caries patologi –vad hÄndar i tanden och pulpan?
TRANSCRIPT
11-05-2015
1
CARIES PATOLOGI – VAD HÄNDAR I TANDEN OCH PULPAN?
Lars Bjørndal
DDS, PHD, DR. ODONT
Section of
Cariology and
Endodontics,
University of
Copenhagen
Treatment concepts
AD 3.
1. There are many different treatment options for the same cariouslesion: We need more consensus!
Dias 2
11-05-2015
2
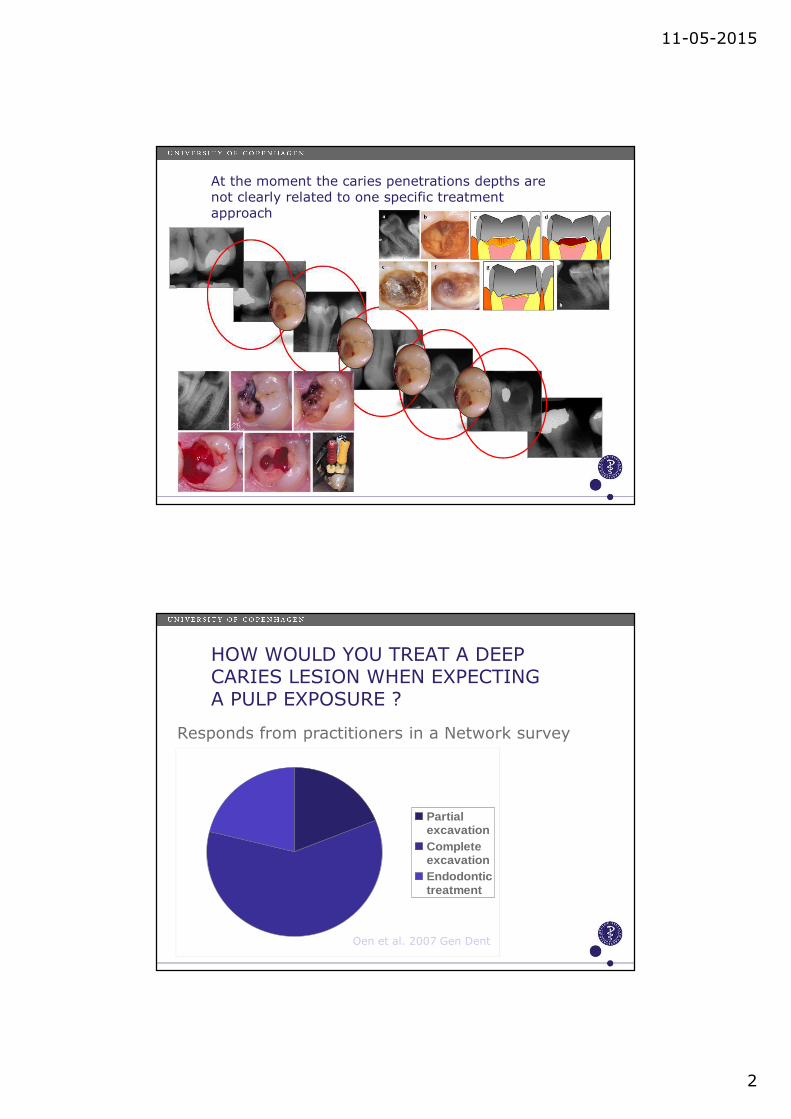
At the moment the caries penetrations depths arenot clearly related to one specific treatmentapproach
HOW WOULD YOU TREAT A DEEP CARIES LESION WHEN EXPECTING A PULP EXPOSURE ?
