cerebral venous thrombosis: newly in the covid-19 spotlight
TRANSCRIPT

OCTOBER 2021 I 1
Leader in digital CPD for Southern African healthcare professionals
COVID-19Earn 2 free CEUs
© 2021 deNovo Medica
Clara SchutteMBChB, MMed (Neurol), MD Consultant, Department of NeurologyUniversity of Pretoria
Best Practice
Cerebral venous thrombosis: Newly in the COVID-19 spotlight
Learning objectivesYou will learn:
• The significance of cerebral venous thrombosis (CVT) in the context of the COVID-19 pandemic and vaccination
• Risk factors and pathogenesis of CVT, sites of thrombotic occlusion
• Clinical presentation, diagnosis and treatment of CVT.
IntroductionCerebral venous thrombosis (CVT, also known as cerebral venous sinus thrombosis) is a rare condition in clinical practice, but with the advent of the COVID-19 pandemic and more recently, the vaccination against the causative virus, this condition has gained significance. Awareness regarding the presentation and management of CVT is important today. A disturbance of coagulation processes leading to a thrombus in a cerebral vein or larger venous sinus of the brain is involved, leading to a wide variety of clinical presentations. If treated adequately, most patients will have a good prognosis.
© iS
tock
/847
4732
16

2 I OCTOBER 2021
Cerebral venous thrombosis: Newly in the COVID-19 spotlight
Epidemiology – Pre-COVID-19 and during COVID-19 eraThe incidence of CVT worldwide currently is reported to be around 13-15.7 cases per million per year.1 With the advent of newer imaging techniques, diagnosis is more read-ily made, thus probably accounting for the reported rise in incidence during the last decade. The condition most often manifests in younger adults between 30 and 41 years of age with a clear female predominance in this group, but children (especially neonates) and older people may also be affected; in older patients, males and females are equally affected.2 In association with COVID-19 infection, the incidence of CVT has been reported at 39 cases per million people, while the incidence after receiving vaccines Ad26.COV2.S (Johnson/Janssen) and ChAdOx1 nCoV-19 (AstraZeneca) were very low at 0.9 and 3.6 per million persons respectively.3-5
Table 1 shows the current figures of incidence of CVT.
Table 1. Incidence of CVT (July 2021)
Incidence Cases per
million
Worldwide 13-15.7
With COVID-19 infection 39
After vaccine Ad26.COV2.S* 0.9
After vaccine ChAdOx1 n CoV-19^ 3.6
*Johnson/Janssen vaccine; ^AstraZeneca vaccine
Risk factorsMost patients presenting with CVT will have at least one risk factor. Females in the child-bearing age are particularly prone to develop CVT, especially during the puerperium and when taking oestrogen-containing contra-ception. Other non-infective causes include iron-deficiency anaemia, dehydration, haema-tological conditions such as Factor V Leiden abnormalities, Protein S and C deficiency, prothrombin mutation and thrombophilia, as well as connective tissue and immunological disorders including Behçet’s disease, sarcoido-sis, inflammatory bowel disease and systemic lupus erythematosus. Malignancy and some medications have also been associated with CVT.
Infective causes for CVT have decreased dur-ing the last years due to the availability of antibiotic treatment; nevertheless, intracranial infections such as meningitis, and extracranial conditions such as mastoiditis, sinusitis and otitis, or penetrating injuries may still predis-pose a patient to the development of intracra-nial venous thrombosis. Systemic conditions like sepsis and the recently described associa-tion with SARS-CoV-2 infection may also give rise to CVT.5-7 While the risk for develop-ing CVT after vaccination against COVID-19 is very low, details on the current knowledge regarding this condition will be discussed under pathogenesis. Table 2 shows the most common risk factors associated with CVT.
Table 2. Most common risk factors associated with CVT
Hormonal causes • Puerperium • Oestrogen-containing contraceptives.
Haematological conditions • Factor V Leiden• Protein S deficiency• Protein C deficiency• Prothrombin mutation
• Thrombophilia • Anaemia• Polycythaemia.
Connective tissue/immunological disorders
• Behcet’s disease• Sarcoidosis
• Inflammatory bowel disease• Systemic lupus erythematosus.
Malignancy • Intracranial • Extracranial.
Medications • Cytotoxic.

OCTOBER 2021 I 3
Cerebral venous thrombosis: Newly in the COVID-19 spotlight
EARN FREECPD POINTS
Join our CPD community at
and start to earn today!
www.denovomedica.com
Infective • Meningitis• Mastoiditis• Sinusitis
• Otitis• Systemic, such as COVID-19.
