cardiac involvement in familial amyloidosis with...
TRANSCRIPT

CARDIAC INVOLVEMENT IN FAMILIAL AMYLOIDOSIS WITH POLYNEUROPATHY
Akademisk avhandling som med vederbörligt tillstånd av Rektorsämbetet vid Umeå Universitet för avläggande av medicine doktorsexamen
kommer att offentligen försvaras i sal 933, byggnad 3 A, 9 tr, Regionsjukhuset i Umeå,
tisdagen den 29 maj, 1984, kl 09.00
av
PETER ERIKSSON
UMEÅ 1984
ABSTRACT
Cardiac involvement in familial amyloidosis with polyneuropathy.
Peter Eriksson, Department of Internal Medicine, University of Umeå, S-901 85 Umeå, Sweden
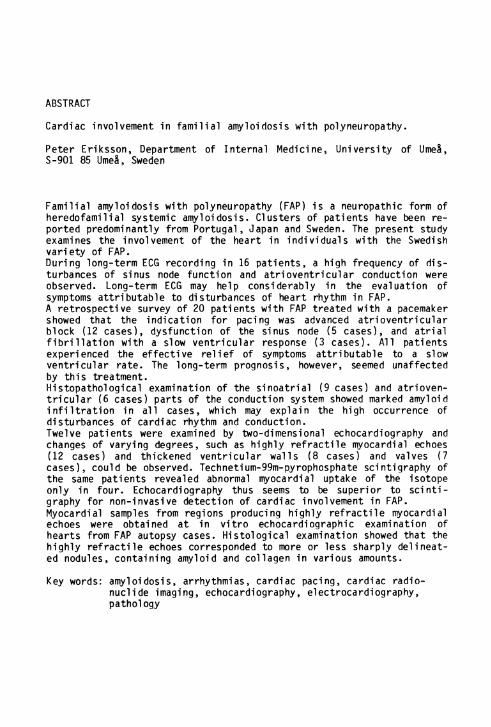
Familial amyloidosis with polyneuropathy (FAP) is a neuropathic form of heredofamilial systemic amyloidosis. Clusters of patients have been reported predominantly from Portugal, Japan and Sweden. The present study examines the involvement of the heart in individuals with the Swedish variety of FAP.During long-term ECG recording in 16 patients, a high frequency of disturbances of sinus node function and atrioventricular conduction were observed. Long-term ECG may help considerably in the evaluation of symptoms attributable to disturbances of heart rhythm in FAP.A retrospective survey of 20 patients with FAP treated with a pacemaker showed that the indication for pacing was advanced atrioventricular block (12 cases), dysfunction of the sinus node (5 cases), and atrial fibrillation with a slow ventricular response (3 cases). All patients experienced the effective relief of symptoms attributable to a slow ventricular rate. The long-term prognosis, however, seemed unaffected by this treatment.Histopathological examination of the sinoatrial (9 cases) and atrioventricular (6 cases) parts of the conduction system showed marked amyloid infiltration in all cases, which may explain the high occurrence of disturbances of cardiac rhythm and conduction.Twelve patients were examined by two-dimensional echocardiography and changes of varying degrees, such as highly refractile myocardial echoes (12 cases) and thickened ventricular walls (8 cases) and valves (7 cases), could be observed. Technetium-99m-pyrophosphate scintigraphy of the same patients revealed abnormal myocardial uptake of the isotope only in four. Echocardiography thus seems to be superior to scintigraphy for non-invasive detection of cardiac involvement in FAP. Myocardial samples from regions producing highly refractile myocardial echoes were obtained at in vitro échocardiographie examination of hearts from FAP autopsy cases. Histological examination showed that the highly refractile echoes corresponded to more or less sharply delineated nodules, containing amyloid and collagen in various amounts.
Key words: amyloidosis, arrhythmias, cardiac pacing, cardiac radionuclide imaging, echocardiography, electrocardiography, pathology

UMEÂ UNIVERSITY MEDICAL DISSERTATIONSNew Series No 118 - ISSN 0346-6612
From the Department of Internal Medicine, University of Umeå, Umeå, Sweden
CARDIAC INVOLVEMENT IN FAMILIAL AMYLOIDOSIS WITH POLYNEUROPATHY
by
PETER ERIKSSON
■Vs'
3
o4 1 \
< o1
1S
Umeå University 1984

2
ABSTRACT
Cardiac involvement in familial amyloidosis with polyneuropathy.
Peter Eriksson, Department of Internal Medicine, University of Umeå, S-901 85 Umeå, Sweden
Familial amyloidosis with polyneuropathy (FAP) is a neuropathic form of heredofamilial systemic amyloidosis. Clusters of patients have been reported predominantly from Portugal, Japan and Sweden. The present study examines the involvement of the the heart in individuals with the Swedish variety of FAP.During long-term ECG recording in 16 patients, a high frequency of disturbances of sinus node function and atrioventricular conduction were observed. Long-term ECG may help considerably in the evaluation of symptoms attributable to disturbances of heart rhythm in FAP.A retrospective survey of 20 patients with FAP treated with a pacemaker showed that the indication for pacing was advanced atrioventricular block (12 cases), dysfunction of the sinus node (5 cases), and atrial fibrillation with a slow ventricular response (3 cases). All patients experienced the effective relief of symptoms attributable to a slow ventricular rate. The long-term prognosis, however, seemed unaffected by this treatment.Histopathological examination of the sinoatrial (9 cases) and atrioventricular (6 cases) parts of the conduction system showed marked amyloid infiltration in all cases, which may explain the high occurrence of disturbances of cardiac rhythm and conduction.Twelve patients were examined by two-dimensional echocardiography and changes of varying degrees, such as highly refractile myocardial echoes (12 cases) and thickened ventricular walls (8 cases) and valves (7 cases), could be observed. Technetium-99m-pyrophosphate scintigraphy of the same patients revealed abnormal myocardial uptake of the isotope only in four. Echocardiography thus seems to be superior to scintigraphy for non-invasive detection of cardiac involvement in FAP. Myocardial samples from regions producing highly refractile myocardial echoes were obtained at in vitro échocardiographie examination of hearts from FAP autopsy cases. Histological examination showed that the highly refractile echoes corresponded to more or less sharply delineated nodules, containing amyloid and collagen in various amounts.
Key words: amyloidosis, arrhythmias, cardiac pacing, cardiac radionuclide imaging, echocardiography, electrocardiography, pathology

To Anita Lisa and Per
4
ABBREVIATIONS
AV = atrioventricular ECG = electrocardiogramFAP = familial amyloidosis with polyneuropathy HREs = highly retractile echoes Tc-99m-PYP = technetium-99m-pyrophosphate

5
CONTENTS
ABBREVIATIONS ................................................................................................ 4
ORIGINAL PAPERS .................................................................................... 6
INTRODUCTION .................................................................................................. 7Amyloid and amyloidosis ........................................................................ 7Classification ......................................................................................... 8Heredofamilial amyloidosis .................................................................. 8Familial amyloidosis with polyneuropathy (Type I) - Swedishvariety ...................................................................................................... 9Involvement of the heart in systemic amyloidosis ......................... 10Senile cardiac amyloidosis .................................................................. 12Involvement of the heart in FAP ......................................................... 12Diagnostic considerations .................................................................... 13
AIMS OF THE STUDY ......................................................................................... 14
PATIENTS .......................................................................................................... 14Study I ...................................................................................................... 14Study II .................................................................................................... 16Studies III, IV and VI ......................................................................... 16Study V ...................................................................................................... 16
METHODS ........................................................................................................... 16Clinical assessment ............................................................................... 16Routine ECG and 24-hour ECG recording ............................................. 16M-mode and two-dimensional echocardiography .................................. 17In vitro echocardiography .................................................................... 17Technetium-99m-pyrophosphate scintigraphy ...................................... 18Histological examinations .................................................................... 18
RESULTS AND DISCUSSION ............................................................................... 19Cardiac rhythm and conduction (Study I) ................................. 19Treatment by pacemaker (Study II) ..................................................... 20Morphological examination of the cardiac conduction system(Studies III and IV) ............................................................................. 22Myocardial acoustic properties and their morphological correlates (Study VI) ....................................................................... 24Non-invasive assessment of involvement of the heart (Study V).. 24
GENERAL SUMMARY AND CONCLUSIONS .............................................................. 27
ACKNOWLEDGEMENTS .................................................................................. 28
REFERENCES ...................................................................................................... 29
STUDY I STUDY II STUDY III STUDY IV STUDY V STUDY VI

