current second tier and future applications of gene ... · current second tier and future...
TRANSCRIPT

February 24, 2017
Current Second Tier and Future Applications of Gene Sequencing in NBS: Sanger Sequencing
Michele Caggana, Sc.D., FACMGFebruary 16, 2017

February 24, 2017 2
Molecular Analysis in Newborn ScreeningA Staged Approach
Ongoing in routine NBS
Experimental in NBS
Offered clinically and research outside NBS
Genotyping Panel of Mutations -- Single Gene
Sequencing Single Gene
Sequencing Panel of Genes
Sequencing of NBS Genes
GenomeExome
Ongoing in routine NBS
Experimental in NBS
Offered clinically and research outside NBS
S. Cordovado, Ph.D.

February 24, 2017 3
Mix deoxynucleotides with ddA, ddT, ddC*, ddG4 lanes per person/fragment~200 readable bases
Mix deoxynucleotideswith ddA, ddT, ddC, ddG1 scan per person/fragment~800 readable bases
Chop up the human genomeMake a library of fragmentsSequence billions of basesMultiplexing multiple peopleMillions of ‘reads’

February 24, 2017 4
http://nobelprize.org/chemistry/laureates/1980/sanger-autobio.html
Frederick Sanger Walter Gilbert
1/4 prize each
Published in 1977

February 24, 2017 5
• DNA replication requires a free 3’-hydroxyl group; uses dideoxyNTPs
• Originally incorporated a single ddCTP*35S or ddCTP*32P
• Mix acrylamide:bis-acrylamide and pour thin gel between 2 glass plates with spacers
• Polymerizes and is assembled on an apparatus and loaded
Sanger Sequencing

February 24, 2017 6
• Sequencing reactions set up (ea. sample set up with ddG, ddA, ddT and ddC); stop buffer; load each well
• Electrophorese for about 4 hours• Disassemble and dry gel• Expose to x-ray film overnight to days• Manual read
Sanger Sequencing

February 24, 2017 7
Schematic of the “Sanger” Method
“however, with people like Francis Crick around it was difficult to ignore nucleic acids or to fail to realize the importance of sequencing them”.
February 24, 2017 8
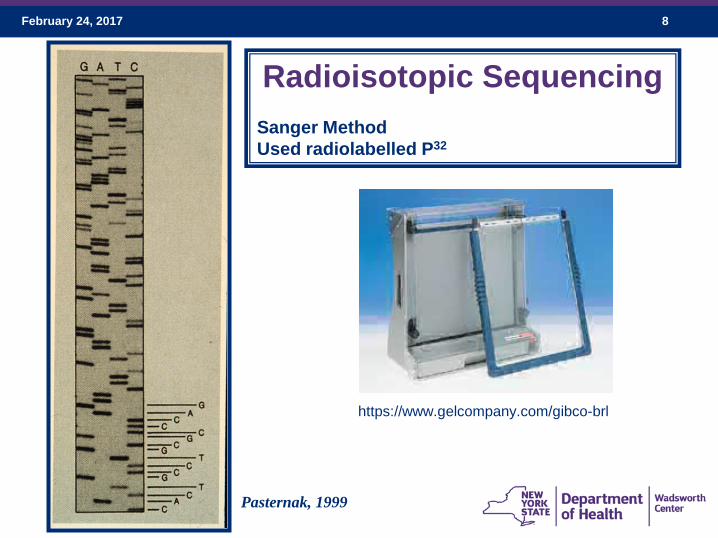
Radioisotopic SequencingSanger MethodUsed radiolabelled P32
Pasternak, 1999
https://www.gelcompany.com/gibco-brl

February 24, 2017 9
• Early 1990’s• Fluorescence-based; got
away from using radioactivity
• 5’-end labeled primers• PCR to amplify• Single tube• Genescan software• Still had to ‘pour’ a gel• Still had to hand load• Eliminated drying• Eliminated manual reading • Longer reads• Human Genome Project
Advancements – ABI 373A
http://www.labrecyclers.com/product.html?InventoryID=2301

