atrial tachycardia in a patient with extracardiac conduit fontan...
TRANSCRIPT

37
ECG
& E
P C
ASE
S
VOL.15 NO.4
Introduction
Thesurvivalrateofpatientswithcomplexcon-
genitalheartdiseasehasrecentlyimproved,most
likely due to the development of new surgical
techniques and improved perioperative medical
management.1Asthenumberofadultpatients
withcongenitalheartdiseasehasincreased,ar-
rhythmiasandheartfailurearebecominggrow-
ingissuesinthesepatients.1Thus,itisnotsur-
prising that the demand for electrophysiologic
(EP) studiesand radiofrequency catheterabla-
tion(RFCA)isincreasing.EPstudiesandRFCA
arechallenginginpatientswhohaveundergone
extracardiac conduitFontanprocedures for the
palliativetreatmentofcongenitalheartdisease,
becausethesystemicvenousbloodisnotdrained
intotheheartinthesetechniques.Here,were-
portacaseoffocalatrialtachycardia,whichwas
ablatedviaatrans-conduitpunctureinapatient
whohadundergoneanextracardiacconduitFon-
tanprocedure.
Case
A14-year-oldmalepatientvisitedtheemer-
gency room complaining of palpitations for 3
Received: May 28, 2014Accepted: December 15, 2014Correspondence: Jae-Sun Uhm, MD, Department of Cardiology, Severance Cardiovascular Hospital, 50 Yonsei-ro Seodaemun-gu, Seoul, Korea, 120-752Tel: +82-2-2228-8441, Fax: +82-2-2227-7732 E-mail: [email protected] Ko, MD, PhD, Division of Cardiology
ABSTRACT
Electrophysiology (EP) studies and radiofrequency catheter ablation (RFCA) are challenging in patients who have undergone extracardiac conduit Fontan procedures, because of the difficult vascular access. Here, we report on a 14-year-old male patient who underwent extracardiac conduit Fontan procedure for a double-inlet left ventricle, complete transposition of the great arteries, and large ventricular septal defect. The EP study was performed via a trans-conduit puncture. Focal atrial tachycardia originating from the mid portion of the interatrial septum was induced. RFCA of the origin of atrial tachycardia was successfully performed. EP studies and RFCA are feasible via a trans-conduit puncture in patients with extracardiac conduit Fontan circulation.
Key words: ■ atrial tachycardia ■ congenital heart disease ■ Fontan procedure
연세대학교 의과대학 내과학교실 엄 재 선, 김 남 균, 박 진 규, 정 보 영, 박 희 남, 이 문 형
Jae-Sun Uhm, MD1; Nam Kyun Kim, MD2; Jin-Kyu Park, MD1; Boyoung Joung, MD1; Hui-Nam Pak1; Moon-Hyoung Lee1
Departments of Cardiology1 and Pediatric Cardiology2, Arrhythmia Center, Severance Cardiovascular Hospital, Yonsei University College of Medicine, Seoul, Korea
Atrial Tachycardia in a Patient with Extracardiac Conduit Fontan Circulation
ECG
& E
P C
ASE
S
38 The Official Journal of Korean Heart Rhythm Society
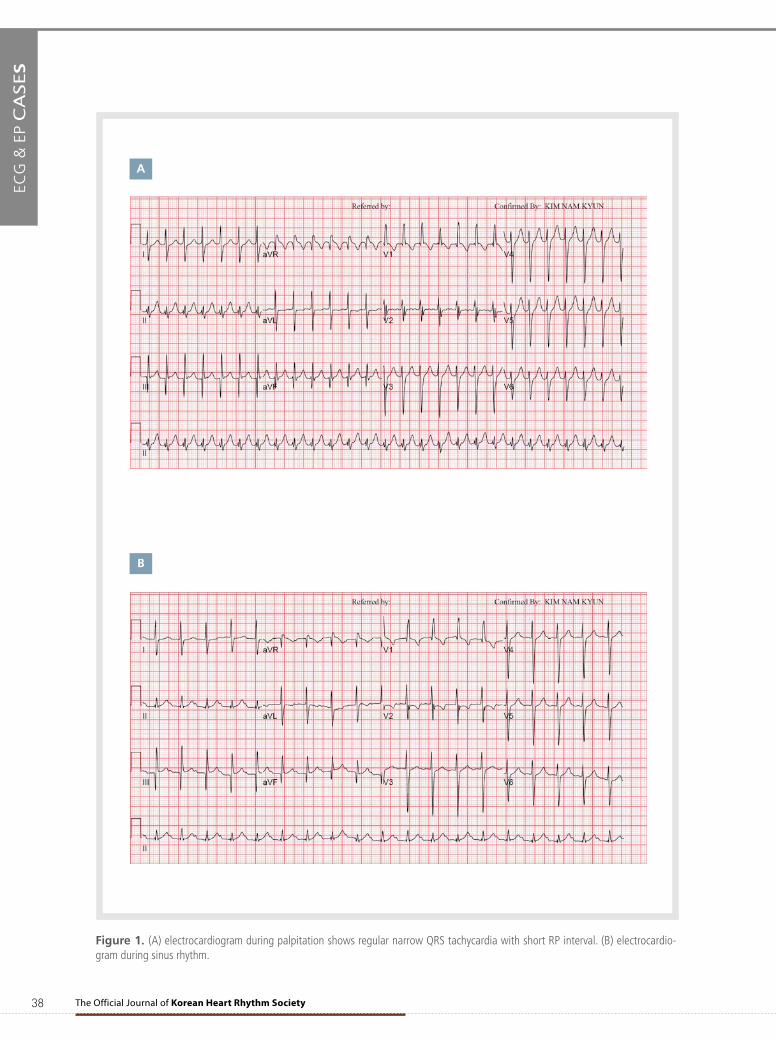
Figure 1. (A) electrocardiogram during palpitation shows regular narrow QRS tachycardia with short RP interval. (B) electrocardio-gram during sinus rhythm.
