defining response in gvhd treatment
TRANSCRIPT
Defining Response in GVHD TreatmentDefining Response in GVHD Treatment Trials
Paul Carpenter, MB.BS. Associate Member, FHCRCAssociate Professor, UW
Disclosures:– Contract Support for clinical trialsContract Support for clinical trials
• Novartis: Nilotinib for relapse prophylaxis after HCT
5/19/09 FDA AGVHD 1
What is Clinical Benefit in Acute GVHD lTreatment Trials?
Direct Benefit:Direct Benefit:– Prompt reversal of Grade III/IV symptoms clearly benefits the patientbenefits the patient
Survival Benefit:l l f b h– Complete resolution of GVHD may be neither
durable nor associated with long survival
P t t GVHD th i th t hi hi h CR t– Potent GVHD therapies that achieve high CR rates may increase infection mortality rates
“Minimal” residual acute GVHD activity may be– “Minimal” residual acute GVHD activity may be compatible with long‐term survival
5/19/09 FDA AGVHD 2

St d Q tiStudy Question
Can response to GVHD therapy be used
as a surrogate for survival in order
to demonstrate clinical benefit?
5/19/09 FDA AGVHD 3
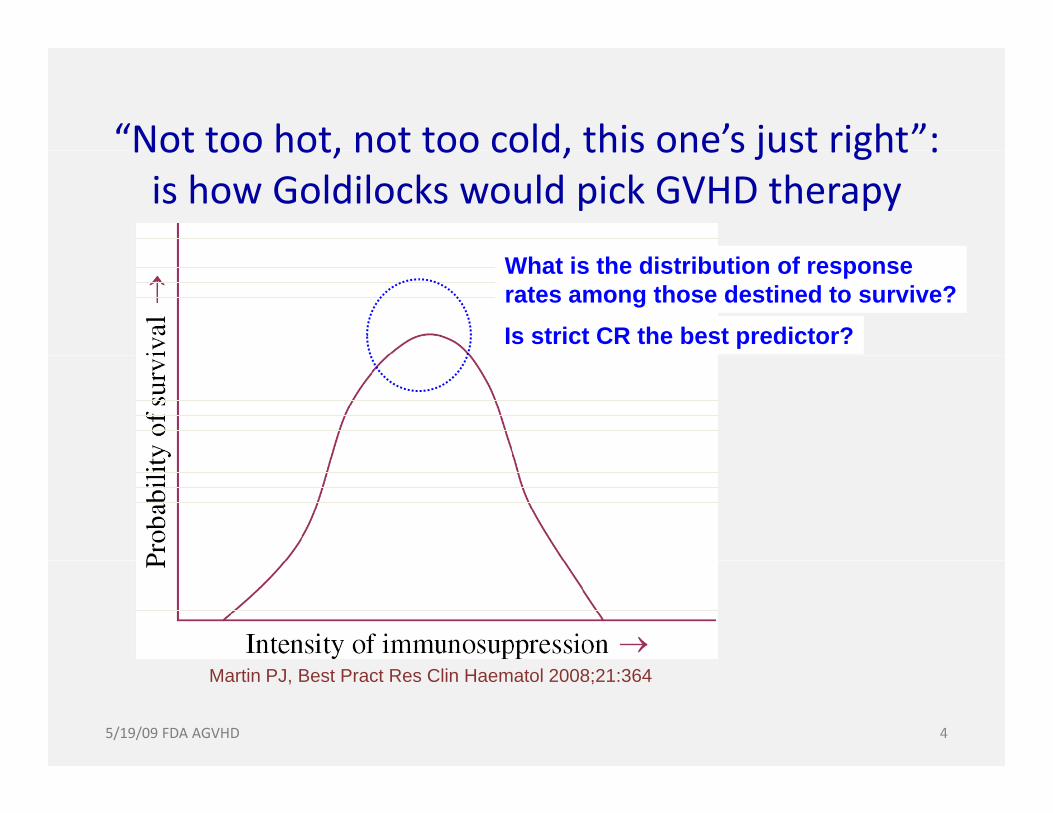
“Not too hot, not too cold, this one’s just right”:Not too hot, not too cold, this one s just right : is how Goldilocks would pick GVHD therapy
What is the distribution of response rates among those destined to survive?Is strict CR the best predictor?
5/19/09 FDA AGVHD 4
Martin PJ, Best Pract Res Clin Haematol 2008;21:364
Study HypothesesStudy HypothesesGVHD responses that are more predictive of 6
h i l h ld idmonth survival should consider:1. Relaxation of the requirement for CR because minimal
residual GVHD activity is not clearly deleteriousresidual GVHD activity is not clearly deleterious.
2. Whether response durability improves prediction
3. Whether steroid dose predicts survivalp
Why choose 6‐month survival ?1. Survival analysis makes fewer assumptions than NRM1. Survival analysis makes fewer assumptions than NRM
2. Deaths < 6 months are often due to acute GVHD
3. Deaths > 6 months have multiple causes (esp, relapse)
5/19/09 FDA AGVHD 5