February 24, 2017 10
Advancements – Capillary Electrophoresis Detection
• Still based on size separation• Still use dideoxy chain terminators• Labeled primers, laser detects specific
fluorescent tags so we can now combine nucleotides in one tube
A, C, G, T• Can automate set-up• Uses PCR to make DNA
February 24, 2017 11
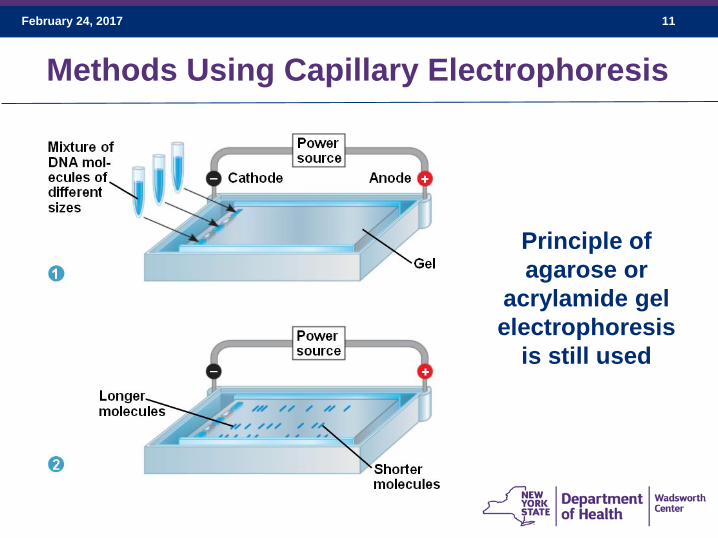
Methods Using Capillary Electrophoresis
Principle of agarose or
acrylamide gel electrophoresis
is still used

February 24, 2017 12
Principle of Capillary Electrophoresis
Multiple capillaries can run samples at the same time
A laser is used to detect fluorescently labeled amplified product

February 24, 2017 13
ABI Prism 3100 Genetic Analyzer
capillaries
Syringe with polymer solution
Autosamplertray
Outlet buffer
Injection electrode
Inlet buffer
laser

February 24, 2017 14
ABI 310016-capillary
array
February 24, 2017 15
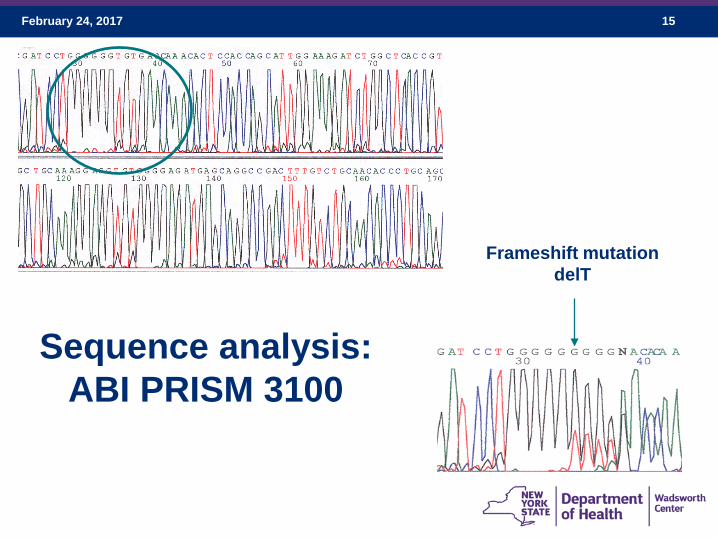
Sequence analysis:ABI PRISM 3100
Frameshift mutationdelT

February 24, 2017 16
Applied Biosystems 3730 48-capillary Genetic Analyzer
Applied Biosystems 3500 8-capillary Genetic Analyzer
DNA Sequence Analysis Using Capillary Electrophoresis

February 24, 2017 17
ABI 3730 Genetic Analyzer
capillaries
cathode/anode bufferspolymer
laser
inlet buffer

