breast biopsy: opportunities for an improved diagnosis
TRANSCRIPT

BREAST BIOPSY:
OPPORTUNITIES FOR ANIMPROVED DIAGNOSIS

This supplement is sponsored by Intact Medical Corporation.Founded in 1998 and based in Natick, Massachusetts, Intact Medical Corporation is a privately-held company focused on the design, develop-ment and marketing of innovative, minimally invasive systems for the volumetric excision of tissue for diagnostic and therapeutic applicationsin select cancer markets. The company's lead product, the Intact™ Breast Lesion Excision System, received market clearance from the Foodand Drug Administration in June 2001. Initial products are targeted at breast biopsy and the excision of high-risk lesions, potentially obviatingthe need for open surgical excisions. For more details on the company’s product family and services, visit www.intactmedical.com.
Faculty DisclosuresThe contents of this supplement were based on comments solicited from the Faculty attending a roundtable discussion sponsored by Intact Medical Corporation, a privately-held company focused on the design, development, and marketing of innovative, minimally invasive systems for the volumetric excision of tissue for diagnostic and therapeutic applications in select cancer markets.
The faculty participants received honoraria for their attendance at this meeting. The following individual has a financial interest, arrangement, or affiliation with the manufacturer of the products discussed in this supplement: Larry K. Killebrew, MD.
The following individuals are on the Scientific Advisory Board for Intact Medical Corporation: Edward P. Dalton, MD; Thomas B. Julian, MD; Larry K. Killebrew, MD; Michael D. Lagios, MD; William R. Poller, MD; Lowell W. Rogers, MD; Jean F. Simpson, MD; Pat W. Whitworth, MD.
Intact™ Breast Lesion Excision System is a trademark of Intact Medical Corporation, Natick, MA. All other trademarks are property of their respective holders.
TABLE OF CONTENTS
1 INTRODUCTION
2 BREAST BIOPSY: CURRENT STATE
2 Historical Perspective
3 Limitations of Current Methods
5 NEW TECHNOLOGICAL ADVANCES
5 Benefits of Minimally-Invasive Procedures
8 Complete Removal of Masses or Calcifications
9 PATIENT SELECTION ISSUES
9 CASE STUDY 1: Radial Scar with ALH
10 CASE STUDY 2: Atypical Ductal Hyperplasia
10 CASE STUDY 3: Intraductal Papilloma
11 CASE STUDY 4: Poor Surgical Risk
11 CASE STUDY 5: ADH and Radial Scar
12 CHALLENGES FOR THE FUTURE
12 Towards Evidence-Based Medicine
13 REFERENCES
“A major goal of modernbreast medicine is to minimize the number ofpatients who undergo open surgical biopsies for diagnosis.”International Consensus Conference II. Silverstein MJ, et al. Image-detected Breast Cancer: State of the Art Diagnosis and Treatment. J Am Coll Surg. 2005:201;586-597

BREAST BIOPSY is a complex,evolving, and controversial topic. In the last 30 years, there has been agradual evolution in the managementof breast disease toward more conser-vative and less invasive techniques.1
Surgeons are applying advanced biopsyprocedures necessitating an adjustmentby pathologists to the receipt of speci-mens that represent these new surgicaltechniques. As breast biopsy technolo-gy evolves, it is being embraced bysome and being questioned by others.
Regardless, the goal remains the same — to minimize the number ofpatients who require open biopsy for diagnosis and to provide the mostdefinitive diagnosis with the least invasive approach.2
Statistics indicate a woman has a 1 in 8 chance of developing breast cancer in her lifetime but that more than 60% of women will develop some typeof benign breast disease.3 Screeningmammography is performed in asymp-tomatic women with the goal of dis-covering invasive breast cancer at an early, curable stage. Professionalorganizations recommend that womenaged 40 to 50 have a screening mam-mography every 1 to 2 years.4 Therewill be more than 33.5 million screen-ing mammograms performed this
and discomfort and irritation whenwearing underclothing are candidatesfor removal. The emotional traumaassociated with having a breast massalone may warrant its excision.3 Often,follow-up procedures are required toreach a definitive diagnosis. There aresituations where a percutaneous intactexcisional biopsy may be appropriateinitially and as follow-up to benignfindings on core or needle biopsy.
On January 28, 2006, a scientificadvisory board composed of radiolo-gists, pathologists, and surgeons met to discuss the current challenges indiagnosing breast disease. This discus-sion focused on the current state-of-the-art, new technological advances inbreast biopsy and the types of patientsand situations that are best served by apercutaneous intact excisional biopsy.Case studies were presented where theIntact™ Breast Lesion ExcisionSystem (BLES) was used to obtain anintact specimen. This supplement sum-marizes the discussions that occurredduring this roundtable meeting.
year, of which 5% to 10% will beabnormal.5 An estimated 1.4 millionbreast biopsies will also be performedand the majority (80%) of these lesionswill prove to be benign.6,7
Mammographic screening now identifies breast lesions that are toosmall to palpate. There is an increasing trend for patients to present withsmaller and smaller lesions as imagingimproves and screening becomes moreroutine.6 Using samples from percuta-neous, large-core, needle biopsy,pathologists can diagnose most benign lesions accurately.8
The most common and worrisomemammographic findings that requirefurther evaluation are masses and calcifications. The sheer number ofpossible diagnoses makes the patholo-gist’s job very complex. Cancers mustbe excised but benign tumors may ormay not require removal, sparing thesewomen considerable trauma andexpense.8 Benign lesions that becomesymptomatic causing pain, uncomfort-able feelings of weight and asymmetry,
INTRODUCTION
“With respect to breast biopsy,we should be moving well awayfrom reports of a suspiciouslesion to a more definitive diagnosis so we can structure anappropriate operative procedureor surgical avoidance altogether.We need to minimize the need totake a majority of patients to the operating room just for diagnostic purposes. The O.R. should be reserved for therapy.”Thomas B. Julian, MD, FACS Allegheny General Hospital
1
FIGURE 1. Gross pathology of core biopsy segments obtained with a 14-gauge percutaneouscore biopsy needle, which will require evaluation of multiple histological levels to determine an accurate diagnosis.

BREAST BIOPSY: CURRENT STATE
surgical biopsy is reserved for instanceswhen a large enough sample of tissue is not obtainable with percutaneousmethods to assess prognostic and predictive factors.
The trend in breast biopsy is shiftingtowards minimally-invasive techniques.The 1990’s brought numerous techno-logical advances including core needlebiopsy (CNB) either automatedspring-loaded or vacuum-assisted, and newer percutaneous intact exci-sional biopsy devices that excise intactlesions (see Table 1).
