bilateral thrombosis of the middle cerebral artery in a child aged 14 months
TRANSCRIPT

Develop. Med. Child Neurol. 1971, 13, 613-620
Bilateral Thrombosis of the Middle Cerebral Artery in a Child Aged 14 Months
I . Pascual Castroviejo J. Larrauri
SUDDEN acquired hemiplegia in childhood is usually attributable to vascular ac- cidents. Ford and Schaffer (1927), for example, recorded the case of a patient aged four years who suffered from a thrombosis of the middle cerebral artery. Thrombosis, embolism and thrombo- phlebitis are the commonest causes. Actual rupture of an artery occurs in- frequently, except when there is haemor- rhage in the course of diseases associated with a bleeding tendency (for example, leukaemia, haemophilia and severe art- erial hypertension). Thrombosis most often affects the internal carotid artery and, less frequently, the middle cerebral, the basilar, and other intracranial vessels. Since the clinical manifestations of obstruc- tion of the middle cerebral artery and the internal carotid artery are similar, the differential diagnosis usually depends upon angiography. Even when thrombosis is demonstrated in one of these vessels, however, its cause is often difficult to determine.
Clinical Report J.J.M.C., male, I4 months. This baby
was the first son of young parents; he was delivered at an estimated 8 months gestation with a birth-weight of 2,200 g.
He could hold his head in the erect position at 3-4 months. He sat without support between 10 and 11 months of age, but when seen at the age of 14 months he was still unable to stand without support. Two weeks before he came to the clinic he showed fever (38.5"C) which responded to treatment. Two days before admission his mouth was noted to be deviated to the right, and there was paresis of the left limbs.
His earlier history was non-contribu- tary. He had suffered from recurrent bronchitis and had always been a rather pale, weak, somewhat backward and lethargic child.
In the family history it was noted that the paternal grandfather had died of cirrhosis of the liver and the maternal grandfather had died as a result of an intracranial haemorrhage.
On examination, the child looked pale and ill. There was a flaccid hemiparesis with facial involvement, central in type. The tendon jerks on the left side were depressed. No plantar response was eli- cited. The fundi were normal.
There was a tachycardia of between 120 and 170 per minute and the liver was palpable two fingers below the costal margin, but no other abnormalities of
Clinica Infantil 'La Paz', Madrid 20, Spain.
61 3
DEVELOPMENTAL MEDICINE AND CHILD NEUROLOGY. 1971, 13
the alimentary, cardiovascular or respira- tory systems were noted.
X-ray of the skull revealed no abnor- mality. The EEG showed evidence of pathological involvement in the right hemisphere, and lesser involvement in the left.
The child was anaemic: red blood count 3,500,000; haemoglobin 9.5 g per cent; haematocrit 32 per cent ; erythrocyte sedimentation rate between 10 and 24; white blood count 9,400. The differential white count showed 46 per cent lympho- cytes, 6 per cent monocytes, 39 per cent leucocytes, 7 per cent basophils, and 2 per cent eosinophils ; platelet count was 182,500; bleeding time was 1 minute, coagulation time was 2 minutes; pro- thrombin index was normal; the serum electrolytes, including calcium and phos- phorus, were within normal limits.