6
ORIGINAL PAPERS
The present thesis is based on the following papers, which are referred to by their Roman numerals:
I Eriksson P, Karp K, Bjerle P, Olofsson B-0.Disturbances of cardiac rhythm and conduction in familial amyloidosis with polyneuropathy.Br Heart J 1984 (In press).
II Eriksson P, Olofsson B-0.Pacemaker treatment in familial amyloidosis with polyneuropathy. PACE 1984 (In press).
III Eriksson A, Eriksson P, Olofsson B-0, Thornell L-E.The sinoatrial node in familial amyloidosis with polyneuropathy.A clinico-pathological study of nine cases from northern Sweden. Virchows Arch (Pathol Anat) 1984;402:239-46.
IV Eriksson A, Eriksson P, Olofsson B-0, Thornell L-E.The cardiac atrioventricular conduction system in familial amyloidosis with polyneuropathy. A clinico-pathologic study of six cases from northern Sweden.Acta Pathol Microbiol Immunol Scand, Sect A, 1983;91:343-9.
V Eriksson P, Backman C, Bjerle P, Eriksson A, Holm S, Olofsson B-0. Non-invasive assessment of the presence and severity of cardiac amyloidosis. A study in familial amyloidosis with polyneuropathy by two-dimensional echocardiography and technetium-99m-pyrophosphate scintigraphy.Br Heart J (In press).
VI Eriksson P, Eriksson A, Backman C, Hofer P-Å, Olofsson B-0.Highly refractile myocardial echoes in familial amyloidosis with polyneuropathy. A correlative échocardiographie and histopathologi- cal study.Acta Med Scand (In press).

7
INTRODUCTION
Amyloid and amyloidosisAmyloidosis comprises a heterogeneous group of disorders, some generalized and some localized. Common to all these conditions are deposits of amyloid which may displace, destroy, and replace normal tissues (35, 50, 65). Amyloid is an extracellular, amorphous, eosinophilic, hyalin substance, ubiquitous in distribution (21, 35). Virchow misnamed the substance "amyloid" because he thought that it resembled starch or cellulose (65). Amyloid deposits are composed of proteinaceous fibrils of great chemical diversity (50). These proteins possess distinct properties, including resistance to solution and to proteolytic digestion, a characteristic fibrillar appearance on electron microscopy (34) and an antiparellel beta-pleated sheet conformation as indicated by x-ray crystallography and infrared spectroscopy (e.g. 18, 40). Amyloid deposition is the first pathologic process to be described with manifestations that are dependent on a specific and unique protein conformation (36, 50), and Glenner (50) has suggested the term "beta-fibrillosis" for this disease complex.
Amyloid can be deposited without clinical consequences or may involve virtually any organ system of the body leading to potentially fatal changes. Of course, the disease may also fall between these two extremes. The tissue changes are qualitatively indistinguishable in the various forms of amyloidosis (49). In each instance, the main effects of amyloid seem to be mediated by the compression of adjacent cells and tissues (50), and possibly also by vascular involvement interfering with blood supply (49). The diverse patterns of distribution of amyloid deposits to different organs seem to account for the various clinical manifestations of these syndromes. The worldwide incidence and prevalence of amyloidosis is unknown, but amyloid deposition may come to be regarded as a more important cause of human illness than is realized today (36, 50). The diagnosis of amyloidosis is established by demonstration of green birefringence of tissue specimens stained with Congo red and examined by polarization microscopy (36, 50). The beta-pleated sheet conformation is responsible for this staining reaction (82).

8
During recent years, several amyloid proteins have been isolated and characterized (36, 50). In primary amyloidosis and amyloidosis associated with myeloma, the amyloid proteins consist of immunoglobulin light chains. In secondary amyloidosis and the amyloidosis of familial Mediterranean fever, a protein unrelated to any known immunoglobulin has been found. In some disorders, the amyloid protein is derived from protein hormones and protein hormone precursors secreted by tumor cells. The amyloid protein in familial amyloidosis with polyneuropathy type I is related to prealbumin (37, 94, unpublished observations).
ClassificationThe classification of amyloidosis most often used in clinical practice, and based mainly on clinical features, was proposed by Reiman et al. (83), and later extended by Kyle & Bayrd (65):1. Primary amyloidosis (no preceeding or coexisting disease)2. Myeloma-associated amyloidosis3. Secondary amyloidosis4. Localized deposits and organ-limited amyloidosis5. Heredofamilial amyloidosis.
Glenner (50) has suggested the term "immunocyte dyscrasias with amyloidosis" for primary and myeloma-associated amyloidosis and "reactive systemic amyloidosis" instead of secondary amyloidosis.Cohen (36) has pointed out that amyloid deposition increases with age. Although not apparent clinically, small deposits can often be found in the heart, brain, pancreas, spleen, and endocrine organs of elderly patients. Thus, a sixth group would be "amyloidosis associated with ageing".
Heredofamilial amyloidosisThere are several different systemic and localized amyloid syndromes with a genetic or familial background (49, 100), but there is no generally accepted nosology for these heredofamilial syndromes. Some authors emphasize the predominant organ involved (e.g. neuropathic, néphropathie, or cardiopathie), while others stress the genetic aspects. Since there are as yet no specific tests that enable one type of amyloidosis to be differentiated from another, the recognizable clini-

9
cal patterns probably provide the best basis for classification at present (cf. 49):5:1 Neuropathic forms; Familial amyloidosis with polyneuropathy
Type I (Portugal, Japan, Sweden) (5-8),Type II (Swiss-Indiana, German-Maryland) (68, 87),Type III (Iowa) (1),Type IV (Finland) (70).
5:2 Nephropathie forms;Familial Mediterranean fever and related disorders (12, 97), Muckle-Wells' syndrome (71),Amyloid nephropathy of Ostertag (79).
5:3 Cardiopathie forms;Progressive heart failure (Denmark) (44),Persistent atrial standstill (Mexican-American) (2).
5:4 Localized hereditary amyloid deposits;E.g. hereditary cerebral hemorrhage (Iceland) (52), medullary carcinoma of the thyroid in multiple endocrine adenomatos type II, and several others (49).
Familial amyloidosis with polyneuropathy (Type I) - Swedish variety Since the first report of this syndrome from Portugal in 1952 (7), familial amyloidosis with polyneuropathy (FAP) type I has been described in Japan, England, Germany, the USA, and several other countries (8, 49).
In Scandinavia, FAP type I has been diagnosed almost exclusively in the two northernmost counties of Sweden (6). Since the first case in 1965 (5) about 150 patients have been recognized. Andersson (6) described 60 Swedish patients in 1976. Forty-two of these had relatives who also had FAP, and 18 cases were classified as sporadic. The male to female ratio was 2:1. The age at onset of clinical symptoms varied between 29 and 75 years (mean 53). The duration of symptomatic illness in 27 patients who had died, varied from 4 to 31 years (mean 11). An autosomal dominant mode of inheritance has been suggested in this as well as in other forms of FAP (6, 49, 100).
The most prominant clinical feature is a sensimotor polyneuropathy usually affecting the legs earlier and more severely than the arms.

10
Autonomie nervous dysfunction with urinary retention, orthostatic hypotension, sexual impotency, and dyshidrosis are common features (6). Cardiovascular manifestations including a high frequency of heart rhythm disturbances are common (76, 78). There is often gastrointestinal involvement with altered bowel habits, malabsorption and malnutrition (98). Vitreous opacities with blurring of vision may also develop (4).
Histopathologically, amyloid deposits were observed in the peripheral nervous system. It also occurred in the perivascular collagenous connective tissue, and adjacent to smooth musculature. Amyloid deposits were also found to a greater or lesser extent in other organs and tissues apart from the central nervous system, which was found to be essentially unaffected. Endocrine organs were also essentially unaffected. Furthermore, amyloid was found only in small quantities in the spleen and the liver. In the kidneys, the degree of amyloid deposits varied. Amyloid deposits were invariably found in the myocardium, the heart valves, the aorta and other vessels (6, 58).
Involvement of the heart in systemic amyloidosisThe presence of amyloid desposits in the heart varies in different types of systemic amyloidoses; in primary and myeloma-associated amyloidosis there are cardiac deposits in about 80 to 90 per cent of autopsy cases (21, 35). Cardiac involvement in secondary amyloidosis has been stated to be less common (23). However, Brandt et al. (21) and Cohen (35) reported involvement of the heart in 54 and 60 per cent, respectively, in secondary amyloidosis. Most surveys on cardiac involvement in systemic amyloidosis either do not state the underlying type of amyloidosis, or include different types of amyloid syndromes. There is, however, no substantial evidence that the various types of systemic amyloidosis differ as regards clinical manifestations when they affect the heart (cf. 21, 35). Nevertheless, the organ distribution as well as the amount of amyloid deposited may vary among different amyloid syndromes (21, 35, 65). Cardiac amyloidosis is most often clinically important in primary and myeloma-associated amyloidosis, but also in the heritable amyloid syndromes (50). The different biochemical composition of various amyloid proteins may be one possible reason for