February 24, 2017 18
Peering into an ABI 35003500 XL 24-capillary

February 24, 2017 19

February 24, 2017 20
• If a laboratory has the technology, the costs are different
than commercial laboratory costs
• “Pseudodeficiency only” specimens ‘rule – out’ Pompe• Some phenotype/genotype correlations
• Turnaround time ~ a work day with pre-preparation
• Physicians like the information – urgency, family
interaction; health care disparity concerns
• Can release premature infants from further work-up or
re-focus efforts; 42% reduction of referrals for Krabbe
disease
Why Even Bother ??

February 24, 2017 21
GAA Enzyme Activity (MS/MS) (<15%) Daily Mean Average Percent
DNA Sequencing
2 Pathogenic
Variants
Referral
No Pathogenic
Variants
Referral
VOUS (<1% in General Population)
No Referral
OnlyPseudodeficiency
Alleles*
No ReferralReferral
1 Pathogenic Variantc/ or s/VOUS /Polys
VOUS = variant of unknown significance Polys – common variants that are not disease-causing*p.Gly576Ser; p.Glu589Lys
February 24, 2017 22
2nd Tier DNA Assay - Overview
• Obtain two 3-mm punches from dried blood spots and
extract DNA
• Amplify 14 separate gene fragments by PCR;
encompasses exons 2-20 including intron/exon
boundaries
• PCR products used for Sanger sequencing
• Sequences analyzed for mutations or variants
• Referral according to the algorithm
• Parental phasing; sibling testing
February 24, 2017 23
Step One : Punch and Extract DNA
Hands on: 5-10 min; Hands-off: 45 minutes

February 24, 2017 24
PCR Number Exons Covered
Base Pairs
1 2 772
2 3 384
3 4-5 630
4 6-8 781
5 9 483
6 10-11 890
7 12 465
PCR Number Exons Covered
BasePairs
8 13-14 679
9 15 486
10 16 583
11 17 497
12 18 400
13 19 342
14 20 460
20 Exons Covered in 14 FragmentsChromosome 17 –952 amino acids
• Primer design• Check for SNPs; minor allele frequencies on dbSNP• Need to amplify all with the same PCR program• Can use different master mixes

February 24, 2017 25
1 2 3 4 5 6 7
A E2 –1a E4/5 –1a E9 –1a E12 –1a E15 –1a E17 –1a E19 –1a
B E2 –1b E4/5 –1b E9 –1b E12 –1b E15 –1b E17 –1b E19 –1b
C E2 –WTC E4/5 –WTC E9 –WTC E12 –WTC E15 –WTC E17 –WTC
E19 –WTC
D E 2 –NTC E4/5 – NTC E9 –NTC E12 –NTC E15 –NTC E17 –NTC E 19 –NTC
E E3 –1a E6/8 –1a E10/11 –1a
E13/14 –1a
E16 –1a E18 –1a E20–1a
F E3 –1b E6/8 –1b E10/11 –1b
E13/14 –1b
E16 –1b E18 –1b E20–1b
G E3 –WTC E6/8 –WTC E10/11 –WTC
E13/14 –WTC
E16 –WTC E18 –WTC
E20 –WTC
H E3 –NTC E6/8 –NTC E10/11 –NTC
E13/14 –NTC
E16 –NTC E18 –NTC E20 –NTC
PCR Plate Map
Hands on: 5 min; Hands-off: 2 hoursWTC = wild type control; NTC = no template control

February 24, 2017 26
Set Up Plates in Batches
• Saves time• Batches better for QI• Minimize pipetting errors• Minimize inconsistencies

February 24, 2017 27
Agarose Gel Electrophoresis
Product Check
• Sizes okay• Amplification• No Contamination
Hands on: 15 min; Hands-off: 45 minutes

