chesapeake physician january/february 2015 issue
DESCRIPTION
Using Lifestyle Practices to Treat Cardiovascular Disease, Caring for Advanced Complex Illnesses, Treating Cardiovascular Disease, Physician Assistants, The Impact of Insurance Changes, Michael Busch, Chesapeake CultureTRANSCRIPT

Maryland/DC/Virginia PhysicianYOUR PRACTICE. YOUR LIFE.
C H E S A P E A K E
VOLUME 5: ISSUE 1 JAN/FEB 2015
USING LIFESTYLE CHANGES TO TREAT CARDIOVASCULAR DISEASE
CARING FOR ADVANCED COMPLEX ILLNESSES
THE IMPACT OF INSURANCE CHANGES ON PATIENTS AND PHYSICIANS
chesphysician.com

10 Using Lifestyle Practices to Treat Cardiovascular Disease16 Caring for Advanced Complex Illnesses
F E A T U R E S
D E P A R T M E N T S
ContentsVOLUME 5: ISSUE 1 JAN/FEB 2015
2820 10
Cases | 7 | 30 Years of Progress in Treating Cardiovascular Disease
Solutions | 8 | PAs Expand Their Reach and Their Roles
HIT | 20 | The Impact of Insurance Changes on Patients and Physicians
Policy | 24 | Michael Busch: 11 Years as Maryland’s House Speaker
Compliance | 27 | False Claims Investigations: Ten Best Practices for Complying with DOJ Subpoenas
Living | 28 | Chesapeake Culture, Chesapeake Life
On the Cover: Vinay Satwah, DO, medical director, Center for Vascular Medicine

One year ago, I wrote a publisher’sletter stating that the year ahead in healthcarewould be rich with challenges and innovation,requiring physicians and healthcare leaders to be especially adaptable to change. Little did I know my words were foreshadowingwhat lay ahead for my own business. Withthis issue, I’m pleased to unveil ChesapeakePhysician – Your practice. Your life. This new
name represents the expansion and re-branding of Maryland Physician Magazine –Your practice. Your life. as we welcome new physicians in Northern Virginia andWashington, D.C. to our readership.
With the advent of the Patient Protection and Affordable Care Act (ACA) in2010, I recognized that there was a void in the Maryland healthcare marketplace for a print and online connection among Maryland-based physicians and healthcarestakeholders. I launched Maryland Physician’s inaugural issue in May/June 2011 tocreate a multi-media platform that spotlighted leading-edge healthcare diagnostic and treatment protocols as well as all aspects of practicing medicine. Our foundingmission was to grow a physician and healthcare stakeholder network with acommitment to achieving the highest standards of quality and efficient patient care.Thanks to the development and support of a dedicated team of writers, artists,advisors, contributors and advertisers over three-plus short, very busy and veryexciting years, I've grown Maryland Physician to fill that void, becoming a renownedand well-regarded resource for Maryland-focused healthcare industry news.
Over the last part of 2014, I launched an online reader poll, met with myAdvisory Board and asked healthcare policy influencers and makers if it made sensefor us to expand our network to encompass the broader Chesapeake region. Theanswer was a clear and resounding ‘yes!’ My mission remains constant, but with anexpanded scope that includes the healthcare industry in the District of Columbia andNorthern Virginia (NOVA). With the name Chesapeake, there is the opportunity forfuture growth from Cooperstown, New York, through Hampton Roads, Virginia(see Living, page 28). For now, though, we focus on Maryland, D.C., and NOVA.
As I wrote back in May 2011, every medical practice today, no matter the size or specialty, is challenged by ever-increasing complexities that impact the art andscience of practicing medicine. It’s my passion and my goal to keep you informed,intrigued and inspired with content and events focused on leading-edge treatmentsand practical advice for managing a clinical practice. Now, it’s my distinct honor toextend our reach beyond Maryland’s borders and into other areas of the ChesapeakeBay, inclusive of providers, healthcare stakeholders, patients and their families.
To life!
Jacquie Cohen RothFounder/Publisher/Executive [email protected]
@chesphysician
4 | CHESPHYSICIAN.COM
JACQUIE COHEN ROTHFOUNDER/PUBLISHER/EXECUTIVE EDITOR
LINDA HARDER, MANAGING [email protected]
JACKIE KINSELLA, MANAGEROPERATIONS,
SOCIAL & DIGITAL [email protected]
CONTRIBUTING WRITERAnne K. Sessions
COPY EDITOREllen Kinsella
LISA WOLFINGTON, BUSINESS [email protected]
PHOTOGRAPHYTracey Brown, Papercamera Photography
Chesapeake Physician – Your Practice. Your Life.™ is published bimonthly by Mojo Media, LLC, a certified MinorityBusiness Enterprise (MBE).
Mojo Media, LLCPO Box 949Annapolis, MD 21404443.837.6948mojomedia.biz
Subscription information: Chesapeake Physician is mailedfree to Maryland licensed and practicing physicians and a selectaudience of Maryland healthcare executives and stakeholders.Subscriptions are available for the annual cost of $52. To beadded to the circulation list, call 443.837.6948.
Reprints: Reproduction of any content is strictly prohibited and protected by copyright laws. To order reprints of articles or back issues, please call 443.837.6948 or email [email protected].
Chesapeake Physician Magazine Advisory Board: An advisory board comprised of medical practitioners and business leaders in diverse practice, business and geographicscopes provides editorial counsel to Chesapeake Physician. Advisory Board members include:
PATRICIA CZAPP, MDAnne Arundel Medical Center
HOLLY DAHLMAN, MDGreenspring Valley Internal Medicine, LLC
PAUL W. DAVIES, MD, FACSKURE Pain Management
MICHAEL EPSTEIN, MDDigestive Disorders Associates
STACY D. FISHER, MDUniversity of Maryland Medical Center
DANILO ESPINOLA, MDAdvanced Radiology
GENE RANSOM, JD, CEOMaryland Medical Society (MedChi)
CHRISTOPHER L. RUNZ, DOShore Health Comprehensive Urology
VINAY SATWAH, DO, FACOICenter for Vascular Medicine
THU TRAN, MD, FACOG Capital Women’s Care
Although every precaution is taken to ensure accuracy of published materials, Chesapeake Physician and Mojo Media,LLC cannot be held responsible for opinions expressed or facts supplied by authors and resources.
Printed on FSC certified, 100%PCW, chlorine-free paper
PhysicianYOUR PRACTICE. YOUR LIFE.
C H E S A P E A K E
Maryland/DC/Virginia www.chesphysician.com

6 | CHESPHYSICIAN.COM

JANUARY/FEBRUARY 2015 | 7
FIRST MET ‘FRED’ WHEN HE WAS32 years old, with his first inferiormyocardial infarct (MI). We treated him with streptokinase within two hoursof chest pain onset. His ejection fraction(EF) remained intact.
However, this tale really started manyyears before that MI. Fred remembersgoing to the National Institutes ofHealth (NIH) when he was 10 years oldand being told that he, his mother and other siblings had a unusual familialhyperlipidemia that would promotepremature cardiovascular disease. Hevividly remembers coming home fromschool to find the paramedics doing CPRon his 37-year-old mother on the frontporch. She died of a massive heartattack. Science had little to treat lipidproblems in the 1960s. While Fred neversmoked and was not diabetic, his otherrisk factors indicated that it was only amatter of time before he also developedheart disease. When he had his first heartattack, he had a one-year-old son and abrilliant career in sales.
Over the next 12 years, we valiantlyworked to control his high lipids withdiet, exercise and every novel therapythat existed, including first-generationstatins, but only achieved modestsuccess. During that time Fred continuedto work in sales and enjoyed hiswonderful family. Then disease andtragedy struck.
They say bad things come in threes.When Fred was barely 42, his only sondied of a brain tumor, his marriage failed, and he had another massiveanterior heart attack. He was rushed tothe catheterization lab within 30 minutesof the onset of chest pain, and theproximal LAD was found to be completelyoccluded. It was successfully opened
using RheoPro® and two TRISTARoverlapping stents, which were state-of-the-art therapy at the time. The heartmuscle damage was mitigated, but sadly,not aborted. His EF was now 20%.
Fred returned to work, but his heartfunction remained low. At the age of 44,he developed short, three-to-five beats,of non-sustained ventricular tachycardia(VT) presenting as dizzy spells. As luckwould have it, the MADIT 2 study hadjust demonstrated that patients such asFred lived longer with an automaticimplantable cardioverter defibrillator(AICD). We implanted an AICD that just a few days later shocked him in themiddle of the night, terminating VT.Without the device, he would have likely died.
It was evident that Fred was not out ofthe woods. His ischemic cardiomyopathyproduced short bursts of VT that theAICD treated with overdrive pacing.However, these frequent episodes wereworsening his condition.
Guided by his team of doctors, Fredfaced the difficult decision of going onamiodarone, an effective yet problematicmedicine with many side effects – for therest of his life – or receiving ventriculartachycardia ablation, a high-riskprocedure that might prove highlysuccessful. Fred chose the ablation, andthankfully his arrhythmia improved.
However, the arrhythmia had worsenedhis EF. Despite maximal medications,Fred struggled to work or perform manyof his typical daily activities. At age 53,
he was suffering from severe Class 3congestive heart failure.
Cardiac resynchronization therapy(CRT) had emerged as a proven, effective strategy of care for patientswith severe heart failure and QRSprolongation. Such patients often hadcardiac dyssyncrony; e.g., the right and the left ventricle did not contractsimultaneously. CRT requires theplacement of an additional coronarysinus lead in the heart and can be life-changing in select patients. We placed a CRT device in Fred’s heart, and hisimprovement was nearly miraculous. He began exercising again, and today he runs a yearly charity golf tournamentthat raises money for children with braincancer. His lipids are as good as they
have ever been on triple therapy thatincludes rusuvastatin.
Fred is now 24 years out from his first heart attack. He can walk for anhour at four miles/hour on a steepincline. Indeed, bad things happened inthrees to Fred many years ago. He couldhave died. However, medical sciencecame to his rescue. He received aprimary stent, an implantablecardiovertor-defibrillator, an ablationand a CRT device. He is now more than “OK.” Good things and sciencealso happen in threes… or more.Dr. Strobos is chief of Cardiology, Johns Hopkins Bayview Medical Center, and
professor of Medicine, Johns Hopkins
University School of Medicine. She can
be reached at [email protected].
I30 Years of Progress in TreatingCardiovascular Disease
By Nisha Chandra Strobos MD, FAHA
While Fred never smoked and was not diabetic, hisother risk factors indicated that it was only a matterof time before he also developed heart disease.
CASES

