chesapeake physician magazine may/june 2016 issue
DESCRIPTION
Women Physician's Leading the Way, Women's Health Detecting Elusive Diseases, Optimizing for an Independent PracticeTRANSCRIPT

chesphysician.comVOLUME 6 ISSUE 3 MAY/JUNE 2016
WOMEN’S HEALTHDETECTING ELUSIVE DISEASESOPTIMIZING FOR ANINDEPENDENTPRACTICE
5thANNIVERSARYISSUE
WOMEN PHYSICIANS EXCEPTIONAL IN THEIR FIELDS
Leading the Way
This team makes this problem go away.
Period. No hospital. No stitches. No downtime.
Connecticut, Maryland, Michigan, New Jersey, New York, Pennsylvania, Virginia, Washington DC (800) FIX-LEGS / (800) 349-5347 / www.centerforvein.com
Center for Vein Restoration is nationally recognized as the leader in the treatment of vein disease and varicose veins. Our physicians and clinical teams
are dedicated to relieving leg pain, treating the vascular cause of severe leg wounds, and eliminating unsightly veins. And with nearly all procedures covered
by insurance, we offer more treatment options than most other vein clinics.
Khanh Q. Nguyen, DO, RPVI Corporate Medical Officer
Zayed Meadows Director of Vascular Technicians
Eddie Fernandez, MD

MAY / JUNE 2016 l 3
CONTENTS
12 Women Physicians Leading the WayThis year’s group of exceptional physician leaders includes the president of the Medical Society of the District of Columbia (MSDC), the founding director of the Rodham Institute, and the critical care medical director for a major hospital system.
18Often-Elusive Diseases: Chronic Fatigue Syndrome and EndometriosisOften considered in the past to be psychosomatic conditions, the medical profession is now getting a better handle on chronic fatigue and pelvic pain.
22Complex Conditions in ChildrenRising rates of children with ADHD and other complex conditions are challenging physicians who care for children to raise the bar in their management practices. Area experts offer their advice.
F E A T U R E S D E P A R T M E N T S
6 CASESUndescended Testes: Less Imaging and Early Referral Reduces Cost, Risk and Other Problems
8 SOLUTIONSSelling a Medical Practice
20 COMPLIANCEMedicare Enrollment– Would Your Practice Survive Screening?
26 HEALTHCARE ITTips for Remaining Independent:Optimizing for an Independent Practice
30 OUR BAY
ON THE COVER: Jamie Barnes, DO, medical director and chief of Critical Care at LifeBridge Health.

4 l CHESPHYSICIAN.COM
Jacquie Cohen RothFounder/Publisher/Executive [email protected] @chesphysician
elcome to the fifth anniversary issue of Chesapeake Physician! Many of you have been loyal readers and advocates for this publication, produced in print and digitally, since our launch in May 2011 as Maryland Physician Magazine – Your practice. Your life. When the Affordable Care Act (ACA) became law in 2010, I saw an opportunity in the local healthcare marketplace to build a network of physicians and healthcare stakeholders with content focused on helping providers optimize the quality and efficiency of their patient care and
practice operations. With collaboration from my team, our advisory board and all of the many healthcare experts we’ve interviewed or who have contributed to Chesapeake Physician over the years, we’ve built it.
Our network now extends beyond Maryland to include the District of Columbia and Northern Virginia. Our mission statement continues to guide our content as we collaborate with the region’s leading clinical providers and practice management experts. The May/June issue is my favorite issue each year, not only because it celebrates another year of publication growth, but also because I am truly inspired by our annual interviews with exceptional women in healthcare. This year’s group does not disappoint. Each female physician leader shares the passion that led her to care for patients and to advance the medical profession, even to go as far as re-designing the way care is delivered (p. 12).
With the goal of reducing healthcare costs, the ACA has transferred more financial risk to providers, with incentives shifting from from volume-based to value-based. Providers are increasingly incentivized for better safety, outcomes, efficiency, and patient experience. Our Healthcare IT feature focuses on various approaches independent physicians can take to optimize their practice operations, including improving technology, staffing, purchasing and marketing, or joining a Clinically Integrated Network (CIN) (p. 26).
Each May/June, we also focus on women’s (p. 18) and children’s health (p. 22). Our clinical experts discuss how to better diagnose two often-elusive diseases that affect women – endometriosis and chronic fatigue syndrome. Too often, these diagnoses are inaccurate, leading to suboptimal treatment and referral. Our pediatric experts focus on better serving the needs of children with complex medical conditions, which have become increasingly common as more premature infants, and those with complex disorders, survive into childhood.
We’ve packed lots of additional advice from peers and consultants in the region into this issue, from tips for selling a practice to avoiding Medicare revocation of your billing privileges. And if you’re traveling this summer, you can always visit us online at chesphysician.com.
To Life!
PUBLISHER’S NOTE
JACQUIE COHEN ROTHFOUNDER/PUBLISHER/EXEUTIVE EDITOR
LINDA HARDER, MANAGING [email protected]
OPERATIONS MANAGER Stefanie Jenkins
MANAGERSOCIAL& DIGITAL MEDIA
Jackie [email protected]
COPY EDITOREllen Kinsella
CREATIVE DIRECTORSusan Smerker
PHOTOGRAPHYTracey Brown, Papercamera
Sharon R. BroomallKevin Parks
Chesapeake Physician – Your practice. Your life.™ is pub-lished bimonthly by Mojo Media, LLC, a certified Minority Business Enterprise (MBE).
Mojo Media, LLC1332 Cape St. Claire Rd. #372Annapolis, MD 21409443.837.6948mojomedia.biz
Subscription Information: Chesapeake Physician is mailed free to licensed and practicing physicians and a select group of healthcare executives and stakeholders throughout Maryland, Northern Virginia and Wash-ington, DC. Subscriptions are available for the annual cost of $52. To be added to the circulation list, call 443.837.6948.
Reprints: Reproduction of any content is strictly prohib-ited and protected by copyright laws. To order reprints of articles or back issues, please call 443.837.6948 or email [email protected].
Chesapeake Physician – Your practice. Your life.™ Advisory Board: An advisory board comprised of medical practitioners and business leaders in diverse practice, business and geo-graphic scopes provides editorial counsel to Chesapeake Physician. Advisory Board members include:
RANDY M. BECKER, MD Advanced RadiologyHARRY BRANDT, MD Sheppard Pratt Health SystemsPATRICIA CZAPP, MD Anne Arundel Medical Center HOLLY DAHLMAN, MD Green Spring Internal Medicine, LLCSTACY D. FISHER, MD University of MD Medical Center MICHAEL FREEDMAN, MD Evolve Medical Clinics JENNIFER MCQUADE, MD Virginia Hospital Center Physician GroupGENE RANSOM, JD, CEO Maryland Medical Society (MedChi) CHRISTOPHER L. RUNZ, DO Shore Health Comprehensive Urology VINAY SATWAH, FACOI Center for Vascular Medicine THU TRAN, MD, FACOG Capital Women’s Care
Although every precaution is taken to ensure accuracy of published materials, Chesapeake Physician and Mojo Media, LLC, cannot be held responsible for opinions expressed or facts supplied by authors and resources.
Printed on FSC certified, 100% PCW, chlorine-free paper
W
DISCUSSION: Undescended testicles, cryptorchidism, occurs in 2-5% of term infants and up to 30% of premature males. During the first three to five months postnatally, testicular descent will be completed in the majority of infants, mediated by a physiologic surge in serum testosterone levels (mini-puberty), leaving 1% still having cryptorchidism. For these males, surgery is recommended by one year of age to hopefully maximize the long-term development of these testicles and provide a scrotal position for consistent examination given a lifelong need to monitor for testicular cancer.
Current literature suggests an overall five-fold increase in testicular cancer risk from an undescended testis, and a clear
reduction in the relative risk for patients who undergo orchidopexy before puberty as compared to those males whose surgery is not performed until after the onset of puberty and beyond. Fertility in a male with a history of unilateral undescended testicle and a normally developed and positioned contralateral testis appears to be equivalent to that of the general population by current studies and does not seem to be impacted by age of orchidopexy.
There is often an inordinate and undesirable delay in diagnosis and treatment of the undescended testis. The average age of orchidopexy diagnosis in the U.S. and internationally is nearly seven years old. Two factors likely contribute to this dismal performance
of our healthcare system. First, there is a delay in diagnosing the
undescended testis and distinguishing this from retractile testis. Testicles that are not descended after the infant is six months old should be assessed by a specialist. Delaying referral in the hopes that descent will occur with growth and development, or to distinguish the retractile from the undescended testicle, may miss the best therapeutic window for developmental and surgical success. Significantly retractile testicles diagnosed at this age can be monitored to assure no “ascent” with linear growth, that appears to occur in a particular “tethered” subset of these testicles, occurs. Cases like this occur in approximately 6-10% of all cases of retractile testes.
Second, the healthcare network for children has become fragmented. For many of our referred patients there is no consistent primary care provider who examines the infant and child periodically. Instead, patients seek care in either urgent care clinics unaffiliated with their pediatric practice, or alternate providers within their practice for whom only an electronic record is available to convey ongoing concern with a genital exam.
Finally, the utility of ultrasound examination prior to specialty examination for questions of testicular descent is negligible at best. Ultrasound rarely offers information not attained upon examination and often leads to misinforming the family about the child’s diagnosis and care. CP
Agarwal, Piyush, et al. J of Urology 2006
Kanaroglou, Niki, MD, et al. Pediatrics 2015
Pettersson, Andreas, MD, et al. New England J of Medicine 2007
Stec, Andrew, et al. J of Urology 2007
Tasian, Gregory, et al. J of Urology 2011
Robert A. Mevorach, MD, FSPU, FAAP, is the director of Pediatric Urology at Chesapeake Urology. He can be reached at [email protected].
6 l CHESPHYSICIAN.COM
CASEn
In this case a 12-year-old boy received a new diagnosis of a right non-palpable undescended testicle, which was discovered on a routine sports physical at an urgent care facility. He had a history of normal physical examinations prior to this, was a full-term birth, had no symptomatic complaints, and reported no trauma. Review of his infant records revealed a question of hydroceles bilaterally up until 10 months old, a note of retractile testis on the right until six years, and only normal exams noted thereafter. After a confirmatory physical examination by his PCP, and prior to referral to pediatric urology evaluation, he was sent for diagnostic ultrasound imaging.
On arrival to pediatric urology he was in no distress, was 25th percentile for weight, and 70th percentile for height. In the past year he reported a four-inch growth spurt, and was otherwise healthy with no surgical history except circumcision at three years of age by an adult provider. A physical examination revealed a normally descended left testis and an ectopically descended right testis to the area of the pubic tubercle, equal in size and consistency to the left with a small right hemiscrotum.
The patient underwent an elective and uneventful operative orchidopexy and at his one-year follow-up has maintained relative size and dependent position for both testes. He has been instructed in testicular self-examination and will have routine primary care follow-up.
CASES
Undescended Testes: Less Imaging and Early Referral Reduces Cost, Risk and Other Problems BY ROBERT A. MEVORACH, MD, FSPU, FAAP

