circulation researchcircres.ahajournals.org/content/circresaha/49/3/557.full.pdf · osmotic...
TRANSCRIPT

Circulation Research SEPTEMBER 1981
VOL. 49 NO. 3
An Official "Journal of the American Heart Ansociation
BRIEF REVIEWS
Capillary Fluid FiltrationStarling Forces and Lymph Flow
AUBREY E. TAYLOR
STARLING (1894, 1896) described the basic forcesresponsible for producing fluid shifts between thecirculating blood and the surrounding tissue spaces.On page 324 of his classical article entitled "On theabsorption of fluids from the connective tissuespaces," Starling described how capillary pressuredetermines transudation into the tissues and theosmotic pressure of the proteins determines absorp-tion from the tissues. The paper also investigatedhow tissue pressure affects absorption, and Starlingcame to the correct conclusion that tissue pressurewould not cause fluid to be absorbed from the tissueunless this pressure was not transmitted to theveins. Starling also recognized that a small amountof fluid was lost continually from the circulation("frictional resistance of the capillary wall") andformed lymph, but believed that this was small andthat the forces tending to move fluid out of and intothe circulation were almost balanced. Finally, Star-ling postulated that tissue colloidal osmotic pres-sure decreased following elevation of capillary pres-sure and provided the opposing forces to limit tran-sudation of fluid into interstitial spaces. Thus, Star-ling defined the basic forces responsible for main-taining fluid balance between the microcirculationand interstitium, and physiologists have termedtissue pressure (Pt), capillary pressure (Pc), plasmacolloidal osmotic (TTP), and tissue colloidal osmotic(wt) pressure as Starling forces. However, a mathe-matical relationship between those forces was notformulated by Starling in his original papers. Staub(1978) presents a delightful discourse concerningthe historical development of the mathematical de-scription of the Starling hypothesis:
P c - P t = 77p - TTt.
From the Department of Physiology, College of Medicine, Universityof South Alabama
Address for reprints: Aubrey E. Taylor, Ph D, Professor and Chair-man, Department of Physiology, College of Medicine, University of SouthAlabama, Mobile, Alabama 366SS
Received July 25, 1980; accepted for publication May 26, 1981.
Staub indicates that the equation was written forthe first time by Iverson and Johansen in 1929,although Landis (1927, 1928), who measured capil-lary pressure for the first time, produced a regres-sion equation which related Pc — 77C to capillaryfiltration rate. Perhaps the most extensive reviewon this subject was presented by Landis in hisclassical review of 1934 in which he discussed notonly the forces, but also how the tissue forceschanged to oppose increases in venous pressure("margin of safety;" Krogh et al., 1932).
Until the more recent work of Guyton and col-leagues (Guyton, 1963; Guyton et al., 1966, 1975)and Wiederhielm (1967, 1972), who introduced theconcept of a subatmospheric interstitial fluid pres-sure and the physiochemical nature of the intersti-tium, respectively, scant attention had been paid tothe interstitium and how forces generated withinthis space affect fluid movement between capillaryand interstitial fluids. From the early 1960's untilthe present, the amount of work in this area hasincreased severalfold, and several excellent experi-mental models have been developed in which Star-ling forces can be estimated at very controlled anddefined physiological states (Garlick and Renkin,1970; Staub, 1971; Gibson, 1974; Drake, 1975; Mor-tillaro and Taylor, 1976; Chen et al., 1976; Grangeret al., 1977; Parker et al, 1978, 1979; Grega et al.,1979).
The objective of this review is not to tabulate themany estimates of tissue pressure, capillary pres-sure, plasma colloid osmotic pressure, tissue colloidosmotic pressure, and lymph flows which have beenpublished over the last twenty years, but to presentstudies in which most of the variables affecting fluidmovement have been measured at well definedsteady states within a single preparation at differenttissue fluid volumes. As this review develops, itshould become increasingly clear that the Starlingforces and lymph flow, like all physiological param-eters, are dynamic, and it is difficult, if not impos-sible, to discuss fluid volume movement across cap-
by guest on June 5, 2018http://circres.ahajournals.org/
Dow
nloaded from

558 CIRCULATION RESEARCH VOL. 49, No. 3, SEPTEMBER 1981
illary walls when only one or two forces responsiblefor the flows are measured. Because of the natureof Starling forces and lymph flow, it is more relevantphysiologically to evaluate how these forces arealtered at different states of tissues swelling than topresent the various published arguments concern-ing their normal values in a variety of mammaliantissues. For the interested reader, there are fourexcellent review sources for these basic argumentsoriginating from the laboratories of Guyton (Guy-ton et al., 1968, 1971) and Wiederhielm (1972, 1979).
The present review begins with a basic discussionof an idealized capillary-tissue fluid exchange sys-tem in which the behavior of each Starling forceand lymph flow is described as fluid enters theinterstitium. A brief description of how each forceis estimated in each tissue bed is later developed tofacilitate data interpretation. The review then fo-cuses on how the Starling forces are altered duringedema formation in several different tissue bedsand what interpretative problems are associatedwith these published findings. Finally, the reviewdevelops possible directions for future researchwhich should lead to an extension of our basicknowledge concerning the control of fluid balanceat the capillary-tissue level.
Fluid Balance: Capillary-Tissue-LyxnphaticSystem
Capillary walls are pierced by many types ofopenings which can serve as conduits for fluidmovement between capillary fluid and the sur-rounding tissues. Most capillary walls are usuallydescribed as continuous but having a few openingsbetween endothelial cells (lung, skeletal muscle,etc.). The brain capillaries appear to have no openjunctions and are referred to as 'tight junction"capillaries. Other capillaries are described as fen-estrated and have very thin diaphragms interspacedbetween endothelial cells (intestinal, bronchial, glo-merular, etc.). Finally, other types of capillary wallsare described as being discontinuous with very largeopenings appearing in their walls (liver, spleen). Forthe purpose of this presentation, only an idealizedcapillary wall will be used to describe fluid move-ment in different organs, but in the real system,fluid can cross the capillary walls through junctionsbetween endothelial cells, through the endothelialcells, or through larger leaks in microvessel walls(Bennet et al., 1959).
The evaluation of Starling forces in any capillary-tissue system requires that tissue volume (orweight), lymph flow, lymph and plasma colloid os-motic pressure, tissue pressure, capillary pressure,and capillary permeability characteristics be mea-sured in a single preparation. More importantly, acomplete analysis requires that all forces and flowsbe in a steady-state and the tissue volume notchange with time. At the present time, these param-eters can be measured simultaneously only in iso-lated, perfused organ systems. The reader can easily
appreciate that each organ's capillary structure isdifferent, depending on its functional role, and toadd more complexity to the problem, most organscontain several distinctly different capillary systems(e.g., intestine: mucosa, submucosa, smooth muscle;lungs: pulmonary-different zones, bronchial, etc.)Therefore, a true description of the actual phenom-ena which occur at each capillary wall cannot beascertained using data determined in total organs.The Starling forces and lymph flows presented inthis review will necessarily represent average organvalues which obviously are gross oversimplificationsof the real system. However, the data collected inorgan systems are extremely useful for describingthe overall fluid balance at a given tissue volumeand provide us with the only means presently avail-able for assessing the behavior of the capillary-tissue-lymphatic system in intact organ systems(Mellander et al., 1964; Wallentin, 1966; Levine etal., 1967; Mellins et al, 1969; Taylor et al., 1973).
Definition of Starling ForcesFigure 1A represents the idealized capillary, in
this case, surrounded by a tissue reservoir with alymphatic system draining the tissues. In this sys-tem, the volume flow occurring across the capillarywalls (Jv) can be described by (Pappenheimer andSoto-Rivera, 1948; Kedem and Katchalsky, 1958):
Jv = Kfc [(PL - Pt) - ad(77p - TTi)]; (1)
where Kfc is the filtration coefficient of the capillarywall (volume flow/unit time per 100 g tissue perunit pressure), Pc is the capillary pressure, Pt is theinterstitial fluid pressure, np is the colloid osmoticpressure of plasma, assuming that all plasma pro-teins can be described in terms of a single species,77, is the colloid osmotic pressure ot the tissue fluids,and <Td is the osmotic reflection coefficient of allplasma proteins. ad is equal to 1 if the capillary wallis impermeable to the colloid and is equal to zero ifthe membrane is freely permeable to the colloid.
Equation 1 represents a stationary state equationwhich requires all forces, Pc, Pt, 7rp and 77,., to be atsteady state values and Kfc and a constant for agiven condition.
Capillary Pressure (Pc)In Figure 1A, the pre- and postcapillary resist-
ances are depicted as inflow and outflow resistancesbecause these parameters determine capillary pres-sure. Capillary pressure has been measured experi-mentally by using direct cannulation procedures(Landis, 1927; Wiederhielm, 1967; Zweifach and In-taglietta, 1968) and estimated indirectly by measur-ing gravimetric pressures in isolated organs (Pap-penheimer and Soto-Rivera, 1948; Johnson andHanson, 1966; Gaar etal., 1967; Diana and Laughlin,1974). Obviously, many hormones, drugs, etc. affectvascular resistance, so capillary pressure is variablefrom moment to moment in all capillary beds. Forthe remainder of this discussion, we will allow cap-
by guest on June 5, 2018http://circres.ahajournals.org/
Dow
nloaded from
STARLING FORCES/Taylor 559
A .CAPlLLAflY + TISSUE *• LYMPHATIC SYSTEM
VOCUdE FLOW
ACROSS CAPILLARY
LYHPH FLOW
WALL
LYMPH
FLW [<Pc " PT> '
EXAMPLES: M I S C L E , S K I N , J O I N T S
B -CAPILLARY TISSUE LYMPHATIC OVERFLOW SYSTEM
LYHPH
FLOW
^ \ _ ^ / OVERFLOW
* SYSTFJ1
VOLUME FLOW
ACROSS CAPILLARY
WALL
LYMPH FLOW + OVERFLOW SYSTEM
EXAMPLES- LUNC, - A L V E O L I , INTESTINE - LUHEHJ
KIDNEY - URINE, L IVER - ASCITES
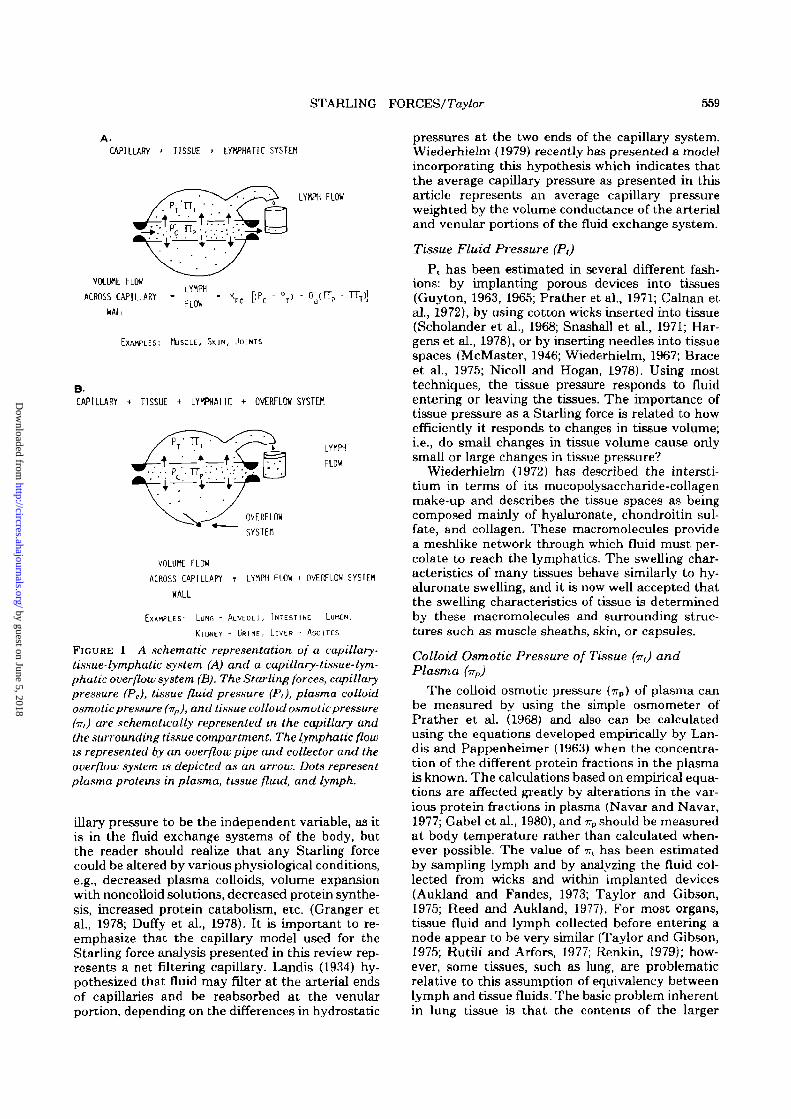
FIGURE 1 A schematic representation of a capillary-tissue-lymphatic system (A) and a capillary-tissue-lym-phatic overflow system (B). The Starling forces, capillarypressure (Pc), tissue fluid pressure (Pi), plasma colloidosmotic pressure (-np), and tissue colloid osmotic pressure(TT,) are schematically represented in the capillary andthe surrounding tissue compartment. The lymphatic flowis represented by an overflow pipe and collector and theoverflow system is depicted as an arrow. Dots representplasma proteins in plasma, tissue fluid, and lymph.
illary pressure to be the independent variable, as itis in the fluid exchange systems of the body, butthe reader should realize that any Starling forcecould be altered by various physiological conditions,e.g., decreased plasma colloids, volume expansionwith noncolloid solutions, decreased protein synthe-sis, increased protein catabolism, etc. (Granger etal., 1978; Duffy et al., 1978). It is important to re-emphasize that the capillary model used for theStarling force analysis presented in this review rep-resents a net filtering capillary. Landis (1934) hy-pothesized that fluid may filter at the arterial endsof capillaries and be reabsorbed at the venularportion, depending on the differences in hydrostatic
pressures at the two ends of the capillary system.Wiederhielm (1979) recently has presented a modelincorporating this hypothesis which indicates thatthe average capillary pressure as presented in thisarticle represents an average capillary pressureweighted by the volume conductance of the arterialand venular portions of the fluid exchange system.
Tissue Fluid Pressure (P,)
P, has been estimated in several different fash-ions: by implanting porous devices into tissues(Guyton, 1963, 1966; Prather et al., 1971; Calnan etal., 1972), by using cotton wicks inserted into tissue(Scholander et al., 1968; Snashall et al., 1971; Har-gens et al., 1978), or by inserting needles into tissuespaces (McMaster, 1946; Wiederhielm, 1967; Braceet al., 1975; Nicoll and Hogan, 1978). Using mosttechniques, the tissue pressure responds to fluidentering or leaving the tissues. The importance oftissue pressure as a Starling force is related to howefficiently it responds to changes in tissue volume;i.e., do small changes in tissue volume cause onlysmall or large changes in tissue pressure?
Wiederhielm (1972) has described the intersti-tium in terms of its mucopolysaccharide-collagenmake-up and describes the tissue spaces as beingcomposed mainly of hyaluronate, chondroitin sul-fate, and collagen. These macromolecules providea meshlike network through which fluid must per-colate to reach the lymphatics. The swelling char-acteristics of many tissues behave similarly to hy-aluronate swelling, and it is now well accepted thatthe swelling characteristics of tissue is determinedby these macromolecules and surrounding struc-tures such as muscle sheaths, skin, or capsules.
Colloid Osmotic Pressure of Tissue (TT,) andPlasma (vp)
The colloid osmotic pressure (wp) of plasma canbe measured by using the simple osmometer ofPrather et al. (1968) and also can be calculatedusing the equations developed empirically by Lan-dis and Pappenheimer (1963) when the concentra-tion of the different protein fractions in the plasmais known. The calculations based on empirical equa-tions are affected greatly by alterations in the var-ious protein fractions in plasma (Navar and Navar,1977; Gabel et al., 1980), and 77P should be measuredat body temperature rather than calculated when-ever possible. The value of TT, has been estimatedby sampling lymph and by analyzing the fluid col-lected from wicks and within implanted devices(Aukland and Fandes, 1973; Taylor and Gibson,1975; Reed and Aukland, 1977). For most organs,tissue fluid and lymph collected before entering anode appear to be very similar (Taylor and Gibson,1975; Rutili and Arfors, 1977; Renkin, 1979); how-ever, some tissues, such as lung, are problematicrelative to this assumption of equivalency betweenlymph and tissue fluids. The basic problem inherentin lung tissue is that the contents of the larger
by guest on June 5, 2018http://circres.ahajournals.org/
Dow
nloaded from