These minimally-invasive techniquesresulted in: smaller histologic samples,quick turnaround times, less morbidity,minimal to no scarring, decreased cost for a definitive diagnosis, more
HISTORICAL PERSPECTIVE
THE ADVENT OF dedicated mam-mography imaging occurred in the1960’s and has remained the mainstayfor breast disease screening.9 Biopsywas, and still is, the confirmatorymethod of choice. Improvements inthese two technologies have increasedsurvival rates dramatically for womenwith malignant disease. The survivalrate for cancers detected early, measur-ing less than 1cm, is 90% and 80% forthose between 1 and 2 cm.9
Prior to the introduction of image-guided needle and core biopsy, opensurgical biopsy was the only option.Open surgical biopsy typically yieldsan intact specimen of the entire mam-mographic lesion and surroundingbreast tissue. It offers the possibility of removing the entire lesion with a clear margin. A surgical biopsy also enables a more comprehensivepathological review.
Open biopsy methods require a skinincision, suture and anesthesia, and are associated with significant cosmeticdefects and morbidity.10,11 The disad-vantages of this invasive techniqueinclude postoperative hematoma,infection, and scarring which may have an effect on future mammograph-ic imaging. Today the role of open
“There is continuing opportunity to educate all of our pathology colleagueswhen defining the gray zone between ADH and proliferative disease. I think that extent criteria are compromised with thesmaller core biopsies.”Lowell W. Rogers, MD Long Beach Memorial Medical Center
DEFINITIONS:
Core Needle Biopsy—a biopsy method used to obtain tissue cylinders from a target organ, via a large bore needle, for paraffin embedding and histological processing. This technique can be performed with and withoutvacuum-assisted sources. Core needle biopsy products include Mammotome®
(Ethicon Endo-Surgery), Vacora® (C.R. Bard, Inc.), ATEC® (Suros SurgicalSystems), EnCore™ (SenoRx) and Cassi™ (Sanarus).
Percutaneous Intact Excisional Biopsy—a biopsy method used to obtain large (10 mm to 20 mm) intact samples for paraffin embedding and histological processing and also having the potential to completely excise the lesion. Products include Site Select® (Site Select Medical Technologies),Encapsule™ (Rubicor) and the Intact™ Breast Lesion Excision System (Intact Medical Corporation).
Underestimates—The rate at which findings from biopsy specimens miscalcu-late the severity of a breast lesion, measured against open surgical excision —the gold standard. For example, ADH underestimates are calculated at the rateat which the histopathological diagnosis of the stereotactic biopsy specimenwas atypical ductal hyperplasia and the histopathological diagnosis of the subsequent surgical excision was either ductal carcinoma in situ (DCIS) orinfiltrating cancer. Similarly, DCIS underestimates are the rate at which thehistopathological diagnosis of the stereotactic biopsy specimen was DCIS and the histopathological diagnosis of the subsequent surgical excision wasinfiltrating cancer.14
Concordance—an agreement in findings that support the accuracy of a particular diagnosis; more specifically, the level or percent agreement betweenmammographic findings and pathological reports or between the results of two comparative biopsy procedures and histopathological findings from surgical specimens.
TABLE 1. Types of Biopsy Techniques
■ Open Surgical Biopsy
■ Percutaneous Methods
• Fine-needle aspiration biopsy
• Core needle biopsy
-Automated spring-loaded core needle
-Vacuum-assisted core needle
• Percutaneous intact excisional biopsy
definitive targeting, minimal risk ofhematoma (vs. surgery), increased sampling accuracy, and the avoidanceof, and costs for, operating room procedures.12,13
2

Although mammographic-pathologiccorrelation is required for all image-directed biopsies, establishing concor-dance is more difficult when the target
LIMITATIONS OF CURRENT METHODS
FINE NEEDLE aspiration, oftenused, has been replaced with vacuum-assisted core biopsy and is nowreserved for a limited number of casesdue to its unreliability in making adefinitive diagnosis of benignity.7 Corebiopsy allows pathologists to accuratelydiagnose and classify carcinomas aswell as establish hormone receptorsand other biomarker status.15 A majordiagnostic limitation of core needlebiopsy is its inability to definitivelyestablish a diagnosis when it reveals a high-risk lesion such as ADH,ALH/LCIS, radial scar, etc. Such biopsies inherently do not permit evaluation of the spatial relationships,extent and margins of the lesionbecause it is sampled in multiple coreswhich have an unknown relationship to one another (See Table 2).
The multiple cores obtained fromthe target make evaluation of marginsimpossible, and the inability to evalu-ate the spatial relationships of the fociof high-risk lesions within the coresmakes decisions about the likelihood of a complete excision or diagnosticupgrade speculative at best.
is disrupted by the biopsy procedurerather than removed intact as in most surgical needle localizations and percutaneous intact devices.
“There are limitations with thecurrent technologies. Most rely on multiple cores, either with a 14-gauge gun or an 11-or 8-gaugevacuum-assisted procedure. Amajor disadvantage is the loss ofspatial orientation. With multiplesamples, the pathologist is not able to establish margins to establish the extent of the disease.This makes mammographic/pathologic correlation very difficult and it requires a great deal of effort to do this.”Michael D. Lagios, MDThe Breast Cancer Consultation Service
3
FIGURE 2. Histological stain of breast tissue depicting poor margins
TABLE 2. Limitations and Problems with Core Needle Biopsies
■ Loss of spatial orientation: inability to establish margin and extent
■ Standard requirement of multiple levels to achieve adequate examination and establish concordance
■ Requirement for open excision of all high-risk lesions (ADH, ALH/LCIS, radial scars, papillary lesions, and CAPSS with hyperplastic and/or atypical features
■ Increased time and costs for pathologist and hospital: reduced net reimbursement per procedure
■ Artifacts: tissue fragmentation, epithelial implantation and benign transport which can create dangerous diagnostic dilemmas (misdiagnoses)
■ Increased difficulty in establishing mammographic-pathologic correlation and concordance

Technical Difficulties: Needle andcore biopsies can underestimate thepresence of invasive disease due tosampling error.9 Inadequate samplingand an inability to demonstrate calcifi-cations within the excised tissue mayoccur. Microclips may be required toguide further procedures; however, sig-nificant clip migration has been report-ed.7 Various step levels are required forpathological evaluation. Poor samplingtechnique and incorrect needle place-ment can lead to false positives or falsenegative results. Breast lesions diag-nosed using large-core biopsy as ADHor ductal carcinoma in situ must stillundergo surgical excision to excludethe presence of a higher grade lesionthat may have been missed because ofsampling error.16 Underestimates usingvarious vacuum-assisted devices have
BREAST BIOPSY: CURRENT STATE
“One of the distinguishing criteria between ADH and low grade DCIS is evaluating the extent of the lesion.When the lesion is disrupted, you cannot evaluate itsextent. Regardless of how well educated the pathologist,when the criterion is extent and it has been disrupted, by definition you can’t distinguish extent.”Jean F. Simpson, MD Vanderbilt University Medical Center
been reported to range from 9.5% toover 50% of cases.17,18,19 Removal ofmost of a malignant lesion by vacuum-assisted biopsy may lead to difficultiesin estimating the true size of the tumorat excision, which would be an impor-tant indicator for adjuvant therapy.20
These types of procedures can beuncomfortable to the patients. Theremay be problems with movement and positioning of patients. Vasovagal
reactions occur in 10% to 20% ofpatients. Wire positioning transectionand migration can lead to missedlesions in up to 22% of cases.7
Cost and Time Implications:Adequate examination of multiple levels of multiple fragments or coresper cassette is time-consuming, diffi-cult and expensive. Currently, themajority of core biopsies are per-formed with devices of 11-gauge orlarger, corresponding to minimal corediameters of 3 – 5 mm. In order todetect a randomly distributed high-risklesion of 1 – 1.5 mm size within such acore, multiple step-levels are requiredto adequately sample the full depth of the core. For example, an 11-gauge, 3 mm diameter core will require step-levels spaced approximately 0.4 – 0.5 mm apart. This results in 5 – 6 histologic slides, each represent-ing a specific step-level or as many as 12 slides per biopsy, requiring 2 cas-settes to process. In contrast, with per-cutaneous intact excisional biopsy, theentire imaged abnormality can beexcised intact and examined completelyin only 1 – 2 blocks without step-levels(i.e., 1 – 2 slides).
