atrioventricular conduction in acute rheumatic fever' - heart · 474 clarke andkeith i i v i_...
TRANSCRIPT

British Heart Journal, I972, 34, 472-479.
Atrioventricular conduction in acute rheumaticfever'
Malcolm Clarke2 and J. D. KeithFrom the Department of Cardiology, Hospital for Sick Children, Toronto, Ontario, Canada
A new study ofnormal PR intervals was undertakenfor the purposes of analysing atrioventricularconduction. Abnormalities of conduction were identified in 84 per cent of So8 patients with acuterheumatic fever. The PR index was used as a simple, reliable method of showing these changes.Such conduction disturbances occur more commonly than carditis, arthritis, subcutaneous nodules,chorea, or erythema marginatum, the five major features of the disease. Streptococcal infectionand acute glomerulonephritis were not associated with similar abnormalities of conduction.
It appears that atrioventricular conduction disturbances that occur after a haemolytic strepto-coccal infection are relatively specific for rheumatic fever, either with or without carditis. It issuggested that reversible PR prolongation be used as a major criterion, when usingJones' criteriafor the diagnosis of rheumatic fever, providing there is proof ofa preceding streptococcal infection.
A number of reports of PR prolongation inrheumatic fever studied by various methodshave been published (Cohn and Swift, I924;Keith, I938; Taran, 1946; Blackman andHamilton, I948; Sokolow, 1948; Mirowski,Rosenstein, and Markowitz, I964). At theHospital for Sick Children in Toronto, fre-quent electrocardiograms have been recordedin children with rheumatic fever, making adetailed study of atrioventricular conductionpossible. In 5o8 patients seen between 1948and I97I, over 2,500 electrocardiograms wereavailable for analysis.
PR intervals in normal childrenTo evaluate atrioventricular conduction, thenormal child must first be studied. The PRinterval varies with both age and heart rate(Ziegler, I95I; Sodi-Pallares et al., 1958). Todate, a number of published tables of normalsexist. Those of Ziegler (I95I) do not give thevariation for heart rate. Ashman and Hull's(I937) figures were considered inadequate byAlimurung and Massell (I956), but their ownfigures are unreliable because of the smallnumbers of patients in many of the groups.Though the latter authors were able to give
Received 6 July 1971.
1 This work was supported by the Ontario HeartFoundation of Canada.2 Present address: Department of Cardiology, St.Bartholomew's Hospital, London E.C.i.
detailed figures for the average PR intervals,it is the maximum normal that is requiredwhen studying atrioventricular conduction.To overcome these objections, a new study
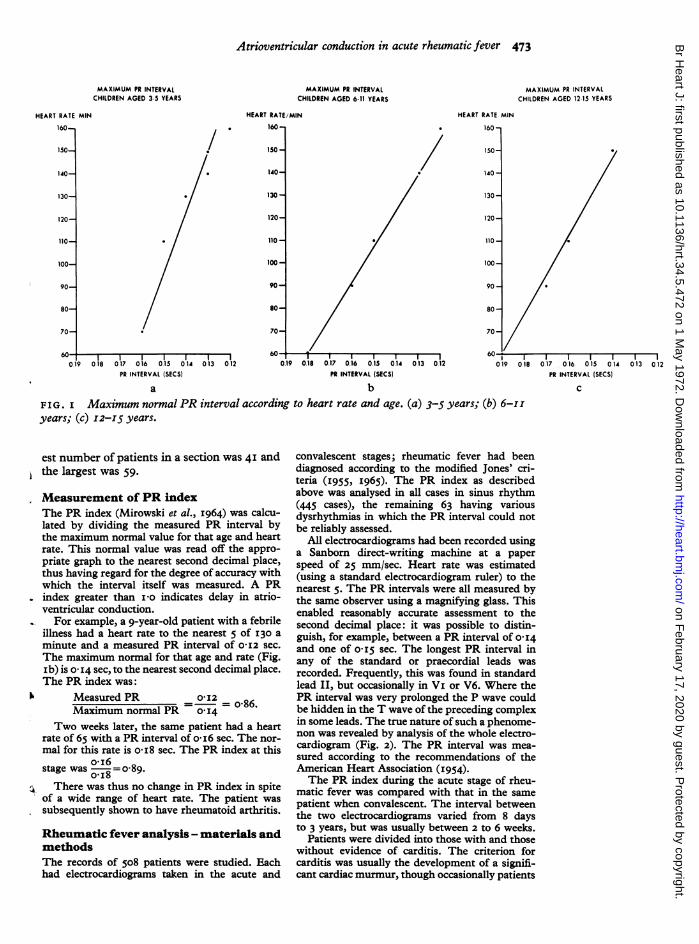