PartialexcavationCompleteexcavationEndodontictreatment
Oen et al. 2007 Gen Dent
Responds from practitioners in a Network survey
11-05-2015
3
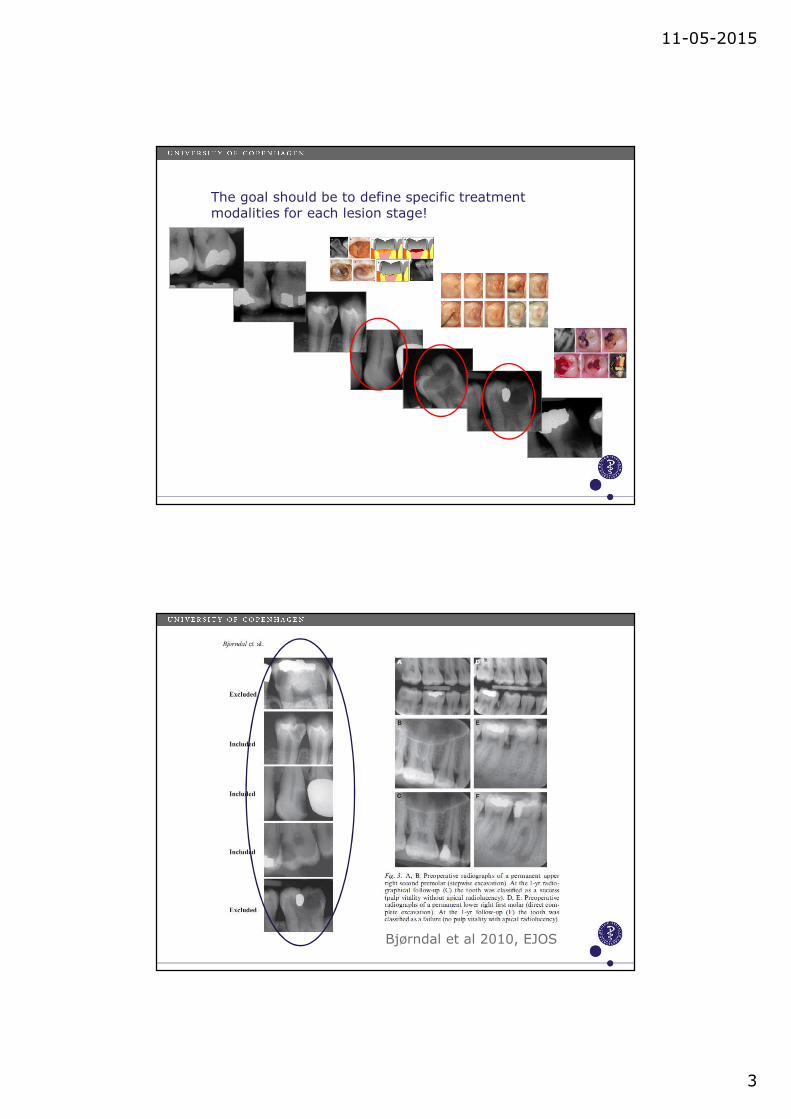
The goal should be to define specific treatment modalities for each lesion stage!
Bjørndal et al 2010, EJOS

11-05-2015
4
In case of carious exposure in deep caries: Direct pulp capping versus Partial Pulpotomy
Pulp
Ketac Molar
Dycal
Direct capping
Pulp
Ketac Molar
Dycal
Partial Pulpotomy
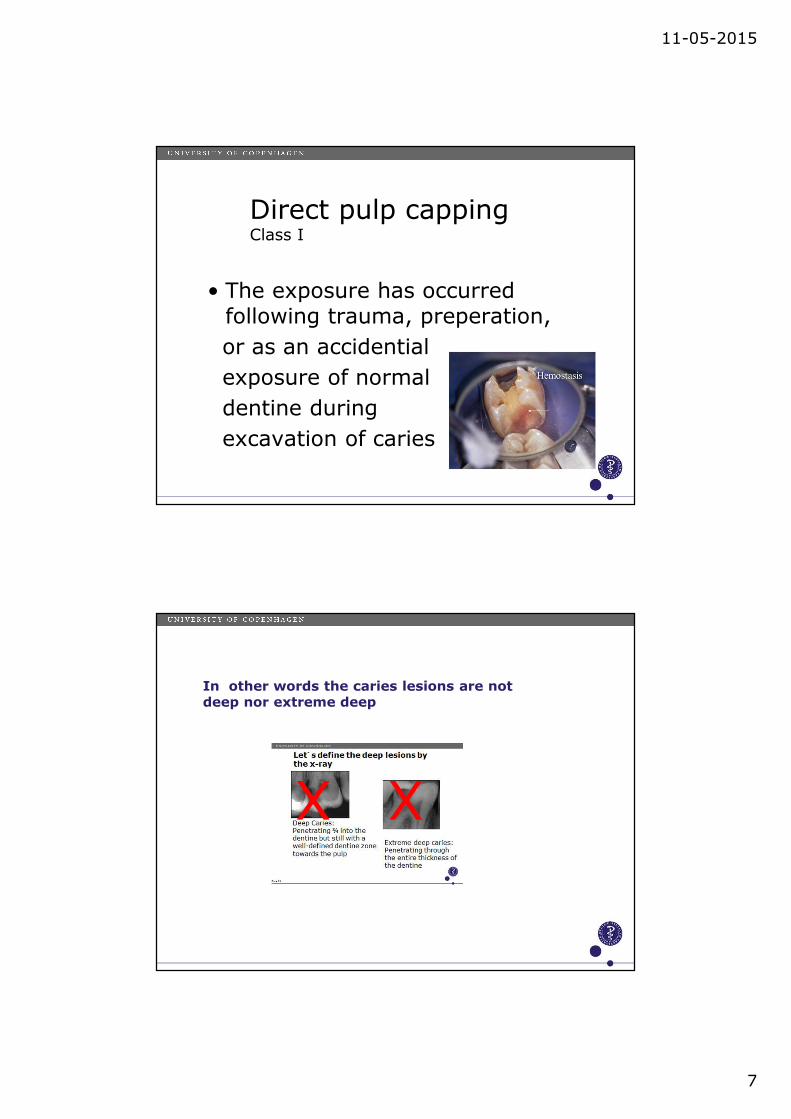
Let´́́́s define the deep lesions by the x-ray
Deep Caries: Penetrating ¾ into the dentine but still with a well-defined dentinetowards the pulp
Extreme deep caries: Penetrating through the entire thickness of the dentine

11-05-2015
5
The outcome of all patients
involved in the excavation trial !
Unexposeddeep
caries lesions
Pulp survivalrate:
88.8%
Cariously exposedpulps
Pulp survivalrate:
32.8%
Area of Cariology and Endodontics
Direct pulp capping versus partial pulpotomy
Pulp CappingTrial
N = 58
Treatment visit: Direct Pulp
Capping N = 27
1. month controlvisit
N = 25
At 1-yr follow-upN = 9
Pain N = 11 Lost N = 5
Pain N = 2
Treatment visit: Partial
PulpotomyN = 31
1. month controlvisit
N = 26
At 1-yr follow-upN = 13
Pain N = 11AP N = 1
Lost N = 1
Pain N = 2Haemostasis
N = 2Lost N = 1A lot of pain !
