congenital sensorineural hearing loss & imaging - dr. girish s
TRANSCRIPT


IMAGING OF CONGENITAL HEARING LOSS
DR.GIRISH. S

CONGENITAL HL Imaging plays an important role in the evaluation of congenital HL. In children who are candidates for cochlear implantation surgery, it
provides vital preoperative information about the inner ear, 8th nerve, and the brain.
HRCT & MRI provide excellent delineation of the intricate anatomy of the inner ear
CT minute details of osseous structures, and MR imaging fluid-filled spaces & 8th nerve.

IMAGING MR imaging is superior to CT for the identification of an enlarged vestibular
aqueduct. Axial T2-weighted MR imaging - evaluation of any coexistent brain
parenchymal abnormalities.
Together, these complementary modalities can aid decision making about the best management strategy - facilitates the identification and characterization of inner ear malformations and neurologic abnormalities. SURGICAL PLANNING

IMAGING PROTOCOLS

CT EXAMINATIONS Image reconstruction - AXIAL AND CORONAL PLANES - evaluate the inner
ear and its malformations. Axial scanning is performed in planes parallel to the INFRAORBITOMEATAL
LINE.
Multidetector CT scanner, the raw axial image data set can be reconstructed with a section thickness of as little as 0.3 mm.
AXIAL IMAGES top of the petrous apex to the inferior tip of the mastoid bone.
CORONAL REFORMATTED IMAGES anterior margin of the petrous apex to the posterior margin of the mastoid.

HRCT HRCT scans are performed on a 64-slice
volume scanner in a straight axial plane: kV: 140, mA: 350, matrix: 512 × 512
Slice thickness: 0.625 mm/10.63, 0.531:1 Scan field of view (FOV): 32 cm, display FOV:
9.6 cm

HRCT The original isometric volume data is used to obtain Coronal reformatted
images.
The images are reviewed with a high-resolution bone algorithm,
using a small FOV for separate right and left ear
documentation.
Coronal reformations along with 3D maximum intensity
projection (MIP) reconstructions.

MR IMAGING The use of a 1.5- or 3-T MR imaging system is preferred for inner ear
examinations.
T2 weighted - evaluation of the fluid- filled spaces of the membranous labyrinth and the 8TH nerve.
A section thickness of as little as 0.4–0.7 mm is preferred for high quality multiplanar reformatted images.
Routine axial T2-weighted imaging of the brain should be performed in all patients to exclude central nervous system causes of SNHL.
MRI MRI scans are performed on 1.5-T MR with an 8-channel head coil.
Sedation is used in most patients.
A 3D-FIESTA (fast imaging enabling steady-state acquisition) axial
sequence (TR: 5.5, TE: 1.7/Fr, FOV: 16 × 16, slice thickness: 1.0/−0.5, matrix: 320
× 320, NEX: 6.0) is performed.
DIRECT OBLIQUE SAGGITTAL PLANE perpendicular to the VII–VIII nerve complexes

MRI - Constructive Interference Steady State (CISS)
Advantage : Combination of high signal levels andextremely high spatial resolution.

EMBRYOLOGY OF THE INNER EAR
Three primary phases of development include: DEVELOPMENT - weeks 4-8 of life GROWTH - weeks 8-16 of life OSSIFICATION - weeks 16-24 of life

DEVELOPMENT
The Otic placode develops during weeks 4-8 of life, beginning as a plaque of neural ectoderm lying between 1st branchial groove & hindbrain.
Otic Placode