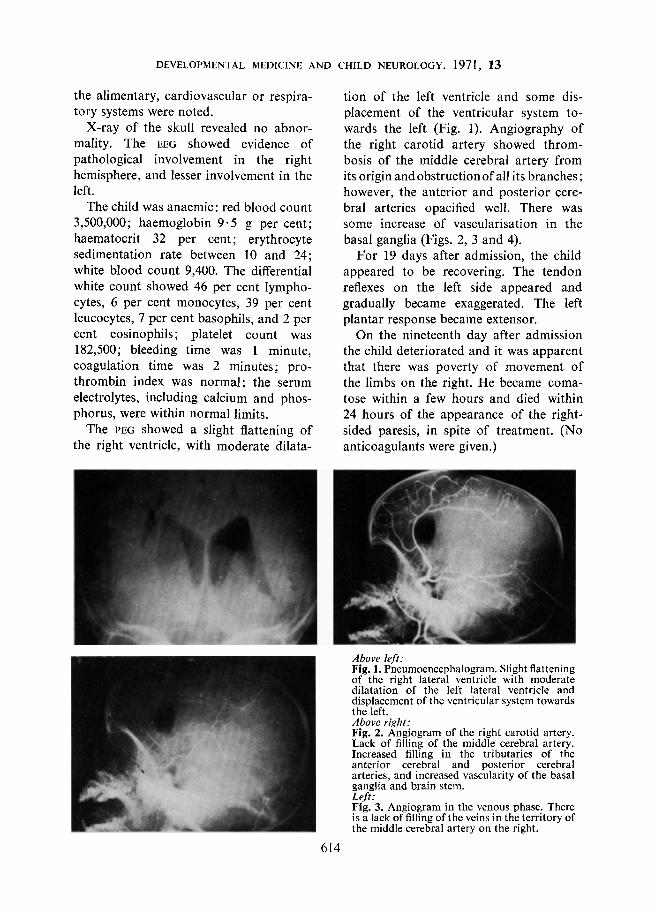
The PEG showed a slight flattening of the right ventricle, with moderate dilata-
tion of the left ventricle and some dis- placement of the ventricular system to- wards the left (Fig. 1). Angiography of the right carotid artery showed throm- bosis of the middle cerebral artery from its origin andobstructionof all its branches; however, the anterior and posterior cere- bral arteries opacified well. There was some increase of vascularisation in the basal ganglia (Figs. 2, 3 and 4).
For 19 days after admission, the child appeared to be recovering. The tendon reflexes on the left side appeared and gradually became exaggerated. The left plantar response became extensor.
On the nineteenth day after admission the child deteriorated and it was apparent that there was poverty of movement of the limbs on the right. He became coma- tose within a few hours and died within 24 hours of the appearance of the right- sided paresis, in spite of treatment. (No anticoagulants were given.)
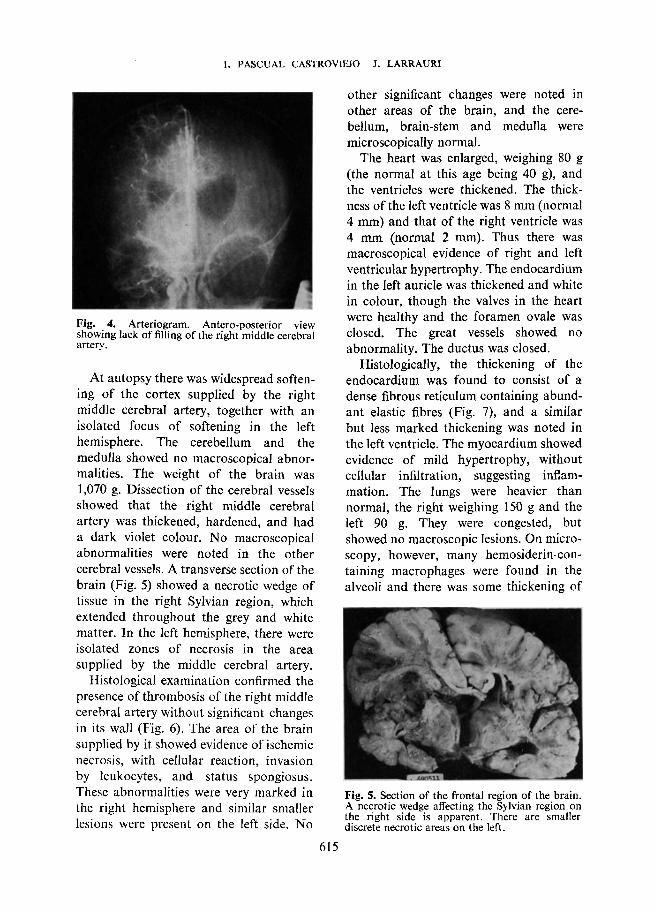
Above left: Fig. 1. Pneumoencephalogram. Slight flattening of the right lateral ventricle with moderate dilatation- of the left lateral ventricle and displacement of the ventricular system towards the left. Above right: Fig. 2. Angiogram of the right carotid artery. Lack of filling of the middle cerebral artery. Increased filling in the tributaries of the anterior cerebral and posterior cerebral arteries, and increased vascularity of the basal ganglia and brain stem. Left: Fig. 3. Angiogram in the venous phase. There is a lack of filling of the veins in the territory of the middle cerebral artery on the right.