Miscellaneous • Penetrating injuries• Dehydration
• Post-vaccination (COVID-19).
Anatomical backgroundThe venous drainage of the brain consists of a superficial and a deep system. The superfi-cial system comprises the cortical veins, the superior anastomotic vein of Trolard and the inferior anastomotic vein of Labbé as well as the superficial middle cerebral vein, which drain into the superior sagittal sinus, the transverse sinus, and the cavernous sinus. The deep system consists of the internal cerebral vein, the vein of Galen and the basal vein of Rosenthal which drain into the straight
sinus as well as the inferior sagittal sinus. The straight sinus also connects the superior and inferior sagittal sinuses, and the transverse sinus eventually becomes the sigmoid sinus which finally drains into the jugular vein. Symptoms of patients presenting with CVT will accordingly vary relative to the location of the thrombotic occlusion. In Figure 1, the venous drainage system of the brain is illustrated.
Cortical veins
Superior sagittal sinus
Vein of Galen and internal cerebral veins
Straight sinus
Transverse sinus
Internal jugular vein
Figure 1A. The venous drainage system of the brain6
Figure 1B. The venous drainage system of the brainhttps://radiologyassistant.nl/neuroradiology/sinus-thrombosis
4 I OCTOBER 2021
Cerebral venous thrombosis: Newly in the COVID-19 spotlight
Sites of thrombotic occlusionMost studies on CVT report the superior sagittal sinus as the most common site for thrombosis (~65%); this is followed by thrombosis in the transverse sinus in 60%; in many patients, however, more than one sinus is involved (~50% to 70%). Thrombosis
of the deep venous system, often associated with an unfavourable outcome, is fortunately relatively rare (10%), as is cavernous sinus thrombosis (1.3%).2,8 Patients with COVID-19 associated CVT tend to have more venous occlusions in the transverse sinuses.7
Clinical presentationThe clinical presentation of CVT is very variable, often leading to a delayed diagnosis. Common manifestations of CVT are shown in Table 3. Most patients (90%) with CVT present with headache and this may be accom-panied in 25% to 40% of cases by a focal neu-rological deficit or seizures.2,8 An altered level of consciousness and coma may also occur. A combination of new onset headache, focal deficit and seizures, especially in a woman of childbearing age, should alert the clinician to a possible underlying CVT – headache is not
usually a primary feature in an arterial stroke, and seizures are also uncommon in ischaemic strokes due to arterial occlusions.5
Most patients with CVT present acutely or sub-acutely, but chronic presentations are also well-described. Acute to sub-acute presentations occur in about 80% of patients, and chronic in 20%; the average time from presentation to diagnosis is seven days, which probably reflects the confusion brought about by the highly variable presentations.2
Table 3. Common clinical manifestations of CVT
Headache • Raised intracranial pressure symptoms• Migraine-type • Thunderclap• Mastoid/occipital.
Focal signs • Motor weakness• Aphasia• Hemisensory deficits• Cranial nerve fallout.
Seizures • Focal• Generalised• Associated with Todd’s paralysis• Status epilepticus.
Altered levels of consciousness
• Mild to moderate (GCS 8-14)• Progressive coma with bilateral motor neuron signs in deep venous system thrombosis.
GCS: Glasgow coma scale
Headache in CVT
The headache reported in patients with CVT may have different characteristics. Many will present with symptoms and signs of raised intracranial pressure, with a headache that worsens on exertion, on lying down or Valsalva manoeuvres, and papilloedema may be seen on fundoscopy. However, the head-ache may also take the form of a migraine, with a pounding component and phono- and
photophobia present. Headaches that occur more rarely in the context of CVT include a thunderclap headache – which may be present with or without an underlying subarachnoid hemorrhage – and pain over the mastoid or occipital area secondary to mastoiditis and subsequent transverse sinus/sigmoid sinus thrombosis.2,5

OCTOBER 2021 I 5
Cerebral venous thrombosis: Newly in the COVID-19 spotlight
EARN FREECPD POINTS
Join our CPD community at
and start to earn today!
