case report: renal cell carcinoma presenting as cutaneous … · 2018-04-01 · in non-rcc...
TRANSCRIPT
Page 50NEWBURGER, PERNICIARO, KRISHNAMURTHY
AbstractAlthough renal cell carcinoma (RCC) is among the top ten most common malignancies in both men and women, cutaneous metastasis is very unusual. We report a man who presented to the dermatology clinic with a metastatic lesion of RCC on the scalp, which was the initial presentation of his disease.
Case Report: Renal Cell Carcinoma Presenting as Cutaneous Metastasis to the ScalpJessica Newburger, DO,* Charles Perniciaro, MD,** Karthik Krishnamurthy, DO***
*Dermatology Resident, 2nd Year, Park Avenue Dermatology/Orange Park Medical Center, Orange Park, FL**Dermatopathologist, Aurora Diagnostics/Bernhardt Laboratories, Jacksonville, FL ***Program Director, Dermatology Residency, Park Avenue Dermatology/Orange Park Medical Center, Orange Park, FL
Disclosures: NoneCorrespondence: Jessica Newburger, DO; [email protected]
IntroductionIn both men and women, renal cell carcinoma (RCC) is among the ten most common malignancies.1 In the United States, 62,700 new cases of RCC were predicted for 2016, with 14,240 deaths.2 RCC has a male predominance, and the peak incidence occurs in the sixth and seventh decades.1 The classic presentation of RCC includes the triad of flank pain, hematuria, and a palpable abdominal mass,3 though the triad is only seen in approximately 10% of patients.4 Approximately 30% of patients with RCC develop metastasis, and the most common metastatic sites are the lungs, liver, bone, brain and lymph nodes.5 Cutaneous metastasis in RCC is rare, having an estimated incidence of 3.4%, and it usually presents as a late metastatic manifestation, not as the initial presentation.6 Approximately 30 cases of scalp metastasis of RCC have been reported in the literature.7 We report a man with RCC
metastasis to the scalp as the initial presentation of his disease.
Case ReportA 54-year-old Caucasian male presented with a lesion on his scalp that had developed and enlarged over seven months. On examination, the patient had a solitary, 3.0 cm, friable, erythematous to violaceous nodule of the right parietal scalp (Figure 1). Our initial differential diagnosis included Merkel cell carcinoma, angiosarcoma, atypical fibroxanthoma, and pyogenic granuloma.
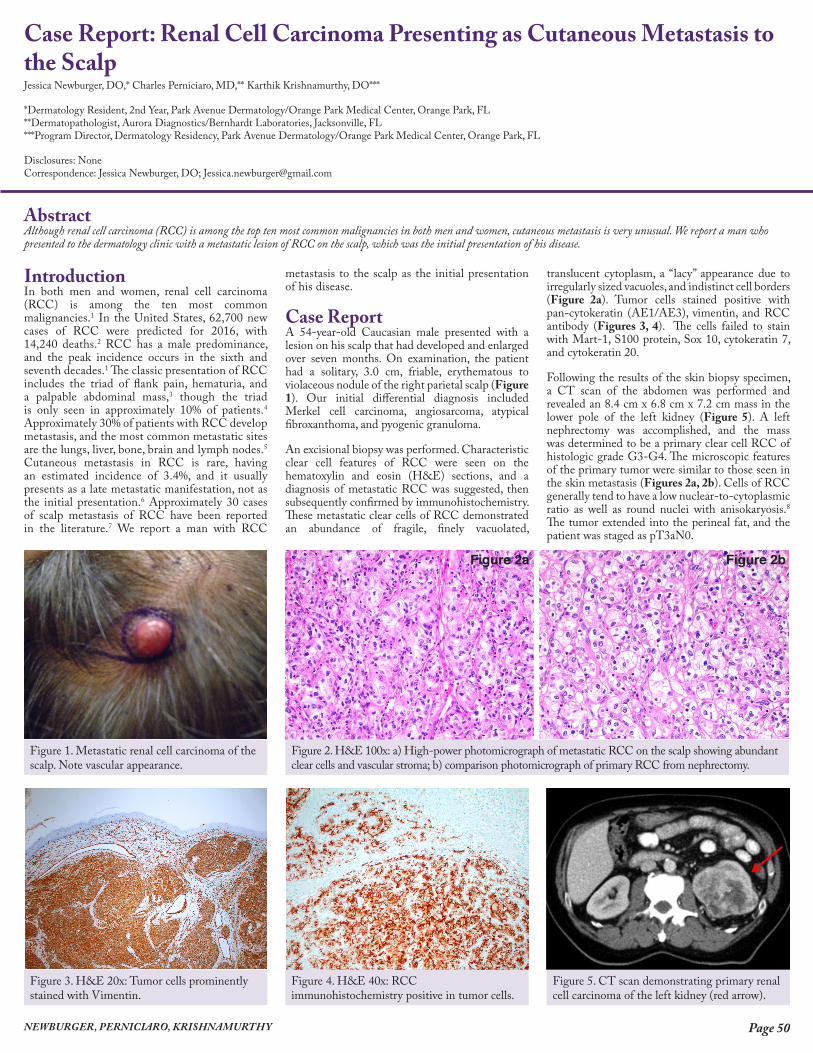
An excisional biopsy was performed. Characteristic clear cell features of RCC were seen on the hematoxylin and eosin (H&E) sections, and a diagnosis of metastatic RCC was suggested, then subsequently confirmed by immunohistochemistry. These metastatic clear cells of RCC demonstrated an abundance of fragile, finely vacuolated,
translucent cytoplasm, a “lacy” appearance due to irregularly sized vacuoles, and indistinct cell borders (Figure 2a). Tumor cells stained positive with pan-cytokeratin (AE1/AE3), vimentin, and RCC antibody (Figures 3, 4). The cells failed to stain with Mart-1, S100 protein, Sox 10, cytokeratin 7, and cytokeratin 20.