ofPR intervals in normal children was under-taken. The results are shown in Fig. I. ThePR interval was measured on the electro-cardiogram of 672 normal children using themethod described below. The results are inessential agreement with the above authorsbut give more details useful for the purposesof this study of rheumatic fever. The maxi-mum normal PR interval was taken as theiooth percentile for that age and heart rate.Nine normals were excluded from the analysisbecause their PR intervals were considerablyprolonged compared with the others in thegroup. This confirms the observation of Zieg-ler (I95I), that 2 per cent of normal childrenhave very long PR intervals for no apparentreason. Only those electrocardiograms withheart rates of plus or minus 5 of 6o, 90, I10,I40, and i6o were selected in the 6 to ii yearsold group (Fig. ib) to increase the accuracyof the relation. (Numerous electrocardiogramswere usually available.) This enabled the re-sults of each section to be plotted as a singlepoint on the graph without further analysis.Similar criteria, but different heart rates, wereused for the patients younger (Fig. Ia) andolder (Fig. ic) than this group. The linearrelation between PR interval and heart rateshown in our graphs agrees with the findingsof Alimurung and Massell (I956). The small-
on February 17, 2020 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.34.5.472 on 1 May 1972. D
ownloaded from
Atrioventricular conduction in acute rheumatic fever 473
MAXIMUM PR INTERVALCHILDREN AGED 3-5 YEARS
MAXIMUM PR INTERVALCHILDREN AGED 611 YEARS
HEART RATE/MIN
160-,
150-
140-
130-
120-
110-
100-
90-
80-
70-
I I017 016 015 014 013 012PR INTERVAL (SECS)
0.19 0.18
MAXIMUM PR INTERVALCHILDREN AGED 1215 YEARS
HEART RATE MIN
II I~~~~~~~~~~
I I I l0.17 0.16 0.15 0.14 013 0.12PR INTERVAL (SECS)
a bFIG . I Maximum normal PR interval according to heart rate and age. (a) 3-5 years; (b) 6-I Iyears; (c) I2-I5 years.
17 016 0.15 014 013 012PR INTERVAL (SECS)
C
est number of patients in a section was 4I andthe largest was 59.
Measurement of PR indexThe PR index (Mirowski et al., I964) was calcu-lated by dividing the measured PR interval bythe maximum normal value for that age and heartrate. This normal value was read off the appro-priate graph to the nearest second decimal place,thus having regard for the degree of accuracy withwhich the interval itself was measured. A PRindex greater than i-o indicates delay in atrio-ventricular conduction.
For example, a 9-year-old patient with a febrileillness had a heart rate to the nearest 5 of I30 a
minute and a measured PR interval of O-I2 sec.
The maximum normal for that age and rate (Fig.ib) is 0- I4 sec, to the nearest second decimal place.The PR index was:
Measured PR 012 o-86.
Maximum normal PR O I4 ° 8Two weeks later, the same patient had a heart
rate of 65 with a PR interval of o i6 sec. The nor-mal for this rate is o-i8 sec. The PR index at this
o-i6stage was =o-89.
o.i8
There was thus no change in PR index in spiteof a wide range of heart rate. The patient wassubsequently shown to have rheumatoid arthritis.
Rheumatic fever analysis - materials andmethodsThe records of 508 patients were studied. Eachhad electrocardiograms taken in the acute and
convalescent stages; rheumatic fever had beendiagnosed according to the modified Jones' cri-teria (I955, I965). The PR index as describedabove was analysed in all cases in sinus rhythm(445 cases), the remaining 63 having variousdysrhythmias in which the PR interval could notbe reliably assessed.