www.denovomedica.com
Focal signs
Focal signs found in patients with CVT depend on the site of occlusion. Motor weak-ness appears to be the most common sign; this may be bilateral with occlusion of the sagittal sinus and subsequent venous infarc-tions in the parasagittal region. Notably, the signs may vary over time and fluctuate, another feature that may alert the clinician to the presence of CVT. Aphasia occurs rela-tively commonly in association with CVT, and is usually as a result of thrombosis in the left transverse sinus and involvement of the adjacent cerebral areas.2 Hemisensory deficits
and various cranial nerve involvements have also been described; in this context, it is important to note the typical and quite dramatic clinical presentation of cavernous sinus thrombosis, where the patient develops proptosis, chemosis, and cranial nerves III, IV, VI and the ophthalmic division of the trigeminal nerve fallout.8 Other cranial nerve deficits, such as proximal facial nerve involve-ment and cranial nerve VIII damage due to transverse sinus occlusion, have also been described.
SeizuresSeizures occurring in conjunction with CVT may be generalised or focal, often with sec-ondary generalisation. Interestingly, a Todd’s paralysis is frequently seen after a seizure
related to CVT and can be an alerting factor for the condition. Status epilepticus may also be a presenting clinical feature in CVT.2,9,10
Level of consciousnessAltered level of consciousness is seen in 20% to 30% of patients with CVT, and is mostly mild to moderate (Glasgow coma score (GCS) of 8-14).2,11 However, another pres-entation of CVT that may be noteworthy is non-specific acute cognitive deterioration followed by progressive coma and bilateral,
sometimes fluctuating, long tract (pyramidal) signs due to thrombosis of the deep venous system and subsequent involvement of the thalami bilaterally.12,13 This condition may be associated more commonly with an adverse outcome.
COVID-19 related CVTCVT in association with SARS-CoV-2 infection is rare; a few case series have been reported and in most instances, the tradi-tional risk factors for CVT were absent. The median time from onset of COVID-19 symp-toms until the onset of focal neurological
signs was three to seven days.7,14 Vaccine-induced immune thrombotic thrombocytope-nia (VITT) with CVT occurs predominantly in women, five to 24 days post-vaccination with a vector-virus vaccination.3
PathogenesisThe pathogenesis of venous occlusion differs from the pathogenesis involved in arterial strokes. Whereas arterial strokes occur often as a result of plaque formation and subse-quent thrombosis or embolisation, venous occlusions are primarily a disorder of coagu-lation with a loss of balance between the prothrombotic and fibrinolytic system. It is believed that the thrombus originates at the junction of smaller veins and larger sinuses; the progressive propagation and extension
of the thrombus then accounts for the acute to sub-acute onset of symptoms. The venous drainage system of the brain has many collat-erals and anastomosing channels, and open-ing of these may help to explain fluctuation of symptoms often seen in patients with CVT. Eventually, however, the thrombus effects may exceed the compensatory mechanisms and venous stasis leads to localised cerebral oedema, ischaemia and possibly haemor-rhages in the affected regions.6,8
6 I OCTOBER 2021
Cerebral venous thrombosis: Newly in the COVID-19 spotlight
COVID-19 related CVT