614
I. PASCUAL CASTROVIEJO J. LARRAURI
Fig. 4. Arteriogram. Antero-posterior view showing lack of filling of the right middle cerebral artery.
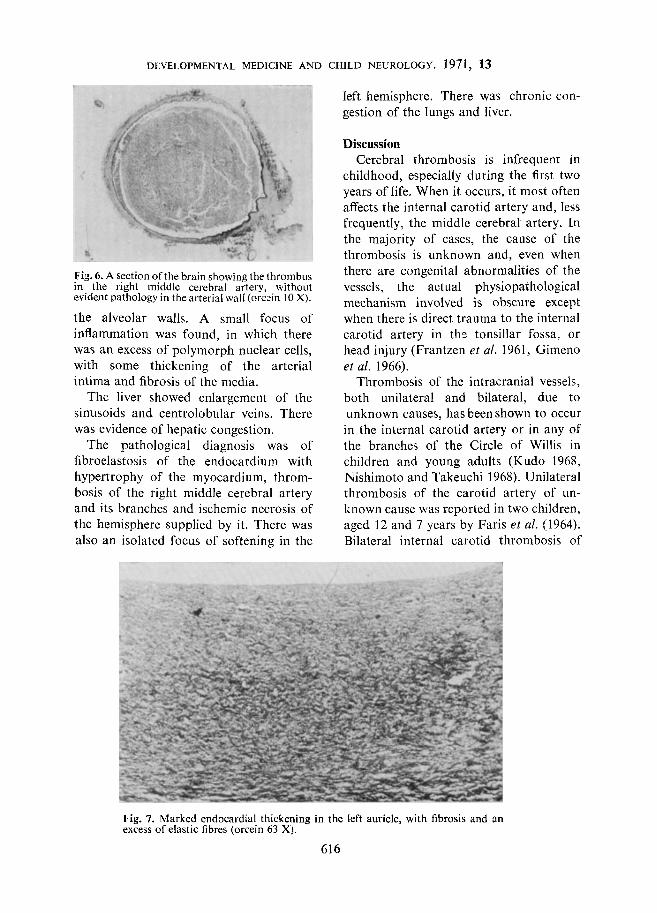
At autopsy there was widespread soften- ing of the cortex supplied by the right middle cerebral artery, together with an isolated focus of softening in the left hemisphere. The cerebellum and the medulla showed no macroscopical abnor- malities. The weight of the brain was 1,070 g. Dissection of the cerebral vessels showed that the right middle cerebral artery was thickened, hardened, and had a dark violet colour. No macroscopical abnormalities were noted in the other cerebral vessels. A transverse section of the brain (Fig. 5) showed a necrotic wedge of tissue in the right Sylvian region, which extended throughout the grey and white matter. In the left hemisphere, there were isolated zones of necrosis in the area supplied by the middle cerebral artery.
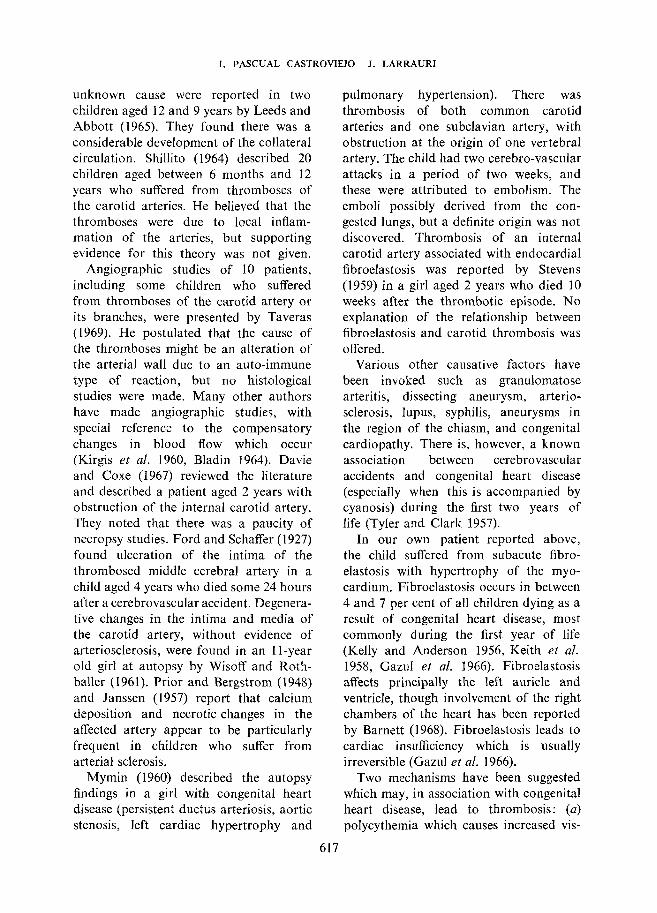
Histological examination confirmed the presence of thrombosis of the right middle cerebral artery without significant changes in its wall (Fig. 6) . The area of the brain supplied by it showed evidence of ischemic necrosis, with cellular reaction, invasion by leukocytes, and status spongiosus. These abnormalities were very marked in the right hemisphere and similar smaller lesions were present on the left side. No
other significant changes were noted in other areas of the brain, and the cere- bellum, brain-stem and medulla were microscopically normal.