Enjoy an evening on the beach with cool drinks, delicious food, jammin’ live music, and dancing—all to benefit the Chesapeake Bay Foundation.
Tickets: cbf.org/BITS • 410/268-8816
Proudly Sponsors
FOUNDING SPONSOR PRESENTING SPONSORTITLE SPONSOR
Saturday, June 11, 20165:00 p.m. to 10:30 p.m.
SOLUTIONS
Selling a Medical PracticeBY BRIAN MACMILLAN
T
8 l CHESPHYSICIAN.COM
he majority of medical practice owners do not know how to sell their practices, and many are not aware that selling to a third party
is even an option. As a result, many roll their practices into a hospital system and begin receiving a salary as an employee, sell their practices for less than they should, or simply close their doors when they are ready to retire. But with some guidance, physicians who are selling their practices can achieve better results for both themselves and their patients.
Timing Is Everything!The medical practice sales climate
is currently excellent in the Baltimore-Washington metropolitan area. Physicians who own their practices and are considering retirement in the near future might want to think about selling their medical practices while conditions are favorable.
This is a great place to live; many doctors across the country recognize this and are interested in owning a medical practice in our region. We have encountered numerous doctors who went to one of the many
excellent medical schools in this area (Johns Hopkins University, University of Maryland, etc.), left the area to practice medicine, and are now interested in returning to the Baltimore-Washington area. Regardless of where they studied medicine, most doctors want to live and practice in an economically affluent area, and Maryland, DC and Northern Virginia are home to many such areas. In addition, our region already has one of the highest physician-to-patient ratios, so there are already many local physicians who might be in the market to purchase their own practices.

MAY / JUNE 2016 l 9
Brian MacMillan is managing director, Mergers & Acquisitions, at Baltimore-Washington Financial Advisors. He can be reached at [email protected].
AMP Systems, LLC specializes inNetwork Support and Technology
Services for medical practices.Electronic Health Records SystemIntegration, On-Site and Remote
Network Support, NetworkMMonitoring and Security, Computer
Virtualization, Server Hosting,Voice over IP Services, and
more. Call today and see whatwe can do for your practice.
410.934.0000CALL TODAY
Plan Ahead for the Best Price and TermsPhysicians who are thinking about
selling their practices should start the sales process a few years before they plan to retire and before they begin to scale back their hours. The process of selling a practice can take six to nine months, on average, and the buyer will want the seller or sellers to stay on for some time to provide a smooth transition for the patients. This transition period could take anywhere from six months to several years.
If a physician is interested in cutting back his or her hours, selling the practice before doing so may be the best option. Once the physician cuts office hours, the sale price for the practice will generally drop because the corresponding revenue generated by the practice decreases. If the physician maintains normal hours until the sale, he or she can obtain a higher sale price and then establish a flexible work schedule (i.e., work fewer hours) as an employee or
contractor for the new owner. By starting the sale process earlier,
while they have more flexibility, physicians who own medical practices can avoid an emergency or “fire” sale, which usually means a reduced sale price and less favorable terms. There are specialty financing options currently available to physicians looking to buy medical practices, making it easier for them to complete the purchase. Lenders can finance up to 100% of the sale price and can provide terms up to 15 years, giving buyers more flexibility.
Work With a Mergers and Acquisitions Advisor for the Best Result
The process of selling a practice can be complicated. Many physicians attempt to sell their practices on their own, and doing so ultimately takes away from the service they provide to their patients. Another pitfall physicians face is hiring a younger physician as an employee in hopes that
the physician will buy the practice in a few years. More often than not, the younger physician does not end up buying the practice or is not willing to pay the owner a reasonable amount for it. This can lead to years wasted. In the end, the owner would need to start the sale process over from scratch.
Hiring an experienced advisor who will sit down with you to understand your goals related to the sale of your practice allows you to continue to focus on running and growing your practice. The advisor can develop confidential marketing materials to position the practice properly in the market, obtain multiple offers for the practice and ultimately help complete the sale. CP

10 l CHESPHYSICIAN.COM
Mobile Apps Make Sharing Data and Images Easy and Secure
BY LINDA HARDER PHOTOGRAPHY BY TRACEY BROWN
Jennifer McQuade, MD, FACS, FASCRS, colorectal surgeon at Virginia Hospital Center Physician Group
Profile / SPONSORED CONTENT /
ROOTED IN DATA AND ARCHIVING
Olah Healthcare, a leading vendor in helping providers retire legacy imaging systems, got its start in the early 2000s as a result of CEO Brian Olah’s experience as a data warehousing consultant to a number of hospitals. At first, the company was solely involved in archiving imaging records. After getting requests from several major health systems, Olah began converting fetal tracings to reduce the costs of this extremely expensive service.
In early 2015, the company received an interesting request that was close to home, providing a variety of clinical imaging services. “My wife’s OB/GYN practice wanted us to automate the capture and storage of their ultrasound images. We built that automated solution for their new Greenway EMR installation.”
While implementing that solution, Olah made a serendipitous observation that led to the company’s newer services. Olah recalls, “In June 2015, I saw a dad trying to take a smartphone photo of his baby’s ultrasound and it dawned on me that there was a tremendous unmet need among expectant parents. We immediately started creating a mobile app to meet this need.”
HIR HEALTHCARE
A Mobile App for Expecting Parents
Olah Healthcare released HIR Healthcare in October 2015. The company’s most consumer-facing product, HIR allows hospitals, clinics and practices to share provider-approved images with patients on their smartphones, regardless of what EMR or imaging equipment they have.
Olah remarks, “Expectant mothers today have grown up in a world with Facebook and other social media as part of their lives. They want their baby’s ultrasound on their smartphone. We provide not only images but also video and sound for enabled ultrasound devices, so expectant parents can see their baby move as well as hear the heartbeat on their phone. The bonding with their infant is tremendous.”
Madihuri Kurup, MD, an obstetrician, says, “HIR has also definitely improved the patient’s experience. By the time I finish my ultrasound, the patient already has it in her device, and she can share it immediately with friends and family. And we’ve saved about $1,500 per month in paper costs.”
Today, patients demand
that providers supply
their images in a less
costly, cumbersome and
antiquated way than
burning CDs or DVDs.
Fortunately for both
patients and physicians,
companies like Olah
Healthcare in Columbus,
Oh., have risen to the
challenge.
MAY / JUNE 2016 l 11
Mobile Apps Make Sharing Data and Images Easy and Secure“Patients love getting the images right to their smartphone,”
Danielle Sartin, RDMS, says. “The images are as sharp as they look on my ultrasound screen.”
SAVING MONEY AND TIME
HIR further benefits physician practices that provide imaging ancillary services by improving their workflow and allowing them to conduct more imaging procedures with the same resources. “Our app improves provider workflow, with facilities able to perform two to three additional ultrasounds per day, which can increase revenues by $4,000 per month,” states Olah. “There’s no additional operating expenses, no device to buy and no cost to the patient.”
Practices also save on thermal paper expenses and cd burning, while increasing patient satisfaction and brand awareness.
GOOD STEWARDS OF YOUR DATA
Of paramount importance to physicians is ensuring that the data is secure. “If a practice wants to share images, they buy our secure interface and we store images in our secure cloud for patients,” states Olah. “There’s no patient data or PHI stored on the app itself, so if a patient loses their phone they don’t lose their PHI. Patients can share images socially with friends and family on Facebook if they want, or securely share with a medical professional.”
Olah explains, “A major concern among obstetricians is the legal malpractice. To address this up front, with HIR, providers control what they share – only the images they approve. We provide the comfort, confidence, attention to detail, and deep understanding of the clinical workflow that physicians want. They can trust us to be stewards of sensitive clinical data.”
EASY TO LAUNCH
Launching HIR is quick and straightforward. Olah explains, “With HIR Healthcare, there’s no software to install. If the obstetrician has an ultrasound machine and a network, we will help guide them through securely connecting to our secure cloud on the internet in a matter of a few hours – remotely.”
CARDIAC IMAGING APP NOW AVAILABLE
Using HIR for obstetrics imaging has been so successful that Olah and his colleagues have now created a cardiac app for patients with heart problems. Patients can get and keep a copy of their EKGs (echocardiograms) on their phone, so that, for example, if they’re on vacation, and they have to visit a hospital emergency department, they can demonstrate their existing heart murmur or an irregular heartbeat and get shorter, more appropriate treatment. “It can avoid a potential three-day
stay and be more cost effective,” Olah explains.He adds, “Our app puts the control in the patient’s hands so
they can manage their care. When patients control their own information, obstacles such as medical records crossing state lines are removed.”
CARE COORDINATION FOR THE WHOLE FAMILY
While patient portals are convenient, patients and their families typically have to log into multiple different portals – one for each physician practice and often one for each member of the family – to access their healthcare information.
Olah Healthcare designed the HIR app to be a care coordination platform for the entire family, instead of making patients have to use a separate portal for each of their doctors.
Olah states, “Parents can even add their child to HIR, recording pediatric visits, immunization records and other health data – all in one place. Closing the loop, we tapped into a secure messaging platform overseen by DirectTrust so that every user can securely message their physician. This allows the physicians to securely communicate and retain conversations within their existing medical record system. We provide free direct message functionality to every patient and physician.”
A patient can, for example, ask the physician about a heartburn drug they’re taking, and the physician can respond back with a change in dose or medication – when it’s convenient for them. All of this occurs within a secure and documented environment.
HIR SUCCESS STORY
The experience of a first-time mom-to-be is a great example of the impact HIR has had. While having her first ultrasound, the mom was a little down because her husband was deployed to the Middle East and unable to share in this exciting moment. She was thrilled to learn that she could share the images via HIR.
The result: The dad-to-be, deployed on the other side of the world, saw the ultrasound images at the same time his wife did. CP
Advantages of HIR Healthcaren Meet HIPAA, Omnibus, HITECH security rules
n Reduce printing and CD costs
n Eliminate mislabeling and handling
n Improve patient satisfaction
n Increase imaging with better workflow
Contact Brian Olah at 614.245.0656 x1002 or visit Olah-healthcare.com
12 l CHESPHYSICIAN.COM
LEADING THE WAY TO HEALTH EQUITYJehan (Gigi) El-Bayoumi, MD, FACP, founding director of the Rodham Institute at
George Washington (GW) School of Medicine & Health Sciences, and a professor of Medicine, says, “I’ve always been very lucky. The reason I became a doctor was to make a difference above and beyond caring for individual patients. It’s nice that what I wanted to do – work in an urban and underserved area – aligned with what I’m doing now.”
Raised in East Lansing by two professors at Michigan State University, Dr. El-Bayoumi decided on medical school as a junior in college. In 1985 she moved to GW for her internship and residency. She recalls, “During my residency, it became clear that the chasm between the haves and have-nots was huge. There was such a disconnect between the VIPs and the homeless.”
After completing her training, she joined the Division of General Internal Medicine at GW, where her interest in developing other teachers and leaders drove her to serve first as clerkship director, and then for the next 15 years as the Internal Medicine Residency program director. “I oversaw 108 residents in four hospitals,” she remembers. “I tried to weave connections to the community during that time.”
Dr. El-Bayoumi has lectured and taught in the School of Medicine and Health Sciences (SMHS), the GW SMHS residency program and the GW Milken Institute School of Public Health, as well as in the general community, about topics such as women and minority health. She is currently a board member for Whitman Walker Health’s Community Health Department, which serves greater Washington’s diverse urban community, including those
Women PhysiciansLeading theWay
THIS YEAR’S GROUP OF
EXCEPTIONAL PHYSICIAN LEADERS
INCLUDES THE PRESIDENT OF
THE MEDICAL SOCIETY OF THE
DISTRICT OF COLUMBIA (MSDC),
THE FOUNDING DIRECTOR OF THE
RODHAM INSTITUTE, AND
THE CRITICAL CARE MEDICAL
DIRECTOR FOR A MAJOR
HOSPITAL SYSTEM. BY LINDA HARDER PHOTOGRAPHY BY TRACEY BROWN

