copper chelation therapy in intrahepaticcholestasis childhood · chelation therapy in intrahepatic...
TRANSCRIPT

Gut, 1983, 24, 42-48
Copper chelation therapy in intrahepatic cholestasis ofchildhoodJ EVANS,* H ZERPA, L NUTTALL, M BOSS, and S SHERLOCK
From the Departments ofMedicine, Histopathology, and Medical Physics, Royal Free Hospital, London
SUMMARY The effect of copper chelation was studied in a group of children with intrahepaticcholestasis of childhood (IHCC) and increased liver copper levels. Initial therapy wasD-penicillamine (10 mg/kg/day), being replaced by triethylenetetramine dihydrochloride (20mg/kg/day) when side-effects of D-penicillamine occurred. Eight children completed two years ofcopper chelation. Pruritis remained the main symptom and did not improve. Two patientsdeveloped D-penicillamine side-effects - one patient after nine months (marked anorexia,lassitude) and one other patient after 19 months (thrombocytopenia). Two patients died duringthe study, in one of these normal hepatic copper concentration was achieved. Hepatic copperconcentrations decreased in seven of eight patients from 8.6 (2.7-16.2) jumoUg to 3.4 (0.6-16.5),umol/g (median and range (OO5<p<0.1) and serum aspartate transaminase increased in seven ofeight patients (p<005). Histological assessment of serial liver sections revealed increased fibrosisand cholestasis despite reductions in hepatic copper levels during the study. This study showedthat D-penicillamine therapy was associated with significant side-effects, while marked clinical,biochemical, or histological improvement did not follow effective copper chelation therapy inintrahepatic cholestasis of childhood.
The liver is the principal organ involved in coppermetabolism.' It is the main site of copper storage aswell as the organ in which caeruloplasmin issynthesised.2 Normal liver copper levels aremaintained by excretion of copper into bile orincorporation of copper into caeruloplasmin andsecretion into plasma. Normally, about 80% ofcopper absorbed from the diet is excreted into bile.3An impairment of hepatic copper excretion is likelyto be associated with increased hepatic copperconcentrations.Abnormal accumulation of copper in the liver (>4
,gmol/g dry weight), brain, and kidney in Wilson'sdisease is associated with tissue damage4 and D-penicillamine therapy effects clinical improvement.5Copper hepatocytotoxicity may also develop withcopper sulphate poisoning in man6 and in experi-mental animals.7 Liver copper concentrationexceeding 4 ,mol/g has been described with chroniccholestasis associated with primary biliarycirrhosis,8-13 intrahepatic cholestasis of childhood* Address for correspondence: Dr J Evans, Department of PaediatricGastroenterology, Mater Children's Hospital, South Brisbane, 4101,Queensland, Australia.Received for publication 13 April 1982
(IHCC),'4 15 extrahepatic biliary obstruction,'6 andIndian childhood cirrhosis.17 Increased liver copperconcentration may contribute to continuing hepaticnecrosis in primary biliary cirrhosis and D-penicillamine therapy effects histologicall' andbiochemical'8 improvement. This beneficial result ofD-penicillamine therapy in primary biliary cirrhosismay be related to an immunological effect or copperchelation.18
Intrahepatic cholestasis of childhood is a raredisorder, usually of unknown aetiology, in whichimmunological mechanisms do not appearprominent in the pathogenesis of the disorder. Lifeexpectancy is reduced, therapy is symptomatic, andliver cell failure is a common mode of death.'9 Highliver copper levels, which might contribute tocontinuing hepatic necrosis, are common14 15 andtend to occur in older children.15 By analogy withWilson's disease and primary biliary cirrhosis a trialof D-penicillamine therapy in selected patients withintrahepatic cholestasis of childhood appearedwarranted. We report the clinical, biochemical, andhistological effect of copper chelation therapy in anon-immunological chronic cholestatic disorder ofchildhood with increased hepatic copper levels.