All electrocardiograms had been recorded usinga Sanborn direct-writing machine at a paperspeed of 25 mm/sec. Heart rate was estimated(using a standard electrocardiogram ruler) to thenearest 5. The PR intervals were all measured bythe same observer using a magnifying glass. Thisenabled reasonably accurate assessment to thesecond decimal place: it was possible to distin-guish, for example, between a PR interval of O-I4and one of o1I5 sec. The longest PR interval inany of the standard or praecordial leads wasrecorded. Frequently, this was found in standardlead II, but occasionally in VI or V6. Where thePR interval was very prolonged the P wave couldbe hidden in the T wave of the preceding complexin some leads. The true nature of such a phenome-non was revealed by analysis of the whole electro-cardiogram (Fig. 2). The PR interval was mea-sured according to the recommendations of theAmerican Heart Association (I954).The PR index during the acute stage of rheu-
matic fever was compared with that in the same
patient when convalescent. The interval betweenthe two electrocardiograms varied from 8 daysto 3 years, but was usually between 2 to 6 weeks.
Patients were divided into those with and thosewithout evidence of carditis. The criterion forcarditis was usually the development of a signifi-cant cardiac murmur, though occasionally patients
HEART RATE MIN
160-
150-
140-
130-
120-
110-
100-
90-
80-
70-
019 018
on February 17, 2020 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.34.5.472 on 1 May 1972. D
ownloaded from

474 Clarke and Keith
I I
V i_ V
AVR
Repeated readings add reliability, and sub-sequent change of PR index is of great value.
PR index greater than I10 during acuteA J\ stage Three-quarters of the patients in
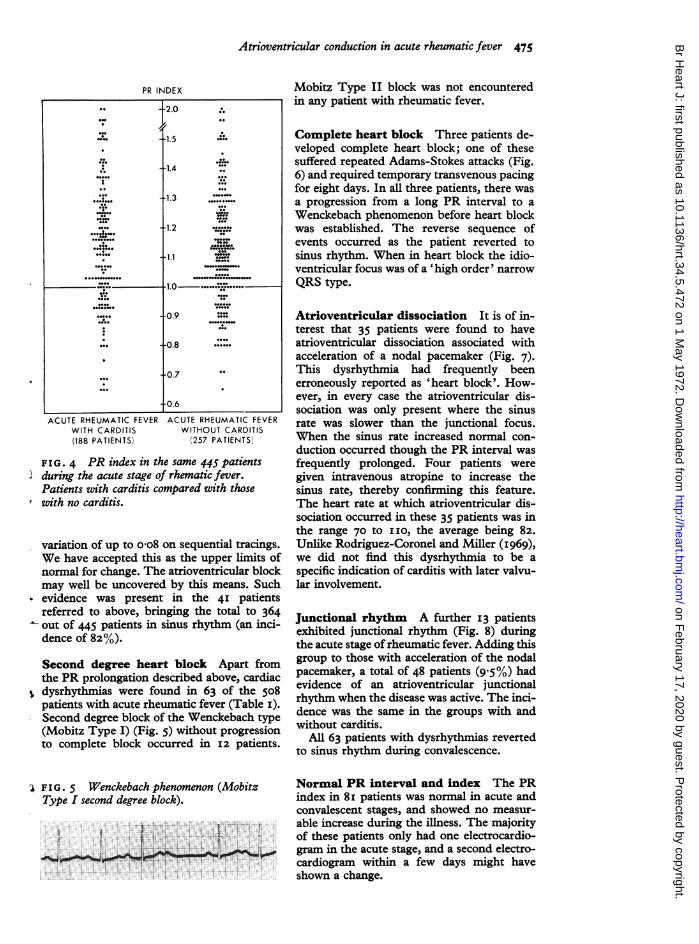
sinus rhythm (323 out of 445) had a PR indexgreater than i o during the acute stage ofrheumatic fever (Fig. 3). There was no differ-ence between those with carditis and thosewith no cardiac involvement (Fig. 4). Nopatient was receiving digitalis at the time ofthe initial electrocardiogram. In every patientwith an increased PR index this subsequentlybecame smaller when the disease became in-active. In all but 3 per cent it reverted to lessthan I o (Fig. 3).
V6
FIG. 2 The rhythm in lead II appears to benodal. Analysis ofAVR and V6 shows a verylong PR interval, with the P wave partiallyhidden in the T wave of the preceding complex.
were placed in this category on the basis of a peri-cardial rub alone. Cardiac murmurs were assessedcarefully by staff cardiologists so that patientswith innocent systolic murmurs were not includedin the group with carditis.
ResultsThe various electrocardiographic abnormali-ties found in the 5o8 patients with acute rheu-matic fever are summarized in Table i. Thepatients were aged 2 to I4 years; the averageage was 7-8 years.
Because of method error, a random PRindex of up to I 03 should only be accordedthe same suspicion as a high-normal reading.