Study DesignStudy DesignAdditional data collection performed on a subgroup f l bli h d l i hfrom a recently published large retrospective cohort (Mielcarek et al, Blood 2009)
D t il d GVHD t i t D 7 28 d 56Detailed GVHD organ staging at Days 7, 28 and 56 after start of GVHD therapy
Assigned complete response (CR) at each time pointAssigned complete response (CR) at each time‐point
Also defined “very good partial response” (VGPR)
D t il d t id d d t il bl f thiDetailed steroid dose data were available for this cohort.
5/19/09 FDA AGVHD 6

Distinguishing VGPR from CR based on Organ Staging
Stage Skin Liver GutBSA (%) Bilirubin (mg/dL) stool (L/day)
0 0 < 2.0 ≤ 0.5
1 <25 2.0 ‐2.9 > 0.51
2 25‐50 3.0 – 5.9 > 1
3 >50 6.0 ‐14.9 >1.5
4 Bullae ≥ 15 0 >224 Bullae ≥ 15.0 >2
1 – or pesistent anorexia, nausea, vomiting2 – or severe abdominal pain ileus
VGPR included: 1.Minor rash resolving, evanescent, but not progressive2.Minor stable or resolving elevations of bilirubin
5/19/09 FDA AGVHD 7
2.Minor stable or resolving elevations of bilirubin3.Minimal but stable or resolving GI symptoms