DEVELOPMENT
Otic placode invaginates to form the otic pit.
Otic Pit
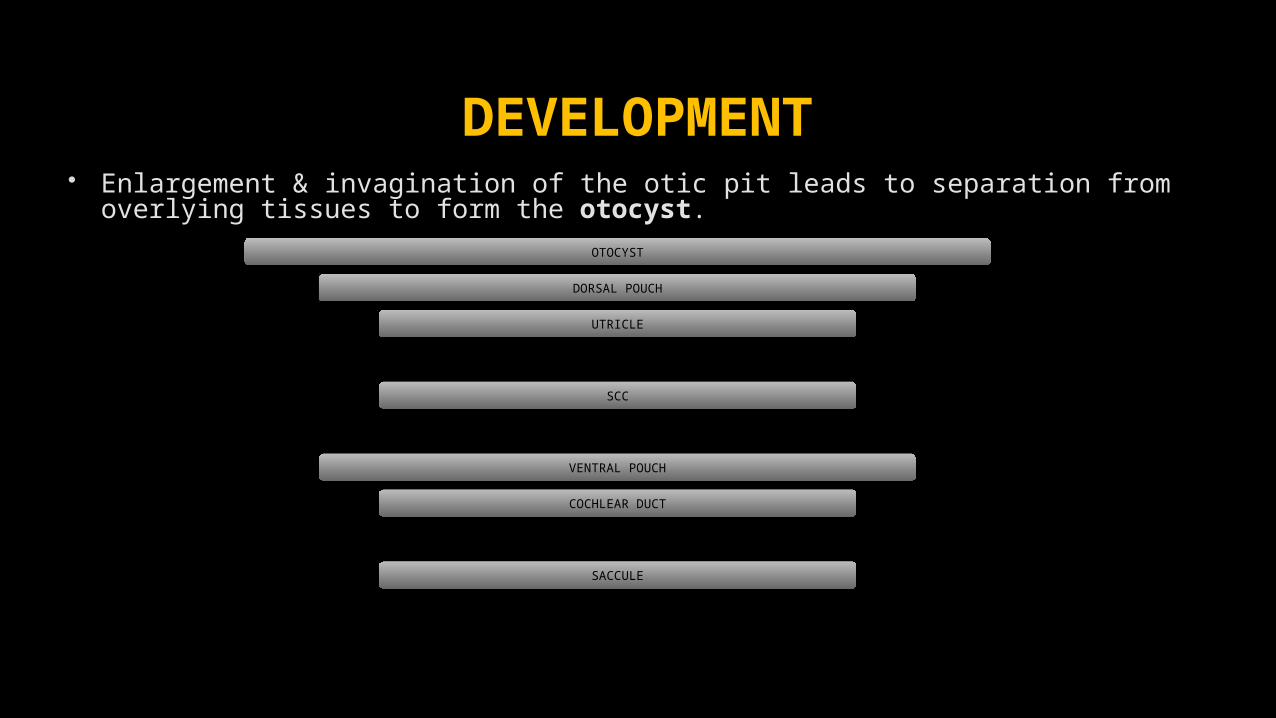
DEVELOPMENT Enlargement & invagination of the otic pit leads to separation from overlying
tissues to form the otocyst.OTOCYST
DORSAL POUCH
UTRICLE
SCC
VENTRAL POUCH
COCHLEAR DUCT
SACCULE


The Endolymphatic duct arises separately.
At end of week 8, membranous labyrinth & cochlea are completely formed
Cartilagenous condensation & ossification begins at this time as well.
DEVELOPMENT

OSSIFICATION Cartilagenous condensation continues. Ossification occurs via 14 separate ossification centers (no growth
plates). Complete by 24 weeks; fetus is then capable of hearing. Ossification complete as endochondral bone.
GROWTH- INNER EAR Occurs between weeks 8-16 of life.

DEVELOPMENT OF THE INNER EAR The inner ear arises from the Otic Placode - early in the 3rd week Cochlea is complete by the 8TH week The vestibule developed 11TH week SCC btwn the 19TH and 22ND weeks Ossification of the labyrinth is complete by the 24TH week The development of the inner ear is complete by the 26TH week.


INNER EAR MALFORMATIONS
Congenital malformations of the inner ear :
(a) malformations that involve ONLY THE MEMBRANOUS LABYRINTH
(b) malformations that involve BOTH THE OSSEOUS AND THE MEMBRANOUS
LABYRINTH
(malformed otic capsules).