Following the results of the skin biopsy specimen, a CT scan of the abdomen was performed and revealed an 8.4 cm x 6.8 cm x 7.2 cm mass in the lower pole of the left kidney (Figure 5). A left nephrectomy was accomplished, and the mass was determined to be a primary clear cell RCC of histologic grade G3-G4. The microscopic features of the primary tumor were similar to those seen in the skin metastasis (Figures 2a, 2b). Cells of RCC generally tend to have a low nuclear-to-cytoplasmic ratio as well as round nuclei with anisokaryosis.8 The tumor extended into the perineal fat, and the patient was staged as pT3aN0.
Figure 2. H&E 100x: a) High-power photomicrograph of metastatic RCC on the scalp showing abundant clear cells and vascular stroma; b) comparison photomicrograph of primary RCC from nephrectomy.
Figure 1. Metastatic renal cell carcinoma of the scalp. Note vascular appearance.
Figure 3. H&E 20x: Tumor cells prominently stained with Vimentin.
Figure 4. H&E 40x: RCC immunohistochemistry positive in tumor cells.
Figure 5. CT scan demonstrating primary renal cell carcinoma of the left kidney (red arrow).
Figure 2a Figure 2b

Page 51 CASE REPORT: RENAL CELL CARCINOMA PRESENTING AS CUTANEOUS METASTASIS TO THE SCALP
The patient underwent adjuvant radiation therapy to the excision site on the scalp with a total dose of 64Gy in 32 fractions. Three months later, an enlarged paratracheal lymph node was noted on follow-up CT scan, subsequently determined to be associated with metastatic RCC, and pazopanib chemotherapy was initiated.
DiscussionGenerally, the tumors that most commonly metastasize to the skin are breast, lung and colon cancer.9 Cancers of the genitourinary tract account for 10% of cutaneous metastatic lesions,10 and RCC is the most common genitourinary cancer to metastasize to the skin.6 RCC accounts for 3% of all solid organ tumors, with cutaneous metastasis occurring in approximately 3.4% of these cases.6 In non-RCC urogenital malignancies, cutaneous metastasis occurs most frequently on the abdomen, while the head and neck region is more commonly affected in RCC.11-13 It is thought that distant metastases in RCC result from hematogenous spread or direct extension of nodal disease, in part due to the rich vascular structure of the tumor.10
Clinically, metastatic RCC lesions are well-circumscribed, cutaneous nodules that can reflect a multitude of colors. As in our patient, these lesions tend to demonstrate a vascular appearance.14 Microscopically, tumor cells are clear and pale-staining, and are usually filled with intracytoplasmic lipid and glycogen, within a fibrous and highly vascular stroma.15 RCC demonstrates an unusual immunohistochemical profile, with tumor cells staining positive for both epithelial and mesenchymal markers.16 The RCC antibody stain is more specific, staining positive in approximately 93% of primary and 84% of metastatic RCC.17
Surgical excision is the primary treatment for RCC. For metastatic disease, the combination of interferon alpha and nephrectomy is superior to interferon alpha alone.18 High-dose interleukin-2 has been the standard therapy for advanced renal cell carcinoma.19 Newer therapies include PDL1 inhibitors, such as atezolizumab,20 and oral angiogenesis inhibitors, such as pazopanib.21 The mean five-year survival rate of patients with cutaneous metastasis is 13% to 50% if a single lesion is present, and decreases to 0% to 8% if multiple lesions are present.22
Prompt diagnosis through biopsy and extensive immunohistochemistry, as well as referral to oncology for workup of the primary lesion and staging, is imperative.
ConclusionCutaneous metastasis in RCC is rare, with an incidence of approximately 3.4%, and usually only presents as a late metastatic manifestation. Our report describes a case of metastatic RCC in which the metastasis to the scalp was the initial presentation of disease.
References1. Jemal A, Murray T, Ward E, Samuels A, Tiwari RC, Ghafoor A, Feuer EJ, Thun MJ. Cancer statistics, 2005. CA Cancer J Clin. 2005;55:10-30.