Study CohortStudy Cohort
Began with data set of Mielcarek et al (Blood 2009;Began with data set of Mielcarek et al (Blood 2009; 113:2888‐2894)
N = 733 adults transplanted 2000‐2005p
N = 248 selected for further data collection because acute GVHD was diagnosed before Day 30 g y
Day 30 criterion balances the need to:
1. Maximize probability for capturing p y p gresponse data at Days 7, 28 and 56.
2. Minimize bias from including subjects whose g jstay in Seattle was prolonged by illness
5/19/09 FDA AGVHD 8
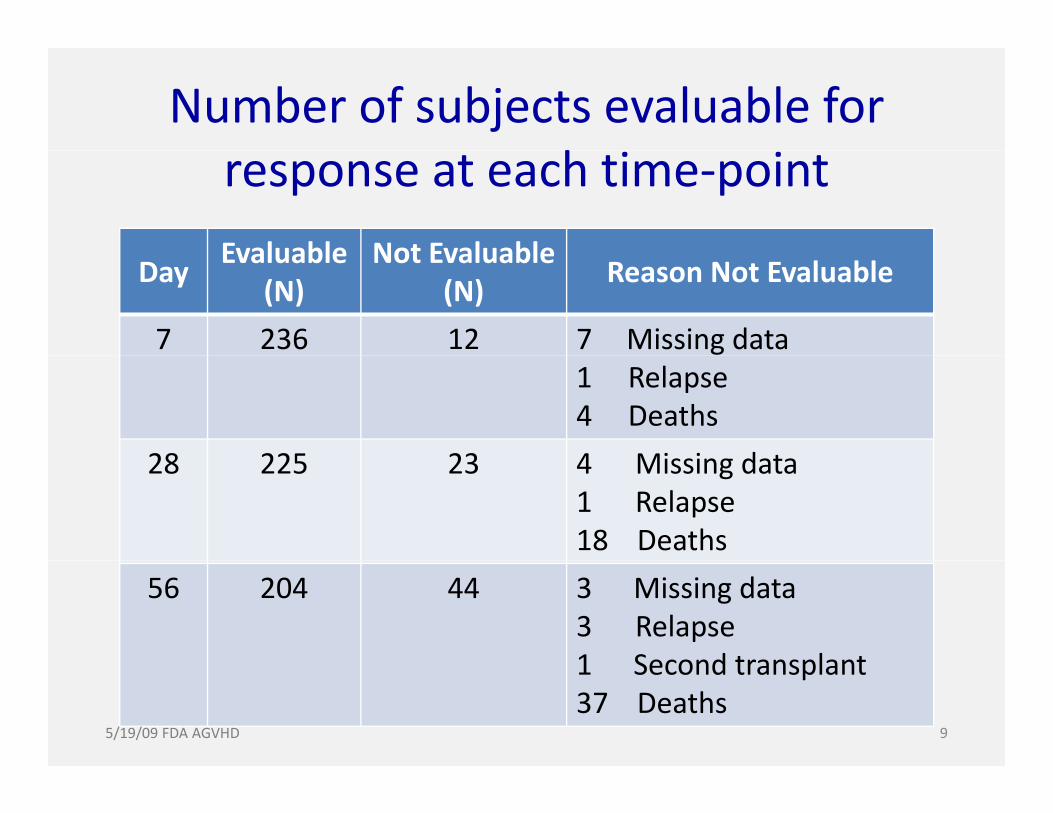
Number of subjects evaluable for hresponse at each time‐point
Evaluable Not EvaluableDay
Evaluable(N)
Not Evaluable (N)
Reason Not Evaluable
7 236 12 7 Missing data1 Relapse4 Deaths
28 225 23 4 Mi i d t28 225 23 4 Missing data1 Relapse18 Deaths
56 204 44 3 Missing data3 Relapse1 Second transplant1 Second transplant37 Deaths