Malformations of the Membranous Labyrinth
Complete membranous labyrinth dysplasia (BING- SIEBENMANN MALFORMATION)
Cochleosaccular dysplasia (SCHEIBE MALFORMATION) Cochlear basal turn dysplasia (ALEXANDER DYSPLASIA).
The classification of these abnormalities is not clinically useful, as their differentiation requires histopathologic examination.

Malformations of Both the Osseous and the Membranous Labyrinth
Most such deformities are linked to the gestational age at which the developmental failure or insult occurred .

SENNAROGLU
SAATCI classificati
on

COMPLETE LABYRINTHINE APLASIA MICHEL APLASIA
Most severe form of inner ear deformity Developmental arrest of the otic placode during the 3rd gestational week RARE, only 1% of all inner ear malformations Complete absence of inner ear structures Narrow, atretic IAC is seen on HRCT Eighth cranial nerve is not visualized on MR images May be unilateral or bilateral

MICHEL APLASIA CHARACTERISTIC FEATURES
Hypoplasia of the petrous bone Absence of the round and oval windows Flattening of the medial wall of the middle ear cavity ( LAB.
OSSIFICANS)


Axial 3D-FIESTA sequence shows absence of the entire vestibulo-cochlear structures, bilaterally (arrow), suggesting Michel deformity. The internal auditory canals are small on both sides, with markedly thin eighth nerve (block arrow on left side)

HRCT shows small left internal auditory canal (black arrow) and absence of the entire vestibulo-cochlear structures (white arrow), consistent with Michel deformity

Oblique sagittal 3D-FIESTA sequence, through the small internal auditory canal shows thinned-out eighth nerve (block back arrow), with no divisions and normal facial nerve antero-superiorly (arrow)
COCHLEAR APLASIA Complete absence of the cochlea Due to arrested development of the inner ear in the latter part of the 3rd/5TH
week of gestation It is a rare anomaly, accounting for only 3% Vestibule and SCC are often malformed but may be normal. Dense otic bone is present at the site where the cochlea normally would be
and is best depicted on CT images.

DD: LABYRINTHITIS OSSIFICANS

COMMON CAVITY DEFORMITY developmental arrest in the 4th week of gestation accounts for about 25% of all cochlear malformations. absence of the normal differentiation between the cochlea and vestibule CT and MR images show confluence of the cochlea and vestibule in a cystic cavity
with no internal architecture The width of the cavity is typically greater than its height, with the average
vertical diameter being 7 mm, and the average horizontal diameter, 10 mm. The semicircular canals are frequently malformed but occasionally normal

absence of cochlear nerve
malformed LSCCDialated IAC

TYPE I INCOMPLETE PARTITION CYSTIC COCHLEOVESTIBULAR MALFORMATION Developmental arrest in the 5th week of gestation MODIOLUS is entirely absent; the cochlea has a cystic appearance; and the
vestibule is often dilated, forming FIGURE EIGHT. Vestibular aqueduct is normal. Cribriform area between the cochlea and IAC is often defective All patients have a large IAC predisposing them to increased risks for
meningitis and for a perilymphatic gusher in the event of surgery