8 | CHESPHYSICIAN.COM
SOLUTIONS
PAs Expand Their Reach and Their Roles
HYSICIAN ASSISTANTS (PAs)have long been on the frontlines ofhealthcare, serving as trusted medicalprofessionals to patients in areas wherehealthcare providers are in short supply.Legislation that took effect this past fall will further increase access to thesepractitioners in rural areas of Maryland.
House Bill (HB) 459 recently extended the Maryland Loan AssistanceRepayment Program for Physicians(MLARP) to include PAs. Approved bythe Maryland General Assembly in its2014 session, it took effect October2014. As is true for similar legislationpassed by states throughout the nation,the law is expected to increase thenumber of PAs practicing in underservedareas by offering them an education loan repayment program.
With the passage of this legislation,Maryland joined Washington, D.C.,Virginia and 45 other states that havemade legislative or regulatoryimprovements for PAs. These loanrepayment programs, which award up to $25,000 per year for a two-yearobligation, usually require a few years of service in exchange for reimbursingloans that PAs have accrued throughouttheir education.
In Virginia, 2014 legislation allowedqualified PAs to testify as expertwitnesses on matters within their scopeof practice, administer topical fluoride to children’s teeth and be consideredhealthcare providers for the purpose of medical malpractice.
PA Training and Scope of PracticePAs receive graduate-level training in an intense medical program that teachesthem to diagnose, treat and prescribemedication. In addition to many medicalprocedures, PAs perform physicalexaminations, order and interpret labtests, assist at surgery, provide patienteducation and counseling, and make
P rounds in hospitals and nursing homes.PAs must graduate from a nationallyaccredited ARC-PA program and passthe national certification exam.
The PA profession has never beenstronger and is projected to grow 38%from 2012 to 2022. Over the years,many of the original barriers to theirscope of practice have been eliminated –including legal, regulatory andemployer-based restrictions. That hasallowed them to practice at the top oftheir education. The incentive programallows a wider range of students toconsider becoming PAs, furtherestablishing them as a viable and trusted option for medical care.
By design, PAs and physicians practice as a team and have practiceagreements and scopes that embrace thestrengths of each provider. Studies haveshown that teams of PAs and physicianscan allow a practice to see morepatients, improve patient outcomes,decrease wait times and improve patient satisfaction.
Survey Data A recent Harris Poll commissioned bythe American Academy of PhysicianAssistants (AAPA) found that 93% of patients who have interacted with a PA in the last year agree that they willbe part of the solution to address theshortage of healthcare providers.Additionally, 91% agree that PAsimprove health outcomes for patients.
Given the high patient satisfactionrates documented for PAs in every aspect of medicine, and the value of thephysician-PA relationship in numerous
practices, PAs have become an integralpart of healthcare, both in primary carepractices and in specialty practices.
More than 6,000 new PAs enter theworkforce each year. Data from theNational Commission on Certificationof Physician Assistants (NCCPA) showsunprecedented levels of demand for PAsupon graduation. Some 78% of recentgraduates receive multiple job offers,and 52% entertain three or more.
As the number of patients increases,due to an aging population and thenewly insured, there will be an increaseddemand for providers of high-quality,patient-centered care. PAs have themedical training and background that
enables them to care for these patients.According to the poll, only 24% of U.S. adults say they have found aprimary healthcare provider whom theylike and trust. These findings suggestthat PAs are needed to help fill the gaps.
The generalist medical knowledge that PAs possess lends itself well to rural environments, where healthcareproviders who have knowledge ofprimary care, as well as surgery andother specialties, are crucial forpopulations that continue to havelimited access to care. PAs are anestablished and highly trusted part of a collaborative healthcare team that depends on collaboration andcommunication among all partiesinvolved, with an emphasis on what’sbest for the patient.Theresa Neumann, PA-C, is the legislativechair and director-at-large of the Maryland
Academy of Physician Assistants. Learn more
about Maryland PAs at mdapa.org.
93% of patients who have interacted with a PA in the last year agree that they will be part of the solution to address the shortage ofhealthcare providers.
By Theresa Neumann, PA-C

10 | CHESPHYSICIAN.COM
BY LINDA HARDER • PHOTOGRAPHS BY TRACEY BROWN
REVERSING WESTERN ‘MALNUTRITION’Most doctors in practice today have received little or no nutrition training,and many have limited knowledge ofhow to use diet to prevent or treat thedisease. Monica Aggarwal, MD, a cardiologist and director of echocardiog-raphy at Mercy Medical Center, was one such physician until she got sick following the birth of her third child.
She recalls, “I met a nutritionist whofelt that dietary changes could help me. I dismissed her comments at first, butshe persisted. She taught me that I knewvery little about nutrition and howimportant it is. Today, I use my ownexperience to help my patients throughbetter nutrition, and I’ve seen it produceamazing results”
Inflammation“Certain factors trigger plaqueformation, such as high cholesterol,diabetes, high blood pressure andsmoking,” says Dr. Aggarwal. “Thoseplaques grow and build over time.
We don’t know, though, which of thoseplaques will rupture and create heartattacks. We do know that if patients’inflammatory markers are high, they are at higher risks for events. So I focus on decreasing inflammation bymodifying risk factors and aggressivelymodifying diet. The transition to awhole-grain, plant-based diet that is lowin processed foods is key to decreasingthat inflammation.”
The American Heart Associationrecommends that CRP tests be limited to those with a 10-20% (moderate) riskof a myocardial infarct in the next 10years. Of course, clinicians mustconsider that inflammation elsewhere in the body can cause an elevated CRP.
Marsha Seidelman, MD, an internistwith a practice based in Silver Spring,Maryland, is another physician whotakes nutrition seriously. While she alsobelieves that some foods can increaseinflammation, she does not monitor CRPlevels. “One of the reasons I don't checkthem,” she says, “is that we have nospecific treatment for inflammation.
TO TREATCARDIOVASCULAR
DISEASE
Using Lifestyle Factors
Western medicine hastended to emphasizemedication andprocedure-basedapproaches to treatcardiovascular disease. A growing number ofphysicians, however, are successfully usinglifestyle changes thatinclude nutrition and TranscendentalMeditation (TM) toprevent disease or serveas a treatment adjunct.

If someone has cardiovascular riskfactors, I will use the usual preventivemeasures such as aspirin and statins.”
“Nutrition has not been extensivelystudied because there’s no money in it, as there is in pharmaceuticals,” explainsDr. Aggarwal. “I am doing smallretrospective studies on how plant-baseddiet affects inflammation in chronicillness.”
Dr. Seidelman agrees that nutritionresearch is limited. “There are so manyconfounding issues and variables – howmuch exercise the person got, how thefood was prepared, etc. – that I takeeverything I read with a grain of salt,”she says. “That said, a Mediterranean-style diet emphasizing whole grains,fruits and vegetables is really important.I encourage physicians not to getoverwhelmed by all the conflicting datain the journals. Just have a generalroadmap – such as increasing vegetables,healthy oils and unprocessed foods –since these recommendations haven’tchanged much for years, and there ismore data to support them.”
JANUARY/FEBRUARY 2015 | 11
Guide Nutrition ChoicesDr. Seidelman continues, “Patients don’t understand that what they eataffects their long-term health. Butphysicians can’t just say ‘lose weight.’That’s not very helpful. For example,many people don’t realize that a whitehamburger bun is a processed food. You have to explain what it is.
“I review nutrition in every yearlyphysical, trying to shift people awayfrom red meat,” she adds. “If they’retrying to lose weight, I focus on portioncontrol, eating slowly and drinkingwater before the meal. Overly restrictivediets can backfire, especially over thelong run. I encourage people to do whatworks for them. If patients can make noother changes, however, I encouragethem to add more vegetables to theirdiet. Even losing five to 10 pounds canstart to make a difference in risk factorsand outlook.”
The Evidence for Eating Your VegetablesWhile research remains limited, often
with conflicting results, it’s hard to denythe evidence for eating more vegetables.An April 2013 study published in theNew England Journal of Medicine foundthat those consuming Mediterraneandiets supplemented with nuts or extra-virgin olive oil had a 3% lower deathrate after 4.8 years than those on a low-fat diet.
Like Dr. McDougall, CaldwellEsselstyn, Jr., MD, a former surgeon at the Cleveland Clinic, believes thatconventional cardiology has failedpatients by developing treatments thatfocus on the symptoms of heart disease,not the cause. He advocates for a plant-oriented diet without added oils toprevent and even reverse heart disease. A study he published in the July 2014issue of The Journal of Family Practicefound that nearly 200 people withestablished heart disease who adhered to a vegan diet for three years had a lowrecurrence of cardiovascular events(0.6%). Dr. Esselstyn hypothesizes that aplant-based diet prevents the creation oftrimethylamine oxide (TMAO), an
Monica Aggarwal, MD, cardiologist and director of Echocardiography at Mercy Medical Center