MAY / JUNE 2016 l 13
14 l CHESPHYSICIAN.COM
who face barriers to accessing care, such as members of the LGBTQ community, and those needing and receiving HIV care. She also serves on the Arts for The Aging board, which uses art to engage members of the elderly community.
“I started slow, learning about the community and D.C.,” she notes. “I’ve learned how to talk to people about HIV testing and what the barriers are for the gay community.”
KEEP ‘TOUCH POINTS’ TO YOUR PASSIONDr. El-Bayoumi gradually has become more directly
involved with promoting health equity. “My advice to other physicians is that you don’t have to go from zero to 60. Have touch points to connect you with your passions and take the pressure off yourself. It’s taken me time to get where I am.”
She also recommends, “You don’t have to be all things to all people, especially if you have a family. Even taking time to feed your soul and combat burnout once a month or once a year can be sufficient. Don’t see it as an extra that you have to feel guilty about – it can help you to be more present in your clinical work. Give yourself a break. Be self-aware about your passion and keep those soft touches with it throughout your career, so that if you want to pursue them full time at some later point, you can.”
FOUNDING THE RODHAM INSTITUTEOne of Dr. El-Bayoumi’s patients was Dorothy Rodham,
Hillary Rodham Clinton’s mother, with whom she became close friends. “She had a difficult childhood. When she was very young, she was sent to live with her grandparents, who kicked her out at age 14. She never went to college, but she audited courses when President Bill Clinton was governor. She was a lifelong learner and a voracious reader. I do believe education is a way to transcend your environment.
I took care of Dorothy Rodham until she passed away in 1992. I was also a physician to Hillary, and we talked about founding the Institute. But, since I also was the physician for the Cheneys and the Rumsfelds, I have to serve both parties!” she jokes.
It wasn’t until age 53, after 15 years as program director, that Dr. El-Bayoumi left her secure position to found the Rodham Institute. “People didn’t want me to leave, but I was stubborn, and founding the Rodham Institute was my passion. We launched in October 2013. One person even told me it was a ‘bad mistake’ to leave, and asked what I would do
if it failed. Fortunately I didn’t let that comment stop me. My father always said it’s okay to take risks. I knew it was now or never – I didn’t want to be too close to retirement.”
Dr. El-Bayoumi held several informal meetings before bringing together 90 stakeholders from all over D.C. for their input on creating the Institute.
The Rodham Institute has three main goals: increasing the number of clinicians from minority backgrounds, giving students and residents first-hand experience serving vulnerable communities, and generating and disseminating best practices to eliminate health disparities.
Dr. El-Bayoumi says, “Our main mission is to establish relationships. I compare our process at the Institute to building a building – you don’t see anything happening for a long time, then suddenly the building goes up.”
RE-DESIGNING CRITICAL CAREWhere Dr. El-Bayoumi took slow steps to connect with
her passion, Jaime Barnes, DO, medical director and chief of Critical Care at LifeBridge Health in Baltimore, plunged full-speed ahead into hers.
“I never wanted to do anything but practice medicine,” she recollects. “When I was a small child, my dad was in podiatry school and we looked at medical textbook photos together. When I got to my medical rotations, critical care was the only specialty that truly resonated with me. From that day on, I knew I wanted to be an intensivist. I loved the fast, intense, exciting pace.
“I put everything I had into everything I did,” she continues. “People tell me that I always had my ‘pedal to the metal’ and that I could slow down, but I just can’t. And I never perceived being female to be a barrier. My mindset was that I could do anything I wanted. “
THE ROLE OF MENTORSLike many physician leaders, Dr. Barnes recalls that several
people were critical to her development. “I had three major mentors in my career – my dad, who became a beloved internist, said, ‘Remember that dead is forever.’ That left an impression on me that taking care of people was a big deal.”
She adds, “The second was a colleague who asked me to join her in my first year as an intensivist. I knew I could divulge any of my uncertainties and ask questions without feeling uncomfortable. The third was the regional medical
Be self-aware about your passion and keep those soft touches with it throughout your career… – JEHAN EL-BAYOUMI, MD, FACP

MAY / JUNE 2016 l 15
director of a company I worked for who taught me several necessary skills needed to set up my first new critical care program. The outcomes were amazing. I continued to advance this skill set in developing new critical care programs.”
DEVELOPING SKILLS, TAKING RISKSDr. Barnes notes that serving as medical director required
a number of skills that didn’t come naturally to her – interacting with administrators, completing performance
improvement projects, analyzing data, and collaborating with other departments. “We don’t learn that in our medical training,” she remarks.
“After eight years of serving in this role, I knew that if I were to jump to the next level, I had to move out on my own. When I found the position at LifeBridge Health, I had to leave my comfort zone without knowing the outcome. Fortunately it was a great decision.
“LifeBridge has been a unique blessing. In an era of instability, it’s very stable, with a progressive administration
Jehan El-Bayoumi, MD, FACP, founding director of the Rodham Institute at the George Washington School of Medicine & Health Sciences and professor of Medicine