560 CIRCULATION RESEARCH VOL. 49, No. 3, SEPTEMBEH 1981
perivascular and peribronchial spaces do not seemto be well mixed. At high lymph flows, this does notconstitute any real problem, but at normal andslightly elevated lymph flows, the mixing effectcould cause a substantial problem (Nicolaysen etal., 1975; Gutyon et al, 1976; Gee and Havill, 1980).
Lymph Flow (LF)When the tissue is neither gaining nor losing
weight, the amount of fluid leaving the capillary isexactly equal to lymph flow. Lymph flow has beenmeasured in several organs by simply measuringthe flow from a lymph vessel draining the organutilizing either calibrated pipettes or lymph weigh-ing procedures. From estimates of lymph flows atdifferent tissue steady states, the Starling forces'balance can be estimated (Johnson and Richardson,1974; Erdmann et aL, 1975; Chen et al., 1976; Taylorand Drake, 1977; Mortillaro et al., 1976; Laine et al.,1979; Richardson et al., 1979). It is well appreciatedthat lymphatics remove proteins from the tissuespaces, yet their capability to oppose tissue volumeexpansion following increases in capillary filtrationis variable among tissues.
Volume Overflow SystemsIn several organs, another system serves as a
means of removing excess tissue fluids and perhapspreventing excessive interstitial swelling—an over-flow system which is depicted schematically in Fig-ure IB. When excessive fluid enters the interstitiumin organs such as lung, intestine, and liver, fluid canbegin to enter the alveoli, intestinal lumen, andperitoneal cavity, respectively (Guyton and Lind-sey, 1959; Staub, 1974; Yablonski and Lifson, 1976;Granger et al., 1977; Laine et al., 1979). However, atleast two fluid systems, the brain and eye, do notpossess lymphatics and their normal drainage sys-tems are best described as an overflow system. Thearachnoid granulations and the canal of Schlemmrepresents the only means by which fluids andtissue protein can be removed from the brain andeye, respectively (Davson, 1960; Rapoport, 1976;Bradbury, 1979).
Filtration Coefficient (K/JThere are two coefficients used to describe the
Starling relationship: the filtration coefficient (Kf,c)and the reflection coefficient (aa). KffC is equal tothe product of the hydraulic conductance of themembrane (Lp) and the surface area of the organ(S). The hydraulic conductance of the capillarymembrane is equal to: NCr*/AXn; where N is thenumber of pores per cm2, C is a constant, r is theradius of the filtering pores, AX is the thickness ofthe capillary wall, and n is the viscosity of thefiltering fluid. Lp is a membrane parameter and isindependent of exchange surface area; however, theKf.c estimated for capillary beds is a function ofavailable surface area. Since different organs pos-
sess different capillary densities, then Kf,c may bequite different among organs, yet their Lp's may besimilar. Also, within the same organ, Kfc may in-crease or decrease because of closure or opening ofmore capillaries with similar conductance charac-teristics.
Kfc has been shown to change 4-fold in someorgans (Johnson and Hanson, 196S; Mortillaro andTaylor, 1976). Although usually a 2-fold change inKfc represents the maximal change associated withthis parameter (Granger et al., 1976; Richardson etal., 1979; Granger et al., 1979a), there is little doubtthat changes in effective surface area can greatlyalter fluid movement into the tissue spaces, inde-pendent of alteration in Starling forces (Haglundand Lundgren, 1972). The methods for measuringKfc in organs rely on weighing isolated organs andanalyzing their weight transients after imposing acapillary pressure change. The range of Kf-C esti-mates from several laboratories are: 0.07-0.25 forlung, 0.08-0.24 for intestine, 0.010-0.015 for skeletalmuscle, and 0.2-0.3 for colon in units of ml/min permm Hg per 100 g.
The importance of Kr,t as it relates to fluid bal-ance is as follows: if the total lymph flow drainingan organ is known as well as the filtration coeffi-cient, then the imbalance in Starling forces (APL)can be estimated when the tissues are not changingvolume by the following equation:
APLtotal lymph flow
K;(2)
•r.c
where APL = (Pc — Pt) — OdiiTp — ni). Some inves-tigators have also used Equation 2 to estimate Kf.t.By measuring or calculating all the Starling forcesand collecting total organ lymph flow, Kf(. can besolved for in Equation 2 provided that the organ isnot losing or gaining weight (Erdmann et al., 1975).Equation 2 points out a very important relationshipbetween lymph flow and its ability to buffer changesin capillary pressure. If Kf,c is small, then smalllymph flows may be important in preventing exces-sive build-up of tissue fluids; however, if Kfc is large,then even large lymph flows may not representimportant volume overflow systems. The point toremember concerning the importance of lymph flowin fluid balance regulation is not the absolute mag-nitude of lymph flow but the lymph flow relative toKf,c. The relationship described by Equation 2 de-termines the lymphatic's ability to remove filteredfluid following changes in capillary pressure ratherthan the absolute magnitude of lymph flow (Nicolland Taylor, 1977; Taylor and Drake, 1977).
For the case of an overflow system (Figure IB),the AP operating across the capillary wall must berelated to the sum of total organ lymph flow plusthe volume flow escaping the tissues via the over-flow system (VOF)
by guest on June 5, 2018http://circres.ahajournals.org/
Dow
nloaded from

STARLING FORCES/Taylor 561
For tissues such as intestine and liver, VOF may beconsiderable following elevations of tissue pressure(Laine et al., 1979), and VOF can be a considerableportion of the lymphatic safety factor relative tointerstitial swelling.
Reflection Coefficient (Sd)
Until very recently, neither the mathemtical ap-proach nor the experimental data were available forestimating the reflection coefficient in any capillarysystem. In the last 3 years, the correct mathematicalapproach and empirical methods have been devel-oped to estimate aa in several organs using lymphprotein fluxes (Patlak et al., 1963; Taylor et al.,1977; Brace et al., 1977a; Brace et aL, 1978; Grangerand Taylor, 1980). The basic approach for assessingthe reflection coefficient is derived from the equa-tion relating the lymph to plasma ratios of a partic-ular plasma protein at different lymph flow states:
CL/C,, =
J L
— CTd
1 —(3)
where x = (1 - od) — (Granger and Taylor, 1980)
and where CL and Cp refer to the concentrations inlymph and plasma of the particular protein, JLrefers to the lymph flow, and PS refers to thepermeability coefficient surface area product. Equa-tion 3 states that the lymph to plasma ratio willapproach 1 — od at high volume flow states whenthe denominator approaches one. Using this theo-retical approach, ad has been obtained for totalplasma proteins and several protein fractions in anumber of organ systems by increasing lymph flowuntil CL/C P is essentially constant. When CL/C P isconstant, the reflection coefficient can be estimatedby:
= 1 - CL/C P . (4)
For total plasma proteins, aa appears to be 0.7 —0.95 for intestine (Granger and Taylor, 1980), lung(Parker et al., 1980), hindpaw (Rutili et aL, 1979),and colon (Richardson et al., 1980). However, ad isclose to 0 for liver sinusoids (Granger et al., 1979b)and has not been evaluated in other capillary beds.For the basic Starling equation to correctly predictvolume flow, the measured Aw acting across thecapillary wall should be multiplied by the appropri-ate value of ad. However, caution should be usedwhen applying this simple logic because the capil-lary permeabilty may be altered by different exper-imental procedures. For example, in the small in-testine histamine reduced od from 0.93 to 0.6 (Mor-tillaro et al., 1979). Therefore, aa must be measuredin each preparation before the effective Air acrossthe capillary wall can be evaluated relative to fluidvolume regulation.
Changes in Starling Forces FollowingElevation in Capillary Pressure
Figure 2A is a schematic representation of eventsthat occur in an idealized capillary bed when cap-illary pressure is elevated. Tissue pressure in-creases, lymph flow increases, and tissue colloidosmotic pressure decreases, but tissue volume doesnot change greatly. These forces change to accom-modate the increased capillary pressure, and theability of these forces to change and offset altera-tions in capillary pressure has been described as the"edema safety factor" (Guyton and Coleman, 1968;Taylor et al., 1973) and the "margin of safety"(Krogh et al., 1932). When the forces can no longerchange, a great amount of fluid will enter the tissuesfor only small changes in capillary pressure; i.e., theedema safety factors are overwhelmed.
Figure 2B represents an overflow tissue systemin which Pl( ITU and lymph flow change to somedegree following elevation of capillary pressure andthen the overflow system becomes operative. Ob-
A.
TTT DECREASES
IMTERST1TAL V0LUM£
INCREASES
LYMPH
FLOW
INCREASES
VHEM P T , TTT AND LYTIPH FLOrf CANHOT CHANGE FURTHER,
THEN EITHER THE TISSUES CONTINUE TO SWELL UNOPPOSED,
OR A SAFETY VALVt WILL OPEH AND FLUID WILL FILL
POTENTIAL SPACES SUCH AS PERITONEAL CAVITY, ALVEOLI.
ETC.
FIGURE 2 Effects of increasing capillary pressure on acapillarytLssue-lymphatic (A) and a capillary-tissue-lymphatic overflow (B) system. This figure depicts whatoccurs when the Starling forces and lymph flow can nolonger buffer the increases in capillary pressure and thetissues swell in the capillary-tissue-lymphatic system (A)and the overflow valve opens in the overflow system (B).
by guest on June 5, 2018http://circres.ahajournals.org/
Dow
nloaded from

