cancer immunotherapy: promises and challenges - … immunotherapy: promises and challenges david b....
TRANSCRIPT

10/30/2017
1
Cancer Immunotherapy:
Promises and Challenges
David B. Page, MD
Medical Oncology
PMG East Hematology & Oncology
Earle A. Chiles Research Institute
Portland, Oregon
Disclosures
Consulting: Celldex, Nektar, Nanostring, Endopredict
Research: IRX Therapeutics, Merck, BMS, Medimmune

10/30/2017
2
The Immune System to treat cancer?
The Immune System to treat cancer?

10/30/2017
3
The Immune System to treat cancer?
Adams S, et al, JCO 2014
Stage I-III Triple Negative Breast Cancers
The Immune System to treat cancer?
Adams S, et al, JCO 2014
Stage I-III Triple Negative Breast Cancers
0% Lymphocytes
70% 5-yr Survival
50% Lymphocytes
90% 5-yr Survival

10/30/2017
4
Agenda
• FDA approved immunotherapies & how they work
• Toxicity management of immunotherapy
• Future directions
Selected Immunotherapy Approvals
1998 2010 2011 2015
Trastuzumab
IL-2
Ipilimumab
Sipuleucel-T T-VEC
2016
Blinatumomab
2014
Nivolumab Ipi+Nivo
“Immune checkpoint antibodies”
2017
CAR T-cell

10/30/2017
5
Classes of Immunotherapy: Antibody Therapy
Example: Trastuzumab
Metastatic
• Increase median survival from
20.3mo to 25.1mo
Early Stage
• Reduce recurrence rate by 36%
Hudis C, et al, NEJM 2007
ADCC
Wikipedia, ADCC, accessed 5/29/2017
Rituximab Daratumumab Cetuximab
10/30/2017
6
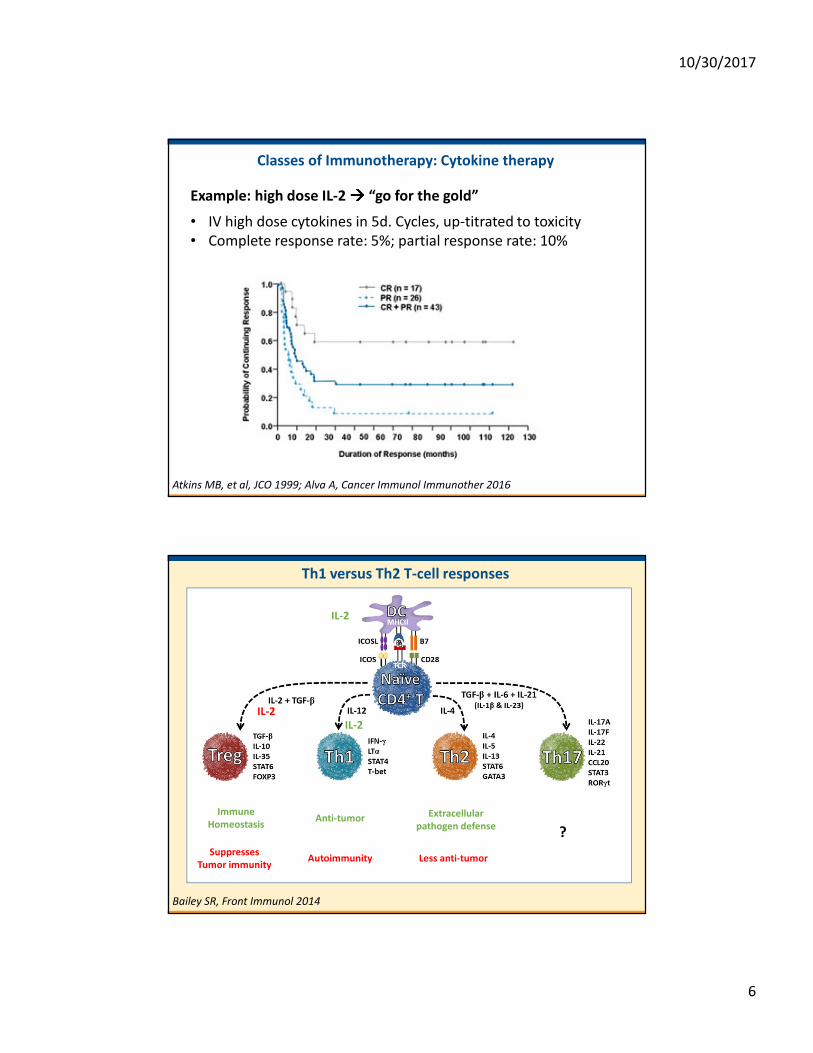
Classes of Immunotherapy: Cytokine therapy
Example: high dose IL-2 ���� “go for the gold”
• IV high dose cytokines in 5d. Cycles, up-titrated to toxicity
• Complete response rate: 5%; partial response rate: 10%
Atkins MB, et al, JCO 1999; Alva A, Cancer Immunol Immunother 2016
Th1 versus Th2 T-cell responses
Bailey SR, Front Immunol 2014
Suppresses
Tumor immunity
Immune
HomeostasisAnti-tumor
Autoimmunity
Extracellular
pathogen defense
Less anti-tumor
?
IL-2
IL-2
IL-2