16 l CHESPHYSICIAN.COM
and vision that aligns with physicians. Brian White, president of Northwest Hospital in Baltimore, has been a huge inspiration to me. His style of leadership and dynamic approach to healthcare is contagious.”
Dr. Barnes notes that the first step was building good relationships. “I’m only one piece of the puzzle. We needed a team with the same vision. We changed the culture and we measured that change with data. Standardizing one hospital’s critical care program was a challenge in itself, but it became more challenging when we decided to expand it to multiple intensive care units. In October 2014, we deployed the strategy across the whole system.”
HOW SHE RE-INVENTED THE ICUAs medical director, Dr. Barnes developed an intensivist-
led, standardized, multi-disciplinary team that committed to a new mission and vision. She also implemented system-wide, evidence-based guidelines, protocols and standardized order sets, and created collaborative relationships with the ED, acute and post-acute services. Her team consistently practiced in a patient/family-centered approach.
Dr. Barnes implemented a policy of taking borderline patients before they ‘crashed. ‘ The ICU team established
standardized bedside multidisciplinary daily rounds that included the family and a daily safety check list. They also established an ICU clinical practice standards workgroup, and collaboratives with ED and hospitalist personnel to evaluate and improve care.
Perhaps most importantly, Dr. Barnes created a ‘yes’ culture in which staff were encouraged to figure out how to solve issues that arose. She created a ‘horizontal’ team structure in which all members were equal partners. She defined roles and responsibilities in such a way that allowed for collegial flexibility, and also created iterative data-driven processes that evaluated current practice, implemented evidence-based protocols, evaluated the results, and modified them as needed.
The initiative resulted in caring for critically ill patients throughout the entire LifeBridge Health system that includes a fully integrated continuum of critical care across the system and community.
“Doctors want to do the right thing and believe we are doing the right thing, but unless we measure with data we don’t know if we are actually doing the right thing,” Dr. Barnes stresses. “If everyone uses best practices, there’s less variability and better outcomes.”
Carla Sandy, MD, FACOG, service chief, OB/GYN, Kaiser Permanente, and president, Medical Society of the District of Columbia

MAY / JUNE 2016 l 17
My advice to women physicians is to never skip opportunities just because you don’t have the experience. As women, we tend to question whether we’re qualified, whereas men tend to assume they are. – CARLA SANDY, MD, FACOG
Dr. Barnes has a 10-year-old daughter and seven-year-old twins, as well as three grown stepchildren. She confesses, “There were times in my life when my kids spent the majority of their days with their nanny. This was a sacrifice my entire family made. Presently, I can say it was worth it for all of us. I do look back on the earlier days and wonder how I did it, though!”
LEADING ON OBSTETRICS AND LEGISLATIVE ISSUESLike Dr. Barnes, Carla Sandy, MD, FACOG, service chief,
OB/GYN, Kaiser Permanente, and president, Medical Society of the District of Columbia (MSDC), grew up wanting to be a doctor. She recalls, “I had a great pediatrician as a child and I participated in summer programs while in college that exposed me to medicine. I thought I wanted to practice pediatrics, but midway through school, I realized that babies don’t talk to you and maybe that wasn’t for me after all!”
Fortunately she found she loved caring for women during her obstetrics rotation. “I could take care of them and still get to see my babies without having to be their doctor,” she laughs.
During her residency at Washington Hospital Center, Dr. Sandy had the opportunity to work with Mid-Atlantic Permanente Medical Group in Fairfax, Va., the physician-led practice group for Kaiser Permanente (KP). She explains, “Their model of care appealed to me because, even during my training, I saw how insurance barriers impacted patient care. I saw that the physicians working at KP didn’t have to cobble together care in the same way. It was the only place I wanted to work, and now I’ve been here 11 years.”
While she was always interested in leadership, Dr. Sandy’s first real opportunity to put that interest into practice came when she joined KP. “I was approached about becoming a module leader – someone who leads efforts on quality, service and efficiency initiatives for all the OB/GYNs at one office. I was hesitant, but decided to try it. It taught me a lot about building consensus and working with teams I didn’t control.”
LEADERSHIP SECRETS: LISTEN AND FOLLOW UPDr. Sandy credits much of her leadership success with
being good at listening and following up. “Take a few seconds to see if the other person is truly finished speaking before you jump in,” she advises. “You can learn what’s really bothering people. I also close the loop to make sure that a task has been completed.”
Dr. Sandy’s next leadership opportunity came in 2009. “We built our first ‘hub,’ a multispecialty center with 24/7 operations and over 20 specialties. I was recommended for the site’s lead role. I was nervous about taking on these responsibilities, but I went for it. I worked with all the departments in the building and brainstormed with physicians about how to meet our goals. After meeting with architects and negotiating vision versus reality, I’m now skilled at reading blueprints!”
After serving as site leader for five years, Dr. Sandy’s current leadership opportunity arose when the chief of Obstetrics and Gynecology stepped down. She applied and was offered the position. “Today, I oversee 60 OB/GYNs in nine locations throughout D.C. and Maryland. I drive a lot,” she observes wryly. Yet she also still sees patients and has been designated for excellence in minimally invasive gynecologic surgery.
“The Kaiser Permanente model has given me wonderful opportunities to develop both clinical and leadership skills. My advice to women physicians is to never skip opportunities just because you don’t have the experience. As women, we tend to question whether we’re qualified, whereas men tend to assume they are.”
PRESIDENT OF THE MEDICAL SOCIETY OF D.C. After serving on the board of MSDC for nearly four years,
Dr. Sandy added yet one more leadership position to her impressive resume by becoming its president in late 2015.
She states, “I feel strongly that we need organizations like this. It’s a great group. I’ve testified on a number of bills and am active in insurance issues. I found that this role takes different types of leadership skills. I can’t make demands as I would in a work situation – I have to do a lot more asking.
But doctors must become more involved in legislation,” she urges. “We’re so busy that we often let others who aren’t medically trained make our decisions for us. It’s no different from voicing a medical point of view so those blueprints I learned to read would become space that worked for clinicians. The legislative process affects our practice tremendously. Medical societies are a great place for doctors to start so that we, as physicians, can lead the way on solving healthcare challenges.” CP
Jehan (Gigi) El-Bayoumi, MD, FACP, founding director of the Rodham Institute at George Washington (GW) School of Medicine & Health Sciences, and professor of MedicineJaime Barnes, DO, medical director and chief of Critical Care at LifeBridge Health, BaltimoreCarla Sandy, MD, FACOG, service chief, OB/GYN, Kaiser Permanente and president, Medical Society of the District of Columbia
18 l CHESPHYSICIAN.COM
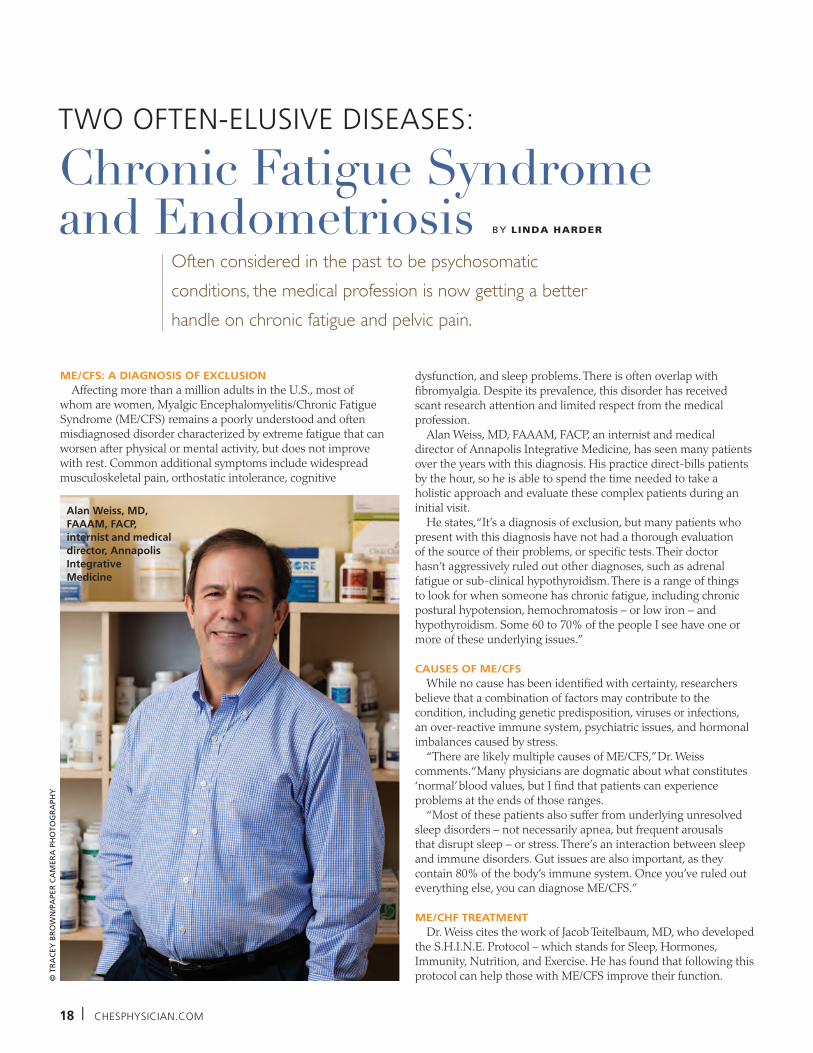
TWO OFTEN-ELUSIVE DISEASES:
ME/CFS: A DIAGNOSIS OF EXCLUSIONAffecting more than a million adults in the U.S., most of
whom are women, Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS) remains a poorly understood and often misdiagnosed disorder characterized by extreme fatigue that can worsen after physical or mental activity, but does not improve with rest. Common additional symptoms include widespread musculoskeletal pain, orthostatic intolerance, cognitive
Chronic Fatigue Syndrome and Endometriosis
© T
RA
CEY
BR
OW
N/P
APE
R C
AM
ERA
PH
OTO
GR
APH
Y
Often considered in the past to be psychosomatic conditions, the medical profession is now getting a better handle on chronic fatigue and pelvic pain.
dysfunction, and sleep problems. There is often overlap with fibromyalgia. Despite its prevalence, this disorder has received scant research attention and limited respect from the medical profession.
Alan Weiss, MD, FAAAM, FACP, an internist and medical director of Annapolis Integrative Medicine, has seen many patients over the years with this diagnosis. His practice direct-bills patients by the hour, so he is able to spend the time needed to take a holistic approach and evaluate these complex patients during an initial visit.
He states, “It’s a diagnosis of exclusion, but many patients who present with this diagnosis have not had a thorough evaluation of the source of their problems, or specific tests. Their doctor hasn’t aggressively ruled out other diagnoses, such as adrenal fatigue or sub-clinical hypothyroidism. There is a range of things to look for when someone has chronic fatigue, including chronic postural hypotension, hemochromatosis – or low iron – and hypothyroidism. Some 60 to 70% of the people I see have one or more of these underlying issues.”
CAUSES OF ME/CFSWhile no cause has been identified with certainty, researchers
believe that a combination of factors may contribute to the condition, including genetic predisposition, viruses or infections, an over-reactive immune system, psychiatric issues, and hormonal imbalances caused by stress.
“There are likely multiple causes of ME/CFS,” Dr. Weiss comments. “Many physicians are dogmatic about what constitutes ‘normal’ blood values, but I find that patients can experience problems at the ends of those ranges.
“Most of these patients also suffer from underlying unresolved sleep disorders – not necessarily apnea, but frequent arousals that disrupt sleep – or stress. There’s an interaction between sleep and immune disorders. Gut issues are also important, as they contain 80% of the body’s immune system. Once you’ve ruled out everything else, you can diagnose ME/CFS.”
ME/CHF TREATMENTDr. Weiss cites the work of Jacob Teitelbaum, MD, who developed
the S.H.I.N.E. Protocol – which stands for Sleep, Hormones, Immunity, Nutrition, and Exercise. He has found that following this protocol can help those with ME/CFS improve their function.
Alan Weiss, MD, FAAAM, FACP, internist and medical director, Annapolis Integrative Medicine
BY LINDA HARDER

