delivering patient safety 2. changing the culture professor james reason
TRANSCRIPT

Delivering Patient SafetyDelivering Patient Safety
2.2.
CHANGING THE CHANGING THE CULTURECULTURE
Professor James ReasonProfessor James Reason

These discussion materials do not follow These discussion materials do not follow the exact running order of the video the exact running order of the video
programme. They are intended to extend programme. They are intended to extend the reach of the project by facilitating the reach of the project by facilitating exploration of error management in exploration of error management in greater depth and the application of greater depth and the application of
these principles to local issues.these principles to local issues.
- Professor James Reason- Professor James Reason
OverviewOverview
What is culture?What is culture? The journeyThe journey Building a safe cultureBuilding a safe culture
The trouble with culture . . .The trouble with culture . . .
Is that it has about as much definitional precision as a cloud
Is that it has about as much definitional precision as a cloud
Safety culture
Yet . . .Yet . . .
Commercial aviation has a high degree Commercial aviation has a high degree of uniformity across world with regard to of uniformity across world with regard to equipment and standards.equipment and standards.
But the chances of being involved in an But the chances of being involved in an accident with one fatality vary across accident with one fatality vary across world by a factor of x 42 (1 in 11m to 1 world by a factor of x 42 (1 in 11m to 1 in 260k)in 260k)
Some of this is down to infrastructure, Some of this is down to infrastructure, but mostly it’s about culture.but mostly it’s about culture.
Safety culture

Culture: A workable Culture: A workable definitiondefinition
Shared values Shared values (what is important)(what is important) and andbeliefs beliefs (how things work)(how things work) that interact that interactwith an organization’s structure and with an organization’s structure and control systems to produce behaviouralcontrol systems to produce behaviouralnorms norms (the way we do things around here).(the way we do things around here).
Safety culture

What is a ‘safe’ culture?What is a ‘safe’ culture?
A safe culture = an informed cultureA safe culture = an informed culture An informed culture is one that knows An informed culture is one that knows
where the ‘edge’ is without having to fall where the ‘edge’ is without having to fall over it first.over it first.
An informed culture is preoccupied with An informed culture is preoccupied with the possibility of failure and works the possibility of failure and works continuously to become more resilient to continuously to become more resilient to its operational hazards.its operational hazards.
Safety culture

A safe culture has many A safe culture has many interlocking elementsinterlocking elements
Reportingculture
Justculture
Flexibleculture
Learningculture
Safety culture

The elements must work The elements must work in harmonyin harmony
Safety culture
Steps along the waySteps along the way
VulnerableSystem
Syndrome
High Reliability
Organisation
The journey
Vulnerable System Vulnerable System SyndromeSyndrome
Three core pathologiesThree core pathologies• Blame• Denial• And the pursuit of (the wrong
kind of) excellence
The journey
Why the urge to blame Why the urge to blame individuals is so strongindividuals is so strong
Attribution errorAttribution error Illusion of free willIllusion of free will Just world hypothesisJust world hypothesis Hindsight biasHindsight bias Managerial convenienceManagerial convenience Legal convenienceLegal convenience Appeasement of patients Appeasement of patients
& relatives& relativesThe journey
Penalties of blaming Penalties of blaming individualsindividuals
Failure to discover resident pathogensFailure to discover resident pathogens Failure to identify error trapsFailure to identify error traps Management having its eye on the Management having its eye on the
wrong ballwrong ball A blame culture and a reporting culture A blame culture and a reporting culture
cannot co-existcannot co-exist
The journey
Westrum’s classification of Westrum’s classification of three types of safety culturethree types of safety culture
PathologicalPathological BureaucraticBureaucratic GenerativeGenerative
Main differences lie in the way organisationstreat safety-related information. Some deny it,
others welcome it.The journey

