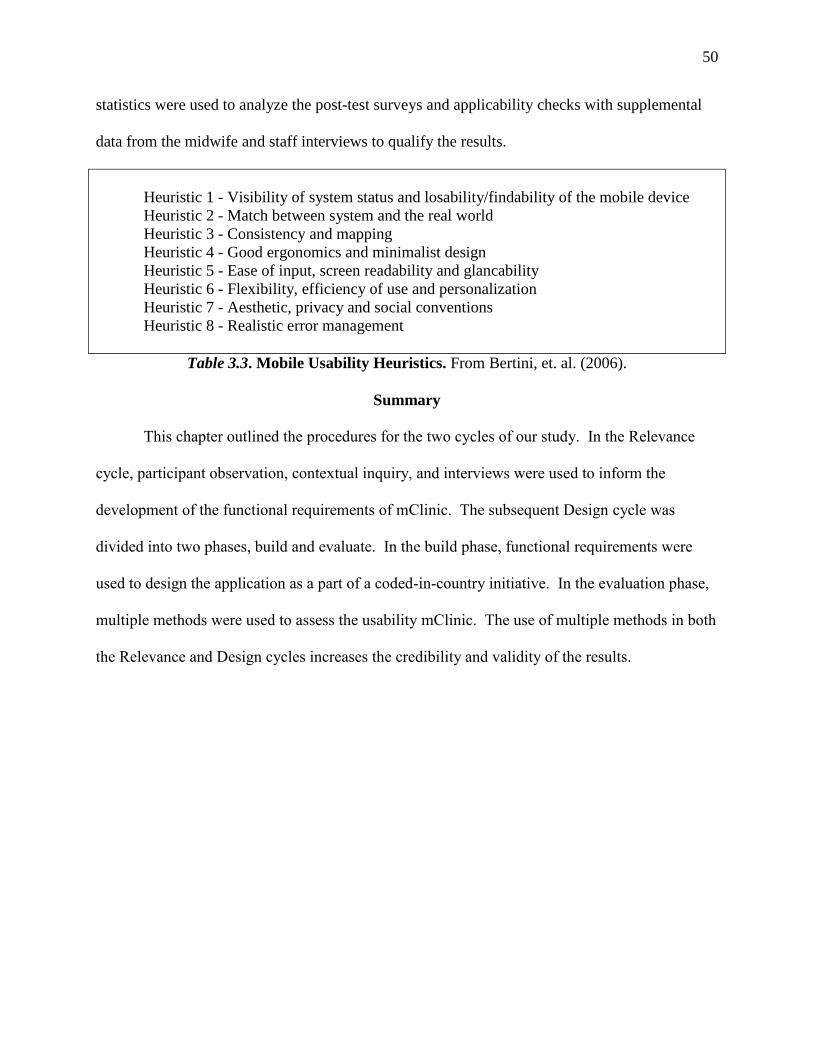
50
statistics were used to analyze the post-test surveys and applicability checks with supplemental
data from the midwife and staff interviews to qualify the results.
Heuristic 1 - Visibility of system status and losability/findability of the mobile device
Heuristic 2 - Match between system and the real world
Heuristic 3 - Consistency and mapping
Heuristic 4 - Good ergonomics and minimalist design
Heuristic 5 - Ease of input, screen readability and glancability
Heuristic 6 - Flexibility, efficiency of use and personalization
Heuristic 7 - Aesthetic, privacy and social conventions
Heuristic 8 - Realistic error management
Table 3.3. Mobile Usability Heuristics. From Bertini, et. al. (2006).
Summary
This chapter outlined the procedures for the two cycles of our study. In the Relevance
cycle, participant observation, contextual inquiry, and interviews were used to inform the
development of the functional requirements of mClinic. The subsequent Design cycle was
divided into two phases, build and evaluate. In the build phase, functional requirements were
used to design the application as a part of a coded-in-country initiative. In the evaluation phase,
multiple methods were used to assess the usability mClinic. The use of multiple methods in both
the Relevance and Design cycles increases the credibility and validity of the results.
51
CHAPTER IV. RESULTS
The results presented in this chapter describe the findings of each of the research cycles.
In the first cycle, the relevance cycle, we studied the people, organizations, and technology that
make up MVP-Ghana. In this cycle we identified the problems and opportunities that exist in the
current system. Finally, we developed functional requirements based on the goals, use cases, and
system qualities to inform the design of an artifact, known as mClinic. In the second cycle, the
design cycle, we tested the usability of our mClinic prototype. We also validated the functional
specifications created in the first cycle.
Cycle 1. Relevance Cycle
The first phase of the relevance cycle involves requirements gathering, which can be
broadly categorized into three topics: people, organizations, and technology. This was done
through participant observation and interviewing midwives using the design-actuality gaps
model to guide our questions. A total of eight midwives were interviewed for this study
representing all the midwives currently working in the Bonsaaso, Ghana cluster of the MVP.
Five of the midwives were interviewed twice, once in September 2010 and again in May of
2011. One midwife was unavailable for the first round of interviews and interviewed only in
May 2011. Another midwife who had been interviewed in September 2010 had quit and her
replacement was interviewed in May of 2011. Table 4.1 is a list of the midwives interviewed
indicating whether they were interviewed in the first, second, or both rounds; the number of
years of experience they have as a practicing midwife; and, their classification as an experienced
or inexperienced using five years as a cutoff.
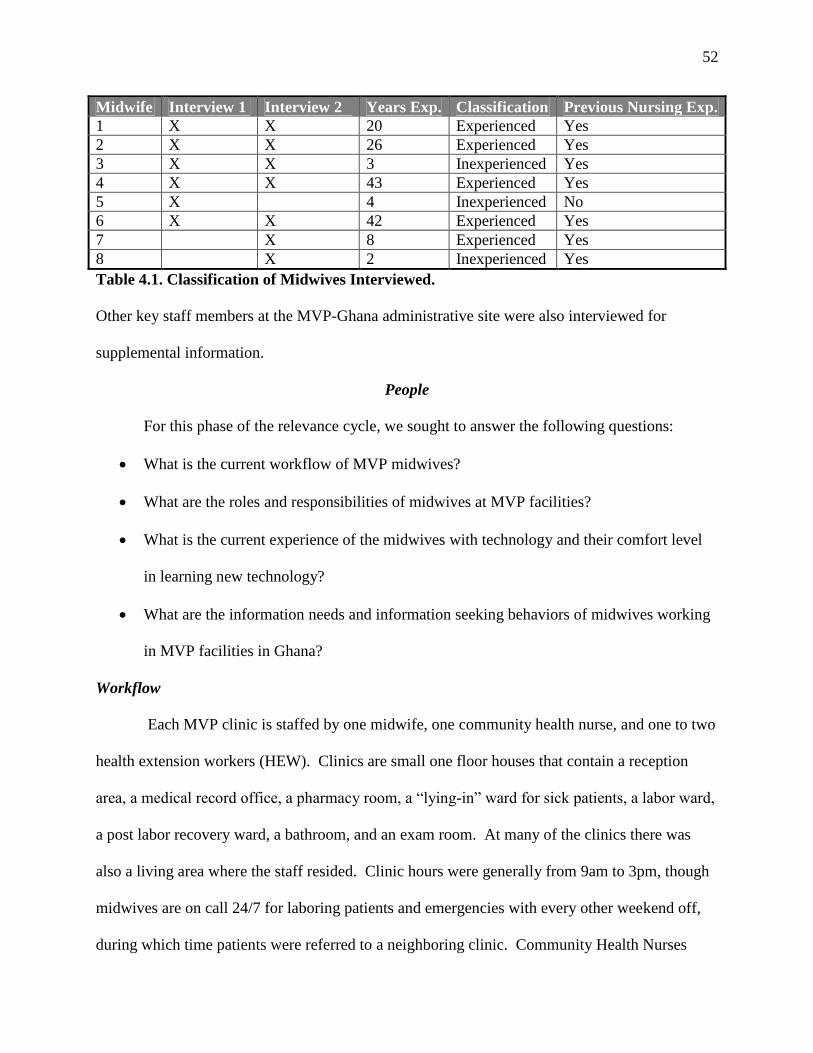
52
Midwife Interview 1 Interview 2 Years Exp. Classification Previous Nursing Exp.
1 X X 20 Experienced Yes
2 X X 26 Experienced Yes
3 X X 3 Inexperienced Yes
4 X X 43 Experienced Yes
5 X 4 Inexperienced No
6 X X 42 Experienced Yes
7 X 8 Experienced Yes
8 X 2 Inexperienced Yes
Table 4.1. Classification of Midwives Interviewed.
Other key staff members at the MVP-Ghana administrative site were also interviewed for
supplemental information.
People
For this phase of the relevance cycle, we sought to answer the following questions:
What is the current workflow of MVP midwives?
What are the roles and responsibilities of midwives at MVP facilities?
What is the current experience of the midwives with technology and their comfort level
in learning new technology?
What are the information needs and information seeking behaviors of midwives working
in MVP facilities in Ghana?
Workflow
Each MVP clinic is staffed by one midwife, one community health nurse, and one to two
health extension workers (HEW). Clinics are small one floor houses that contain a reception
area, a medical record office, a pharmacy room, a “lying-in” ward for sick patients, a labor ward,
a post labor recovery ward, a bathroom, and an exam room. At many of the clinics there was
also a living area where the staff resided. Clinic hours were generally from 9am to 3pm, though
midwives are on call 24/7 for laboring patients and emergencies with every other weekend off,
during which time patients were referred to a neighboring clinic. Community Health Nurses
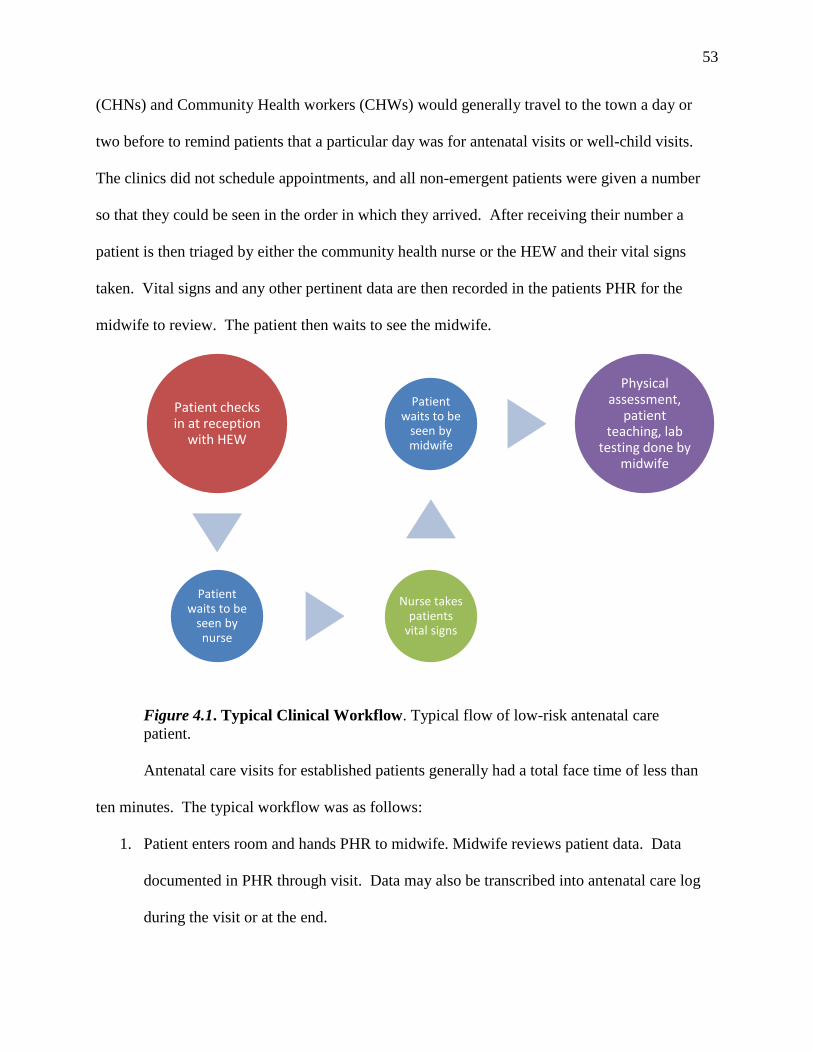
53
(CHNs) and Community Health workers (CHWs) would generally travel to the town a day or
two before to remind patients that a particular day was for antenatal visits or well-child visits.
The clinics did not schedule appointments, and all non-emergent patients were given a number
so that they could be seen in the order in which they arrived. After receiving their number a
patient is then triaged by either the community health nurse or the HEW and their vital signs
taken. Vital signs and any other pertinent data are then recorded in the patients PHR for the
midwife to review. The patient then waits to see the midwife.
Figure 4.1. Typical Clinical Workflow. Typical flow of low-risk antenatal care
patient.
Antenatal care visits for established patients generally had a total face time of less than
ten minutes. The typical workflow was as follows:
1. Patient enters room and hands PHR to midwife. Midwife reviews patient data. Data
documented in PHR through visit. Data may also be transcribed into antenatal care log
during the visit or at the end.
Patient checks in at reception
with HEW
Patient waits to be
seen by nurse
Nurse takes patients
vital signs
Patient waits to be
seen by midwife
Physical assessment,
patient teaching, lab
testing done by midwife
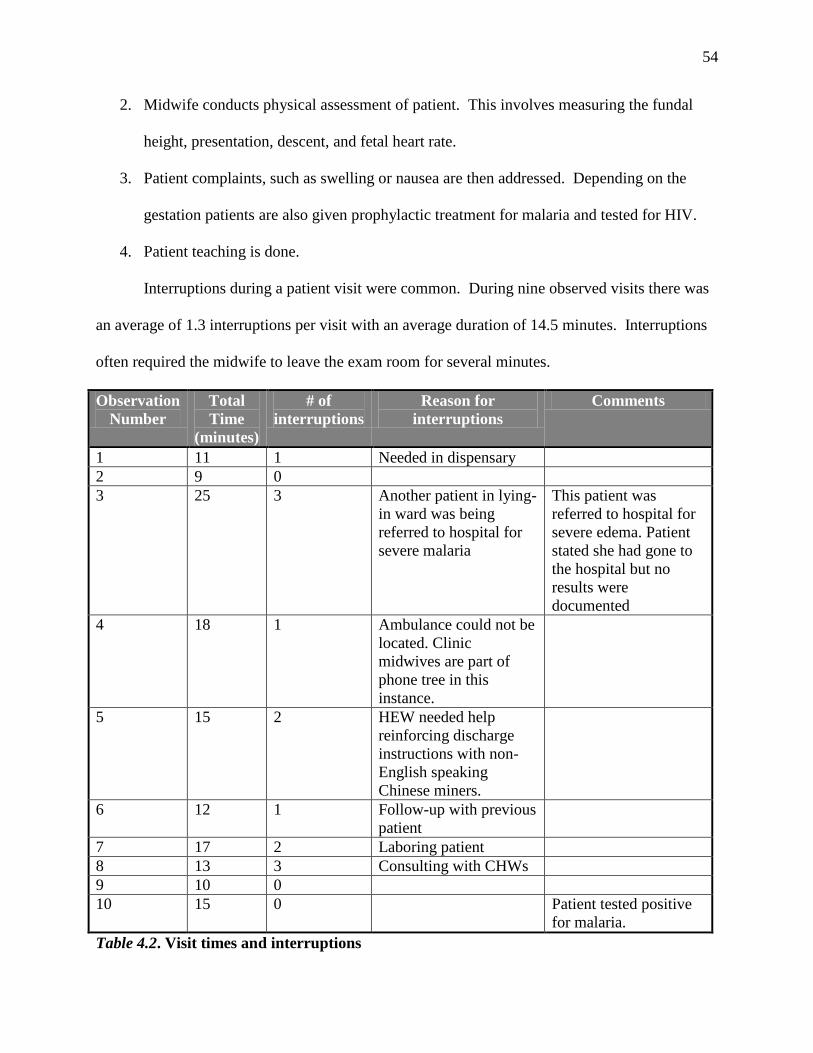
54
2. Midwife conducts physical assessment of patient. This involves measuring the fundal
height, presentation, descent, and fetal heart rate.
3. Patient complaints, such as swelling or nausea are then addressed. Depending on the
gestation patients are also given prophylactic treatment for malaria and tested for HIV.
4. Patient teaching is done.
Interruptions during a patient visit were common. During nine observed visits there was
an average of 1.3 interruptions per visit with an average duration of 14.5 minutes. Interruptions
often required the midwife to leave the exam room for several minutes.
Observation
Number
Total
Time
(minutes)
# of
interruptions
Reason for
interruptions
Comments
1 11 1 Needed in dispensary
2 9 0
3 25 3 Another patient in lying-
in ward was being
referred to hospital for
severe malaria
This patient was
referred to hospital for
severe edema. Patient
stated she had gone to
the hospital but no
results were
documented
4 18 1 Ambulance could not be
located. Clinic
midwives are part of
phone tree in this
instance.
5 15 2 HEW needed help
reinforcing discharge
instructions with non-
English speaking
Chinese miners.
6 12 1 Follow-up with previous
patient
7 17 2 Laboring patient
8 13 3 Consulting with CHWs
9 10 0
10 15 0 Patient tested positive
for malaria.
Table 4.2. Visit times and interruptions
55
Interruptions may disrupt clinical reasoning thus compromising patient safety and/or
cause patient dissatisfaction (Potter et al., 2005). A high frequency of interruptions may impact
patient safety as well as being an important aspect of clinical workflow, as the artifact will have
to allow for easy movement between patients (Martikainen, Ikavalko, & Korpela, 2010).
Roles and Responsibilities
Midwives were responsible for documenting nearly all of the patient care. The majority
of documentation took place in the patient’s PHR with an abbreviated note written on the paper
chart. Additional patient data were logged into one of the following registers: antenatal care,
well child, fever, cash, delivery, and/or outpatient. Registers serve as the primary data source for
monthly reporting.
There was a high burden of monthly reporting. There were over a dozen monthly (or
more frequent) reports, listed in Table 4.3, required to be submitted to GHS and/or MVP
administration.