10/30/2017
7
Classes of Immunotherapy: Vaccine Therapy
Example: Sipuleucel-T
• Metastatic Prostate Cancer
• Survival: 25.8 v. 21.7mo
• No change in tumor growth
• $100k = 259k/life year?
Di Lorenzo G, et al, Nature Reviews in Clinical Onc 2011; Kantoff PW et al, NEJM 2010
Vaccine = exogenous tumor
antigen
• Peptide / carbohydrate
• DNA/RNA, vector
• Cellular
Antigen Presentation
Wikipedia, Antigen Presentation, Accessed 5/29/2017

10/30/2017
8
Classes of Immunotherapy: Antibody conjugates
Example: Blinatumumab
• ALL (B-cell leukemia)
• Survival 7.7mo, v 4.0mo for chemotherapy
• May also eradicate minimal residual disease
Kantarjian H, et al. NEJM 2017
Leukemia
(ALL)
CD19 Cytotoxic
T-cell
CD3
Genetic Engineering of Antibodies
Bassan R, et al, Blood 2012
Bispecific antibody
BITE “Bispecific T-cell engager”
Blinatumumab
Antibody drug conjugate
T-DM-1 = trastuzumab + chemo

10/30/2017
9
Classes of Immunotherapy: Immune Checkpoint Antibodies
Larkin J et al, NEJM 2015; Littleton MJ et al, JCO 2000
TemozolamideDTIC
Classes of Immunotherapy: Immune Checkpoint Antibodies
Larkin J et al, NEJM 2015; Littleton MJ et al, JCO 2000
TemozolamideDTIC

10/30/2017
10
Immune Checkpoints
Page DB et al, Oncologist 2016
Classes of Immunotherapy: Immune Checkpoint Antibodies
Melanoma
NSCLC
RCC
Bladder Ca
Hodgkin’s Lymphoma
Merkel’s Cell
HEENT Ca
MSI-High Colorectal