11
this. Cardiac manifestations reflect myocardial involvement, as well as involvement of the specialized conduction tissue, the endo- and pericardium and the valves (23, 26, 62, 85).
According to the WHO/ISCF Task Force on definition and classification of cardiomyopathies (104) cardiac amyloidosis is designated as a "specific heart muscle disease of metabolic origin".
Brigden (23) estimated that amyloid heart disease accounted for some 5 to 10 per cent of all forms of non-coronary myocardial disorders. Cardiac amyloidosis may produce various manifestations from the cardiovascular system, and has been called "one of the great cardiac masqueraders" (85). Congestive heart failure is a common presentation of cardiac amyloidosis (e.g. 23, 35, 85). In Roberts & Waller's series (85) of 54 necropsy patients (42 with primary amyloidosis, 7 with myeloma- associated amyloidosis, and 5 with familial amyloidosis), congestive heart failure occurred in 46 (85 per cent). The duration of heart failure before death ranged from 1 to 108 months (mean 18) and the clinical course was often progressively downhill. The remaining 8 patients (15 per cent) died suddenly and unexpectedly.
Disturbances of rhythm and conduction are present in a large proportion of patients with cardiac amyloidosis (e.g. 23, 25, 26, 85), the most commonly observed abnormalities being atrial fibrillation, incomplete or complete heart block, and fascicular or bundle branch block. Dysfunction of the sinus node has also been described (e.g. 16, 51, 61, 63).
Both supine and orthostatic hypotension occur in patients with all types of amyloidosis (65, 85), and amyloidosis is one cause of spontaneous cure of hypertension (85).
Amyloid heart disease may also clinically and hemodynamically resemble constrictive pericarditis or restrictive cardiomyopathy (29, 53, 59, 69), hence the designations "infiltrative cardiomyopathy" and "stiff heart syndrome". Less common manifestations of cardiac amyloidosis are valvular dysfunction (41, 47), angina pectoris and myocardial infarc-

12
tion (88, 95), cor pulmonale, heart rupture, and pericardial tamponade (24, 67).
Senile cardiac amyloidosisSenile cardiac amyloidosis is an organ-limited amyloidosis. The reported prevalence has varied from under 2 per cent to over 80 per cent, and in a prospective study of 244 consecutive autopsy cases over the age of 60 years, 121 had microscopic evidence of cardiac amyloidosis (57). The prevalence and severity of cardiac amyloid deposits increase with age, but the senile type often produces no macroscopic changes suggesting involvement. At least two different forms have been proposed, one affecting only the atria, while the other is more widespread within the heart and sometimes is also found in other organs (102). The presence of small amounts of amyloid does not seem to be of any clinical importance, while atrial fibrillation and congestive heart failure are more common in patients with evidence of substantial amyloid deposits (57). The conduction tissues are notably often spared even in severe senile cardiac amyloidosis (84). Although senile cardiac amyloidosis appears to be common in elderly patients, it may have little or no clinical significance in most of them, and diagnosis is, with few exceptions (92), made post mortem.
Involvement of the heart in FAPIn a retrospect!*ve survey of ECGs from patients with the Swedish variety of FAP (73), a high frequency of disturbances of atrioventricular and interventricular conduction and also atrial fibrillation were found, and several patients were treated with a pacemaker. The findings were in line with the results of similar studies on FAP from Portugal (45), and Japan (90). Dysfunction of the sinus node in patients with the Swedish variety of FAP was recently reported (77), and this is, to our knowledge, the only report of the sick sinus syndrome in the heredofamilial forms of amyloidosis.
A series of patients underwent echocardiography (9) and most of them showed échocardiographie abnormalities, such as thickened septum and free ventricular walls. Ventricular dimensions were usually within normal limits, and a few patients showed signs of reduced systolic fune-

13
tion. With the two-dimensional technique, the myocardium in several patients exhibited a strongly reflective appearance.
Cardiac catheterization and angiocardiography were carried out on a group of patients with FAP (75). Some showed ventricular pressure curves indicating impaired diastolic function, and several had signs of right or left ventricular outflow tract obstruction. The ejection fraction was normal in all but one patient, and only one had significant coronary artery stenosis. No uniform hemodynamic pattern could thus be identified. Several patients were believed to be in a comparatively early stage of amyloid heart disease, in contrast to most patients in previous reports on hemodynamics in cardiac amyloidosis (e.g. 29, 69, 99).
Diagnostic considerationsDefinite ante mortem diagnosis of cardiac involvement in systemic amyloidosis requires the demonstration of amyloid in a cardiac biopsy (cf. 54, 92, 99). Amyloid heart disease may be suspected when there are symptoms and signs of involvement of the heart in conjunction with systemic amyloidosis diagnosed with a biopsy from e.g. the skin or rectal mucosa. Electrocardiographic abnormalities, when present, may be helpful but are non-specific. Apart from disturbances of heart rhythm and conduction, low QRS voltage and a myocardial infarction pattern may be present (13, 26, 47). Cardiomegaly may or may not be present on a chest x-ray. Echocardiography may show thickened heart walls, decreased wall motion, and reduced systolic thickening (19, 31, 32, 48). It has been stated that a hyperrefractile myocardial appearance is characteristic of cardiac amyloidosis (9, 30, 81, 93). The combination of electrocardiographic low voltage and échocardiographie thickened heart walls is rarely seen in other conditions (27). Radionuclide cardiac imaging with, above all, technetium-99m-pyrophosphate, has shown abnormal myocardial uptake in a substantial proportion of patients with amyloidosis (42, 64, 66, 105).
14
AIMS OF THE STUDY
The prinicipal aims of the present series of investigations were:
1. To assess the frequency of disturbances of cardiac rhythm and conduction in patients with FAP, and to evaluate the clinical significance of such disturbances.
2. To assess the applicability of echocardiography and cardiac scintigraphy in detecting involvement of the heart in FAP.
3. To examine the possible morphological basis of altered electro- physiological and acoustic properties of the heart in FAP.
PATIENTS
Patients with the Swedish variety of familial amyloidosis with polyneuropathy (FAP type I) were the subject of this study. Thus, they all had a characteristic progressive polyneuropathy, affecting the legs more severely than the arms, and often also autonomic neuropathy. The diagnosis was confirmed in all by verification of amyloid in biopsies from the rectal mucosa or the skin, or both. There was no evidence of acute, recurrent or chronic infections, chronic inflammatory conditions, neoplastic disease, immunocyte dyscrasia, or other conditions associated with amyloidosis in any of the patients. Table I identifies the individual patient in the seperate studies. In a proportion of the patients, no close relatives with typical FAP have yet been identified, these are so called "sporadic" cases. However, the characteristic clinical features, the occurrence of the condition in a geographically localized area, and the absence of other diseases associated with amyloidosis justify the designation "familial" for all patients.
Study I. Sixteen patients admitted consecutively to the Department of Internal Medicine, University Hospital, Umeå, were included in this study. Seven patients had symptoms attributable to disturbances of heart rhythm or conduction, and three were receiving drugs known to affect the cardiac conduction system.

15
Table I. Survey of patients included in the studies
Patno.
Age*(yrs)
SexM/F
Duration of symptomatic disease* (yrs)
Pat
I
no. i
II
n study
III IV V VI
I 67 F 5 1 _ _ _ 1 _
II 49 (49) F 16 (16) 2 16 - - 2 -III 67 F 11 3 - - - - -IV 54 F 8 4 - - - 3 -V 68 F 17 5 - - - - -
VI 59 (59) M 6 (6) 6 17 - - 4 -
VII 54 F 5 7 - - - 5 -
Vili 63 (63) F 10 (10) 8 18 - - 6 -
XI 59 M 12 9 - - - - -
X 44 (44) F 7 (7) 10 20 - - 7 -
XI 39 M 2 11 _ _ _ - _
XII 42 M 2 12 - - - 8 -XIII 48 F 16 13 - - - - -XIV 69 M 4 14 - - - 9 -XV 49 (49) F 7 (7) - 12 - - 10 -XVI 66 (66) M 7 (7) - 19 - - 11 -XVII 32 M 2 15 - - - 12 -XVIII 41 (42) F 7 (8) 16 - - - - -XIX 43 M 11 - - 1 1 - 1XX 65 F 7 - - 2 2 - 2
XXI 78 (76) M 3 (1) _ 1 3 3 « 3XXII 79 M 3 - - 4 4 - 4XXIII 79 M 7 - - 5 5 - 5XXIV 89 (82) M 15 (8) - 2 6 6 - 6XXV 75 (71) M 13 (9) - 3 7 - - 7XXVI 76 (74) M 5 (3) - 4 8 - - 8XXVII 77 M 5 - - 9 - - 9XXVIII 63 F 10 - - - - - 10XXIX (64) F (1) - 5 - - - -
XXX (77) M (4) - 6 - - - -
XXXI (63) M (3) _ 7 _ - _
XXXII (66) M (8) - 8 - - - -
XXXIII (63) M (3) - 9 - - - -
XXXIV (70) M (1) - 10 - - - -
XXXV (53) M (5) - 11 - - - -
XXXVI (77) M (4) - 13 - - - -
XXXVII (69) M (4) - 14 - - - -
XXXVIII (75) M (5) ■ 15 “ -
F = female; M = male^Parenthesis indicates age/duration of symptomatic disease when pacemaker was implantated.