A recent cost comparison analysis of vacuum-assisted core needle to per-cutaneous intact excisional biopsy in apathology consulting service setting ispresented in Table 3. The profit mar-gin for both the physician componentand the hospital component was sub-stantially higher for the Intact BLESprocedure compared to that of conven-tional vacuum-assisted devices, whichactually lost money billing under aCPT code of 88305.
TABLE 3. Cost Comparison of Two Breast Biopsy Procedures*
Physician Component Hospital Component
$47.25 $35.70
Interpretation: 18 min.** 12 slides
Report, edit: 6 min. @ $6.00 each: $72.00
Total Time: 24 min. Report: $10.00
Total Cost: $48.00† Total Cost: $82.00
Profit/Loss: ($0.75) Profit/Loss: ($46.30)
Interpretation: 3 min.** 2 slides
Report, edit: 6 min. @ $6.00 each: $12.00
Total Time: 9 min. Report: $10.00
Total Cost: $18.00‡ Total Cost: $22.00
Profit/Loss: $29.25 Profit/Loss: $13.70
* Ductal carcinoma in situ, intermediate grade (NG II with zonal necrosis), cribiform pattern with associated microcalcifications
** Calculated as a mean of 1.5 minutes per slide
† Calculated as 18/60 x $ 120 per hour
‡ Calculated as 9/60 x $ 120 per hour
CPT Code:88305Reimbursement
Core Needle:11-gauge x two six levels
PercutaneousIntact ExcisionalBiopsy 15 mm basketone level
4

NEW TECHNOLOGICAL ADVANCES
BENEFITS OF MINIMALLY-INVASIVE PROCEDURES
THE GOAL of minimally-invasivebreast biopsy procedures is to limit the physical impact on the patients byreducing the invasiveness of the proce-dure and to reduce the proceduralcosts without sacrificing accuracy.3
Percutaneous intact excisional biopsy is a new category of devices. Theyremove a single, large block of tissue
with one smallincision. Theirmain advantage iscomplete excisionof an intact lesion.Subsequently, thepathologist canprovide a diagno-
sis, and also confirm that the entirelesion has been removed in one piece.The advantages these systems provideare precise targeting, tissue conserva-tion, and cost savings from avoidingoperating room charges. Table 4 out-lines several other benefits that radiol-ogists, surgeons, and pathologists haveidentified with percutaneous intactexcisional
biopsy, specifically from their practicalclinical experience with the IntactBreast Lesion Excision System.Although use of these types of systems is becoming more and more common, care is still required in selecting patients appropriate forthese less invasive modalities.
The Intact BLES is an innovativebreast biopsy system whereby a large, intact, specimen is removedpercutaneously under ultrasound orstereotactic image guidance. A smallincision (6 to 8 mm) is made in thebreast to accommodate the wand’sshaft; however, the tissue retrieved is far larger than this incision. TheRF energy cauterizes a channel to thelesion. When the lesion is reached,five struts open to a maximum of 20 mm to circumscribe the entirelesion. The Intact BLES captures aspecimen in one pass within 10 sec-onds or less. Since no breast tissue is removed from the channel, it collapses upon itself after removal of the lesion and heals normally. The RF energy allows easy passagethrough a variety of tissue types,including dense breast tissue. Theincision is closed with a SteriStrip™
or liquid bandage; no stitches arerequired. Experience has shown that less bleeding occurs with theIntact BLES compared to conven-tional core needle biopsies. A varietyof capture basket sizes (10 mm, 12 mm, 15 mm, 20 mm) are available.
TABLE 4. Advantages of Percutaneous Intact Excisional Biopsy Techniques
■ Preservation of spatial relationships: ability to establish margins and extent
■ No standard requirement of levels: most biopsies can be processed in 2 cassettes without levels
■ Avoidance of open excision for high-risk lesions in which pathologic and mammographic evaluation establish excision and concordance
■ Decreased cost and time required for pathologist and hospital: increased reimbursement per procedure
■ Elimination of artifact of tissue fragmentation, epithelial implantation and benign transport
■ Greater ease in establishing mammographic-pathologic correlation and concordance
“We perform about 1,500biopsies per year. Over thelast 15 years, we have usedVacora, Mammotome, Intact,and Bard systems. We nowprefer the Intact BreastLesion Excision System anduse it in about three-fourthsof our biopsy patients. I prefercatching microcalcificationswith a basket instead of a spear.”Larry K. Killebrew, MD Oklahoma Breast Care Center
FIGURE 4. Intact BLES specimen sizes
FIGURE 3.
Intact wand.
5
20 MM (actual size)
15 MM (actual size)
12 MM (actual size)
10 MM (actual size)

6
FACULTY
MODERATOR:
MICHAEL D. LAGIOS, MDThe Breast Cancer Consultation ServiceA San Francisco native, Michael D. Lagios, MD, has beenactive in clinical breast cancer research since his dischargefrom the U.S. Army Medical Corps in 1972. His group pioneered breast conservation therapy without irradiation for ductal carcinoma in situ at a small community hospital,publishing the first results in 1982, research which initiated a paradigm shift inthe treatment of that disease. Subsequently, his team developed nuclear gradingas a basic method of risk classification and refined methods of tissue processingfor both ductal carcinoma in situ and mammographically-directed biopsies. Dr. Lagios is currently Medical Director of the Breast Cancer ConsultationService in Tiburon, California, Director of Breast Services at St. Mary’s Hospital and Medical Center, and holds academic appointments at both StanfordUniversity and the University of California, San Francisco. Dr. Lagios writesextensively on breast cancer pathology and treatment, having authored or co-authored numerous original papers, editorials, clinical reviews, and chapters. Hereceived his undergraduate degree from the University of California, Berkeley,and his MD from the University of California, San Francisco School of Medicine.