Area of Cariology and Endodontics

11-05-2015
6
•Direct pulp caps
•Class I (accident, ie pulp exposure in normal dentine)
•Class II (Intended ie carious dentine)
A suggested classification of DPC:
•Direct pulp caps
•Class I (accident, ie pulp exposure in normal dentine)
• Class II (Intended ie carious dentine)
A suggested classification of DPC:
11-05-2015
7
• The exposure has occurredfollowing trauma, preperation,
or as an accidential
exposure of normal
dentine during
excavation of caries
Direct pulp cappingClass I
In other words the caries lesions are not deep nor extreme deep
X X
11-05-2015
8
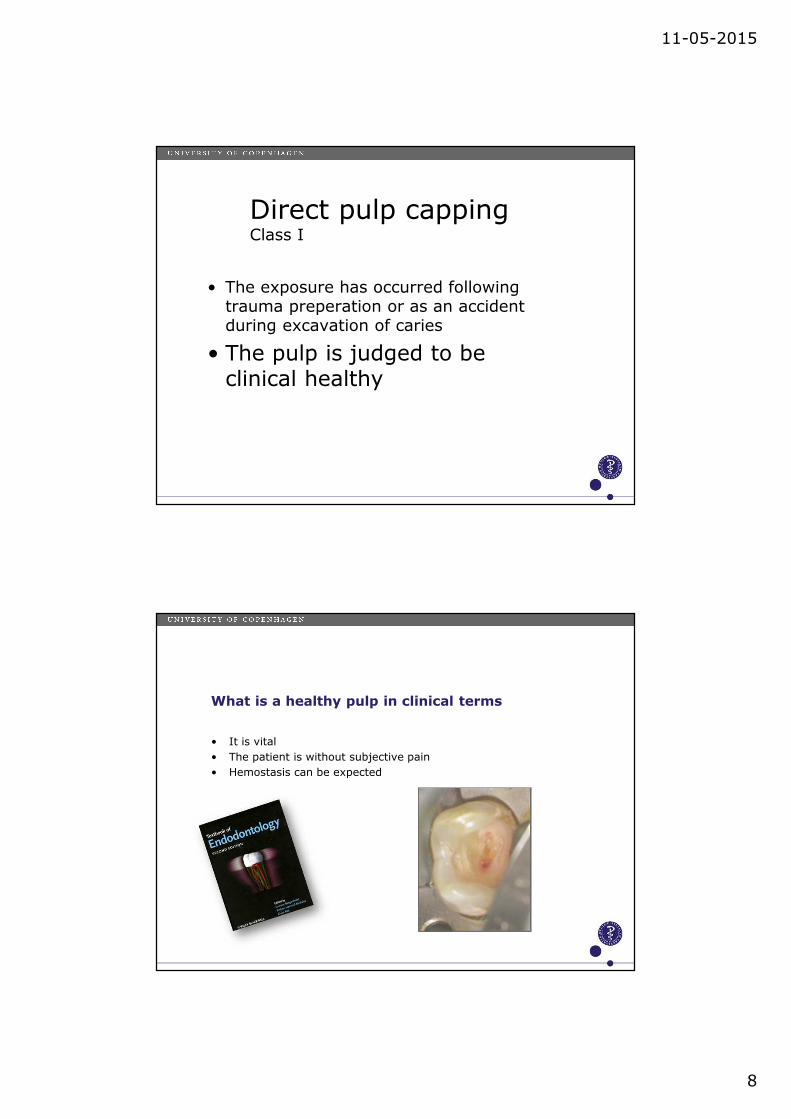
• The exposure has occurred following trauma preperation or as an accident during excavation of caries
• The pulp is judged to be clinical healthy
Direct pulp cappingClass I
What is a healthy pulp in clinical terms
• It is vital
• The patient is without subjective pain
• Hemostasis can be expected
11-05-2015
9
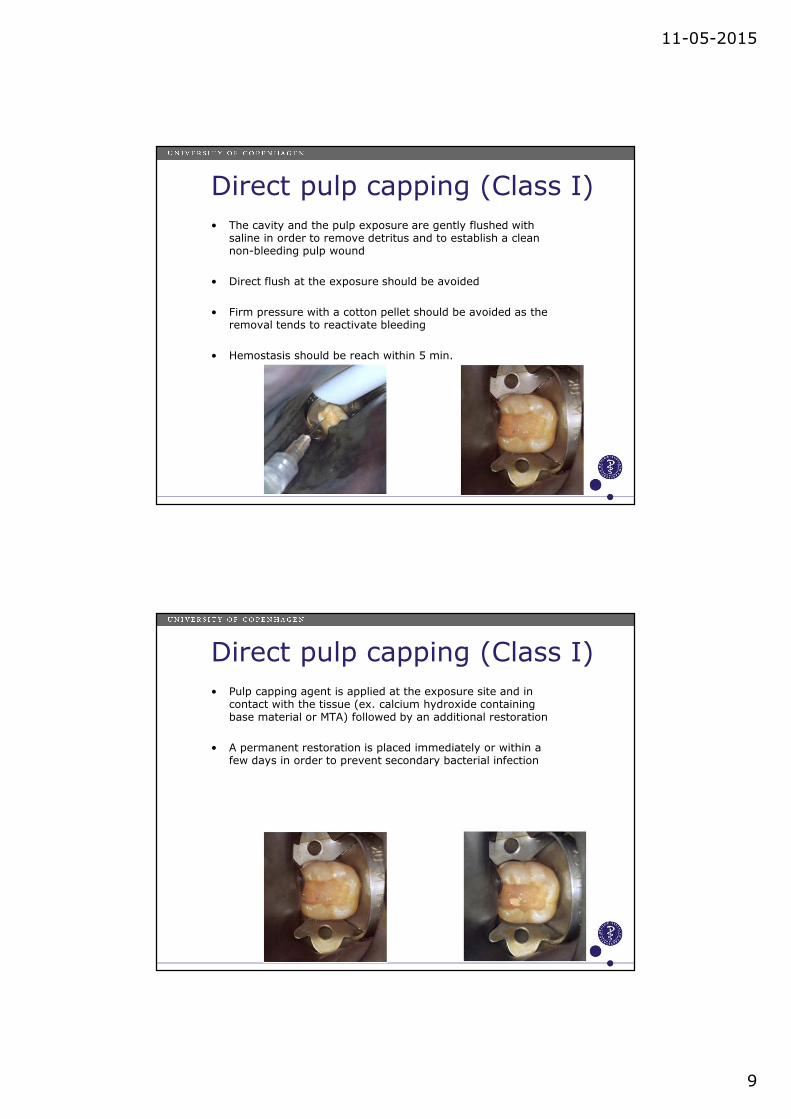
Direct pulp capping (Class I)
• The cavity and the pulp exposure are gently flushed with saline in order to remove detritus and to establish a clean non-bleeding pulp wound
• Direct flush at the exposure should be avoided
• Firm pressure with a cotton pellet should be avoided as the removal tends to reactivate bleeding