5/19/09 FDA AGVHD 9
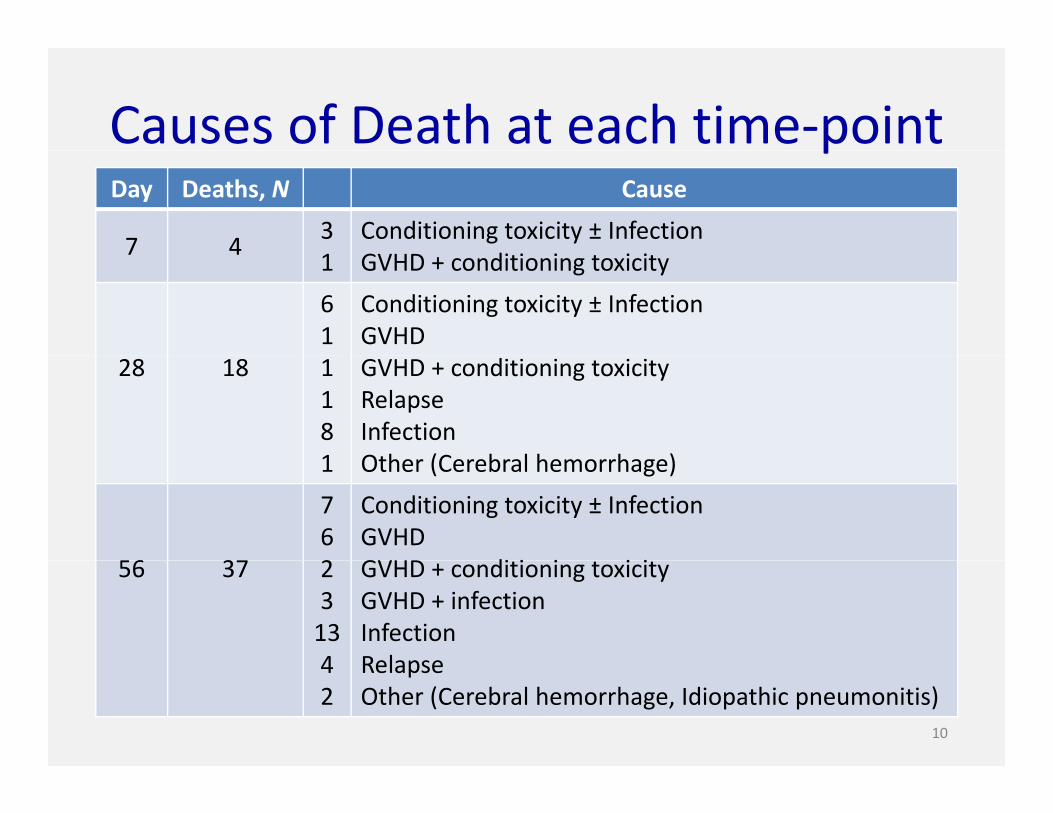
Causes of Death at each time‐pointpDay Deaths, N Cause
7 43 Conditioning toxicity ± Infection
d7 4
1 GVHD + conditioning toxicity
61
Conditioning toxicity ± InfectionGVHD
28 18 1181
GVHD + conditioning toxicityRelapseInfectionOth (C b l h h )1 Other (Cerebral hemorrhage)
56 37
762
Conditioning toxicity ± InfectionGVHDGVHD di i i i i56 37 2
3134
GVHD + conditioning toxicityGVHD + infectionInfectionRelapse4
2RelapseOther (Cerebral hemorrhage, Idiopathic pneumonitis)
10
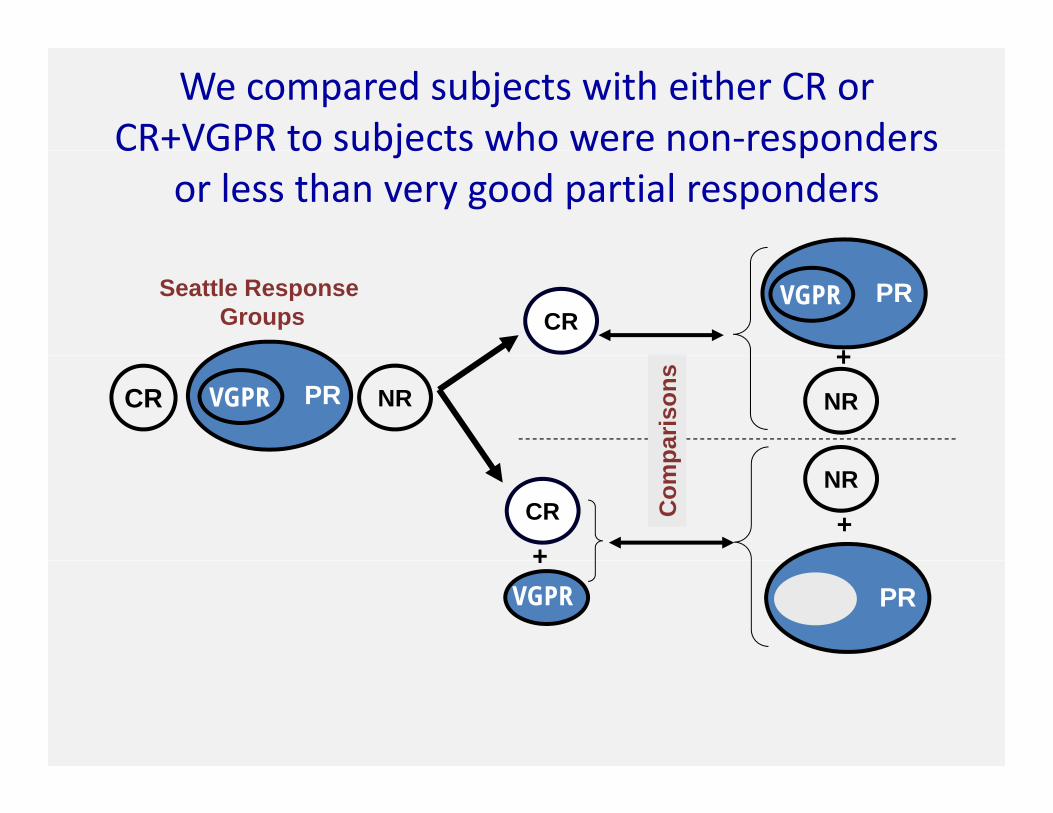
We compared subjects with either CR or CR+VGPR to subjects who were non‐respondersCR VGPR to subjects who were non responders
or less than very good partial responders
CRSeattle Response
GroupsPRVGPR
+PR NRCR VGPR NR
+
paris
ons
+CR
+
NR
Com
p
VGPR+
PR