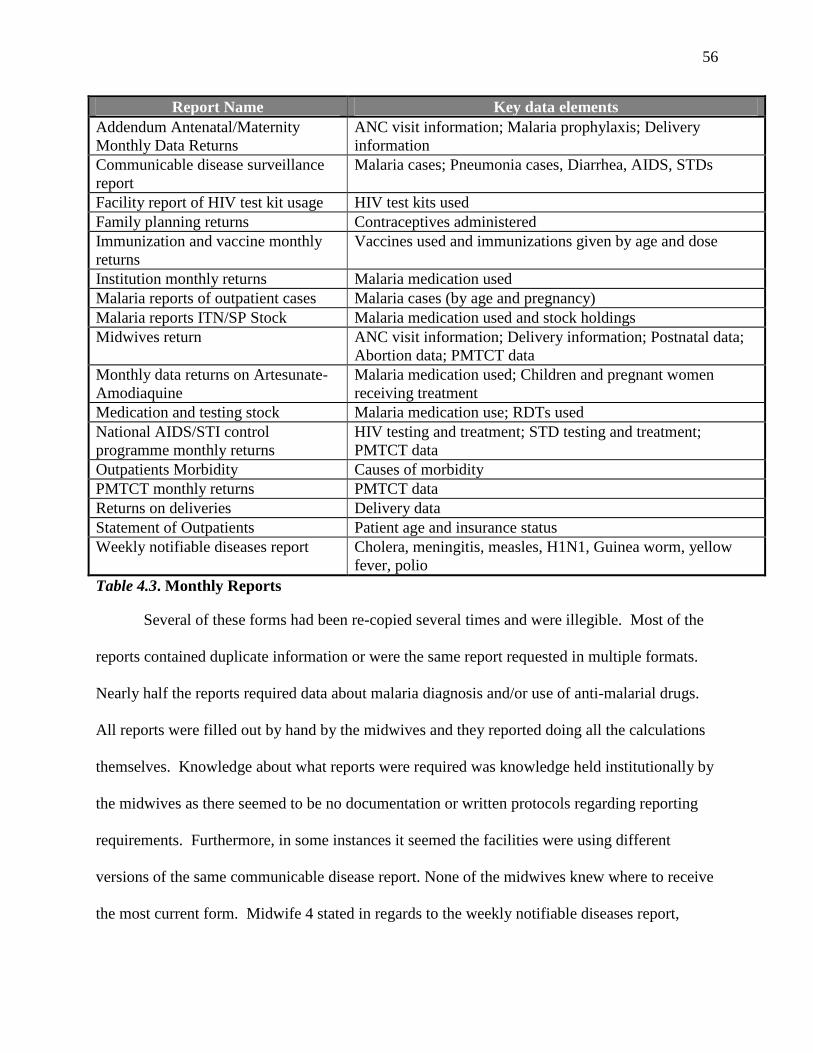
56
Report Name Key data elements
Addendum Antenatal/Maternity
Monthly Data Returns
ANC visit information; Malaria prophylaxis; Delivery
information
Communicable disease surveillance
report
Malaria cases; Pneumonia cases, Diarrhea, AIDS, STDs
Facility report of HIV test kit usage HIV test kits used
Family planning returns Contraceptives administered
Immunization and vaccine monthly
returns
Vaccines used and immunizations given by age and dose
Institution monthly returns Malaria medication used
Malaria reports of outpatient cases Malaria cases (by age and pregnancy)
Malaria reports ITN/SP Stock Malaria medication used and stock holdings
Midwives return ANC visit information; Delivery information; Postnatal data;
Abortion data; PMTCT data
Monthly data returns on Artesunate-
Amodiaquine
Malaria medication used; Children and pregnant women
receiving treatment
Medication and testing stock Malaria medication use; RDTs used
National AIDS/STI control
programme monthly returns
HIV testing and treatment; STD testing and treatment;
PMTCT data
Outpatients Morbidity Causes of morbidity
PMTCT monthly returns PMTCT data
Returns on deliveries Delivery data
Statement of Outpatients Patient age and insurance status
Weekly notifiable diseases report Cholera, meningitis, measles, H1N1, Guinea worm, yellow
fever, polio
Table 4.3. Monthly Reports
Several of these forms had been re-copied several times and were illegible. Most of the
reports contained duplicate information or were the same report requested in multiple formats.
Nearly half the reports required data about malaria diagnosis and/or use of anti-malarial drugs.
All reports were filled out by hand by the midwives and they reported doing all the calculations
themselves. Knowledge about what reports were required was knowledge held institutionally by
the midwives as there seemed to be no documentation or written protocols regarding reporting
requirements. Furthermore, in some instances it seemed the facilities were using different
versions of the same communicable disease report. None of the midwives knew where to receive
the most current form. Midwife 4 stated in regards to the weekly notifiable diseases report,
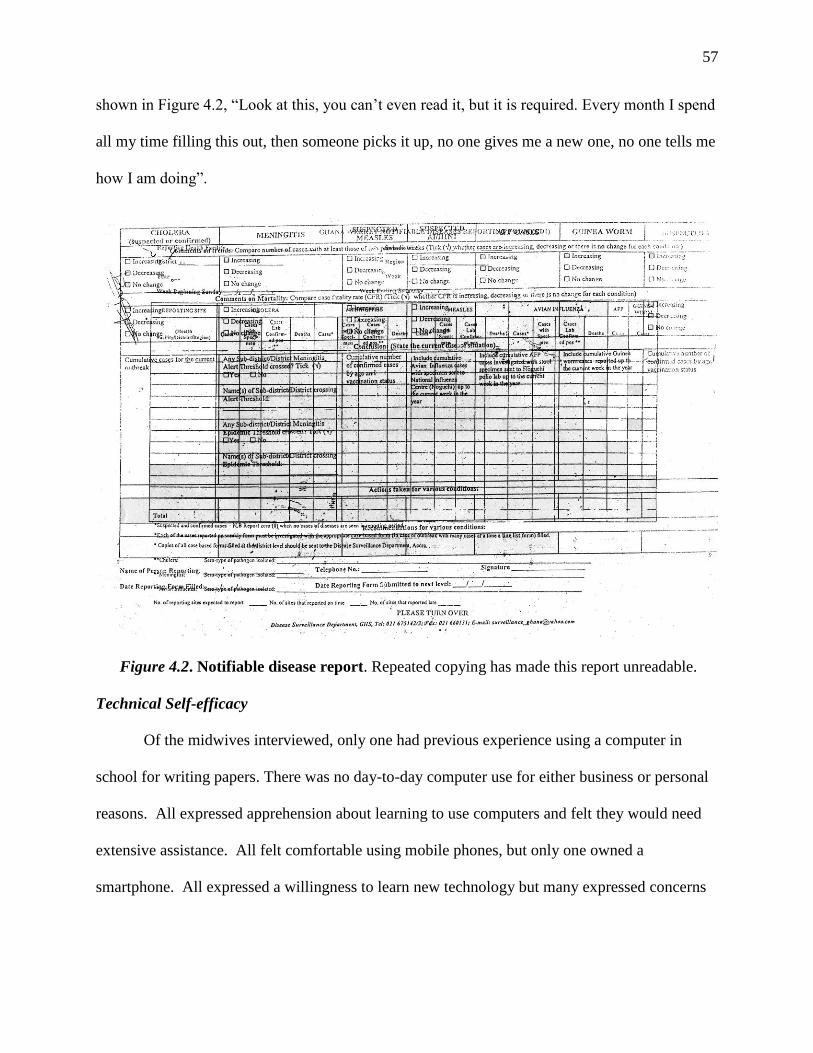
57
shown in Figure 4.2, “Look at this, you can’t even read it, but it is required. Every month I spend
all my time filling this out, then someone picks it up, no one gives me a new one, no one tells me
how I am doing”.
Figure 4.2. Notifiable disease report. Repeated copying has made this report unreadable.
Technical Self-efficacy
Of the midwives interviewed, only one had previous experience using a computer in
school for writing papers. There was no day-to-day computer use for either business or personal
reasons. All expressed apprehension about learning to use computers and felt they would need
extensive assistance. All felt comfortable using mobile phones, but only one owned a
smartphone. All expressed a willingness to learn new technology but many expressed concerns
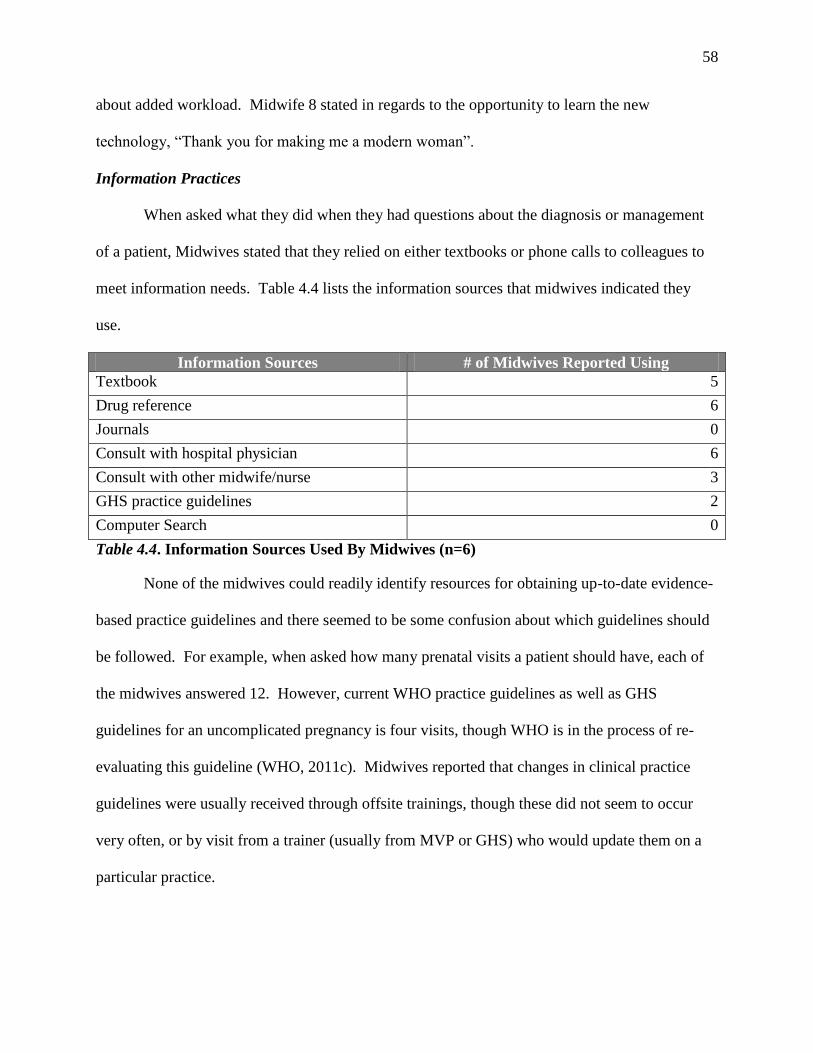
58
about added workload. Midwife 8 stated in regards to the opportunity to learn the new
technology, “Thank you for making me a modern woman”.
Information Practices
When asked what they did when they had questions about the diagnosis or management
of a patient, Midwives stated that they relied on either textbooks or phone calls to colleagues to
meet information needs. Table 4.4 lists the information sources that midwives indicated they
use.
Information Sources # of Midwives Reported Using
Textbook 5
Drug reference 6
Journals 0
Consult with hospital physician 6
Consult with other midwife/nurse 3
GHS practice guidelines 2
Computer Search 0
Table 4.4. Information Sources Used By Midwives (n=6)
None of the midwives could readily identify resources for obtaining up-to-date evidence-
based practice guidelines and there seemed to be some confusion about which guidelines should
be followed. For example, when asked how many prenatal visits a patient should have, each of
the midwives answered 12. However, current WHO practice guidelines as well as GHS
guidelines for an uncomplicated pregnancy is four visits, though WHO is in the process of re-
evaluating this guideline (WHO, 2011c). Midwives reported that changes in clinical practice
guidelines were usually received through offsite trainings, though these did not seem to occur
very often, or by visit from a trainer (usually from MVP or GHS) who would update them on a
particular practice.
59
Patient information came primarily from the patient’s paper-based personal health
records (PHRs) and patient self-report. These are paper booklets given to the patient at the time
of their first visit for a particular condition that are produced by Ghana Health Services. There
are booklets for maternal health, family planning, child health, and adult health. It is uncommon
for patients to come to the clinic without the PHRs. Paper-based medical records are also kept at
the clinic but the records are 8.5 by 5.5 inch index cards that hold sparse information. New
medical records are created every year with the previous year’s record number contained on the
new card for reference. The record numbers are created by the order in which the patient is seen
throughout the year, for example, the fifth patient seen in 2011 would have a record number of
5/2011. Midwives reported that these records are rarely useful for patient history since more
pertinent and up-to-date information would be in the patient’s PHR.
Midwives reported a number of barriers to accessing information. First, while all the
midwives had both personal and MVP supplied cellular phones, many felt they did not receive
adequate credit (air time) for placing calls to follow-up on referrals or for collaborating with
colleagues. Several of the midwives reported feeling isolated and disconnected from the
administrative offices and that their needs were often unaddressed. Midwife 1 stated: “They [the
administrators] come here and they don’t even tell us they are coming. We need things they can
bring us but they don’t call. I don’t have a car; I don’t even have a bicycle. We need food, we
need supplies, but they don’t let us know.”
While all the clinics had computers installed, only five of the seven clinics were able to
access the internet. The midwives all reported having little-to-no experience using computers
and no experience searching for clinical practice resources online. Midwife 3 stated: “They have
60
to come and train us so we are more confident with the computer. We don’t know what we are
doing with the computer. None of us.”
Experienced midwives were less likely to report consequences of not having access to
information. Midwife 4 stated: “I have all the information I need”, though this same midwife
later complained about not receiving follow-up information from both referrals and from reports
sent to the MOH. Inexperienced midwives were more likely to vocalize having unmet
information needs resulting in unnecessary patient referrals and a lack of confidence in clinical
practice. Midwife 5, who later quit stated: “Sometimes I don’t know what to do, and I refer a
patient to the hospital. I probably don’t need to do it, but no one tells me, and I never know what
the results were.”
The midwives reported a number of unmet information needs. All reported difficulty in
receiving follow-up information on patients referred to the local district hospital. Patients were
most often referred for HIV and other lab testing, severe malaria, complications of pregnancy, or
for complex diagnoses. Inexperienced midwives in particular were concerned that they were
referring patients unnecessarily but since no feedback was available there was no opportunity for
learning how to manage a particular case.
Preparation for Knowledge Work
Nurses and midwives are unable to function as knowledge workers when clinical data is
“fragmented, incomplete, and unreliable” (Snyder-Halpern, et al., 2001, p. 19). In the MVP-
Ghana clinics, clinic data is fragmented across multiple sources. The most complete records, the
patient’s PHR is not kept in the clinic. Additional data elements are spread across multiple
registries and incomplete paper records. The quality of the data is questionable as evidence
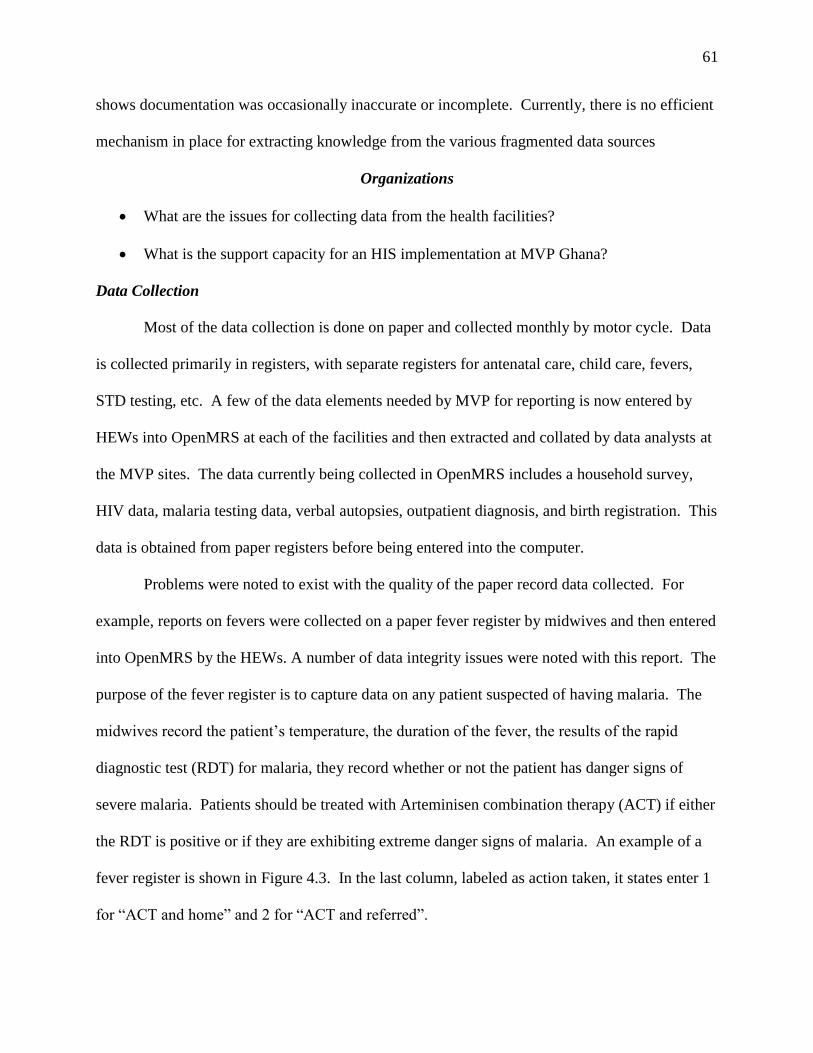
61
shows documentation was occasionally inaccurate or incomplete. Currently, there is no efficient
mechanism in place for extracting knowledge from the various fragmented data sources
Organizations
What are the issues for collecting data from the health facilities?
What is the support capacity for an HIS implementation at MVP Ghana?
Data Collection
Most of the data collection is done on paper and collected monthly by motor cycle. Data
is collected primarily in registers, with separate registers for antenatal care, child care, fevers,
STD testing, etc. A few of the data elements needed by MVP for reporting is now entered by
HEWs into OpenMRS at each of the facilities and then extracted and collated by data analysts at
the MVP sites. The data currently being collected in OpenMRS includes a household survey,
HIV data, malaria testing data, verbal autopsies, outpatient diagnosis, and birth registration. This
data is obtained from paper registers before being entered into the computer.
Problems were noted to exist with the quality of the paper record data collected. For
example, reports on fevers were collected on a paper fever register by midwives and then entered
into OpenMRS by the HEWs. A number of data integrity issues were noted with this report. The
purpose of the fever register is to capture data on any patient suspected of having malaria. The
midwives record the patient’s temperature, the duration of the fever, the results of the rapid
diagnostic test (RDT) for malaria, they record whether or not the patient has danger signs of
severe malaria. Patients should be treated with Arteminisen combination therapy (ACT) if either
the RDT is positive or if they are exhibiting extreme danger signs of malaria. An example of a
fever register is shown in Figure 4.3. In the last column, labeled as action taken, it states enter 1
for “ACT and home” and 2 for “ACT and referred”.
62
Figure 4.3. Fever register. This form is indicative of data quality issues with existing paper
documentation.
In the last column all the patients have 1, indicating that they were treated with ACT and sent
home. However, none of the patients had danger signs of malaria and only eight of 17 had a
positive RDT. This problem was found in three of four clinics where we checked for the issue.
To further complicate this matter, the data analyst reported that this format was not consistent
with what was required by GHS. That report lists the following options for the “Action Taken”
column: “1. ACT and Home”, “2. Treated for Severe malaria”, “3. ACT and antibiotics”; “4.
Antibiotics”; “5. Referral to hospital”, “6. Observed and sent home”, and “7. Other”. Additional,
another data element for post-48 hour follow-up is needed but not captured in the current form.
63
Technical Support
There are currently two full-time IT staff members employed at the main administrative
site. This site is located one to two hours’ drive from any of the clinics, limiting the availability
of on-site technical support. There is likely to be limited resources for providing on-site support
for the phones.
Technology
What is the current technology infrastructure at MVP Ghana?
Infrastructure and resources. Internet access at the health clinics is delivered via
cellular service. Only five of the seven sites had a reliable cellphone signal due the location of
cell towers. An additional tower is expected to be constructed in the next year to resolve signal
issues at the remaining two sites. Both network outages and slowdowns were reported as
occurring occasionally. The clinics are supplied electricity using solar panels. Black outs and
brown outs occur occasionally.
Outage Type Time 1 Time 2
Network Outages 1 3
Internet Outages N/A 2
Table 4.5. Network and Internet Outages
While 3G is supposed to be widely available, the most commonly picked up signal was general
packet radio service (GPRS) Edge (2.9G).
Each facility maintained one charging station for cell phones which was also where
computers were connected to a power supply. All of the sites had computers in place but facility
staff reported that they had not received adequate training on their use. At the sites with internet
access, the HEWs were doing some data entry into OpenMRS, otherwise the computers were
unused. The IS manager reported one computer had become unusable when a community
member had inserted a USB drive with a virus into it. Additionally, another computer was
64
observed to have been moved under a window into direct sunlight, potentially causing damage.
The IS manager reported limited resources for adequately maintaining and keeping the
computers on site up-to-date. Remote desktop management software is not currently in use at
MVP. He also reported there is no plan in place for training users on computer competence and
basic maintenance. Additionally, he stated security of computers in the facilities as inadequate.