MAY / JUNE 2016 l 19
“I support their adrenal function with optimal sleep and nutrition, recommending appropriate supplements that may include CoQ10 or D-ribose, and make sure they’re not on medications that adversely affect their blood pressure,” he explains.
While no one treatment approach works for all patients, Dr. Weiss has achieved improvement or even complete resolution in 80 to 90% of his patients by taking a holistic approach that includes lifestyle changes. “I optimize gut function, try thyroid hormones and discuss a possible course of antiviral medications. I also support them in getting on disability. They tend to tread water while applying for it because they don’t have an incentive to get better, but once it’s been granted, they start improving.
“I have patients read “The Relaxation Response” and “Why Zebras Don’t Have Ulcers.” Even those with classic CSF can make changes that allow their bodies to better deal with any viruses they may have,” Dr. Weiss remarks.
Follow-up with patients to ensure ongoing compliance is important. “I schedule a follow-up visit every few months, because if they resume their old lifestyle, they regress. They may be out of shape and have muscle atrophy due to deconditioning, so they may also need a gradual rehab program.”
Dr. Weiss reflects, “This disorder doesn’t lend itself to the medical model. I think that physicians tend to err on the side of thinking that if we can’t measure it, it doesn’t exist. And if we can’t diagnose and treat a patient, we feel impotent and blame the patient for that. I take the view that the person is truthful until proven otherwise.”
NARROW BAND IMAGING: SHINING A LIGHT ON ENDOMETRIOSIS
An estimated six million American women suffer from endometriosis, a chronic condition in which endometrial cells grow outside the uterus, causing pelvic pain before and after menstruation that can also lead to infertility.
Kevin Audlin, MD, gynecologist and co-director of The Endometriosis Center at Mercy Medical Center in Baltimore, says, “We don’t know the exact cause of endometriosis. Retrograde menstruation likely plays a role.”
It can be important to correctly diagnose and treat endometriosis, as treatments for the pelvic pain associated with this disease often lead to addiction. However, no simple diagnostic blood test exists.
Dr. Audlin explains, “Our goal is to catch it through their history. Endometriosis is a time-intensive diagnosis and many physicians don’t like to treat it. Sometimes physicians are guilty of not listening well enough or taking the appropriate first step of hormone therapy. Many patients who come in for a consultation have seen three or more gynecologists who have told them that their pain is normal, or in their heads. Only after diagnostic laparoscopy, do we prove otherwise.”
Using narrow-band imaging on the laparoscope, the light changes, making endometriosis stand out, and therefore much easier to detect. - KEVIN AUDLIN, MD
© K
EVIN
PA
RK
S
NBI ENHANCES DETECTIONA relatively new technique may improve the diagnosis of this
condition for these women. Narrow band imaging (NBI) is a high-resolution endoscopy that increases the visibility of blood vessels with a narrow spectrum of blue and green wavelengths.
Dr. Audlin states, “In our study of 167 patients, published in the Journal of Minimally Invasive Gynecology in July-August 2015, NBI had a sensitivity of 100% versus traditional white light of 79%. Using NBI, endometriosis tends to stand out as red patches, while normal vasculature appears green. Increased collection of vasculature tends to highlight a roadmap to the more difficult-to-identify endometriosis, which increases vascular recruitment. Increased detection and excision of lesions gives us a better chance to resolve pain.”
NBI was used initially to detect colorectal cancer in the early 2000s. “The approach is best for women with pain and symptoms of endometriosis who have minimal disease that is difficult to detect with traditional laparoscopy,” Dr. Audlin says.
“In 2008, we conducted a pilot study to determine if NBI could find endometriosis in patients where normal light failed to detect it. Otherwise, patients are likely to be inappropriately referred to a psychiatrist or gastroenterologist for follow-up. The condition is difficult to diagnose because we can’t see it well. We’ve been using this approach for almost eight years now and have shown that NBI improves our detection.”
He adds, “The Olympus laparoscope has a light filter on it to identify the vasculature, which is much more obvious under filtered light. If the facility has an Olympus Exera CV-190 system, you don’t have to switch cameras and there is no additional cost. I now use it on all my patients because many times I found additional pathology even after thinking I had identified it all.
“Under full-spectrum light, everything looks just as we would see it. Using narrow-band imaging on the laparoscope, the light changes, making endometriosis stand out and therefore much easier to detect,” Dr. Audlin says. CP
Alan Weiss, MD, FAAAM, FACP, an internist and medical director of Annapolis Integrative MedicineKevin Audlin, MD, gynecologist and co-director of The Endometriosis Center at Mercy Medical Center, Baltimore

20 l CHESPHYSICIAN.COM
COMPLIANCE
The risk of a Medicare revocation of billing privileges may be far greater than a licensure sanction, yet many physicians do not understand the
Medicare enrollment rules and are not actively involved in taking the necessary steps to avoid a revocation. CMS and its contractors are placing significant emphasis on compliance with these rules, and a misstep could carry grave consequences. The first major overhaul of the enrollment rules began in mid-2006, when Medicare implemented an every-five-year revalidation requirement and sanctions for noncompliance. The types of sanctions available to CMS and the reasons for imposing such sanctions have increased over the last 10 years.
Billing Privilege Revocations Have Serious Consequences
One of the most common sanctions, a billing privilege revocation, not only results in the loss of Medicare billing privileges, but is followed by a mandated one- to three-year bar to re-enrollment. Furthermore, other federal payers are required to terminate an enrollment or contract with a revoked physician or physician group, and many commercial payers will follow suit. Thus, the collateral damages associated with a Medicare billing privilege revocation are significant.
The regulations at 42 C.F.R. § 424.535 set forth the basis for CMS to take a revocation action against an enrolled physician. A review of the reasons for revocation quickly reveals the expansive nature of this revocation authority. CMS may determine that a claim for services “could not have been furnished to a specific individual on the date of service” or may find “a pattern
or practice of submitting claims that fail to meet Medicare requirements.”
Minimal Inadvertent Claims Errors Could Result in Revocation
CMS has confirmed that as few as three claims errors could indicate a “pattern or practice.” Physicians and physician groups are currently having their billing privileges revoked for inadvertent errors in claims, such as a few unrelated claims submitted under the wrong account number associated with a person who is deceased. Sometimes the claims errors account for less than 1% of the total claims for the audit period.
CMS is not the only governmental agency determining physician compliance with these rules. To illustrate, in June 2015, the Government Accountability Office (GAO) issued a report that analyzed randomly selected physician practices’ 2013 enrollment data against four other databases:
n Data from the United States Postal Service to assist in determining if a reported practice location address is a valid address, i.e., an actual physical location and not a PO Box or address associated with a mailing store such as a UPS storen The Federation of State Medical Boards licensure data to determine whether any licensed provider had a disciplinary action that was unreported, which would make the provider ineligible for continued enrollment in Medicaren The Social Security Administration’s deceased individuals file to confirm if any physician noted to still have a current Medicare enrollment on file was deceased
n The Office of Inspector General’s List of Excluded Individuals and Entities to verify that a provider was not excluded from conducting business with the federal government
The GAO’s data analysis identified 105,234 (approximately 11%) of the listed practice location addresses that appeared to be a vacant or invalid address. Of the potential noncompliant locations, 22% had no associated claims data that could indicate a closed or sold location that remained listed in a provider’s enrollment file. For locations that appeared to be in a mailing store, the GAO made observational visits to five selected locations, which included sites in Maryland, Texas and California, and all five were noncompliant locations.
Update Your Compliance PlansFurther, of the 1.3 million physicians
whose active enrollments were reviewed, 174 of the 321 physicians who had a reportable adverse licensing action had a Medicare billing privilege revocation; however, 147 were neither revoked from the Medicare program until months after the adverse action, or were still enrolled in Medicare. Based on reported revocations, it was apparent the CMS acted upon the GAO’s findings to revoke noncompliant physicians.
With the upcoming revalidation requirement and the increased auditing for compliance with the Medicare enrollment rules, it is important to have a comprehensive understanding of the rules. Additionally, if your compliance program does not include periodic claims reviews and reviews of enrollment data for accuracy, now would be the time to update your practice’s compliance plan to include these activities. CP
Donna J. Senft, PT, JD, is a principal at Ober|Kaler. She can be reached at [email protected].
Medicare Enrollment – Would Your Practice Survive Screening? BY DONNA J. SENFT, PT, JD
1 CMS recently announced it is beginning its second cycle of revalidations. Refer to CMS’ website at: www.cms.gov/medicare/provider-enrollment-and-certification/medicareprovidersupenroll/revalidations.html for additional information on the revalidation process.
2 Available on the Internet at: www.ecfr.gov/cgi-bin/text-idx?SID=2ff20b37b62dcd649481d84e0b1b2781&mc=true&node=se42.3.424_1535&rgn=div8.
3 “MEDICARE PROGRAM Additional Actions Needed to Improve Eligibility Verification of Providers and Suppliers,” GAO-15-448 (June 2015). Available at: www.gao.gov/assets/680/671021.pdf.