FIGURE EIGHT
COCHLEAR HYPOPLASIA Aberration in the development of the cochlear duct during the 6th week of
gestation Accounts for 15% of cochlear malformations. At CT and MR imaging, a small cochlear bud of variable length (usually 1–3
mm) is seen protruding from the vestibule and an abnormally small IAC may be seen.
Although the cochlea is visible, it has only one turn or a partial turn. The vestibule and semicircular canals are usually malformed but may be
normal.
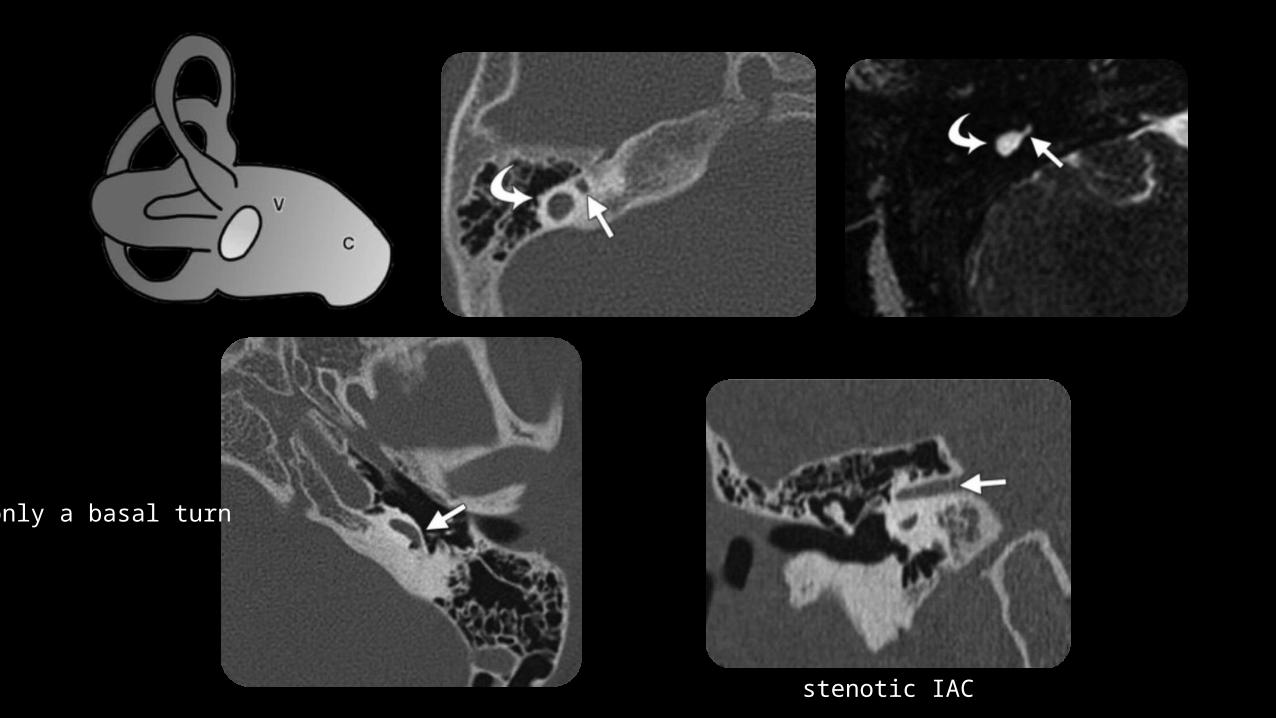
stenotic IAC
only a basal turn
BRANCHIOTORENAL SYNDROME Leads to cochlear hypoplasia / aplasia , LVA, Ossicular chain
abnormalities & Cochear nerve hypoplasia. + preauricular sinus.

TYPE II INCOMPLETE PARTITION MONDINI DEFORMITY
developmental arrest in the 7th week of gestation most common type, >50% of all cochlear Cochlea consists of 1½ turns, and the interscalar septum and osseous
spiral lamina are absent. The basal cochlear turn appears normal, but the middle and apical turns
coalesce to form a cystic apex. The modiolus is present only at the level of the basal turn.

TRIAD IN MONDINI DEFORMITY Cochlea with a normal basal turn and cystic apex Enlarged vestibular aqueduct and vestibule Normal semicircular canals


MALFORMATIONS OF THE VESTIBULE AND SEMICIRCULAR CANALS

APLASIA OF THE SEMICIRCULAR CANALS
Development of SCC btn the 6th and 8th weeks Completed btwn the 19th and 22nd weeks .
The superior SCC develops first, and the lateral SCC develops last.
Hence, malformation of the superior and posterior semicircular canals without involvement of the lateral canal is unusual.
The malformed canals are usually short and wide but may be narrow.

LATERAL SCC –VESTIBULE DYSPLASIA In extensive malformations, the vestibule is dilated and forms a common
lumen with the lateral canal .