42
on May 22, 2020 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.24.1.42 on 1 January 1983. D
ownloaded from
Copper chelation therapy in intrahepatic cholestasis of childhood
Methods
PATIENTSEight children with intrahepatic cholestasis of child-hood and raised hepatic copper levels were studied.Diagnosis was based on clinical, biochemical, andhistological evidence. 19 Extrahepatic biliaryobstruction was excluded by laparotomy (four cases)or by ultrasound examination and percutaneoustranshepatic cholangiography (four cases). Sevencases were sporadic, while the eighth case had a
brother with intrahepatic cholestasis of childhoodwho had died earlier after haemorrhage fromoesophageal varices. Pulmonary flow murmurs were
present in two children; one of these, in addition,had congenital glaucoma. In these two cases therewas no evidence of pulmonary valve stenosis as
assessed clinically, with ECG, radiograph of thechest, or echocardiography. Arteriography was notperformed. On entry to the study all cases werenegative for HBsAg, anti-HBs, and anti-HBc andhad normal levels of serum alpha-1-antitrypsin.Children with characteristic facies and cardiaclesions,20 Byler's syndrome,21 or arteriohepaticdysplasia22 were not present in this series. Thepatients were of various nationalities: Arabian, one;
Italian, one; Portuguese, one; Greek, two; English,three. This group was composed of five females andthree males. The ages of children in the group
ranged from 2 years to 22 years and the median age
was 7 years. None had had portal-systemic shuntsurgery.
PROTOCOLTreatment with D-penicillamine was started at adose of 5 mg/kg/day and increased to 10 mg/kg/dayafter two months in the hope of minimising theincidence of side-effects. D-penicillamine was
prescribed as a single dose, to be taken eachmorning on an empty stomach 30 minutes before theother medication or meals. Triethylenetetraminedihydrochloride (20 mg/kg/day), another cuprureticagent,23 was substituted when side-effects to D-penicillamine occurred. Approval for copperchelation therapy in intrahepatic cholestasis ofchildhood, on a trial basis, was obtained from theDepartment of Health and Social Services and theconduct of the study was approved by the EthicsCommittee of the Royal Free Hospital. Informedconsent was obtained from the parents beforeentering each patient into the study and before eachliver biopsy.
Before initiating copper chelating therapy in eachpatient, a clinical history was obtained withparticular reference to the major symptom; dailyintake of cholestyramine was noted; the height and
weight of each patient was recorded; liver functiontests (bilirubin, aspartate transaminase, alkalinephosphatase) and fasting bile acids wereperformed.24 As well, copper metabolism wasstudied in general with plasma caeruloplasmin andcopper, 24 hour urinary copper excretion and livercopper concentration before the start of therapy. Ameasure of circulating immune complexes was madewith the Clq binding assay.25 The above investi-gations were repeated at annual visits.
PROCEDURELiver function tests were determined by routinemethods. Total plasma copper and 24 hour urinarycopper excretion were determined by atomicabsorption spectroscopy.26 Normal values are 15 to22 gmol/l (100-140 gg/100 ml) and <08 ,umol/24 h(<50 ,ug/24 h) respectively. The 24 hour urinarycopper excretion was the mean of three consecutive24 hour urine collections obtained in preparedplastic containers. Caeruloplasmin was measured byimmunodiffusion and normal values are 0.25-0.4 g/l.Fasting bile acids were measured by the method ofMurphy.24Each liver biopsy was obtained with a Menghini
needle which had been rendered copper free. Thebiopsy needle was washed with a 1% solution ofethylenediamine tetraacetic acid (EDTA), rinsedwith ion-free water, and sterilised in similarlyprepared glass containers. A portion of each liverbiopsy was obtained for copper concentration andthe remaining portion was examined histologically.The copper concentration was measured by neutronactivation analysis.27 Normal hepatic copperconcentration is 0-2 to 0-9 ,umol/g (15-55 ,ug/g) dryliver. The coefficient of variation for duplicatemeasurements of liver copper levels measured byneutron activation analysis is 7% to 15%.
Clq bindingThe effect of D-penicillamine on immune complexeswas monitored by the modified Clq binding testwhich detects immune complexes of greater than 20sin size.25
Histological assessmentAll the liver biopsies were reviewed (HZ and JE) atthe end of the study without knowledge of results ofbiochemical tests or measured liver copper concen-trations. Each biopsy was examined with routinehistological stains (H and E, and reticulin) and withhistochemical stains for copper28 and copperassociated protein.29 The histological features ofinflammation, necrosis, cholestasis, and fibrosiswere specifically semi-quantitatively assessed andgraded +, ++, +++, for mild, moderate, and
43
on May 22, 2020 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.24.1.42 on 1 January 1983. D
ownloaded from
Evans, Zerpa, Nuttall, Boss, and Sherlock
severe changes. In each biopsy at least 12 portaltracts were viewed and bile ducts counted. Bile ductpaucity was considered if there were less than fourbile ducts counted in these portal tracts, and bileducts were absent if none was counted.