atherogenic compound produced only by omnivores who eat animal products.
“Red meat contains carnitine which,when digested, is turned into TMAO by our gut bacteria,” Dr. Aggarwalnotes. “And TMAO has been found to increase atherosclerosis. Eating fishincreases urinary TMAO, which meansyou’re excreting more of it. Gut bacteriais an exciting field of study and it mayturn out to be more important thansaturated fats.”
She adds, “A meat diet is catching up to us. I recommend completelyeliminating red meat and strongly adviseeliminating dairy and processed foods.Because we pasteurize milk, we destroyall of the enzymes, and our microbiomecan’t deal with it. Studies have shownthat consuming dairy doesn’t decreaseour osteoporosis risk, and greens provide significant calcium. I tell all ofmy patients that I can treat their heartdisease with medications, but why nottry a plant-oriented diet?”
A meta analysis of studies involving a total of 900,000 people, published inthe South American Journal ofEpidemiology in September 2014, foundthat increased fiber from cereal and, to a lesser extent, vegetable sources,
decreased the risk of several chronicdiseases, including cardiovascular disease and diabetes.
Potential Benefits from Spices“I believe that spices, such aspomegranates, turmeric and cinnamon,can be beneficial,” Dr. Aggarwal states.“Pomegranates today are available inpowder form, juice, seeds, or whole inmost grocery stores. Turmeric is one of the most potent anti-inflammatoriesand anti-bacterials. Raw turmeric is hard to use, so powder is okay. I buy itfrom an Asian grocery store because it’s fresher. Including ground blackpepper with the turmeric allows yourbody to absorb the spice.”
The National Institutes of Health(NIH) reports that data on the value ofpomegranates in heart disease preventionis mixed. Some studies have shown thatit may lower cholesterol and systolicblood pressure, while others have shownno value. Likewise, the evidence forcurcumin, the active ingredient inturmeric that prevents platelets fromclumping together, to improvecholesterol levels, is inconclusive. Clearly,more research would be invaluable inhelping physicians guide their patients.
TM REDUCES CV RISK FACTORSDeveloped by Maharishi Mahesh Yogi and brought to this country in the1960s, Transcendental Meditation (TM)is one of many meditation approachesavailable to help people achieve a stateof relaxed awareness. Its proponentspoint out that it is the most clinicallystudied form of meditation, with morethan 380 peer-reviewed published studies documenting its health benefits,including a significant impact on cardiovascular health.
Norman Rosenthal, MD, clinicalprofessor of psychiatry at GeorgetownUniversity School of Medicine, is a well-known physician who espouses and practices TM. He explains, “Allmeditation practices are different. It’sunderstandable that people try to lumpthem together, but it’s like saying that all antibiotics are the same. TM involves sitting in a comfortableposition, closing one’s eyes and thinkingof the mantra that has been given to you by your teacher. It’s easy to learn but is a subtle process that helps to clear thoughts and distractions. Youlearn to let thoughts come and go, andto let the mantra come to you ratherthan working to go back to it.”
12 | CHESPHYSICIAN.COM
Marsha Seidelman, MD, internist in Silver Spring, Md.

JANUARY/FEBRUARY 2015 | 13
Stuart Rothenberg, MD, FAAFP,national director, TM HealthProfessionals Program, and teacher of continuing education in AyurvedicMedicine at the University of MarylandCenter for Integrative Medicine, adds,“The hallmark of TM is ‘transcending,’which means the mind automaticallysettles down to quieter and quieter levelsand ultimately goes beyond thoughtaltogether. TM is not mindfulness, whichprevents the mind from transcending.Instead, TM is experienced as a state ofcomplete relaxation that’s even deeperthan sleep. Patients tend to stick with itbecause it’s easy to do and pleasant.”
Like Dr. Rosenthal, Dr. Rothenbergpractices TM and has experienced itsbenefits first hand, both personally and in his medical practice. “I was myown first case study,” he recalls. “TMimmediately helped me feel less stressedand need less sleep. And shortly after Ibegan prescribing it to patients, a youngman found it helped him to quit smokingin six weeks, after other approaches hadfailed. Later, an 82-year-old malesignificantly reduced his blood pressureafter only two weeks of TM.”
Extensive Research DocumentsTM’s BenefitsNine randomized clinical trials havedemonstrated that TM has a significantimpact on hypertension, and concludedthat anti-hypertension medications can be decreased on average by 25%with this practice over a one-year period.In a June 2014 issue of Hypertension,the AHA stated that TM was the onlydocumented meditation practice forlowering hypertension, and endorses itsconsideration for use in clinical practice.
Additionally, a series of NIH-sponsored clinical trials and meta-analyses found that TM significantlyreduced insulin resistance, smoking and alcohol abuse, carotid intima-mediathickness and left ventricular hypertrophy.
More importantly, a five-yearrandomized controlled study publishedNovember 2012 in Circulation found anearly 50% decrease in death, heartattack and stroke in those who practicedTM, compared to the control group.
MD Referrals Cut Costs, ImproveComplianceDr. Rosenthal acknowledges, “There’sreal data from controlled studies of TM.But unless the physician really flags TMas helpful, patients won’t pursue it. Youcan’t just lump it in generally with other
recommendations like ‘exercise more.’You also can’t just give patients apamphlet – it must be taught. Physiciansshould refer patients to a qualifiedcenter.”1
Contributes Dr. Rothenberg, “Patients receive a discount if referred by a doctor, and free introductorysessions are offered to help patients learn more. The fee can be paid ininstallments and there’s a sliding scalefor those with financial needs.”
“Practitioners should check in with their TM teacher regularly,” Dr. Rosenthal adds. “There’s no extracharge, and the influence of the groupreinforces the practice. For those whoclaim they don’t have time, I say thatkeeping healthy takes time – you canspend that time in cardiac rehab afteryou have a heart attack, or in TMbeforehand.”
“You might think that I’ve just ‘drunkthe Kool-Aid,’” he laughs, “but I’ve beenrepaid many times over. You have to doTM regularly or it does no good. Butslowly, good things start to happen, and
thanks to TM, small stressors during the day bounce off my shoulders. Iwould no more think of skipping it than I would skip brushing my teeth.Your brain is different – ‘lightened’ –afterwards. TM is like a surge protectorfor life’s daily stresses.”
Dr. Rothenberg concludes, “TMcreates a state of transcendence. It’seffortless and a delight to learn andpractice.” Surely no patient ever felt that way about a pill they were taking.
OPTIMAL MANAGEMENT OF PADPatients with coronary artery disease arealso at higher risk for peripheral arterydisease (PAD). As with cardiovasculardisease, it’s critical for patients to comply with long-term lifestyle changesas part of PAD management.
Vinay Satwah, DO, medical director at the Center for Vascular Medicine(CVM), notes, “PAD risk factors aresimilar to cardiovascular risk factors –smoking, poor diet and lifestyle leadingto diabetes, high blood pressure andcholesterol, and increased age.Atherosclerosis begins in the coronaryarteries and migrates to the peripheralvessels eventually.” Patients may presentwith a variety of symptoms, includingbuttock or leg pain, cramping, ortightness that worsens with activity and alleviates with rest.
He adds, “The disease process can beasymptomatic starting in one’s 30s and40s, and manifest itself later on in life in the 60s or 70s. Patients will tell methat they’ve been good with diet, butthey don’t realize that the disease hasaccumulated over years and that it maytake years of lifestyle changes to halt the progression of PAD.”
Diagnosis Starts with Non-invasive MeasuresDiagnosing PAD starts with a simpleAnkle Brachial Index test (ABI), a blood pressure ratio that can performedin the primary care office. However, Dr. Satwah cautions physicians, “Whendetermining the ratio of blood pressurein the arm to that in the ankle, makesure that the higher brachial number is used as the denominator for bothmeasurements, regardless of which sideof the body it was on.
“The gold standard is a ratio of 1,with 0.6 to 0.7 indicating a definite caseof PAD; under 0.6 indicating a severecase and under 0.5 denoting critical limb ischemia, in which case it must betreated quickly,” he continues. ”If youget a reading above 1.2, it could indicatea diabetic with non-compressable vesselsthat have hardened so much we cannotget an accurate reading. In those cases,ABI is not a good predictor of PAD andwe may need to obtain toe pressures.”
The next test is pulse volumerecording, a physiological study thatlooks at changes in blood-vessel volumefrom the proximal leg down through thedistal thigh and into the calf, andtranslates it into waveforms. Dr. Satwahnotes, “If the waveforms are high in the
THERE’S REAL DATA FROM CONTROLLED STUDIES OF TM. BUT UNLESS THE PHYSICIAN REALLY
FLAGS TM AS HELPFUL, PATIENTSWON’T PURSUE IT.
- Norman Rosenthal, MD