N
Thinking in causal series Thinking in causal series rather than causal networksrather than causal networks
Unaware of side-effectsUnaware of side-effectsThe journey
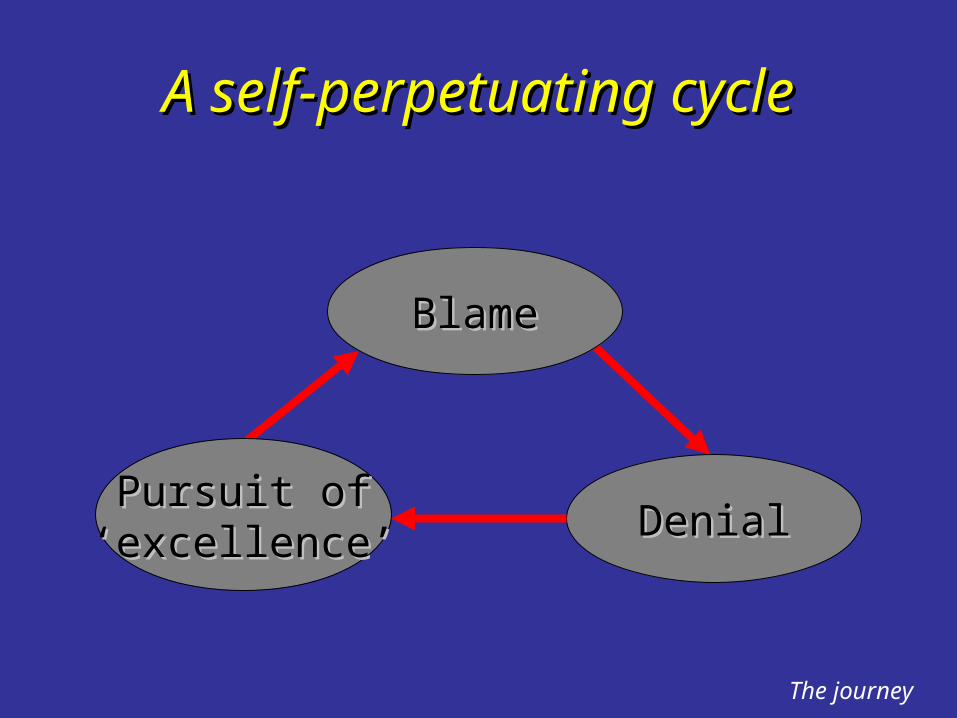
A self-perpetuating cycleA self-perpetuating cycle
BlameBlame
DenialDenialPursuit ofPursuit of
‘‘excellence’excellence’
The journey
A health warningA health warning
No organisation is entirely free of VSSNo organisation is entirely free of VSS Deeply rooted in human psychologyDeeply rooted in human psychology Need to be constantly on the look out for Need to be constantly on the look out for
the signs and symptomsthe signs and symptoms The ability to detect incipient indicators and The ability to detect incipient indicators and
the collective will to fight them are essential the collective will to fight them are essential prerequisites for effective risk managementprerequisites for effective risk management
The journey
A case study from the NHSA case study from the NHS
The incident: During a syringe change-over,a nurse incorrectly re-calibrated a syringe pumpdelivering a morphine infusion to a patient withstomach cancer, resulting in a fatal overdose.
The response: Institution suspended the nursepending an investigation. She was subsequentlygiven a formal written warning, reinstated andretrained in the use of syringe pumps.
The journey
Case study (cont.)Case study (cont.)
Incident investigation: Showed that a GrasebyMS26 syringe driver was being used. Whereasthis pump is calibrated in mm per hr, a secondwidely used pump, the Graseby MS16A, iscalibrated in mm per day. During the syringechange-over, the nurse applied the calibrationprinciples for the MS16A to a MS26 pump.
Early warning signs: Two similar errors hadrecently been reported. Both errors were detected before harm was done.
The journey

Case study (cont.)Case study (cont.)
Recommendation: Chief Pharmacist and twoconsultants wrote to management requestingthat a single pump be used throughout theTrust.
Management response: Suggestion rejectedbecause cost would make it impossiblefor the institution to stay within the budgetlimits set by the regional health authority
The journey
Recurrent system problemsRecurrent system problems
In all 3 cases, nurses had been working on In all 3 cases, nurses had been working on under-staffed wards. Sisters had under-staffed wards. Sisters had complained but mgt. accepted this as a complained but mgt. accepted this as a ‘sad fact of life’ and did not act.‘sad fact of life’ and did not act.
Key situational factors (equipment design, Key situational factors (equipment design, workload, etc.) were not thought relevant. workload, etc.) were not thought relevant. Sole focus on nurses involved: naming, Sole focus on nurses involved: naming, blaming, retraining.blaming, retraining.
The journey