10/30/2017
11
Classes of Immunotherapy: Oncolytic Viruses
Example: T-VEC
• Metastatic Melanoma
• Survival: 23.3 v. 18.9mo
• Responses in injected, non-
injected, and viscera
• Viral vector (HSV1)
• Replicate and lyse injected
tumor
• Manipulate genome to
enhance effect: - suppressive
genes; + GM-CSF
Andtbacka R, et al, JCO 2015; Amgen website, accessed 5/29/2017
CAR T-cell Therapy: Tisagenlecleucel
Maude S, et al. NEJM 2014
T-cell
ALL cell
CD19
T-cell
ALL cell
CD19
Pediatric ALL Response
10/30/2017
12
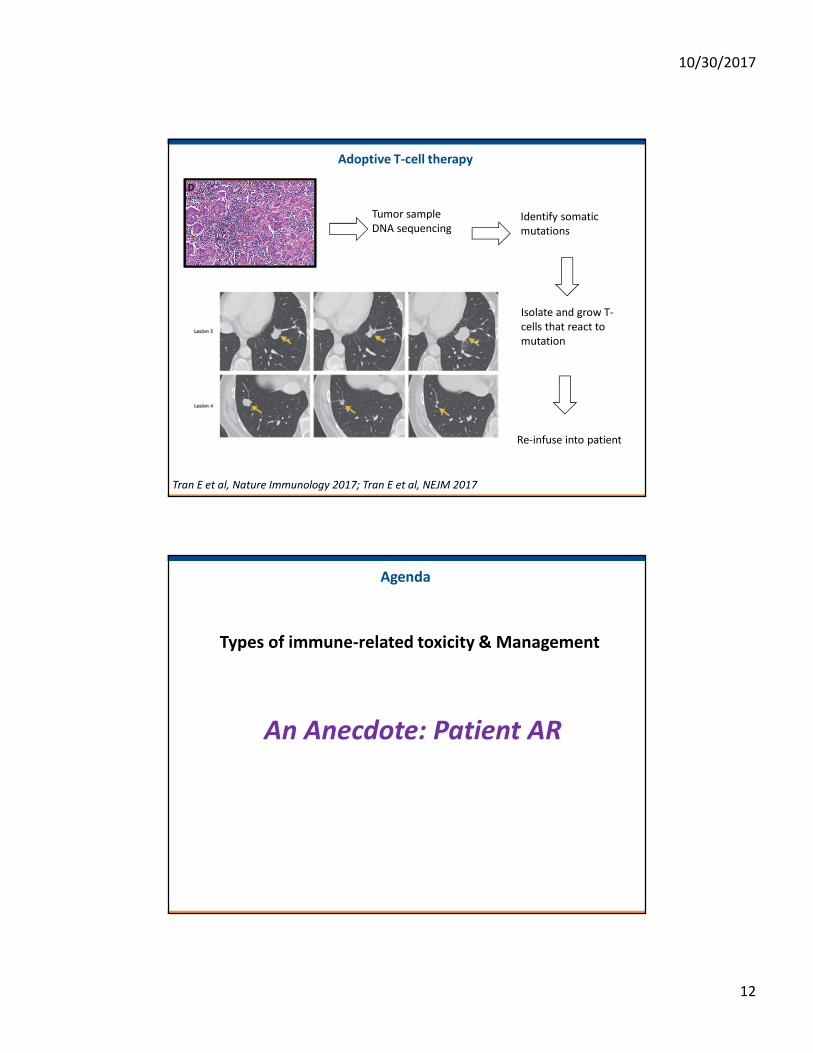
Adoptive T-cell therapy
Tumor sample
DNA sequencingIdentify somatic
mutations
Isolate and grow T-
cells that react to
mutation
Re-infuse into patient
Tran E et al, Nature Immunology 2017; Tran E et al, NEJM 2017
Agenda
Types of immune-related toxicity & Management
An Anecdote: Patient AR
10/30/2017
13
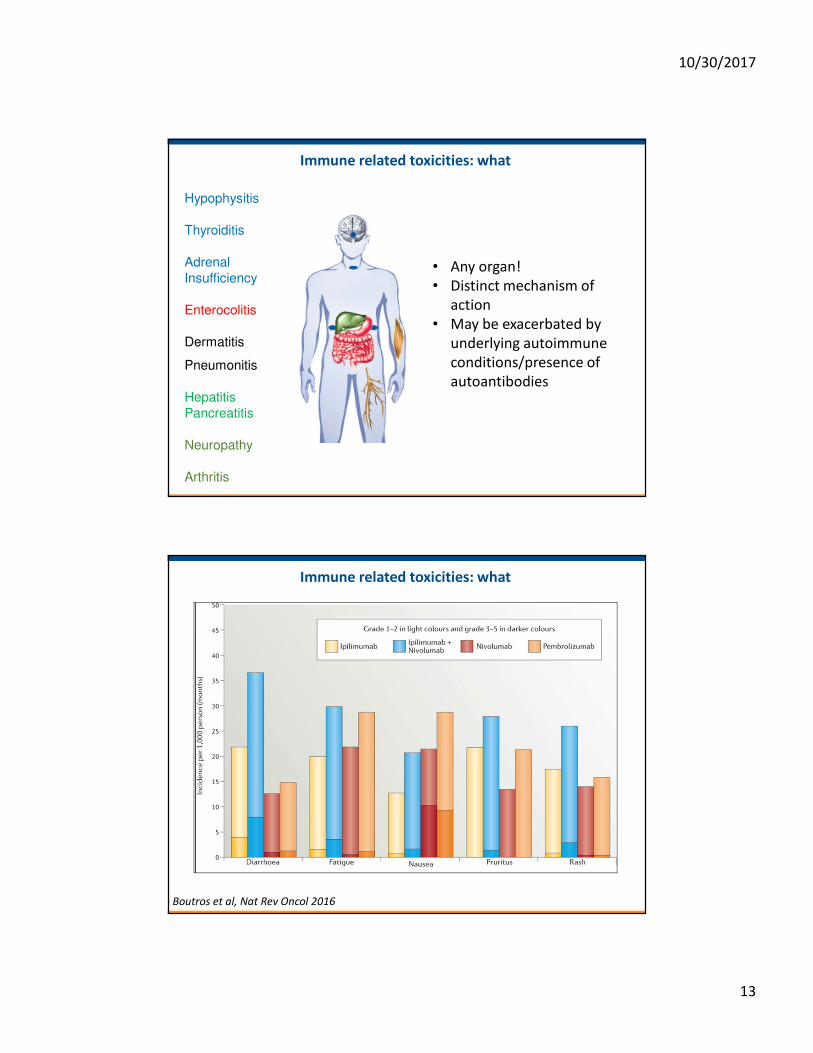
Immune related toxicities: what
Hypophysitis
Thyroiditis
Adrenal
Insufficiency
Enterocolitis
Dermatitis
Pneumonitis
Hepatitis
Pancreatitis
Neuropathy
Arthritis
• Any organ!
• Distinct mechanism of
action
• May be exacerbated by
underlying autoimmune
conditions/presence of
autoantibodies
Boutros et al, Nat Rev Oncol 2016
Immune related toxicities: what