The heart was enlarged, weighing 80 g (the normal at this age being 40 g), and the ventricles were thickened. The thick- ness of the left ventricle was 8 mm (normal 4 mm) and that of the right ventricle was 4 mm (normal 2 mm). Thus there was macroscopical evidence of right and left ventricular hypertrophy. The endocardium in the left auricle was thickened and white in colour, though the valves in the heart were healthy and the foramen ovale was closed. The great vessels showed no abnormality. The ductus was closed.
Histologically, the thickening of the endocardium was found to consist of a dense fibrous reticulum containing abund- ant elastic fibres (Fig. 7), and a similar but less marked thickening was noted in the left ventricle. The myocardium showed evidence of mild hypertrophy, without cellular infiltration, suggesting inflam- mation. The lungs were heavier than normal, the right weighing 150 g and the left 90 g. They were congested, but showed no macroscopic lesions. On micro- scopy, however, many hemosiderin-con- taining macrophages were found in the alveoli and there was some thickening of
Fig. 5. Section of the frontal region of the brain. A necrotic wedge affecting the Sylvian region on the right side is apparent. There are smaller discrete necrotic areas on the left.
615
DEVELOPMENTAL MEDICINE AND CHILD NEUROLOGY. 1971, 13
Fig. 6. A section of the brain showing the thrombus in the right middle cerebral artery, without evident pathology in the arterial wall (orcin 10 X).
the alveolar walls. A small focus of inflammation was found, in which there was an excess of polymorph nuclear cells, with some thickening of the arterial intima and fibrosis of the media.
The liver showed enlargement of the sinusoids and centrolobular veins. There was evidence of hepatic congestion.
The pathological diagnosis was of fibroelastosis of the endocardium with hypertrophy of the myocardium, throm- bosis of the right middle cerebral artery and its branches and ischemic necrosis of the hemisphere supplied by it. There was also an isolated focus of softening in the
left hemisphere. There was chronic c o n gestion of the lungs and liver.
Discussion Cerebral thrombosis is infrequent i n
childhood, especially during the first two years of life. When it occurs, it most often affects the internal carotid artery and, less frequently, the middle cerebral artery. In the majority of cases, the cause of the thrombosis is unknown and, even when there are congenital abnormalities of the vessels, the actual physiopathological mechanism involved is obscure except when there is direct trauma to the internal carotid artery in thc tonsillar fossa, or head injury (Frantzen et al. 1961, Gimeno et al. 1966).
Thrombosis of the intracranial vessels, both unilateral and bilateral, due to unknown causes, has been shown to occur in the internal carotid artery or in any of the branches of the Circle of Willis in children and young adults (Kudo 1968, Nishimoto and Takeuchi 1968). Unilateral thrombosis of the carotid artery of un- known cause was reported in two children, aged 12 and 7 years by Faris et al. (1964). Bilateral internal carotid thrombosis of
Fig. 7. Marked endocardia1 thickening in the left auricle, with fibrosis and an excess of elastic fibres (orcein 63 X).