proximal thigh but drop significantly at the calf, it’s likely hemodynamicallysignificant disease between the twosegments. Those patients should bereferred to a vascular center.”
Arterial duplex ultrasound is anotheruseful tool used to evaluate blood flowin the leg. “Only a specialized vascularultrasound technologist should performthis study,” cautions Dr. Satwah.“Increased velocity is suspicious forPAD, but not foolproof. Patients whoare obese, have significant gas oredematous legs may not have accurateresults.”
Invasive Testing Angiograms remain the gold standardfor evaluation of patients who haveabnormal non-invasive test findings.“We look for the anatomical location,degree of narrowing and presence of
complete obstructions to help plan ourinterventional treatment strategy,”explains Dr. Satwah. “If we find a lesion,my preference is usually to fix it in thesame setting, unless, in rare cases, thepatient requires open bypass surgery or has a renal issue.”
Conservative TreatmentThe first ‘prescription’ for PAD is 30 to 45 minutes of continuous aerobicactivity at least five times a week.According to Dr. Satwah, “As long asthe heart rate increases to our target rate(about 220 minus the patient’s age) forthat time frame, whatever activity thepatient prefers is fine. Patients who haveintolerable pain should discontinueexercise, but pain from mild PAD oftendiminishes with continuing activity.”
Other conservative approaches involveswitching to a low-cholesterol, low-fatdiet that will also help keep the patient’sblood glucose levels under control, andsmoking cessation. Dr. Satwah says “We typically try these approaches forthree months in patients with mild tomoderate PAD. If they have pain at restor a non-healing leg ulcer, however, webypass conservative measures, since thistypically indicates very advanced PADwith tissue threat. These patients shouldbe referred for a PAD workup by avascular physician immediately.”
Atherectomy and BypassWhen the plaque is eccentric and bulky,an atherectomy can be performed to‘shave off’ some of the plaque beforeperforming balloon angioplasty. Dr.Satwah points out, “Studies that have
compared angioplasty alone withangioplasty plus atherectomy found that the rate of restenosis is higher withangioplasty alone. There are a variety of modalities we can choose from,depending on the patient’s anatomy,plaque location and amount ofcalcification. All entail a small risk ofembolization, but heparinization duringthe case, and new technologies havegreatly reduced that risk. For very high-risk patients with chronic totalocclusions (CTOs), we can insert a distalprotection device that catches debrisbefore it can lodge into a tiny vessel.”
In Dr. Satwah’s experience,interventional treatment can last manyyears in a compliant patient, but lessthan six months in someone that is non-compliant. Bypass surgery can beefficacious over the long term in theabsence of multiple comorbidities.
The FutureToday in the U.S., stents for PAD arenitinol based (bare metal), but Dr. Satwahbelieves that drug-coated balloons, whichare currently in use in Europe, will bewidely available here soon. “I think FDAapproval is coming within the next year,and it’s available now in clinical trials.The physician will inflate the balloon, letthe medicine coat the arterial wall, thendeflate the balloon,” he explains. “Themedicine helps control the amount ofplaque recoil.”
“It’s a privilege that patients entrusttheir bodies to my vascular care,” heconcludes.
1 Visit www.tm.org for a listing of area TM centers.
14 | CHESPHYSICIAN.COM
Monica Aggarwal, MD, a cardiologistand director of Echocardiography,
Mercy Medical Center
Marsha Seidelman, MD, an internist in Silver Spring, Md.
Norman Rosenthal, MD, clinicalprofessor of psychiatry at Georgetown
University School of Medicine and
author of Transcendence: Healing and
Transformation Through Transcendental
Meditation
Stuart Rothenberg, MD, nationaldirector, TM Health Professionals
Program
Vinay Satwah, DO, interventionalcardiologist and medical director,
Center for Vascular Medicine
...IT MAY TAKE YEARS OF LIFESTYLE
CHANGES TO HALTPROGRESSION
OF PAD.- Vinay Satwah, DO
Vinay Satwah, DO, interventional cardiologist and medical director, Center for Vascular Medicine

H O S P I C E
R O Y A L EM A R C H 2 1 , 2 0 1 5
6 P M - M I D N I G H T
H I L T O N B A L T I M O R E B W I H O T E L
F o r m o r e i n f o r m a t i o n o n s p o n s o r s h i p s o r t i c k e t s , p l e a s e v i s i t www. h o s p i c e c h e s a p e a k e . o r g o r
c o n t a c t C h r i s W i l s o n a t 4 4 3 - 8 3 7-1 5 3 0 o r c w i l s o n @ h o s p i c e c h e s a p e a k e . o r g .
B O N D W I T H U S
16 | CHESPHYSICIAN.COM
Life expectancy in the U.S. has increased, but lifewithout disability has not.This means physicians are treating more patients with advanced complexillnesses (ACI). ThreeMaryland physicians discuss how they providecompassionate, anticipatorycare for patients andcaregivers.
Caring For
{ADVANCED}COMPLEX ILLNESSES
BY LINDA HARDER
MOST PROTOCOLS AND GUIDELINES AREwritten for a single disease that is amenable totreatment. Yet the number of frail patients withmultiple diseases continues to increase. These patientsaren’t dying, but they are in the final stage of life.Finding the balance that will help them live well with illness is one of our greatest challenges. While a growing number of physicians understand thistrajectory, recognizing the point at which aggressivecare may be detrimental is not easy, and the task of getting patients and caregivers on the same page can be daunting.
WHAT IS ACI?Lou Lukas, MD, director of Chesapeake PalliativeMedicine, uses the term Advanced Complex Illness, or ACI, to describe the syndrome of failingphysiology that is common to many late-stage illnesses.ACI patients have high, though unpredictable,mortality, complex bio-psycho-social symptoms andfrequent or intense healthcare utilization. The hospitalhas become a regular part of their treatment. “It’s thepoint at which the risk/benefit ratio of treatment is

skewed permanently toward risk, and the burdens oftreatment may outweigh the benefits,” she explains.“It doesn’t mean you throw in the towel, but youmake very selective treatment choices.”
ACI typically involves one of three trajectories,each with its own pattern of decline:
z End organ damage such as CHF and COPDz Metastatic or highly aggressive malignanciesz Medical frailty and/or advanced dementia
Patricia Czapp, MD, a primary care physician and chair of Clinical Integration at Anne ArundelMedical Center (AAMC), notes, “ACI is progressive,regardless of what we do. I ask patients if thestandard treatment they’ve received has helped themmaintain or improve their quality of life or regain lost functionality. If not, they likely have ACI and it’stime to have a different type of treatment discussion.”
PRACTICE ANTICIPATORY GUIDANCEWhen a patient has ACI, physicians should shift intoanticipatory guidance mode. Dr. Lukas explains,“Physicians have to use the knowledge andexperience we have gained about advanced illness and use it to help patients understand the road ahead.We need to be honest in helping them understand that their condition is progressive, and will haveexacerbations and decline, but that we can improveboth the quality and length of life by taking a two-pronged approach to planning. We need ‘Plan A’ toavoid complications and maintain function, and ‘Plan B’ for what we do we do when things get worse.”
She goes on to say, “If we focus on ‘end of life’ weget caught up in conversations about code status andventilators. Instead the conversations we should beencouraging are those about what makes life worthliving and how to get more of that into the time theyhave. Then we can help them decide which medicaltreatment will support their goals and whichtreatment exposes them to more risk than benefit.”
Aimee Yu, MD, FCCP, a pulmonologist andintensivist at AAMC, says, “I explain that the body has a budget of energy. Treatments such aschemotherapy can zap that energy store withoutbenefit and sometimes even cause harm. For example,it’s not widely known that inserting a feeding tubewill actually hasten death in patients with dementia.The American Thoracic Society has issued newguidelines that contraindicate feeding tubes for these patients.”
THE PROBLEM WITH “END OF LIFE” CONVERSATIONSThe Institute of Medicine released a report in the fall of 2014 entitled, “Dying in America: ImprovingQuality and Honoring Individual Preferences Near the End of Life,” that urges clinicians to havefrequent conversations with their patients about end-of-life care. Yet, while 80% of patients would
like to have an end-of-life conversation with theirdoctors, only 8% have actually done so, according to 2012 data.
Dr. Lukas says, “All doctors who have treated frail patients have been surprised by how long somepatients live and how unexpectedly some patients die.That uncertainty keeps us from having conversationswith patients who are experiencing a downwardtrajectory.”
“Ideally, physicians should make this conversationroutine so it’s part of the history and physical,” Dr. Yu advises. “Ask patients what their wishes arebefore they’re in crisis.”
Dr. Czapp adds, “Physicians should ask themselvesif they think the patient can ever get back to where heor she was before. If not, is it okay for us to continuesolely with this conventional treatment, or is it time to offer treatment that fits with this patient’sunique situation and goals?”
A good resource for physicians, patients andcaregivers is The Conversation Project(theconversationproject.org), an initiative started by Boston Globe columnist Ellen Goodman andothers in 2010. The site contains a ‘conversationstarter kit’ in both Spanish and English that can helppatients converse with family members and doctors.
TOUGH DECISIONSSometimes families wait too long to have theseconversations. “When a patient can’t speak for herself and the family isn’t sure what to do, I start by asking caregivers to tell me about their Mom,” Dr. Yu explains. “What does she like, how did shegrow up? And knowing Mom, what do you think we should do? I make it clear that I care about theperson, and tell them up front I’ll be honest withthem and let them know how things are going. The family wants to see that you’re making an effortand caring. That approach works across cultures.”
JANUARY/FEBRUARY 2015 | 17
Aimee Yu, MD, FCCP, a pulmonologist and intensivist at AAMCand Patricia Czapp, MD, a primary care physician and chair ofClinical Integration at Anne Arundel Medical Center.
PHOTO COURTESY OF AAMC