TABLE i Atrioventricular conduction changesin acute rheumatic fever
Rhythm Carditis No Totalcarditis
PR index > i during acutestage I36 I87 323
PR index greater in acutestage than in quiescence i6 25 4I
Wenckebach seconddegree AV block 7 5 I2
Complete AV block I 2 3Junctional rhythm 5 8 I3AV dissociation with
accelerated nodal pace-maker 19 i6 35
Normal PR index 34 47 8i
Totals 2I8 290 5o8
PR index greater during acute stageForty-one patients without obvious atrio-ventricular conduction delay had a PR indexchange from the acute stage to the quiescentphase that was O I4 or greater, though at notime was the PR index greater than I 0. Asample of serial electrocardiograms in thesame number of normal children showed a
FIG. 3 PR index in 445 patients with acuterheumatic fever in sinus rhythm, comparedwith the same patient when convalescent.
PR INDEX
PR INDEXDURING ACUTE
RHEUMATIC FEVER(445 PATIENTS)
-0.6
PR INDEXIN THE SAME PATIENTSWHEN RHEUMATICFEVER INACTIVE
+-2.0
-1.5
-1.4
1.3
-1.2
-1.1
1.0-........:0.9._.........
--- *-----
T-09 --I
-0.8
-0.7
00
00.
.0
...00
O**.O.-O.0
000"
0 0000
.00.0.0.0O.O..o...0-0.
O.-.0..:...0
....OI
O.O.
.0
.-O
O.O.
....
.......
.......... .
on February 17, 2020 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.34.5.472 on 1 May 1972. D
ownloaded from
Atrioventricular conduction in acute rheumatic fever 475
PR INDEX
.. -2.0
1.5
-1.4
1.3
1.2J.~~~~~~
* 1.1
........... "~~~~~~~~~~............2..
J. @ - 1.0o.Mo". -.0.o.....
-0.9 r
0~~~~...... -0.7
o.o
0.6
ACUTE RHEUMATIC FEVER ACUTE RHEUMATIC FEVERWITH CARDITIS(188 PATIENTS)
WITHOUT CARDITIS(257 PATIENTS)
FIG. 4 PR index in the same 445 patientsduring the acute stage of rhematic fever.Patients with carditis compared with thosewith no carditis.
variation of up to o o8 on sequential tracings.We have accepted this as the upper limits ofnormal for change. The atrioventricular blockmay well be uncovered by this means. Suchevidence was present in the 4I patientsreferred to above, bringing the total tO 364Out of 445 patients in sinus rhythm (an inci-dence of 82%).
Second degree heart block Apart fromthe PR prolongation described above, cardiac
> dysrhythmias were found in 63 of the 508patients with acute rheumatic fever (Table i).Second degree block of the Wenckebach type(Mobitz Type I) (Fig. 5) without progressionto complete block occurred in I2 patients.
'I F I G . 5 Wenckebach phenomenon (MobitzType I second degree block).
Mobitz Type II block was not encounteredin any patient with rheumatic fever.
Complete heart block Three patients de-veloped complete heart block; one of thesesuffered repeated Adams-Stokes attacks (Fig.6) and required temporary transvenous pacingfor eight days. In all three patients, there wasa progression from a long PR interval to aWenckebach phenomenon before heart blockwas established. The reverse sequence ofevents occurred as the patient reverted tosinus rhythm. When in heart block the idio-ventricular focus was of a 'high order' narrowQRS type.
Atrioventricular dissociation It is of in-terest that 35 patients were found to haveatrioventricular dissociation associated withacceleration of a nodal pacemaker (Fig. 7).This dysrhythmia had frequently beenerroneously reported as 'heart block'. How-ever, in every case the atrioventricular dis-sociation was only present where the sinusrate was slower than the junctional focus.When the sinus rate increased normal con-duction occurred though the PR interval wasfrequently prolonged. Four patients weregiven intravenous atropine to increase thesinus rate, thereby confirming this feature.The heart rate at which atrioventricular dis-sociation occurred in these 35 patients was inthe range 70 to IO, the average being 82.Unlike Rodriguez-Coronel and Miller (I969),we did not find this dysrhythmia to be aspecific indication of carditis with later valvu-lar involvement.
Junctional rhythm A further 13 patientsexhibited junctional rhythm (Fig. 8) duringthe acute stage of rheumatic fever. Adding thisgroup to those with acceleration of the nodalpacemaker, a total of 48 patients (9.5%) hadevidence of an atrioventricular junctionalrhythm when the disease was active. The inci-dence was the same in the groups with andwithout carditis.