MAY / JUNE 2016 l 21
Is there a doctor in the house?
Physician’s Mortgage ProgramPurchase or Refinance
Primary or Second/Vacation Homes
High Loan-to-Value with No Mortgage Insurance
Great Rates
Loans Serviced Locally
Million Dollar+ Loans
Low Down Payment
*Applicant must be an existing or newly licensed doctor. Loans subject to program availability and credit approval. Terms and conditions may apply.
Call or visit410.260.2000
severnbank.com
ADVERTISER INDEX
volume 3, S p r i n g / S u m m e r 2011
Community radiology assoCiates
IN THIS ISSUE:When to Order Musculoskeletal MRICRA Pledges to Image WiselyNew Technology:3T MRI, 1.2T Open MRI,16-Slice CT
Win a free lunchfor the whole office!(see page 13)
Â
volume 3, S p r i n g / S u m m e r 2011
www.communityradiology.com
A publication from MedStar good SaMaritan hoSpital
WINTER 2016 MedStargoodSam.org/goodhealth
Keeping a professional dancer on her toes
good newS for thoSe with non-healing woundS
a new year’S guide to health ScreeningS
DestinationsHealing Ethelette’s Hands So She Can Communicate With The WorldDEboraH’S GoT HEr rHyTHm baCk
Pain-FrEE marGarET’S DoinG WHaT SHE LovES
A publication from mEDSTar Union mEmoriaL HoSPiTaL
WINTER 2016 medStarUnionmemorial.org/Destinations
chesphysician.comVOLUME 6 ISSUE 2 MARCH/APRIL 2016
AdvancingDigestive Disease DETECTION AND CAREHELPING PATIENTS BREATHE EASIER
CONNECTED HEALTH AND THEINTERNET OF THINGS
mojomedia.biz l 443.837.6948 | @mojomediallc
HEALTHCARE MARKETING STRATEGIES
Healthcare content specialists.Innovation drives results.
Center for Vein Restoration ...............2centerforvein.com
Ober Kaler Attorneys at Law .............5ober.com
Chesapeake Bay Foundation ..............7cbf.org/BITS
Integrative Medicine for Mental Health .....................................8immh2016.com
Amp Systems, LLC ...............................9ampsysllc.com
Olah Healthcare ...........................10-11olah-healthcare.com
Severn Savings Bank ........................21severnbank.com
Papercamera ......................................21papercamera.com
Maryland Healthcare Education Institute ............................29mhei.org
PNC Bank ...........................................31pnc.com/hcprofessionals
Advanced Radiology .........................32advancedradiology.com
22 l CHESPHYSICIAN.COM
ChildrenCOMPLEX CONDIT IONSin
Mark Mahone, PhD
Rising rates of
children with ADHD
and other complex
conditions are challenging
physicians who care for
children to raise the bar
in their management
practices. Area experts
offer their advice.
MAY / JUNE 2016 l 23
SUCCESSFUL MANAGEMENT OF ADHDChances are good that you know at least one child with
attention-deficit hyperactivity disorder (ADHD). Characterized by persistent inattention, hyperactivity and often impulsivity, ADHD is the most frequently diagnosed developmental neuropsychiatric disorder. The CDC estimates that nearly 10% of children ages four to 17 have ADHD, with 13% of boys and 7% of girls affected.
Mark Mahone, PhD, a child neuropsychologist, research scientist, and the director of the Department of Neuropsychology at the Kennedy Krieger Institute in Baltimore, says, “We now know that ADHD is a development disability that starts in childhood and has a known genetic risk that is not confined to a single gene. A number of factors, including a stressful or unpredictable environment, or exposure to environmental toxins, make you more prone to manifest ADHD, while a supportive, nurturing environment and being in good health mitigates it.”
He adds, “Many studies are examining the role of sleep issues in ADHD. Given that sleep problems are epidemic in our current society, if they go on long enough, they can change the brain and exacerbate the manifestations of the disorder. Obesity also increases one’s risk, and the mother’s health during pregnancy may lead to greater risk for the condition.”
ADHD IN GIRLS While ADHD is also common in girls, they are less likely to be
diagnosed early. Dr. Mahone explains, “We now know that boys and girls present differently. Boys tend to be hyperactive and impulsive, loud and boisterous even as toddlers, while girls often present with less hyperactivity and impulsivity. The hypothesis is that girls’ brains develop earlier, so that symptoms of ADHD manifest later. They more typically present with distractibility, spaciness, chattiness, bossiness, or inattention. They tend not to be identified until later in childhood.”
MISSING COMORBID CONDITIONS Despite the fact that ADHD has been detected and treated
for decades, many children still don’t have good outcomes. Dr. Mahone explains why this apparent contradiction exists. “These children usually have a comorbid condition – learning disabilities, language problems, tics, Tourette’s syndrome, anxiety, or depression. These kids are also more likely to be on the autism spectrum. And the majority of these children are only getting their ADHD treated. About one-third of those with ADHD
have dyslexia, and vice versa.” He notes that some boys with anxiety, depression or oppositional defiance disorder can also be misdiagnosed with ADHD.
TIPS FOR DIAGNOSING ADHDThe American Academy of Pediatrics (AAP) has published
guidelines for diagnosing and managing ADHD, which include:n Evaluate any child aged four to 18 who shows orpresents with academic or behavioral problems andsymptoms of inattention, hyperactivity, or impulsivity.n Ensure that the diagnosis meets the criteria in the Diagnostic and Statistical Manual of Mental Disorders – Fifth Edition (DSM-5). n Rule out other possible causes.n Document that the child has difficulties in more than one setting and include reports from parents or guardians, teachers, and/or other school and mental health clinicians involved in the child’s care. n Determine any comorbid physical, emotional, behavioral or development conditions.n Follow the principles of the chronic care model and the medical home.
Dr. Mahone offers this additional advice for diagnostic accuracy. “For those in kindergarten and first grade, it’s important for physicians to get information from the child’s teachers, but recognize that the teacher’s assessment is dependent on a comparison with the rest of the class. A child who is young for his or her grade is more likely to be labeled with ADHD than an older child in that grade. In kindergarten, boys tend to be about a year behind girls in their development.”
A new study by Mu-Hong Chen, MD, and colleagues, published in March 2016 in the Journal of Pediatrics, underscores this point. The study, which examined records from over 378,000 children ages four to 17 in Taiwan, found that the youngest boys in a grade were most often diagnosed with the disorder, while the oldest girls least often received this diagnosis.
“Those with ADHD don’t engage in play the same way and are more likely to get injured because they have less impulse control,” notes Dr. Mahone. “They are more likely to walk into the street, climb onto a countertop, or get stitches. Their motor development often is delayed – not surprising, perhaps, because the motor cortex and executive control systems are adjacent to each other.”