562 CIRCULATION RESEARCH VOL. 49, No. 3, SEPTEMBER 1981
viously in lung, fluid-filled alveoli are de-trimental to blood oxygenation; in intestine, fluidentering the lumen opposes the active absorptionprocess and increases in ascitic fluid formationcause large losses of solute and water from theplasma. However, it may well be necessary to pro-tect the liver interstitium against excessive tissueswelling because of its metabolic functions. Al-though ascitic fluid formation is abnormal, it mayserve as a safety factor as far as the liver-tissuevolume is concerned (Laine et al., 1979).
Tissue PressureWhen tissue pressure is measured, by whatever
means, it has been found to behave as shown inFigure 3. At low capillary pressure changes, tissuefluid pressure changes markedly for only smallchanges in tissue volume. However, when the tis-sues begin to swell excessively, tissue pressure doesnot change greatly in most beds even when largeamounts of fluid accumulate in the tissues (Guyton,1965; Guyton et al., 1975; Mortillaro and Taylor,1976; Chen et al., 1976; Parker et al., 1978). Thisbehavior has been observed in many tissue bedsand is related to the swelling characteristics of theinterstitium (Wiederhielm, 1972). As volume beginsto enter the interstitium, only small volume changesare necessary to raise tissue pressure (low tissuecompliance; compliance = AV/AP). However, as thetissues expand, tissue elements expand more easilyand large amounts of fluid enter the interstitium(high compliance) (Guyton, 1965). In capillary bedswith overflow systems, such as the alveoli in lung,the amounts of fluid which can accumulate in thesepotential spaces are tremendous. Conversely, or-gans which do not possess overflow systems mayrespond by producing very high tissue fluid pres-sures. This condition is seen in skin before somestress relaxation occurs in the tissue. As fluid firstbeings to accumulate in the leg, the skin is very taut
TISSUE
oncoTicPRESSURE
TISSUE
VOLUTE
TISSUE PRESSURE
(PT>
EITHER A HIGH DEGREE OF
TISSUE EDEMA (SUBCUTANEOUS)
OB OPENING Of OVERFLOW
SYSTEM (ALVEOCAR EDEMA)
FIGURE 3 Effect of increasing capillary filtration (or-dinate) on tissue pressure (P,). Note that P, changesgreatly at lower filtration rates, indicating a low inter-stitial compliance (&V/&P). At high capillary filtrationrates, tissue fluid pressure changes are small (high tissuefluid compliance). Therefore, P, can change to opposethe filtration for small changes in tissue volume. How-ever, as the tissues swell, P, can only change when largefluid volumes enter the interstitium.
IHCBEASED CAPILLAPV
RERMABILITf
, FLUID ENTERING TISSUES
REPRESENT A TRUE
CAPILLARY FILTRATE
CAPILUWf FILTRATION
FIGURE 4 Effect of increasing capillary filtration ontissue oncotic pressure. The solid line represents thechanges associated with a capillary bed that is slightlypermeable to plasma proteins. The dotted line representsa capillary that is more leaky to plasma proteins thanthat described by the solid line.
and high tissue pressures oppose further filtration.However, with time, the pressure causes the skin tobecome more elastic and the tissue pressure de-creases, which results in greater tissue fluid accu-mulation.
Tissue Oncotic PressureFigure 4 demonstrates how tissue colloid osmotic
pressure behaves as capillary pressure is increasedacross an idealized capillary wall. As filtration pro-ceeds, tissue oncotic pressure will decrease until itfinally attains values associated with a true capil-lary filtrate. This behavior has been observed in allcapillary beds studied, with the exception of theliver. The decrease in 7rt increases the magnitude ofthe second term in the Starling equation [tJd {irP —77t)] and thus buffers the change in capillary pres-sure. The liver is an interesting organ in regard tochanges in irt with filtration because the changesare opposite to those observed in other tissues (i.e.,77i actually increases with increasing filtration). Thisfinding has been interpreted as indicating that theliver tissue limits the movement of proteins betweenlymph and capillaries at normal tissue hydrationstates. When the tissues swell, the interstitial matrixno longer restricts protein movement and the fluidentering the lymphatics approaches the concentra-tion in plasma (Granger et al., 1979b; Laine et al.,1979). If capillaries become "leaky," then irt will notchange to the same extent as observed in normalcapillaries when filtration is increased (dottedlines). This phenomenon has been demonstrated inlung (Brigham et al., 1974; Brigham and Owen,1975a; Brigham et al., 1976), hindpaw (Rutili et al.,1979), and intestine (Granger etal., 1980) followingadministration of histamine, Pseudomonas, and insome cases, Escherichia coli endotoxin. In mostcapillaries, 77t decreases when filtering forces areincreased; however, any factor which tends to in-crease capillary permeability to plasma proteinswill certainly affect this phenomenon and decreasethe effectiveness of Trt in opposing capillary filtra-tion. Moreover, the importance of the second termin the Starling equation will be diminished evenfurther when the capillary wall becomes leakier to
by guest on June 5, 2018http://circres.ahajournals.org/
Dow
nloaded from

STARLING TORCES/Taylor 563
plasma proteins because, not only will 77t be larger,but od will be smaller; i.e., the effect is not simplyadditive, but amplified.
Why does wt decrease when filtration is increasedabove normal values? There are several mecha-nisms responsible for the decreased tissue colloidosmotic pressure: (1) a simple dilution of tissueproteins occurs due to the filtration of a relativelyprotein-poor fluid into the tissues, (2) a bulk re-moval of tissue proteins by the lymphatics occurswhen fluid enters the tissues, and (3) a change inthe volume of distribution of tissue proteins occursat higher tissue volumes. All three mechanisms areoperative in different capillary beds, and their spe-cific contribution to the overall decrease in 77, isvariable (Drake, 1975; Chen et al., 1976; Granger,1979; Parker et al., 1980).
Lymph FlowIn most organs, lymph flow increases when cap-
illary pressure is elevated, but the magnitude ofchange varies greatly from tissue to tissue. Figure5 schematically represents the experimental find-ings from several different capillary beds. Lymphflow appears to increase linearly with increasedcapillary filtration in most organs, reaches a plateauat high filtration rates (subcutaneous tissue, mus-cle), or actually decreases at high tissue volumestates (intestine, lung). Since lymph flow is pro-pelled by either tissue motion or intrinsic lymphaticpumping ability and rilled by the tissue pressure-lymphatic pressure gradient, it is evident that thelymphatic system can respond differently at differ-ent hydration states (Casley-Smith, 1977). Basi-cally, the lymphatics finally must reach their max-imum flow rate, but this may not be attainable insome organs. However, the lymphatics do attain amaximum flow rate in subcutaneous tissue (hind-paw) unless the observed effect is due simply to theincreased tissue pressure somehow retarding lymphflow.
The decrease observed in lymph flow at hightissue hydration states occurs in intestine (Granger
LYMPH
FLOW
( L F )
PLATEAU BECAUSE OC
WATERFALL EFFECT, OR
LYMPHATIC HA/IMUH
""OVERFLOW VALVE HAS
OPEUED
CAPILLARY FILTRATION
FIGURE 5 Effect of increasing capillary filtration onlymph flow (LF). In some capillary beds, lymph flowappears to be a linear function of filtration. In othercapillary beds, the lymph flow attains a plateau, or anoverflow value opens which causes lymph flow to de-crease.
et al., 1977) and lung (Parker et al., 1979) and issomehow related to opening of mucosal and alveolarmembranes, respectively, with a concomitant de-crease in tissue pressure which decreases the lym-phatic filling pressure. The possibility exists thatopening of an overflow system causes the resultinginterstitial spaces to behave like a balloon. Theeffect is described mathematically by the Laplacerelationship between radius and wall tension. Ba-sically, if the tissues behaved as a balloon, theninitially, a large change in pressure would resultfrom only small changes in tissue volume; then thepressure may well decrease as the volume increases(a negative compliance) until a critical volume isreached at which the pressure again rises. Thiseffect has been described in detail as it applies toalveolar stability and explains how a small volumeballoon can empty into a larger volume balloon.The possibility does exist that a negative compli-ance portion of the interstitium exists, especially ifthe organ demonstrates a Laplace effect. This pos-sibility has not been examined specifically but, ifoperative, could explain why lymphatic flow de-creases at high tissue volume states in some over-flow systems.
Finally, it should be emphasized that lymph flowcan increase to tremendous values [90 times controlin right duct lymph following decreases in plasmaproteins (Gee and Spath, 1980)]. Yet, when capil-lary pressure is increased in steps and lymph flowmeasured at each steady state, the high valueswhich are associated with the non-steady state mea-surements never are attained by the system. In fact,Chen et al. (1977) have published a very interestingarticle along these lines. Chen's study revealed thatlymph flow increased immediately after elevationsof capillary pressure, but that lymph flow decreasedto values roughly two-thirds of the maximal valueafter a few minutes. This effect was even morepronounced at high capillary pressures. They inter-preted these findings as indicating that lymph flowincreases in response to the rate of change in tissuepressure, not in response to its absolute value. Sincetissue compliance usually increases with hydration,more volume must be filtered to change the tissuepressure, and this would explain the lower lymphflows relative to those obtained when tissue pres-sure was changing greatly in the low compliancerange. However, the failure of lymph flow to main-tain its highest possible flow rates when the tissuesare in an edematous state is a very puzzling obser-vation relative to fluid volume regulation. Why doeslymph flow not maintain its maximal value to pro-vide the tissues with a better volume overflowmechanism as predicted by theory rather than de-creasing to lower values? Perhaps future researchrelative to how tissue forces affect the behavior ofthe lymphatic system will provide the necessaryinformation to answer this important physiologicalquestion.
by guest on June 5, 2018http://circres.ahajournals.org/
Dow
nloaded from