• Hemostasis should be reach within 5 min.
Direct pulp capping (Class I)
• Pulp capping agent is applied at the exposure site and in contact with the tissue (ex. calcium hydroxide containing base material or MTA) followed by an additional restoration
• A permanent restoration is placed immediately or within a few days in order to prevent secondary bacterial infection

11-05-2015
10
In short accepting the condition for case selection for the so-called Class I CAP –
The prognosis is traditionally expected to be good !
It is very rare that we get information about the depth of the caries lesions in clinical studies reporting vital pulp therapies!
………. is the pulp exposure performed in sound dentine or is it carried out within carious dentine during treatment of deep / extreme deep caries

11-05-2015
11
•Direct pulp caps• Class I (accident, ie pulp
exposure in normal dentine)
•Class II (Intended ie carious dentine)
A suggested classification of DPC:
• The pulp exposure is not an accident
• Stringent protocol using magnification, caries detector, high conc. of sodium hypoclorite and MTA –like cement
• Deep or Extreme deep caries (Caries reaching the pulp)
Direct pulp cappingClass II (ad modem Bogen)
11-05-2015
12
Area of Cariology and Endodontics
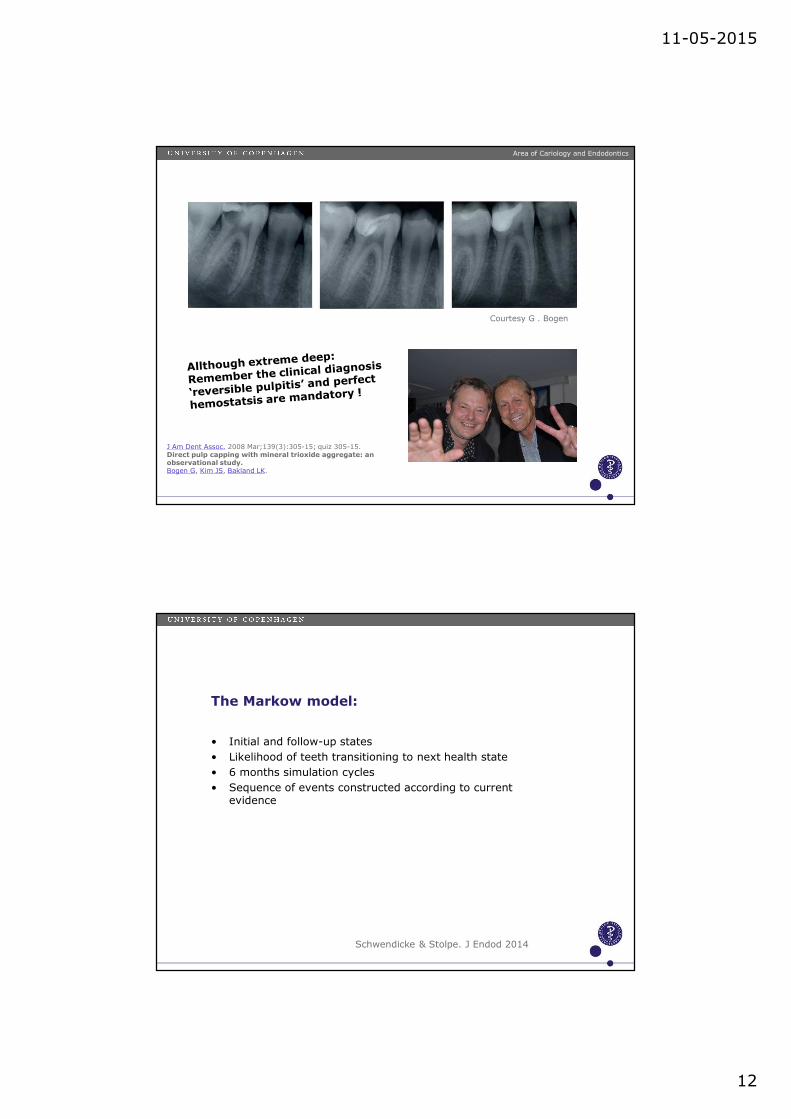