Absence of all semicircular ducts CHARGE SYNDROME
Isolated aplasia of the posterior semicircular duct WAARDENBURG SYNDROME ALAGILLE SYNDROME

HRCT confirms the diagnosis of semicircular canal aplasia.
APLASIA and FIBROUS/CALCIFIED obliteration of the canals have the same appearance at MR imaging.
CT - SCC is absent in cases of aplasia, whereas a normal canal is seen in cases of fibrous obliteration (since fibrous tissue cannot be seen at CT) and calcifications within the canal are seen in cases of Labyrinthitis ossificans

LARGE VESTIBULAR AQUEDUCT Enlarged endolymphatic duct and sac Most frequent CT / MR imaging finding in patients with early-onset SNHL. Most frequent inner ear malformation Bilateral in as many as 90% of cases Asymmetric, and is slightly more common in females

CT - enlargement of the osseous vestibular aqueduct. MR imaging, the characteristic feature is enlargement of the endolymphatic
duct and sac. The vestibular aqueduct is considered enlarged when its diameter midway
between the common crus and the external aperture is greater than 1.5 MM on CT images

The fluid containing posterior semicircular duct also has a diameter of approx 1.5 mm, and
its ascending portion is situated anterior and parallel to the endolymphatic duct and sac.
Endolymphatic duct and sac enlarged when their diameters exceed that of the posterior
semicircular duct on thin-section T2-weighted gradient-echo images.


Mild Enlargement of Vestibular Aqueduct and Cochlear Dysplasia
CT: The opening for vestibular aqueduct is enlarged. The cochlea is dysplastic with fusion of its middle and apical turns.
MRI: Axial CISS image shows enlarged endolymphatic sac with high T2 signal.

LARGE ENDOLYMPHATIC SAC
MRI: T2 axial image shows enlarged aqueducts (white arrows) and a very large right sac. The cochleas are dysplastic..

MARKEDLY ENLARGED ENDOLYMPHATIC SACS
MRI: Axial CISS image demonstrates markedly enlarged enolymphatic sacs bilaterally.

PENDRED SYNDROME An enlarged vestibular aqueduct is frequently
seen. Characterized by congenital SNHL and goiter.
IAC AND COCHLEAR NERVE ANOMALIES Normal diameter of the IAC ranges from 2 to 8 mm, with an average of 4
mm.
IAC with a diameter of less than 2 mm is described as stenotic.
IAC may also be atretic or may have a bony septum that partitions it into
two or more separate canals.

Morphology and size of the IAC are not reliable indicators of the integrity of
the cochlear nerve
Normal size of the IAC and normal inner ear anatomy do not exclude a nerve
deficiency
High-resolution MR imaging is the preferred modality for accurate
assessment of the cochlear nerve.

COCHLEAR NERVE ANOMALIES SAGITTAL OBLIQUE IMAGES obtained in a plane perpendicular to the long
axis of the IAC four major nerves of the IAC
Three types of cochlear nerve anomalies have been described : TYPE 1 Cochlear nerve anomaly TYPE 2A Cochlear nerve anomaly TYPE 2B Cochlear nerve anomaly

COCHLEAR NERVE ANOMALIES TYPE 1 cochlear nerve anomaly, a STENOTIC IAC is seen with an absent
eighth nerve
TYPE 2 anomaly, A Common Vestibulocochlear Nerve is found, with
hypoplasia or aplasia of its cochlear branch.
Associated with other inner ear malformations type 2A malformation.
Anomaly occurs in isolation type 2B
malformation.


Oblique sagittal - shows the facial and vestibular nerves in their normal location, with the cochlear nerve barely or almost not seen in the anteroinferior quadrant.