Problems and Opportunities
In this second phase of the relevance cycle, we used the data from the first phase to
develop functional specifications for an artifact, known as mClinic, for use at MVP-Ghana. The
research question for this phase was:
What are the functionality requirements for the application based on the needs and
constraints of the application environment?
Goals
Functional requirements were specified for mClinic over an eight month period from July
2010 – March 2011. Initial goals were gathered from senior staff at MVP and it was determined
there was a need for a mobile interface to interact with OpenMRS within the facilities. The
initial focus of the application would be on patient registration, Antenatal care (ANC) patients,
and malaria treatment, but with the flexibility to incorporate other types of patients in the future,
such as family planning, referral tracking, and child health. The results of the initial six
interviews with MVP midwives in September 2010, analysis of current paper based reporting
and record tools, and comparison with the WHO’s clinical practice guidelines were used to
answer the following questions regarding functional requirements. The results of the interviews
validated the need for better documentation practices regarding ANC and malaria treatment.
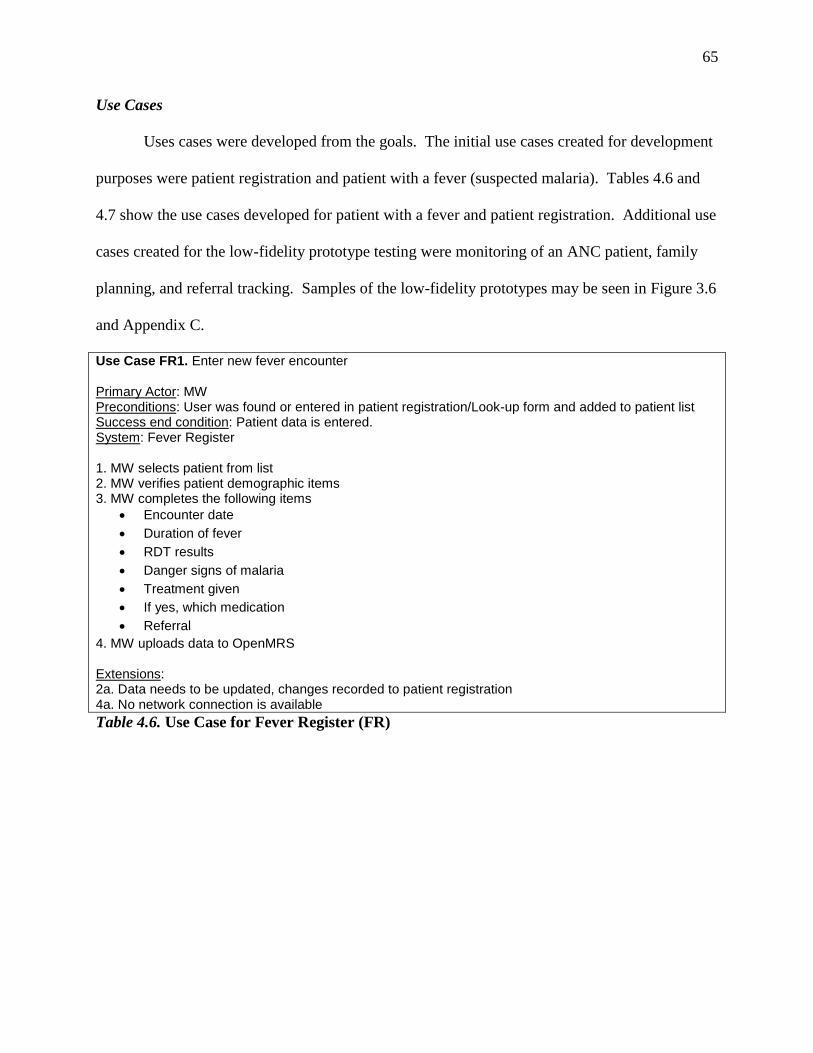
65
Use Cases
Uses cases were developed from the goals. The initial use cases created for development
purposes were patient registration and patient with a fever (suspected malaria). Tables 4.6 and
4.7 show the use cases developed for patient with a fever and patient registration. Additional use
cases created for the low-fidelity prototype testing were monitoring of an ANC patient, family
planning, and referral tracking. Samples of the low-fidelity prototypes may be seen in Figure 3.6
and Appendix C.
Use Case FR1. Enter new fever encounter Primary Actor: MW Preconditions: User was found or entered in patient registration/Look-up form and added to patient list Success end condition: Patient data is entered. System: Fever Register 1. MW selects patient from list 2. MW verifies patient demographic items 3. MW completes the following items
Encounter date
Duration of fever
RDT results
Danger signs of malaria
Treatment given
If yes, which medication
Referral
4. MW uploads data to OpenMRS Extensions: 2a. Data needs to be updated, changes recorded to patient registration 4a. No network connection is available
Table 4.6. Use Case for Fever Register (FR)
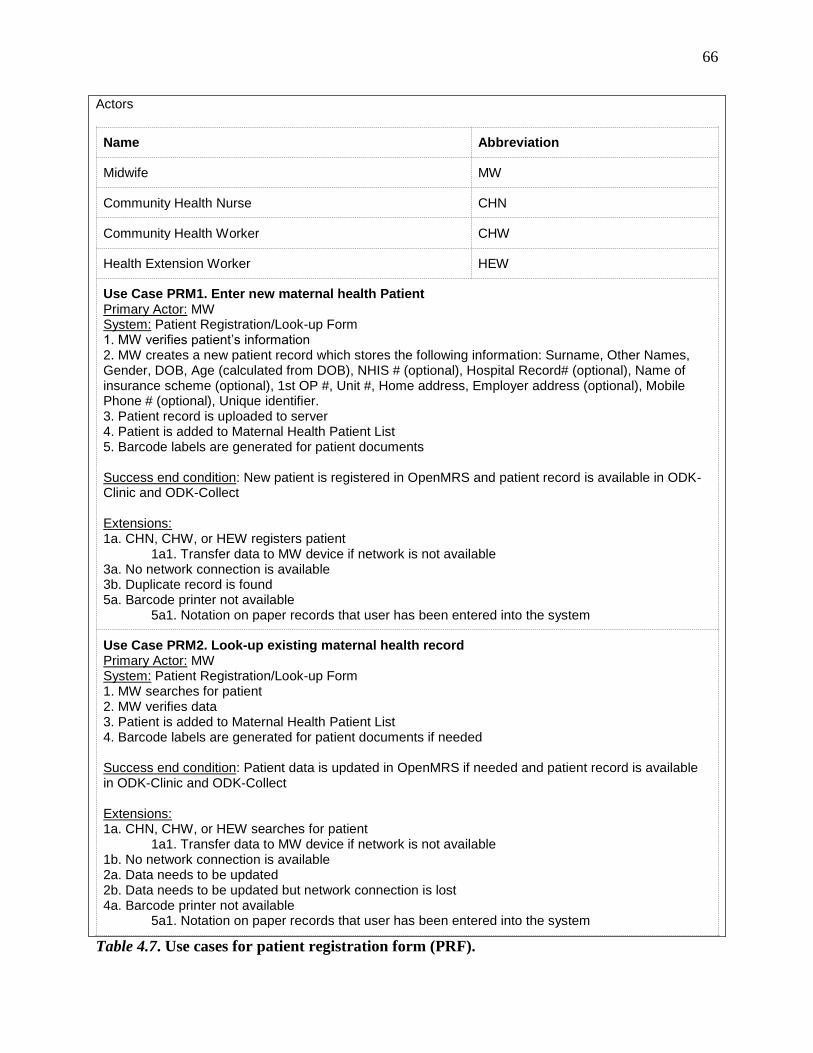
66
Actors
Name Abbreviation
Midwife MW
Community Health Nurse CHN
Community Health Worker CHW
Health Extension Worker HEW
Use Case PRM1. Enter new maternal health Patient Primary Actor: MW System: Patient Registration/Look-up Form 1. MW verifies patient’s information 2. MW creates a new patient record which stores the following information: Surname, Other Names, Gender, DOB, Age (calculated from DOB), NHIS # (optional), Hospital Record# (optional), Name of insurance scheme (optional), 1st OP #, Unit #, Home address, Employer address (optional), Mobile Phone # (optional), Unique identifier. 3. Patient record is uploaded to server 4. Patient is added to Maternal Health Patient List 5. Barcode labels are generated for patient documents Success end condition: New patient is registered in OpenMRS and patient record is available in ODK-Clinic and ODK-Collect Extensions: 1a. CHN, CHW, or HEW registers patient 1a1. Transfer data to MW device if network is not available 3a. No network connection is available 3b. Duplicate record is found 5a. Barcode printer not available 5a1. Notation on paper records that user has been entered into the system
Use Case PRM2. Look-up existing maternal health record Primary Actor: MW System: Patient Registration/Look-up Form 1. MW searches for patient 2. MW verifies data 3. Patient is added to Maternal Health Patient List 4. Barcode labels are generated for patient documents if needed Success end condition: Patient data is updated in OpenMRS if needed and patient record is available in ODK-Clinic and ODK-Collect Extensions: 1a. CHN, CHW, or HEW searches for patient 1a1. Transfer data to MW device if network is not available 1b. No network connection is available 2a. Data needs to be updated 2b. Data needs to be updated but network connection is lost 4a. Barcode printer not available 5a1. Notation on paper records that user has been entered into the system
Table 4.7. Use cases for patient registration form (PRF).
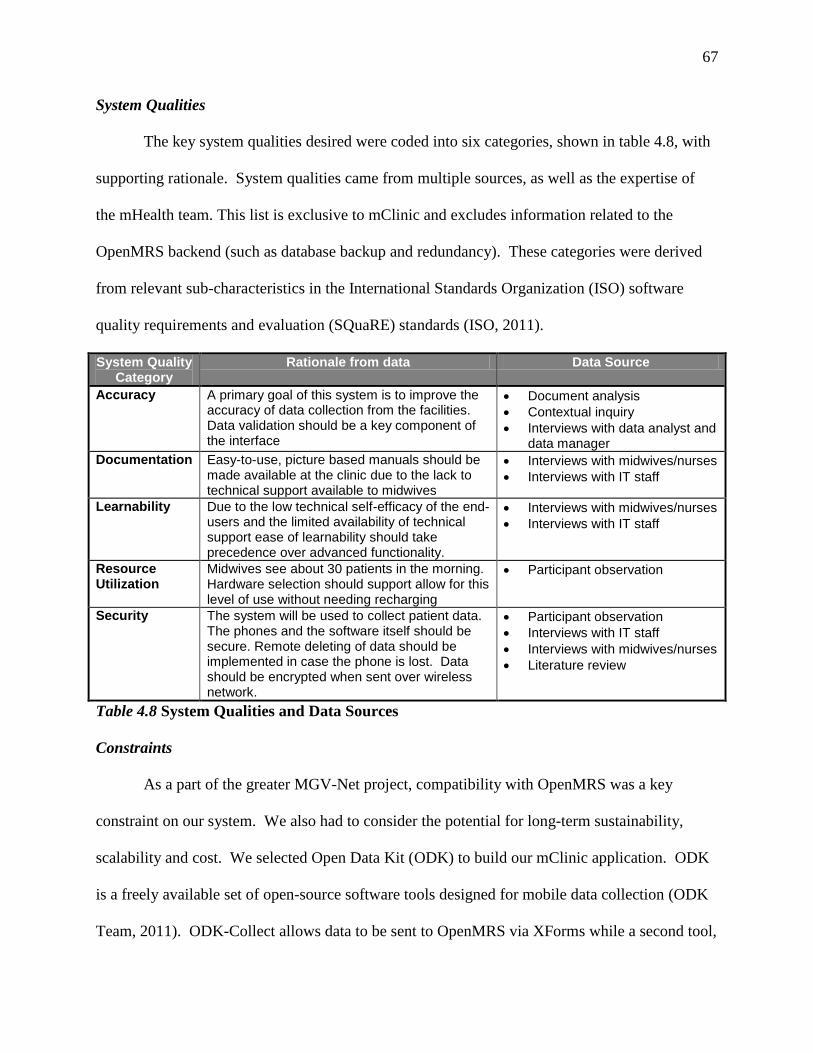
67
System Qualities
The key system qualities desired were coded into six categories, shown in table 4.8, with
supporting rationale. System qualities came from multiple sources, as well as the expertise of
the mHealth team. This list is exclusive to mClinic and excludes information related to the
OpenMRS backend (such as database backup and redundancy). These categories were derived
from relevant sub-characteristics in the International Standards Organization (ISO) software
quality requirements and evaluation (SQuaRE) standards (ISO, 2011).
System Quality Category
Rationale from data Data Source
Accuracy A primary goal of this system is to improve the accuracy of data collection from the facilities. Data validation should be a key component of the interface
Document analysis
Contextual inquiry
Interviews with data analyst and data manager
Documentation Easy-to-use, picture based manuals should be made available at the clinic due to the lack to technical support available to midwives
Interviews with midwives/nurses
Interviews with IT staff
Learnability Due to the low technical self-efficacy of the end-users and the limited availability of technical support ease of learnability should take precedence over advanced functionality.
Interviews with midwives/nurses
Interviews with IT staff
Resource Utilization
Midwives see about 30 patients in the morning. Hardware selection should support allow for this level of use without needing recharging
Participant observation
Security The system will be used to collect patient data. The phones and the software itself should be secure. Remote deleting of data should be implemented in case the phone is lost. Data should be encrypted when sent over wireless network.
Participant observation
Interviews with IT staff
Interviews with midwives/nurses
Literature review
Table 4.8 System Qualities and Data Sources
Constraints
As a part of the greater MGV-Net project, compatibility with OpenMRS was a key
constraint on our system. We also had to consider the potential for long-term sustainability,
scalability and cost. We selected Open Data Kit (ODK) to build our mClinic application. ODK
is a freely available set of open-source software tools designed for mobile data collection (ODK
Team, 2011). ODK-Collect allows data to be sent to OpenMRS via XForms while a second tool,
68
ODK-Clinic, allows for viewing of data from OpenMRS. We contracted with a Kenyan-based
software company, Mindflow, to modify the tools so that patient data can be viewed, added, and
updated seamlessly with ODK-Clinic. We chose this software because it worked on Android-
based cellphones which are widely available in Africa and becoming increasingly less expensive.
Furthermore, forms for ANC patients, malaria, and our other use cases could easily be created
and added to ODK-Clinic by non-programmers thus keeping the cost of development low. We
wanted to use smartphones over java-based phones because of the desire to offer decision
support, such as for malaria treatment or PMTCT, and to display and increased amount of
clinical data that would not be viewable on a smaller phone. Secondly, the modularity of ODK
meant we could start with one or two data collection tools, such as antenatal progress notes, and
it expand it by simply adding more forms as the midwives become comfortable using the system.
It was also our desire that by using XForms that non-programmers could design and create
additional forms using the XForms builder in OpenMRS, thus increasing the ease of scalability
of the system.
Functional Specification
Table 4.9 is a list of an initial set of forms we planned to develop based on the first phase
of the relevance cycle and the use cases. Due to time constraints, only the patient lookup and
registration form and the fever registry form were ready in time for testing. However, these form
sets were useful for the applicability checks that were conducted with the midwives, the results
of which will be discussed later.
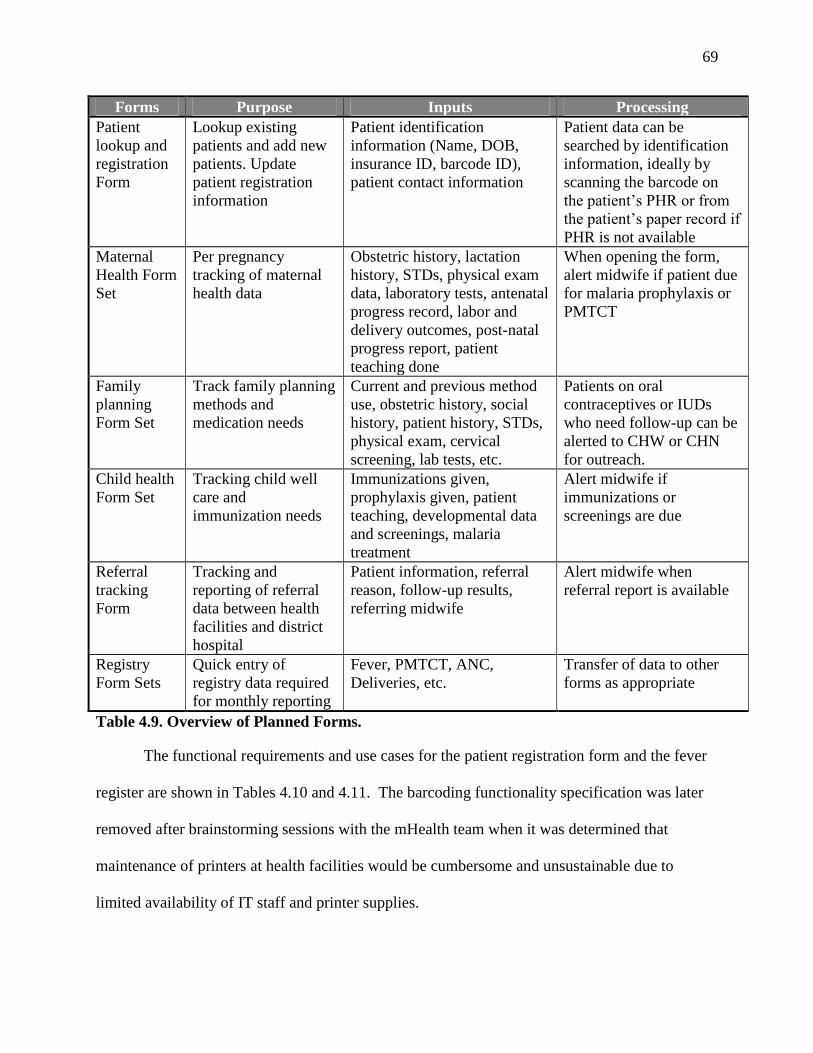
69
Forms Purpose Inputs Processing
Patient
lookup and
registration
Form
Lookup existing
patients and add new
patients. Update
patient registration
information
Patient identification
information (Name, DOB,
insurance ID, barcode ID),
patient contact information
Patient data can be
searched by identification
information, ideally by
scanning the barcode on
the patient’s PHR or from
the patient’s paper record if
PHR is not available
Maternal
Health Form
Set
Per pregnancy
tracking of maternal
health data
Obstetric history, lactation
history, STDs, physical exam
data, laboratory tests, antenatal
progress record, labor and
delivery outcomes, post-natal
progress report, patient
teaching done
When opening the form,
alert midwife if patient due
for malaria prophylaxis or
PMTCT
Family
planning
Form Set
Track family planning
methods and
medication needs
Current and previous method
use, obstetric history, social
history, patient history, STDs,
physical exam, cervical
screening, lab tests, etc.
Patients on oral
contraceptives or IUDs
who need follow-up can be
alerted to CHW or CHN
for outreach.
Child health
Form Set
Tracking child well
care and
immunization needs
Immunizations given,
prophylaxis given, patient
teaching, developmental data
and screenings, malaria
treatment
Alert midwife if
immunizations or
screenings are due
Referral
tracking
Form
Tracking and
reporting of referral
data between health
facilities and district
hospital
Patient information, referral
reason, follow-up results,
referring midwife
Alert midwife when
referral report is available
Registry
Form Sets
Quick entry of
registry data required
for monthly reporting
Fever, PMTCT, ANC,
Deliveries, etc.
Transfer of data to other
forms as appropriate
Table 4.9. Overview of Planned Forms.
The functional requirements and use cases for the patient registration form and the fever
register are shown in Tables 4.10 and 4.11. The barcoding functionality specification was later
removed after brainstorming sessions with the mHealth team when it was determined that
maintenance of printers at health facilities would be cumbersome and unsustainable due to
limited availability of IT staff and printer supplies.