All 63 patients with dysrhythmnias revertedto sinus rhythm during convalescence.
Normal PR interval and index The PRindex in 8i patients was normal in acute andconvalescent stages, and showed no measur-able increase during the illness. The majorityof these patients only had one electrocardio-gram in the acute stage, and a second electro-cardiogram within a few days might haveshown a change.
on February 17, 2020 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.34.5.472 on 1 May 1972. D
ownloaded from

476 Clarke and Keith
Streptococcal infections The PR indexwas assessed in 5I patients with streptococcalinfections. This group included i6 with acutestreptococcal glomerulonephritis. No increasein PR index was found either in the acutefebrile state or some weeks later (Fig. 9). Thisevidence refutes those suggestions that feveror streptococcal infections per se cause fre-quent atrioventricular conduction delay (Fein-stein, I966). On the contrary, it implies thatPR prolongation after a streptococcal infectionis a relatively specific indication of rheumaticfever.
Intracardiac electrocardiogram A 5-year-old girl with acute streptococcal glo-merulonephritis was also felt to have acuterheumatic fever. The evidence for this wasthe appearance of an apical systolic murmurof mitral regurgitation, at a time when theblood sedimentation rate was raised to 85 mmin the first hour and the PR interval was pro-longed. Though there was no history of jointpains, a previous streptococcal infection waspresent as indicated by an antistreptolysin 0titre of 800 Todd units.An intracardiac electrocardiogram to in-
clude His bundle potentials was recorded onthis girl. The electrode was introduced intothe heart from the long saphenous vein underfluoroscopic control. After a recording hadbeen taken, the heart rate was fixed by atrialpacing at a faster rate and atropine o03 mggiven intravenously. The results are shown inTable 2. Because the PR interval on the intra-cardiac electrocardiogram is shorter than thatmeasured in the standard leads, we will referto the former as the P'R interval. The pro-longed P'R interval was due to an abnormallylong P'H segment, indicating delay in conduc-tion proximal to the bundle of His. The HVinterval remained unchanged throughout,and was normal for this age (Roberts andOlley, I97I). Atropine temporarily reversedthe P'H prolongation. This effect was not dueto any change in heart rate as this was fixedby atrial pacing.
DiscussionThe frequent occurrence of PR interval pro-longation in acute rheumatic fever has beenrecognized for over 50 years (Parkinson,Gosse, and Gunson, 1920). By using the moreelegant method of measuring the PR indexand comparing the acute with the convalescentstages, some atrioventricular conduction ab-normality has been shown in 84 per cent ofour patients. This is a somewhat higher inci-dence than previously reported (Parkinson
FIG. 6 Ventricular asystole occurring in apatient with acute rheumatic fever and com-plete heart block.
et al., I920; Blackman and Hamilton, 1948;Mirowski et al., I964). Though the publishedvalues for normal children that were availableto these and other authors were inadequate,none made a special study to determine thenormal maximum PR interval. Our higherincidence is partly due to the assessment ofnormal children and partly to the acceptancethat a variation in PR index reflects a changein atrioventricular conduction. His bundlecardiograms could probably show this change,but the simpler non-invasive technique ofmeasurement of index is adequate in themajority of instances.One of us has shown that atropine reverses
the PR interval prolongation of rheumaticfever (Keith, 1938). Study on one patient byintracardiac electrocardiogram showed thatthe site of reversible delay was proximal tothe bundle of His, as expected from otherevidence cited below. The effect of atropineis to block vagal receptors in the heart; theprinciple of these receptors are the sinoatrialand atrioventricular nodes. It is known thatacetylcholine may produce heart block by theaction on the AV node. The effect has beenlocalized to the atrial margin fibres of the AVnode in animal experiments (Cranefield, Hoff-man, and de Carvalho, I958). Further evi-dence to implicate a parasympathomimeticaspect in rheumatic fever is the sinus brady-cardia that frequently occurs in the mildly illpatients (Keith, I938). It is not known whe-ther these conduction changes which occurso frequently are mediated by acetylcholine-like substances or by direct vagal action.
This phenomenon of PR prolongation isonly one aspect of a cardiac disturbance thatoccurs in acute rheumatic fever. Wheresecond degree heart block occurred in our
FIG. 7 Atrioventricular dissociation withaccelerated nodal rhythm.