16
Study II. Hospital records of patients with a diagnosis of amyloidosis, who had been hospitalized in the counties of Västerbotten and Norrbotten since 1965 were reviewed to establish a correct classification, and 20 FAP patients treated with a pacemaker were included in this study. Nine patients were given pacemakers in Umeå University Hospital. The remaining 11 received theirs at seven other centres in Sweden.
Studies III, IV and VI. The hearts of ten patients were examined in Study VI. Nine of them were also used in Study III and six in Study IV. All patients had an established diagnosis of FAP ante mortem, and they constitute a consecutive autopsy series of patients with FAP. The cause of death was in all cases cachexia with terminal heart failure or pneumonia.
Study V. Twelve patients with FAP of varying severity and with differing duration of symptoms were included in this study.
METHODS
Clinical assessmentPolyneuropathy was graded as follows (74, 76, 98); + = subjective symptoms of polyneuropathy but no functional disturbances ("slight"); ++ = subjective symptoms of polyneuropathy and minor functional disturbances, but the patient is able to undertake all activities of normal everyday life ("moderate"); +++ = subjective symptoms of polyneuropathy and major functional disturbances, the patient being partially incapable of undertaking activities of everyday life ("severe"); ++++ = the patient is in a wheel-chair or bedridden and incapable of performing most activities of everyday life ("very severe").
Routine ECG and 24-hour ECG recordingA 12-lead ECG (aVL, I, -aVR, II, aVF, III, and 6-chest leads) was recorded using a direct-writing ECG apparatus.
Two ECG chest leads were recorded for 24 hours by a two-channel electrocardiographic recorder. The recordings were checked on an oscillo-

17
scope, and the channel with the best registration was replayed, digitized and stored on a micro-computer disk. Analysis of the stored ECG was carried out using a software developed by Nygårds et al. (72). Abnormalities detected by the automatic analysis were visually checked using a graphic terminal. Thus, the computer analysis could be corrected and reclassified when necessary. Every patient was asked to describe his/hers activities and symptoms in a diary during the long-term ECG recording.
The recommendations of the WHO/ISFC Task Force on definition of terms related to cardiac rhythm (103) were followed.
M-mode and two-dimensional echocardiographyEchocardiography was performed with a 90° wide-angle mechanical sector scanner with three revolving 3.0 MHz transducers. The heart was scanned from the sternal, apical, and subcostal positions (55). All examinations were made using a 45 dB logarithmic grey scale curve, which gives the best differentiation of low amplitude echoes, and a linear grey scale curve was also used to obtain grey shades in a uniform matter regardless of the amplitudes of the echo signals (15). Images were recorded on video tape. M-mode registrations could be obtained from one of the transducers in the scanner head, or alternatively, a single beam 2.25 MHz crystal was used. The M-mode traces were recorded using a fibreoptic strip chart recorder. Measurements were made in accordance with the standards of the American Society of Echocardiography (89) and normal values were obtained from Feigenbaum (43). Highly refractile myocardial echoes (HREs) were defined as distinct and very bright echoes that could be visualized from different projections and persisted at gain settings low enough to completely eliminate the echoes of the adjacent endo- and myocardium (15).
In vitro echocardiographyEchocardiographie examination of hearts in vitro was carried out in accordance with a technique developed by Bhandari & Nanda (15). The fixed heart specimens were suspended in a water bath at +22°C at a depth of 4-6 cm, and the transducer was placed at the water surface. Multiple échocardiographie views of the hearts could then be obtained,

18
some simulating in vivo views. HREs were defined as described above. Under échocardiographie control, an ultrasonically visible metallic needle was used to recognize and penetrate regions with changed echo patterns. The contact between the tip of the needle and the myocardium was identified echocardiographically by motion of the normal myocardial echoes and by the motion and changing shape of the HREs. Specimens containing the myocardium around the tip of the needle were then dissected for histopathological analysis.
Technetium-99m-pyrophosphate scintigraphy350 MBq of the isotope was injected intravenously. Two hours later, at least three supine views were obtained, including the anterior, left anterior oblique 45° and left lateral 90°. About 600.000 counts were collected during three minutes from each view. The scans were registered on transparent and polaroid films, and also stored and analysed using a computer. Depending on the activity in the myocardium, radioisotope images were graded from 0 to ++++; 0 = no activity in the region of the heart, + = faint activity believed to be in the blood pool or chest wall ("equivocal"), ++ = definite activity in the myocardium but less intense than in the ribs ("weak"), +++ = activity in the myocardium equal in intensity to the ribs but less than the sternum ("moderate"), ++++ = activity in the myocardium equal to or greater in intensity than the sternum ("intense") (cf. 80).
Histological examinationsThe sinoatrial node as well as the atrioventricular node, bundle and the proximal parts of the bundle branches were removed according to Hudson (60). Together with the myocardial samples obtained from the in vitro échocardiographie examinations, all specimens were dehydrated, embedded in paraffin and sectioned. About 30 sections from the sinus node and 400 to 500 sections from the atrioventricular part (AV node, bundle and proximal bundle branches) of the conduction system were studied in each case. Sections were stained with alkaline Congo red, or al ternatingly with hematoxylin-eosin, or according to the van Gieson or the van Gieson-elastin method. Sections were interpreted as amyloid positive when they showed dichroic biréfringence after staining with alkaline Congo red. The degree of amyloid deposition was graded on a scale of 0 to +++ (cf. 58).

19
RESULTS AND DISCUSSION
Cardiac rhythm and conduction (Study I)Sinus rhythm was the basic rhythm in 15 patients and atrial fibrillation in one. Four patients had sinus pauses exceeding 2 seconds. Frequent atrial premature complexes (more than 30/h) and/or other non-sus- tained supraventricular arrhythmias were observed in nine patients. Ventricular premature complexes were observed in 12 patients and they were frequent (more than 30/h) in four. Two patients had bouts of ventricular tachycardia. Six patients had intermittent disturbances of atrioventricular (AV) conduction; five patients had first degree AV block, in four combined with type I or type II second degree AV block or both. An additional patient had alternating type I and type II second degree AV block. No patient showed complete AV block during this study. Intermittent left bundle branch block was seen in one patient.
Pacemakers were implanted in five of the patients during a follow-up period of 3 to 14 months after the long-term ECG monitoring. (Four of these patients were also included in Study II.) All five had a history of dizziness and/or syncope before the ambulatory ECG recording. Three developed symptomatic complete AV block, despite the withdrawal of negative dromotropic drugs in two cases. Two of these patients showed type II second degree AV block and one intermittent left bundle branch block during the ambulatory ECG recording. Since Study I finished, an additional patient has also proved to have symptomatic complete heart block, and she too had type II second degree AV block during the longterm ECG recording. One patient received a pacemaker because of symptomatic sinus node dysfunction, this patient had sinus pauses up to 2.9 seconds several times during the study. A patient with alternating type I and type II second degree AV block and congestive heart failure had a pacemaker implanted prior to surgery.
The frequency of arrhythmias and disturbances of conduction in the patients studied far exceeded those found in apparently healthy individuals (cf. 10, 17, 33, 56), and the results are consistent with previous reports on systemic amyloidosis with cardiac involvement (e.g. 16, 23, 25, 26, 51, 61, 63, 65, 85), including FAP (45, 73, 77, 90).