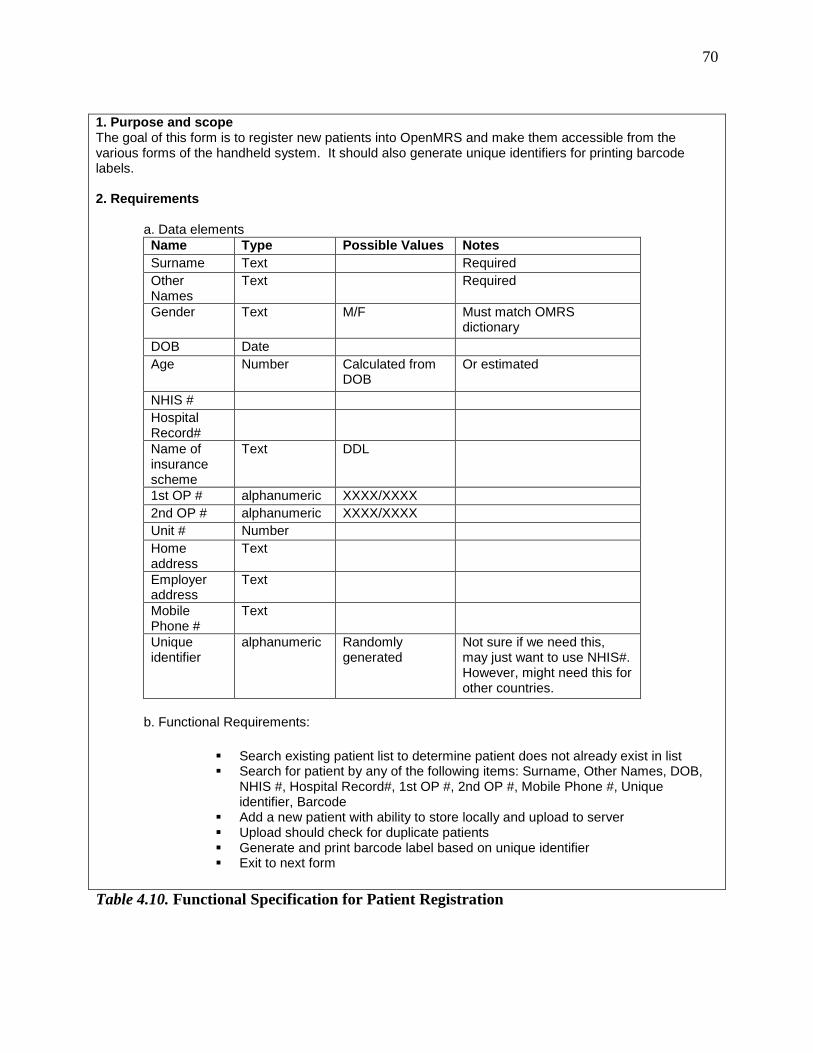
70
1. Purpose and scope The goal of this form is to register new patients into OpenMRS and make them accessible from the various forms of the handheld system. It should also generate unique identifiers for printing barcode labels. 2. Requirements a. Data elements
Name Type Possible Values Notes
Surname Text Required
Other Names
Text Required
Gender Text M/F Must match OMRS dictionary
DOB Date
Age Number Calculated from DOB
Or estimated
NHIS #
Hospital Record#
Name of insurance scheme
Text DDL
1st OP # alphanumeric XXXX/XXXX
2nd OP # alphanumeric XXXX/XXXX
Unit # Number
Home address
Text
Employer address
Text
Mobile Phone #
Text
Unique identifier
alphanumeric Randomly generated
Not sure if we need this, may just want to use NHIS#. However, might need this for other countries.
b. Functional Requirements:
Search existing patient list to determine patient does not already exist in list Search for patient by any of the following items: Surname, Other Names, DOB,
NHIS #, Hospital Record#, 1st OP #, 2nd OP #, Mobile Phone #, Unique identifier, Barcode
Add a new patient with ability to store locally and upload to server Upload should check for duplicate patients Generate and print barcode label based on unique identifier Exit to next form
Table 4.10. Functional Specification for Patient Registration
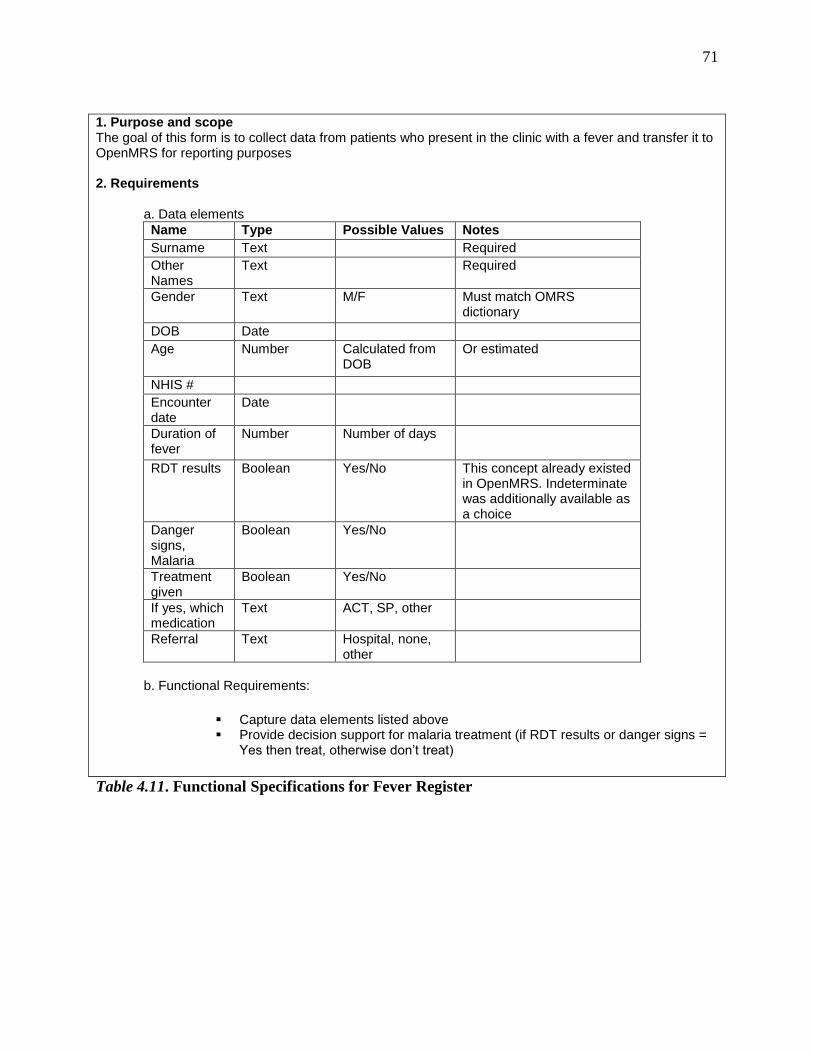
71
1. Purpose and scope The goal of this form is to collect data from patients who present in the clinic with a fever and transfer it to OpenMRS for reporting purposes 2. Requirements a. Data elements
Name Type Possible Values Notes
Surname Text Required
Other Names
Text Required
Gender Text M/F Must match OMRS dictionary
DOB Date
Age Number Calculated from DOB
Or estimated
NHIS #
Encounter date
Date
Duration of fever
Number Number of days
RDT results Boolean Yes/No This concept already existed in OpenMRS. Indeterminate was additionally available as a choice
Danger signs, Malaria
Boolean Yes/No
Treatment given
Boolean Yes/No
If yes, which medication
Text ACT, SP, other
Referral Text Hospital, none, other
b. Functional Requirements:
Capture data elements listed above Provide decision support for malaria treatment (if RDT results or danger signs =
Yes then treat, otherwise don’t treat)
Table 4.11. Functional Specifications for Fever Register
72
Cycle 2. Design Cycle
This cycle also consisted of two phases. In the first phase, mClinic was developed as part
of a coded-in-country initiative. In the second phase, we tested and evaluated the patient
registration and fever register forms of mClinic. We evaluated the usability of mClinic using the
H-ITUES survey and mobile usability heuristics. Our goal was to identify usability issues with
mClinic and refine the functional specifications for further iterative development. The research
questions for this cycle were as follows:
What usability issues exist with the artifact?
What are the deficiencies in functionality or qualities of the artifact that need to be
addressed to improve acceptance?
How does the artifact meet heuristic standards?
Build Phase
Development took place for January through May of 2011. The focus of the
development was on modification of ODK-Clinic so that data could be both sent and retrieved
via XForms. Additionally, a module was developed for OpenMRS to allow for XForms
developed within OpenMRS to be easily incorporated in ODK-Clinic. The OpenMRS XForms
helper module and the modified version of ODK-Clinic are collectively what we refer to as
mClinic.
It has been suggested that coded-in-country development will help support sustainability
of ICT projects in Sub-Saharan Africa by building technology workforce capacity (Dimagi,
2011). However, such an undertaking is not without challenges. Lack of face time and cultural
differences between the Kenyan software team and the mHealth team based in New York likely
contributed to communication errors that slowed the development of the project. Additionally, it
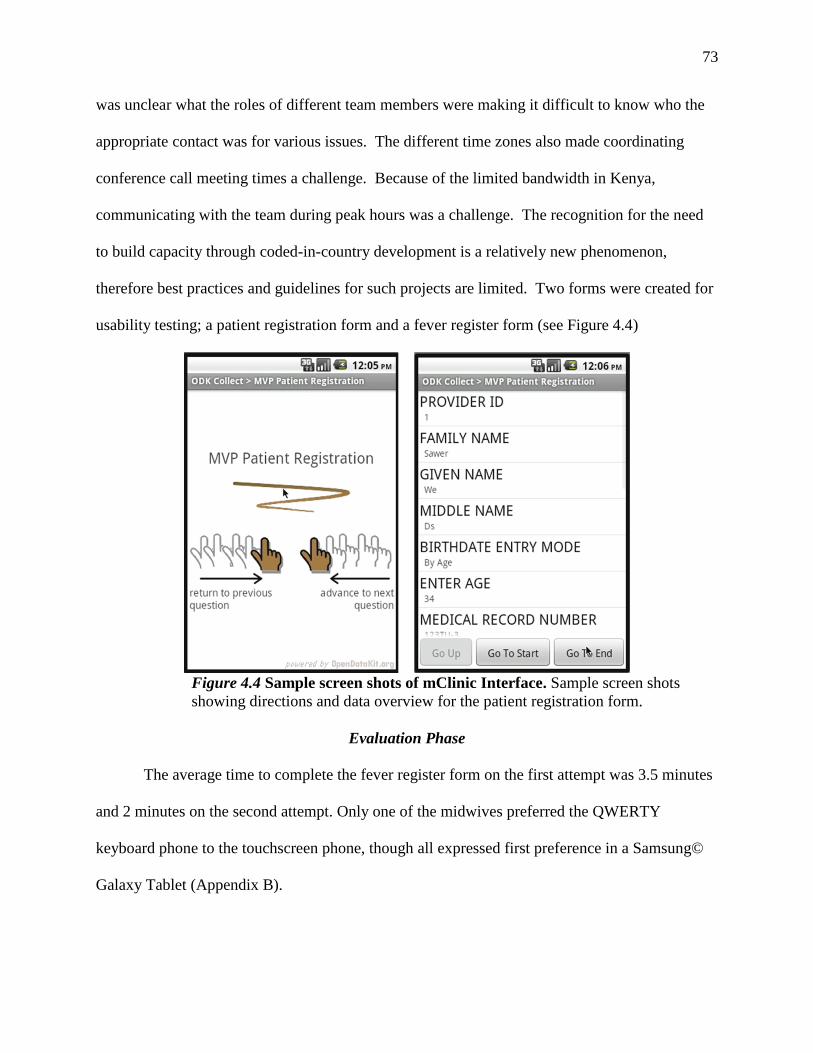
73
was unclear what the roles of different team members were making it difficult to know who the
appropriate contact was for various issues. The different time zones also made coordinating
conference call meeting times a challenge. Because of the limited bandwidth in Kenya,
communicating with the team during peak hours was a challenge. The recognition for the need
to build capacity through coded-in-country development is a relatively new phenomenon,
therefore best practices and guidelines for such projects are limited. Two forms were created for
usability testing; a patient registration form and a fever register form (see Figure 4.4)
Figure 4.4 Sample screen shots of mClinic Interface. Sample screen shots
showing directions and data overview for the patient registration form.
Evaluation Phase
The average time to complete the fever register form on the first attempt was 3.5 minutes
and 2 minutes on the second attempt. Only one of the midwives preferred the QWERTY
keyboard phone to the touchscreen phone, though all expressed first preference in a Samsung©
Galaxy Tablet (Appendix B).
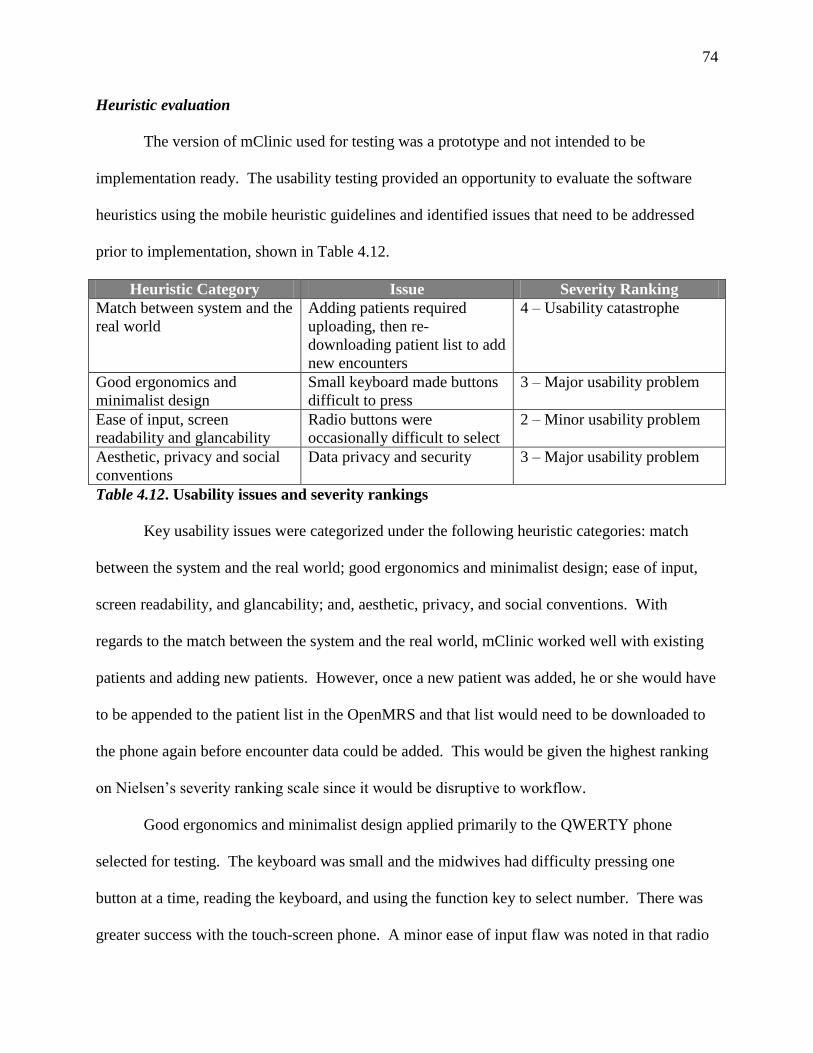
74
Heuristic evaluation
The version of mClinic used for testing was a prototype and not intended to be
implementation ready. The usability testing provided an opportunity to evaluate the software
heuristics using the mobile heuristic guidelines and identified issues that need to be addressed
prior to implementation, shown in Table 4.12.
Heuristic Category Issue Severity Ranking
Match between system and the
real world
Adding patients required
uploading, then re-
downloading patient list to add
new encounters
4 – Usability catastrophe
Good ergonomics and
minimalist design
Small keyboard made buttons
difficult to press
3 – Major usability problem
Ease of input, screen
readability and glancability
Radio buttons were
occasionally difficult to select
2 – Minor usability problem
Aesthetic, privacy and social
conventions
Data privacy and security 3 – Major usability problem
Table 4.12. Usability issues and severity rankings
Key usability issues were categorized under the following heuristic categories: match
between the system and the real world; good ergonomics and minimalist design; ease of input,
screen readability, and glancability; and, aesthetic, privacy, and social conventions. With
regards to the match between the system and the real world, mClinic worked well with existing
patients and adding new patients. However, once a new patient was added, he or she would have
to be appended to the patient list in the OpenMRS and that list would need to be downloaded to
the phone again before encounter data could be added. This would be given the highest ranking
on Nielsen’s severity ranking scale since it would be disruptive to workflow.
Good ergonomics and minimalist design applied primarily to the QWERTY phone
selected for testing. The keyboard was small and the midwives had difficulty pressing one
button at a time, reading the keyboard, and using the function key to select number. There was
greater success with the touch-screen phone. A minor ease of input flaw was noted in that radio
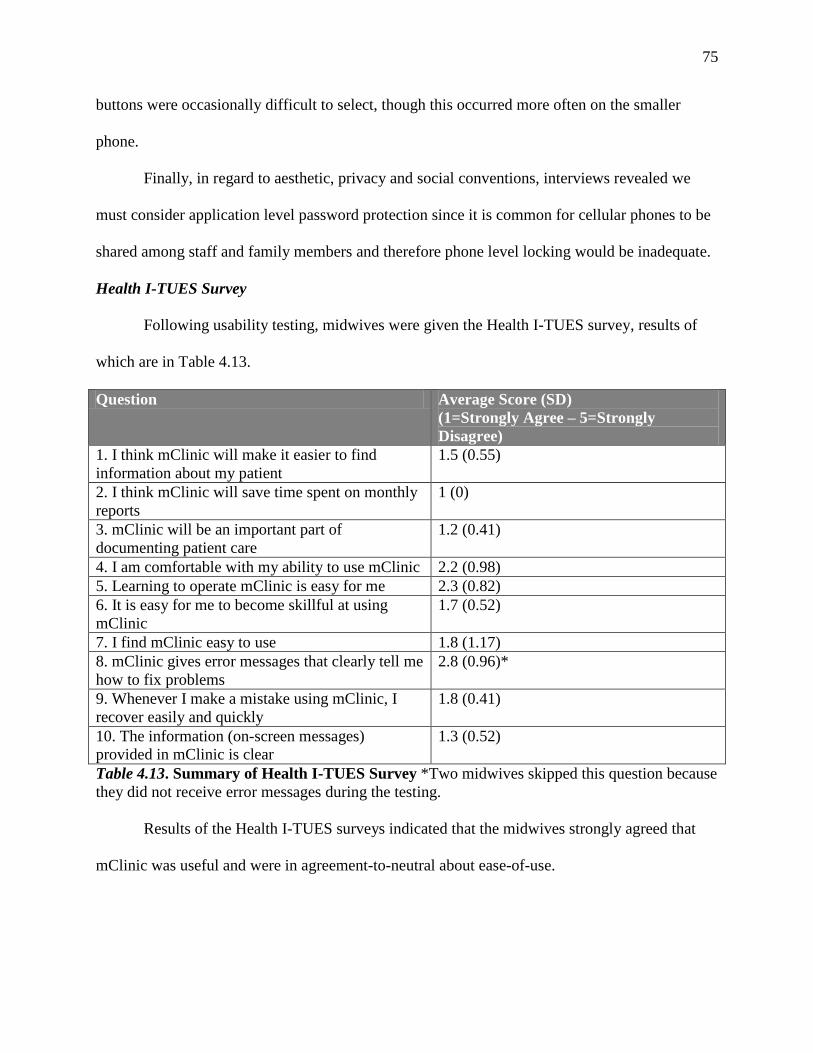
75
buttons were occasionally difficult to select, though this occurred more often on the smaller
phone.