PARTICIPANTS:
EDWARD P.DALTON, MD,FACSElliot Breast Health Center Edward P. Dalton, MD,maintains a clinical prac-
tice at the Elliot Breast Health Centerin Manchester, New Hampshire, wherehe specializes in breast surgery andbreast problem solving. He focuses hisclinical interests on challenges related to breast cancer diagnosis and surgery.The goal of placing screening and problem solving under one roof at the Center will be achieved in 2006.
Dr. Dalton was previously Chief of Surgery at Elliot Hospital inManchester, New Hampshire. He is a Fellow of the American College ofSurgeons and is active in a number ofprofessional societies, including theAmerican Cancer Society, the AmericanSociety of Breast Surgeons, and theNational Consortium of Breast Centers,where he served as both Trustee andPresident. Dr. Dalton is a graduate ofSt. Louis University School of Medicineand did postgraduate training at theUniversity of Michigan and the StateUniversity of New York at Buffalo. Hehas been in private practice since 1977,with a breast specialization for almost20 years.
THOMAS B.JULIAN, MD, FACSAllegheny GeneralHospital Thomas B. Julian, MD,is an accomplished breastcancer surgeon,
researcher, and educator, currently serv-ing as Associate Director of theAllegheny Breast Center, Staff Surgeonin the Division of Surgical Oncology at Allegheny General Hospital, bothlocated in Pittsburgh, Pennsylvania, and Associate Professor of HumanOncology at Drexel University Collegeof Medicine in Philadelphia. He hasbeen a principal investigator for numer-ous breast cancer pre- and post-launchclinical trials studying topics such as pri-mary systemic combination drug thera-py in postmenopausal hormone-recep-tor-positive breast cancer patients, theGeneSearch™ breast lymph node assayfor intraoperative molecular testing,digital mammography imaging, andMRI evaluation of the contralateralbreast in recently diagnosed femalebreast cancer patients, among others.Together with colleagues Yoed Rabin,PhD, and Norman Wolmark, MD, Dr.Julian was awarded two U.S. patents fordeveloping new methods and equipmentfor use in cryosurgery. From 2002through 2005, he has been the ProtocolOfficer for three breast cancer trialsconducted by the National Surgical
Adjuvant Breast and Bowel Project(NSABP), for which he serves asAssociate Director of Medical Oversight.Dr. Julian’s research has been widelypublished; appearing in over 120 arti-cles, reviews, book chapters, audiovisualdisplays, abstracts, and scientificexhibits. He completed his undergradu-ate work in chemistry at Ohio StateUniversity and the University ofPittsburgh and obtained his MD degreefrom the University of PittsburghSchool of Medicine.
LARRY K.KILLEBREW, MDOklahoma Breast Care Center Larry K. Killebrew, MD,founded the OklahomaBreast Care Center in
1985. The Center has achieved manyhistorical milestones over the years,with Dr. Killebrew serving as MedicalDirector. It was the first breast center inthe state to receive accreditation fromthe American College of Radiology and the first to provide a successfulstatewide mobile imaging program(with two mobile coaches), which also provides no-cost and low-costscreenings to indigent patients. In 1992, Dr. Killebrew pioneered the minimally invasive stereotactic biopsy inOklahoma as an option to surgical biop-sy, a procedure that has since becomethe standard of care throughout theUnited States; he also became the firstto introduce the Intact™ Breast LesionExcision System (BLES) in the southernUnited States. Dr. Killebrew’s body ofwork is reflected in many original arti-cles published in several journals. Heco-authored with Dr. Steve Parker the landmark study that establishedstereotactic biopsy use, published inRadiology (The Grey Journal) in 1994. Other articles have appeared in the Journal of the American Medical Association (JAMA), MedicalEconomics, and The Breast Journal.
WILLIAM R.POLLER, MD,FACRAllegheny CancerCenterWilliam R. Poller, MD,specializes in breast
imaging, which captured his interest

7
while reading mammograms for anational screening project in the early1980s. An accomplished clinician,researcher, author, and educator, he is Associate Director of Radiology at Drexel University and AssociateDirector of the Breast Care Center,Division of Breast Imaging, atAllegheny General Hospital inPittsburgh. He attended the Universityof Pittsburgh, where he obtained hisBachelor of Science in Biology and MDfrom the same medical school. He com-pleted his Radiology Residency at theAlbert Einstein College of Medicine in New York City. Dr. Poller’s recentresearch has concentrated on such top-ics as CAD techniques, digital imaging,whole breast ultrasound and breastbiopsy (e.g., selective lymphadenectomy,sentinel node, stereotactic, and mini-mally invasive). His research has beenwidely presented in numerous articlesand scientific exhibits, seven of whichwon “first place” or “excellent” recogni-tion. Dr. Poller’s state-of-the-art breastcancer center, equipped with four fullfield digital mammography units, twostereotactic tables, and two ultrasoundunits, participates in the AmericanCollege of Radiology Imaging Network(ACRIN) trials related to breast imag-ing. For demonstrated excellence in the conduct of these clinical trials, he received the Network Chair’sInstitutional Achievement Award at ACRIN’s 2005 Fall Meeting. A dedicated teacher, Dr. Poller has delivered or directed over 300 medicaleducation courses and lectures.
LOWELL W. ROGERS, MDLong Beach Memorial Medical CenterLowell W. Rogers, MD, is an accom-plished surgical and anatomic patholo-gist, who has devoted most of his med-ical career to the study of solid tumorsof the breast. He is Director of both theAnatomic Pathology and BreastPathology Departments at California’sLong Beach Memorial Medical Center.Dr. Rogers also serves on the faculty of two medical schools, the Universityof California (Irvine) and VanderbiltUniversity Medical School (Nashville),where he teaches pathology and gyne-cology. A distinguished author, guestspeaker, and international lecturer, Dr. Rogers has written or delivered over 45 papers and presentations on numer-
ous breast cancer topics, including inva-sive lobular carcinoma of the breast,ductal carcinoma in situ of the breast,lobular neoplasia of the breast, the rela-tionship between fibrocystic diseasecomplex and breast cancer, ductal pat-tern lesions in biopsies as they relate tobreast cancer risk, adjunctive use ofultrasound and core biopsy in diagnosis,and diagnostic aspects of stereotactic/percutaneous breast biopsy. He has also authored a textbook, DiagnosticPathology of the Breast. Dr. Rogersreceived his BA in chemistry from theUniversity of Arizona, and his MD fromJohns Hopkins University School ofMedicine, where he also completed hisresidency training. He was elected toboth Phi Beta Kappa and Phi Kappa Phiand is a member of numerous hospitalcommittees and professional societies.