In COVID-19 associated CVT, a proinflam-matory state may contribute to thrombus for-mation. Smaller case series have shown that the erythrocyte sedimentation rate, C-reactive protein, lactate dehydrogenase and ferritin as peripheral biomarkers for inflammation are elevated in patients with COVID-19 infec-tion and subsequent CVT; a marked raise in D-dimer levels was also often seen.7
As mentioned previously, some of the COVID-19 vaccines may induce a prothrom-botic inflammatory state in certain vulnerable
individuals, leading to a thrombocytopenia and activation of the coagulation system with formation of thrombi in the venous system. The pathogenesis of VITT is not fully under-stood at present, but possibly involves leakage of DNA from the cells infected by the vac-cine’s vector virus, an adenovirus, which may bind to platelet factor 4 and set off a cascade of autoantibody production.3 In the interim data analysis of the SA Sisonke implemen-tation study that was aimed at vaccinating health care professionals, no cases of VITT have been reported.15
DiagnosisRadiological investigations are necessary for a definite diagnosis of CVT. In most acute-care units, the first investigation of a patient with neurological symptoms and signs will be a computerised tomography (CT) of the brain. Pre-contrasted CT may show haemorrhages as well as oedema and ischaemic lesions typi-cally exceeding arterial vascular territories; on post-contrast scans an “empty delta” sign, signifying a thrombus in the sagittal sinus, or a “cord” sign, indicating involvement of the transverse sinus, may be visualised. Unfortunately, up to one-third of patients with CVT will have a normal CT scan, but a CT venogram may be able to show thrombi better. Magnetic resonance imaging (MRI) is often preferred when CVT is suspected, and most lesions will be visualised on MRI veno-grams. In addition, MRI can demonstrate thrombus material effectively, and may even help to estimate the time of onset of the CVT. The full extent of parenchymal involvement, ischaemia and oedema is visible on MRI. Other radiological investigations such as
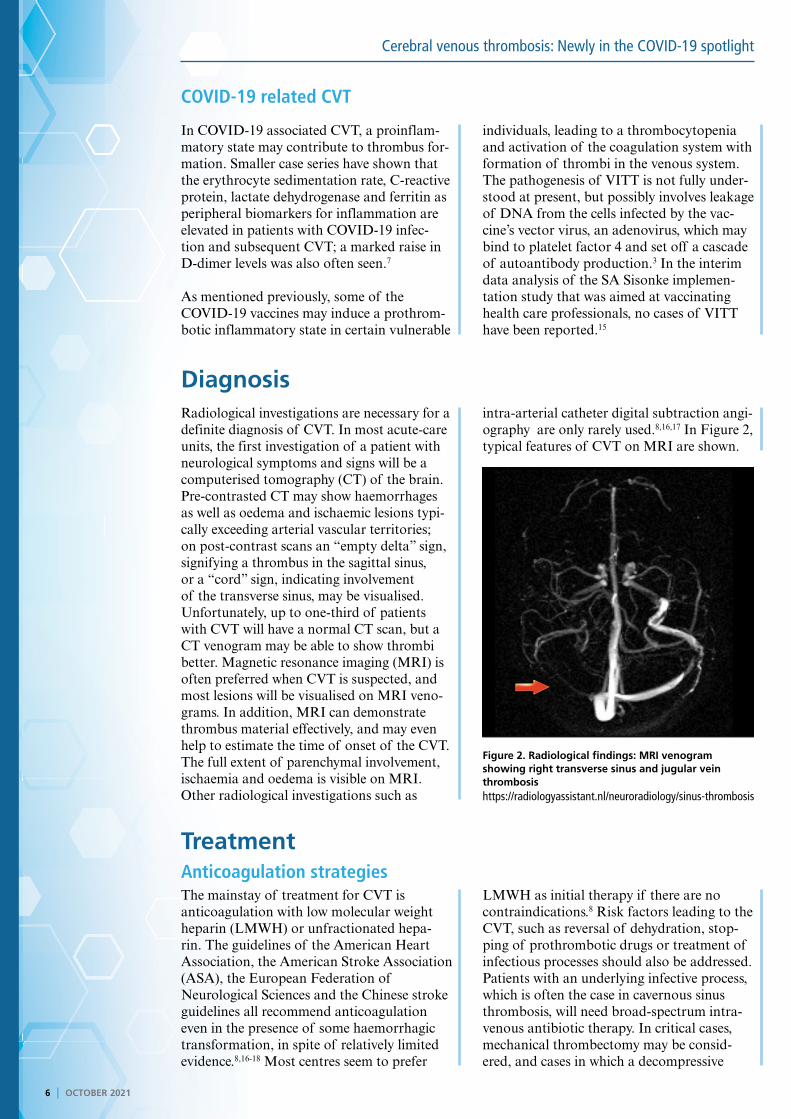
intra-arterial catheter digital subtraction angi-ography are only rarely used.8,16,17 In Figure 2, typical features of CVT on MRI are shown.
TreatmentAnticoagulation strategiesThe mainstay of treatment for CVT is anticoagulation with low molecular weight heparin (LMWH) or unfractionated hepa-rin. The guidelines of the American Heart Association, the American Stroke Association (ASA), the European Federation of Neurological Sciences and the Chinese stroke guidelines all recommend anticoagulation even in the presence of some haemorrhagic transformation, in spite of relatively limited evidence.8,16-18 Most centres seem to prefer
LMWH as initial therapy if there are no contraindications.8 Risk factors leading to the CVT, such as reversal of dehydration, stop-ping of prothrombotic drugs or treatment of infectious processes should also be addressed. Patients with an underlying infective process, which is often the case in cavernous sinus thrombosis, will need broad-spectrum intra-venous antibiotic therapy. In critical cases, mechanical thrombectomy may be consid-ered, and cases in which a decompressive
Figure 2. Radiological findings: MRI venogram showing right transverse sinus and jugular vein thrombosishttps://radiologyassistant.nl/neuroradiology/sinus-thrombosis

OCTOBER 2021 I 7
Cerebral venous thrombosis: Newly in the COVID-19 spotlight
EARN FREECPD POINTS
Join our CPD community at
and start to earn today!