Applying the ‘logic’ of VSSApplying the ‘logic’ of VSS
BlameBlame: There may be a few bad apples, : There may be a few bad apples, but the barrel is OKbut the barrel is OK
DenialDenial: If the barrel’s OK, then anyone : If the barrel’s OK, then anyone who says differently is either stupid or who says differently is either stupid or malicious—anyway, when did we last malicious—anyway, when did we last have a bad event?have a bad event?
Pursuit of ‘excellence’Pursuit of ‘excellence’: Now we’ve : Now we’ve sanctioned the bad apples and gagged sanctioned the bad apples and gagged the whistleblowers, we can focus on the whistleblowers, we can focus on meeting our financial targetsmeeting our financial targets
The journey
Culture: Two aspectsCulture: Two aspects
Something an organisation Something an organisation isis: shared : shared values and beliefs.values and beliefs.
Something an organisation Something an organisation hashas: : structures, practices, systems.structures, practices, systems.
Changing practices easier than changing Changing practices easier than changing values and beliefs.values and beliefs.
Engineering a safe culture

Building a safety cultureBuilding a safety culture
Practices and
structures
Beliefs andvalues
Using anddoing
Thinking and
believing
Building a safe culture
Can a safe culture be Can a safe culture be socially engineered?socially engineered?
Up to a point, YES:Up to a point, YES:• By creating a safety information system that
collects, analyses and disseminates the knowledge gained from incidents, near misses and other ‘free lessons’: A REPORTING CULTURE.
• To do this, however, we need the trust of the workforce: A JUST CULTURE.
Building a safe culture

Building a just cultureBuilding a just culture
A ‘no blame’ culture is neither feasible nor A ‘no blame’ culture is neither feasible nor desirable.desirable.
Some unsafe acts deserve sanctions.Some unsafe acts deserve sanctions. A ‘just’ culture depends on: A ‘just’ culture depends on:
• the trust of the workforce• knowing and agreeing the difference between
acceptable and unacceptable behaviour.
Building a safe culture
Can the law help?Can the law help?
NegligenceNegligence:: involves bringing about a involves bringing about a bad consequence that a ‘reasonable bad consequence that a ‘reasonable and prudent person’ would have and prudent person’ would have foreseen and avoided. Actions do not foreseen and avoided. Actions do not need to be intended. Mainly an issue for need to be intended. Mainly an issue for civil law.civil law.
RecklessnessRecklessness:: involves taking a involves taking a deliberate and unjustifiable risk. Mainly deliberate and unjustifiable risk. Mainly an issue for criminal law.an issue for criminal law.
Building a safe culture

The behavioural rangeThe behavioural range
SabotageSubstance abuse
Reckless violations, etc.
System-induced violations‘Honest’ errors
System-induced errorsetc.
Culpable Blameless
10% 90%
Building a safe culture

Diminishing culpability
Passsubstitution
test?
Deficienciesin training &selection orinexperience?
NO
Possiblenegligent
error
NO
System-induced
error
YES
YESWere the
actionsas intended?
Were the consequencesas intended?
Sabotage, malevolentdamage,
suicide, etc.
YES
YES
NO
NO
Unauthorisedsubstance?
Medicalcondition?
Substanceabuse without
mitigation
Substanceabuse withmitigation
NO YES
YES
NO
Blamelesserror
History of unsafe
acts?
YES NO
Blamelesserror butcorrectivetraining or
counsellingindicated
Knowinglyviolating
safe operatingprocedures?
Were proceduresavailable, workable
intelligible andcorrect?
Possiblerecklessviolation
System-inducedviolation
YES
YES
NO
NO
10% 90%
Decision tree
Building a safe culture

Building a reporting Building a reporting cultureculture
Qualified indemnity against sanctions.Qualified indemnity against sanctions. Confidentiality and/or de-identification.Confidentiality and/or de-identification. Separation of data collection from Separation of data collection from
disciplinary proceedings.disciplinary proceedings. Rapid, useful and intelligible feedback.Rapid, useful and intelligible feedback. Ease of making reportEase of making report
Building a safe culture