February 24, 2017 28
PCR Clean-up Before SequencingExoSap-IT Treatment
1 2 3 4 5 6 7 8
A E2 –1a E6/8 –1a E12 –1a E16 –1a E20–1a
B E2 –1b E6/8 –1b E12 –1b E16 –1b E20–1b
C E2 –1a E6/8–1a E13/14 –1a E17 –1a
D E2 – 1b E6/8–1b E13/14 –1b E17 –1b
E E3 –1a E9 –1a E13/14 –1a E18 –1a
F E3 –1b E9 –1b E13/14 –1b E18 –1b
G E4/5 –1a E10/11 –1a E15 –1a E19 –1a
H E4/5 – 1b E10/11 –1b E15 –1b E19 –1b
Hands on: 5 min; Hands-off: 30 minutes

February 24, 2017 29
Cycle Sequencing1 2 3 4 5 6 7 8 9 10
A E2 F–1a
E 6/8 F–1a
E12 F–1a
E16 F–1a
E 20 F–1a
E2 R–1a
E 6/8 R–1a
E12 R–1a
E16 R–1a
E20 R– 1a
B E2 F–1b
E 6/8 F–1b
E12 F–1b
E16 F–1b
E 20 F–1b
E2 R–1b
E 6/8 R–1b
E12 R–1b
E16 R–1b
E20 R– 1b
C E2 SEQF
1a
E6/8SEQF1a
E13/14 F–1a
E17 F–1a
E2 SEQR –
1a
E6/8–SEQR1a
E13/14 R–1a
E17 R–1a
D E2 SEQF1
b
E6/8SEQF1b
E13/14 F–1b
E17 F–1b
E2 SEQR1
b
E6/8 SEQR1b
E13/14 R–1b
E17 R–1b
E E3 F–1a
E9F–1a
E13/14 SEQF
1a
E18 F–1a
E3 R–1a
E 9 R–1a
E13/14 SEQR1a
E18 R–1a
F E3 F–1b
E9 F–1 b
E13/14 SEQF
1b
E18 F–1b
E3 R–1b
E9R–1a
E13/14 SEQR1b
E18 R–1b
G E4/5 F–1a
E10/11F–1a
E15 F–1a
E19 F–1a
E4/5 R–1a
E10/11 R–1a
E15 R–1a
E19 R–1a
H E 4/5 F–1b
E10/11 F–1b
E15 F–1b
E 19 F–1b
E4/5 R– 1b
E10/11 R–1b
E15 R–1b
E19 R–1b
Hands on: 5 min; Hands-off: 2.5 hoursSEQ primers are internal sequencing primers

February 24, 2017 30
The Rest of the Story• Centri-sep columns to remove dye terminators• Hands-on: 5 minutes; Hands-off: 10 minutes
• Load Sequencer and run• Hands-on: 5 minutes; Hands-off: 2 hours