JEAN F. SIMPSON, MDVanderbilt UniversityMedical CenterJean F. Simpson, MD, isa noted clinician, educa-tor, and researcher in the
fields of pathology and immunohisto-chemistry, with a special interest in theepidemiology and progression of breasttumors. Currently affiliated withVanderbilt University in Nashville,Tennessee, she serves as professor ofpathology and anatomic pathology,Director of Anatomic Pathology at theMedical Center, and interimPathologist-in-Chief at VanderbiltChildren’s Hospital. Dr. Simpson hasparticipated in breast cancer researchfunded by the City of Hope CancerCenter, the American Cancer Societyand the National Institutes of Health,investigating such topics as molecularcytogenics and tumor progression inepithelial proliferative breast disease,breast tumor cell receptors, and themechanisms of targeted anti-tumorstrategies in breast cancer. A well-pub-lished writer, she has authored or co-authored over 100 scientific papers,books, and abstracts, and served on theeditorial boards of Advances inAnatomic Pathology and HumanPathology. She also lectures extensivelyinside and outside the United States onsubjects ranging from the role of breastpathology in risk assessment and molec-
ular markers in premalignant breast dis-ease to the histopathology of stereotac-tic core biopsy. Dr. Simpson obtainedher MD from the Medical College ofGeorgia in Augusta, Georgia, and com-pleted her residency and fellowship atVanderbilt University.
PAT W.WHITWORTH,MD, FACS Nashville Breast Center Vanderbilt University Pat W. Whitworth, MD,developed a passion for
breast cancer research and educationafter completing the fellowship in surgical oncology at the M. D.Anderson Cancer Center in Houston,Texas, after completing his residency at the University of Louisville. Dr. Whitworth is now Director of the Nashville Breast Center. A dedicated researcher and educator, Dr. Whitworth holds numerous aca-demic and medical appointments:Associate Clinical Professor of Surgeryat Vanderbilt University in Nashville,Tennessee; longstanding membershipon the American College of Surgeonsultrasound faculty; Vice-Chair of theBreast Organ Site Committee for the American College of SurgeonsOncology Group (ACOSOG); andChairman of the Board of Directors for the American Society of BreastSurgeons (ASBS). Dr. Whitworth hascompiled a long list of achievements inbreast cancer research and education.He was one of 11 surgeons participatingin the first national multi-institutionalstudy to validate sentinel lymph nodestaging for breast cancer. In April 2002,he directed the ASBS sentinel lymphnode staging course in Boston. He hasauthored and co-authored a number ofpublications on state-of-the-art, image-guided percutaneous breast biopsy withvarious technologies. In 2003, hisNashville Breast Center received anaward from the American Society of Clinical Oncology for its work inASOCOG clinical trials. Finally, as co-chair of the ASBS course in OncoplasticSurgery, Dr. Whitworth is dedicated to helping the patients of all Societymembers secure access to state-of-the-art oncoplastic surgical therapies.

The Intact BLES offers lower cost for preparation and review.Percutaneous stereotactic needle corebiopsies have been reported to cutbiopsy costs by more than half compared to open biopsy.10, 9 Theelimination of additional procedures by initially obtaining an intact speci-men may cut costs even further.
Procedures using the Intact BLEScan be performed rapidly in the outpa-tient setting, and are inexpensive whencompared to open surgery.
Will these types of systems beapplied therapeutically? The basicpremise of surgical oncology lies in theability to remove diseased tissue, whichthese systems can achieve when smalllesions are present.1 Future resultsfrom surgical avoidance trials may beable to address this pressing question.
COMPLETE REMOVAL OF MASSES ORCALCIFICATIONS
THE CONCEPT OF totally remov-ing small lesions has been proven with large core needle biopsy devices.Others have reported that 90 to 96%of lesions under 1.5 cm could be com-pletely eliminated, sparing a surgicalprocedure in most women.3 Removalof a larger, fully intact specimen takesthis concept one step further allowingthe pathologist to view the architectureof specimens with adequate spatialrecognition of the extent of the
process. Specimens retrieved with the Intact BLES provide an anatomicrelationship view, the ability to evalu-ate margins, and a reduced require-ment for levels. This system allowsexcision of less tissue with better diagnostic quality.
The Intact BLES reduces samplepreparation time, the number of slidesto review, and the pathologist’s reviewtime. Studies have shown that morethan one-quarter of breast lesions areheterogeneous, yielding different histological results from the targetedcenter and periphery. Biopsy tech-niques that sample only part of a heterogeneous mass may result in a misdiagnosis.1 Because the IntactBLES provides a complete tissueblock, a more definitive diagnosis can be established. This minimizes the need for upgrades and reduces the number of open surgical biopsies.