If families argue among themselves over theappropriate course of care for their loved one, Dr. Czapp suggests, “Physicians can tell patients thatit’s not our decision to make. The patient’s body has already made the decision. If a patient or familymember says, ‘I’m holding out for a miracle,’ you can say, ‘me, too, and let’s prepare in case that doesn’t happen.’”
Dr. Yu describes the situation of one elderly man in the ER who had advanced esophageal cancer. “The family was urging that all possible interventionsbe used. The patient was weak, but alert. Using allthe breath he could muster, he slowly whispered asingle word: ‘dig-ni-ty’. That turned the familyaround immediately.”
“Family members who want futile, aggressivetreatments may equate these treatments with love,”Dr. Czapp notes. “We need to help them see in cases like these, love can be expressed by providingcompassionate care that respects the body’slimitations.”
PALLIATIVE AND HOSPICE CAREBy the time a patient has ACI, there are few, if any,truly “curative” treatments. Palliative medicine is an approach to patient care that acknowledges thisand emphasizes symptom control and good decision-making. It doesn’t place any limits on the patient’streatment and is appropriate at any point in a serious diagnosis.
Hospice can be an appropriate next step forpatients with ACI. Unfortunately, both the public and the medical community may have misconceptionsabout these services. Hospice is a specific benefit thatentitles patients and families to team-based servicesprovided in the patient’s home to help them come toterms with circumstances when aggressive treatmentdoesn’t bring additional benefit.
As Dr. Lukas points out, “At the center of hospiceand palliative care is the belief that each of us has the right to die pain-free and with dignity, and thatour families will receive the necessary support toallow us to do so.”
A BETTER WAY TO WRITE THE PLAN Once a plan is in place, it should be written in a waythat will be respected even when the physician is notthere to direct care. Living Wills were developed forthis purpose, but have been found to suffer fromseveral major limitations. They are conditional, often not available when or where needed, and maynot apply to the actual situation because they werewritten years earlier. They also don’t carry the weightand durability of a medical order.
To address these issues, more specific, portable and durable medical order forms have been createdby many states. Nationally, these forms are known as Physician Orders for Life Sustaining Treatment(POLST). In Maryland they are called MedicalOrders for Life-Sustaining Treatment (MOLST) and
in Virginia, where forms are still in development, they are called POST.
MOLST, which became law in 2013, conveysorders for CPR and other life-sustaining treatments. It must be completed for patients entering a nursinghome, home healthcare, hospice, dialysis or assistedliving, but can be useful for anyone with a seriousillness. A physician, physician assistant, nursepractitioner or medical resident can completeMOLST. More information can be found atMarylandMOLST.org.
Dr. Czapp points out, “The key to using MOLST is to understand that it can be your friend. Don’t beoverwhelmed by it. We all have to fill out page one,which addresses resuscitation status. When it comesto the specific treatment sections on page two, youonly need to discuss the options that fit your patient.For example, a congestive heart failure patient shouldexpress an opinion about intubation and dialysis.”
Dr. Yu concludes by saying that doctors shouldoffer to help people with hard decisions. “Sometimesdoctors don’t make recommendations because wewere taught to honor patient autonomy and not to be ‘paternalistic.’ Now we understand that, in thesesituations of deep emotion and complex decisions,patients and families appreciate it when we are‘parental,’ offering nurturing, informed advice whilerespecting their need to make up their own minds.”
18 | CHESPHYSICIAN.COM
Lou Lukas, MD, CMO, director of Chesapeake Palliative Medicine
Patricia Czapp, MD, chair of Clinical Integration, Anne Arundel Medical Center
Aimee Yu, MD, FCCP, pulmonologist and intensivist,Anne Arundel Medical Center
IS MEDICARECOVERAGE IN SIGHT?Lack of reimbursement has been one barrier to
these conversations. At the time of publication,
while some Medicare Advantage plans and a few
state Medicaid providers reimburse for specific
end-of-life conversations, traditional Medicare
coverage does not. That may be changing in 2015,
if CMS approves coverage of the billing codes
for end-of-life conversations submitted by the
American Medical Association in 2014. Medicare
coverage likely would spur expanded private
coverage. While no universal code currently
exists for this conversation, physicians can bill for
their additional time when counseling and
coordinating care using existing E&M codes.
Clinical FeaturesIn each issue, Chesapeake Physician interviews some ofthe region’s top specialists to spotlight the latest clinical developments, including leading-edge diagnostic and treatment options.
Healthcare ITChesapeake Physician explores ongoing major healthcareIT developments and the new care delivery models thatdepend on them, from interoperability issues to the lateston Meaningful Use, ACOs, Medical Homes, mobile health,hospital employment, mega groups, and more. Don't be left behind – read what Chesapeake physicians andhealthcare IT experts have to say that keeps you abreast of the latest technology changes in every size and type of medical practice.
In Every Issue and OnlineCases xSolutions xCompliance xPolicy
@chesphysician
Jacquie Cohen RothFounder/Publisher/Executive Editor
443.837.6948 x[email protected]
JANUARY/FEBRUARY 2015 | 19
PhysicianYOUR PRACTICE. YOUR LIFE.
C H E S A P E A K E
Maryland/DC/Virginia www.chesphysician.com
20 | CHESPHYSICIAN.COM
HEALTHCARE IT
BY LINDA HARDER • PHOTOGRAPHS BY TRACEY BROWN
The Impact of Insurance Changeson Patients and Physicians
Daniel Levy, MD,owner of The Childand Teen WellnessCenter, a pediatricgroup practice in Owings Mills, Md.

JANUARY/FEBRUARY 2015 | 21
S HEALTHCARE COSTSrose far faster than inflation in the pastdecades, employers and insurers alikelooked for strategies to rein in theirexpenses. With the average cost ofinsuring a family in excess of $17,000per year, they are shifting costs onto theend user in the form of higher premiums,co-pays, co-insurance and deductibles,plus implementing tiered prescriptiondrug plans, to the point where patientsare pinched by higher out-of-pocket costs.
In 2013, a Deloitte study found thateven employer-sponsored plans had an
average deductible of $1,135, and aKaiser study determined that the averagedeductible in a high deductible plan was$2,098 for a single person and $4,037for a family.
The Affordable Care Act (ACA)capped the amount that can be shiftedonto patients in its healthcare exchangeplans, but even its out-of-pocket limitsare higher than the average householdcan afford - $6,600 for an individual and $13,200 for a family in a bronzeplan in 2015.
According to a survey of largeemployers by the National BusinessGroup on Health, nearly one-third willoffer only high deductible plans in 2015,up from 10% in 2010. Slightly morethan 80% of these companies offer suchplans as one option of several, up from53% in 2010.
Drowning in Medical DebtKaren Pollitz, senior fellow at the Kaiser Family Foundation, says, “Nearlyall exchange plans have high deductibles.A study conducted by the FederalReserve this summer found that mosthouseholds couldn’t handle anemergency of $400, let alone thousandsof dollars. Providers usually want to bepaid within 90 days, but people don’tkeep much in reserve, and medical debthas become a huge problem, even among those with health insurance.”
In fact, NerdWallet reports thatmedical debt is the chief cause ofpersonal bankruptcy and responsible for more collections efforts than creditcards. An astonishing 40% of Americansare being pursued by collection agenciesfor unpaid medical bills.
Growth in Consumer-Directed Health PlansEven as healthcare cost increases havebeen moderating – estimated to grow6.5% in 2015 – employers continue tolook for innovative approaches to reducecosts. Consumer-directed health plansseek to reduce healthcare spending byexposing consumers to the financialimplications of their treatment decisions.However, that approach doesn’t workwell for major medical emergencies.
Do Patients Know What They’re Buying?“The biggest issue is that so many issues haven’t been adequately explainedto the public,” says Daniel Levy, MD,owner of The Child and Teen WellnessCenter, a pediatric group practice inOwings Mills, Md. “We have to explainthe insurance parameters to patients –they don’t know what they’re buying.People are then angry when we ask to be paid for our services. The medicalindustry office is the only place wherepeople are shocked when asked to pay at the time of service.”
However, Carolyn O’Conor, MD, afamily practitioner at Spectrum FamilyMedicine in Rockville, Md., has found that her patients are fairly costconscious. She notes, “We have a large,internationally-diverse practice. Peopleare more aware of what things cost. My patients are very aware of whenthey’ve met their deductible. As a result,they get a lot of their care at the end of the year. The flip side is that manyplans now provide a wellness visit at no charge, so it has had a positiveimpact on physicals.”
Dr. O’Conor has also seen a positiveimpact from the ACA’s provision thatallows children to stay on their parents’plan until age 26. “Previously, thatgroup was often uninsured. We try tohelp patients work through the issues to help them. We also see the impactwith our own employees – we used tocover the entire medical bill, but nowthey pay a small percentage. And wehave gradually gone to a higherdeductible plan, but we have done ourbest to keep them insured.”
New Tactics to Curb Medication CostsAnother tactic, the creation of specialtytiers with graduated copays forexpensive medications, has requiredmany patients to pay 20 to 40% of their annual prescription costs until their deductible is met. According to aDecember 2013 study by Avalere Health,a private research company, 91% ofplans sold through the healthcareexchanges in 2014 had four or more‘tiers,’ for medications and diseases.
A
Healthcare has longbeen paid for in theU.S. via a byzantine set of policies andstructures. As costshave risen, patients arepaying a higher shareout of their ownpockets. Our expertsexamine the latesttrends and their impacton your practice.

22 | CHESPHYSICIAN.COM
Crohn’s disease, rheumatoid arthritis,MS and some cancers were all in thehighest tier. HR 490, federal legislation,first introduced in 2011 and slated to be reintroduced in 2015, attempts toaddress this issue. However, its passageis far from certain.
In addition to specialty tiers, so-called ‘step therapy,’ the practice ofrequiring patients to try less costly drugs before using more expensivespecialty medications, is on the rise.These policies can have direconsequences for some patients, such as those with primary immune disorders,where switching medications or beingrequired to get sick before they canreceive appropriate treatment, has a high cost to their health.
Dr. O’Conor says, “I encouragepatients to call us if something we have prescribed is costly, as there may be another way to go. I never want to prescribe somethingunnecessarily expensive.”
Prior AuthorizationsAnother approach to control costsrequires doctors to obtain priorauthorization for some medications. Dr. Levy notes he now spendsconsiderable time obtaining priorauthorization for medications that hispatients have used for years, noting, “It boggles the mind. These childrenhave had ADHD or other chronicdisorders for years, yet suddenly we need authorization. Once we arrive at a good homeostasis, we want tomaintain, not jeopardize that.”
He adds, “Less than 10% of medicalcare dollars are spent on children, yetthose dollars have been shown to besome of the most worthwhile dollars we could spend. A dollar spent now on a child’s care is worth hundreds orthousands of dollars later, preserving his or her ability to thrive.”
Debbie Redd, CEO of CapitalWomen’s Care, a group of about 160 OB/GYNs in multiple locations
throughout Maryland, notes that theirspecialty presents a unique challenge.“We treat our obstetric patients for nine months without getting paid. Thatmakes it very important for us to knowup front what insurance they have. Wedo a lot of pre-authorization work afterthey call to make an appointment andwe collect a deposit and copays up front even if we have to later refund thepatient some money. We do a good jobon that. As a result, we haven’t seen anincrease in our bad debt.”
Redd acknowledges that it may be
harder for smaller practices to verifyeligibility. “Our large size allows us to put more processes in place. Thesystem automatically goes out to verifyeligibility with all of the payers thepatient provided. We outsource thisservice to a billing company, and thisservice is part of their fee. We then verifytheir insurance again after the secondand third trimester, as it can change.”
She adds that many women who are
planning to get pregnant select a lowerdeductible plan if they have the option.
Insurer-Hospital Partnerships, Narrow NetworksAnother insurance trend affectingphysicians are partnerships betweenhospital systems and insurers. Redd cites Innovation Health, a joint venturebetween Aetna and Inova in Virginiathat initially covered Inova’s employeesbut that has expanded to cover manyresidents of Northern Virginia. “Ourgroup is no longer a Tier 1 provider, sopeople have to pay more to see ourobstetricians. Ironically, that will cost the healthcare system more in the longrun because it’s cheaper for us to providecare than it is for OB/GYNs employedby the hospitals.”
A NBGH survey found that about25% of employers now offer a ‘narrownetwork’ plan among their options toworkers. These plans lower the premiumcost but offer a narrower choice ofparticipating providers.
A McKinsey & Co. survey found that nearly half of ACA plans offerednarrow networks in 2014. Care providedoutside of the networks receives little orno coverage. Surprisingly, however, astudy by the Robert Wood JohnsonFoundation of the ACA implementationin six states, including Maryland andVirginia, found few consumercomplaints about these narrow
My impression is that, overall, the ACA is a goodthing. It’s the history of the way health insuranceis set up in this country that’s the problem. – Carolyn O’Conor, MD
Debbie Redd, CEO of Capital Women’s Care