February 24, 2017 31
The Rest of the Story 2• Analyze results on SeqScape
• Map new mutations
• Search databases, literature for detected mutations
• Run new variants / VOUS through programs to determine if pathogenic
• Make referral with best interpretation possible in absence of any clinical information
• Results available the next morning• Total time: 10-12 hours
Hands on: 1 - 2 hours
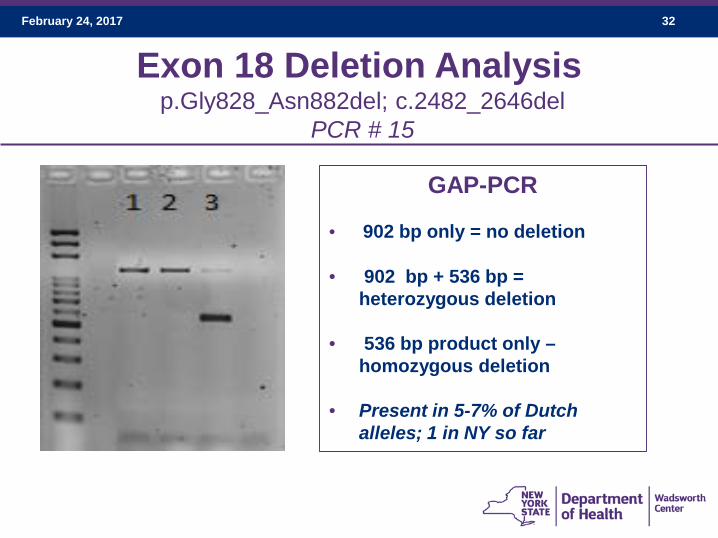
February 24, 2017 32
Exon 18 Deletion Analysisp.Gly828_Asn882del; c.2482_2646del
PCR # 15
GAP-PCR
• 902 bp only = no deletion
• 902 bp + 536 bp = heterozygous deletion
• 536 bp product only –homozygous deletion
• Present in 5-7% of Dutch alleles; 1 in NY so far
February 24, 2017 33
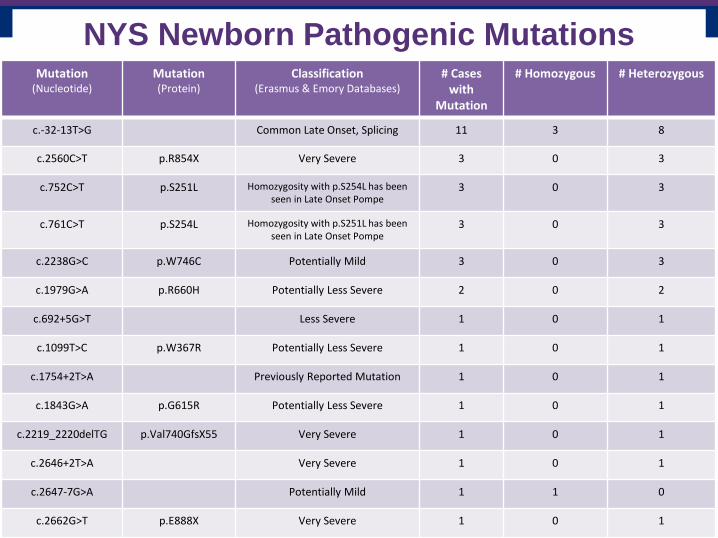
Mutation(Nucleotide)
Mutation(Protein)
Classification(Erasmus & Emory Databases)
# Cases with
Mutation
# Homozygous # Heterozygous
c.-32-13T>G Common Late Onset, Splicing 11 3 8
c.2560C>T p.R854X Very Severe 3 0 3
c.752C>T p.S251L Homozygosity with p.S254L has been seen in Late Onset Pompe
3 0 3
c.761C>T p.S254L Homozygosity with p.S251L has been seen in Late Onset Pompe
3 0 3
c.2238G>C p.W746C Potentially Mild 3 0 3
c.1979G>A p.R660H Potentially Less Severe 2 0 2
c.692+5G>T Less Severe 1 0 1
c.1099T>C p.W367R Potentially Less Severe 1 0 1
c.1754+2T>A Previously Reported Mutation 1 0 1
c.1843G>A p.G615R Potentially Less Severe 1 0 1
c.2219_2220delTG p.Val740GfsX55 Very Severe 1 0 1
c.2646+2T>A Very Severe 1 0 1
c.2647-7G>A Potentially Mild 1 1 0
c.2662G>T p.E888X Very Severe 1 0 1
NYS Newborn Pathogenic Mutations

February 24, 2017 34
Variant of Unknown
Significance(Nucleotide)
Variant of Unknown
Significance(Protein)
Information Found in Literature
andOther Notes
# Cases with
Mutation
# Homozygous
# Heterozygous
c.664G>A p.V222M Reported as likely non-pathogenic based on in vitro
studies, however this mutation was reported in several infants
identified by the Hungarian NBS program as having low
GAA enzyme activity. Diagnostic info was not
published.
3 2 1
c.858+17_858+23
delCGGGCGG
Likely benign due to its location in the intron
3 0 3
c.1194+37G>A 3 2 1
c.316TC>T p.R106C 2* 2 0
c.2051C>T p.P684L Seen once by Duke; only mut detected in a 21 y.o. with progressive scoliosis and diminished GAA activity.
Predictive algorithms conflicting as to whether its
pathogenic. Reported in dbSNP and ExAC, but rare.
2 0 2
*Twins
NYS Newborn Screening VOUS