564 CIRCULATION RESEARCH VOL. 49, No. 3, SEPTEMBER 1981
Changes in Starling Forces Associated withIncreased Capillary Pressure
The following examples of Starling force analysisin various tissue beds represent portions of studiesin which rather large changes in capillary forces(>20 mm Hg) were imposed on the organ by alteringcapillary pressure. These selected studies will em-phasize primarily the maximal change which canoccur in tissue pressure, tissue colloidal osmoticpressure, and lymph flow before excessive tissueedema occurs. However, in most analyses presentedin this section, other tissue hydration states alsowere studied which demonstrated that the contri-bution of each Starling force to the total opposingforce may be different at lower tissue hydrationstates. In each organ, tissue volume, lymph flow,and lymph and plasma colloid osmotic pressurewere measured when the organ neither lost norgained weight, lymph flow was constant, and lymphprotein was unchanging for a defined period of time(usually 30-50 minutes). In some instances, capil-lary pressure, tissue pressure, the filtration coeffi-cient, and the reflection coefficient were also mea-sured. Once these parameters were considered to bein a steady state, the venous pressure was elevatedto increase capillary pressure and the parameterswere again measured after the system had attaineda new steady state. The contribution of Pt, ad (TTP— ?7t), and lymph flow to the overall ability of thetissues to oppose changes in capillary pressure andprevent excessive edema, the total edema safetyfactory, can then be evaluated from the data.
Small IntestineFigure 6, A and B, represents estimates of the
changes observed in lymph flow (LF, dotted histo-gram), colloid osmotic pressure gradient (T7P — m,striped histogram), and tissue pressure (Pt, clearhistogram) relative to the total increase in capillarypressure imposed on two different intestinal prep-arations. In both experimental models, the Starlingforces increased sufficiently to provide a bufferingcapacity (or edema safety factor) equal to the im-posed change in capillary pressure. The percent ofthe total change in Starling forces is shown for eachparameter on the ordinate, and the pressure equiv-alent of each force change is shown under eachhistogram.
In the work of Mortillaro and Taylor (1976) (Fig.6A), capillary pressure was increased by 20 mm Hgin a cat ileal preparation. The change in tissuecolloids provided 50% of the tissue force changeopposing filtration, whereas increased lymph flowand tissue pressure provided 20 and 30% of thecounterbalancing force, respectively. Figure 6B rep-resents the findings from Johnson and Richardson's(1974) study, which was conducted on an isolateddog ileal preparation. Capillary pressure was in-creased by 9 mm Hg, and the major portion of thecapillary pressure change was buffered by the in-
A.
ISAFETY
FACTOR
00,
75
50
25
INTESTINE
TT.-TTLF ' T p
1
INTESTIKE
100
75
50-•
25 1NORTILLARO AND TAYLOR
COLON
1.5 7.5 (0)
J0WJ5ON AND R1CHARD5OH
D.
100
I 75SAFETY
50FACTOR
25
VALUE (H/HQ)
LFTTp-r
I0.5 6.2
RICHARDSOfl ET
5,3
Al
100-I
75
50'
25-
nf,-
niLF
|
10 0
PT
FIGURE 6 A replot of Starling force and lymph flowanalyses from the intestinal studies of Mortillaro andTaylor (1976) (A) and Johnson and Richardson (1974)(B), the colon study of Richardson et al. (1980) (C), andthe liver study of Laine et al. (1979) (D). The % of thetotal safety factor for each Starling force is representedby histograms. Lymph flow (LF) is represented by adotted histogram; the colloid osmotic pressure gradient(itp — ttt) is represented by a striped histogram, andtissue fluid pressure (PJ is represented by a clear his-togram. In each study capillary pressure was changedby the sum of the numbers shown on the abscissa. Thenumbers below each histogram represent how muchforce changed (in mm Hg). For each study at least twosteady state measurements were made: (I) at normalcapillary pressures, and (2) at relatively high capillarypressures.
creased colloid osmotic pressure gradient actingacross the capillary wall. Lymph flow can be esti-mated to provide approximately 20% of the tissue'sability to buffer the increased capillary pressure inthis study.
The reason that different tissue pressures areobtained in two similar studies of intestine is notclear at the present time, but it could be the resultof several different factors. (1) P, was estimated inMortillaro's study using the Starling equation (P,and Od were the only parameters in the Starlingequation not measured in this study). If the reflec-tion coefficient differed from unity, then the calcu-lated Pt would be in error. It now is well known thatfat absorption increases capillary permeability inthe small intestine. In fact, aa decreased from 0.9 to0.7 during fat absorption (Granger and Taylor,1978). If permeability was changing during thecourse of the experiment, then the P, calculation
by guest on June 5, 2018http://circres.ahajournals.org/
Dow
nloaded from

STARLING FORCES/Taylor 565
would be in error. (2) Pt was measured in Johnsonand Richardson's study using a needle. Brace et al.(1975) have shown recently that a needle will notfollow tissue pressure changes except under verycontrolled conditions. Therefore, the actual tissuepressure may have been different from that mea-sured using the needle method. (3) The possibilityalways exists that different species have differentmeans of providing fluid balance control. However,Granger and Taylor (1980) have demonstrated re-cently that the lymphatic protein concentrationdecreases to 10% of plasma levels when venouspressure is elevated to 30 mm Hg in the cat intes-tine, and this is similar to the colloid osmotic pres-sure changes observed in Johnson and Richardson'sstudy. (4) The magnitude of volume absorption inthe small intestine greatly affects Pi and irx. Forinstance, if the tissues were absorbing in eitherstudy, then w, would be expected to behave in adifferent fashion since absorption will increase thetissue volume and also dilute tissue proteins. In-creasing capillary pressure in an absorbing or vol-ume expanded state will result in different behaviorof 77t (Granger and Taylor, 1978). (5) The increasein capillary pressures was quite different betweenthe two studies: 9 vs. 20 mm Hg. However, Mortil-laro also estimated Starling forces at other hydra-tion states and at the same capillary pressure rangeas studied by Johnson and Richardson, and thetissue proteins did not decrease to the same extent.Thus, it appears that the differences observed be-tween these two studies could be explained by dif-ferent capillary permeabilities and tissue hydrationstates existing in the preparations, but a more com-plete description of how the intestine behaves dur-ing edema formation requires further study. Themost important finding in these investigations isthat studies from different laboratories, using simi-lar tissues, demonstrate that the Starling forces dochange to oppose increased filtration, although dif-ferent mechanisms ultimately may be responsiblefor the final force balance.
Colon and LiverFigure 6, C and D, represents Starling force anal-
yses conducted on colon and liver preparationswhen capillary pressure was altered by 12 and 24mm Hg, respectively. In the colon preparation usedby Richardson et al. (1980) (Fig. 6C), lymph flowdid not provide a substantial safety factor and onlythe increases in the colloid osmotic pressure gra-dient and tissue pressure changed to provide theopposing forces.
Since the liver sinusoids are extremely permeableto plasma proteins, nc — irt was not changed whencapillary pressure was altered in the study of Laineet al. (1979) (Fig. 6D). In liver, lymph flow and/orascites formation provides 40% of the tissue's re-sponse to increase capillary filtration. Surprisingly,tissue pressure increases to levels which provide60% of the retarding force.
Thus, no generalizations can be made from thestudies presented in this section, except to pointout that 77P — 77t appears to be the most importantchange in the Starling forces occurring in the gas-trointestinal tract following elevations of capillarypressure. However, it must be emphasized that admust be measured for each tissue at each hydrationstate before inferences can be made concerning theactual osmotic effect of decreasing tissue proteinconcentrations. Tissue pressure changes provide amajor portion of the safety factor in the data pre-sented in Figure 6, A, C, and D, and it is unclear atthe present time why this was not demonstrated inthe data from Johnson and Richardson's study.Lymph flow appears to provide some buffering abil-ity in all tissues, with the exception of the colonwhere it is quite clear that the lymphatic systemdoes not provide any force relative to volume re-moval.
LungFigure 7, A and B, represents Starling force anal-
yses performed on lung tissue. Figure 7A showsdata replotted from the study of Erdmann et al.(1975) which was conducted in the intact sheepmodel developed by Staub (1971, 1978).
In this study, lymph flow and lymph and plasmacolloid osmotic pressures were measured and cap-illary pressure was calculated using the equationdeveloped empirically by Gaar et al. (1967, 1968).Using these measurements, the only two forceswhich changed to oppose the capillary filtrationwere the increased lymph flow and colloid osmoticpressure gradient.
Figure 7B is a representation of the data fromthe work of Drake (1975) who estimated the Star-ling forces in isolated dog lungs. Lymph flow, lymphand plasma colloid osmotic pressure, the filtrationcoefficient, and isogravimetric capillary pressurewere measured in each preparation. Using thesevalues and assuming that the reflection coefficient= 1, Pt could be calculated using Equation 1. Again,it is evident that the major force which changes tooppose capillary filtration is the decrease in tissue
ISAFETY
FACTOR
100
75
50
25
1 0 0 ,
75-
50-
25
ERDI1AMN ET »L
5 6 7
DRAKE AND TAYLOR
FIGURE 7 Plot of the data obtained by Erdmann et a I(1975) (A) and Drake and Taylor (1977) (B) from sheepand dog lungs. The data representation Li described inthe legend of Figure 6 and the text.
by guest on June 5, 2018http://circres.ahajournals.org/
Dow
nloaded from

566 CIRCULATION RESEARCH VOL. 49, No. 3, SEPTEMBER 1981
colloids (50%) while lymph flow and tissue pressureincreases provide approximately 25% each to thetissue's ability to buffer changes in capillary pres-sure.
There is excellent agreement between Erdmann'sand Drake's studies relative to the changes ob-served in tissue colloid osmotic pressure. Drake'sstudy indicates that both lymph flow and tissuepressure play a role in opposing capillary pressurechanges, whereas only the former appeared to beimportant in the intact sheep lung studies. Severalother investigations have employed the sheepmodel to evaluate changes in capillary permeability,and an analysis of these data indicates that lymphflow and the osmotic pressure changes are the im-portant factors opposing edema formation in thatmodel (Brigham et al, 1974; Brigham and Owens,1975b; Bland et al., 1977; Malik, 1977). It appearsthat the differences observed between the studiesconducted in sheep and dog lungs can only beresolved when all Starling forces are measured in asingle preparation. To accomplish this in intactanimals is difficult at the present time; yet, newtechniques should make this type of study possiblein the very near future.
Nordin et al. (1978) recently measured vascularpressures, tissue pressure, and tissue and plasmacolloidal osmotic pressure in bronchial tissues usingmicrotechniques. From this study the authors builtan interesting fluid balance model for bronchialtissue. The model predicts how the capillaries pro-vide the fluid which accompanies the Cl transportoccurring across the bronchial epithelium to formthe bronchial fluid layer. Moreover, these investi-gators also were able to analyze the effects of lungheight on interstitial fluid accumulation in bron-chial tissue as it related to capillary filtration. Al-though some measurements reported in this studyare open to serious arguments, they do indicate themagnitude of the Starling force changes and providea great deal of information with which to describethe physiology of a very complex capillary-tissue-lymphatic system. Studies of this type are neededfor all organ systems in order that the exact mech-anism of fluid exchange can be assessed at themicrocirculatory level. However, many technicallimitations exist, and experimental designs must beimproved before assessments of fluid volume con-trol can be accomplished at the microcirculatorylevel in lung tissue.
It also is important to point out that differentinvestigators recently have applied Starling forceanalyses as a means of evaluating the effects ofvarious pathophysiological states on lung fluid dy-namics (Bland et al., 1977; Malik, 1977; Demling,1978). This approach certainly indicates the direc-tional changes of the forces and constitutes animportant experimental method to study lung fluidbalance. Although qualitative in nature, this ap-proach does provide a great deal of insight into themechanisms associated with lung fluid balance and
will serve as the basis for the design of more com-plete Starling force balance studies in intact lungmodels.
Finally, Drake et al. (1980) have developed meansto determine the total edema safety factor in intactdog lungs. They have defined a "critical capillarypressure" by extending the observations made byGuyton and Lindsey (1959) that left atrial pressuremust be increased to approximately 25 mm Hgbefore the lung gains weight at a continuous rate.In the experimental model used by Drake et al., anintact dog lung is weighed continuously, and leftatrial pressure is elevated until the lung gainsweight at a constant rate. The pressure at whichthe lung gains weight in a continuous fashion hasbeen termed the "critical capillary pressure." This"critical pressure" then can be used to interprethow efficiently the Starling forces can change indifferent pathological and physiological conditionssince the "critical pressure" represents the totaledema safety factor. If the lung capillaries are leakyto plasma proteins, then the "critical capillary pres-sure" will decrease. By measuring the "critical pres-sure," lymph flow, and lymph colloids, the contri-bution of these forces in opposing filtration forceshas been established by the investigators in severalpathological conditions (Gabel et al., 1978).
Hindlimb and HindpawFigure 8, A and B, represents the data obtained
by Brace et al. (1975) and Chen et al. (1976) forhindlimb and hindpaw preparations, respectively.Brace measured lymph and plasma colloid osmoticpressure and tissue pressure using implanted cap-sules when capillary pressure was increased by 7mm Hg. From these measurements, they deducedthat changes in Starling forces were confined totissue pressure (70%) and osmotic gradient (30%)effects. Obviously, without a measurement of lymphflow and capillary permeability (both Kf,c and od),it is difficult to assess the importance of each Star-ling factor and lymph flow in this particular study.
HIND PAH
np-TTTI
SAFETY
FACTOR
100
75-
50
25
HIND LIMB 100,LF " ' " " T p
T 75
50.
25-
VALJE (M«HG)
BRACE ET «L
7 4 18
CHEN ET AL
FIGURE 8 Plot of the Starling force analyses from thestudies of Brace et al. (1977b) (A) and Chen et al. (1976)(B) conducted in dog hindlimb and hindpaw, respec-tively. The data representation is described in the legendof Figure 6 and text.
by guest on June 5, 2018http://circres.ahajournals.org/
Dow
nloaded from