24 l CHESPHYSICIAN.COM
REFERRAL TO A SPECIALTY CENTERWhen should the child be referred to a specialty
center? According to Dr. Mahone, “When the behavior is causing social problems for the child – if they can’t sit to be read to or to eat, or can’t play with other children – physicians should refer the child to a specialty center for evaluation.
“The key is whether the problem is interfering with the child’s life on a regular basis,” he continues. “Even if everyone agrees that it’s ADHD, it’s also important to pick up on comorbidities. At a minimum, you should screen for them. Review the child’s report cards, etc. We look for other things to rule out – such as cognitive problems, anxiety or depression. We use psychological testing and structured observation of behavior and take a careful history.”
EVIDENCE-BASED ADHD TREATMENTThe American Academy of Pediatrics recommends
that preschool-age children should start by receiving behavioral interventions without medication. Only if there is no benefit or when the child is older should medications be added.
“Physicians should work with the school and family to educate them about treatment,” Dr. Mahone advises. “I still see doctors hesitant to consider the diagnosis in preschool. While you do have to be careful, as long as you rule out other disorders, it’s better to treat the child. There are clear risks to waiting, with studies showing that children who are identified and treated earlier fare better and vice versa.”
For most children, stimulants such as methylphenidate are still the first medication to be prescribed. “They work best for most children. Other medications generally are used when you can’t prescribe stimulants.”
Children with ADHD tend to seek immediate rewards. Dr. Mahone recommends that parents help their children learn to tolerate boredom and waiting, and reinforce the behaviors they want to see. Clinicians can help the family develop different ways of responding to the child’s behavior.
Improving behavior has other benefits, Dr. Mahone notes. “When behavioral therapy is effective, it typically decreases the amount of medication needed.”
I’ve worked with families over the long term, and I see that ADHD is a lifelong condition in most people. You don’t treat it and have it go away completely. I tell parents to be prepared to work on it over a child’s lifetime,” he concludes.
COMPLEX MEDICAL CONDITIONS BECOME MORE COMMON
As better technology and care protocols have improved our ability to safely deliver and raise infants with prematurity and other complex conditions, the need for physicians to better manage their care after discharge has grown.
Virginia Keane, MD, a pediatrician who specializes in the
care of children with medical complexity at Mt. Washington Pediatric Hospital in Baltimore, says, “I’ve been interested in children with more complex chronic medical and social problems for the past 30 years. Over that time, the technology has gotten so much better that we’ve been able to save preemies and infants who previously would have died. We’ve created a large population of children with chronic diseases.
“Infants aren’t spending as long in the NICU as they used to,” she continues. “Our rehab unit at Mt. Washington cares for children following elective surgery and preemies who aren’t ready to go home yet but who no longer require an acute care setting.”
She notes that children are increasingly being discharged from a hospital with tracheostomies and ventilators. “Many can’t eat and must be fed with a gastric tube. Parents have been taught how to care for their children, but the typical
Virginia Keane, MD, pediatrician specializing in the care of children with medical complexity, Mt. Washington Pediatric Hospital
MAY / JUNE 2016 l 25
pediatric residency doesn’t teach physicians to care for these children in the community.”
She also sees children with severe chronic conditions such as ADHD, autism, asthma, and diabetes. Typically, her patients have three or more systems involved, five or more medications and/or technology dependence.
Dr. Keane modestly says, “Any pediatrician could do in their office what I do, but they can’t bill enough to make a living doing this because these children often require 60-minute visits. Physicians also may not be comfortable prescribing the medications needed or dealing with sleep issues, hyperactivity, aggression, self-harm, and harm of others. These children are often difficult to manage.”
Dr. Keane echoes Dr. Mahone’s comments about sleep issues contributing to behavioral problems in children. “Many daytime behavioral issues are due to inadequate sleep, causing irritability. They can be easily treated with clonidine. If a child was only sleeping one to two hours a night and you can get them to sleep six to eight hours, everyone can cope better. Parents are so grateful once we’ve ‘put the sleep issue to bed.’ That lets us address the other issues much better.”
She notes that some hyperactive children respond well to ADHD medications, but others actually become more hyperactive on these medications. Her advice? “Learn about these medications and don’t be afraid to experiment, because there aren’t enough psychiatrists in the community to treat these children.”
ABA FOR AUTISMThe only effective behavioral therapy for autistic children
is Applied Behavior Analysis (ABA), but there aren’t enough practitioners trained in this approach. Dr. Keane recommends, “Advocate for your patients to get into these programs but don’t put children who have cognitive impairments but good social skills into these programs. Many autistic children also have comorbid conditions. They should get a neuropsychiatric evaluation and treatment should build on their strengths.”
MANAGING G TUBESDr. Keane bemoans the frequency with which many
premature infants or those on gastric feeding tubes post-operatively return to the hospital several months later because their feeding regimen was never adjusted as they grew, or the tube was malfunctioning.
“Pediatricians should become familiar with these tubes, or at least call a gastroenterologist for a consult,” she advocates. “Because getting an appointment with a pediatric gastroenterologist can be challenging, pediatricians should consider making a change themselves, then sending the GI a note. The specialist can contact you if they would manage the patient differently.”
She adds, “At a minimum, children with medical complexity should be followed at least quarterly or within a month if something changes. We need to adapt the standard number of calories for their activity level. Seeing them every month or two allows you to adjust their feeding regimen up or down by 10% or whatever is appropriate.”
There’s a small window of opportunity to ensure that infants learn to eat by mouth. “Infants only develop the ability to suck at 32 weeks of gestational age,” she explains. “If they’re too sick to suck at that age because they’re still on a ventilator, for example, they may miss the opportunity to learn. If they don’t have an opportunity by the time they’re two to two and a half months old, they may give up permanently on mouth eating.”
While there are no optimal solutions, Dr. Keane advises that having the child suck on a pacifier while being fed by G-tube may help them learn to eat by mouth later on. Caregivers also should read the manual on how to care for the G-tube. “If it’s leaking, you may be able to deflate it, take it out for 20 minutes, then reinsert it. It’s easy to do, but most parents only know how to change the tube.”
MED-PEDS SPECIALTYA new specialty – ‘Med-Peds’ – synthesizes the disciplines
of both internal medicine and pediatrics to deal with complex disorders that persist from childhood into adulthood. Pediatric specialists, such as pediatric cardiologists, also are expanding their practice into adult cardiology and vice versa. Today, both Johns Hopkins and the University of Maryland offer these residency programs. As children with medical complexity become young adults, families and pediatricians will look to these physicians to care for them.
A March 28, 2016, Wall Street Journal article documents how many hospitals are subsidizing the care of these children, providing dedicated teams with the knowledge and skills needed to care for them. A February 2016 article by Dr. Jay Berry in the Journal of Pediatrics showed that care coordination in special clinics can decrease overall healthcare costs.
Dr. Keane observes, “We’re victims of our own success. There are enough of these children with complex medical issues today that every pediatrician should feel comfortable caring for them.” CP
Mark Mahone, PhD, a child neuropsychologist, research scientist, and the director of the Department of Neuropsychology at the Kennedy Krieger Institute in BaltimoreVirginia Keane, MD, a pediatrician who specializes in the care of children with medical complexity at Mt. Washington Pediatric Hospital in Baltimore
There are enough of these children with complex medical issues today that every pediatrician should feel comfortable caring for them. – VIRGINIA KEANE, MD

26 l CHESPHYSICIAN.COM
HEALTHCARE IT
ancy Smit, MBA, RPT, RRT, a partner in the healthcare division of RS&F, LLC (RS&F Healthcare Advisors), states, “Every medical practice is leaving dollars on the table, especially the insurance-based practices. To maximize practice profitability today, you have to continually strengthen your revenue cycle (billing) processes and embrace technology. Keeping overhead down can be a good goal, but not if you don’t invest in the technology you need, including scanners and a robust EHR. In the long run, that makes your staff less efficient and costs you more.
“Having higher staff-to-physician ratios can actually make practices more profitable. You typically get a 3:1 return on the cost of medical assistants because they help to make the physicians much more productive,” Smit explains.
She also advises physicians to take the time to hire the right people, then compensate and reward them sufficiently to keep them. She states, “They are the gas in the engine and the cost of employee turnover is huge!”
Being employed is not appealing to many physicians, but remaining and even thriving in independent practice today is challenging. Optimizing practice operations, leveraging technology and effective marketing can help. So can joining an association of independent physicians, MSO-like entities, or the right clinically independent network (CIN).
TIPS for REMAINING INDEPENDENT
NNancy Smit, MBA, RPT, RRT, partner, healthcare division of RS&F, LLC

MAY / JUNE 2016 l 27
Many practices also make it hard for patients to access them, and fail to recognize how critical patient satisfaction is to the practice’s success. Smit recommends that practices ask themselves the following questions: Do your phones get answered in a timely way, does your web portal work well, can patients get their results online, and what does your practice feel like to current and prospective patients?
“Many practices also struggle to keep up with the continually evolving list of compliance demands,” Smit adds. “Every practice must have a HIPAA privacy and security plan, a billing compliance plan and should be conducting internal coding audits. Predictions are that every practice will be audited by at least one payer in the next few years. If you aren’t already conducting internal audits, hire outside help.”
Peter Uggowitzer, MD, a family practitioner who owns Carroll Family Medicine in Hampstead, Md., is one of the increasingly rare physicians in solo private practice. He recalls, “I started practicing in Carroll County in 1994, moving back from Canada. After working as an employee from 1994 to 1996, three physicians and I split off to become Carroll Family Medicine. We knew nothing about finance or management, so we hired too many people and tried to run two offices. By 1999, we had run out of capital. I was the only one who stayed, and I bought the charts and the name.
“The kind of medicine I practice is old school, with fewer than 18% of physicians doing what I do,” continues Dr. Uggowitzer. “When I offered to serve as a mentor to residents at the University of Maryland, the residency director told me that not a single graduate of the prior year went into family medicine.”
Dr. Uggowitzer went back to in-house billing after a brief experience outsourcing it in 2001. His advice: “You have to learn
how to code well and take advantage of Level 3 and Level 4 visits. The EHR helps you code higher than a paper-based system.”
He adds, “You need people in your office who pursue every cent. Have good billing and coding practices, and do as much yourself as you can, from running cable to fixing the plumbing. Like any business, you have to work hard and have consistent employees. We offer flexibility to our staff because we can’t afford to pay the higher salaries. We do incentivize people and give them bonuses as much as we possibly can.”
MSO-Like GroupsCarl Noback, MD, medical director,
ALLYNE Health, Inc., in Alpharetta, Ga., says, “Our company works with physicians to supply solutions to their ‘pain points.’ We have three goals for our clients: save time, cut expenses and make dollars.”
ALLYNE offers consulting services, managed service agreements, joint venture assistance, investment partnerships, and more, tailored to the needs of each practice. It shares in the risk with participating physicians, offering services such as procurement and asset management.
“We vet various opportunities out there – whether they be new devices, products or drugs,” Dr. Noback says. “That saves physicians three or more hours per week. We also offer group purchasing agreements that are more favorable to physicians. We saved a group of seven primary care providers $27,000 per month (39%) on same or similar supplies of paper, gloves, drugs, etc., by cutting out the middle man.”
The company says it can also help practices improve their collections, claiming that one surgi-center recouped over $1.5 million on $5 million of uncollected claims. It can help physicians invest legally in certain health services, such as diagnostic lab or imaging, or help them adopt a new
service line, such as allergy testing, to add income streams.
Clinically Integrated NetworksThe definition of a Clinically Integrated
Network (CIN) varies, but generally they share common protocols across network providers to achieve measurable targets and improve population health, monitor provider performance and have a physician-driven governance structure. Providers in a CIN typically share IT systems and have staff dedicated to performance improvement.
While many CINs involve hospitals, some are strictly physician-run, including Privia Medical Group, an Arlington, Va.-based physician practice management and population health technology company. It offers physicians a CIN that spans six states and has over 1,400 providers who deliver healthcare services to more than three million patients.
Privia Medical Group combines technology, team-based care and unique wellness programs to help doctors better manage the health of their populations. It also offers reimbursement programs that reward doctors for improving outcomes and delivering high-value care.
Tibor Frekko, MD, managing member of Frekko Primary Care, LLC, a Gaithersburg, Md.-based medical practice he runs with his three physician daughters, is one of Privia’s participating physicians. “My daughters joined my practice in 2000, 2003 and 2005,” he recalls. “Two years ago, they told me that we needed to join Privia if we wanted to keep practicing. At first, I said that it was the dumbest thing I had ever heard, but I started to think about it. I realized we were making less while being hassled more, and decided after a few months of research that it was the only way to go.”
Dr. Frekko originally considered joining
Optimizing for an Independent Practice
TIPS for REMAINING INDEPENDENT