Sie, et al. (2004) conducted a retro-spective, multicenter study in womenwho underwent stereotactic biopsy ofthe breast for mammographic lesionspresenting as microcalcifications andclassified as BIRADS IV or BIRADS Vto determine whether biopsy of thebreast using a percutaneous intactspecimen-sampling device (Intact BLES)was more accurate than percutaneousbiopsy using a vacuum-assisted core needle biopsy device (Mammotome®).14
Two groups of women consisting of742 patients each were selected to represent each biopsy technique. Thepathology distribution of the lesionsretrieved by both biopsy techniqueswere comparable. After comparison to specimens retrieved surgically,underestimation of DCIS and ADHoccurred significantly less frequently in the biopsy samples taken with theIntact BLES system compared to thosetaken with the Mammotome system(see Table 5).14 Complete excision ofADH at biopsy was twice as frequentwith the Intact BLES than with theMammotome device. These resultsconfirm previously observed improve-ments in concordance with the IntactBLES than those seen with vacuum-assisted core needle biopsy.21
“I am excited about the potential to reduce the numberof surgical biopsies for patientswith high risk lesions. This is currently being investigated in alarge, multicenter clinical trial.”Pat W. Whitworth MD, FACSNashville Breast Center
TABLE 5. Diagnostic Gauge Accuracy of Intact BLES Compared to 11-Gauge Vacuum-Assisted Core Biopsy
DCIS BLES VACB p-value
Underestimates n=110 n=112
5 (4.6%) 15 (13.4%) 0.03
ADH n=32 n=30
Underestimates 3 (9.4%) 11 (36.7%) 0.01
Complete n=32 n=30
Excision of 21 (65.6%) 10 (33.3%) 0.02
ADH
NEW TECHNOLOGICAL ADVANCES
8
“With the Intact Breast LesionExcision System, a larger basketdoesn’t mean a larger incision. The incision is the same for allpatients. I am not going to put asuture in the breast, so patientcomfort is enhanced.”William R. Poller, MD, FACR
are other scenarios where this optionmay be appropriate; suggested uses arelisted in Table 6. The following casestudies present evidence for the selec-
PATIENT SELECTION ISSUES
WHEN IS AN Intact BLES proce-dure a good choice? Generally, it isappropriate in most cases as a firstbiopsy option. An Intact BLES proce-dure is appropriate when a lesion thatappears benign is expected to requirecomplete removal. This may be thecase when a benign palpable mass isbothersome to the patient. It is a bene-ficial procedure for women who havemasses or microcalcifications of a sizeor extent that can be encompassed byan Intact BLES capture basket.Approximately 10% of all mammo-graphic or ultrasonographic targetswill contain either ADH, lobular neo-plasia (ACH, LCIS) or other purport-ed high-risk lesions, such as radial scar,papilloma, complex sclerosing lesionand/or columnar alteration with atypia.Lesions graded as BIRADS IV or V,and of an appropriate size, are candi-dates for complete excision with anIntact BLES procedure reducing theneed for re-excision. High-risk lesions,initially diagnosed using needle biopsyspecimens, requiring re-excision arealso candidates for an Intact BLESprocedure if they meet the sizerequirements. Complete re-excisioncan be accomplished percutaneously —accurately and precisely — with lesspotential morbidity and cost. There
TABLE 6. Patient Selection: Intact Breast Lesion Excision System
SUGGESTED USES
■ Initial biopsy■ Benign, palpable masses that are bothersome to the patient ■ Dense or fibrous breasts■ Small, tightly clustered microcalcifications visualized on ultrasound
or mammography■ Small fibroadenomas■ Radial scars■ Lesions with mucus-like material on biopsy■ Papillomas■ Stereotactic-biopsy with ADH
2
■ Lesions likely to be obliterated or missed with core biopsy■ Fat necrosis, TRAM flaps■ Small breast cancers in poor-risk women (co-morbid disease)
PATIENTS NOT SUITED
Patients with:■ Implants or pacemakers■ Image abnormalities of an extent greater than available Intact BLES
capture baskets, e.g., 25 mm■ Lesions immediately behind the areola or in front of the chest wall (i.e.,
a stroke margin < 6 mm)
tion of excisional biopsy using anIntact BLES procedure. In most cases,surgical avoidance was, or would havebeen, the outcome.
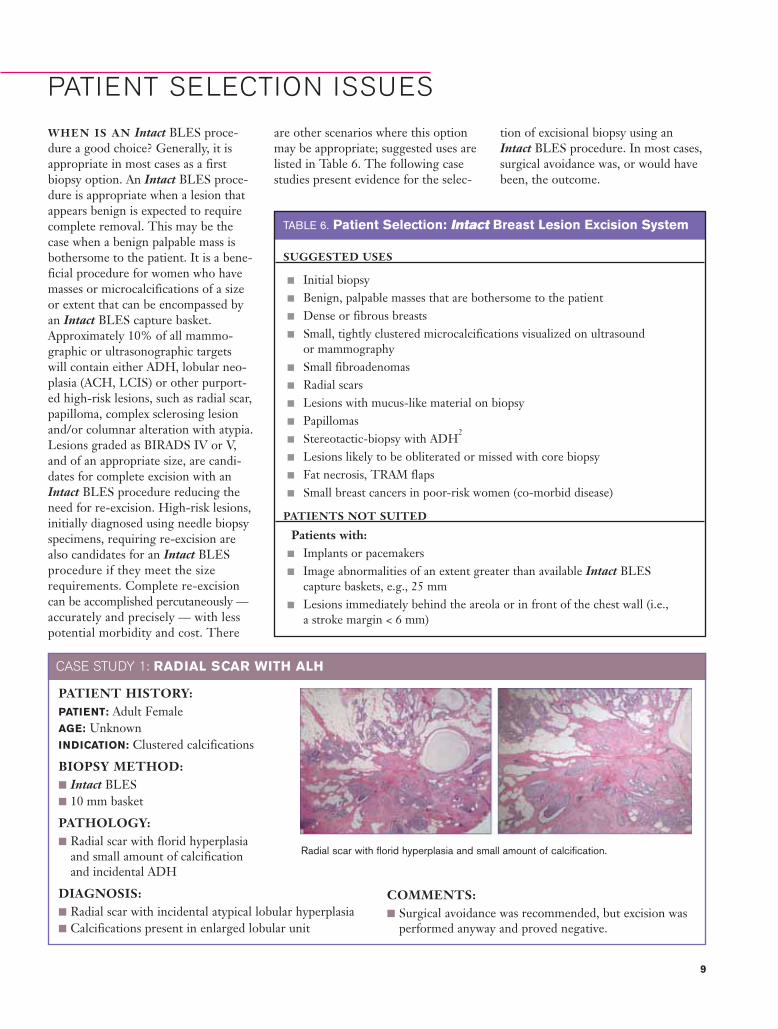
PATIENT HISTORY:PATIENT: Adult Female AGE: UnknownINDICATION: Clustered calcifications
BIOPSY METHOD: ■ Intact BLES■ 10 mm basket
PATHOLOGY:■ Radial scar with florid hyperplasia
and small amount of calcification and incidental ADH
DIAGNOSIS:■ Radial scar with incidental atypical lobular hyperplasia ■ Calcifications present in enlarged lobular unit
Radial scar with florid hyperplasia and small amount of calcification.
COMMENTS: ■ Surgical avoidance was recommended, but excision was
performed anyway and proved negative.
9
CASE STUDY 1: RADIAL SCAR WITH ALH

PATIENT HISTORY:PATIENT: NN with a history of vernacular melanoma AGE: 67 yearsINDICATION: Screening mammogram reveled a new, small
tight cluster of microcalcification within a fatty breast
BIOPSY METHOD: ■ Stereotactic guidance■ 11-gauge Mammotome
PATHOLOGY:■ Focal atypical ductal hyperplasia■ Intraductal papilloma with columnar cell change■ Fibrocystic disease and dystrophic calcification
CASE STUDY 2: ATYPICAL DUCTAL HYPERPLASIA
Mammogram showing a small tight clusterof calcifications
Numerous core samples obtained with Mammotome demonstrated various cellular changes
Pathological evaluations after retrieval of intact specimen showed no malignant disease
PATIENT HISTORY:■ PATIENT: JH ■ AGE: 53 years■ INDICATION: History of intermittent
nipple discharge, now bloody.Negative mammogram and CBE.Ultrasound showed solitary papillarylesion.