Statistical methodsThe paired t test was used for statistical analysis ofvalues of hepatic copper concentration, plasmacopper and caeruloplasmin values, 24 hour urinecopper excretion, liver function tests, and fastingbile acids before and after copper chelation therapy.The mean score of standard deviations was used
to analyse the. effect of therapy on each patient'sheight and weight.30
Results
CLINICALMarked symptomatic improvement was notobserved. Pruritis remained the major symptom andwas unchanged during the study period. Twopatients developed significant side-effects with D-penicillamine therapy. One patient developedmarked anorexia and lassitude after nine months.Triethylenetetramine dihydrochloride (20 mg/kglday) was substituted and continued for 15 monthswithout side-effects. The other patient developedsignificant thrombocytopenia after 19 months ofD-penicillamine therapy and declined furthercopper chelating treatment. Two patients diedduring the study. One patient died while overseas
from a massive gastrointestinal haemorrhage aftertwo years of D-penicillamine therapy, the livercopper concentration just before death was normal.The other patient died from a combination ofliver cell failure and repeated gastrointestinal
haemorrhages. This patient had received 19 monthsof D-penicillamine therapy. Hepatic tissue from thispatient was obtained at necropsy.
Children entering the study were slightly under-sized and underweight. After copper chelationtherapy a spurt in height and weight was notobserved, despite major falls in hepatic copper
concentration in the patients.
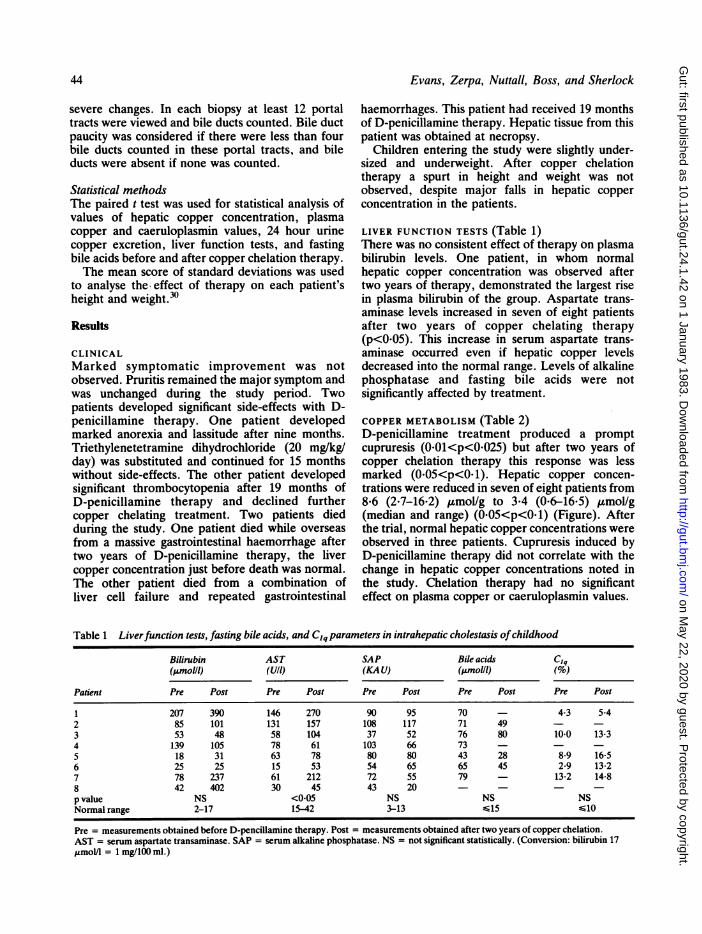
LIVER FUNCTION TESTS (Table 1)There was no consistent effect of therapy on plasmabilirubin levels. One patient, in whom normalhepatic copper concentration was observed aftertwo years of therapy, demonstrated the largest risein plasma bilirubin of the group. Aspartate trans-aminase levels increased in seven of eight patientsafter two years of copper chelating therapy(p<005). This increase in serum aspartate trans-aminase occurred even if hepatic copper levelsdecreased into the normal range. Levels of alkalinephosphatase and fasting bile acids were notsignificantly affected by treatment.