28 l CHESPHYSICIAN.COM
a hospital group, but decided that they wanted more control over his practice than he was willing to give. “Hospitals’ objectives don’t usually mesh with ours. Privia’s incentives are aligned with ours – if we make more, they make more, whereas a hospital makes less if we make more.”
The practice joined Privia Medical Group in January 2015 and went live that June. “With reimbursement moving towards global payments, if we can add more value through preventive measures, such as ensuring patients get their yearly mammograms, hopefully we can make more money and stay alive.”
Proceed With CautionMarni Jameson, executive director
of the national Association of Independent Doctors (AID) based in Florida, warns physicians to read the fine print carefully before agreeing to join a hospital-based CIN.
“Be wary of hospitals that talk a lot about the CIN benefits, but have no operating agreements available for review,” she cautions. “When the paperwork suddenly materializes, they want you to hurry up and sign. The devil is in the details.”
Smit notes that CINs can provide an essential edge in negotiating with insurance plans, but agrees that physicians should do their due diligence first, whether or not hospitals are involved. She recommends, “You need to carefully analyze and understand the financial implications of these relationships – they’re very complicated and often expensive.
“Some models also work better for primary care providers than for certain specialists, such as OB/GYNs, who have a very different reimbursement methodology,” Smit adds. “All of today’s arrangements demand a much higher level of financial analysis and sophistication than in the past. That’s why our boutique healthcare consulting firm, SHR Associates, merged with RS&F, which offers business advisory, consulting, accounting, auditing, and tax services. Together, we now provide all the services our clients need today.”
One of the benefits of the CIN for Dr. Frekko was their EHR. “I didn’t like our existing EHR system – if something went wrong, we called the vendor and had to wait for them to call us back. We were considering switching to athenahealth, when we realized that Privia supplied their system free of charge and enhanced
Medicine is in the process of switching from fee-for-service to global payments. I can’t see how solo physicians or small groups can handle this effectively or efficiently. – TIBOR FREKKO, MD
Tibor Frekko, MD, managing member of Frekko Primary Care, LLC, shown with his three daughters, all physicians in the practice

MAY / JUNE 2016 l 29
integration. But make sure you have a few months’ worth of cash on hand to draw on while you adjust to a new EHR. You can’t see as many patients initially.”
He continues, “Privia is reaching a critical mass. It’s only 20 minutes from us and they provide great, prompt support. They negotiate with the insurers to get better rates. Medicine is in the process of switching from fee-for-service to global payments. I can’t see how solo physicians or small groups can handle this effectively or efficiently.”
Join a Physician AssociationA national nonprofit, AID works
on behalf of physicians, patients and employers to raise awareness and represent the interests of independent physicians. It currently has over 1,000 members and four chapters.
One of its services is offering physicians access to group purchasing organizations. “Most members save 15 to 20%, and the savings pay for our dues very quickly,” Jameson says. “Associations can offer a discount on services, such as collections services, a directory of other physicians to refer to, a 10% discount on medical malpractice, and a voice.”
The Association of American Physicians and Surgeons (AAPS) is another option. It has advocated for physicians since 1943 and offers members a discount on disability and other insurance products.
Personal Contacts Still Get ReferralsJameson advises, “Physicians need to
know who their referral sources are and meet with them, not just send a holiday card or fruit basket. If you can’t get out of the office, have someone in your front office visit them and break the ice.”
She also encourages physicians to create a Fast Fax referral form that the referring source can keep handy. “Make sure you and your staff follow up with them if you do get a referral. They can fax you a referral before the patient leaves their office, and within a few hours, your office should have called that patient, scheduled an appointment, and reported back to the referring provider,
assuring that their patient is getting prompt attention.”
Make friends with the press, adds Jameson, a veteran journalist and former health reporter for the Los Angeles Times and the Orlando Sentinel. “When looking for a physician source, a reporter’s first call is often to the hospital’s PR department, which refers to employed physicians. Bypass that by letting reporters know you’re available as an expert source. Don’t just pitch your agenda.”
Furthermore, create and maintain a strong community presence, Jameson says. Contact community centers to give health talks on your area of expertise. Support a local sports team. This will help you compete with physicians employed by hospitals that receive promotional support.
Dr. Uggowitzer believes, “Things won’t improve for physicians until there’s more
value placed on what we do. But I really enjoy what I do and I know that working for someone else gives me fewer options. I want to keep my independence.” CP
Nancy Smit, MBA, RPT, RRT, a partner in the healthcare division of RS&F, LLC (RS&F Healthcare Advisors), with offices in Owings Mills, Columbia, and Annapolis, Md., and Delray Beach, Fl.Tibor Frekko, MD, managing member of Frekko Primary Care, LLC, a Gaithersburg, Md.-based medical practice Carl Nobak, MD, medical director, ALLYNE Health, LLC, Alpharetta, Ga.Peter Uggowitzer, MD, family practitioner, owner of Carroll Family Medicine, in Hampstead, Md.Marni Jameson, executive director, Association of Independent Doctors
Be wary of hospitals that talk a lot about the CIN benefits, but have no operating agreements available for review. – MARNI JAMESON
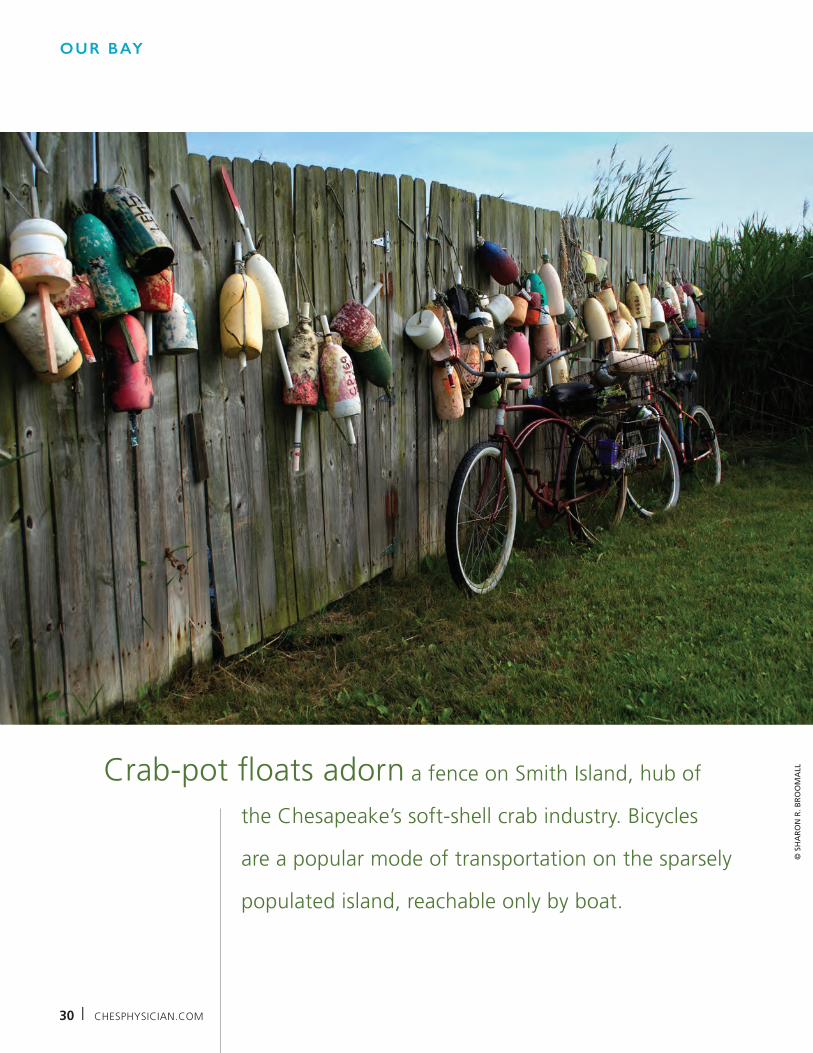
30 l CHESPHYSICIAN.COM
OUR BAY
Crab-pot floats adorn a fence on Smith Island, hub of
the Chesapeake’s soft-shell crab industry. Bicycles
are a popular mode of transportation on the sparsely
populated island, reachable only by boat.
© S
HA
RO
N R
. BR
OO
MA
LL

© S
HA
RO
N R
. BR
OO
MA
LL