BIOPSY METHOD: ■ Ultrasound guidance ■ Intact BLES ■ 20 mm basket
CONFIRMING BIOPSY METHOD:■ None needed
DIAGNOSIS:■ Benign papillary lesion
Histopathology showing full extent of a benign papillary lesion
CONFIRMING BIOPSY METHOD:■ Complete excision performed using the
Intact Breast Lesion Excision System
DIAGNOSIS:■ Sclerosing adenosis■ Fibrocystic change■ Some microcalcifications■ No atypical ductal hyperplasia
COMMENTS: ■ Surgical avoidance after excisional biopsy
Ultrasound showing solitary papillary lesion
CASE STUDY 3: INTRADUCTAL PAPILLOMA
10
COMMENTS: ■ Surgical avoidance of subareolar
resection by excision of entirelesion on biopsy. Asymptomaticone year later

CASE STUDY 4: POOR SURGICAL RISK
PATIENT HISTORY:PATIENT: AL, wheelchair dependent, diabetic, hypertensive, post
CVA with minimal residualAGE: 77 yearsINDICATION: Mammogram detected lesion in left breast
BIOPSY METHOD: ■ Ultrasound guidance■ Intact BLES■ 20 mm basket
PATHOLOGY:■ Well differentiated invasive ductal carcinoma 0.7 cm■ DCIS absent■ Focally present at cauterized margin
CONFIRMING BIOPSY METHOD:■ None required
DIAGNOSIS:■ Invasive ductal carcinoma
COMMENTS: ■ The Intact BLES sample made surgical avoidance possible in a
poor-risk patient having a small mass because clear margins werevisualized and adequate.
■ Interval mammogram showed no evidence of recurrence.
PATIENT HISTORY:PATIENT: JSAGE: 70 yearsINDICATION: Subareolar mass 1.5 x 2 cm
BIOPSY METHOD: ■ Intact BLES■ 10 mm basket
CONFIRMING BIOPSY METHOD:■ None required
DIAGNOSIS:■ Atypical ductal hyperplasia■ Radial scar
Pathology of excised mass showing clear margins
COMMENTS: ■ Because an intact specimen includes the entirety of the
lesion, the location and a definitive diagnosis of ADHcould be confirmed.
■ No upgrade needed■ A surgical excision was unnecessary, but was
performed anyway
Ultrasound demonstrating 5 mm mass
Histopathology of radial scar and ADH in radial scar. No malignancy observed.
11
CASE STUDY 5: ADH AND RADIAL SCAR

CHALLENGES FOR THE FUTURE
THE FDA APPROVED the IntactBLES for diagnostic sampling of breastabnormalities in 2001. The systemproved to provide superior specimensfor histological evaluation.22 Due tothe intact nature of the tissue sampled,a more accurate diagnosis occurs,which minimizes the need for opensurgical excision in many cases. In2005, the FDA expanded indicationsfor the system, for partial or completeremoval of an imaged abnormality toobtain tissue samples for histologicalexamination or partial removal of apalpable abnormality that has beenclassified as benign.
Therapeutic Potential?
The well-characterized, intact speci-mens provided by an Intact BLES procedure offer the option of surgicalavoidance for high-risk lesions. Thepotential to obtain intact specimenswith clear margins makes therapeuticapplications an obvious expansion ofthe system’s use.
Application of this instrumentation is still in its infancy; ongoing clinicaltrials will be needed to quantitativelyassess its value in surgical avoidance for malignant lesions. It remains to be determined which histologicalparameters and mammographic con-cordance will be required to movefrom diagnostic applicability to a treatment modality.
Integrated Approach NeededFor breast biopsy to provide the mostdefinitive diagnosis possible, an inter-disciplinary approach must occur.Breast imaging, pathological diagnosis,and treatment decisions are an inte-grated function. There is a need tobring the specialties of radiology,pathology, and surgery together.Practice management and the businessaspects of breast diagnosis and treat-ment call for breast programs withaccountability from all aspects of thediscipline. There is a need for thesevarious specialties to embrace thechanging trends in breast biopsy andbecome educated on new technological
advances. It will also be important forphysicians and their patients to readilyaccept more conservative treatment forbenign tumors.23
More concordance reporting isneeded and direct communicationbetween pathologists and other clinicians is essential because not all pathology reports contain the information needed for clinical deci-sion making.10 An initiative that hasworked at various centers is having adefined system to handle the need forreaching and reporting concordancebetween mammographic findings and breast biopsy. Individual centerswill need to sort out the roles andresponsibilities of the pathologist, the interventional radiologist, or ateam encompassing various membersof a review committee.
Financial ConsiderationsThere is a need within the industry to resolve reimbursement issues.Currently, the reimbursement forbreast biopsies has not kept up withthe technology. A CPT code of 88305currently covers biopsy procedures,including the percutaneous breast exci-sion systems, for the tissue acquisition
of skin, breast, or other diagnosticbiopsies exclusive of cysts.Unfortunately, the collectable physi-cian component and the hospital component do not cover actual costsfor the complex nature of diagnosingbreast tissues providing minimal profitsand disincentives to diagnosticians. A more reasonable code for the newertechnologies might be 88307, (breastexcision of lesion surgical pathologyrequiring microscopic evaluation of margins), which is used to covercomplete excision for a small mass. A redefinition of the scope and amountof work required to diagnose palpablemasses in the breast is needed.
Breast programs, as a whole, whenmanaged properly are very reasonablein terms of reimbursement. Ratherthan viewing the compensation andreimbursement for imaging or pathol-ogy as separate sectors, we must consider the income brought fromtherapy, and return a percentage backto the imaging centers and pathology.
The era of open biopsy has ended.Pathologists, radiologists, and surgeonsmust come together to understand and promote among themselves theappropriate use of needle, core, andlarge specimen capture devices andbegin to supplant open biopsy as much as possible.
TOWARDS EVIDENCE-BASED MEDICINE:
SUPPORTING THE USE OF INTACT BLES FOR SURGICAL AVOIDANCE
JEAN F. SIMPSON, MD, from the Vanderbilt University Medical Center has con-ducted a Proliferative Lesion Trial: a retrospective review of cases looking at variouspatient types or disease entities, without mammographic evidence for context,where an Intact BLES procedure was performed followed by surgical incision.24
She presented her findings at the 2006 US and Canadian Academy of PathologyCongress. Preliminary results from this ongoing review have demonstrated thatexcised specimens obtained from the BLES procedure are able to definitively pro-vide a diagnosis as well as provide a therapeutic option. Positive data (zeroupgrades; n=40) obtained from the results of this retrospective trial have set thestage for a larger prospective trial: the Intact Percutaneous Excision Trial (i-PET).