A 2 x 2 type analysis was performed
Classic 2 x 2 GVHD Response“Test” 2 x 2With
DiseaseWithout Disease
st Disease & No Disease &
Dead Alive
Dead & Alive &
Test 2 x 2
R
POS
tes Disease &
POS testNo Disease &
POS test
a = true +ve b = false +ve
Dead & not in CR
Alive & not in CR
a = true +ve b = false +ve
Not
in C
R
test
Disease & NEG test
No Disease & NEG test
Dead & in CR
Alive & in CR
NR
NEG
t
c = false -ve d = true -ve c = false -ve d = true -veC
A positive “not in CR” test predicts for death at 6 months

GVHD Response “ROC” plotGVHD Response ROC plot
Sensitivity/
ity)
= a / a+c= proportion of dead without CR= “Correctly Predicted Dead”
(Sen
sitiv
i
1 minus Specificity= b / b+d= proportion of survivors without CR
“F l l P di t d D d”= “Falsely Predicted Dead”
Dead & not in CR
Alive & not in CR
(1 - Specificity)
not in CR
Dead & in CR
not in CR
Alive & in CR
a b
5/19/09 FDA AGVHD 13
in CR in CRc d

Day 7 CR or CR/VGPR “Tests” Lack Sensitivity d S ifi i f P di i D h 6 M hand Specificity for Predicting Death at 6 Months
SurvivorsAll patients SurvivorsAll patients(includes deaths before endpoint)
CR CRCR CR
CR + VGPR CR + VGPR
5/19/09 FDA AGVHD 14
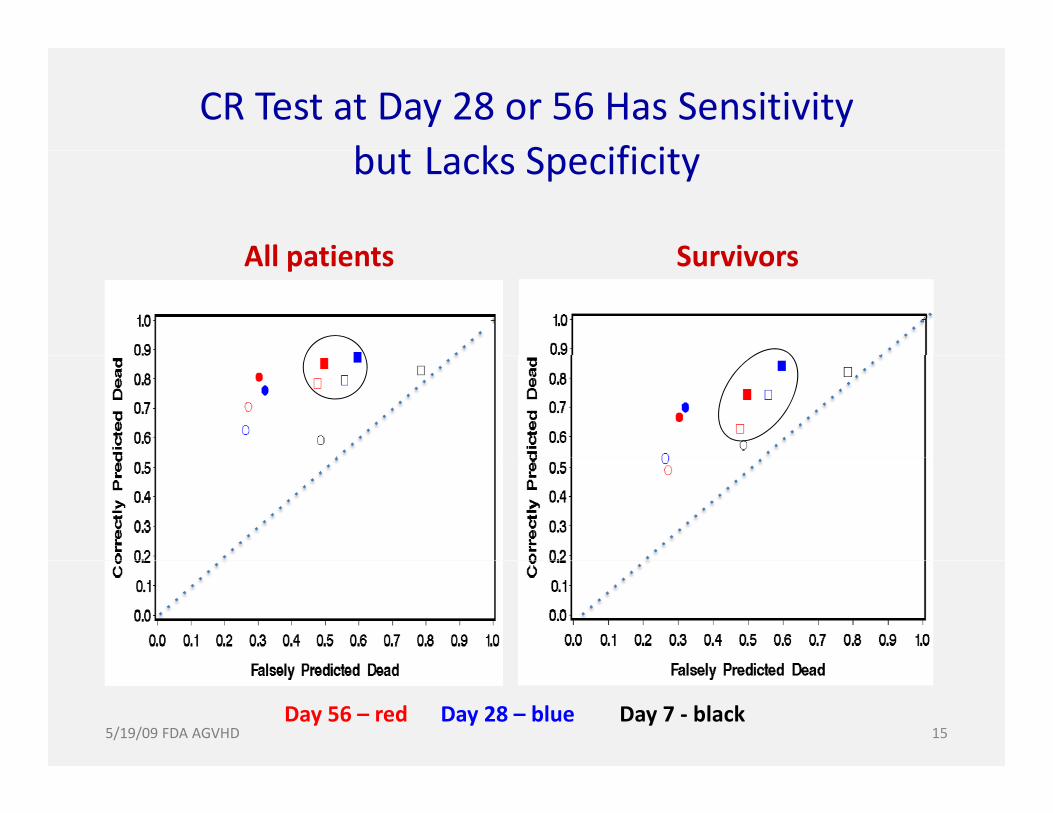
CR Test at Day 28 or 56 Has Sensitivity b t L k S ifi itbut Lacks Specificity
All patients SurvivorsAll patients Survivors
5/19/09 FDA AGVHD 15Day 56 – red Day 28 – blue Day 7 ‐ black