20
Most important clinically are the disturbances of sinus node function and AV conduction, as these often necessitate treatment with a pacemaker. Sudden cardiac death occurs among patients with cardiac amyloidosis (21, 35, 65, 85), and this may also be a manifestation of disturbances of rhythm or conduction.
Drugs known to affect cardiac impulse formation or conduction, e.g. digitalis, antiarrhythmics, and carbamazepine (cf. 11) may impair the function of an already compromised conduction system, and may precipitate symptomatic disturbances of conduction. Increased sensitivity to digitalis has been documented in cardiac amyloidosis (23, 26, 28, 85, 86), while the effects of other cardiotrophic drugs are less well- known. Hence, close follow-up is adviseable if such drugs are used. Further studies in this field are needed.
Episodic faintness, light-headedness or giddiness are common complaints in patients seen by general practitioners and internists. Long-term ECG monitoring may not be the first measure used to evaluate the etiology in most of these patients. The results of the present investigation, however, indicate that long-term ECG monitoring should be considered in all FAP patients with such symptoms. Long periods of monitoring may be needed to make a diagnosis in those with only sporadic symptoms.
Treatment by pacemaker (Study II)Twenty patients, 15 men and 5 women, with FAP were treated with a pacemaker between 1968 and August 1983. There was complete AV block in 11 patients; syncope was the predominant symptom in 9 and dizziness in conjunction with bradycardia in the other two. One patient had second degree AV block and cardiac failure, and was given a pacemaker prior to surgery. Five patients had sinus node disease; four had sinus pauses long enough to induce syncopal attacks and one experienced dizziness with decreased physical capacity. One of these patients also had paroxysmal atrial tachycardia, and four had concomitant disturbances of AV or intraventricular conduction or both. Atrial fibrillation with a slow ventricular response was the indication for pacemaker implantation in the remaining three patients, all of whom had heart failure and one also had syncopal attacks. All patients received transvenous right ven-

21
tricular electrodes. There was prompt relief of symptoms referrable to a low ventricular rate in all. Twelve patients have died; their age at implantation was 63 - 82 years (mean 71), and they survived 1-7 years (mean 3.2). The cause of death was in no case found to be associated with pacemaker failure. The patient survival time was short compared with a general pacemaker population (cf. 46), and in ten cases the patients obviously succumbed to other complications arising from the underlying disease than disturbances of cardiac rhythm. There are as yet no documented cases of sudden cardiac death in FAP. Qespite this, the prognosis of patients with severe symptoms because of advanced AV block may well be improved by pacemaker treatment. This would, however, require an untreated control group for definite settlement.
Dislocation of the electrode occurred in four patients, of whom one had a second dislocation diagnosed since Study II was completed. In this latter patient, it was impossible to attach the electrode in the right ventricle via the transvenous route, despite attempts with several different electrode types, and an epicardi al "screw in" electrode had to be used. It is not possible from the present series, to decide whether the incidence of dislocation of electrodes is increased in FAP (cf. 22). Anatomical alterations, secondary to amyloid infiltration with fibrosis and/or muscular hypertrophy might be a predisposing factor for dislodgement. However, alternative explanations may lie in the use of unsuitable electrodes or unsatisfactory operative procedures.
Voltage stimulation thresholds were available for 18 patients; 1.0 V (mean) + 0.14 V (SD) (range 0.6 - 1.8 V). However, the types of electrodes varied, as well as the experience of the operating surgeons, and different or unverified procedures and equipment for testing were used. Nevertheless, there were no records on abnormal stimulation thresholds at implantations or during follow-up (demanding re-operation) in this group of patients.
A large proportion of patients with FAP thus needed treatment with a pacemaker because of advanced AV block or dysfunction of the sinus node. This is also consistent with the results of Study I. In FAP, cardiac pacing may be needed at any time after the onset of symptoms and
22
at any stage of the disease, perhaps with the exception of an early stage with a slight (+) degree of polyneuropathy. This treatment effectively relieved symptoms referable to a slow ventricular rate in all patients. There is as yet no experience of advanced pacing with maintenance of atrioventricular synchrony in FAP. It seems reasonable to assume that the atrial contribution to ventricular filling could be of hemodynamic importance in this disease, especially in cases with thickened ventricular walls and reduced ventricular compliance.
Morphological examination of the cardiac conduction system (Studies III and IV)Six hearts were enlarged, of which three exhibited calcification of the aortic valves with stenosis in two. Eight cases showed no or minimal extramural coronary luminal narrowing, only one case showed moderate narrowing. Microscopically, moderate to severe amyloid deposits were seen in the myocardium proper of all four chambers of all hearts. Amyloid deposits were especially abundant in and near the endocardium and epicardi urn and seemed more abundant in the atria than in the ventricles.
There was marked amyloid infiltration in the sinoatrial node in all the hearts examined. The cells of the sinoatrial node were significantly reduced in number and often replaced or dislocated by amyloid. In all the hearts examined there was a marked amyloid infiltration in all parts of the atrioventricular conduction system. The infiltration of the AV node and bundle seemed to be slightly less than in the bundle branches. Sometimes the amyloid deposits were extensive and almost totally replaced the conduction cells with distal loss of fibres. Amyloid deposits were seen in both sinoatrial and AV nodal arteries, but in no case were obstructed lumina observed. In two cases, there was fatty infiltration of the sinoatrial node and its approaches. Slight or moderate infiltration of the AV node by fat was observed in three cases and fibrosis of the right bundle branch in two. Of the six hearts so examined, calcific deposits were observed in the proximity of the AV bundle in one case with calcific aortic stenosis.
The cause of the cardiac electrophysiological disturbances in amyloidosis is a matter of controversy. Detailed correlative studies of the

23
conduction system in cardiac amyloidosis are few and have produced conflicting results. James (62), Isokane et al. (61) and Bharati et al. (16) favour the hypothesis that the disturbances in cardiac rhythm and conduction are directly caused by amyloid deposition. Buja et al. (26) think that direct amyloid infiltration may be of certain importance. Davies (38) and Ri dol fi et al. (84) consider that direct amyloid infiltration of the conduction tissue is of minor importance and that fibrosis with atrophy is the most important factor.
However, the materials previously reported have been heterogeneous and dominated by the senile type of cardiac amyloidosis. Studies II and IV are the first detailed studies of the conduction system in FAP. Significant infiltration of the myocardium proper and the conduction system has been demonstrated, and it is reasonable to assume that this may account for most of the electrocardiographic abnormalities. Correlation between the ECG findings and the histopathological observations was impeded by the fact that amyloid infiltration was so extensive. Thus, amyloid deposits could in each case fully explain the electrophysiolog- ical disturbances. The lack of conformity between the findings in FAP and the results of some of the previous reports may be ascribed to the different properties of various amyloid proteins (cf. 36, 50), which may have different affinities for conduction tissues. Differences intechnique and extent of examination may also be contributory factors.
The contribution of autonomic neuropathy to the electrocardiographic abnormalities cannot, however, be excluded (cf. 20, 101) and amyloid was also demonstrated in subepicardial neural tissue in our cases. The importance of this finding is not clear and needs further investigation. In no case were drugs or other myocardial disorders found to be the cause of ECG disturbances. Normal lesions from ageing were found in a few cases, but these seemed insignificant compared to the severity and extent of the amyloid infiltration. Disturbances of electrolytebalance could be a further factor contributing to the arrhythmias inthis syndrome. In Study I, 12 out of the 16 patients had moderate or severe gastrointestinal disturbances with altered bowel habits and malabsorption, but plasma concentrations of potassium, sodium and calcium were within normal limits in all. However, the intracellular levels of

24
electrolytes have not been studied, and these may be deranged In spite of normal serum levels (39).
Myocardial acoustic properties and their morphological correlates (Study VI)In Study VI, in vitro two-dimensional echocardiography showed highly retractile myocardial echoes (HREs) in all ten hearts from cases with FAP. The HREs were localized, single or multiple, distinct and very bright echoes. With a linear grey scale curve the HREs emerged more clearly than with a 45 dB logarithmic grey scale curve.
Histologically, the canal caused by the needle could easily be identified in all cases. At the end of this canal a more or less sharply demarcated nodule containing varying amounts of collagen and amyloid was found, and in two thirds amyloid was the predominant component. There were no nodules or other major focal abnormalities in the sections except those indicated by the canal of the needle. The myocardium in general exhibited diffuse amyloid infiltration (cf. Study III, IV). These findings in hearts from cases with FAP are somewhat different from the results of Bhandari & Nanda (15) who found that HREs correlated to deposits of amyloid without fibrosis (or calcification) in two cases examined in vitro. They did not state, however, the type of amyloidosis they reported on.
In conclusion, amyloid deposits in the heart has been found in all autopsy cases of FAP (58, Studies III, IV, VI). The HREs correlated to nodules containing amyloid and collagen, and there was no myocardial nodule without amyloid. Thus, cardiac involvement with amyloid infiltration and HREs must be considered as typical features of FAP, and the presence of HREs seems to be a reliable sign of cardiac amyloid in FAP.
Non-invasive assessment of involvement of the heart (Study V)Eight of the 12 patients investigated had increased thickness of the interventricular septum, and the thickening was asymmetric in two. Six had increased thickness of the left ventricular posterior wall, and the right ventricular wall was thickened in another two. Highly retractile myocardial echoes (HREs) were observed in all patients. The HREs were