Finally, in regard to aesthetic, privacy and social conventions, interviews revealed we
must consider application level password protection since it is common for cellular phones to be
shared among staff and family members and therefore phone level locking would be inadequate.
Health I-TUES Survey
Following usability testing, midwives were given the Health I-TUES survey, results of
which are in Table 4.13.
Question Average Score (SD)
(1=Strongly Agree – 5=Strongly
Disagree)
1. I think mClinic will make it easier to find
information about my patient
1.5 (0.55)
2. I think mClinic will save time spent on monthly
reports
1 (0)
3. mClinic will be an important part of
documenting patient care
1.2 (0.41)
4. I am comfortable with my ability to use mClinic 2.2 (0.98)
5. Learning to operate mClinic is easy for me 2.3 (0.82)
6. It is easy for me to become skillful at using
mClinic
1.7 (0.52)
7. I find mClinic easy to use 1.8 (1.17)
8. mClinic gives error messages that clearly tell me
how to fix problems
2.8 (0.96)*
9. Whenever I make a mistake using mClinic, I
recover easily and quickly
1.8 (0.41)
10. The information (on-screen messages)
provided in mClinic is clear
1.3 (0.52)
Table 4.13. Summary of Health I-TUES Survey *Two midwives skipped this question because
they did not receive error messages during the testing.
Results of the Health I-TUES surveys indicated that the midwives strongly agreed that
mClinic was useful and were in agreement-to-neutral about ease-of-use.
76
Applicability Checks
Post-testing interviews were consistent with the results of the Health I-TUES survey in
that the midwives indicated that they believed that mClinic will be helpful to them and reduce
time they spend creating monthly reports. Midwife 4 stated: “Look at the number of reporting
formats we have to complete. The end of the month is so hectic for us. If this will help, I will use
it.”
After being shown the low fidelity prototypes, several midwives expressed concern that
the maternal health form set would be too time intensive and cumbersome to use. Midwife 1
stated, “Last week I was up for 48 hours delivering babies, seeing patients, and then more
deliveries. This will be too much. Someone else should do it”.
More positive interest was generated for expanding the register-type forms and
expanding it to capture more monthly reporting data. Midwife 5 stated, “We really need that for
PMTCT, Morbidity and the Midwife Monthly. That would help. I would like to use that.”
Summary
This chapter has provided the results of the two research cycles, Relevance and Design.
The requirements analysis phase of the Relevance cycle found that midwives had heavy patient
burdens, high reporting requirements, and poor access to patient and aggregate data. In the
functional requirements phase we developed a number of use-cases while focusing on the initial
areas of patient registration and prevention and treatment of malaria.
In the design cycle, functional requirements were used to develop the prototype of
mClinic as part of a coded-in-country initiative in the build phase. Results from this process
provide valuable insight to the continuation of this, and other coded-in-country initiatives. In the

77
usability phase we found that the overall usability was high but issues about how to address ease-
of-use remain.
78
CHAPTER 5. DISCUSSION
This chapter summarizes the results of the study and contains a discussion of those results
including addressing the contributions, implications, strengths, limitations, recommendations for
future research, and conclusion.
Summary of Study
The purpose of this study was to design an mHealth application for Midwives in rural
Ghana using the Information Systems Research (ISR) Framework to guide the design science
research process. The first cycle, the relevance cycle, was divided into two phases, requirements
analysis and functional specifications. In the requirements gathering phase we used the design-
actuality gaps model to assess the current system actuality to determine functional requirements
and system qualities. Important gaps were noted between the current system and the desired
future system. In the second phase of the relevance cycle, we developed functional
specifications based on the findings of the first phase and the development of use cases.
In the second research cycle, the design cycle, we developed a prototype of mClinic
through a coded-in-country initiative and then tested its usability. Overall, the midwives rated
mClinic as usable and easy-to-use, though improving midwives technical self-efficacy will be
necessary for implementation success. The applicability checks noted key issues in the
perceived priorities of the designers versus the midwives that should drive future refinement of
the prototype.
Discussion of Results
Numerous policy makers and academics have called for an expanded use of mHealth in
developing countries for facilitating health-related data collection, decision-making, and health
promotion (Gerber, et al., 2010; Mechael, 2009a; Mechael & Sloninsky, 2008; United Nations
79
Foundation, 2010; WHO, 2011b). This case study demonstrated that there remains
considerable work to be done closing the design-actuality gaps for achieving success in mHealth
deployments. The Information Systems Research Framework applies both behavioral and design
science to our understanding, testing, and evaluation of informatics research (Hevner & March,
2003). We will revisit the research cycles of this study to guide the discussion of our results.
Relevance Cycle
Requirements analysis for this research were done by interviewing and observing
midwives and other clinical staff, interviewing key administrative staff, and analyzing current
documentation tools. The results of the requirements analysis can be divided into three
categories which make up the application domain: people, organization, and technology.
People
Through observation and interview, we gained an understanding of the clinical workflow
of the midwives, their roles and responsibilities within the organization, their technical self-
efficacy, their current information practices, and their potential to act as knowledge workers.
The workflow of the midwives presents challenges to the application design. There is no
easy way to share data collected by nurses and midwives during the course of a single visit in
real-time because a continual server connection is not possible for syncing data between mobile
devices. As noted in other work, matching technology to workflow is a key component of HIS
implementation success (Williamson, et al., 2001). Unlike highly structured applications
designed for community health works, mClinic should allow midwives to change seamlessly
between patients and limit forced or controlled data entry (DeRenzi, et al., 2008). The design of
forms will have to be considered carefully as this flexibility can also increase the potential for
inaccurate or incomplete data (Strong, Lee, & Wang, 1997). Midwives may see 30 or more
80
patients in a day, the application should be responsive to the need to quickly add key elements of
data during the visit, move between simultaneous patient visits, providing appropriate decision
support and feedback to relieve cognitive burden, and limit the need to enter long, text-based
narratives.
The midwives had a heavy burden of administrative reporting, as was found in other
studies reviewed in the literature (Mechael, 2009b; Prosser, et al., 2006). Many of the tools used
for reporting contained duplicate data and information particularly those regarding malaria. The
bulk of data entry went into patient’s personal health records (PHR) which remained in
possession of the patient, with the same data duplicated into the various registers. Improving the
quality, accuracy, and accessibility of data collected at the clinics should be a priority.
Data accessibility refers to the ability to access data in a timely manner (Strong, et al.,
1997). The data collected for reporting is inaccessible to midwives. They receive little to no
feedback on the reports that they generate. They are unaware of their quality or productivity in
comparison to their colleagues and they report that they are not given feedback about the overall
health status of the patient population that they are serving. Providing access to aggregated data
on the midwives patient population has the potential to provide them with knowledge to better
serve their communities (Chaudhry, et al., 2006). The Aceh Besar mobile phones for midwives
project found that access to information and resources improves midwives’ self-reported
confidence to solve clinical problems (Chib, 2010). However, just providing information is not
sufficient for evidence-based decision support, it must be integrated into clinical workflow in
order to be effective (Bakken et al., 2008). Furthermore, community health nurses and
midwives should be able to create lists of patients that need follow-up care so that community
outreach efforts can be improved.
81
Overall, the midwives were enthusiastic about learning a new technology and the
potential for mClinic to cut down on their burden of reporting. However, many of the midwives
expressed concern about the additional burden of learning and entering data into the system
would place on them. As noted in the literature review, buy-in from end-users is essential for
project success (Cole-Ceesay, et al., 2010). Previous studies on HIS implementations showed
that requiring system use by withholding pay or other punitive measures is ineffective as a means
of ensuring use and is generally detrimental to project success (Joos, Chen, Jirjis, & Johnson,
2006; Scott, Rundall, Vogt, & Hsu, 2005; van der Meijden, Tange, Troost, & Hasman, 2003).
Proving the value of the mClinic to the midwives will be an essential component of successful
implementation, particularly in the early stages when double documentation is high and return
data value for reporting and measuring outcomes is low.
Information Practices. In this research, we identified a number of information resources
that are needed by the midwives that are not readily available to them. This includes referral and
laboratory data from the district hospital and current guidelines on care practices. A separate
laboratory information system is currently being developed at MVP-Ghana though it remains to
be seen if integrating these separate systems will be successful. Additionally, a telemedicine
center is under implementation at the district hospital site that may aid in obtaining referral data.
Standardization of data formats across these systems is necessary to ensure that data exchange
between them will be possible. For example mClinic and OpenMRS use a common concept
dictionary to facilitate data exchange between the two systems (Kanter, et al., 2009).
Another key issue with information access relates to inadequate knowledge of clinical
practice guidelines and reporting expectations. This was consistent with findings from the
literature on the need for improving knowledge dissemination and continuing education
82
opportunities for midwives in rural Ghana (Dohrn, Miller, & Bakken, 2006; Prosser, et al.,
2006). Furthermore, midwives rely primarily on books for clinical information which have the
potential to be out of date or inappropriate (Musoke, 2000). For the system be successful, more
attention will be needed to ensure the flow of knowledge management between the midwives,
administrative staff at MVP, and the system designers. When the study was initiated, it was
identified that midwives were unaware of current World Health Organization (WHO) practice
guidelines regarding the number of antenatal care visits for a low risk patients. Midwives
verbalized that patients should have twelve visits, while WHO guidelines recommend a
minimum of four visits and GHS only reimburses four visits. To further complicate this matter,
a Cochrane review published after the initiation of this study found that the recommended
reduced visit model was associated with an increase in perinatal mortality, and as a result the
guidelines are currently under reevaluation by WHO (Dowswell et al., 2010; WHO, 2011c).
This emphasizes the importance of the modularity of the system in allowing rapid development
and deployment of new forms congruent with evolving practice guidelines. Previous work has
integrated clinical practice guideline (CPG)-based decision support into documentation tools that
assisted users through screening reminders, diagnosis generation, a tailored care plans (Bakken,
et al., 2008). The tool was found to increase diagnoses related to obesity and decrease missed
diagnoses (Lee et al., 2009). CPG-Based decision support could be applied similarly in our work
User centered methods, such as participant observation and contextual inquiry, proved
very useful in understanding the information uses and needs of the midwives. These methods
have been widely used in developed countries as a means for assessing functional requirements
for tools and software for the elderly because decrease technical knowledge makes participatory
design methods impractical (Lundell & Morris, 2005). Further refinement of user centered
83
methods for determining functional specifications in developing countries may lead to the
creation of more relevant and usable artifacts.
Midwives as Knowledge Workers. The current system of data management and data
flow does not permit midwives to function as knowledge workers. The ability to act as
knowledge workers will allow midwives to recognize patterns amongst patients and
communicate knowledge across the organization to improve clinic care processes and patient
outcomes (Snyder-Halpern, et al., 2001). An important component of mClinic is that it matches
the mental model of the midwives documentation practices. This is important for midwives in
that it will allow them access data that they use in clinical decision making in a format that is
familiar to them. A top goal of mClinic has been to not merely function as a data collection tool,
but as an information resource that allows midwives to apply their domain knowledge to both
individual patient and population data.
Organization
Data Collection. Currently, the key source of patient data is stored in the patient’s PHR.
This will make adding patient historical data into the MGV-Net system nearly impossible as this
data is in ownership of the patient. Paper records kept on site are limited and not easy to search,
as shown in Figure 5.1. The midwives stated that they only search the paper record for
information when the patient comes in without their PHR and that the information there is not
necessarily valuable for their day-to-day practice.
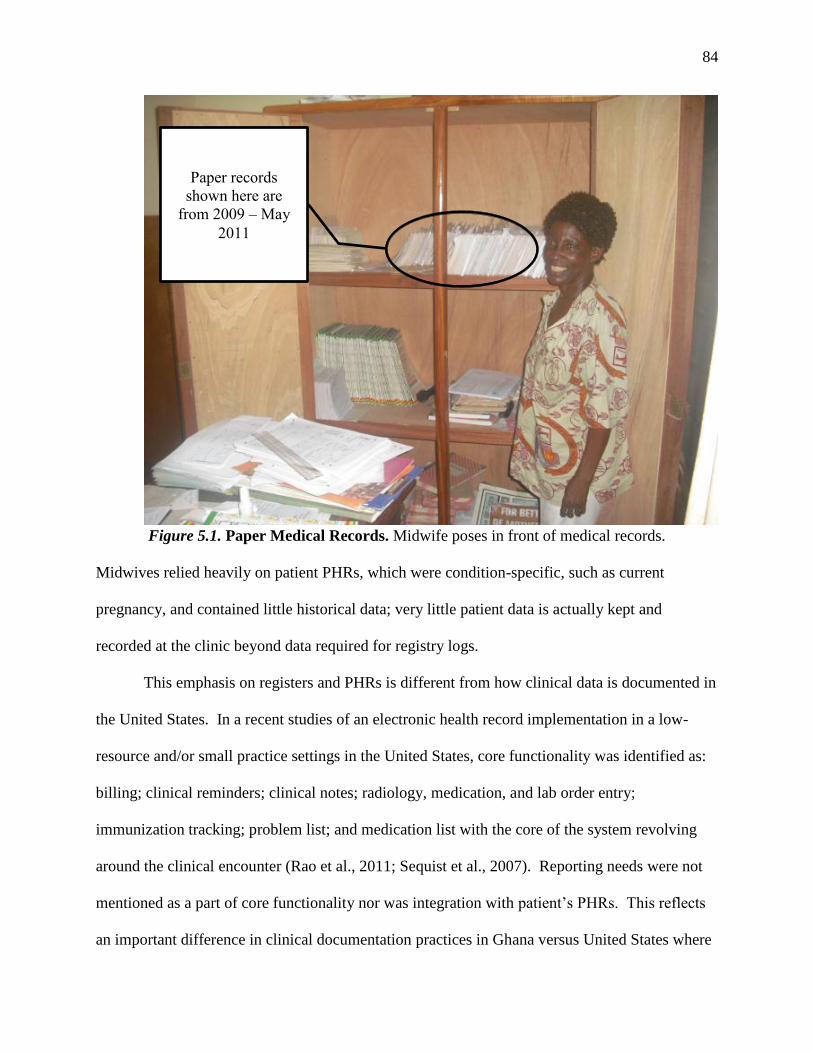
84
Figure 5.1. Paper Medical Records. Midwife poses in front of medical records.
Midwives relied heavily on patient PHRs, which were condition-specific, such as current
pregnancy, and contained little historical data; very little patient data is actually kept and
recorded at the clinic beyond data required for registry logs.
This emphasis on registers and PHRs is different from how clinical data is documented in
the United States. In a recent studies of an electronic health record implementation in a low-
resource and/or small practice settings in the United States, core functionality was identified as:
billing; clinical reminders; clinical notes; radiology, medication, and lab order entry;
immunization tracking; problem list; and medication list with the core of the system revolving
around the clinical encounter (Rao et al., 2011; Sequist et al., 2007). Reporting needs were not
mentioned as a part of core functionality nor was integration with patient’s PHRs. This reflects
an important difference in clinical documentation practices in Ghana versus United States where
Paper records
shown here are
from 2009 – May
2011
85
the burden of reporting falls on administrative staff rather than clinicians and PHRs are not
widely used. If we design the system centering on registry data rather than clinical notes it will
likely be more consistent with the midwives practice while still capturing essential data for
reporting and clinical decision making.
The registry logs contain important information for reporting requirements and could
prove useful as a source of historical data and demographic data if staff could be identified with
adequate skill and time to do the data entry. Registries may also prove an important source of
data for baseline and post-intervention results. While we can add essential data at each visit, it
will be impossible from a staffing and resource perspective to retroactively include past data at
the time of the visit. This means that considerable time will pass before there is enough patient
data in the system to make it useful for evaluating patient outcomes and effectiveness of the
system itself or as a resource for other interventions. This is particularly true because only a few
thousands patients are seen at each facility throughout the year. It is important to keep this
knowledge in mind as there will likely be considerable pressure for outcomes and evaluation
data.
Our goal, at this point, will not be to create a completely paperless system since
widespread adoption of HIS in Ghana is unlikely, paper will still be needed to communicate with
other organizations (Dykstra et al., 2009). Determining the key data elements of data to digitize
should focus on data that is needed to improve health quality and outcomes in the clinics.
Technical Support. Midwives expressed considerable concern about their technical self-
efficacy, which has been found to be an important predictor of technology adoption by clinicians
(Brown & Coney, 1994; Carayon, et al., 2011). Opportunities for improving technical skills
appear to be limited. Extensive on-site support during the initial rollout will likely be required,
86
placing an additional human resource burden on MVP. On-going technical support via the IT
and data staff at the main MVP administrative site may be possible, however, the distance may
prove challenges. Solutions for providing remote support should be investigated. Currently,
there are only two full-time staff members working in the IT department at MVP-Ghana. This
level of staffing will likely be inadequate given the amount of support that the midwives
indicated that they would require.
Technology
Technology, particularly with regards to infrastructure, will remain a limitation to the
deployment of mClinic. During both the first and second site visits, cellular coverage was only
adequate at five of the seven sites. While increasing use of cellular phones and mobile
technology indicate wider technology acceptance, the bandwidth capacity is not keeping pace
with the number of new users. During the first visit, bandwidth was sufficient for making video
calls via Skype and there was only one instance of a network outage in a 14 day period. During
the second visit, eight months later, bandwidth was no longer sufficient for video calling and
there were at least three instances of network outages over a 14 day period. In addition, during
the second trip, the internet connection at the main administrative site, where the OpenMRS
server for this project is housed, was unavailable for three continuous days as well as
occasionally being out of service on other days.
Though ICT infrastructure is expanding rapidly in Sub-Saharan Africa it is not keeping
pace with demand (Gerhan & Mutula, 2007). We must continue to account for low and
unreliable bandwidth in our system design as the issue will not likely be resolved in the near
future.
Design Cycle
87
Build
While our research questions did not include the actual software development process,
the coded-in-country initiative has long-term implications for this and other mHealth and HIS
projects. The long-term sustainability of HIS in Sub-Saharan Africa will not be possible with
building human resource capacity in information technology to support the implementations and
on-going maintenance of the software and equipment.
Usability
Midwives identified usability issues through testing, completion of the Health I-TUES
survey, and post-testing interviews. While the results of the Health I-TUES survey were
generally positive the heuristic evaluation suggests there are still some important usability issues
that need to be addressed prior to implementation. This, however, is to be expected in the first
round of field testing. Some of the heuristic flaws observed, such as frequent typos or difficulty
entering numbers, were related to the hardware selected for the project rather than the software.
This stresses the importance of the careful selection of hardware in addition to the attention and
detail paid to the actual software development.
The Health I-TUES survey proved useful in providing a tool to measure of usability.
Post-test interviews qualified the results of the Health I-TUES survey as midwives were able to
express what features they found easy to use and which they found difficult. As is consistent
with the literature, the midwives preferred when the screen contained less data and did not
require scrolling (Gong & Tarasewich, 2004). Questions regard ability to learn and use the
system were ranked lower than the others. This may be attributed to the midwives low technical
self-efficacy and reinforces the need for hands on training in general technology in addition to
mClinic itself.
88
Applicability
Overall, the midwives indicated that they felt the use cases in development reflected their
clinical practice while some of the prototypes that called for more narrative note documentation
would not be useful to them or too cumbersome to use. They indicated that the need to collect
registry data was a top priority and that electronic documentation of clinic notes may be too
burdensome given their high patient loads. Completing the usability tests prior to the
applicability checks provided a technical baseline whereby the midwives became familiar with
the potential of mobile technology. This allowed the midwives to provide richer feedback on the
functional requirements and use cases developed in this research. This work provides further
evidence to the appropriateness of low-fidelity testing for developing country HIS projects as
proposed by other researchers (Maunder, et al., 2007; Ramachandran, et al., 2007).