The Outdoor Kitchen ExpertsThe Outdoor Kitchen Experts
SHOWROOM: 1526 Jabez Run, Unit C Millersville, MD 21108
www.chesapeakeoutdoorliving.com 410-696-7300
Over 15 Manufacturers on Display including Alfresco, Lynx & Twin EaglesOver 15 Manufacturers on Display
hesapeakeoutdoorli
1526 J
.cwwww
: WROOMSHO
Ly
410-696-7300
including Alfresco,Over 15 Manufacturers on Display
, MD 21108
ving.comhesapeakeoutdoorli
illersvilleabez Run, Unit C M1526 J
nx & Twin Eagles
410-696-7300
Ly
, MD 21108
JANUARY/FEBRUARY 2015 | 23
networks. A greater issue for patientswas the inaccuracy of many listings ofparticipating providers.
Implementation of Strong Verificationand Collections SystemsPollitz advises doctors to evaluate theircollections practices to see how muchtime patients have to pay their bills.When patients’ bills go to a collectionagency, they may no longer be able to get auto or other types of loans, and ifthey start charging up their credit cardsthey could be paying double-digitinterest rates. She notes that what theyowe is a pressing issue on many patients’minds, even if they don’t bring it up with their doctors.
A recent Gallup poll found that thesteady climb in those delaying care dueto costs had reached its highest levels yet – some 33% of respondents – sincethe question was first asked in 2001.
At the same time, Dr. Levy laments the growth in his practice’s accountsreceivables. “People don’t understandthey are partners in helping to pay fortheir care.“ To address the problem, he has retrained his front office staff.“As soon as people walk in and we’vewelcomed them, we verify theirinsurance. If a patient owes us moneyfrom a prior visit, we trained our staff to say, ‘You have an outstanding bill,how would you like to pay?’ If thepatient is unable to pay, and has aroutine or longstanding complaint rather than an urgent medical problem,we tell them we have to reschedule their appointment and ask that theybring payment next time.”
While acknowledging that the ACAisn’t perfect, Dr. O’Conor views it as an improvement. “I’m here to help mypatients with their health issues. Myimpression is that, overall, the ACA is a good thing. It’s the history of the wayhealth insurance is set up in this countrythat’s the problem. I think the ACA willbe seen as an incredible legacy forPresident Obama.”
Is there a doctor in the house?
Physician’s Mortgage ProgramPurchase or Refinance
Primary or Second/Vacation Homes
High Loan-to-Value with No Mortgage Insurance
Great Rates
Loans Serviced Locally
Million Dollar+ Loans
Low Down Payment
*Applicant must be an existing or newly licensed doctor. Loans subject to program availability and credit approval. Terms and conditions may apply.
Call or visit410.260.2000
severnbank.com
Karen Pollitz, senior fellow at the Kaiser Family Foundation Daniel Levy, MD, pediatrician, owner of The Child and Teen Wellness CenterCarolyn O’Conor, MD, familypractitioner at Spectrum Family Medicine Debbie Redd, CEO, Capital Women’s Care

BY LINDA HARDER • PHOTOGRAPH BY TRACEY BROWN
24 | CHESPHYSICIAN.COM
ESPITE HIS 28 YEARS INthe Maryland state legislature, SpeakerMichael Busch has never taken thesplendor of the House chamber forgranted. With its soaring, ornately fluted columns and curving rows ofplush tufted chairs, the chamber is aninspirational setting for the years oflegislative wrangling that have takenplace within its walls.
In addition to having a RepublicanGovernor, for the first time in years,Maryland’s General Assembly willinclude four physicians. NewcomersTerri Hill, MD, Jay Jalisi, MD, andClarence Lam, MD, were elected to servealong with incumbent Dan Morhaim,MD. A fourth physician running thispast year, Dr. Tim Robinson, lost to JimBrochin.
Q: You’ve had a long tenure asSpeaker of the House (since 2003).Looking back, what healthcareaccomplishments are you most proudof? What were the biggest challengesyou faced in the healthcare arena? I’vebeen part of the House for 28 years. Itell people that I was only elected for afour-year term but stayed for 28. I washere as chair of the committee thathandled health insurance in 1995 whenwe passed the Patient Access Act, whichrequired insurers to offer a point-of-service plan in addition to a closed-panelHMO, so that individual patients couldget to the doctor they had a relationshipwith.
That model was duplicated elsewherearound the country. It was a big battleand a significant piece of legislation. Wehad to battle the insurers over it. We alsoeliminated withholds. The insurerspromised primary care physicians theywould give them a pool of patients andwithhold, say, $2 per member per month
and if they kept costs down, thephysicians would get it back. Physicianskept the costs down but never got theother $2. We did away with that andpassed the Patients’ Bill of Rights.
Q: What do you think about thatnew waiver? The new waiver is goingto cause some constraints and movesome people out of the traditionalhospital setting into primary care andambulatory care groups. So, I think itwill be a challenge initially for hospitalsto make their numbers, but hope that theultimate result will be better overallhealth outcomes for patients. If youremoved the all-payer system or thewaiver, you’d have tremendousinstability in the marketplace, withhospital closings all over the state.
Q: What are the challenges facingyou in the upcoming Marylandlegislative session? I think the greatest
challenge we’ll face is finding a healthsecretary to head what is a verycumbersome agency with a lot of movingparts. You have the physician reviewboard and all of the professional boardsto oversee. [Secretary of the Departmentof Health and Mental Hygiene] Dr.Joshua Sharfstein and [Chairman of theHealth Services Cost ReviewCommission] John Colmers are bothtalented guys who have been tremendouspublic servants. Colmers had served onthe transition of CareFirst and headedthe HSCRC. There was a tremendousamount of pressure on both men.
The greatest undertaking is to find ahealth secretary that understands thecomplex delivery system in the state, andthen to deal with the federal mandates ofboth Medicare for the dual eligibles andMedicaid. I’ve had a conversation withGovernor-elect Hogan, who has to get abudget secretary first and has a lot on hisplate, but then health and transportationhave to be next. The Department ofHealth and Mental Hygiene has one of
POLICY
Michael Busch: 11 Years as Maryland’s House Speaker
D

JANUARY/FEBRUARY 2015 | 25
the largest budgets in the state, and ontop of that is charged with the care ofsome of our most vulnerable citizens.
Physicians have had it tough becausetheir reimbursement has gone down atthe same time that costs are rising andtheir medical malpractice has gone up. In an all-payer system, the hospitals getpaid but the physicians don’t. Manyhospitals have a dwindling physicianbase in certain specialties, such asOB/GYNs that are supplemented by thehospitals they serve or solely owned bythe institution. At one point, we didn’teven have an obstetrician in WesternMaryland – fewer people are going intothat field. After you get done payingmalpractice and other administrativeexpenses you get tail insurance so that if something happens 15 years later, you have to pay for that even when you stop practicing.
Q: What can physicians do toincrease their influence in thelegislative process? My suggestion tophysicians is to let your patients knowwhen they come into your office what’simportant, and to suggest that theycontact their legislators.
Q: How do you think therepublican majority in the U.S.legislature will impact the AffordableCare Act (ACA)? For all the screamingand yelling, I think they will let the ACAplay out. It’s too far down the road toeliminate it now.
Q: Maryland’s Medical MarijuanaCommission continues to struggle tocreate a viable model for making thisaccessible to patients. How do you seethis process unfolding this year? Whatyou want to do is see whether or not thestructure that was set up works. There’sa practical application to how youactually deliver the service withoutviolating the law. Delegate Morhaimworked very hard at that and it was acontroversial issue. I don’t think its
medicinal benefits to certain patients canbe challenged; the argument is clear thatit can be helpful, but how do younavigate its use for medical purposesonly, and keep it out of the hands ofpeople who want to use it recreationally?
Q: There apparently is a longwaiting list for people withdevelopmental disabilities to getneeded care. What have you done toaddress this problem? What are thekey barriers to care? What futurechanges do you see coming? When wepassed the alcoholic beverage tax, wededicated quite a bit of money – about$30 million annually – to developmentaldisabilities, which includes a wide spectrum of disabilities, with autismbeing one of the primary ones. Thosewith severe autism fall under the school
system until they’re 18, but once they’reout of school it can be hard for familiesto deal with them as young adults whocan’t function without some level ofsupervision. We’ve tried to increase thefunding of disabilities through this tax.There is a waiting list, but everythingcomes down to whether there issufficient money.
Q: What was your involvement inpromoting the Patient CenteredMedical Home (PCMH) concept inMaryland and how do you think it’sworking? PCMH is nice in theory and itgoes back to the primary care physician,obviously, but I would suggest thatPCMH is something for which hospitals,physicians and insurers all have adifferent definition. It’s a great idea butit’s a question of who designed thatmedical home and who is the gatekeeper– is it the insurance company that paysthe physician or the physician group thattries to make sure healthcare is deliveredappropriately, or is it the hospital? Thetwo models in the state – CareFirst BlueCross Blue Shield’s and the state’s model– are vastly different, and it comes down
to which stakeholder makes thedetermination of what a medical home is.
Q: You worked hard to preventBlue Cross Blue Shield from becomingprivatized. Talk about that experience.At the time, I felt that privatization wasa windfall for the members of the boardand the executive staff of Blue CrossBlue Shield and a detriment to thehealthcare resources in the state. Most ofthe Blue Cross plans in the country wereundervalued when they were sold andthen became extraordinarily wealthyorganizations. One side said that the fairprice for Maryland’s plan was $2 billionand the other side said that was too low.I felt it was very important to keep anonprofit insurer in the state.
At the end of the day we had anestablished process to go through thatworked for us. Candidly, when westopped the conversion here, it was thelast attempted conversion in the country.It was no easy task to convince thenational Blue Cross Blue Shield boardthat they should continue to give use tothe ‘mark,’ as they call it. But theycouldn’t justify the compensation thatwas going to go to the individuals.
Our fear was that as soon as theybecame a for-profit, they would bereluctant to take on risk. It’s easy toinsure the healthiest people, but it’s notso easy to insure the sicker ones. Assomeone once said, pre-existingconditions mean you can get healthcarefor everything except what you were sick with.
Q: What are your predictions aboutthe healthcare exchange this year andits ability to serve new and re-enrolling consumers? There’s still someskepticism around the ACA. In theory,it’s the right way to go, but it’s thepractical delivery of that service thatpeople are concerned about. InMaryland, as with other states aroundthe country, we experienced somedifficulty in our initial attempts to enrollindividuals in coverage. Having madesome significant changes to the stateexchange, we seem to be on betterfooting with this second wave ofenrollment. Now the question becomesthe degree to which we improveaccessibility and cost for the individual.
Physicians have had it tough because their reimbursement has gone down at the sametime that costs are rising, and their medicalmalpractice has gone up.