2. American Cancer Society: Cancer Facts & Statistics [Internet]. Atlanta: American Cancer Society; c2016. Cancer statistics 2016 estimates; 2016 [cited 2016 Mar 19]. Available from: https://www.cancer.org/research/cancer-facts-statistics/all-cancer-facts-figures/cancer-facts-figures-2016.html.
3. Cohen HT, McGovern FJ. Renal-cell carcinoma. N Engl J Med. 2005;353(23):2477-90.
4. Ather MH, Masood N, Siddiqui T. Current management of advanced and metastatic renal cell carcinoma. Urology. 2010;7:1-9.
5. Flanigan RC, Campbell SC, Clark JI, Picken MM. Metastatic renal cell carcinoma. Curr Treat Options Oncol. 2003;4:385-90.
6. Mueller TJ, Wu H, Greenberg RE. Cutaneous metastases from genitourinary malignancies. Urology. 2004;63:1021-6.
7. Smyth LG, Casey RG, Quinlan DM. Renal cell carcinoma presenting as an ominous metachronous scalp metastasis. Can Urol Assoc J. 2010;4:E64-6.
8. Dhingra V, Misra V, Singh AP, Agarwal S. Cytodiagnosis of cutaneous metastasis from renal cell carcinoma: a case report with review of literature. J Cytol. 2011;28:30-2.
9. Krathen RA, Orengo IF, Rosen T. Cutaneous metastasis: a meta-analysis of data. South Med J. 2003;96:164-7.
10. Saeed S, Keehn CA, Morgan MB. Cutaneous metastasis: a clinical, pathological, and immunohistochemical appraisal. J Cutan Pathol. 2004;31:419-30.
11. Weiss L, Harlos JP, Torhorst J, Gunthard B, Hartveit F, Svendsen E, Huang WL, Grundmann E, Eder M, Zwicknagl M. Metastatic patterns of renal carcinoma: an analysis of 687 necropsies. J Cancer Res Clin Oncol. 1988;114:605-12.
12. Gottlieb MD, Roland Jr JT. Paradoxical spread of renal cell carcinoma to the head and neck. Laryngoscope. 1998;108:1301-05.
13. Koga S, Tsuda S, Nishikido M, Matsuya F, Saito Y, Kanetake H. Renal cell carcinoma metastatic to the skin. Anticancer Res. 2000;20:1939-40.
14. Hanson RP, Kneafsey B, Royston D. Cutaneous lesions, not just skin deep! Ir J Med Sci. 2006;175:66-8.
15. Peris K, Fargnoli MC, Lunghi F, Chimenti S. Unusually large cutaneous metastases of renal cell carcinoma. Acta Derm Venereol. 2001;81:77-8.
16. Truong LD, Shen SS. Immunohistochemical Diagnosis of Renal Neoplasms. Arch Pathol Lab. Med 2011;135:92-109.
17. Leica Biosystems: Novocastra Primary Antibodies [Internet]. Buffalo Grove, IL: Leica Biosystems; c2016. Immunohistochemistry Antibodies; 2016 [cited 2016 Mar 19]. Available from: http://www.leicabiosystems.com/ihc-ish-fish/immunohistochemistry-ihc-antibodies-novocastra-reagents/primary-antibodies/.
18. Mickisch GH, Garin A, van Poppel H, de Prijck L, Sylvester R. Radical nephrectomy plus interferon-alfa-based immunotherapy compared with interferon alfa alone in metastatic renal-cell carcinoma: a randomised trial. Lancet. 2001;358:966-70.
19. Yang JC, Sherry RM, Steinberg SM, Topalian SL, Schwartzentruber DJ, Hwu P, Seipp CA, Rogers-Freezer L, Morton KE, White DE, Liewehr DJ, Merino MJ, Rosenberg SA. Randomized study of high-dose and low-dose interleukin-2 in patients with metastatic renal cancer. J Clin Oncol. 2003;21:3127-32.
20. Jilaveanu LB, Shuch B, Zito CR, Parisi F, Barr M, Kluger Y, Chen L, Kluger HM. PD-L1 Expression in clear cell renal cell carcinoma: an analysis of nephrectomy and sites of metastases. J Cancer. 2014;5:166–72.
21. Sternberg CN, Davis ID, Mardiak J, Szczylik C, Lee E, Wagstaff J, Barrios CH, Salman P, Gladkov OA, Kavina A, Zarbá JJ, Chen M, McCann L, Pandite L, Roychowdhury DF, Hawkins RE. Pazopanib in locally advanced or metastatic renal cell carcinoma: results of a randomized phase III trial. J Clin Oncol. 2010;28:1061-8.
22. Menter A, Boyd AS, McCaffree DM. Recurrent renal cell carcinoma presenting as skin nodules: two case reports and review of the literature. Cutis. 1989;44:305-8.