February 24, 2017 35
• The IDUA gene codes for the alpha-L-iduronidaseenzyme
• Cytogenetic Location: 4p16.3• Gene spans approximately 19 kb and has 14 exons;
653 amino acids; GC-rich gene – tricky • Approximately 100 mutations have been reported• Majority seem to be private mutations but a few have
been seen with some frequency
• In North America two of the most common mutations are p.W402* (45-60%) and p.Q70* (17%)
The IDUA Gene – MPS 1

February 24, 2017 36
Molecular analysis: c.235G>A (p.A79T); c.246C>G (p.H82Q); c.755G>A (p.D223N); c.965T>A (p.V322E); • 3 Black infants are p.A79T / p.A79T [MAF=2.8%; Blacks only]
• 2 Black infants are p.A79T / p.V322E [MAF<1% Blacks & Eur. Am.]
• 1 Black infant is p.A79T / p.D223N [MAF <1%; Blacks only]
• p.H82Q (MAF<1% in both European and Blacks) was detected in 2 infants: homozygous in a Caucasian infant, and compound heterozygous with p.V322E in a biracial infant.
• Too early to rule out MPS 1 in these patients based on clinical features; however six of the eight have had urine studies performed and had normal chromatography/electrophoresis.
• Previously described pseudodeficiency allele c.898G>A (p.A300T)Three apparent pseudo-deficiency alleles in the IDUA gene identified by newborn screening. L. M. Pollard1, S. R. Braddock2, K. M. Christensen2, D. J. Boylan2, L. D. Smith3, B. A. Heese3, A. M. Atherton3, C. E. Lawson3, M. E. Strenk3, M. Willing4, L. Manwaring4, T. C. Wood1
Possible Pseudodeficiency Alleles

February 24, 2017 37

February 24, 2017 38
Third Tier: DNA Sequencing – ALD• Full sequencing of ABCD1 gene• Not intended to reduce referrals• Helps to determine
o if females are ALD carriers (ALD females)o if males have mutationo if no mutation, consider other PBD
• Neither marker concentration nor genotype correlates with phenotype!!
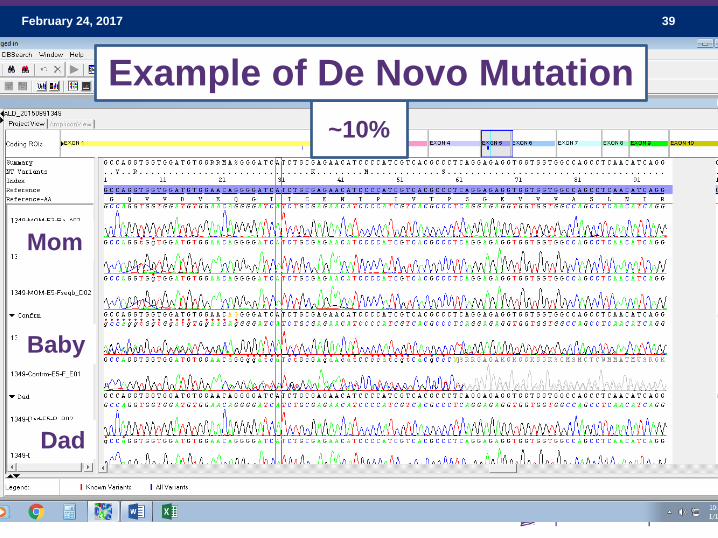
February 24, 2017 39
Dad
Mom
Baby
~10%
Example of De Novo Mutation

February 24, 2017 40
Thank you to Colleen Stevens, Ph.D. and Suzanne Cordovado, Ph.D. for slides
and to you for your attention!