Functional Specifications Revisited
The field testing resulted in further refinement of functional specifications. A focus on
registry data, as suggested by the applicability checks, will stream line data collection and be
more suitable to the workflow and mental model of the midwives. Reduction of scrolling and
text based data entry will allow for more rapid form filling and better ease-of-use given the high
patient volume seen by the midwives.
Contributions
This study makes contributions in three areas: information systems theory; user-centered
design methods; and, mHealth for developing countries.
Theory
Few formal studies have used design science research in a developing country context.
Our study provides evidence to the growing body of literature on design science research. We
89
modified the framework from previous researchers proposed use by incorporating earlier field
testing (Hevner, 2007; Iivari, 2007). This research will contribute to the literature on design
science research and help illuminate how design science can be used to improve the quality of
artifacts produces for developing countries.
Methods
At the 2010 mHealth Summit many attendees called for increased use of user centered
design methods in mHealth (Torgan, 2010). Traditional user centered design methods often
assume a baseline understanding of technology that may not be present in a developing country
context (Smith & Dunckley, 2007). Our methods will contribute to the literature on the use of
user-centered design techniques in developing countries. Including low-fidelity prototyping after
testing of mClinic allowed the Midwives to provide us with richer feedback on the applicability
of our application and plans for future work by increasing their technological baseline.
Applicability checks were important in validating the results of the relevance cycle and
providing important information for the refinement of mClinic.
mHealth in Developing Countries
While there has been increased enthusiasm for using mHealth for improving healthcare
infrastructure in Sub-Saharan Africa there is little evidence in the literature to guide design and
implementation of such tools and even less data on their effectiveness (Mechael, 2009a; Tamrat
& Kachnowski, 2011). This work will contribute to the much needed evidence to support
mHealth for development. Furthermore, few mHealth implementations have targeted midwives
despite the important role they play in the rural healthcare systems of Sub-Saharan Africa.
Understanding the distinct needs of midwives, as opposed to other types of clinicians or
90
community health workers, will be an important contribution to building health information
systems infrastructure in Ghana and other parts of Sub-Saharan Africa.
Project Implications
The results of this project stressed the need to alleviate and streamline the midwives
administrative reporting burdens with multiple expected outcomes of improving job satisfaction,
increasing data accuracy, and moving midwives away from passive data collectors into a true
knowledge worker role. Our top priority will be to reduce the redundancy and increase the
quality of malaria data reporting. Additionally, we will continue to improve upon the mClinic
framework so that additional forms can be created and used for other purposes. We are already
in the process of form development for collecting verbal autopsy data. This form will help us
improve the quality of data and better understand the causes of mortality in the Millennium
Village clusters.
General Implications
This research has implications for both informatics and midwifery. We have shown the
utility of design science research for developing countries. Increased usage of design science
research and user centered methods should help decrease the failure rate of health information
systems implementations. Furthermore, even with successful projects, time and money can be
wasted on features that lack utility to end-users. The framework and methods used in this study
may help increase the utility of earlier prototypes resulting in reduced development costs.
The methods used in this work will be of particular interest to those who do research and
development in ICT for developing countries. As noted in the literature review, participatory
design methods assume more familiarity with technology than is commonly found in developing
91
countries (Gitau, et al., 2010). Increased use of contextual inquiry and low-fidelity testing may
result in more relevant artifact development leading to more successful HIS deployments.
Evidence from this study indicates the central role that midwives play in the reporting of
public health data. This role would be considered atypical for clinician from developed
countries. It was clear from the interviews that midwives mental model for documenting patient
care centered on collecting data for reporting registries rather than the collection of narrative
data. Understanding this difference in clinical documentation practices will be important in the
design of any health information system that collects data from midwives in Ghana. As the data
from these reports are needed for aid organizations, it is likely that these findings are
generalizable to other developing countries that depend on foreign aid to support their healthcare
infrastructure. Furthermore, this study directly targeted midwives. Midwives are the largest
group of primary health care providers in Ghana and much of Sub-Saharan Africa yet studies
regarding their information needs and tools supporting their work have been few and limited
(Prosser, et al., 2006; Tamrat & Kachnowski, 2011). Building a continuing body of evidence to
support nurses and midwives in developing countries is a key element to supporting the
healthcare infrastructure where extreme workforce shortages exist.
Strengths
This study had several strengths. First, the framework provided clear guidelines for the
overall study and balanced the research between the behavioral and design science paradigms.
Secondly, nearly all of the requirements data was collected on sites at the clinics and MVP
administrative offices using multiple methods in both the relevance and design cycles. This
allowed for triangulation of our results, improving their credibility and validity. Additionally,
this provided a rich picture for how mClinic could be used and gave greater insight to the
92
cultural and organizational challenges the future implementation might face. Third, interviews
with midwives took place at least once at each site, allowing us to reach our entire target end-
user population.
Limitations
Our study was limited by several factors. Poor recording quality and background noise in
made post-interview analysis challenging. Secondly, the study site, which is part of the
Millennium Villages Project, is a unique initiative that may limit generalizability of the results to
non-MVP clinic sites. Third, only one observer was used to collect data. Additionally there was
some indication that the clinic staff perceived the researcher to have some type of managerial
role within MVP and this may have affected their behavior or willingness to share. Finally, each
phase of the study was conducted in two-week trips. Longer in-country time could have
provided more detailed data, particularly regarding time-specific tasks such as end-of-the month
reporting.
Future Research
Future research on this project will include the continued iterative development of
mClinic using the ISR framework. Additionally, measuring the impact of mClinic post-
implementation on midwives time and job satisfaction and effect on data quality will be an
important component of evaluating its utility. It will be important to measure if use of mClinic
aids midwives ability to conduct knowledge work, improves opportunities for collegial
communication, and contributes to improved perceptions of professionalism. Future studies may
also include patients’ perceptions on how mHealth impacts the quality of care and effects
privacy.

93
Conclusions
Ghana continues to face a critical shortage of midwives, particularly in rural areas. A
multifaceted approach is needed to improve the recruitment and retention of midwives in rural
Ghana. The use of mHealth can provide mechanisms for improving the efficiency and
effectiveness of care provided by midwives while reducing their administrative burdens. The
midwives in our study voiced high levels of frustration regarding reporting requirements and the
lack of feedback, information, and support available to them. mClinic can address some of these
issues; however, careful and thoughtful design is essential for successful implementation,
scalability, and long-term sustainability of the project. This study contributes to the use of
design science research in developing countries. It is imperative that we seek and employ
frameworks and methods for rapidly designing highly useful tools given the limited resources
and increasing health challenges in rural Ghana. Supporting the work of rural Ghanaian
midwives is essential for maintaining the country’s progress towards reduction of maternal
mortality and improves in rural primary healthcare services.
94
REFERENCES
Aheto, D. W., & Gbesemete, K. P. (2005). Rural perspectives on HIV/AIDS prevention: a
comparative study of Thailand and Ghana. Health Policy, 72(1), 25-40. doi:
10.1016/j.healthpol.2004.06.013
Allotey, P. A., & Redipath, D. (2000). Information quality in a remote rural maternity unit in
Ghana. Health policy and planning, 15(2), 170-176. doi: 10.1093/heapol/15.2.170
Alvarez, J., Gil, R., Hernandez, V., & Gil, A. (2009). Factors associated with maternal mortality
in Sub-Saharan Africa: an ecological study. BMC Public Health, 9(1), 462.
Anand, S., & Bärnighausen, T. (2007). Health workers and vaccination coverage in developing
countries: an econometric analysis. The Lancet, 369(9569), 1277-1285. doi:
10.1016/s0140-6736(07)60599-6
Andreatta, P., Gans-Larty, F., Debpuur, D., Ofosu, A., & Perosky, J. Evaluation of simulation-
based training on the ability of birth attendants to correctly perform bimanual
compression as Obstetric first aid. International Journal of Nursing Studies, In Press,
Corrected Proof. doi: 10.1016/j.ijnurstu.2011.03.001
Antrobus, S. (1997). Developing the nurse as a knowledge worker in health--learning the artistry
of practice. J Adv Nurs, 25(4), 829-835.
Apalayine, G. B., & Ehikhamenor, F. A. (1996). The information needs and sources of primary
health care workers in the Upper East Region of Ghana. Journal of information science,
22(5), 367-373. doi: 10.1177/016555159602200505
Aronson, B. (2004). Improving Online Access to Medical Information for Low-Income
Countries. The New England journal of medicine, 350(10), 966-968. doi:
10.1056/NEJMp048009
Asamoah, B. O., Moussa, K. M., Stafstrom, M., & Musinguzi, G. (2011). Distribution of causes
of maternal mortality among different socio-demographic groups in Ghana; a descriptive
study. BMC Public Health, 11, 159. doi: 1471-2458-11-159 [pii]
10.1186/1471-2458-11-159 [doi]
Bakken, S., Currie, L. M., Lee, N. J., Roberts, W. D., Collins, S. A., & Cimino, J. J. (2008).
Integrating evidence into clinical information systems for nursing decision support. Int J
Med Inform, 77(6), 413-420. doi: S1386-5056(07)00162-1 [pii]
10.1016/j.ijmedinf.2007.08.006 [doi]
Bates, D. W., Kuperman, G. J., Wang, S., Gandhi, T., Kittler, A., Volk, L., . . . Middleton, B.
(2003). Ten commandments for effective clinical decision support: making the practice of
evidence-based medicine a reality. Journal of the American Medical Informatics
Association, 10(6), 523-530. doi: 10.1197/jamia.M1370
Bennett, J. (1984). Visual display terminals. Englewood Cliffs, N.J.: Prentice-Hall.
Berg, M. (2001). Implementing information systems in health care organizations: myths and
challenges. International Journal of Medical Informatics, 64(2-3), 143-156. doi:
10.1016/s1386-5056(01)00200-3
Bertini, E., Gabrielli, S., & Kimani, S. (2006). Appropriating and assessing heuristics for mobile
computing (pp. 119).
Best, M. L., & Kumar, R. (2008). Sustainability Failures of Rural Telecenters: Challenges from
the Sustainable Access in Rural India (SARI) Project. Information Technologies and
International Development, 4(4), 31-45. doi: 10.1162/itid.2008.00025
95
Blaya, J. A., Fraser, H. S. F., & Holt, B. (2010). E-Health Technologies Show Promise In
Developing Countries. Health affairs (Millwood, Va.), 29(2), 244-251. doi:
10.1377/hlthaff.2009.0894
Braa, J. (2004). Networks of action: sustainable health information systems across developing
countries. MIS Quarterly, 28(3), 337.
Braa, J., Hanseth, O., Heywood, A., Woinshet, M., & Shaw, V. (2007). Developing health
information systems in developing countries: the flexible standards strategy. MIS
Quarterly, 31(2), 381.
Brooks, F., & Scott, P. (2006). Knowledge work in nursing and midwifery: an evaluation
through computer-mediated communication. Int J Nurs Stud, 43(1), 83-97. doi: S0020-
7489(05)00041-6 [pii]
10.1016/j.ijnurstu.2005.02.003 [doi]
Brown, S. H., & Coney, R. D. (1994). Changes in Physicians' Computer Anxiety and Attitudes
Related to Clinical Information System Use. Journal of the American Medical
Informatics Association, 1(5), 381-394. doi: 10.1136/jamia.1994.95153426
Buabeng, K., Matowe, L., Smith, F., Duwiejua, M., & Enlund, H. (2010). Knowledge of
medicine outlets’ staff and their practices for prevention and management of malaria in
Ghana. Pharmacy World & Science, 32(4), 424-431. doi: 10.1007/s11096-010-
9397-6
Burton, K. R., Howard, A., & Beveridge, M. (2005). Relevance of Electronic Health Information
to Doctors in the Developing World: Results of the Ptolemy Project’s Internet-based
Health Information Study (IBHIS). World journal of surgery, 29(9), 1194-1198. doi:
10.1007/s00268-005-7938-2
Carayon, P., Cartmill, R., Blosky, M. A., Brown, R., Hackenberg, M., Hoonakker, P., . . .
Walker, J. M. (2011). ICU nurses' acceptance of electronic health records. Journal of the
American Medical Informatics Association. doi: 10.1136/amiajnl-2010-000018
Chandler, C., Whitty, C., & Ansah, E. (2010). How can malaria rapid diagnostic tests achieve
their potential? A qualitative study of a trial at health facilities in Ghana. Malaria
Journal, 9(1), 95.
Chandramohan, D., Rodrigues, L., Maude, G., & Hayes, R. (1998). The validity of verbal
autopsies for assessing the causes of institutional maternal death. Stud Fam Plan, 29(4),
414-422. doi: 10.2307/172253
Chaudhry, B., Wang, J., Wu, S., Maglione, M., Mojica, W., Roth, E., . . . Shekelle, P. G. (2006).
Systematic Review: Impact of Health Information Technology on Quality, Efficiency,
and Costs of Medical Care. Annals of internal medicine, 144(10), 742-752.
Chib, A. (2010). The Aceh Besar midwives with mobile phones project: Design and evaluation
perspectives using the information and communication technologies for healthcare
development model. Journal of Computer-Mediated Communication, 15(3), 500-525.
doi: 10.1111/j.1083-6101.2010.01515.x
CIA. (2011). Ghana Retrieved March 2011, from https://www.cia.gov/library/publications/the-
world-factbook/geos/gh.html
Coble, J. M., Maffitt, J. S., Orland, M. J., & Kahn, M. G. (1995). Contextual inquiry: discovering
physicians' true needs. Proc Annu Symp Comput Appl Med Care, 469-473.
Cole-Ceesay, R., Cherian, M., Sonko, A., Shivute, N., Cham, M., Davis, M., . . . Southall, D.
(2010). Strengthening the emergency healthcare system for mothers and children in The
Gambia. Reprod Health, 7, 21. doi: 1742-4755-7-21 [pii]
96
10.1186/1742-4755-7-21 [doi]
Danquah, J. B., Appah, E., Djan, J., Ofori, M., Essegbey, I., & Opoku, S. (1997). Improving
recordkeeping for maternal mortality programs, Kumasi, Ghana. International Journal of
Gynecology and Obstetrics, 59, 149.
DataDyne. (2011). EpiSurveyor, May 2011, from http://www.datadyne.org/episurveyor
de-Graft Aikins, A. (2005). Healer shopping in Africa: new evidence from rural-urban
qualitative study of Ghanaian diabetes experiences. Bmj, 331(7519), 737. doi:
331/7519/737 [pii]
10.1136/bmj.331.7519.737 [doi]
de-Graft Aikins, A., Boynton, P., & Atanga, L. (2010). Developing effective chronic disease
interventions in Africa: insights from Ghana and Cameroon. Globalization and Health,
6(1), 6.
de-Graft Aikins, A., Unwin, N., Agyemang, C., Allotey, P., Campbell, C., & Arhinful, D. (2010).
Tackling Africa's chronic disease burden: from the local to the global. Global Health, 6,
5. doi: 10.1186/1744-8603-6-5 [doi]
Debpuur, C., Welaga, P., Wak, G., & Hodgson, A. (2010). Self-reported health and functional
limitations among older people in the Kassena-Nankana District, Ghana. Glob Health
Action, 3. doi: 10.3402/gha.v3i0.2151 [doi]
DeRenzi, B., Lesh, N., Parikh, T., Sims, C., Maokla, W., Chemba, M., . . . Borriello, G. (2008).
E-imci: improving pediatric health care in low-income countries. Paper presented at the
Proceeding of the twenty-sixth annual SIGCHI conference on Human factors in
computing systems, Florence, Italy.
Dimagi. (2011). Coded in Country Retrieved July 2011, from
http://www.dimagi.com/collaborate/coded-in-country/
Dohrn, J., Miller, N., & Bakken, S. (2006). Assessment of South African nurse-midwives'
knowledge pre- and post-short-term training in antiretroviral treatment. J Assoc Nurses
AIDS Care, 17(4), 46-49. doi: 10.1016/j.jana.2006.05.001 [doi]
Donkor, N. T., & Andrews, L. D. (2011). 21st century nursing practice in Ghana: challenges and
opportunities. International Nursing Review, 58(2), 218-224. doi: 10.1111/j.1466-
7657.2010.00856.x
Dorflinger, J., & Gross, T. (2010). Mobile HCI and technical ICTD: a methodological
perspective. Paper presented at the Proceedings of the 12th international conference on
Human computer interaction with mobile devices and services, Lisbon, Portugal.
Dowswell, T., Carroli, G., Duley, L., Gates, S., Gülmezoglu, A. M., Khan-Neelofur, D., &
Piaggio Gilda, G. P. (2010). Alternative versus standard packages of antenatal care for
low-risk pregnancy. Cochrane Database of Systematic Reviews, (10). Retrieved from
http://www.mrw.interscience.wiley.com/cochrane/clsysrev/articles/CD000934/frame.htm
l doi:10.1002/14651858.CD000934.pub2
Duda, R., Anarfi, J., Adanu, R., Seffah, J., Darko, R., & Hill, A. (2011). The Health of the
“Older Women” in Accra, Ghana: Results of the Women’s Health Study of Accra.
Journal of Cross-Cultural Gerontology, 1-16. doi: 10.1007/s10823-011-9148-8
Dykstra, R. H., Ash, J. S., Campbell, E., Sittig, D. F., Guappone, K., Carpenter, J., . . .
McMullen, C. (2009). Persistent paper: the myth of "going paperless". AMIA Annu Symp
Proc, 2009, 158-162.
Ede, C., Sousa, S., Dhaliwal, H., & Munait, W. (2011). HIV/AIDS in Ghana and South Africa.
In A. Kumar & A. Scott (Eds.), Governance, Social and Physical Infrastructure, and
97
Development: Department of Economics, University of Victoria. Retrieved from
http://web.uvic.ca/~kumara/econ329/329%5B1%5D.pdf#page=107.
Finn, C. P. (2001). Autonomy: an important component for nurses' job satisfaction. International
Journal of Nursing Studies, 38(3), 349-357. doi: 10.1016/s0020-7489(00)00065-1
Fofie, C., & Baffoe, P. (2010). A two-year review of uterine rupture in a regional hospital.
Ghana Med J, 44(3), 98-102.
Fraser, H. S., & Blaya, J. (2010). Implementing medical information systems in developing
countries, what works and what doesn't. AMIA Annu Symp Proc, 2010, 232-236.
Friedman, C. P. (1995). Where's the science in medical informatics? J Am Med Inform Assoc,
2(1), 65-67.
Fullerton, J. T., Johnson, P. G., Thompson, J. B., & Vivio, D. (2011). Quality considerations in
midwifery pre-service education: Exemplars from Africa. Midwifery, 27(3), 308-315. doi:
10.1016/j.midw.2010.10.011 [doi]
Gerber, T., Olazabal, V., Brown, K., & Pablos-Mendez, A. (2010). An Agenda For Action On
Global E-Health. Health Aff, 29(2), 233-236. doi: 10.1377/hlthaff.2009.0934
Gerein, N., Green, A., & Pearson, S. (2006). The Implications of Shortages of Health
Professionals for Maternal Health in Sub-Saharan Africa. Reproductive Health Matters,
14(27), 40-50. doi: 10.1016/s0968-8080(06)27225-2
Gerhan, D., & Mutula, S. M. (2007). Testing a recent model of ICT in development: Botswana
and its university. Information technology for development, 13(2), 177-197. doi:
10.1002/itdj.20060
Ghana Statistical Services, Ghana Health Service, & Macro International. (2009). Ghana
Maternal Health Survey 2007. Calverton, MD, USA.
Gitau, S., Mardsen, G., & Donner, J. (2010). After access - Challenges facing mobile-only
internet users in the developing world. Paper presented at the CHI 2010, Atlanta, GA,
USA.
Gong, J., & Tarasewich, P. (2004). Guidelines for handheld mobile device interface design.
Paper presented at the 35th Decision Science Institute Annual Meeting, Boston, MA.