J Am Dent Assoc. 2008 Mar;139(3):305-15; quiz 305-15.Direct pulp capping with mineral trioxide aggregate: an observational study.Bogen G, Kim JS, Bakland LK.
Courtesy G . Bogen
• Initial and follow-up states
• Likelihood of teeth transitioning to next health state
• 6 months simulation cycles
• Sequence of events constructed according to current evidence
The Markow model:
Schwendicke & Stolpe. J Endod 2014
11-05-2015
13
• Deeply carious molar with a sensible, nonsymptomatic (ie painless) pulp being exposed during caries excavation
• NO discrimination between carious exposures and ‘accidential’ (sound dentine) exposures
• DPC were restored either by Calcium hydroxid or MTA followed by direct restoration
• RCT (vital pulpectomy) followed by cast coronal restoration
• Caries lesion involved both approximal and occlusal caries
COST BENFITE ANALYSES:
The assumptions for the simulated scenario using a Markow model:
• Optimal scenario:• Younger pt (< 40 yrs) occlusal exposure sites in
posterior teeth
• Less effective and more costly scenario:• Older patients (> 40 yrs) approximal sites in anterior
teeth. In particular the time until follow-up treatments was short leading to early need of RCT
Results from the simulation scenario:
Schwendicke & Stolpe 2014 JOE

11-05-2015
14
State transition diagram simulating the lifetime of a tooth with an exposed, sensible, non-symptomatic pulp