26 | CHESPHYSICIAN.COM
Physicians Physical Therapists
yregrusrosgurdredisnocylesicreptahtsreudecorpstsiparehTlaalcisyhPdnaruO.llatisyaaysemanehT
uoyreKuotyaaywtsebehtreovcsidyniapkcendnakcabruoyhtiwlaedyyteiravanidecneirepxeylhgihreasnaemhcaorppayranilpicsid-itlmur
.niapru oyreoffoeB.
l acigrus-nonfoysnaicisyhPruosn
Most Insur
epain.comkur
ances AcceptedMost Insur
epain.com
ADVERTISER INDEXAdvanced Radiology .............................................................2advancedradiology.com
Pain & Spine Specialists of Maryland ...........................5passmd.com
PNC .................................................................................................6pnc.com/hcprofessionals
Greenwich Group ....................................................................9ncrmc.greenwichgrp.com
Hospice of the Chesapeake Foundation...................15hospicechesapeake.org
Papercamera............................................................................19papercamera.com
Sheppard Pratt Health System ......................................19eatingdisorder.org
Chesapeake Outdoor Living ...........................................23chesapeakeoutdoorliving.com
Severn Savings Bank ..........................................................23severnbank.com
KURE Pain Management ...................................................26kurepain.com
Center for Vein Restoration ............................................31CenterforVein.com
CVM .............................................................................................32cvmus.com
Strategize and increase the power of your marketing to Chesapeake-based physicians, healthcare executives and
stakeholders via chesphysician.com and with Chesapeake Physician eNews blasts.
Chesapeake Physician eNews exceeds all leading industry digital performers.
Drive a higher volume of targeted traffic with Chesapeake Physician online.
Jacquie Cohen RothFounder/Publisher/Executive Editor
ONLINEchesphysician.com
@chesphysician
We’ve Listened & We’ve Expanded!
PhysicianYOUR PRACTICE. YOUR LIFE.
C H E S A P E A K E
Maryland/DC/Virginia www.chesphysician.com
PhysicianYOUR PRACTICE. YOUR LIFE.
C H E S A P E A K E
Maryland/DC/Virginia
Maryland Physician welcomes new physicians and healthcare stakeholders in D.C. and Northern Virginia to our readership. Our quality-driven content and events focus on leading-edge treatments and practical
advice for managing clinical practices of all sizes.
Maryland Physician re-brands as:
www.chesphysician.com

JANUARY/FEBRUARY 2015 | 27
COMPLIANCE
False Claims Investigations:Ten Best Practices for Complyingwith DOJ Subpoenas
By Ilana Subar
HE OBAMA ADMINISTRATIONhas made healthcare fraud cases a toppriority since for the past five years. In2009, Attorney General Eric Holder andHealth and Human Services SecretaryKathleen Sebelius established aninteragency task force, the FraudPrevention and Enforcement ActionTeam, to increase coordination andoptimize civil and criminal enforcement.This coordination has yielded historicresults: from January 2009 through theend of the 2014 fiscal year, theDepartment of Justice (DOJ) used theFalse Claims Act (FCA) to recover $14.5billion in federal healthcare dollars.
What can physicians and otherhealthcare providers do to prepare for,and respond to, DOJ subpoenas in thecurrent enforcement climate? Here are 10tips that can help mitigate the challengesin responding to DOJ subpoenas:
z Be Proactive and Prepare In AdvanceEven before you or your company isserved with a subpoena, you shouldmake sure that you have an activecompliance plan and policies forresponding to subpoenas and governmentinvestigations. Such policies shouldprovide for the involvement of insideand/or outside counsel. This will helpprotect the attorney-client privilege in the company’s assessment and response.
z Engage Legal Counsel and PreserveDocuments Immediately after receiving asubpoena, the company should involvecounsel. Counsel will work with thecompany to take necessary steps topreserve potentially responsivedocuments, including electronic records.Counsel generally needs to issue a“litigation hold” letter, which notifies
the company of its obligation to preservedocuments. If directed to do so bycounsel, the company should send out an internal memo notifying anyone whomay have responsive documents of theirpreservation obligation.
z Try to Establish a Good Relationshipwith DOJ Establishing a good relation-ship with DOJ (and any U.S. attorney’soffice involved in the investigation) isimportant. It is often the best way toreduce the compliance burden ofresponding to a subpoena. Recipients,through counsel, should seek to learnwhatever details can be shared about theinvestigation and the company’s status,and to discuss the potential narrowing of the subpoena scope. Having a goodrelationship with DOJ also will be usefulif you ultimately decide to negotiate asettlement of FCA claims.
z Review Your Document ProductionBefore you produce documents to DOJ,you should have counsel carefully reviewyour production to ensure subpoenacompliance, to adequately protectattorney-client/work product privilegesand to identify any areas of risk.
z Be Prepared for Interview RequestsDOJ often asks to interview companypersonnel in connection with itsinvestigation. These interviews may be conducted under oath. With the helpof counsel, you should assess whethercompany personnel should berepresented by separate counsel.
z Conduct an Internal InvestigationYou should conduct an investigation ofthe relevant facts in order to determine if you need to take corrective/remedial
actions. An early fact assessment also willbetter prepare you to address any futurequestions regarding the investigation.
z Review Insurance Policies Respondingto a DOJ subpoena or investigation canbe quite expensive and disruptive. Thecompany should have counsel review itsinsurance policies to determine whetherthe company has coverage for legalexpenses (or any settlement payment).
z Determine If There Are ParallelProceedings Physicians and healthcarecompanies should remain aware of thepotential risk of “parallel proceedings” –i.e., simultaneous criminal, civil, and/oradministrative investigations. You wantto avoid the mistake of realizing too latethat an investigation is proceeding onmore than one track.
z Evaluate Your Potential ExposureFCA contains significant penaltyprovisions. The government is entitled to three times the amount of its loss.Also, it may be entitled to civil penaltiesof $5,500-$11,000 for each false claimsubmitted and/or false document used toget a false claim approved for payment.
z Remember OIG’s Role. If DOJ agrees to settle its FCA claims against you,remember that the OIG often plays a role. The OIG may require a CorporateIntegrity Agreement with you as part of any settlement of FCA claims. Thecurrent enforcement environment showsno signs of abating, so it is critical to knowwhat to do if you receive a DOJ subpoena.Ilana Subar, a partner at Whiteford, Taylor & Preston, LLP, has represented healthcare
providers facing government investigations.
She can be reached at [email protected]
T
28 | CHESPHYSICIAN.COM
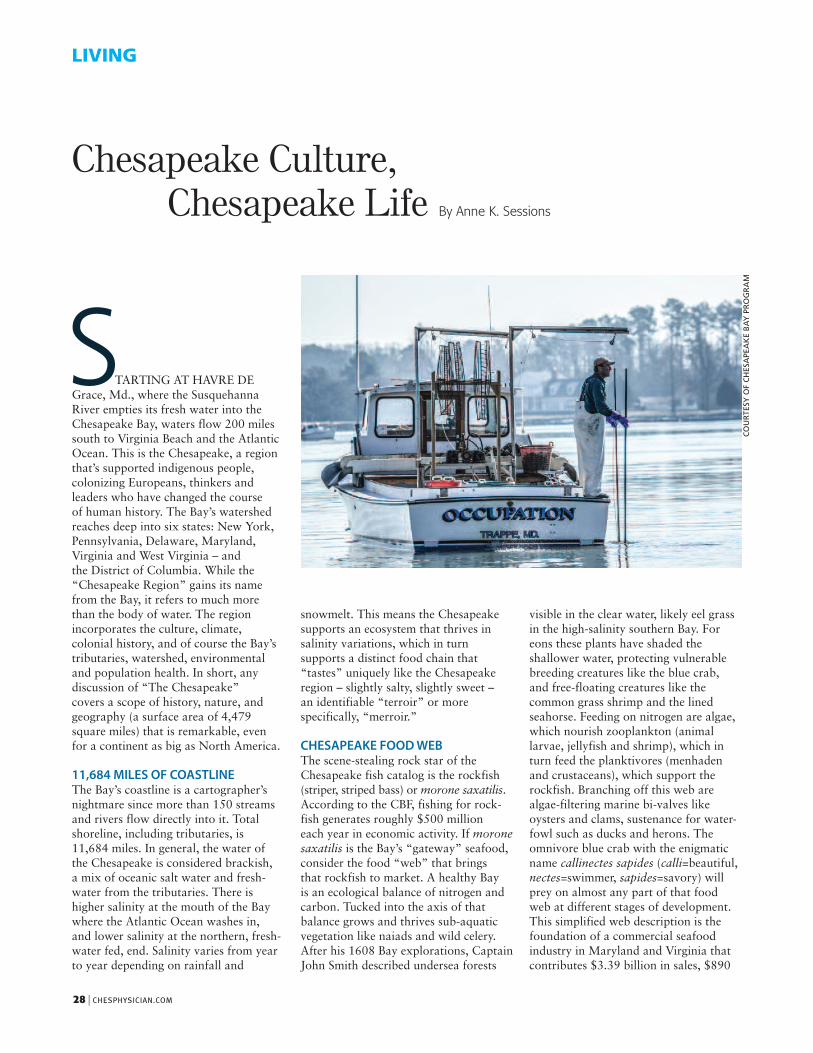
TARTING AT HAVRE DEGrace, Md., where the SusquehannaRiver empties its fresh water into theChesapeake Bay, waters flow 200 milessouth to Virginia Beach and the AtlanticOcean. This is the Chesapeake, a regionthat’s supported indigenous people,colonizing Europeans, thinkers andleaders who have changed the course of human history. The Bay’s watershedreaches deep into six states: New York,Pennsylvania, Delaware, Maryland,Virginia and West Virginia – and the District of Columbia. While the“Chesapeake Region” gains its namefrom the Bay, it refers to much morethan the body of water. The regionincorporates the culture, climate,colonial history, and of course the Bay’stributaries, watershed, environmentaland population health. In short, anydiscussion of “The Chesapeake” covers a scope of history, nature, andgeography (a surface area of 4,479square miles) that is remarkable, evenfor a continent as big as North America.
11,684 MILES OF COASTLINEThe Bay’s coastline is a cartographer’snightmare since more than 150 streamsand rivers flow directly into it. Totalshoreline, including tributaries, is 11,684 miles. In general, the water of the Chesapeake is considered brackish, a mix of oceanic salt water and fresh-water from the tributaries. There ishigher salinity at the mouth of the Baywhere the Atlantic Ocean washes in, and lower salinity at the northern, fresh-water fed, end. Salinity varies from yearto year depending on rainfall and
LIVING
Chesapeake Culture, Chesapeake Life
S
snowmelt. This means the Chesapeakesupports an ecosystem that thrives insalinity variations, which in turn supports a distinct food chain that“tastes” uniquely like the Chesapeake region – slightly salty, slightly sweet – an identifiable “terroir” or more specifically, “merroir.”
CHESAPEAKE FOOD WEBThe scene-stealing rock star of theChesapeake fish catalog is the rockfish(striper, striped bass) or morone saxatilis.According to the CBF, fishing for rock-fish generates roughly $500 million each year in economic activity. If moronesaxatilis is the Bay’s “gateway” seafood,consider the food “web” that brings that rockfish to market. A healthy Bay is an ecological balance of nitrogen andcarbon. Tucked into the axis of that balance grows and thrives sub-aquaticvegetation like naiads and wild celery.After his 1608 Bay explorations, CaptainJohn Smith described undersea forests
visible in the clear water, likely eel grassin the high-salinity southern Bay. Foreons these plants have shaded the shallower water, protecting vulnerablebreeding creatures like the blue crab, and free-floating creatures like the common grass shrimp and the lined seahorse. Feeding on nitrogen are algae,which nourish zooplankton (animal larvae, jellyfish and shrimp), which inturn feed the planktivores (menhadenand crustaceans), which support therockfish. Branching off this web arealgae-filtering marine bi-valves like oysters and clams, sustenance for water-fowl such as ducks and herons. The omnivore blue crab with the enigmaticname callinectes sapides (calli=beautiful,nectes=swimmer, sapides=savory) willprey on almost any part of that foodweb at different stages of development.This simplified web description is thefoundation of a commercial seafood industry in Maryland and Virginia thatcontributes $3.39 billion in sales, $890
COURTESY OF CHESAPEAKE BAY PROGRAM
By Anne K. Sessions