616
unknown cause were reported in two children aged 12 and 9 years by Leeds and Abbott (1965). They found there was a considerable development of the collateral circulation. Shillito (1964) described 20 children aged between 6 months and 12 years who suffered from thromboses of the carotid arteries. He believed that the thromboses were due to local inflam- mation of the arteries, but supporting evidence for this theory was not given.
Angiographic studies of 10 patients, including some children who suffered from thromboses of the carotid artery or its branches, were presented by Taveras (1969). He postulated that the cause of the thromboses might be an alteration of the arterial wall due to an auto-immune type of reaction, but no histological studies were made. Many other authors have made angiographic studies, with special reference to the compensatory changes in blood flow which occur (Kirgis et al. 1960, Bladin 1964). Davie and Coxe (1 967) reviewed the literature and described a patient aged 2 years with obstruction of the internal carotid artery. They noted that there was a paucity of necropsy studies. Ford and Schaffer (1927) found ulceration of the intima of the thrombosed middle cerebral artery in a child aged 4 years who died some 24 hours after a cerebrovascular accident. Degenera- tive changes in the intima and media of the carotid artery, without evidence of arteriosclerosis, were found in an I 1-year old girl at autopsy by Wisoff and Roth- baller (1961). Prior and Bergstrom (1948) and Janssen (1957) report that calcium deposition and necrotic changes in the affected artery appear to be particularly frequent in children who suffer from arterial sclerosis.
Mymin (1960) described the autopsy findings in a girl with congenital heart disease (persistent ductus arteriosis, aortic stenosis, left cardiac hypertrophy and
I . PASCUAL CASTROVIEJO J. LARRAURI
617
pulmonary hypertension). There was thrombosis of both common carotid arteries and one subclavian artery, with obstruction at the origin of one vertebral artery. The child had two cerebro-vascular attacks in a period of two weeks, and these were attributed to embolism. The emboli possibly derived from the con- gested lungs, but a definite origin was not discovered. Thrombosis of an internal carotid artery associated with endocardia1 fibroelastosis was reported by Stevens (1959) in a girl aged 2 years who died 10 weeks after the thrombotic episode. No explanation of the relationship between fibroelastosis and carotid thrombosis was offered.
Various other causative factors have been invoked such as granulomatose arteritis, dissecting aneurysm, arterio- sclerosis, lupus, syphilis, aneurysms in the region of the chiasm, and congenital cardiopathy. There is, however, a known association between cerebrovascular accidents and congenital heart disease (especially when this is accompanied by cyanosis) during the first two years of life (Tyler and Clark 1957).
In our own patient reported above, the child suffered from subacute fibro- elastosis with hypertrophy of the myo- cardium. Fibroelastosis occurs in between 4 and 7 per cent of all children dying as a result of congenital heart disease, most commonly during the first year of life (Kelly and Anderson 1956, Keith et al. 1958, GazuI et aZ. 1966). Fibroelastosis affects principally the left auricle and ventricle, though involvement of the right chambers of the heart has been reported by Barnett (1968). Fibroelastosis leads to cardiac insufficiency which is usually irreversible (Gazul et al. 1966).
Two mechanisms have been suggested which may, in association with congenital heart disease, lead to thrombosis: (a) polycythemia which causes increased vis-

DEVELOPMENTAL MEDICINE AND CHILD NEUROLOGY. 1971. 13
cosity of the blood and slowing of the circulatory flow; and (b) severe hypoxia without polycythemia, especially when there is dehydration and fever (Taussig 1 947).
In their review of the literature, Tyler and Clark (1957) observed that, in younger patients, hypoxia and polycythemia tended to have an inverse relationship. If hypoxia was severe, thrombosis could occur with a normal red count. On the other hand, when there was polycythemia, even minor hypoxia could precipitate thrombosis.
There are many similarities between our patient and those described by Stevens (1959) and by Mymin (1960). These authors found that patients survive for some time following the initial cerebro- vascular accident and even partially re- cover from it, in spite of the presence of a congenital heart disease confirmed at autopsy. However, the cases they reported showed thromboses in the internal carotid arteries, whereas in the patient reported above it occurred in both middle cerebral arteries, with an interval of 19 days elapsing between the two episodes of thrombosis. Neither in the cases of Stevens and Mymin nor in our patient was the thrombosis due to polycythemia. In the patients reported by Stevens and Mymin, the blood counts were normal but our patient was anaemic (see case report).