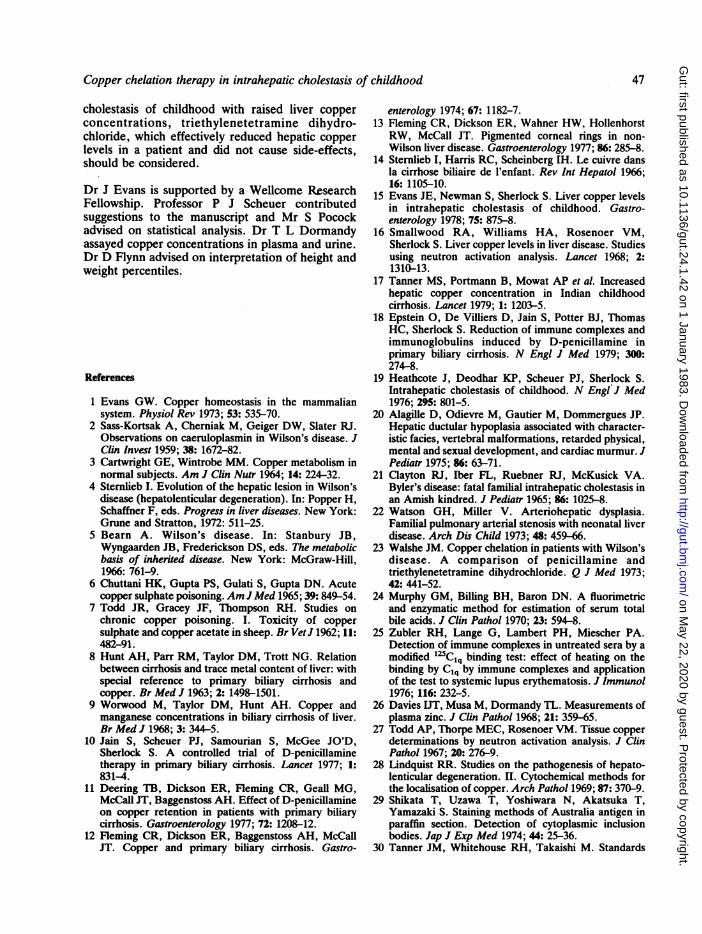
COPPER METABOLISM (Table 2)D-penicillamine treatment produced a promptcupruresis (0.01<p<0025) but after two years ofcopper chelation therapy this response was lessmarked (0.05<p<O. 1). Hepatic copper concen-trations were reduced in seven of eight patients from8.6 (2.7-16.2) ,umol/g to 3.4 (0.6-16.5) ,umol/g(median and range) (0O05<p<0O1) (Figure). Afterthe trial, normal hepatic copper concentrations wereobserved in three patients. Cupruresis induced byD-penicillamine therapy did not correlate with thechange in hepatic copper concentrations noted inthe study. Chelation therapy had no significanteffect on plasma copper or caeruloplasmin values.
Table 1 Liverfunction tests, fasting bile acids, and Clq parameters in intrahepatic cholestasis ofchildhood
Bilirubin AST SAP Bile acids Clq(pmolll) (U/i) (KAU) (pmolll) (%)
Patient Pre Post Pre Post Pre Post Pre Post Pre Post
1 207 390 146 270 90 95 70 - 4-3 5.42 85 101 131 157 108 117 71 49 - -3 53 48 58 104 37 52 76 80 10.0 13-34 139 105 78 61 103 66 73 - - -5 18 31 63 78 80 80 43 28 8-9 16-56 25 25 15 53 54 65 65 45 2-9 13-27 78 237 61 212 72 55 79 - 13.2 14.88 42 402 30 45 43 20 - - - -p value NS <0.05 NS NS NSNormal range 2-17 15-42 3-13 6 15 . ..G10
Pre = measurements obtained before D-pencillamine therapy. Post = measurements obtained after two years of copper chelation.AST = serum aspartate transaminase. SAP = serum alkaline phosphatase. NS = not significant statistically. (Conversion: bilirubin 17jumol/l = 1 mg/100 ml.)