25
distinct, single or multiple, and very bright echoes. Their size was 2-5 mm and their shape was rounded or somewhat irregular. The HREs were invariably found in the interventricular septum and often in the free ventricular walls and on occasions in the papillary muscles. Seven patients had thickened cardiac valves and six had pericardial effusion, although the amount of fluid was small.
Abnormal myocardial uptake of technetium-99m-pyrophosphate was observed in four patients, in one patient the uptake was intense (++++), in two moderate (+++), and in one weak (++). The remaining eight patients either had equivocal (+) or no (0) activity in the region of the heart and were considered to have normal scans.
Important échocardiographie findings reported in amyloidosis include increased thickness of the interventricular septum and free ventricular walls, a hyperrefractile myocardial appearance, thickened cardiac valves, and pericardial effusion (9, 14, 15, 19, 30, 31, 32, 48, 81, 93). Thus, all patients in this series showed échocardiographie changes compatible with cardiac amyloidosis. The thickening of the cardiac valves in FAP is caused mainly by pure amyloid deposits (unpublished observations). All patients suffering from heart failure had abundant HREs, thickened heart valves and an interventricular septal thickness exceeding 15 mm.
Previous reports on cardiac scintigraphy in amyloidosis (3, 42, 64, 66, 91, 96, 105) have indicated that, above all, Tc-99m-PYP scintigraphy is a sensitive indicator of cardiac amyloidosis, especially in patients suffering from heart failure. In the series of Falk et al. (42) all patients with heart failure had abnormal scans and three additional patients also showed abnormal myocardial uptake in the absence of heart failure. The patients reported on had myeloma-associated amyloidosis, which is known to affect the heart in about 80-90 per cent of cases (21, 35). Wiesenberg et al. (105) reported that all ten patients in a series showed intense myocardial uptake and all had moderate to severe ventricular hypertrophy while seven also had heart failure. Unfortunately, these authors did not state the type of amyloidosis examined. These results together with a number of case reports (e.g. 3, 64, 91,

26
96) diverge somewhat from our results. Only four of our patients had positive scans and moderate or intense myocardial uptake was found in three patients with heart failure. The reason for this difference is unknown, but there are at least three possible explanations; although all FAP autopsy cases have shown abundant amyloid in the heart, the amount of amyloid of the examined patients may well be less or have a different distribution than in some other forms of amyloidosis. Secondly, several of our patients may have been examined at an earlier stage with less advanced involvement of the heart. Thirdly, different amyloid proteins may well have different properties regarding uptake of Tc-99m- PYP.
Our results, together with those of previous clinical échocardiographie studies in amyloidosis, including the results of Bhandari & Nanda (15) can be used in two ways. First, in patients with biopsy-proven amyloidosis, echocardiography can be used to establish the degree of cardiac involvement. Also very minute changes, i.e. a small number of HREs without any other obvious abnormalities, may indicate early cardiac involvement. Secondly, echocardiography may contribute considerably to the diagnosis of cardiac amyloidosis in a patient with a cardiac dysfunction of uncertain origin. However, in this situation more advanced changes are necessary to avoid incorrect diagnosis. HREs affecting more than one wall of the heart in an adult patient are highly indicative of cardiac amyloidosis (cf. 9, 15, 30, 81, 93, Study V, Study VI). In conjunction with HREs, thickened heart valves and/or thickened ventricular walls are additional indications of the presence of amyloid heart disease, and definite confirmation through biopsy (of cardiac or non-cardiac origin) should be considered.
In conclusion, two-dimensional échocardiographie findings seem to be a sensitive indicator of cardiac involvement in FAP, while the outcome of scintigraphy is more unpredictable and a normal scan does not exclude severe échocardiographie changes or decreased myocardial function.

27
GENERAL SUMMARY AND CONCLUSIONS
1. Disturbances of sinus node function and atrioventricular conduction are common in FAP, and long-term ECG monitoring is a valuable method for detecting otherwise unrecognized intermittent disturbances of the heart rhythm in this condition.
2. A large proportion of patients with FAP need cardiac pacing because of symptomatic dysfunction of the sinus node or disturbances of the atrioventricular conduction. Treatment by pacemaker offers effective symptomatic relief, although the long-term prognosis may not be affected by this treatment.
3. Histopathologically, a marked amyloid infiltration in the sinus node as well as in the atrioventricular conduction system is present, and this may be the major cause of electrophysiological disturbances.
4. Two-dimensional échocardiographie imaging makes it possible to detect discrete changes indicating early cardiac involvement in FAP. Technetium-99m-pyrophosphate scintigraphy is not a sensitive method for establishing involvement of the heart in this disease.
5. In FAP, the morphological substratum for the highly retractile myocardial echoes (HREs) observed by two-dimensional echocardiography is nodules containing collagen and amyloid in varying proportions. Thus, the presence of HREs seem to reflect amyloid deposition in the heart.

28
ACKNOWLEDGEMENTS
I wish to express my sincere gratitude to all who have assisted and helped me to accomplish this study. In particular I want to thank:
Professor Per Olov Wester, Head of the Department of Internal Medicine, for placing time and excellent working facilities at my disposal and for positive criticism and interest,
Professor Håkan Linderholm, Head of the Department of Clinical Physiology, for valuable advice and generous support,
Dr Karl-Anders Jacobsson, Head of the Cardiology Section, my teacher in clinical cardiology, who gave friendly support and encouragement throughout these investigations,
Dr Bert-Ove Olofsson, my friend and tutor, who introduced me to the field of myocardial disorders, and has been my close co-worker throughout these studies. His guidance, support, irrepressible optimism and constructive criticism were invaluable,
Dr Per Bjerle, my teacher in clinical physiology and co-worker, for most valuable advice, positive criticism, sincere enthusiasm, and brilliant analysis,
Dr Anders Eriksson, Head of the Institute of Forensic Medici ne,for his superb guidance, creative spirit, scientific intuition, and excellent collaboration,
Dr Christer Backman, my instructor in echocardiography, and fellow- traveller in the land of shadows,
Dr Per-Äke Hofer, Dr Sonja Holm, Dr Kjell Karp, Dr Lars-Eric Thornell for stimulating cooperation and Mr Sune Westman for skilful assistance,
Dr Börje Ek and Dr Lars Steen, Gastroenterology Section, and Dr Ingmar Lafvas and Dr Bert Isaksson, County Hospital, Skellefteå, for referring their patients for this study,
Miss Loi ornai Örnehult, for typing and retyping and retyping with skill and enthusiasm,
Dr Harold E Vickers, Liverpool, and Dr John Hardy, who corrected the language.
This study was supported by grants from the University of Umeå, the Swedish Medical Research Council (12X-3934), and the Swedish National Association against Heart and Chest Diseases.

29
REFERENCES
1. van Allen MW, Fröhlich JA, Davis JR. Inherited predisposition to generalized amyloidosis. Clinical and pathological study of a family with neuropathy, nephropathy and peptic ulcer. Neurology 1969;19:10-25.
2. Allensworth DC, Rice GJ, Lowe GW. Persistent atrial standstill in a family with myocardial disease. Am J Med 1969;47:775-84.
3. Ali A, Turner DA, Rosenbush SW, Fordham EW. Bone scintigram in cardiac amyloidosis: A case report. Clin Nucl Med 1981;6:105-8.
4. Andersson R, Kassman T. Vitreous opacities in primary familial amyloidosis. Acta Ophthalmol 1968;46:441-7.
5. Andersson R. Hereditary amyloidosis with polyneuropathy. Acta Med Scand 1970;188:85-94.
6. Andersson R. Familial amyloidosis with polyneuropathy. A clinical study based on patients living in northern Sweden. Acta Med Scand; Suppl 590:1-64.
7. Andrade C. A peculiar form of peripheral neuropathy. Familiar atypical generalized amyloidosis with special involvement of the peripheral nerves. Brain 1952;75:408-27.
8. Araki S, Mawatari S, Ohta M, Nakajima A, Kuroiwa Y. Polyneuritic amyloidosis in a Japanese family. Arch Neurol 1968;18:593-602.
9. Backman C, Olofsson B0. Echocardiographie features in familial amyloidosis with polyneuropathy. Acta Med Scand 1983;214:273-8.
10. Barrett PA, Peter CT, Swan HJC, Singh BN, Mandel WJ. The frequency and prognostic significance of electrocardiographic abnormalities in clinically normal invi di duals. Progr Cardiovasc Dis 1981;23:299- 319.
11. Beermann B, Edhag 0, Vallin H. Advanced heart block aggravated by carbamazepine. Br Heart J 1975;37:668-71.
12. Bergman F, Warmenius S. Familial peri reticular amyloidosis in a Swedish family. Am J Med 1968;45:601-6.
13. Bernreiter M. Cardiac amyloidosis. Electrocardiographic findings. Am J Cardiol 1958;1:644-7.
14. Bhandari AK, Nanda NC. Two-dimensional échocardiographie recognition of abnormal changes in the myocardium. Ultrasound Med Biol 1982;8:663-71.