0
on February 17, 2020 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.34.5.472 on 1 May 1972. D
ownloaded from

Atrioventricular conduction in acute rheumatic fever 477
patients this was always of the Wenckebachtype (Mobitz Type I). Furthermore, in our
three patients with complete heart block thepattern was identical. The cardiac rhythmprogressed through the stages ofPR prolonga-tion and Wenckebach block before completeblock occurred. When in heart block, the idio-ventricular focus was of a 'high order' narrow
QRS pattern. His-electrocardiogram studieshave shown that these characteristics occurmost typically where the block is proximal tothe bundle of His (Damato et al., I969;Narula et al., I97I). Mobitz Type II block,which indicates almost exclusively disease
L distal to the His bundle (Narula et al., 1971),was not encountered in this series. None of the508 patients had a left hemiblock or rightbundle-branch block, further supporting theevidence that the rheumatic affectation ofatrioventricular conduction is proximal to thetrifascicular system.
Other evidence pointing to the locality ofthe disorder in rheumatic fever is the inci-dence of junctional rhythms. Atrioventriculardissociation has been reported to be common(Cristal, Stern, and Gueron, I97I), and more
frequent electrocardiogram monitoring in our
patients might have uncovered a higher inci-dence than that found. As it was, a random
J electrocardiogram recorded some time duringthe first 7 days of a child's admission to hos-pital showed an incidence of 9.5 per cent ofjunctional rhythms and atrioventricular dis-sociation.A large international multicentre study of
rheumatic fever (British Medical Journal,I955) gave the incidence of the major mani-festations of the disease as follows: arthritis(43.3%); nodules (I4.3%); chorea (Io'9%);erythema marginatum (5 8%); carditis(75*I%). Atrioventricular conduction abnor-malities detected by the methods describedin this paper are thus much more common
(84%) than any of the recognized majormanifestations of rheumatic fever.
It has long been established that rheumaticfever is invariably preceded by a Group Afl-haemolytic streptococcal infection (Rantz,Boisvert, and Spink, I945; Rammelkamp andStolzer, I954). During epidemics with viru-lent organisms, about 3 per cent of the popula-tion affected by such a streptococcal infectionwill develop rheumatic fever (Rammelkampand Stolzer, I954). Levander-Lindgren (I952)found 3.9 per cent of patients admitted to
hospital with scarlet fever had electrocardio-graphic changes similar to those describedabove, and it seems probable that this was dueto the occurrence of rheumatic activity in-duced by the streptococcus. Rantz, Spink,
FIG. 8 junctional rhythm with spontaneousreversion to sinus rhythm at a faster rate.
and Boisvert reached a similar conclusion in1946. In confirmation of this, our own seriesof streptococcal infections (Fig. 9) showed noconduction abnormalities unless rheumaticfever developed. It is clear that detectableabnormality of atrioventricular conductionoccurs in a high percentage of patients withrheumatic fever (Keith, I938; Taran, I946;Blackman and Hamilton, 1948; Sokolow,I948; Alimurung and Massell, I956). Theabove evidence suggests that if these changes(including increased PR index, second andthird degree heart block, atrioventricular dis-sociation, and junctional rhythms) occur aftera haemolytic streptococcal infection, they arespecific for rheumatic fever.The exact mechanism by which the rheu-
matic process causes this vagal effect is un-known. Though Goldstein, Halpern, andRobert (1967) have shown an immunologicalrelation between the Group A streptococcusand the glycoprotein of cardiac valves, to dateno such relation with the glycoproteins ofconducting tissue has been described. Fur-thermore, the atrioventricular node has a verylow content of glycoprotein compared withthe peripheral conducting system (Gee, I969).It is possible that glycogen, of which thereis an abundance in the AV node (Otsuka andHara, I965), is the substance affected by therheumatic process. That glycogen is involvedin atrioventricular conduction is further impli-cated by the presence of a short PR intervalin the cardiac glycogen storage diseases(Ehlers et al., I962).