44
on May 22, 2020 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.24.1.42 on 1 January 1983. D
ownloaded from

Copper chelation therapy in intrahepatic cholestasis of childhood
Table 2 Copper parameters in intrahepatic cholestasis ofchildhood during study period
PlasmaPlasma caerulo- 24h urinecopper plasmin copper(,umolll) (gil) (,imolld)
Patient Pre Post Pre Post Pre Initial Post
1 23-7 27-2 0-42 0.51 - - -2 22-6 27-3 0-40 0-45 0-8 1-9 10-73 33.0 30-1 0-33 0-57 0-8 1-2 1-94 27-8 22-8 0.51 0-41 1*5 4-1 2-25 28-7 12.4 0.51 0.31 1-1 6-4 5-46 27-2 40-8 0-53 0-68 1-3 3-4 6-47 26-7 24-2 0.43 0-3 0-2 1.0 0-78 18-5 - 0-32 - 1-2 3.2 -p value NS NS 001<p<0025
OO5<p<O-lNormal range 15-22 0.25-04 <0.8
Pre = values obtained before D-penicillamine therapy.Initial = mean of three consecutive 24 hour urinary copperexcretions after initiation of D-pencillamine therapy.Post = values obtained in the study after two years' copperchelation. NS = not significant statistically. (Conversion: copper63.5jug= 1 mol.)
IHCC LIVER COPPER
16
14 -
wn 12-0E
o 10-
c:8
U-
Q>I 4
0.
Ciq BINDINGAfter treatment, Ciq binding increased in fivepatients of whom three had normal levels beforetreatment (0.05<p<0. 1) (Table 1).
HISTOLOGICAL ASSESSMENTIn all patients liver sections were assessed before,during, and after two years of treatment (Table 3).After copper chelation therapy there was no
improvement in the liver sections and all histologicalfeatures of necrosis, fibrosis, or bile stainingappeared more obvious at the end of the studydespite marked reductions in hepatic copper levels.Semi-quantitative assessment of copper and copperassociated protein by histochemical staining was notaltered by effective copper chelation with oneexception. In this patient, who died with liver failureafter repeated gastrointestinal haemorrhages, thesehistochemical stains suggested increased amounts ofboth copper and copper associated protein despitesignificant reductions in hepatic copper levels.
Discussion
Hepatic copper levels are increased in intrahepaticcholestasis of childhood from an early age, as inWilson's disease, but there are several featureswhich distinguish abnormal copper metabolism ofthis type of cholestasis from that of Wilson'sdisease.15 This study provides information on therole of copper chelation therapy in intrahepatic
............. ..............-",f. .
Entry 1 yr. 2 yr.
Figure Effect ofcopper chelation therapy on hepaticcopper levels in IHCC (0.05cp<O.1). Dotted arearepresents normal hepatic copper values. Solid linesrepresentperiod ofD-penicillamine therapy. Dashed linerepresents period oftriethylenetetramine dihydrochloridetreatment. Crosses representperiod ofabsent copperchelation in a patient before death. Daggers refer to patients'deaths. (Conversion: copper 63 5,ug=1 ,umol.)
Table 3 Histologicalfeatures in intrahepatic cholestasis bfchildhood after copper chelation (n=8)
Feature Initial 2 years
Necrosis + (4) + (2)++ (4) ++ (6)
+++ (0) +++ (0)Fibrosis + (4) + (0)
++ (4) ++ (8)+++ (0) +++ (0)
Bile + (5) + (5)++ (0) ++ (3)
+++ (O) +++ (0)Bile ducts 0 (4) 0 (5)
a (2) l (2)
Histological features of necrosis, fibrosis, bile in intrahepaticcholestasis of childhood were semi-quantitatively assessed andgraded +, + +, + + + for mild, moderate, or severe changes. Totalamount of fibrosis surrounding and involving hepatic nodules wasestimated after viewing several sections. In each biopsy 12 portaltracts were viewed and bile ducts counted. Bile duct paucity wasconsidered if there were less than four bile ducts counted in 12portal tracts and scored ( J). No bile ducts in 12 portal tracts werescored (0).