STARLING FORCES/ Taylor 567
The study of Chen et al. represents the onlycomplete study published to date relative to de-scribing all Starling forces and lymph flow at severaldifferent tissue hydration states. They measuredlymph flow, the filtration coefficient, tissue pres-sure, lymph and plasma colloidal osmotic pressure,and the capillary pressure at three different statesof fluid hydration. Chen's findings are very similarto those observed by Brace et al. over the samecapillary pressure range. But Chen's data obtainedat higher capillary pressures indicates two veryimportant mechanisms relative to fluid volume reg-ulation in subcutaneous tissue. First, w, is low inboth hindpaw and hindlimb; therefore, this factorcannot change as greatly as has been observed inother tissues which contain high concentrations oftissue proteins. Secondly, since w, can change byonly 5-6 mm Hg, tissue pressure must absorb mostof the change in capillary pressure in organs forwhich tissue proteins cannot change greatly, espe-cially at high capillary pressures. Lymph flow alsomay provide a substantial buffering capacity inthese types of organs provided that K^ is small Itis of interest to note that tissue pressure changes 15mm Hg as capillary pressure is increased from 12.8to 38.0 mm Hg. Since the hindpaw is a dependentregion, it appears that the low compliance of thetissues provides an additional safety factor which isnot present in many tissues; i.e., the lower compli-ance characteristics of the hindpaw at relativelyhigh tissue volume states prevents excessive fluidfrom entering the tissues even at rather high capil-lary pressures, which is not the case for most organs.
Other OrgansI will not review the extensive literature concern-
ing the Starling force estimates made in the kidney.There are several excellent reviews on this subject(Brenner et al., 1976; Brenner and Humes, 1977;Essig and Caplan, 1979; Robertson, 1980), but thekidney poses some very interesting and physiologi-cally important questions: How do the Starlingforces behave in postglomerular capillaries? Whatdifferences exist between upper cortical vs. lowercortical capillaries? What types of capillary dynam-ics are present in the vasa recta? These are all veryimportant questions and presently are under exten-sive investigation in several laboratories throughoutthe world.
The evaluation of Starling forces in the nervoussystem also has seen new and exciting experimentalapproaches. A simple model presented 4 years agoindicated that essentially no Starling forces hadbeen measured in the brain at that time (Taylorand Granger, 1976). The only Starling force knownwith any certainty at that time was the colloidosmotic pressure of brain interstitial fluid, which isessentially zero. The article pointed out that: (1) afew interstitial fluid pressures had been measuredin brain tissue, but the results ranged from -7 mmHg to the positive cerebrospinal fluid pressure; (2)
the brain fluid is composed of different fluid com-partments, i.e., cerebrospinal fluid, white and graymatter, etc., which may have different swellingcharacteristics; (3) the fluids in various brain inter-stitial compartments are the results of active pro-cesses (choroid plexus), capillary filtration and cellswelling, not just capillary filtration alone; and (4)since the brain parenchymal capillaries are notpermeable to most solutes, the crystalloid osmoticpressure gradient across the capillary wall would bean important regulator of tissue fluid volume.
That article stimulated several new studies in thearea including two that have shown how tissuepressure, fluid conductance pathways, and crystal-loids (as well as colloids) provide safety factors inbrain tissue which oppose edema formation (Ra-poport, 1978, 1979). Although the brain is an ex-tremely difficult organ with which to work, severalinvestigators Eire now measuring interstitial pres-sures and fluid conductance pathways during var-ious phases of brain edema (Marmarou et al., 1975;Marmarou and Shulman, 1976; Bruce, 1978; Mar-marou et al., 1978). Future studies using techniquesdeveloped in other organ systems should provideestimates of brain Starling forces, fluid drainagepatterns, tissue fluid formation, and osmotic effects,not only within the vascular system, but also rela-tive to how crystalloids in the tissues buffer in-creases in capillary pressure (Rapoport, 1979).
Complete Starling force and lymph flow analyseahave not been conducted in other tissues. Fluidbalance studies usually were confined to measuringone or two Starling forces in a particular organbecause of technical limitations. In most instances,the tissue hydration states and capillary permeabil-ity estimates were not investigated, and these pa-rameters must be evaluated before a complete fluidbalance study can be interpreted in any organ sys-tem. As can be seen from this section, interpreta-tions of data using only a few of the four Starlingparameters are extremely difficult. In some in-stances a particular force may not change duringedema formation and the force can rightly be ig-nored in an overall fluid balance analysis. However,each force must be evaluated experimentally ineach organ system before eliminating it as a com-ponent of the tissue's edema safety factor.
Functional StudiesVery recently, a few studies have appeared which
indicate the responsiveness of the Starling forcesand lymph flow in different functional states. Forexample, the data from Granger and Taylor's (1978)study indicate that the absorptive force increasesacross the capillary wall when the ileum is absorb-ing fluid, since the transported volume contains noprotein and 77t decreases. This A77 change providesthe major force allowing the capillaries in the intes-tine to remove the majority of the absorbed volume.The intestinal capillary permeability to plasma pro-teins also increased in this study. Therefore, the
by guest on June 5, 2018http://circres.ahajournals.org/
Dow
nloaded from

568 CIRCULATION RESEARCH VOL. 49, No. 3, SEPTEMBER 1981
Xe£
CC
(ftUJCC
0"d (TTp - T T L )
I I CONTROL
EZ3 GLUCAGON
INTESTINE
GRANGER «t ol
FIGURE 9 Plot of Starling force analyses from the stud-ies of Granger et al. (1980) conducted in a cat intestinalpreparation. The clear histograms refer to P,, LF, andoj(iTp — -TTL) for controls and the striped histograms referto the same parameters measured after the infusion ofglucagon into the intestinal circulation. The ordinaterepresents the value of each parameter (mm Hg). Notethat tissue pressure increased from negative to positivevalues and lymph flow was not greatly changed. Od(wp
— -nL) actually decreased, which indicates an increasedcapillary permeability to plasma proteins and reflectsboth a decreased ad and an increased TTL followingglucagon infusions.
effect of changing ATF on capillary fluid exchangewas not as great as would be predicted using normalvalues for the protein reflection coefficient.
Figure 9 represents another recent functionalstudy by Granger et al. (1980). In this study, lymphflow and all Starling forces (with the exception ofPt) were measured, and in addition, both the filtra-tion and reflection coefficients were measured ateach tissue hydration state. The control values ofPt, LF, and ffd^p — "i) shown as clear histograms,then were compared to those measured followinginfusions of glucagon, shown as hatched histograms.Tissue pressure increased by 6 mm Hg, lymph flowincreased but not significantly, and ad(wP — wt)actually decreased, indicating that glucagon in-creased the capillary permeability to plasma pro-teins. In fact, in these studies, the intestine was"secreting" rather than absorbing during the glu-cagon infusions. Therefore, this study indicates thatglucagon, a physiological hormone, affects the Star-ling forces and indirectly affects net volume trans-port across the intestinal mucosa.
The use of Starling force analysis for evaluatingfunctional states of organs represents an importantnew area of research, and only by designing studiesof this nature can the fluid balance in differentorgans be related to its physiological function. Forexample, in the two studies cited above, the changein ad allows the investigator to more fully interpret
the change associated with A-n\ It is now becomingmore apparent that Starling forces may behavequite differently when both functional and patho-logical conditions have changed within any partic-ular organ system. Therefore, future studies alongfunctional lines should greatly enhance our knowl-edge concerning the interaction of Starling forces,not only in opposing edema formation but also asthey relate to altered functional roles in differentphysiological and pathological conditions.
Interpretation of Starling Force StudiesFor the purpose of placing the preceding Starling
force analyses into their proper perspectives, it isimportant to consider how the Starling forces be-have at both normal and expanded tissue volumestates. The study conducted by Chen et al. (1976)in dog hindpaw contains sufficient data to beginthis discussion. Using values obtained for Pt, Pr,7TP, 7TL, and lymph flow and assuming ad = 1, thefollowing Starling relations are obtained:
Force imbalance
[(Pc - Pt) - (ATT)]Kf,
Force imbalance
Jv= = [12.8 - (-4.7)] -(20.9 - 3.8)
Kf.r
= 0,4 mm Hg;(Normal tissue volume, normal lymph flow)
Force imbalance
= — = [24.8 - (-0.1)] - (20.9 - 1.6)Kf.c
= 5.6 mm Hg;
(AV = 1.7 ml/100 g; LF = 10X control)Force imbalance
= — = [37.9 - (+10)] - (20.9 - 0.5)Kf,c
= 7.5 mm Hg.
(AV = 17.5 ml/100 g; LF = 13x control)
At normal tissue hydration states, the forces arenear a balance point. Only a small driving forceexists across the capillary wall, which representsthe normal lymph flow factor. The tissue volume isexpanded only slightly when capillary pressure isaltered by 12 mm Hg; the change in tissue pressure(4.6 mm Hg) and the decreased tissue colloids (2.2mm Hg) compensate to oppose the increased filtra-tion tendency of the capillary. The imbalance inforces at this hydration state is 5.6 mm Hg, whichrepresents the lymph flow safety factor. At thislevel of capillary pressure, no visible edema waspresent; in fact, the tissues had only gained 1.7 ml/
by guest on June 5, 2018http://circres.ahajournals.org/
Dow
nloaded from