TABLE 2 His-bundle cardiogram in acuterheumatic fever
Heart P'R P'H HVrate interval interval interval
Resting sinus rhythm 68 I90 155 35Atrial pacing (continued throughout
remainder of test) I33 255 220 35Before atropine I33 255 220 3530 sec after atropine 133 205 175 3060 sec after atropine I33 i65 130 35120 sec after atropine 133 225 I90 35
All measurements are in milliseconds.
on February 17, 2020 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.34.5.472 on 1 May 1972. D
ownloaded from

478 Clarke and Keith
PR INDEX
1.5
'.14
1.3
1.2
11
101.0-~
t~~~~~~~~~~t." r09
. 08 *-" **~~~~~O......*07 " -
0.6
PR INDEX DURINGSTREPTOCOCCAL INFECTION
(51 PATIENTS)
PR INDEXIN SAME PATIENTS
2 to 6 WEEKS LATER
FIG. 9 PR index in 5i patients with strepto-coccal infection: acute stage compared with 2to 6 weeks later.
Studies on the incidence of prolongedatrioventricular conduction times in normaland abnormal children are scanty. A list ofconditions that may be associated with PRinterval changes is shown in Table 3. If thoseconditions can be ruled out, and one is dealingwith a child who has definite evidence of arecent streptococcal infection (usually a raisedantistreptolysin-O titre), the prolonged con-duction time becomes highly significant.
TABLE 3 PR prolongation in children
Diagnosis Per cent incidence ofPR prolongation ineach condition
L-transposition of great arteries 57Ebstein's anomaly 50Atrial septal defect 43Coarctation of aorta I2Total anomalous pulmonaryvenous drainage 8
Ventricular septal defect 6Persistent ductus arteriosus 3.4Pulmonary stenosis 3Tetralogy of Fallot 2Diphtheria CommonNormal children Very rare
Adapted from Keith, Rowe, and Vlad, I967.
Under such circumstances, it should be con-sidered for inclusion with the major Jones'criteria, with the provision that such signifi-cance only applies if the conduction time re-turns to normal, or significantly lower levels.In the absence of evidence of carditis, PRprolongation does not appear to have a badlong-term prognosis, but may carry the re-quirement for long-term antistreptococcalprophylaxis. Rheumatic fever can, of course,occur in the above congenital cardiac defectswhich have permanent prolongation of thePR interval. A further increase of PR indexduring the acute stage will still have the samesignificance as in a normal child.
Atrioventricular conduction abnormalitieswere found in 84 per cent of our patients withacute rheumatic fever, though in some patientsthey could only be identified in retrospectwhen the convalescent recording was com-pared with that taken in the acute stage.Junctional rhythm, sometimes with atrioven-tricular dissociation, is part of the abnormalresponse. The changing pattern of acute rheu-matic fever can make definite diagnosis diffi-cult (Feinstein and Spagnuolo, I962; Bester-man, I970). The judicious use of the PRindex with comparison of acute and quiescentstages may make the PR prolongation a moreimportant criterion in the diagnosis of acuterheumatic fever.
ReferencesAlimurung, M. M., and Massell, B. F. (1956). The
normal PR interval in infants and children.Circulation, 13, 257.
American Heart Association (I954). Report of theCommittees on Electrocardiography. Recommen-dations for standardization of electrocardiographicand vectorcardiographic leads. Circulation, I0, 564.
Ashman, R., and Hull, E. (1937). Essentials of Electro-cardiography. McMillan, New York.
Besterman, E. (1970). Editorial: The changing face ofacute rheumatic fever. British Heart Journal, 32,579.
Blackman, N. S., and Hamilton, C. I., Jr. (I948).Serial electrocardiographic changes in young adultswith acute rheumatic fever: report of 62 cases.Annals of Internal Medicine, 29, 4I6.
British Medical Journal (Ig95). Treatment of acuterheumatic fever in children. A co-operative clinicaltrial of A.C.T.H., cortisone, and aspirin. A JointReport by the MRC of Great Britain and theAmerican Heart Association. I, 555.
Cohn, A. E., and Swift, H. F. (1924). Electrocardio-graphic evidence of myocardial involvement inrheumatic fever. Journal of Experimental Medicine,39,31I
Cranefield, P. F., Hoffnan, B. F., and de Carvalho,A. P. (1958). Effects of acetylcholine on singlefibers of the atrioventricular node. CirculationResearch, 7, 19.
Cristal, N., Stern, J., and Gueron, M. (I97i). Atrio-ventricular dissociation in acute rheumatic fever.British Heart Journal, 33, 12.
on February 17, 2020 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.34.5.472 on 1 May 1972. D
ownloaded from
Atrioventricular conduction in acute rheumatic fever 479
Damato, A. N., Lau, S. H., Helfant, R., Stein, E.,Patton, R. D., Scherlag, B. J., and Berkowitz,W. D. (I969). A study of heart block in man usingHis bundle recordings. Circulation, 39, 297.