HYPOPLASIA OF THE BONY CANAL OF THE COCHLEAR NERVE
COCHLEAR APERTURE is a small canal at the fundus of the IAC through
which the cochlear nerve passes to enter the cochlea
Here the site of the cochlear aperture is filled by bone.
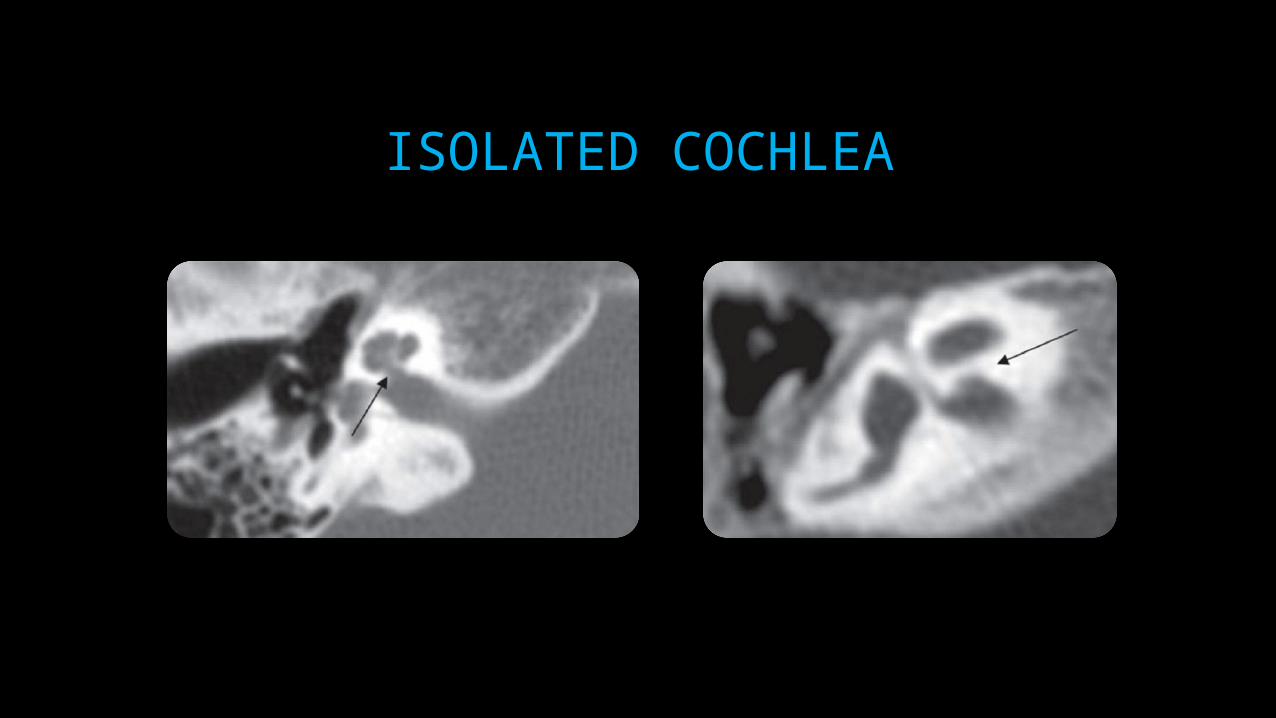
ISOLATED COCHLEA

BRAIN ABNORMALITIES Posterior fossa abnormalities such as asymmetric dilatation of the fourth
ventricle and arachnoid cysts has been observed among patients with complete labyrinthine aplasia .
Neuronal migration abnormalities in children with congenital sensorineural hearing loss also have been described .

(a)Axial T2- weighted MR image obtained in a child with complete labyrinthine aplasia shows an arachnoid cyst.
(b) Axial T2-weighted MR image obtained in another child with congenital SNHL shows focal white matter signal abnormalities

CMV INFECTION
Congenital cytomegalovirus infection leads to
SNHL in many infant populations.
The discrete foci of white-matter signal
abnormality that are frequently seen on MR
images obtained in children with SNHL have
been attributed to CMV at birth.
IMPLICATIONS OF IMAGING ABNORMALITIES FOR COCHLEAR
IMPLANTATION

CONGENITAL INNER EAR MALFORMATIONS
RAMOS ET AL classified Congenital inner ear malformations:
(A) gross malformations constituting surgical contraindications
(B) major malformations contributing to increased risks for
complications,
(C) minor malformations.
GROSS MALFORMATIONS Gross malformations such as
COMPLETE LABYRINTHINE APLASIA, COCHLEAR APLASIA n COCHLEAR
NERVE DEFICIENCY are contraindications for cochlear implantation surgery.
Patients in whom the cochlear nerve is not seen on MR images—
the nerve is too slender to discern
its fibers parallel those of the vestibular nerve and are inseparable from it.