Gordon, A. N., & Hinson, R. E. (2007). Towards a sustainable framework for computer based
health information systems (CHIS) for least developed countries (LDCs). International
journal of health care quality assurance, 20(6), 532-544. doi:
10.1108/09526860710819468
Gould, J. D., & Lewis, C. (1985). Designing for usability: key principles and what designers
think. Commun. ACM, 28(3), 300-311. doi: 10.1145/3166.3170
Greenemeier, L. (2011). Aqua plan: Could cell phones help aid workers ensure Haiti's supply of
clean drinking water? Scientific American.
Gregg, D. G., Kulkarni, U. R., & Vinze, A. S. (2001). Understanding the Philosophical
Underpinnings of Software Engineering Research in Information Systems. Information
Systems Frontiers, 3(2), 169-183.
Gregor, S., & Jones, D. (2007). The Anatomy of a Design Theory. Journal of the Association for
Information Systems(Forthcoming).
Hawari, A., & Heeks, R. Y. (2010). Explaining ERP failure in a developing country: a Jordanian
case study. Journal of Enterprise Information Managment, 23(2). doi:
10.1108/17410391011019741
98
Heeks, R. (2002). Information Systems and Developing Countries: Failure, Success, and Local
Improvisations. The Information society, 18(2), 101-112. doi:
10.1080/01972240290075039
Heeks, R. (2006). Health information systems: Failure, success and improvisation. International
Journal of Medical Informatics, 75(2), 125-137. doi: 10.1016/j.ijmedinf.2005.07.024
Heeks, R. (2008). ICT4D 2.0: The Next Phase of Applying ICT for International Development.
Computer, 41(6), 26-33.
Heukleman, D. (2006). Can a user centred approach to designing a user interface for rural
communities be successful? Paper presented at the CHI-SA, Cape Town, South Africa.
Hevner, A. R. (2007). A three cycle view of design science research. Scandinavian journal of
information systems, 19(2).
Hevner, A. R., & Chatterjee, S. (2010). Design Research in Information Systems: Theory and
Practice (Vol. 22). New York, NY: SpringerLink.
Hevner, A. R., & March, S. T. (2003). The information systems research cycle. Computer,
36(11), 111-113.
Hevner, A. R., March, S. T., Park, J., & Ram, S. (2004). Design Science in Information Systems
Research. MIS Quarterly, 28(1), 75-105.
HIV InSite. (2011). Ghana: Comprehensive Indicator Report Retrieved July 2011, from
http://hivinsite.ucsf.edu/global?page=cr09-gh-00&post=19&cid=GH
Ho, M. R., Smyth, T. N., Kam, M., & Dearden, A. (2009). Human-Computer Interaction for
Development: The Past, Present, and Future. Information Technologies and International
Development, 5(4), 1-18.
Hogan, M. C., Foreman, K. J., Naghavi, M., Ahn, S. Y., Wang, M., Makela, S. M., . . . Murray,
C. J. L. (2010). Maternal mortality for 181 countries, 1980-2008: a systematic analysis of
progress towards Millennium Development Goal 5. The Lancet, 375(9726), 1609-1623.
doi: 10.1016/s0140-6736(10)60518-1
Iivari, J. (2007). A paradigmatic analysis of information systems as a design science.
Scandinavian journal of information systems, 19(2), 5.
International Development Research Center. (2009). ENACQKT: Enhancing Nurses Access for
Care Quality and Knowledge Through Technology Retrieved January 2011, from
http://www.idrc.org.sg/waterdemand/ev-139858-201-1-DO_TOPIC.html
International Telecommunication Union. (2009). Information Society Statistical Profiles 2009:
Africa.
ISO. (2011). Systems and Software Quality Requirements and Evaluation (SQUARE): ISO
25010.
Istepanian, R., Laxminarayan, S., & Pattichis, C. S. (Eds.). (2006). M-health: Emerging mobile
health systems. New York, N.Y.: Springer.
James, J., & Versteeg, M. (2007). Mobile phones in Africa: how much do we really know?
[10.1007/s11205-006-9079-x]. Social Indicators Research, 84(1), 117-126.
Johnson, F. A., & Madise, N. J. (2011). Targeting women at risk of unintended pregnancy in
Ghana: Should geography matter? Sexual & Reproductive Healthcare, 2(1), 29-35. doi:
10.1016/j.srhc.2010.10.003
Jones, M., & Marsden, G. (2006). Mobile Interaction Design. West Sussex, England: John Wiley
& Sons, Ltd.
99
Joos, D., Chen, Q., Jirjis, J., & Johnson, K. B. (2006). An electronic medical record in primary
care: Impact on satisfaction, work efficiency and clinic processes. Paper presented at the
AMIA Annu Symp Proc. 2006.
Kanter, A. S., Negin, J., Olayo, B., Bukachi, F., Johnson, E., & Sachs, S. E. (2009). Millennium
Global Village-Net: Bringing together Millennium Villages throughout sub-Saharan
Africa. International Journal of Medical Informatics, 78(12), 802-807. doi: DOI:
10.1016/j.ijmedinf.2009.08.002
Kapiriri, L., & Bondy, S. J. (2006). Health practitioners' and health planners' information needs
and seeking behavior for decision making in Uganda. Int J Med Inform, 75(10-11), 714-
721.
Kaplan, B. (1997). Addressing Organizational Issues into the Evaluation of Medical Systems.
Journal of the American Medical Informatics Association, 4(2), 94-101. doi:
10.1136/jamia.1997.0040094
Kaplan, W. A. (2006). Can the ubiquitous power of mobile phones be used to improve health
outcomes in developing countries? Globalization and Health, 2(9). doi: 10.1186/1744-
8603-2-9
Kelloway, E. K., & Barling, J. (2000). Knowledge work as organizational behavior.
International Journal of Management Reviews, 2(3), 287-304. doi: 10.1111/1468-
2370.00042
Khalil, D. D. (2006). Experiences of Teaching Nursing in Four Countries. Nursing Forum, 41(2),
88-94. doi: 10.1111/j.1744-6198.2006.00042.x
Kimaro, H. C., & Titlestad, O. H. (2008). Challenges of user participation in the design of a
computer based system: the possibility of participatory customisation in low income
countries. Journal of Health Informatics in Developing Countries, 2(1).
Kinkade, S., & Verclas, K. (2008). Connecting health clinics and remote health works (Uganda),
Case study 2 Wireless Technology for Social Change: Trends in mobile use by NGOs:
UN Foundation, Vodafone Group Foundation. Retrieved from
http://www.mhealthinfo.org/project/uganda-health-information-network-uhin.
Kober, K., & Van Damme, W. (2004). Scaling up access to antiretroviral treatment in southern
Africa: who will do the job? The Lancet, 364(9428), 103-107. doi: Doi: 10.1016/s0140-
6736(04)16597-5
LaFraniere, S. (2005). Cell phone frenzy in Africa, world's top growth market, The San Diego
Union Tribune. Retrieved from
http://www.signonsandiego.com/uniontrib/20050826/news_1n26phones.html
Lalji, Z., & Good, J. (2008). Designing new technologies for illiterate populations: A study in
mobile phone interface design. Interacting with Computers, 20(6), 574-586. doi:
10.1016/j.intcom.2008.09.002
Lang, T. (2011). Advancing Global Health Research Through Digital Technology and Sharing
Data. Science, 331(6018), 714-717. doi: 10.1126/science.1199349
Lee, N. J., Chen, E. S., Currie, L. M., Donovan, M., Hall, E. K., Jia, H., . . . Bakken, S. (2009).
The effect of a mobile clinical decision support system on the diagnosis of obesity and
overweight in acute and primary care encounters. ANS Adv Nurs Sci, 32(3), 211-221. doi:
10.1097/ANS.0b013e3181b0d6bf [doi]
Leshabari, S., Blystad, A., de Paoli, M., & Moland, K. (2007). HIV and infant feeding
counselling: challenges faced by nurse-counsellors in northern Tanzania. Human
Resources for Health, 5(1), 18.
100
Lim, J. L., Yih, Y., Gichunge, C., Tierney, W. M., Le, T. H., Zhang, J., . . . Mamlin, J. J. (2009).
The AMPATH Nutritional Information System: Designing a Food Distribution Electronic
Record System in Rural Kenya. Journal of the American Medical Informatics
Association, 16(6), 882-888. doi: 10.1197/jamia.M3139
Littlejohns, P., Wyatt, J. C., & Garvican, L. (2003). Evaluating computerised health information
systems: hard lessons still to be learnt. Bmj, 326(7394), 860-863. doi:
10.1136/bmj.326.7394.860
Lundell, J., & Morris, M. (2005). Tales, Tours, Tools, and Troupes: A Tiered Research Method
to Inform Ubiquitous Designs for the Elderly. In S. Fincher, P. Markopoulos, D. Moore
& R. Ruddle (Eds.), People and Computers XVIII - Design for Life (Vol. 4). London:
Springer-Verlag.
March, S. T., & Smith, G. F. (1995). Design and natural science research on information
technology. Decision Support Systems, 15(4), 251-266.
Marshall, S. J. (2004). Developing countries face double burden of disease. Bulletin of the World
Health Organization, 82, 556-556.
Martikainen, S., Ikavalko, P., & Korpela, M. (2010). Participatory interaction design in user
requirements specification in healthcare. Stud Health Technol Inform, 160(Pt 1), 304-308.
Martinez, A., Villarroel, V., Seoane, J., & del Pozo, F. (2005). Analysis of information and
communication needs in rural primary health care in developing countries. IEEE Trans
Inf Technol Biomed, 9(1), 66-72.
Maunder, A., Marsden, G., Gruijters, D., & Blake, E. (2007). Designing interactive systems for
the developing world - reflections on user-centred design. Paper presented at the
Information and Communication Technologies and Development, 2007. ICTD 2007.,
Bangalore, India.
Mechael, P. N. (2009a). The Case for mHealth in Developing Countries. Innovations:
Technology, Governance, Globalization, 4(1), 103-118. doi:
doi:10.1162/itgg.2009.4.1.103
Mechael, P. N. (2009b). MoTECH: mHealth Ethnography Report: Dodwa Health Research
Center.
Mechael, P. N., Douglas, G., Lesh, N., & Kwan, A. (2009). Mobile point-of-care support and
data collection tools for health workers in low- and middle-income countries. Paper
presented at the AMIA Spring Congress, Orlando, FL.
Mechael, P. N., Nemser, B., & Kanter, A. S. (2010). MGV-Net Consolidated Study Design: The
Earth Institute at Columbia University.
Mechael, P. N., & Sloninsky, D. (2008). Toward the Development of an mHealth Strategy: A
Literature Review: World Health Organization.
mHealth Alliance. (2010). Frequently Asked Questions, 2011, from
http://www.mhealthalliance.org/about/frequently-asked-questions
Montoya, I. D., & Carlson, J. W. (1996). Point-of-care systems, informatics, and health care
delivery. The Health care supervisor, 15(2), 17-26.
Musoke, M. G. (2000). Information and its value to health workers in rural Uganda: a qualitative
perspective. Health Libr Rev, 17(4), 194-202.
Musoke, M. G. (2002). Maternal health care in rural Uganda: Leveraging traditional and modern
knowledge systems. IK Notes, 40.
101
NGO Connect Africa Network. (2011). EReadiness: Self Assessment Tool for NGOs Retrieved
March 2011, from
http://ngopedia.org/wiki/EReadiness:Self_Assessment_Tool_for_NGOs
Nguyen, H. T., Rajkotia, Y., & Wang, H. (2011). The financial protection effect of Ghana
National Health Insurance Scheme: evidence from a study in two rural districts. Int J
Equity Health, 10, 4. doi: 10.1186/1475-9276-10-4 [doi]
Nielsen, J. (2003). Usability 101: Introduction to Usability, 2011, from
http://www.useit.com/alertbox/20030825.html
ODK Team. (2011). OpenDataKit Retrieved July 2011, from http://opendatakit.org/
OpenXData. (2011). OpenXData Retrieved May 2011
Ordi, J., Ismail, M. R., Carrilho, C., Romagosa, C., Osman, N., Machungo, F., . . . Menéndez, C.
(2009). Clinico-Pathological Discrepancies in the Diagnosis of Causes of Maternal Death
in Sub-Saharan Africa: Retrospective Analysis. PLoS Med, 6(2), e1000036.
Orr, K. (1981). Structured Requirements Definition. Topeka, KA: K. Orr and Associates.
Ozbolt, J. G., & Graves, J. R. (1993). Clinical nursing informatics. Developing tools for
knowledge workers. Nurs Clin North Am, 28(2), 407-425.
Pakenham-Walsh, N., Priestly, C., & Smith, R. (1997). Meeting the information needs of health
workers in developing countries. BMJ, 314(7074), 90.
Patel, V. L., & Kaufman, D. R. (1998). A case for medical informatics as a local science of
design. Journal of the American Medical Informatics Association, 5(6), 489-492. doi:
10.1136/jamia.1998.0050489
Pierce, L. L., Hazel, C. M., & Mion, L. C. (1996). Effect of a professional practice model on
autonomy, job satisfaction and turnover. Nursing Management, 27(2), 48M-48M.
Potter, P., Wolf, L., Boxerman, S., Grayson, D., Sledge, J., Dunagan, C., & Evanoff, B. (2005).
An Analysis of Nurses' Cognitive Work: A New Perspective for Understanding Medical
Errors Findings). doi: NBK20475 [bookaccession]
Prosser, M., Sonneveldt, E., Hamilton, M., Menottie, E., & Davis, P. (2006). The Emerging
Midwifery Crisis in Ghana: mapping of Midwives and Service Availability Highlights
Gaps in Maternal Care POLICY Project. Washington, DC: USAID.
Purao, S. (2002). Design Research in the Technology of Information Systems: Truth or Dare (pp.
48). State College Penn and Atlanta Ga: The Pennsylvania State University and State
Georgia State University.
Ramachandran, D., Kam, M., Chiu, J., Canny, J., & Frankel, J. F. (2007). Social dynamics of
early stage co-design in developing regions. Paper presented at the SIGCHI conference
on Human factors in computing systems, San Jose, California, USA.
Rao, S. R., DesRoches, C. M., Donelan, K., Campbell, E. G., Miralles, P. D., & Jha, A. K.
(2011). Electronic health records in small physician practices: availability, use, and
perceived benefits. Journal of the American Medical Informatics Association, 18(3), 271-
275. doi: 10.1136/amiajnl-2010-000010
Rosemann, M., & Vessey, I. (2008). Toward improving the relevance of information systems
research to practice: the role of applicability checks. [Article]. MIS Quarterly, 32(1), 1-
22.
Rotich, J. K., Hannan, T. J., Smith, F. E., Bii, J., Odero, W. W., Vu, N., . . . Tierney, W. M.
(2003). Installing and Implementing a Computer-based Patient Record System in Sub-
Saharan Africa: The Mosoriot Medical Record System. Journal of the American Medical
Informatics Association, 10(4), 295-303. doi: 10.1197/jamia.M1301

102
Scott, J. T., Rundall, T. G., Vogt, T. M., & Hsu, J. (2005). Kaiser Permanente's experience of
implementing an electronic medical record: a qualitative study. Bmj, 331(7528), 1313-
1316. doi: 10.1136/bmj.38638.497477.68
Sehlhorst, S. (2006). Foundation Series: Structured Requirements Retrieved June 2011, from
http://tynerblain.com/blog/2006/01/04/foundation-series-structured-requirements/
Sequist, T. D., Cullen, T., Hays, H., Taualii, M. M., Simon, S. R., & Bates, D. W. (2007).
Implementation and use of an electronic health record within the Indian Health Service. J
Am Med Inform Assoc, 14(2), 191-197. doi: M2234 [pii]
10.1197/jamia.M2234 [doi]
Sherwani, J., Ail, N., Tongia, R., Rosenfield, R., Memon, Y., Karim, M., & Pappas, G. (2007).
HealthLine: Speech-based Access to Health Information by Low-literate Users. Paper
presented at the IEEE/ACM Int'l Conference on Information and Communication
Technologies and Development, Bangalore, India.
Simon, H. A. (1996). The Sciences of the Artificial (3rd ed.). Cambridge, Mass.: MIT Press.
Smith, A., & Dunckley, L. (2007). Issues for Human-Computer Interaction in Developing
Countries. Paper presented at the CHI 2007, San Jose, CA, USA.
Snow, R. C., Asabr, K., Mutumba, M., Koomson, E., Gyan, K., Dzodzomenyo, M., . . .
Kwansah, J. (2011). Key factors leading to reduced recruitment and retention of health
professionals in remote areas of Ghana: a qualitative study and proposed policy solutions.
Human Resources for Health, 9(1), 13. doi: 10.1186/1478-4491-9-13
Snyder-Halpern, R., Corcoran-Perry, S., & Narayan, S. (2001). Developing clinical practice
environments supporting the knowledge work of nurses. Comput Nurs, 19(1), 17-23; quiz
24-16.
Sorrells-Jones, J., & Weaver, D. (1999). Knowledge Workers and Knowledge-Intense
Organizations, Part 1: A Promising Framework for Nursing and Healthcare. The Journal
of Nursing Administration, 29(7/8), 12-18.
Sorrells-Jones, J., & Weaver, D. (1999). Knowledge workers and Knowledge-intense
organizations, Part 3: Implications for preparing healthcare professionals. The Journal of
Nursing Administration, 29(10), 14.
Speybroeck, N., Kinfu, Y., Dal Poz, M. R., & Evans, D. B. (2006). Reassessing the relationship
between human resources for health, intervention coverage and health outcomes The
World Health Report. Geneva: World Health Organization.
Strong, D. M., Lee, Y. W., & Wang, R. Y. (1997). Data quality in context. Commun. ACM,
40(5), 103-110. doi: 10.1145/253769.253804
Talley, B. (2006). Nurses and nursing education in Ghana: creating collaborative opportunities.
International Nursing Review, 53(1), 47-51. doi: 10.1111/j.1466-7657.2006.00431.x
Tamrat, T., & Kachnowski, S. (2011). Special Delivery: An Analysis of mHealth in Maternal
and Newborn Health Programs and Their Outcomes Around the World. Maternal and
Child Health Journal, 1-10. doi: 10.1007/s10995-011-0836-3
Taylor, J. E. (1992). Life-saving skills training for midwives: report on the Ghanaian experience.
International Journal of Gynecology & Obstetrics, 38(Supplement 1), S41-S43. doi:
10.1016/0020-7292(92)90029-i
The World Bank. (2011). Data Catalog - Ghana Retrieved June 2011, from
http://data.worldbank.org/country/ghana

103
Tomasi, E., Facchini, L., & Santos Maia, M. d. F. (2004). Health information technology in
priamary health care in developing countries: a literature review. Bulletin of the World
Health Organization, 82(11). doi: 10.1590/S0042-96862004001100012
Torgan, C. (2010). mHealth Summit 2010: A context check list Retrieved July 2011, from
http://www.caroltorgan.com/mhealth-summit-2010-context-check-list/
Toyama, K., & Muneeb, A. (2009). Computing for global development: is it computer science
research? Computer communication review, 39(5), 40.
Trudell, B. (2009). Local-language literacy and sustainable development in Africa. International
Journal of Educational Development, 29(1), 73-79. doi: 10.1016/j.ijedudev.2008.07.002
UNAIDS. (2010). UNAIDS report on the global AIDS epidemic 2010.
UNICEF. (2010). Ghana Statistics Retrieved March 2011, from
http://www.unicef.org/infobycountry/ghana_statistics.html
United Nations. (2000). United Nations Millennium Declaration.
United Nations Foundation. (2010). mHealth for the Developing World. New York: United
Nations.