It is impossible to assign a definite cause to the thromboses, in this case though they appear to be secondary to the congenital heart disease which was associated with a degree of cardiac failure (congestion in the liver and lungs). In addition thzre was hypoxia and this, together with the anaemia, resulted in tachycardia. It may be postulated that the combination of an abnormal heart and
the tachycardia resulted in overloading of the heart; heart failure probably super- vened, and the transient retention of blood in the left ventricular chamber may have resulted in the recurrent thromboses. A similar course of events, with recurrent thromboses occurring over a period of a few weeks, was reported in the patients described by Stevens (1959) and Mymin (1960).
Clinical diagnosis depends upon demon- strating arterial obstruction by angio- graphy. This procedure not only shows the site of the thrombosis, but also the presence of any compensatory collateral circulation and the lack of venous filling in the territory supplied by the obstructed artery. This is especially evident in the acute phase.
The findings on pneumoencephalo- graphy differ according to the time at which the investigation is carried out. In the acute stage following the thrombosis, there tends to be a shift of the ventricular system towards the healthy hemisphere, the lateral ventricle on the thrombosed side being a little flattened since the area supplied by the thrombosed artery is oedematous. It is important to distinguish this picture from that which results from a subdural haemorrhage which may cause a similar shift of the ventricles. On the other hand, a pneumoencephalogram ob- tained during the stage of recovery will show a shift towards the damaged side, for the affected area of the hemisphere retracts as the oedema disappears and cerebral atrophy supervenes. This picture may also be confusing, for there are many causes of cerebral atrophy in infancy. Thus, it is always necessary to carry out angiography so that any vascular patho- logy may be demonstrated.
SUMMARY A case of bilateral thrombosis of the middle cerebral arteries in a child of 14 months of
age is presented. The clinical findings and angiography demonstrated that there was
618

I. PASCUAL CASTROVIEJO J. LARRAURI
thrombosis, even though the child was anaemic. At autopsy the thromboses were found to be associated with endocardial fibroelastosis and myocardial hypertrophy. Though it IS
difficult to explain the mechanism by which the thromboses were caused, it seems likely that it was secondary to cardiac failure associated with tachycardia and cardiac failure with hypoxia.
RGSUMC Thrombose bilatkrale des sylviennes chez un enfant de 14 mois
Les auteurs rapportent le cas d’une thrombose bilattrale des artkres sylviennes chez un enfant de 14 mois. L‘examen clinique et l’angiographie dimontrkrent qu’il s’agissait d’une thrombose bien que l’enfant fut antmique. A I’autopsie, les thromboses se rCvClkrent associCes B une fibro-Clastose endocardique et a une hypertrophie du myocarde. Quoiqu’il soit difficile d’expliquer le mtcanisme des thromboses, il est vraisemblable qu’elles Ctaient secondaires & une dtfaillance cardiaque associCe a une tachycardie et hypoxie.
ZUSAMMENFASSUNG Bilaterale Tlwombose der A . cerebralis media bei einem Kind mit 14 Monaten
€in Fall von bilateraler Thrombose in der A. Cerebrale media bei einem Kind von 14 Monaten wird vorgestellt. Die klinischen Befunde und die Angiographie demonstrierte die Thrombose, obwohl das Kind anaemisch war. Bei der Autopsie bestanden aufler der Thrombose eine endocardiale Fibroelastose und eine Hypertrophie des Myokard. Obwohl es schwierig ist, den ursachlichen Mechanismus der Thrombosen zu erklaren, scheint es wahrscheinlich, dal3 sie auf dem Boden eines Herzversagens mil Tachykardie und Hypoxie entstanden sind.
RESUMEN Trombosis bilateral de la arteria cerebral media en un niEo de I4 meses
Se presenta un caso de trombosis bilateral de la arteria cerebral media en un niiio de 14 meses. Los datos clinicos y angiograficos demostraron que existia trombosis, a pesar de que el niiio era antmico. En la autopsia se encontro que la trombosis estaba asociada a una fibroelastosis endocardica y a hipertrofia miocardica. Aunque es dificil explicar el mecanismo que caus6 la trombosis, parece probable que fuC secundaria a un fall0 cardiac0 asociado a taquicardia e hipoxia.