30
15. Bhandari AK, Nanda NC. Myocardial texture characterization by two- dimensional echocardiography. Am J Cardiol 1983;51:817-25.
16. Bharati S, Lev M, Denes P, et al. Infiltrative cardiomyopathy with conduction disease and ventricular arrhythmia: Electrophysiologic and pathologic correlations. Am J Cardiol 1980;45:163-73.
17. Bjerregaard P. Prevalence and variability of cardiac arrhythmias in healthy subjects. In: Chamberlain DA, Kulbertus H, Mogensen L, Schlepper M, eds. Cardiac arrhythmias in the active population. Prevalence, significance and management. Mölndal, Sweden: AB Hassle, 1980:24-34.
18. Bonar L, Cohen AS, Skinner MM. Characterization of the amyloid fibril as a cross-beta protein. Proc Soc Exp Biol Med 1969; 131: 1373-5.
19. Borer JS, Henry WL, Epstein SE. Echocardiographie observations in patients with systemic infiltrative disease involving the heart. Am J Cardiol 1977;39:184-8.
20. Boudoulas H, Schaal SF, Leier CY, Lewis RP. The role of the autonomic nervous system in patients with sinoatrial and atrioventricular node dysfunction. Eur J Cardiol 1981;12:311-19.
21. Brandt K, Cathcart ES, Cohen AS. A clinical analysis of the course and prognosis of forty-two patients with amyloidosis. Am J Med 1968;44:955-69.
22. Brewster GM, Evans AL. Displacement of pacemaker leads - a 10-year survey. Br Heart J 1979;42:266-70.
23. Bridgen W. Cardiac amyloidosis. Progr Cardiovasc Dis 1964;7:142-50.24. Brodarick S, Paine R, Higa E, Carmichael KA. Pericardial tamponade,
a new complication of amyloid heart disease. Am J Med 1982;73: 133-5.
25. Brownstein MH. Cardiac amyloidosis and complete heart block. NY State J Med 1966;66:397-9.
26. Buja LM, Khoi NB, Roberts WC. Clinically significant cardiac amyloidosis. Clinicopathologic findings in 15 patients. Am J Cardiol 1970;26:394-405.
27. Carroll JD, Gaasch WH, McAdam KPWJ. Amyloid cardiomyopathy: Characterization by a distinctive voltage/mass relation. Am J Cardiol 1982;49:9-13.
28. Cassidy JT. Cardiac amyloidosis. Two cases with digitalis sensitivity. Ann Intern Med 1961;55:989-94.
31
29. Chew C, Zi ady GM, Raphael MJ, Oakley CM. The functional defect in amyloid heart disease. The "stiff heart" syndrome. Am J Cardiol 1975;36:438-44.
30. Chi arami da SA, Goldman MA, Zema MJ, Pizzarello RA, Goldberg HM. Real-time cross-sectional échocardiographie diagnosis of infiltrative cardiomyopathy due to amyloid. J Clin Ultrasound 1980;8:58- 62.
31. Child JS, Levisman JA, Abbasi AS, MacAlphin RN. Echocardiographie manifestations of infiltrative cardiomyopathy. A report of seven cases due to amyloid. Chest 1976;70:726-31.
32. Child JS, Krivokapich J, Abbasi AS. Increased right ventricular wall thickness on echocardiography in amyloid infiltrative cardiomyopathy. Am J Cardiol 1979;44:1391-5.
33. Clarke JM, Hamer J, Shelton JR, Taylor S, Yenning GR. The rhythm of the normal human heart. Lancet 1976;2:508-12.
34. Cohen AS, Calkins E. Electron microscopic observations on a fibrous component in amyloid of diverse origins. Nature 1959;183:1202-3.
35. Cohen AS. Amyloidosis. N Engl J Med 1967;277:522-30, 574-83, 628- 38.
36. Cohen AS. An update of clinical, pathologic, and biochemical aspects of amyloidosis. Int J Dermatol 1981;20:515-30.
37. Costa PP, Figueira AS, Bravo FR. Amyloid fibril protein related to prealbumin in familial amyloidotic polyneuropathy. Proc Natl Acad Sci USA 1978;75:4499-503.
38. Davies MJ. Pathology of conducting tissue of the heart. London: Butterworths, 1971.
39. Dyckner T. Interrelations between magnesium, potassium and cardiac arrhythmias. Stockholm/Umeå: Departments of Medicine, Karolinska Institutet at Serafimerlasarettet/University Hospital Umeå, Stockholm 1979. Dissertation.
40. Eanes ED, Glenner GG. X-ray diffraction studies on amyloid filaments. J Hi stochern Cytochem 1968;16:673-7.
41. Engelmeier RS, O'Connell JB, Subramanian R. Cardiac amyloidosis presenting as severe mitral regurgitation. Int J Cardiol 1983;4: 325-7.
42. Falk RH, Lee VW, Rubi now A, Hood WB, Cohen AS. Sensitivity of tech- netium-99m-pyrophosphate scintigraphy in diagnosing cardiac amyloidosis. Am J Cardiol 1983;51:826-30.
32
43. Feigenbaum H. Echocardiography. 3rd ed. Philadelphia: Lea and Febiger, 1981:549-63.
44. Frederiksen T, Gtftzsche H, Harboe N, Kiær W, Mellemgaard K. Familial primary amyloidosis with severe amyloid heart disease. Am J Med 1962;33:328-48.
45. de Freitas AF, Barbedo A. Conduction disturbances in 190 patients with familial amyloidotic polyneuropathy (Andrade's type). Avd Cardiol 1978;21:206-9.
46. Furman S, Whitman R. Cardiac pacing and pacemakers IX. Statistical analysis of pacemaker data. Am Heart J 1978;95:115-25.
47. Garcia R, Saeed SM. Amyloidosis: Cardiovascular manifestations in five illustrative cases. Arch Intern Med 1968;121:259-66.
48. Giles TD, Leon-Galindo J, Burch GE. Echocardiographie findings in amyloid cardiomyopathy. South Med J 1978;71:1393-6.
49. Glenner GG, Ignaczak TF, Page DL. The inherited systemic amyloidoses and localized amyloid deposits. In: Stanbury JB, Wyngaarden JB, Fredrickson DF, eds. Metabolic basis of inherited disease. 4th ed. New York:McGraw-Hill, 1978:1308-39.
50. Glenner GG. Amyloid deposits and amyloidosis. The beta-fibrilloses. N Engl J Med 1980;302:1283-92, 1333-43.
51. Gray LW, Duca PR, Chung EK. Sick sinus syndrome due to cardiac amyloidosis. Cardiology 1978;63:212-19.
52. Gudmundsson G, Hallgrimsson J, Jonasson TA, Bjarnason 0. Hereditary cerebral haemorrhage with amyloidosis. Brain 1972;95:387-404.
53. Gunnar RM, Dillon RF, Wallyn RJ, Elisberg El. The physiologic and clinical similarity between primary amyloid of the heart and constrictive pericarditis. Circulation 1955;12:827-32.
54. Hedner P, Rausing A, Steen K, Torp A. Diagnosis of cardiac amyloidosis by myocardial biopsy. Acta Med Scand 1975;198:525-8.
55. Henry WL, DeMaria A, Gramiak R et al. Report of the American society of echocardiography committee on nomenclature and standards in two-dimensional echocardiography. Circulation 1980;62:212-7.
56. Hinkle Jr LE, Carver ST, Stevens M. The frequency of asymptomatic disturbances of cardiac rhythm and conduction in middle-aged men. Am J Cardiol 1969;24:629-50.
57. Hodkinson HM, Pomerance A. The clinical significance of senile cardiac amyloidosis: A prospective clinico-pathological study. Q J Med 1977;46:381-7.