Area of Cariology and Endodontics
Schwendicke & Stolpe. J Endod 2014
• Optimal scenario:• Younger pt (< 40 yrs) occlusal exposure sites in
posterior teeth
• Less effective and more costly scenario:• Older patients (> 40 yrs) approximal sites in anterior
teeth. In particular the time until follow-up treatments was short leading to early need of RCT
Results from the simulation scenario:
Schwendicke & Stolpe 2014 JOE

11-05-2015
15
Of course many limitations within a simulating environment:
• Can’t integrate all clinical parameters
• Does not account for cost caused by pain and loss of patient time
Direct pulp capping versus partial pulpotomy
Pulp CappingTrial
N = 58
Treatment visit: Direct Pulp
Capping N = 27
1. month controlvisit
N = 25
At 1-yr follow-upN = 9
Pain N = 11 Lost N = 5
Pain N = 2
Treatment visit: Partial
PulpotomyN = 31
1. month controlvisit
N = 26
At 1-yr follow-upN = 13
Pain N = 11AP N = 1
Lost N = 1
Pain N = 2Haemostasis
N = 2Lost N = 1A lot of pain !
Area of Cariology and Endodontics
11-05-2015
16
Of course many limitations within a simulating environment:
• Can’t integrate all clinical parameters
• Does not account for cost caused by pain and loss of patient time
• Prof. experience
• The data building up the the simulation is from the start not the high level evidence data!