MAJOR MALFORMATION Major malformations like COMMON CAVITY or SEVERE HYPOPLASIA
-result of cochlear implantation is often difficult to predict.
Severe malformations - higher intraoperative risks
Cerebrospinal fluid leakage
Post implantation meningitis
Potential electrode displacement.

MINOR MALFORMATIONS Minor malformations
Partition defects such as hypoplasia,
Abnormalities of the aqueduct, and
Abnormalities of the vestibule.
If bilateral malformations are found, the surgeon will want to know which
inner ear has the more normal structure and the larger cochlear nerve
HRCT Gives info regarding
inner ear malformations other anatomic variants might affect surgical
decision making. status of the external and middle ear
HRCT FEW ANATOMIC VARIANTS - when planning cochlear implantation surgery
ABERRANT COURSE OF THE CAROTID ARTERY
HIGH-RIDING OR DEHISCENT JUGULAR BULB
ABERRANT COURSE OF THE FACIAL NERVE
DEHISCENT FACIAL NERVE CANAL

CONGENITAL CONDUCTIVE HEARING LOSS
CONG. AURAL ATRESIA Are often associated with ossicular chain anomalies. Inner ear abnormalities are less frequent. EAC may be stenotic or truly atretic membraneous /
bony Often malleus n incus are fused into one malformed
ossicle Course of facial nerve is often abnormal – 2nd genu n
mastoid segment are frequently diasplaced anteriorly.



OTHER CAUSES LATERAL CHAIN FIXATION
Bony bridge btwn malleus head/ body incus lateral wall of attic
CONGENITAL STAPES FIXATION CT nl/ thickening of footplate. Wide IAC with enlarged connection to entrance
of cochlear nerve ( HABENULAE PERFORATA) OVAL / ROUND WINDOW ATRESIA


Thank You… !

SEMICIRCULAR CANAL DEHISCENCE(SSCD)
Rare cause of conductive hearing loss . SSCD introduces a 'third' window into the inner ear which produces the
airbone gap (1) shunting air-conducted sound away from the cochlea, thus elevating air
conduction thresholds (2) increasing the difference in impedance between the scala tympani and
scala vestibuli, thus improving thresholds for bone-conducted sound

BILATERAL SSCD• Reformatted sagittal- oblique CT
image through the left semicircular canal shows full size of the dehiscence.
STAPES FIXATION Juvenile otosclerosis Treacher collins Klippel-feil Pfeiffer Branchio-oto-renal Ear pits-deafness Cervico-acoustic syndromes Crouson X linked mixed deafness with
gusher Osteogenesis imperfecta

CHOLESTEATOMA Accumulation of desquamated keratin epithelium in the middle ear cleft or
any other pneumatized portion of the temporal bone. Imaging demonstrates non dependant soft tissue in the Prussack's space
with scutum, ossicle or lateral epitympanic wall erosion. CT is performed to look for extent and complications of
cholestatoma( labyrinthine fistula, tegmen erosion etc). Surgery is treatment of choice with follow up to look for recurrance

• middle ear soft tissue with ossicular destruction
• soft tissue in mastoid with erosion of bony septae

COCHLEAR OTOSPONGIOSIS Also know as RETROFENESTRAL OTOSCLEROSIS. Replacement of normal endochondral bone with Haversian bone, most likely
secondary to an inciting inflammatory event. Female predominance with majority of cases bilateral. Appears in second to third decade of life. Presents as focal or diffuse demineralization of the otic capsule with
abnormal enhancement.

COCHLEAR OTOSPONGIOSIS. CT: Coronal and axial images demonstrate diffuse demineralization of the otic capsule.

COCHLEAR OTOSPONGIOSIS
MRI: T1 axial and coronal post-contrast images demonstrate abnormal signal in the otic capsule