Ehlers, K. H., Hagstrom, J. W. C., Lukas, D. S.,Redo, S. F., and Engle, M. A. (I962). Glycogen-storage disease of the myocardium with obstructionto left ventricular outflow. Circulation, 25, 96.
Feinstein, A. R. (I966). The natural histories of acuterheumatic fever. Bulletin on Rheumatic Diseases, 17,423.
Feinstein, A. R., and Spagnuolo, M. (I962). The clini-cal patterns of acute rheumatic fever; a reappraisal.Medicine, 41, 279.
*Gee, D. J. (I969). A glycoprotein in cardiac conductingtissue. British Heart3journal, 3I, 588.
Goldstein, I., Halpern, B., and Robert, L. (I967).Immunological relationship between streptococcusA polysaccharide and the structural glycoproteinsof heart valve. Nature (London), 213, 44.
Jones Criteria (i955). (Modified) for guidance in thediagnosis of rheumatic fever. American HeartAssociation, New York.
-*Jones Criteria (I965). (Revised) for guidance in thediagnosis of rheumatic fever. American HeartAssociation. Circulation, 32, 664.
Keith, J. D. (1938). Overstimulation of the vagus nervein rheumatic fever. Quarterly Journal of Medicine,7, 29.
Keith, J. D., Rowe, R. D., and Vlad, P. (I967). HeartDisease in Infancy and Childhood, 2nd ed., p. I052.Macmillan, New York; Collier-Macmillan, Lon-
u don.Levander-Lindgren, M. (I952). Electrocardiographic
studies in scarlet fever. Acta Paediatrica, Suppl. 9I,pp. I-2II.
Mirowski, M., Rosenstein, B. J., and Markowitz, M.(I964). A comparison of atrio-ventricular conduc-tion in normal children and in patients with rheu-
w matic fever, glomerulonephritis and acute febrileillnesses. Pediatrics, 33, 334.
,Narula, 0. S., Scherlag, B. J., Samet, P., and Javier,R. P. (I97i). Atrioventricular block. Localization
and classification by His bundle recordings.American Journal of Medicine, 50, I46.
Otsuka, N., and Hara, T. (I965). Gross demonstrationof the mammalian atrioventricular bundle by aperiodic acid-Schiff procedure. Stain Technology,40, 305.
Parkinson, J., Gosse, A. H., and Gunson, E. B. (I920).The heart and its rhythm in acute rheumatism.Quarterly Journal of Medicine, 13, 363.
Rammelkamp, C. H., Jr., and Stolzer, B. L. (I954).The treatment and prevention of rheumatic fever.Pediatric Clinics of North America, I, 265.
Rantz, L. A., Boisvert, P. J., and Spink, W. W. (1945).The etiology and pathogenesis of rheumatic fever.Archives of Internal Medicine, 76, I31.
Rantz, L. A., Spink, W. W., and Boisvert, P. J. (1946).Abnormalities in the electrocardiogram followinghemolytic streptococcus sore throat. Archives ofInternal Medicine, 77, 66.
Roberts, N. K., and Olley, P. M. (I97i). His bundleelectrocardiography in children. Proceedings of theCanadian Federation of Biological Societies, 14, 122.
Rodriguez-Coronel, A., and Miller, R. A. (I969).Accelerated nodal pacemaker. Pediatrics, 43, 430.
Sodi-Pallares, D., Portillo, B., Cisneros, F., de la Cruz,M. V., and Acosta, A. R. (I958). Electrocardio-graphy in infants and children. Pediatric Clinics ofNorth America, 5, 87I.
Sokolow, M. (I948). Significance of electrocardiogra-phic changes in rheumatic fever. American Journalof Medicine, 5, 365.
Taran, L. M. (1946). Laboratory and clinical criteriaof rheumatic carditis in children. J7ournal of Pedi-atrics, 29, 77.
Ziegler, R. F. (I95I). Electrocardiographic Studies inNormal Infants and Children. Charles C. Thomas,Springfield, Illinois.
Requests for reprints to Dr. Malcolm Clarke,Department of Cardiology, St. Bartholomew'sHospital, London E.C.i.
t
il. t
on February 17, 2020 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.34.5.472 on 1 May 1972. D
ownloaded from