• Attitudes toward various treatments
• Exposure in sound or carious dentine (unknown)
Of course many limitations within a simulating environment:
• Can’t integrate all clinical parameters
• Does not account for cost caused by pain and loss of patient time
• Prof. experience
• The data building up the the simulation is from the start not the high levelevidence data!
• Attitudes toward various treatments
• Exposure in sound or carious dentine (unknown)
• The general lack of being able to estimate pulp inflammation
• The health care system varies
11-05-2015
17
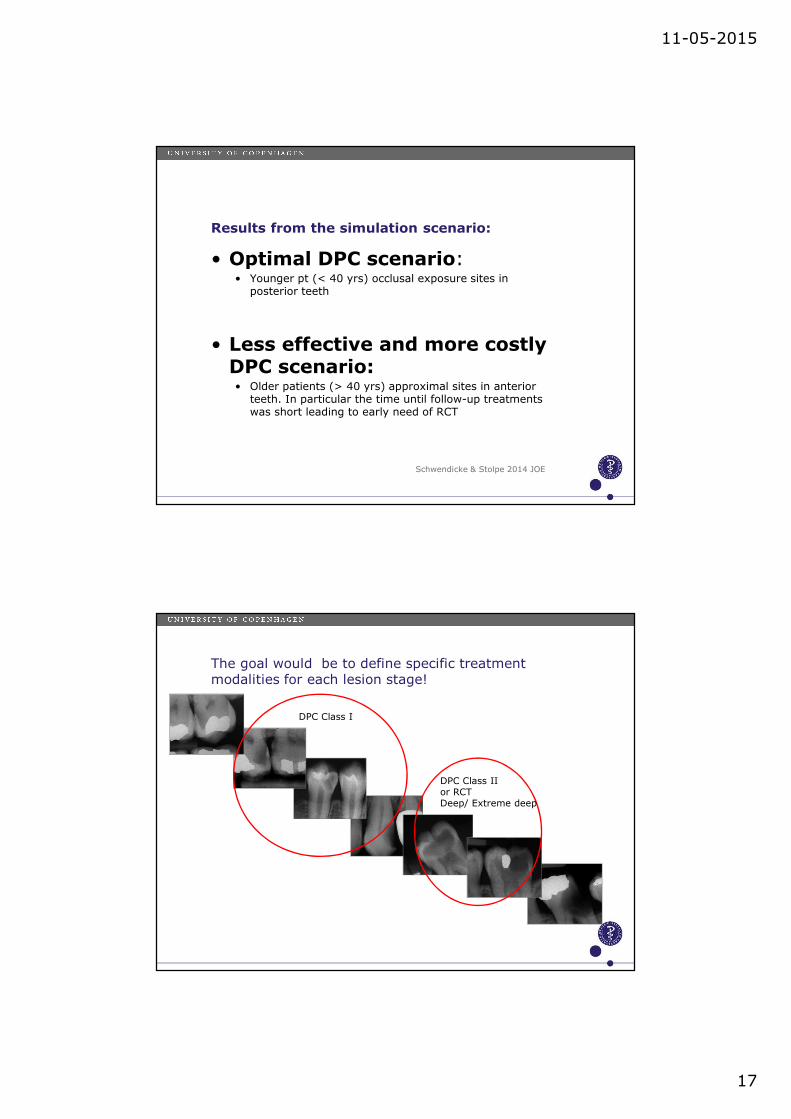
• Optimal DPC scenario:• Younger pt (< 40 yrs) occlusal exposure sites in
posterior teeth
• Less effective and more costly DPC scenario:• Older patients (> 40 yrs) approximal sites in anterior
teeth. In particular the time until follow-up treatments was short leading to early need of RCT
Results from the simulation scenario:
Schwendicke & Stolpe 2014 JOE
The goal would be to define specific treatment modalities for each lesion stage!
DPC Class I
DPC Class IIor RCT Deep/ Extreme deep
11-05-2015
18
At the moment based on the few high quality RCTs in adults a rather traditional approach is suggested:
If you perform the exposure by accident in deep or ectreme deep caries and without being able to do a Class II protocol you should not consider the direct cap, neither the partial pulpotomy nor the full pulpotomy in deep caries lesions in adults
– but facing the pulpectomy!
…………..or avoid the exposure by a less invasive excavation approach!