45
t
on May 22, 2020 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.24.1.42 on 1 January 1983. D
ownloaded from

Evans, Zerpa, Nuttall, Boss, and Sherlock
cholestasis of childhood with increased liver copperconcentrations.
Intrahepatic cholestasis of childhood is a raresyndrome and the small number of patients did notallow a control group. Thus, the data from the studyhave been interpreted carefully. A historical controlgroup was not included because the severity of thedisorder varies from patient to patient and mayresult from several aetiologies. Did the results fromthis study support a view that increased liver copperconcentrations are an important factor in liverdamage in intrahepatic cholestasis of childhood?The major reductions in hepatic copper concen-trations appeared to be without benefit - that is,there was no symptomatic improvement, a spurt inheight and weight were not observed, and liverdamage progressed. Also, in an earlier report,markedly increased hepatic copper levels wereobserved in three patients with intrahepatic chole-stasis of childhood (before chelation therapy) overperiods ranging from 2-3 years to 6-5 years withoutevidence of deteriorating liver cell function.'" Thisstudy appears to support the second possibility thatprogressive liver damage was independent of livercopper concentration. One patient, with evidence ofdeteriorating liver cell function, died from a massivegastrointestinal haemorrhage and liver copperconcentration before death was normal. A rise inplasma aspartate transaminase and bilirubin levelsoccurred in one patient, while a marked reduction inliver copper values occurred with D-penicillaminetherapy.Under physiological conditions hepatic copper
levels are predominantly maintained by excretion ofcopper into bile.10 The mechanism/s wherebycopper chelation treatment reduced hepatic copperconcentrations in intrahepatic cholestasis of child-hood was not studied directly. Plasma alkalinephosphatase and fasting bile acids, indices ofcholestasis, were not significantly altered bytreatment. Thus it would appear that chelationtherapy did not affect cholestasis and liver coppercontent was reduced by other mechanisms.Recently, D-penicillamine has affected
histological and biochemical improvement inprimary biliary cirrhosis.l1 18 31 The mechanism ofthis beneficial effect is uncertain and may be relatedto copper chelation or an immunological effect (asmeasured by reduced Clq levels). Does this study inintrahepatic cholestasis of childhood, a non-immunological chronic cholestasis disorder ofchildhood, add comment on the D-penicillamineeffect in primary biliary cirrhosis? Despite effectivecopper chelation with D-penicillamine in intra-hepatic cholestasis of childhood liver damageprogressed and levels of Clq binding increased.
Thus, the eneficial effect of D-penicillamine inprimary biliary cirrhosis may be independent ofcopper chelation.
In intrahepatic cholestasis of childhood 24 hoururinary copper excretion- (before treatment) wasincreased but the values observed were less thanthose in Wilson's disease32 or primary biliarycirrhosis." D-penicillamine increased 24 hoururinary copper excretion about two to four times thepretreatment value in most children with intra-hepatic cholestasis of childhood. This response ofurinary copper excretion cannot be compared withpatients with Wilson's disease23 or primary biliarycirrhosis." The dose of D-penicillamine given topatients with Wilson's disease is usually greater than1.0 g dose and therapy generally begins with the fullmaintenance dose, while patients with primarybiliary cirrhosis often achieve a 1.0 g dose ofD-penicillamine after six weeks. After two years ofcopper chelation urinary copper excretion wasincreased but less than at the outset, probablyreflecting a diminished size of the available copperpool. A similar decrease of urinary copper excretionwith time has been observed after treatment ofpatients with Wilson's disease33 and primary biliarycirrhosis."