www.denovomedica.com
craniectomy was lifesaving have also been described. After the acute phase, oral anti-coagulation is recommended. The duration of anticoagulation therapy is not clear, but current recommendations suggest that oral anticoagulants should be continued for three months in patients who have reversible risk factors such as anaemia and dehydra-tion; patients with unknown risk factors should be anticoagulated for a period of six to 12 months and patients with recurrent
thrombosis or clear genetic predisposition to thrombotic episodes such as homozygous factor V Leiden should probably receive prophylactic anticoagulation lifelong.8,16 Currently, there is too limited evidence for the administration of the direct oral anticoagu-lants (DOACs) in CVT to make suggestions for their use, but studies are ongoing and data is looking promising. The treatment of CVT in association with COVID-19 infection is similar to this description of therapy.
COVID-19 vaccine-related CVTIt is important to note that the treatment for COVID-19 vaccine-induced CVT or VITT differs fundamentally from the treatment for non-vaccine related CVT. Updated recommen-dations from the ASA state that patients with VITT may not receive heparin in any form as this could aggravate the condition. The treat-ment of VITT consists of a DOAC or other non-heparin components such as argatroban, bivalirudin, danaparoid, or fondaparinux. The dose of the medications may need to be
adjusted in the presence of extreme thrombo-cytopenia or very low fibrinogen, and platelet transfusions should be avoided.3 The sugges-tion of using intravenous immunoglobulins (IVIG) as a treatment modality has been made, since VITT bears close resemblance to heparin-induced thrombocytopenia which may respond to IVIG; currently there are no specific studies addressing this.3 (For a detailed review and recommendations for special inves-tigations, please consult reference 3 and 19.)
PrognosisOverall, the prognosis of CVT is good: stud-ies show a good functional outcome in 75% of patients. Mortality is reported between 3% and 15% in the acute phase; more exten-sive venous sinus involvement, older age and a lower GCS have been shown to have a worse outcome. A high index of suspicion
for the condition and prompt treatment are associated with favourable outcome. The few reported patients with COVID-19 associ-ated CVT have shown an overall mortality of 12.5% to 25.7%, which is comparable to or slightly higher than the mortality in non-COVID-19 patients with CVT.7,8,16
Concluding remarksRelative to other forms of stroke, CVT is a rare condition that has been brought into focus recently due to the reported association with COVID-19 infection and a COVID-19 post-vac-
cination syndrome. Presentation is variable and a high index of suspicion with adequate radio-logical investigations and prompt anticoagula-tion therapy are associated with good outcomes.
Key learnings
• If treated adequately, most patients with CVT will have a good prognosis• CVT most often manifests in younger adults• The incidence of COVID-19 vaccine-related CVT is significantly lower than the incidence of CVT associated with COVID-19
infection• Most patients presenting with CVT will have at least one risk factor that includes hormonal causes, haematological
conditions, connective tissue/immunological disorders, malignancy, medications, infection and other miscellaneous causes• Symptoms of CVT will vary according to the location of the thrombotic occlusion, most commonly the superior sagittal
sinus• Radiological investigations are necessary for a definite diagnosis of CVT• Treatment for CVT is LMWH or unfractionated heparin but in the context of COVID-19 vaccine-related CVT/VITT, treatment
consists of a DOAC or other non-heparin components such as argatroban, bivalirudin, danaparoid, or fondaparinux.

DisclaimerThe views and opinions expressed in the article are those of the presenters and do not necessarily reflect those of the publisher or its sponsor. In all clinical instances, medical practitioners are referred to the product insert documentation as approved by relevant control authorities.
8 I OCTOBER 2021
Cerebral venous thrombosis: Newly in the COVID-19 spotlight
EARN FREECPD POINTS
Are you a member of Southern Africa’s leading
digital Continuing Professional Development
website earning FREE CPD points with access to
best practice content?