33
58. Hofer P-Å, Andersson R. Postmortem findings in primary familial amyloidosis with polyneuropathy. A study based on six cases from northern Sweden. Acta Pathol Microbiol Scand Sect A 1975;83:309-22.
59. von Hoyningen-Huene CBJ. Systemic amyloidosis presenting as constrictive pericarditis. A case studied with cardiac catheterization. Am Heart J 1964;67:290-4.
60. Hudson REB. The human conducting-system and its examination. J Clin Pathol 1963;16:492-8.
61. Isokane N, Fukushima N, Miyazaki T, Dohi I. A case of sick sinus syndrome in primary systemic amyloidosis. J Electrocardiol 1978;11 : 191-6.
62. James TN. Pathology of the cardiac conduction system in amyloidosis. Ann Intern Med 1966;65:28-36.
63. Kaplan BM, Langendorf R, Lev M, Pick A. Tachycardia-bradycardia syndrome (so-called "sick sinus syndrome"). Pathology, mechanisms and treatment. Am J Cardiol 1973;31:497-508.
64. Kula RW, Engel WK, Line BR. Scanning for soft-tissue amyloid. Lancet 1977;1:92-3.
65. Kyle RA, Bayrd ED. Amyloidosis: Review of 236 cases. Medicine 1975; 54:271-99.
66. Lee VW, Caldarone AG, Falk RH, Rubi now A, Cohen AS. Amyloidosis of heart and liver: Comparison of Tc-99m pyrophosphate and Tc-99m methylene diphosphonate for detection. Radiology 1983;148:239-42.
67. Lindberg J. Rupture of the right ventricle of the heart in a case of advanced heart amyloidosis. Acta Pathol Microbiol Scand Sect A 1971;79:53-4.
68. Mahloudji M, Teasdall RD, Adamkiewicz JJ, Hartmann WH, Lambird PA, McKusick VA. The genetic amyloidoses. With particular reference to hereditary neuropathic amyloidosis, type II (Indiana or Rukavina type). Medicine 1969;48:1-37.
69. Meaney E, Shabetai R, Bhargava V et al. Cardiac amyloidosis, constrictive pericarditis and restrictive cardiomyopathy. Am J Cardiol 1976;38:547-56.
70. Meretoja J. Familial systemic paramyloidosis with lattice dystrophy of the cornea, progressive cranial neuropathy, skin changes and various internal symptoms: A previously unrecognized heritable syndrome. Ann Clin Res 1969;1:314-24.

34
71. Mückle TJ, Wells M. Urticaria, deafness and amyloidosis: A new heredo-familial syndrome. Q J Med 1962;31:235-48.
72. Nygårds M-E, Ahrén T, Tranesjö J, Wigertz 0. A computer program for analysis of long-term ECG recordings. Computers in Cardiology. Long Beach, California: IEEE Computer Society, 1979:429-32.
73. Olofsson BO, Andersson R, Furberg B. Atrioventricular and intraventricular conduction in familial amyloidosis with polyneuropathy. Acta Med Scand 1980;208:77-80.
74. Olofsson BO. Pulmonary function in familial amyloidosis with polyneuropathy. Acta Med Scand 1981;209:379-84.
75. Olofsson B0, Bjerle P, Österman G. Hemodynamic and angiocardiographic observations in familial amyloidosis with polyneuropathy. Acta Med Scand 1982;212:77-81.
76. Olofsson B-0. Cardio-pulmonary function in familial amyloidosis with polyneuropathy. A clinical study of cases from northern Sweden. Umeå University Medical Dissertations, New Series No 86, ISSN 0346-6612, 1982.
77. Olofsson B-0, Eriksson P, Eriksson A. The sick sinus syndrome in familial amyloidosis with polyneuropathy. Int J Cardiol 1983;4: 71-3.
78. Olofsson B0. Cardiac involvement in familial amyloidosis with polyneuropathy. Int J Cardiol 1983;4:379-82.
79. Ostertag B. Demonstration einer eigenartigen familiären "Paraamy- 1oidose". Zentral bl Al lg Pathol 1932;56:253-4.
80. Parkey RW, Bonte FJ, Meyer SL, et al. A new method for radionuclide imaging of acute myocardial infarction in humans. Circulation 1974; 50:540-6.
81. Piérard L, Verheugt FWA, Meitzer RS, Roelandt J. Echocardiographie aspects of cardiac amyloidosis. Acta Cardiol 1981;36:455-61.
82. Puchtier H, Sweat F, Levine M. On the binding of Congo red by amyloid. J Hi stochern Cytochem 1962;10:355-64.
83. Reimann HA, Koucky RF, Eklund CM. Primary amyloidosis limited to tissue of mesodermal origin. Am J Pathol 1935;11:977-88.
84. Ri dol fi RL, Buikley BH, Hutchins GM. The conduction system in cardiac amyloidosis. Clinical and pathologic features of 23 patients. Am J Med 1977;62:677-86.

35
85. Roberts WC, Waller BF. Cardiac amyloidosis causing cardiac dysfunction: Analysis of 54 necropsy patients. Am J Cardiol 1983;52: 137-46.
86. Rubinow A, Skinner M, Cohen AS. Digoxin sensitivity in amyloid cardiomyopathy. Circulation 1981;63:1285-8.
87. Rukavina JG, Block WD, Jackson CE, Falls HF, Carey JH, Curtis AC. Primary systemic amyloidosis: A review and an experimental, genetic, and clinical study of 29 cases with particular emphasis on the familial form. Medicine 1956;35:239-334.
88. Saffitz JE, Sazama K, Roberts WC. Amyloidosis limited to small arteries causing angina pectoris and sudden death. Am J Cardiol 1983:51:1234-5.
89. Sahn DJ, DeMaria A, Kisslo J, Weyman A. Recommendations regarding quantitation in m-mode echocardiography : Results of a survey of échocardiographie measurements. Circulation 1978;58:1072-83.
90. Sawayama T, Kurihara T, Araki S. Noninvasive cardiovascular findings in familial amyloid polyneuropathy. Br Heart J 1978;40:1288- 92.
91. Schiff S, Bateman T, Moffatt R, Davidson R, Berman D. Diagnostic considerations in cardiomyopathy: Unique scintigraphic pattern of diffuse biventricular technetium-99m-pyrophosphate uptake in amyloid heart disease. Am Heart J 1982;103:562-3.
92. Schroeder JS, Billingham ME, Rider AK. Cardiac amyloidosis. Diagnosis by transvenous endomyocardial biopsy. Am J Med 1975;59:269- 73.
93. Siqueira-Filho AG, Cunha CLP, Tajik AJ, Seward JB, Schattenberg TT, Giuliani ER. M-mode and two-dimensional échocardiographie features in cardiac amyloidosis. Circulation 1981;63:188-96.
94. Skinner M, Cohen AS. The prealbumin nature of the amyloid protein in familial amyloid polyneuropathy (FAP)-Swedish variety. Biochem Biophys Res Commun 1981;99:1326-32.
95. Smith RRL, Hutchins GM. Ischemic heart disease secondary to amyloidosis of intramyocardial arteries. Am J Cardiol 1979;44:413-7.
96. Sobol SM, Brown JM, Bunker SR, Patel J, Lull RJ. Noninvasive diagnosis of cardiac amyloidosis by technetium-99m-pyrophosphate myocardial scintigraphy. Am Heart J 1982;103:563-6.

36
97. Sohar E, Gafni J, Präs M, Heller H. Familial Mediterranean fever. A survey of 470 cases and review of the literature. Am J Med 1967; 43:227-53.
98. Steen L. Gastrointestinal involvement in familial amyloidosis with polyneuropathy. A clinical study. Umeå University Medical Dissertations, New Series No 93, ISSN 0346-6612, 1983.
99. Swanton RH, Brooksby IAB, Davies MJ, Col tart DJ, Jenkins BS, Webb- Peploe MM. Systolic and diastolic ventricular function in cardiac amyloidosis. Studies in six cases diagnosed with endomyocardial biopsy. Am J Cardiol 1977;39:658-64.
100. Thomas PK. Genetic factors in amyloidosis. J Med Genet 1975;12:317-26.
101. Tonkin AM, Tornos P, Heddle WF, Rapp H. Autonomic effects on the human cardiac conduction system. Evaluation by intracardiac elec-
techniques. Br Heart Jtrocardiography1980;44:168-74.
102. Westermark P, Johansson B/, Natvig JB. Senile cardiac amyloidosis: Evidence of two different amyloid substances in the ageing heart. Scand J Immunol 1979;10:303-8.
103. WH0/ISFC Task Force. Definition of terms related to cardiac rhythm. Am Heart J 1978;95:796-806.
104. WH0/ISFC Task Force. Definition and classification of cardiomyopathies. Br Heart J 1980; 44: 672-3.
105. Wizenberg TA, Muz J, Sohn YH, Samlowksi W, Weissler AM. Value of positive myocardial technetium-99m-pyrophosphate scintigraphy in the noninvasi ve diagnosis of cardiac amyloidosis. Am Heart J 1982; 103:468-73.