Single vs. double-loopSingle vs. double-looporganisational learningorganisational learning
from event reportsfrom event reports
Assumptions
Actions
Actual results
Results gap
Desired results
Single-looplearning
Double-looplearning
Building a safe culture
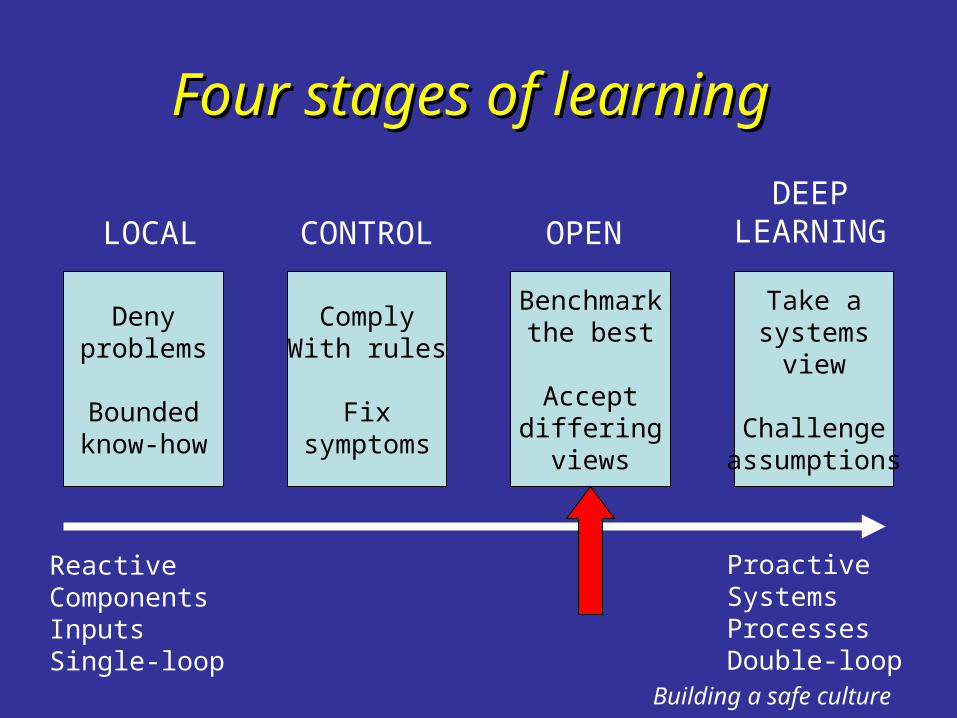
Four stages of learningFour stages of learning
Denyproblems
Boundedknow-how
LOCAL
ComplyWith rules
Fixsymptoms
CONTROL
Benchmarkthe best
Acceptdiffering
views
OPEN
Take asystems
view
Challengeassumptions
DEEPLEARNING
ReactiveComponentsInputsSingle-loop
ProactiveSystemsProcessesDouble-loop
Building a safe culture
Collective mindfulnessCollective mindfulness
A continuing awareness of the possibility of A continuing awareness of the possibility of human, technical and/or systemic failure.human, technical and/or systemic failure.
Expect that errors will be made and train Expect that errors will be made and train personnel to anticipate & recover them.personnel to anticipate & recover them.
Work hard to create a reporting culture & Work hard to create a reporting culture & make the most out of limited event data.make the most out of limited event data.
Generalise rather than localise failures.Generalise rather than localise failures. Brainstorm novel ways in which system could Brainstorm novel ways in which system could
fail.fail.
Building a safe culture
ConclusionsConclusions
The keys to a safe culture are intelligent The keys to a safe culture are intelligent wariness and knowing where the ‘edge’ is.wariness and knowing where the ‘edge’ is.
This requires:This requires:• An effective safety information system• The trust of the workforce• All hinge critically on a JUST CULTURE
Culture is crucial because it alone can have a Culture is crucial because it alone can have a uniform effect (for good or ill) upon the uniform effect (for good or ill) upon the system’s many and varied defences.system’s many and varied defences.