The Percutaneous Excision Trial is designed to confirm that surgical interven-tion can be avoided by demonstrating that a definitive diagnosis can be madefrom the tissue sample collected using the Intact BLES. This prospective, multi-center trial will enroll up to 400 patients over the age of 18 who have a lesionthat is likely to be entirely excised with the Intact BLES. The study designincludes two arms: (1) patients previously having had a biopsy procedure and (2)patients not having a previous biopsy. A pathological diagnosis will be made andan evaluation of concordance with the radiologic findings will occur.
12

REFERENCES1. Iwuagwu O, Drew P. Vacuum-
assisted biopsy device-diagnostic and therapeutic applications inbreast surgery. Breast.2004;13(6):483-487.
2. Silverstein MJ, Lagios MD, Recht A, et al. Image-detected breast cancer: state of the art diagnosis and treatment. J Am Coll Surg. 2005;201(4):586-597.
3. Fine RE, Whitworth PW, Kim JA,Harness JK, Boyd BA, Burak WE Jr.Low-risk palpable breast massesremoved using a vacuum-assistedhand-held device. Am J Surg.2003;186(4):362-367.
4. Kerlikowske K, Smith-Bindman R,Ljung BM, Grady D. Evaluation ofabnormal mammography results andpalpable breast abnormalities. AnnIntern Med. 200319;139(4):274-284.
5. Ghosh K, Melton LJ, Suman VJ, etal. Breast biopsy utilization: a popu-lation based study. Arch Intern Med.2005;165:1593-1598.
6. Singletary SE. New approaches tosurgery for breast cancer. EndocrRelat Cancer. 2001;8(4):265-286.
7. Kepple J, Van Zee KJ, DowlatshahiK, Henry-Tillman RS, Israel PZ,Klimberg VS. Minimally-invasivebreast surgery. J Am Coll Surg.2004;199(6):961-975.
8. Singletary SE, Dowlatshahi K,Dooley W, et al. Minimally-invasiveoperation for breast cancer. CurrProbl Surg. 2004;41(4):394-447.
9. Winchester DP, Jeske JM,Goldschmidt RA. The diagnosis andmanagement of ductal carcinoma in-situ of the breast. CA Cancer J Clin.2000;50:184-200.
10. Logrono R. Primer: cytopathologyfor the clinician—how to interpretthe results of aspiration cytology.Nat Clin Pract GastroenterolHepatol. 2005;2(10):484-491.
11. Bassett L, Winchester DP, CaplanRB, et al. Stereotactic core-needlebiopsy of the breast: a report of theJoint Task Force of the AmericanCollege of Radiology, AmericanCollege of Surgeons, and College ofAmerican Pathologists. JacksonvilleMedicine. 1998. Available at:http://www.dcmsonline.org/jax-medicine/1998journals/march98/index.htm. Accessed12/31/05.
12. Liberman L, Kaplan JB.Percutaneous core biopsy of nonpal-pable breast lesions: utility andimpact on cost of diagnosis: In:Pisano ED, ed. Breast Imaging.Amsterdam: IOS Press; 2001, BreastDisease; vol. 13;49-57
13. Golub RM, Bennet CL, Stinson T,Venta L, Morrow M. Cost mini-mization study of image-guided corebiopsy versus surgical excisionalbiopsy for women with abnormalmammograms. J Clin Oncol.2005;201:14-17.
14. Sie A. Comparison of the diagnosticaccuracy of a vacuum-assisted percu-taneous intact specimen biopsydevice to 11-guage vacuum-assistedcore procedures for biopsy of breastcancer: a multi-center experience.Paper presented at: RadiologicalSociety of North AmericanScientific Assembly and AnnualMeeting: November 27-Decenber 2,2004, Chicago, IL.
15. Nerurkar A, Osin P. The diagnosisand management of pre-invasivebreast disease: the role of new diag-nostic techniques. Breast CancerRes. 2003;5(6):305-308.
16. Darling MLR, Smith DN, LesterSC, et al. Atypical ductal hyperplasiaand ductal carcinoma in situ asrevealed by large-core needle breastbiopsy: results of surgical excision.AJR.2000;175:1341-1346.
17. Philpotts LE, Lee CH, Horvath LJ,Lange RC, Carter D, Tocino I.Underestimation of breast cancerwith 11-gauge vacuum suction biopsy. AJR. 2000;175:1047-1050.
18. Burak WE, Owens KE, Tighe MB,et al. Vacuum-assisted stereotacticbreast biopsy. Arch Surg.2000;135:700-703.
19. Jackman RJ, Birdwell R, Ikeda DM.Atypical ductal hyperplasia: cansome lesions be defined as probablybenign after stereotactic 11-gaugevacuum-assisted biopsy, eliminatingthe recommendation for surgicalexcision. Radiol. 2002;224;548-554.
20. Hoorntje LE, Peeters PH, Mali WP,Borel Rinkes IH. Vacuum-assistedbreast biopsy: a critical review. Eur JCancer. 2003;39(12):1676-1683.
21. Killebrew LK. Comparison of thediagnostic accuracy of a percuta-neous intact specimen samplingdevice to a core needle samplingdevice for biopsy of breast cancer:initial experience. Paper presentedat: Radiological Society of NorthAmerican Scientific Assembly andAnnual Meeting; November 30-December 5, 2003; Chicago, IL.
22. Rogers LW, Ries SG, Sie A.Electrosurgical en-bloc stereotactic/percutaneous breast biopsy: an accu-rate method of diagnosis. Posterpresented at the United States andCanadian Academy of PathologyMeeting. February 26-March 4,2005; San Antonio, TX.
23. Hoffman J. Analysis of surgical anddiagnostic quality at a specialistbreast unit. Breast. 2005; (In Press).
24. Simpson JF. IntactTM Image-guidedbreast biopsy reduces need for subsequent open excision in benign proliferative lesions. Poster presented at the UnitedStates and Canadian Academy ofPathology Meeting. February 11-17, 2006; Atlanta, GA.
13
This is not a surgical sample.
Intact“ Breast Lesion Excision System 15mm Sample (Actual Size)
™
BREAST LESIONEXCISION SYSTEM
©20
06 In
tact
Med
ical
Cor
pora
tion
Remove the intac t sample and the uncer ta int y
In fact, this surgical-quality sample came from a minimally invasive procedure, using only local
anesthesia and a 7mm incision.
Yet the Intact™ Breast Lesion Excision
System (BLES) lets you remove the whole lesion,intact, preserving its architectural
integrity with excellent mammo-graphic correlation. So you can clearly see and evaluate the lesion.
Confidently make the call. And avoid sending patients with high-risk lesions to surgery.
Learn more at intactmedical.comtoday. Or call: (888) 430-4490
Surprised?
ww w.intactmedical.com ¥ (888) 430-4490