VGPR/CR Test at Day 28 or 56 Improve Specificity with Loss of Sensitivity
All patients SurvivorsAll patients Survivors
CRVGPR/CR
CRVGPR/CR
VGPR/CR
5/19/09 FDA AGVHD 16Day 56 – red Day 28 – blue Day 7 ‐ black

Durable Day 28/56 VGPR/CR Tests Improve f fSensitivity with Little Loss of Specificity
All patients SurvivorsAll patients Survivors
Durable CR
Durable CR
5/19/09 FDA AGVHD 17Day 56 – red Day 28 – blue Day 7 ‐ black

Steroid Dose or % Dose Reduction at Day 28 or 56 t P di ti f D th t 6 M th56 was not Predictive of Death at 6 Months
Day 56y
Day 28
Day 7
Day 28steroid dose% reduction
5/19/09 FDA AGVHD 18

ConclusionsConclusions
Poor surrogates for 6 month survival include:Poor surrogates for 6 month survival include:– Day 7 CR or VGPR response rates– Day 28 or 56 CR or durable CR ratesy
Durable VGPR/CR response has marginal potential as a surrogate for survivalp gA critical unknown is how a treatment that changes response will change 6 month g p gmortality via other downstream effects
5/19/09 FDA AGVHD 19

Difference between Minnesota and Seattle results might relate to definition of PRmight relate to definition of PR. Where do PRs best fit in the analysis?
CRSeattle Response Groups PRVGPR
+PR NRCR VGPR
NR
CR NR
Comparisons
VGPR
++
PR
Minnesota Response GroupsCR NR
5/19/09 FDA AGVHD 20
CR PR NR ComparisonsPR NR
Future DirectionsFuture Directions
Prospective evaluate durable VGPR/CR as anProspective evaluate durable VGPR/CR as an endpoint in clinical trials because it may be more useful than strict CR.Need to better understand the relationship between beneficial effects (response induction) of GVHD treatments and harmful effects that can occur downstream of CR/VGPR ( i i i f i lCR/VGPR (opportunistic infection, relapse, chronic GVHD).
5/19/09 FDA AGVHD 21

Acknowledgementsg
Barry Storer, PhDy ,Marco Mielcarek, MDPaul Martin, MDPaul Martin, MD
5/19/09 FDA AGVHD 22