STARLING FORCES/Teryto/" 569
100 g, which represents approximately a 10% changein interstitial volume. Thus, the tissue Starlingforces and lymph flow can absorb a change incapillary pressure of 12 mm Hg in such a fashionthat very little fluid enters the interstitium.
When capillary pressure is elevated to higherlevels (37.9 mm Hg), visible tissue edema resultssince the tissue volume expands to approximatelytwice its control value and tissue fluid pressureincreases by an additional 10 mm Hg. Lymph flowdid not increase significantly above the previousstate of tissue hydration (lymphatic safety factorincreased by only: 7.5 — 5.6 = 1.9 mm Hg).
The data presented in Figure 9 from an intestinalpreparation can also be used to estimate the balancein Starling forces (Granger et al., 1980):
Force imbalance
= 0.5 mm Hg;
(Normal interstitial volume)
Force imbalance
JvKf.c
= (12 - (+4) - 7)
= 1 mm Hg.(Gross edema)
At normal hydration states within the small intes-tine, the Starling force imbalance is only 0.5 mmHg. This study is not complicated by assuming thatad = 1, since it was measured in each preparation.After glucagon infusions, the tissues became grosslyedematous, and yet the imbalance in forces wasonly 1 mm Hg.
There are both important differences and simi-larities between these two Starling force studies.The two important differences between these twofluid balance studies are. (1) Lymph flow provideda substantial safety factor in the hindpaw at mod-erately high capillary pressures because Kr,c wassmall. However, in the small intestine, glucagonincreased permeability and Kf,c increased, and thisresulted in almost no lymphatic safety factor, evenin the face of gross interstitial edema. (2) Tissuepressure provided a large portion of the edemasafety factor at moderate levels of capillary pressureand almost the entire compensating force at highcapillary pressures in the hindpaw. Yet in the smallintestine, tissue pressure increased to only 4 mmHg following the glucagon infusions, but could notincrease to higher values. This is to be expectedsince the compliance of the intestinal interstitiumincreases greatly at tissue pressures between 2 and2.5 mm Hg and the mucosal membrane is disruptedat tissue pressures exceeding approximately 3 mmHg (Mortillaro and Taylor, 1976; Yablonski andLifson, 1976). The two studies demonstrated clearly
the differences in the behavior of Starling forcesand flows in hydrostatic and permeability edemas.
The important similarities between the tissuesare: (1) Interstitial pressure is negative in bothintestinal and subcutaneous tissues at normal ve-nous pressures and hydration states. (2) The im-balance in Starling forces is very small a t normalcapillary pressures. (3) The normal effective colloi-dal osmotic pressure gradient acting across bothtypes of capillary walls is within 90-95% of thedifference in the colloid osmotic pressure of plasmaminus the colloid osmotic pressure of the tissuefluid. It appears that lymph represents tissue fluidsin both subcutaneous and intestinal tissues, al-though one organ contains a low protein concentra-tion in its interstitium, whereas the other organcontains a high protein fluid interstitium.
The Starling force analyses conducted in subcu-taneous tissue and intestinal tissues appear to beeasily interpreted relative to interstitial fluid bal-ance control and represent excellent experimentalapproaches with which to study functional andpathological fluid balance states in these organs.Complexities could exist within these tissues rela-tive to fluid balance analyses especially in the smallintestine, since it contains at least three differentvascular systems: smooth muscle, submucosal, andmucosal. But, this does not appear to cause anygreat difficulties in Starling force interpretationsince the behavior of the small intestine in primarilypredicated by events which occur in the mucosalregion.
It is of interest to note that the recent model ofcapillary fluid exchange presented by Wiederhielm(1979) predicts behavior of the Starling forces whichare similar to those obtained in the study of Chenet al. (1976). Wiederhielm developed a very complexmodel which incorporated the differences in pres-sures and volume conductances along the length ofthe capillary, as well as tissue mucopolysaccharideinteractions. However, the Wiederhielm modelwould not predict the subatmospheric pressuresobtained in the Chen study, but would predict thehigh tissue pressure obtained at the higher tissuevolumes. The discrepancies obtained betweenmodel predictions and experimental results couldbe caused by many factors but most probably em-phasize the problems associated with extrapolatingthe behavior of the forces in a particular tissue toanother capillary bed. Comparisons are furthercomplicated by the methods used to assess theforces in different experimental models; e.g., capil-lary pressure is assessed by using either zero flowor zero flow extrapolation procedures in differentlaboratories which may alter its experimental mag-nitude. Finally, as more data become available,more complete models can be constructed concern-ing whole organ predictions as compared to micro-measurements.
Future studies in these organs should certainly
by guest on June 5, 2018http://circres.ahajournals.org/
Dow
nloaded from

570 CIRCULATION RESEARCH VOL. 49, No. 3, SEPTEMBER 1981
concentrate their efforts toward microtechniques.Gore and his associates are presently measuring Pc,77P, and Kf.c in the smooth muscle layer of the smallintestine (Gore and McDonagh, 1980; Pappenfusset al., 1980). They have developed experimental andmathematical models which allow estimations ofKf,c and Starling forces to be made in differentsegments of the intestinal circulation. Perhaps inthe near future, investigations will be conducted onthe mucosal capillaries in the intestine which aresimilar to those reported by Nordin et al. (1978) forbronchial tissue. Microscopic fluid balance studieshave been reviewed critically in the past (Intagliettaand Zweifach, 1974; Gore and McDonagh, 1980) andare certainly the direction which should be taken infuture fluid balance studies. However, the micro-scopic studies should be focusing on mechanisms atthe microcirculatory level and at least three of thefour Starling forces, capillary filtration rate, inter-stitial volume, and capillary permeability, must bemeasured in each preparation at defined steadystates before any mechanisms can be ascertainedconcerning the regulation of fluid volume at themicrocirculatory level.
Finally, I will apply a Starling force analysis ondata collected in lung tissue since it will point outthe complexities associated with interpreting aver-age Starling force balance measurements (organvalues) when the tissue fluid is compartmentalized.The following Starling force balance was derivedusing the accepted values for the dog lung capillaryStarling forces:
Force imbalance
Kf,• - [ ( 7 - (-6)) - (20 -15) ]
= 8 mm Hg.(Normal)
From this calculation, it appears that the imbalancein Starling forces is quite large in lung tissue. Thislarge imbalance indicates that the lymphatic safetyfactor is quite large; i.e., either Kf>c is small or lymphflow is extremely high or both. In fact, the largeStarling force imbalance at normal pressures pre-dicts that the lung should be able to withstandcapillary pressure increases of 40-60 mm Hg beforeedema develops, since lymph flow can easily in-crease 5- to 7-fold before fluid enters the airways.How can the lymphatic force be this large? Thetheory predicts a large Starling force imbalance,but it is well known that pulmonary capillary pres-sure can only be increased to 25-30 mm Hg beforegross pulmonary edema ensues. Also, Kf,c's mea-sured in lung tissue using gravimetric techniquesare quite large, indicating only a small lymph flowsafety factor, unless lymph flow draining the lung isextremely large. The Starling forces simply do notagree with well established experimental findings,so perhaps the lung cannot be considered as asimple well mixed organ system.
The lung's fluid volume is certainly divided intoat least two different compartments: (1) the small,rather rigid septal regions surrounding the alveolarcapillaries, and (2) the larger and easily expandablepotential spaces which surround the vascular andbronchial systems.
Figure 10 represents a model which describes thelung interstitium as a two-compartment system(Guyton et al., 1976). The septal fluid volume isconsidered to be the smaller of the two compart-ments and is connected to the larger perivascularspaces by a high resistance pathway. It has beenwell documented that perivascular pressures arenegative (Lai-Fook, 1980), and because of the cur-vature of the alveoli and their surface tension, theseptal interstitial fluid pressure should also besubatmospheric in that region. The graph in Figure10 represents the model's prediction when capillarypressure is increased and assuming that: (1) theseptal capillaries have a high Kf,c; (2) the resistanceto fluid movement between septal and perivascularfluid compartments is high and decreases as thetissues expand; and (3) the lymphatics drain theperivascular region of the lung.
At normal capillary filtration rates, a pressuredifference of 6-7 mm Hg is required to overcomethe resistance between the septal and perivascularregions and provide the fluid which eventuallyforms lymph. As capillary pressure is increased to
4EPTALSPACE
|
FLOW
LUNG TISSUE
PATHWAY 1
PERIVASCULARSPACE
>— . LYMPH
FLOWr
n F
PULMONARY CAPILLARY PRESSURE(mmHg)
FIGURE 10 Plot of septal and penbronchial pressuresfrom a lung fluid exchange model developed by Guytonet al. (1976). In this model it was assumed that the fluidcompartments of the lung could be represented as septaland perivascular spaces. The spaces are connected by ahigh resistance pathway, and lymph is drained onlyfrom the perivascular spaces.
by guest on June 5, 2018http://circres.ahajournals.org/
Dow
nloaded from

STARLING FORCES/Taylor 571
higher values, the peribronchial pressure begins toincrease at a greater rate than septal pressuresbecause the flow resistance between the two com-partments is decreasing as the tissues expand. At20-30 mm Hg, the resistance between the compart-ments is reduced to essentially zero, and the twopressures become equal. Further capillary filtrationwill not increase either pressure since fluid nowfloods the alveoli.
This mathematical model suggasts several mech-anisms which can be tested experimentally andshould help to resolve the apparent discrepancybetween the various estimates of Starling forcesand physiological observations in the lung. (1) Themodel predicts that perivascular pressures rises rap-idly as compared to septal interstitial fluid pressure,especially at high capillary pressures. This modelprediction has been verified experimentally in therecent studies of Lai-Fook (1980) and Hida et al.(1980). These investigators demonstrated that morepressure is reflected from small pulmonary spaces(measured with 2-5 /zm pipettes) to the largerperivascular spaces at higher levels of edema. Theyalso have established experimentally that perivas-cular pressures of -1 to -2 mm Hg are associatedwith intra-alveolar edema. The model predicts bothexperimental findings. (2) The model also predictsthat the Kf,c estimated by using lymph flow dividedby the estimates of Starling forces (an apparentKf,c) will be much less than the septal capillaryfiltration coefficient. This results because fluid mustflow through a high resistance pathway to reachthe perivascular spaces. Recently, Oppenheimerand Goldberg (1980) have demonstrated experimen-tally that Kf.c's estimated by gravimetric proceduresmay seriously underestimate the "true septal Kr,c"because the resistance of fluid movement betweenthe lung fluid compartments is high. (3) Since fluidwill take a long time to flow from the small septalvolume to the larger perivascular region, there willalso be differences between perivascular and septalfluids with respect to plasma protein concentrationsin relative short term experiments (1—4 hours) (Par-ker et al., 1980; Gee and Spath, 1980).
Since the three major assumptions used to buildthe mathematical model have been experimentallyconfirmed, model predictions should allow us toexplain why a simple Starling force analysis usingorgan values fails to explain fluid balance in thelung. The model predicts the following Starlingforce balance, assuming an equivalence betweenperivascular osmotic pressure and lymph usingperivascular interstitial fluid pressures as intersti-tial pressure and assuming values of 28 mm Hg forplasma colloid osmotic pressure:
Force imbalance
= - ^ = [7 - (-10) - (28 - 20)]
= 9 mm Hg.(Normal volume)
However, if the Starling force balance is calculatedusing the assumed septal colloid osmotic pressureand septal fluid pressure, the following results:
Force imbalance
Kf.c= [7 - (-3.3) - (28 - 18)]
= 0.3 mm Hg.(Normal volume)
This indicates that the real imbalance in Starlingforces is only 0.3 mm Hg at the filtering capillaries,which is similar to that calculated in other capillarybeds. The implications of the model are that: (1)the capillary-lymphatic safety factor in lung tissueis not an important factor opposing fluid filtration,even for high lymph flow states; (2) the implantedcapsules (Guyton, 1963) must measure a pressureclose to that in perivascular regions and do notreflect the pressure responsible for events occurringat the filtering capillaries; (3) the protein content ofperivascular spaces is higher than that surroundingthe septa! capillaries. Gee and Spath (1980), Geeand Havill (1980), and Parker et al. (1980) havepresented very convincing data which indicate thatthe protein concentrations in the perivascular re-gions are not well mixed and that newly formedcapillary filtrate is quite different from fluid withinthe large perivascular spaces; and (4) a tissue re-sistance factor may provide a major portion of thetotal edema safety factor at low tissue hydrationstates.
Therefore, it appears that the discrepancy ob-served between measured and calculated values forStarling forces in lung tissue can be resolved par-tially by using a compartmentalized model ap-proach since the model's predictions have beenverified in several different animal experiments.However, the exact value of the septal pressure isnot known at the present time, but this valuechanges relative to the compliance characteristicsof the two compartments and the resistance con-necting the two fluid volumes.
For tissues such as hindpaw, hindlimb, and intes-tine, it appears that compartmentalization of fluidsdoes not constitute any appreciable problem whenassessing average Starling forces. However, for lungtissues, the compartmentalization of fluids betweenfiltering and nonfiltering regions (Goldberg et al.,1977) poses such a restraint on data interpretationthat a Starling force analysis using implanted cap-sules to estimate Pt and lymph protein concentra-tion for tissue fluids may yield results which do notexplain the basic mechanisms involved in intersti-tial fluid volume regulation.
In summary, this review has focused on how thetissue Starling forces and lymph flow oppose theformation of interstitial edema, i.e., edema safetyfactors. When capillary pressure is increased, tissuepressure increases in most tissues, the colloid os-motic pressure gradient acting across the capillary
by guest on June 5, 2018http://circres.ahajournals.org/
Dow
nloaded from