Despite increased urinary copper excretion in allpatients with D-penicillamine, hepatic copperconcentration increased in one patient in the study.This increase in hepatic copper concentration wasmarked. The explanation for this massive increase isnot clear. The increase was greater thanaccumulation of hepatic copper content with time1sand may be related to several factors including metalcontamination of liver biopsy material; deepeningcholestasis (not apparent); or an effect of D-penicillamine therapy. Likewise, increased livercopper levels of lesser magnitude have been noted insix of 19 patients with primary biliary cirrhosistreated with D-penicillamine.11
This study has shown that both D-penicillamine(10 mg/kg/day) and triethylenetetramine dihydro-chloride (20 mg/kg/day) are effective in reducinghepatic copper levels in intrahepatic cholestasis ofchildhood. Significant side-effects to D-penicillamine occurred in two patients, whilecomplications did not develop with triethylene-tetramine dihydrochloride. Thus, side-effects toD-penicillamine appear common in intrahepaticcholestasis of childhood, primary biliarycirrhosis,"1 31 and rheumatoid arthritis34 but not inWilson's disease. This study did not definitelyexclude the possibility that increased liver copperconcentrations may be toxic to hepatocytes inintrahepatic cholestasis of childhood. Thus, ifcopper chelation is contemplated in intrahepatic
46
on May 22, 2020 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.24.1.42 on 1 January 1983. D
ownloaded from
Copper chelation therapy in intrahepatic cholestasis of childhood 47
cholestasis of childhood with raised liver copperconcentrations, triethylenetetramine dihydro-chloride, which effectively reduced hepatic copperlevels in a patient and did not cause side-effects,should be considered.
Dr J Evans is supported by a Wellcome ResearchFellowship. Professor P J Scheuer contributedsuggestions to the manuscript and Mr S Pocockadvised on statistical analysis. Dr T L Dormandyassayed copper concentrations in plasma and unne.Dr D Flynn advised on interpretation of height andweight percentiles.
References
1 Evans GW. Copper homeostasis in the mammaliansystem. Physiol Rev 1973; 53: 535-70.
2 Sass-Kortsak A, Cherniak M, Geiger DW, Slater RJ.Observations on caeruloplasmin in Wilson's disease. JClin Invest 1959; 38: 1672-82.
3 Cartwright GE, Wintrobe MM. Copper metabolism innormal subjects. Am J Clin Nutr 1964; 14: 224-32.
4 Sternlieb I. Evolution of the hepatic lesion in Wilson'sdisease (hepatolenticular degeneration). In: Popper H,Schaffner F, eds. Progress in liver diseases. New York:Grune and Stratton, 1972: 511-25.
5 Bearn A. Wilson's disease. In: Stanbury JB,Wyngaarden JB, Frederickson DS, eds. The metabolicbasis of inherited disease. New York: McGraw-Hill,1966: 761-9.
6 Chuttani HK, Gupta PS, Gulati S, Gupta DN. Acutecopper sulphate poisoning. Am J Med 1965; 39: 849-54.
7 Todd JR, Gracey JF, Thompson RH. Studies onchronic copper poisoning. I. Toxicity of coppersulphate and copper acetate in sheep. Br VetJ 1962; 11:482-91.
8 Hunt AH, Parr RM, Taylor DM, Trott NG. Relationbetween cirrhosis and trace metal content of liver: withspecial reference to primary biliary cirrhosis andcopper. Br Med J 1963; 2: 1498-1501.
9 Worwood M, Taylor DM, Hunt AH. Copper andmanganese concentrations in biliary cirrhosis of liver.Br Med J 1968; 3: 344-5.
10 Jain S, Scheuer PJ, Samourian S, McGee JO'D,Sherlock S. A controlled trial of D-penicillaminetherapy in primary biliary cirrhosis. Lancet 1977; 1:831-4.
11 Deering TB, Dickson ER, Fleming CR, Geall MG,McCall JT, Baggenstoss AH. Effect of D-penicillamineon copper retention in patients with primary biliarycirrhosis. Gastroenterology 1977; 72: 1208-12.
12 Fleming CR, Dickson ER, Baggenstoss AH, McCallJT. Copper and primary biliary cirrhosis. Gastro-
enterology 1974; 67: 1182-7.13 Fleming CR, Dickson ER, Wahner HW, Hollenhorst
RW, McCall JT. Pigmented corneal rings in non-Wilson liver disease. Gastroenterology 1977; 86: 285-8.
14 Sternlieb I, Harris RC, Scheinberg IH. Le cuivre dansla cirrhose biliaire de l'enfant. Rev Int Hepatol 1966;16: 1105-10.
15 Evans JE, Newman S, Sherlock S. Liver copper levelsin intrahepatic cholestasis of childhood. Gastro-enterology 1978; 75: 875-8.