10/30/2017
14
Boutros et al, Nat Rev Oncol 2016
Immune related toxicities: what
Immune related toxicities: when?
Weber et al, JCO 2012; Antonia et al, ESMO 2015

10/30/2017
15
Immune related toxicities: general management
Principles for the generalist
1) Always suspect immune-
related toxicity
2) Rule out common causes
3) Seek confirmatory diagnosis
4) Grade toxicity and utilize
algorithms
5) Oncology consult ���� clinical
trials implications
Grade 1Grade 1Grade 1Grade 1: - Supportive care
- Consider drug withhold
Grade 2Grade 2Grade 2Grade 2:
- Withhold drug.
- Low-dose corticosteroids
(prednisone 0.5-1mg/kg/day or equivalent).
- Consider re-dose if toxicity resolves to
≤ Grade 1.
Grade 3Grade 3Grade 3Grade 3----4444: - Discontinue drug.
- High-dose corticosteroids
- (prednisone 1-2mg/kg/day or equivalent)
tapered over ≥ 1 month once toxicity
resolves to ≤ Grade 1.
Immune related toxicities: colitis
Diagnostic WorkupDiagnostic WorkupDiagnostic WorkupDiagnostic Workup
- Rule out alternative diagnosis:
C.difficile, other GI infections
- Distinguish between diarrhea and
colitis
- Consider invasive testing with
colonoscopy
ManagementManagementManagementManagement
- Low threshold for starting
corticosteroids
- No benefit for corticosteroid pre-
treatment (budesonide)
- Colitis that is slow to
improve/refractory to steroids: treat
with anti-TNF
- Infliximab 5mg once or twice every
14 days
10/30/2017
16
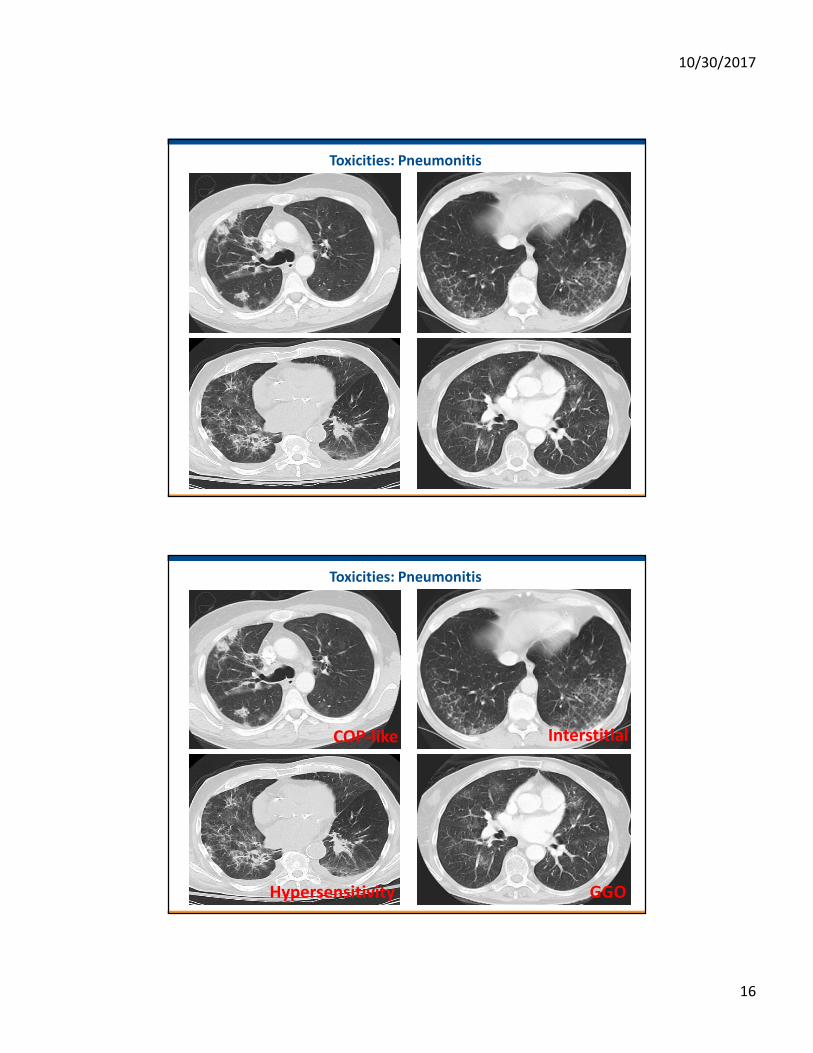
Toxicities: Pneumonitis
Toxicities: Pneumonitis
Hypersensitivity
COP-like
GGO
Interstitial