Only a few clicks and you can register to start
earning today
Visit
For all Southern African healthcare professionals
www.denovomedica.com
DeNovo Medica
@deNovoMedica
deNovo Medica
Find us at
Published by
70 Arlington Street, Everglen, Cape Town, 7550Tel: (021) 976 0485 I [email protected]
© 2021 deNovo MedicaReg: 2012/216456/07
This summary report was compiled for deNovo Medica byClara Schutte, MBChB, MMed (Neurol), MD, Consultant, Department of Neurology, University of Pretoria
NOW EARN FREE CPD POINTS
Click here to access and submit deNovo Medica’s CPD modules
ReferencesClick on reference to access the scientific article1. Devasagayam S, Wyatt B, Leyden J, et al. Cerebral venous
sinus thrombosis incidence is higher than previously thought: a
retrospective population-based study. Stroke 2016; 47: 2180-
2182.
2. Luo Y, Tlan X, Wang X. Diagnosis and treatment of cerebral
venous thrombosis: a review. Front Aging Neurosci 2018; 10: 2.
3. Furie K, Cushman M, Elkind MS, et al. On behalf of the
American Heart Association/American Stroke Association,
Stroke Council Leadership. Diagnosis and management of
cerebral venous sinus thrombosis with vaccine-induced immune
thrombotic thrombocytopenia. Stroke 2021; 52(7): 2478-2482.
4. Barnes GD, Cuker A, Piazza G, et al. Vaccine-induced
thrombotic thrombocytopenia (VITT) and COVID-19 Vaccines:
What cardiovascular clinicians need to know. Cardiology
Magazine June 8 2021.
5. Behrouzi R, Punter M. Diagnosis and management of cerebral
venous thrombosis. Clin Med 2018; 18(1): 75-79.
6. Stam J. Thrombosis of the cerebral veins and sinuses. N Eng J
Med 2005; 352(17): 1791-1798.
7. Abdalkader M, Shaik SP, Siegler J, et al. Cerebral venous sinus
thrombosis in Covid-19 patients: A multicentre study and
review of the literature. J Stroke Cerebrovasc Dis 2021; 30(6):
105733.
8. Ulivi L, Squitieri M, Cohen H, et al. Cerebral venous thrombosis:
a practical guide. Pract Neurol 2020; 20: 356-367.
9. Ferro JM, Canhão P, Bousser M-G, et al. Early seizures in
cerebral vein and dural sinus thrombosis: risk factors and role
of antiepileptics. Stroke 2008; 39(4): 1152-1158.
10. Mahale R, Mehta A, John AA, et al. Acute seizures in cerebral
venous sinus thrombosis: What predicts it? Epilepsy Res 2016;
123: 1-5.
11. Sassi SB, Touati N, Baccouche H, et al. Cerebral venous
thrombosis: A Tunisian monocenter study on 160 patients. Clin
Appl Thromb Hemost 2017; 23(8): 1005-1009.
12. Allroggen H, Abbott RJ. Cerebral venous sinus thrombosis.
Postgrad Med J 2000; 76: 12-15.
13. Pfefferkorn T, Crassard I, Linn J, et al. Clinical features, course
and outcome in deep cerebral venous system thrombosis: An
analysis of 32 cases. J Neurol 2009; 256(11): 1839-1845.
14. Cavalcanti DD, Raz E, Shapiro M, et al. Cerebral venous
thrombosis associated with COVID-19. Am J Neuroradiol 2020;
41(8): 1370-1376.
15. Takuva S, Takalani, A, Garrett N, et al. Thromboembolic events
in the South African Ad26.COV2.S vaccine study. N Engl J Med
2021; 385(6): 570-571.
16. Saposnik G, Barinagarrementeria F, Brown RD, et al. On
behalf of the American Heart Association, Stroke Council and
the Council on Epidemiology and Prevention. Diagnosis and
management of cerebral venous thrombosis: A statement for
healthcare professionals from the American Heart Association/
American Stroke Association. Stroke 2011; 42(4): 1158-1192.
17. Ferro JM, Bousser M-G, Canhao P, et al. European Stroke
Association Guideline for the diagnosis and treatment of
cerebral venous thrombosis – endorsed by the European
Academy of Neurology. Eur J Neurol 2017; 24: 1203-1213.
18. Fan Y, Yu J, Chen H, et al. Chinese stroke association guidelines
for clinical management of cerebrovascular disorders: executive
summary and 2019 update of clinical management of cerebral
venous sinus thrombosis. Stroke Vasc Neurol 2020; 5(2): 152-
158.
19. Thakur KT, Tamborska A, Wood GK, et al. Clinical review
of cerebral venous thrombosis in the context of COVID-19
vaccinations: Evaluation, management, and scientific questions.
J Neurol Sci 2021; 427: 117532.