JANUARY/FEBRUARY 2015 | 29
million in income, and almost 34,000jobs to the local economy, according tothe 2009 Fisheries Economics of the U.S.report by the National Oceanic and Atmospheric Administration (NOAA).
Beth McGee, senior water qualityscientist with the Chesapeake BayFoundation states, “The more people weengage in the Bay, who come to love theBay, the more they’re going to supportthe Bay and restoration efforts.Chesapeake Bay Foundation (CBF) has award-winning education programsto get kids to know life on the water,exactly for that reason.”
BAY HEALTH - PUBLIC HEALTH It would be folly to think that the healthof a population who reside within the64,000 square miles of the watershed isnot in a few ways linked to the Bay. InMay 2004 Johns Hopkins BloombergSchool of Public Health launched theChesapeake Bay Health Indicators Project, “to preserve and improve boththe human health and the ecologicalhealth of populations living in andaround the Chesapeake Bay watershedthrough improved recognition of thelinkage between the quality of the environment and the protection of public health.” The landmark 1983Chesapeake Bay Agreement was the first codified effort to monitor the ecological status of the Bay and developscience-based policy to protect theecosystem. The JHSPH project sought to mirror those efforts by measuringrisks to the human population within the Chesapeake’s ecosystem. Hopkins’researchers created a matrix for trackingthe effect on human health of Bay degradation, looking at three indicators:
drinking water protection; microbialrisks in surface waters; and toxic pollutants. Those Environmental PublicHealth Indicators (EPHI), were selectedbecause they are commonly monitoredand can be used to measure complex environment/health relationships.
McGee says, “People can see theexplicit connections between their healthand the health of the Bay: if the water’s not safe for swimming, or there arewater-born illnesses, or algae blooms.”
PROTECTING THE BAYThe 1983 Chesapeake Bay Agreementcodified efforts to protect the health of the Chesapeake Bay, creating an Executive Council with the governors of the six watershed states and the District of Columbia, and the chair of the Chesapeake Bay Commission. The 2009 White House signing of Executive Order 13508 established a Federal Leadership Committee to oversee activities by agencies involved in Bay restoration. The committee ischaired by a representative from the Environmental Protection Agency, andincludes senior representatives from the Department of Agriculture, includingthe Natural Resources ConservationService and the Forest Service. Also onboard are the Departments of Commerce(which includes NOAA), Defense andHomeland Security. Additionally there is the Department of the Interior – bringing with it the United States Geological Service, National Park Service and Fish and Wildlife Service.
Beyond these federal efforts are thenonprofit organizations so familiar inthe Chesapeake region. The granddaddyof them all is the Chesapeake Bay
Foundation, actively involved at theExecutive-Council level as part of theIndependent Evaluator team. Also inthese leadership groups are Alliance for the Chesapeake Bay, county and city governments, water control boardsand universities. These are the groupsthat reach into local communities to help support riverkeeper programs,stream restoration and water analysis.There are now less than six degrees ofseparation between the White House andthe spats (juvenile oysters) elementarychildren nurture off docks duringenvironmental science field trips.
At the federal, state and local level it’srecognized that the conditions of theChesapeake Bay directly affect theconditions of a significant population –be it a mater of clean water, commerceor national security. Jeff Corbin of theEPA states, “There are nearly 18 millionpeople in the Chesapeake Bay watershed,and each one of us has an impact on theBay ecosystem.”
SAVE THE DATEBay Fundraisers and CelebrationsJanuary 29-February 1, 2015 BaltimoreHarbor – Baltimore Boat ShowApril 19, 2015 Leonardtown, Md. – Earth Day on the SquareMay 2, 2015 Chincoteague Island, Va. – Annual Chincoteague Seafood FestivalSeptember 19-20, 2015 Gloucester, Va.– Bluegrass by the Bay FestivalOctober 10, 2015 Chincoteague Island,Va. – Annual Chincoteague island Oyster FestivalOctober 17, 2015 Virginia Beach, Va. –First Landing Fall Festival
COURTESY OF CHESAPEAKE BAY PROGRAM (2)
30 | CHESPHYSICIAN.COM
LIVING
Seventeen million people live, work and play in the Chesapeake Bay watershed. Home to 3,600 species of plants and animals,
the Chesapeake is more than just “the Bay,” it’s considered a national treasure.
COURTESY OF CHESAPEAKE BAY PROGRAM


Call today to make a referral:8 6 6 - 9 1 6 - 9 2 0 2
Pelvic Pain C E N T E R F O R
o f V a s c u l a r O r i g i n
I S Y O U R PAT I E N T F R U S T R AT E D W I T H
Chronic Pelvic Pain?
Pelvic Congestion Syndrome (PCS) is a condition which is associated with varicose veins in the pelvic area, lower abdomen and thighs.
Often accompanied by chronic pelvic pain, it is estimated that this condition affects 15% of women between the ages of 20-50.
outpatient-based endovascular techniques.
IMMEDIATE APPOINTMENTS AVAILABLEAnnapolis | Glen Burnie | Greenbelt | Prince Frederick | Silver Spring
Call today to make a referral:8 6 6 - 9 1 6 - 9 2 0 2
www.StopPelvicPain.com
C E N T E R F O R VA S C U L A R M E D I C I N E I S A N AT I O N A L L E A D E R I N T H E T R E AT M E N T O F P C S
3:18 PM