572 CIRCULATION RESEARCH VOL. 49, No. 3, SEPTEMBER 1981
wall increases in all tissues with the exception ofthe liver, and lymph flow is an important compo-nent of the edema safety factor in most capillarybeds. Some tissues, such as the liver, have overflowsystems other than the lymphatic system, whichcan become operative when filtration is increasedto prevent excessive tissue swelling. All capillaryand tissue Starling forces are near equilibrium inintestinal and subcutaneous tissues, but a Starlingforce analysis of lung indicates that the forces mea-sured in several experimental models are far fromequilibrium. To explain the differences between thedata obtained in different experimental models oflung, a mathematical approach was used in whichthe lung was represented as a two-compartmentsystem. When fluid accumulation is considered tooccur in a septal compartment which is connectedby a high resistance pathway to the perivascularspaces, the fluid balance characteristics can be eval-uated. Finally, the review indicates that Starlingforce analyses in whole organs are very useful ex-perimental models with which to study fluid bal-ance in a wide variety of tissues in both functionaland pathological states.
However, most published studies concerningfluid balance either measured too few Starlingforces or no steady state was defined during thecourse of the experimental procedures. To describefluid movement adequately all Starling forcesshould be measured at steady state conditions, i.e.,when lymph flow, lymphatic proteins, and tissuevolume are nonchanging with time. Indications arethat some tissues may require several hours toattain a true steady state with respect to tissuecolloids. Therefore, each experimental model mustattain steady state conditions which are clearlydefined before any inference can be made concern-ing the behavior of Starling forces as edema devel-ops.
Future research using microscopic techniquesshould allow more complete models to be developedconcerning the mechanisms responsible for fluidmovement at the microcirculatory level. Starlingforce analyses still provide the major means ofassessing an organ's ability to regulate its interstitialvolume, and several organ systems have not beenstudied. It is hoped that this review will stimulateworkers to investigate capillary and tissue Starlingforces in other capillary beds, e.g., heart, stomach,muscle, etc., and relate these important determi-nants of fluid balance not only to edema formation,but also to the functional state of the particularorgan. The extension of Starling force analyses tochronic edema states, e.g., myxedema, diabetes, left-sided heart failure, etc., promises to provide phys-iologists and clinicians with the basic informationnecessary to explain how interstitial fluid volume isregulated in both healthy and diseased states. Thisbasic approach certainly will provide new diagnosticprocedures and treatment regimens in the clinicalsetting.
At the present time, investigators can measuretissue pressure, lymph flow, KfiC, and tissue volumein human leg and forearm. Although a completeStarling force analysis has not been conducted inhuman tissues, the techniques are available to es-timate Pi, irt, lymph flow, mv, tissue volume, and Pc.Perhaps studies will soon be conducted in the hu-man model similar to those presented in this review,using simple maneuvers such as cuffs to elevatevenous pressure.
AcknowledgmentsI would like to thank Drs. P. Kvietys, M. Perry, and J. Parker
for their very thoughtful criticism of this review. In addition, Iwish to acknowledge Penelope Cook for her excellent art workand Leigh Cosper for preparing and editing this manuscript.
ReferencesAukland K, Fandes HO (1973) Protein concentration of intersti-
tial fluid collected from rat skin by a wick method. ActaPhysiol Scand 88: 350-358
Bennet HS, Luft JH, Hampton JC (1959) Morphological classification of vertebrate blood capillaries. Am J Physiol 196:381-390
Bland RD, Demling RH, Selinger SL, Staub NC (1977) Effectsof alveolar hypoxia on lung fluid and protein transport inunanesthetized sheep. Circ Res 40: 269-274
Brace RA, Guyton AC, Taylor AE (1975) Reevaluation of theneedle method for measuring interstitial fluid pressure. Am JPhysiol 229: 603-607
Brace RA, Granger DN, Taylor AE (1977a) Analysis of lym-phatic protein flux data. II. Effect of capillary heteroporosityon estimates of reflection coefficients and PS products. Micro-vase Res 14: 215-226
Brace RA, Guyton AC, Taylor AE (1977b) Determinants ofisogravimetric capillary pressure in the isolated dog hindlimb.Am J Physiol 233: H130-H135
Brace RA, Granger DN, Taylor AE (1978) Analysis of lymphaticprotein flux data. III. Use of the nonlinear flui equation toestimate o and PS. Microvas Res 16: 297-303
Bradhury M (1979) The Concept of a Blood-Brain Barrier. NewYork, John Wiley & Sons, pp 116-136
Brenner BM, Humes Hd (1977) Mechanics of glomerular ultrafiltration. N Engl J Med 297: 148-154
Brenner BM, Deen WM, Robertson CR (1976) Determinants ofglomerular filtration rate. Annu Rev Physiol 38: 11-19
Bngham K, Owen P (1975a) Increased sheep lung vascularpermeability caused by histamine. Circ Res 37: 647-657
Brigham KL, Owen PJ (1975b) Mechanism of the serotonineffect on lung transvascular fluid and protein movement inawake sheep. Circ Res 36: 761-770
Brigham K, Woolverton W, Blake L, Staub N (1974) Increasedsheep lung vascular permeability caused by Pseudomonasbacteremia. J Clin Invest 54: 792-304
Bngham KL, Owen PJ, Bowers RE (1976) Increased permeabil-ity of sheep lung vessels to proteins after Pseudomonas bac-taremia. Microvasc Res 11: 415—419
Bruce DA (1978) The pathophysiology of increased intracranialpressure. In Current Concepts, Upjohn Co, pp 20-47
Calnan JS, Ford PM, Holt PLJ, Pflug JJ (1972) Implanted tissuecages. Br J Plast Surg 25: 164-174
Casley-Smith JR (1977) The functioning of the lymphatic systemunder normal and pathological conditons: Its dependence onthe fine structures and permeabilities of the vessels. In Prog-ress in Lymphology, edited by A Ruttiman. Stuttgart, Thieme,pp 348-359
Chen HI, Granger HJ, Taylor AE (1976) Interactions of capillary,interstitial and lymphatic forces in the canine hindpaw. CircRes 38: 245-254
Chen HI, Granger HJ, Taylor AE (1977) Lymph flow transients
by guest on June 5, 2018http://circres.ahajournals.org/
Dow
nloaded from

STARLING FORCES/Taylor 573
following elevation of venous pressure in the dog's hind paw.In Progress in Lymphology, edited by RC Mayall and WWitte. London, Plenum Press, pp 19-26
Davson H (1960) Intracranial and intraocular fluids. In Hand-book of Physiology, section 1, vol 111, edited by HW Magonn.Baltimore, The Williams & Willons Co, pp 1761-1788
Demling W (1978) Effect of furosemide on the pulmonary trans-vascular fluid filtration rate. Crit Care Med 6: 317-319
Diana JN, Laughlin MH (1974) Effect of ischemia on capillarypressure and equivalent pore radius in capillaries of the iso-lated dog hind limb. Cire Res 35: 77-101
Drake RE (1975) Changes in Starling forces during the formationof pulmonary edema. PhD Dissertation, University of Mis-sissippi
Drake RE, Smith JH, Gabel JC (1980) Estimation of the filtra-tion coefficient in uilact dog lungs. Am J Physiol 238: H430-H438
Drake RE, Taylor AE (1977) Tissue and capillary force changesduring the formation of intra-alveolar edema. In Progress in
.lymphology, edited by RC Mayall, MH Witte. New York,Plenum Press, pp 13-18
Duffy PA, Granger DN, Taylor AE (1978) Intestinal secretioninduced by volume expansion in the dog. Gastroenterologv 75:413-418
Erdmann AJ III, Vaughn T, Brigham W, Staub NC (1975) Effectof increased vascular pressure on lung fluid balance in unan-esthetized sheep Circ Res 37: 271-284
Essig A, Caplan RS (1979) The use of nonequilibrium thermo-dynamics in the study of renal physiology. Am J Physiol 236:F211-F219
Gaar KA, Taylor AE, Owens LJ, Guyton AC (1967) Effect ofcapillary pressure and plasma protein on development ofpulmonary edema. Am J Physiol 213: 79-82
Gaar KA, Taylor AE, Owens LJ, Guyton AC (1968) Pulmonarycapillary pressure and filtration coefficient in the isolatedperfused lung. Am J Physiol 213: 910-914
Gabel JC, Drake RE, Arens JF, Taylor AE (1978) Unchangedpulmonary capillary filtration coefficients after E. coli endo-toxin infusions. J Surg Res 25: 97-104
Gabel J, Scott K, Adiar T, Drake D, Traber D (1980) Evaluationof equations used to calculate oncotic pressure (abatr). FedProc 39: 280
Garlick DG, Renkin EM (1970) Transport of large moleculesfrom plasma to interstitial fluid and lymph in dogs. Am JPhysiol 219: 1595-1605
Gee M, Havill AM (1980) The relationship between pulmonarypenvascular cuff fluid and lung lymph in dogs with edema.Microvasc Res 19: 209-216
Gee MH, Spath JA Jr (1980) The dynamics of the lung fluidfiltration systems in dogs with edema Circ Res 46: 796-801
Gibson WH (1974) Dynamics of lymph flow, tisssue pressure andprotein exchange in subcutaneous connective tissues. Ph D.Dissertation, University of Mississippi
Goldberg HS, Mitzner W, Batra G (1977) Effect of transpulmo-nary and vascular pressures on rate of pulmonary edemaformation. J Appl Physiol 43: 14-19
Gore RW, McDonagh PF (1980) Fluid exchange across singlecapillaries. Annu Rev Physiol 42: 337-57
Granger HJ (1979) Role of the interstitial matrix and lymphaticpump in regulation of transcapillary fluid balance. MicrovascRes 18: 209-216
Granger DN, Taylor AE (1978) Effects of solute-coupled trans-port on lymph flow and oncotic pressures in cat ileum. Am JPhysiol 23S: E429-E436
Granger DN, Taylor AE (1980) Permeability of intestinal capil-laries to endogenous molecules. Am J Physiol 238: H457-H464
Granger HJ, Goodman AH, Granger DN (1976) Role of resist-ance and exchange vessles in local microvascular control ofskeletal muscle oxygenation in the dog. Circ Res 38: 379-385
Granger DN, Mortillaro NA, Taylor AE (1977) Interaction ofintestinal lymph flow and secretion. Am J Physiol 232: E13-E18
Granger DN, Gabel JC, Drake RE, Taylor AE (1978) Physiolog-
ical basis for the clinical use of albumin solutions. Surg GynObstet 146: 97-104
Granger DN, Richardson PDI, Taylor AE (1979a) Volumetricassessment of the capillary' filtration coefficient in the catsmall intestine. Pfluegers Arch 381: 25-33
Granger DN, Miller T, Allen R, Parker RE, Parker JC, TaylorAE (1979b) Permselectivity of cat liver blood-lymph barrierto endogenous macromolecules. Gastroenterology 77: 103-109
Granger DN, Kvietys PR, Wilborn WH, Mortillaro NA, TaylorAE (1980). Mechanism of glucagon-induced intestinal secre-tion. Am J Physiol 239: G30-G38
Grega GJ, Dobbins DE, Scott JB, Haddy FJ (1979) Effects ofhistamine and increased venous pressure on transmicrovas-cular protein transport. Microvasc Res 8: 95-104
Guyton AC (1963) A concept of negative interstitial pressurebaaed on pressures in implanted capsules. Circ Res 12: 399-414
Guyton AC (1965) Interstitial fluid pressure. II Pressure-volumecurves of interstitial space. Circ Kes 16: 452-460
Guyton AC, Coleman TG (1968) Regulation of interstitial fluidvolume and pressure Ann NY Acad Sci 150: 537-547
Guyton AC, Lindsey AW (1959) Effect of elevated left atrialpressure and decreased plasma protein concentration on thedevelopment of pulmonary edema Circ Res 7: 649-657
Guyton AC, Scheel K, Murphree U (1966) Interstitial fluidpressure. III. Its effect on resistance to tissue fluid mobility.Circ Res 19: 412-419
Guyton AC, Granger HJ, Taylor AE (1971) Interstitial fluidpressure Physiol Rev 51: 527-563
Guyton AC, Taylor AE, Granger HJ (1975) Circulatory Physi-ology, vol II Philadelphia, WB Saunders Co, pp 18-52
Guyton AC, Taylor AE, Draie RE, Parker JC (1976) Dynamicsof subatmospheric pressure in the pulmonary interstitial fluid.
Haglund U, Lundgren O (1972) Reactions witlim consecutivevascular sections of the small intestine of the cat duringprolonged hypotension. Acta Physiol Scand 84: 151-163
Hargens AE, Scholander PF, Orns WL (1978) Positive tissuefluid pressure in the feet of antarctic birds Microvasc Res 15:239-244
Hida W, Inoue W, Inoue C, Hildebrandt J (1980) Peribronchialinterstitial fluid pressure. (Px(f)) during weight gain in doglobes (abstr.). Fed Proc 39: 486
Intaglietta M, Zweifach BW (1974) Microcirculatory basis offluid exchange. Adv Biol Med Phys 15: 111-159
Iverson P, Johansen EH (1929) Pathogenese und Resorptionvon Trans- und Exudation in der Pleura. Klin Wochenschr 8:1311-1319
Johnson PC, Hanson KM (1966) Capillary filtration in the smallintestine of the dog. Circ Res 19: 766-773
Johnson PC, Richardson DR (1974) The influence of venouspressure on filtration forces in the intestine. Microvasc Res 7:296-306
Kedem 0, Katchalsky A (1958) Thermodynamic analysis of thepermeability of biological membranes and electrolytes.Biochim Biophys Acta 27: 229-246
Krogh A, Landis EM, Turner AH (1932) The movement of fluidthrough the human capillary wall in relation to venous pres-sure and to the colloid osmotic pressure of the blood. J ChnInvest 11: 63-95
Lai-Fook S (1980) Penvascular interstitial fluid pressure mea-sured by 2-5/i pipettes: The effect of water accumulation(abstr) Fed Proc 39: 486
Laine GA, Hall JT, Laine SH, Granger HJ (1979) Transsinu-soidal fluid dynamics in canine liver during venous hyperten-sion. Circ Res 45: 317-323
Landis EM (1927) The relationship between capillary pressureand the rate at which fluid passes through the walls of singlecapillaries. Am J Physiol 82: 217-238
Landis EM (1928) Micro-injection studies of capillary permea-bdity. III. The effect of lack of oxygen on the permeability ofthe capillary wall to fluid and the plasma proteins. Am JPhysiol 83: 523-542
Landis EM (1934) Capillary pressure and capillary permeability.Physiol Rev 14: 404-481
by guest on June 5, 2018http://circres.ahajournals.org/
Dow
nloaded from