16 Smallwood RA, Williams HA, Rosenoer VM,Sherlock S. Liver copper levels in liver disease. Studiesusing neutron activation analysis. Lancet 1968; 2:1310-13.
17 Tanner MS, Portmann B, Mowat AP et al. Increasedhepatic copper concentration in Indian childhoodcirrhosis. Lancet 1979; 1: 1203-5.
18 Epstein 0, De Villiers D, Jain S, Potter BJ, ThomasHC, Sherlock S. Reduction of immune complexes andimmunoglobulins induced by D-penicillamine inprimary biliary cirrhosis. N Engl J Med 1979; 300:274-8.
19 Heathcote J, Deodhar KP, Scheuer PJ, Sherlock S.Intrahepatic cholestasis of childhood. N Engl J Med1976; 295: 801-5.
20 Alagille D, Odievre M, Gautier M, Dommergues JP.Hepatic ductular hypoplasia associated with character-istic facies, vertebral malformations, retarded physical,mental and sexual development, and cardiac murmur. JPediatr 1975; 86: 63-71.
21 Clayton RJ, Iber FL, Ruebner RJ, McKusick VA.Byler's disease: fatal familial intrahepatic cholestasis inan Amish kindred. J Pediatr 1965; 86: 1025-8.
22 Watson GH, Miller V. Arteriohepatic dysplasia.Familial pulmonary arterial stenosis with neonatal liverdisease. Arch Dis Child 1973; 48: 459-66.
23 Walshe JM. Copper chelation in patients with Wilson'sdisease. A comparison of penicillamine andtriethylenetetramine dihydrochloride. Q J Med 1973;42: 441-52.
24 Murphy GM, Billing BH, Baron DN. A fluorimetricand enzymatic method for estimation of serum totalbile acids. J Clin Pathol 1970; 23: 594-8.
25 Zubler RH, Lange G, Lambert PH, Miescher PA.Detection of immune complexes in untreated sera by amodified 125Clq binding test: effect of heating on thebinding by Clq by immune complexes and applicationof the test to systemic lupus erythematosis. J Immunol1976; 116: 232-5.
26 Davies UT, Musa M, Dormandy TL. Measurements ofplasma zinc. J Clin Pathol 1968; 21: 359-65.
27 Todd AP, Thorpe MEC, Rosenoer VM. Tissue copperdeterminations by neutron activation analysis. J ClinPathol 1967; 20: 276-9.
28 Lindquist RR. Studies on the pathogenesis of hepato-lenticular degeneration. II. Cytochemical methods forthe localisation of copper. Arch Pathol 1969; 87: 370-9.
29 Shikata T, Uzawa T, Yoshiwara N, Akatsuka T,Yamazaki S. Staining methods of Australia antigen inparaffin section. Detection of cytoplasmic inclusionbodies. Jap J Exp Med 1974; 44: 25-36.
30 Tanner JM, Whitehouse RH, Takaishi M. Standards
on May 22, 2020 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.24.1.42 on 1 January 1983. D
ownloaded from

48 Evans, Zerpa, Nuttall, Boss, and Sherlock
from birth to maturity for height, weight and heightvelocity and weight velocity. British children, 1965 Part2. Arch Dis Child 1966; 41: 613-35.
31 Epstein 0, Lee RG, Ross AM, Jain S, Cook DG,Scheuer PJ, Sherlock S. D-penicillamine treatmentimproves survival in primary biliary cirrhosis. Lancet1981; 1: 1275-7.
32 Sternlieb I, Scheinberg IH. Prevention of Wilson'sdisease in asymptomatic patients. N Engl J Med 1968;
278: 352-9.33 Goldstein NP, Randall RV, Gross JB, Tanxe WN,
McCall JT. Wilson's disease (hepatolenticulardegeneration). Treatment with D-penicillamine andchanges in hepatic trapping of radioactive copper. ArchNeurol 1971; 24: 391-400.
34 Day AT, Golding JR, Lee PN, Butterworth AD.Penicillamine in rheumatoid disease: a long-term study.BrMedJ1974; 1: 180-3.
on May 22, 2020 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.24.1.42 on 1 January 1983. D
ownloaded from