UsabilityNet. (1998). ISO 9241-11: Guidance on Usability Retrieved July 2011, from
http://www.usabilitynet.org/tools/r_international.htm#9241-11
Vaishnavi, V., & Kuechler, W. (2004, August 16, 2009). Design Research in Information
Systems Retrieved March 2011, from http://desrist.org/design-research-in-information-
systems
Van Belle, J. P. (2009). Building an E-readiness Self-Assessment Tool for NGOs: an African
Experience Paper presented at the 7th Annual Conference on Information Science and
Technology Management, New Delhi, India.
van der Meijden, M. J., Tange, H. J., Troost, J., & Hasman, A. (2003). Determinants of Success
of Inpatient Clinical Information Systems: A Literature Review. Journal of the American
Medical Informatics Association, 10(3), 235-243. doi: 10.1197/jamia.M1094
Venkatesh, V., Morris, M. G., Davis, G. B., & Davis, F. D. (2003). User acceptance of
information technology: Toward a unified view. MIS Quarterly, 27(3), 425-478.
Walsham, G., & Sahay, S. (2006). Research on information systems in developing countries:
Current landscape and future prospects<FN>Ramiro Montealegre was the accepting
Associate Editor for this paper </FN>. [Article]. Information technology for development,
12(1), 7-24. doi: 10.1002/itdj.20020
Ward, S. F., & Kozakowski, J. L. (1987). The Nurse as the Knowledge Worker: A Management
Challenge. AORN, 46(5), 896-897, 900-903. doi: 10.1016/s0001-2092(07)67412-2
Waters, E., Rafter, J., Douglas, G. P., Bwanali, M., Jazayeri, D., & Fraser, H. S. (2010).
Experience implementing a point-of-care electronic medical record system for primary
care in Malawi. Stud Health Technol Inform, 160(Pt 1), 96-100.
Were, M. C., Emenyonu, N., Achieng, M., Shen, C., Ssali, J., Masaba, J. P. M., & Tierney, W.
M. (2010). Evaluating a scalable model for implementing electronic health records in
resource-limited settings. Journal of the American Medical Informatics Association,
17(3), 237.
Whitty, C. J., Chandler, C., Ansah, E., Leslie, T., & Staedke, S. G. (2008). Deployment of ACT
antimalarials for treatment of malaria: challenges and opportunities. Malar J, 7 Suppl 1,
S7. doi: 10.1186/1475-2875-7-S1-S7 [doi]
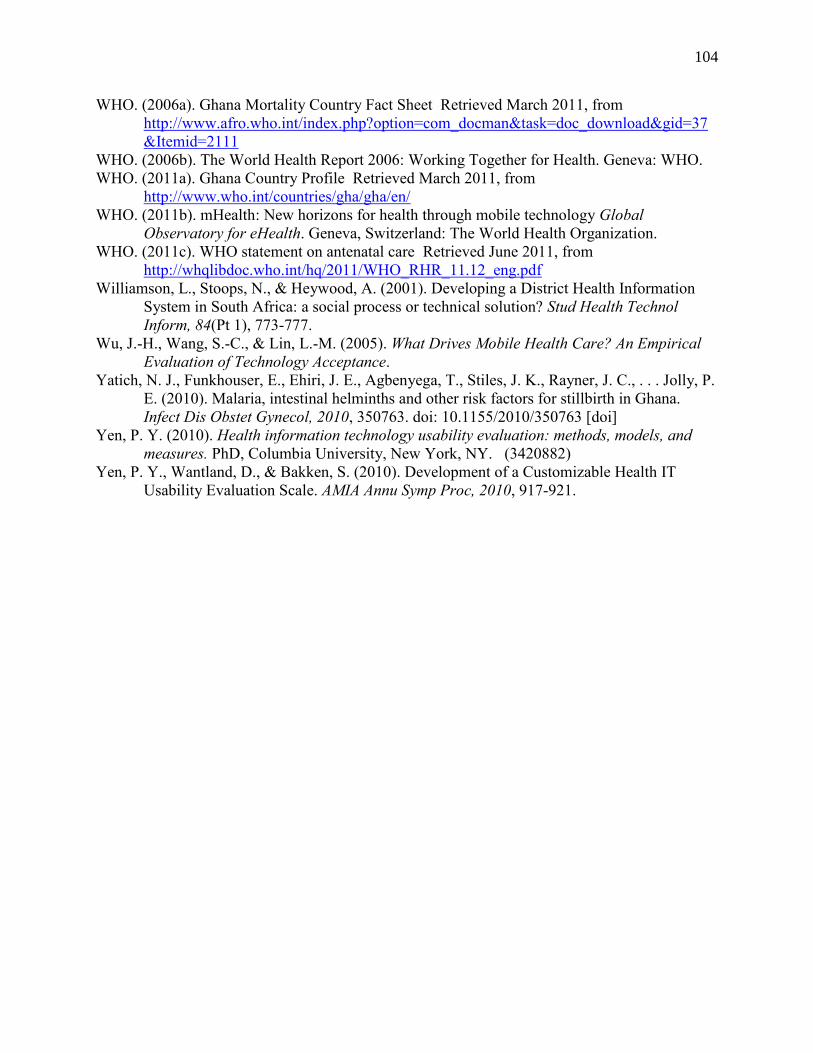
104
WHO. (2006a). Ghana Mortality Country Fact Sheet Retrieved March 2011, from
http://www.afro.who.int/index.php?option=com_docman&task=doc_download&gid=37
&Itemid=2111
WHO. (2006b). The World Health Report 2006: Working Together for Health. Geneva: WHO.
WHO. (2011a). Ghana Country Profile Retrieved March 2011, from
http://www.who.int/countries/gha/gha/en/
WHO. (2011b). mHealth: New horizons for health through mobile technology Global
Observatory for eHealth. Geneva, Switzerland: The World Health Organization.
WHO. (2011c). WHO statement on antenatal care Retrieved June 2011, from
http://whqlibdoc.who.int/hq/2011/WHO_RHR_11.12_eng.pdf
Williamson, L., Stoops, N., & Heywood, A. (2001). Developing a District Health Information
System in South Africa: a social process or technical solution? Stud Health Technol
Inform, 84(Pt 1), 773-777.
Wu, J.-H., Wang, S.-C., & Lin, L.-M. (2005). What Drives Mobile Health Care? An Empirical
Evaluation of Technology Acceptance.
Yatich, N. J., Funkhouser, E., Ehiri, J. E., Agbenyega, T., Stiles, J. K., Rayner, J. C., . . . Jolly, P.
E. (2010). Malaria, intestinal helminths and other risk factors for stillbirth in Ghana.
Infect Dis Obstet Gynecol, 2010, 350763. doi: 10.1155/2010/350763 [doi]
Yen, P. Y. (2010). Health information technology usability evaluation: methods, models, and
measures. PhD, Columbia University, New York, NY. (3420882)
Yen, P. Y., Wantland, D., & Bakken, S. (2010). Development of a Customizable Health IT
Usability Evaluation Scale. AMIA Annu Symp Proc, 2010, 917-921.
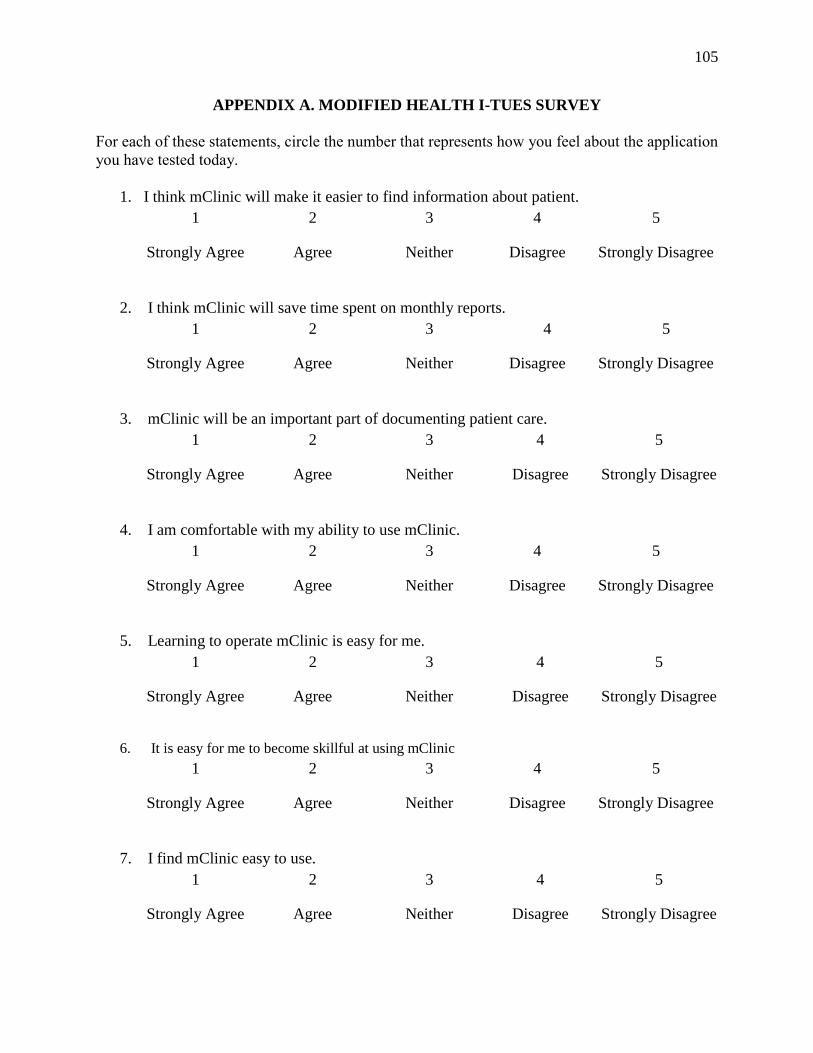
105
APPENDIX A. MODIFIED HEALTH I-TUES SURVEY
For each of these statements, circle the number that represents how you feel about the application
you have tested today.
1. I think mClinic will make it easier to find information about patient.
1 2 3 4 5
Strongly Agree Agree Neither Disagree Strongly Disagree
2. I think mClinic will save time spent on monthly reports.
1 2 3 4 5
Strongly Agree Agree Neither Disagree Strongly Disagree
3. mClinic will be an important part of documenting patient care.
1 2 3 4 5
Strongly Agree Agree Neither Disagree Strongly Disagree
4. I am comfortable with my ability to use mClinic.
1 2 3 4 5
Strongly Agree Agree Neither Disagree Strongly Disagree
5. Learning to operate mClinic is easy for me.
1 2 3 4 5
Strongly Agree Agree Neither Disagree Strongly Disagree
6. It is easy for me to become skillful at using mClinic
1 2 3 4 5
Strongly Agree Agree Neither Disagree Strongly Disagree
7. I find mClinic easy to use.
1 2 3 4 5
Strongly Agree Agree Neither Disagree Strongly Disagree
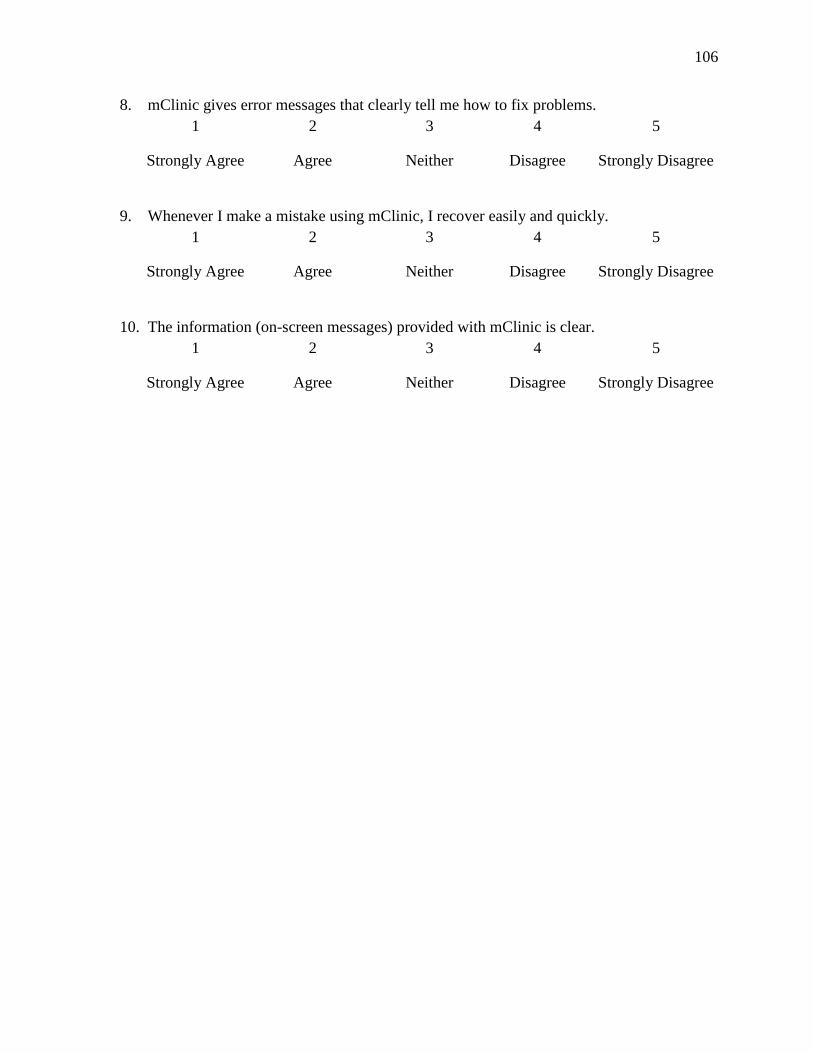
106
8. mClinic gives error messages that clearly tell me how to fix problems.
1 2 3 4 5
Strongly Agree Agree Neither Disagree Strongly Disagree
9. Whenever I make a mistake using mClinic, I recover easily and quickly.
1 2 3 4 5
Strongly Agree Agree Neither Disagree Strongly Disagree
10. The information (on-screen messages) provided with mClinic is clear.
1 2 3 4 5
Strongly Agree Agree Neither Disagree Strongly Disagree
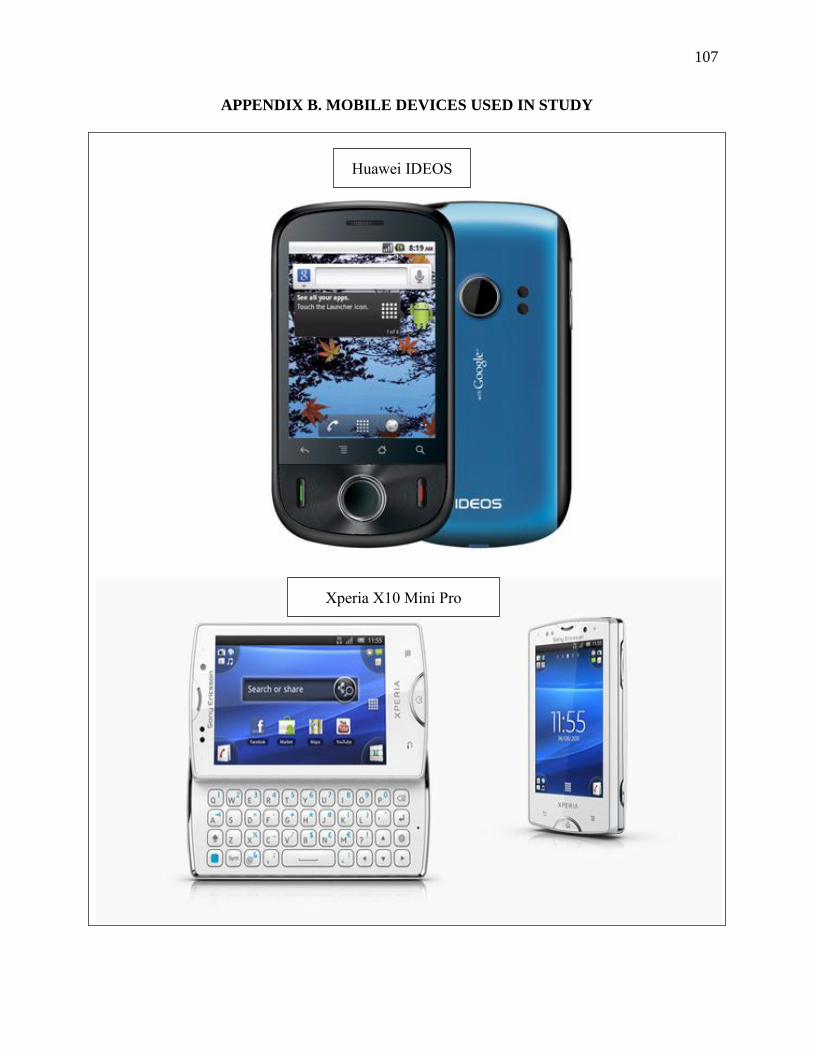
107
APPENDIX B. MOBILE DEVICES USED IN STUDY
Huawei IDEOS
Xperia X10 Mini Pro
108
Samsung Galaxy Tablet
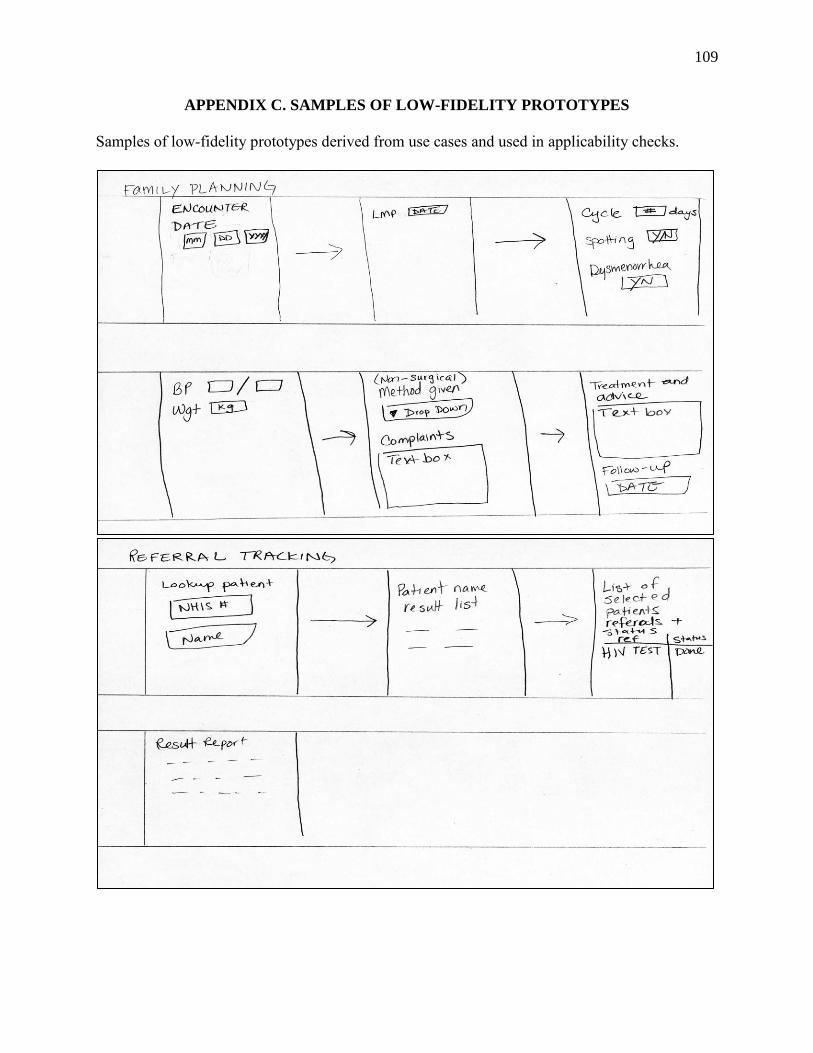
109
APPENDIX C. SAMPLES OF LOW-FIDELITY PROTOTYPES
Samples of low-fidelity prototypes derived from use cases and used in applicability checks.