10/30/2017
17
Toxicities: Pneumonitis
Naidoo et al, JCO 2016
Pneumonitis Management Algorithm
Grade Investigations Management Follow-up
1Asymptomatic,
Radiologic changes
only
2Mild/moderate new
symptoms
3-4Severe/life-threatening
new symptoms or
worsening hypoxia
• Radiologic
imaging
(High resolution
CT chest)
• Microbial
assessment where
necessary
• Consider
Pulmonary/Infecti
ous Diseases
Consults and
Bronchoscopy
• Withhold immunotherapy
• Monitor for symptoms daily
• Oral prednisone 1mg/kg/day or
equivalent
• Continue immunotherapy
• Monitor for symptoms every 3
days
• Discontinue immunotherapy
• Hospitalization
• IV methylprednisolone
2-4mg/kg/day or equivalent
• Prophylactic antibiotics
• Repeat CT every cycle
• If develops symptoms, treat as
higher grade
• If improves to ≤Grade 1 within 3
days of supportive care, resume
immunotherapy at next dose
• If persistent beyond 3 days,
discontinue immunotherapy
• After symptoms improve, taper
steroids over ≥1 month
• After symptoms improve to
≤Grade 1 or baseline, taper
steroids over ≥6 weeks
• If worsens in 48 hours consider
additional immunosuppression
(infliximab, cyclophosphamide,
mycophenolate mofetil)
Naidoo et al, JCO 2016

10/30/2017
18
Profound Fatigue
Think endocrine!
PituitaryHypophysitis
ThyroidThyroiditis
AdrenalInsufficiency
Consider MRI pituitary protocol
TSH, FT4 +/- T3
Cortisol, ACTH Stim
***Check serially!
Treatment:
Hormone Replacement
Endocrinology Consultation
Profound Fatigue
Think endocrine!
PituitaryHypophysitis
ThyroidThyroiditis
AdrenalInsufficiency
Consider MRI pituitary protocol
Serial TSH, FT4 +/- T3
Cortisol, ACTH Stim
***Check serially!

10/30/2017
19
Toxicities: Rash
Maculopapular Papulopustular Sweet’s syndrome
Lichenoid DermatitisBullous Pemphigoid
Toxicities: Rash
Maculopapular Papulopustular Sweet’s syndrome
Lichenoid DermatitisBullous Pemphigoid
All of the above!

10/30/2017
20
Toxicities: Rash
Maculopapular Papulopustular
Bullous Pemphigoid
20-40% Patients with anti-PD-1
Rarely serious, <5% Tx d/c rate
Management:
• Mild, <10% BSA: topical steroid
• 10-30% BSA: oral steroid, hold Tx
• >30% BSA or severe� derm
consult
Antibody mediated (against BP180)
Also found on melanomas
• Presentation
- Mainly asymptomatic elevations in AST/ALT
- 10% with anti-CTLA4 mAb
- <5% with anti-PD-1/PD-L1 mAb
- Grade 3+ events: 1-2%
- Increased toxicity with combinations (vemurafenib)
• Management
- Minimize alcohol intake
- Oral steroid taper of at least 3 weeks
- *No infliximab* (FDA Blackbox warning)
- Mycophenolate 500mg-1000mg bid
Toxicities: Immune Related Hepatitis

10/30/2017
21
Can you treat a patient with prior autoimmune conditions?
Yes!
Anti-PD-1 JHU cohort:
52 patients with previous autoimmune disease
• 38% had mild flare of prior condition;
• 4% required discontinuation;
• 29% developed other irAEs, 8% requiring discontinuation
Can you treat a patient with prior autoimmune conditions?

10/30/2017
22
Agenda
Immune related response criteria & implications
Nishino M et al, Nature Reviews Clin Oncology 2017
Agenda: Future Directions
IL-2 + SBRT
Pegylated IL-2
Intramammary IRX
Anti-OX40
Anti-PD-1 + Chemotherapy
Anti-TGFb+
Radiotherapy

10/30/2017
23
Thank you!