REFERENCES Barnett, H. L. (1968) Pediatrics, 14th edn. London: Butterworth. Bladin, P. F. (1964) ‘A radiologic and pathologic study of embolism of the internal carotid-middle cerebral
arterial axis.’ Radiology, 82, 615. Davie, J. C., Coxe, W. (1967) ‘Occlusive disease of the carotid artery in children: carotid thrombectomy
with recovery in a two-year-old boy.’ Arch. Neurol. (Chic.), 17, 313. Faris, A. A,, Guth, C., Youmans, R. A., Poser, C. M. (1964) ‘Internal carotid artery occlusion in children.
Diagnosis by arteriography.’ Amer. J. Dis. Child., 107, 188. Ford, F. R., Schaffer, A. J. (1927) ‘The etiology of infantile acquired hemiplegia’ Arch. Neurol. Psychiat.
18, 323. Frantzen, E., Jacobsen, H. H., Therkelsen, J. (1961) ‘Cerebral artery occlusions in children due to trauma
to the head and neck: a report of six cases verified by cerebral angiography.’ Neurology (Minneup), 11, 695.
Gazul, B. M., Arcilla, R. A., Lev, M. H. (1966) Heart Disease in Children. Philadelphia: Lippincott. Gimeno, A., Escudero, L., Zunzunegui, J. (1966) ‘Trombosis traumitica de carotida en una nifia.’ Arch.
Janssen, W. (1957) ‘Arteriosclerosis, especially of the coronary vessels during childhood.’ Mschr. Kinder-
Keiht, J. D., Rowe, R. D., Vlad, P. (1958) Heart Diseases in Infancy and Childhood. New York: Macmillan.
619
Neurobiol. (Madrid), 29, 42.
heilk., 105, 361.

DEVELOPMENTAL MEDICINE AND CHILD NEUROLOGY. 1971, 13
Kelly, J., Andersen, D. H. (1956) ‘Congenital endocardia1 fibroelastosis. 11. A clinical and pathologic investigation of those cases without associated cardiac mdformations including a report of two familial instances.’ Pediatrics, 18, 539.
Kirgis, H. D., Llewellyn, R. C., Peebles, E. M. (1960) ‘Functional trifurcation of the internal carotid artery and its potential clinical significance.’ J. Neurosurq., 17, 1062.
Kudo, T. (1968) ‘Spontaneous occlusion of the circle of Willis. A disease apparently confined to Japanese.’ Neurology (Minneap.), 18,485.
Leeds, N. E., Abbott, K. H. (1965) ‘Collateral circulation in cerebrovascular disease in childhood via rete mirabile and perforating branches of anterior choroidal and posterior choroidal arteries.’ Radiology, 85, 628.
Mymin, D. (1960) ’Carotid thrombosis in childhood.‘ Arch. Dis. Childh. 35, 515. Nishimoto, A., Takeuchi, S. (1968) ‘Abnormal cerebrovascular network related to the internal carotid
arteries.’ J. Neurosurg., 29, 255. Prior, J. T., Bergstrom, V. (1948) ‘Generalized arterial calcification in infants.’ Amer. J. Dis. Child., 76, 91. Shillito. J. (1964) ‘Carotid arteritis: a cause of hemiolegia in childhood.’J. Neurosurp.. 21. 540.
I, I I
Stevens, H. (1959) ‘Carotid artery occlusion in childhogd.’ Pediatrics, 23, 699. Taussig, B., (1947) Congenital Malformation of the Heart. New York: The Commonwealth Fund. Taveras, J. M. (1969) ‘Multiple progressive intracranial arterial occlusions. A syndrome of children and
Tyler, H. R., Clark, D. B. (1957) ‘Cerebrovascular accidents in patients with congenital heart disease.’
Wisoff, H. S., Rothballer, A. B. (1961) ‘Cerebral arterial thrombosis in children: review of the literature
young adults.’ Amer. J. Roentpnol., 106, 235.
Arch. Neurol. Psychiat., 77, 483.
and addition of two cases in apparently healthy children.’ Aich. Neurol. (Chic.), 4, 258.
620