574 CIRCULATION RESEARCH VOL. 49, No. 3, SEPTEMBER 1981
Landis EM, Pappenheimer JR (1963) Eichange of substancesthrough the capillary walk. In Handbook of Physiology, sec-tion 2, vol II, edited by WF Hamilton, P Dow. Baltimore, TheWilliams & Wilkina Co, pp 961-1034
Levine OK, Mellins RB, Senior RM, Fishman AP (1967) Theapplication of Starling's law of capillary exchange to the lungs.J Clin Invest 46: 934-944
McMaster PD (1946) The pressure and interstitial resistanceprevailing in the normal and edematous skin of animals andman. J Eip Med 84: 473--194
Malik AB (1977) Pulmonary vascular response to increase inintracramnl pressure- Role of sympathetic mechanisms. J ApplPhysiol42: 335-343
Marmarou A, Shulman K (1976) Pressure-volume relation-ships—basic aspects. In Head Injuries, edited by RC Mc-Laurin. New York, Grune & Stratton, pp 233-236
Marmarou A, Shulman K, La Morgese J (1975) Compartmentalanalysis of compliance and outflow resistance of the cerebro-spinal fluid system. J Neurosurg 43: 523-534
Marmarou A, Shulman K, Rosende R (1978) A non-linear anal-ysis of the cerebrospinal fluid system and intracranial pressuredynamics J Neurosurg 48: 332-334
Mellander SB, Oberg B, Odelram O (1964) Vascular adjustmentsto increased transmural pressure in cat and man with specialreference to shifts in capillary fluid trajisfer. Acta PhysiolScand 61: 31-46
Mellins RB, Levine OR, Skalak R, Fishman AP (1969) Intersti-tial pressure of the lung. Circ Res 24: 197-212
Mortillaro NA, Taylor AE (1976) Interaction of capillary andtissue forces in the cat small intestine. Circ Res 39: 348-358
Mortillaro NA, Granger DN, Taylor AE (1979) Effects of hista-mine on lymph flow and capdlary permeability in the catileum (abstr). Microvasc Res 17: 513
Navar PD, Navar LG (1977) Relationship between colloid os-motic pressure and plasma proteins concentration in the dog.Am J Physiol 233: H295-H298
Nicolaysen G, Nicolaysen A, Staub NC (1975) A quantativeradiographic comparison of albumin concentration in differentsized lymph vessels in normal mouse lungs. Microvas Res 10:138-152
Nicoll PA, Hogan RD (1978) Pressures associated with lym-phatic capillary contraction. Microvasc Res 15: 257-259
Nicoll PA, Taylor AE (1977) Lymph formation and flow. AnnuRev Physiol 39: 73-95
Nordin U, Kallakog O, Lindholm C-E, Wolgast M (1978) Trans-vascular fluid exchange in the trachea! mucosa. Microvasc Res15: 299-308
Oppenheimer L, Goldberg HS (1980) Transudation versus slowvascular recruitment in the isolated lobe (abstr). Fed Proc 39:280
Papenfuss HD, Gore RW. Gross JF (1980) Effect of variablehydraulic conductivity on transcapillary fluid exchange: Ap-plication to the microcirculation of rat intestinal muscle. Mi-crovasc Res 19: 263-276
Pappenheimer JR, Soto-Rivera A (1948) Effective osmotic pres-sure of the plasma proteins and other quantities associatedwith the capillary circulation in the hindlimb of cats and dogs.Am J Physiol 152: 471^»91
Parker JC, Cuyton AC, Taylor AE (1978) Pulmonary interstitialand capillary pressures estimated from intra-alveolar fluidpressures. J Appl Physiol 44: 267-276
Parker JC, Falgout HJ, Parker RE, Granger DN, Taylor AE(1979) The effect of fluid volume loading on exclusion oninterstitial albumin and lymph flow in the dog lung. Circ Res45: 440-450
Parker JC, Ro3elli RJ, Brigham KL (1980) Effects of prolongedleft atrial pressure elevation on lung microvascular proteinsieving in unanesthetized sheep (abstr). Fed Proc 39: 279
Parker JC, Parker RE, Granger DN, Taylor AE (1981) Vascularpermeability and transvascular fluid and protein transport inthe dog lung. Circ Res 48: 549-561
Patlak CS, Goldstein DA, Hoffman JF (1963) The flow of soluteand solvent across a two membrane system. J Theor Biol 6:426-442
Prather JW, Gaar KA, Guyton AC (1968) Direct continuousrecording of plasma colloid osmotic pressure of whole blood.,1 Appl Physiol 24: 602-605
Prather JW, Bowes BN, Warrell DA, Zweifach BW (1971) Com-parison of capsule and wick techniques for measurement ofinterstitial fluid pressure. J Appl Physiol 31: 942-945
Rapoport SI (1976) Blood Brain Barrier in Physiology andMedicine. New York, Raven Press, pp 87-127
Rapoport SI (1978) A mathematical model for vasogenic brainedema. J Theor Biol 74: 439-467
Rapoport SI (1979) Roles of cerebrovascular permeability braincompliance and brain hydraulic conductivity in vasogenicbrain edema. In Neural Trauma, edited by AJ Popp. NewYork, Raven Press, pp 51-62
Reed RK, Aukland IC (1977) Transcapillary fluid balance inimmature rats. Interstitial fluid pressure, serum and interstitialprotein concentration, and colloid osmotic pressure. MicrovasRes 14: 37-43
Renkin EM (1979) Lymph as a measure of the composition ofinterstitial fluid. In Pulmonary Edema, edited by A FishmanEM Renkin, Baltimore, The Williams & Wilkins Co, pp 145-159
Richardson PDI, Granger DN, Taylor AE (1979) Capillary fil-tration coefficient: The technique and its application to thesmall intestine. Cardiovasc Res 13: 547-561
Richardson PDI, Granger DN, Kvietys PR, Mailman D (1980).Permeability characteristics of colonic capillaries. Am J Phys-iol 239: G300-G3O5
Robertson CR (1980) A review of transcapillary fluid and soluteexchange in the renal glomerulus. Microvasc Res 19: 131-141
Rutili G, Arfors K-E (1977) Protein concentration in interstitialand lymphatic fluids from the subcutaneous tissues. ActaPhysiol Scand 99: 1-8
Rutili G, Granger DN, Mortillaro NA, Parker JC, Taylor AE(1979) Analysis of blood-lymph transport in resting ajid pas-sively flexed hind-leg (abstr). Physiologist 22: 110
Scholander PF, Hargens AR, Miller SL (1968) Negative pressurein the interstitial fluid of animals. Science 161: 321-328
Snashall PD, Lucas J, Guz A, Floyer MA (1971) Measurementsof interstitial fluid pressure by means of a cotton wick in manand animals: An analysis of the origin of the pressure. Clin Sci41: 35-53
Starling EH (1894) The influence of mechanical factors on lymphproduction. J Physiol (Lond) 10: 14-155
Starling EH (1896) On the absorption of fluid from the connec-tive tissue spaces. J Physiol (Lond) 19: 312-326
Staub NC (1971) Steady-state pulmonary transvascular waterfiltration in unanesthetized sheep. Circ Re* 28/29 (suppl I):135-139
Staub NC (1974) Pulmonary edema. Physiol Rev 54: 679-811Staub NC (1978) Lung fluid and solute eichange. In Lung
Biology in Health and Disease, vol 9., edited by NC Staub,New York, Marcel DekJter, pp 3-16
Taylor AE, Drake RE (1977) Fluid and protein movement acrossthe pulmonary microcirculation. In Lung Biology in Healthand Disease, vol 9, edited by NC Staub, New York, MarcelDekker, pp 129-182
Taylor AE, Gibson H (1975) Concentrating ability of lymphaticvessels. Lymphology 8: 43-49
Taylor AE, Granger HJ (1976) Interstitial fluid pressure—Basicconcepts. In Head Injuries, edited by RL McLaurin, NewYork, Grune & Stratton, pp 266-271
Taylor AE, Gibson WH, Granger HJ, Guyton AC (1973) Theinteraction between intracapillary and tissue forces in theoverall regulation of interstitial fluid volume. Lymphology 6:192-208
Taylor AE, Granger DN, Brace RA (1977) Analysis of lymphaticprotein flux data. I. Estimation of the reflection coefficientand surface area product for total protein. Microvasc Res 13:297-313
Wallentm I (1966) Importance of tissue pressure for the fluidequilibrium between the vascular and interstitial compart-ments in the small intestine. Acta Physiol Scand 68: 304-315
Wiederhielm CA (1967) Analysis of small vessel function. In
by guest on June 5, 2018http://circres.ahajournals.org/
Dow
nloaded from

STARLING FORCES/ Taylor 575
Physical Bases of Circulatory Transport. Regulation and Ex-change, edited by EB Reeve, AC Guyton. Philadelphia, WBSaunders Co, pp 313-326
Wiederhielm CA (1972) The interstitial space. In Biomechanicg'Its Foundations and Objectives, edited by YC Fung, N Per-rone, M Anliker. Englewood Cliffs, N.J., Prentice-Hall, pp273-286
Wiederhielm CA (1979) Dynamics of capillary fluid exchange: Anon-linear computer stimulation. Microvasc Res 18: 49-82
Yablonski ME, Lifeon N (1976) Mechanism of production ofintestinal secretion by elevated venous pressure. J Clin Invest57: 904-915
Zweifach BW, Intaglietta M (1968) Mechanics of fluid movementacross single capillaries in the rabbit. Microvasc Res 1: 83-101
by guest on June 5, 2018http://circres.ahajournals.org/
Dow
nloaded from

A E TaylorCapillary fluid filtration. Starling forces and lymph flow.
Print ISSN: 0009-7330. Online ISSN: 1524-4571 Copyright © 1981 American Heart Association, Inc. All rights reserved.is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation Research
doi: 10.1161/01.RES.49.3.5571981;49:557-575Circ Res.
http://circres.ahajournals.org/content/49/3/557.citationWorld Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circres.ahajournals.org//subscriptions/
is online at: Circulation Research Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer about this process is available in the
located, click Request Permissions in the middle column of the Web page under Services. Further informationEditorial Office. Once the online version of the published article for which permission is being requested is
can be obtained via RightsLink, a service of the Copyright Clearance Center, not theCirculation Research Requests for permissions to reproduce figures, tables, or portions of articles originally published inPermissions:
by guest on June 5, 2018http://circres.ahajournals.org/
Dow
nloaded from