A
B
39
ECG
& E
P C
ASE
S
VOL.15 NO.4
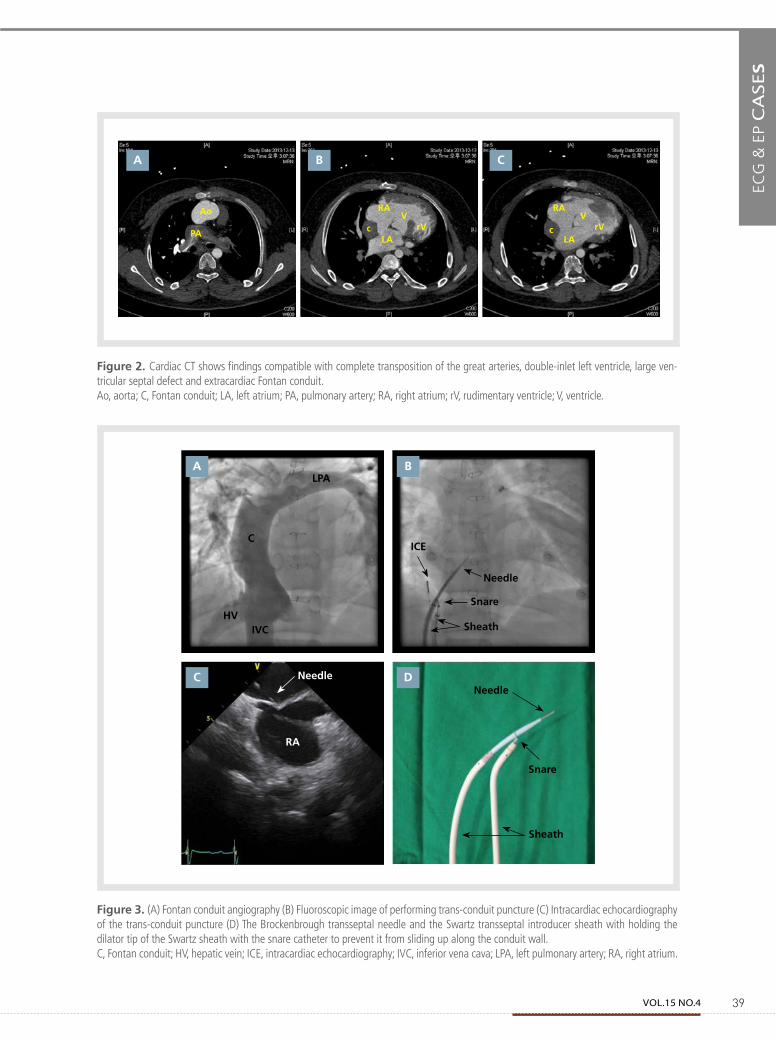
Figure 2. Cardiac CT shows findings compatible with complete transposition of the great arteries, double-inlet left ventricle, large ven-tricular septal defect and extracardiac Fontan conduit. Ao, aorta; C, Fontan conduit; LA, left atrium; PA, pulmonary artery; RA, right atrium; rV, rudimentary ventricle; V, ventricle.
Figure 3. (A) Fontan conduit angiography (B) Fluoroscopic image of performing trans-conduit puncture (C) Intracardiac echocardiography of the trans-conduit puncture (D) The Brockenbrough transseptal needle and the Swartz transseptal introducer sheath with holding the dilator tip of the Swartz sheath with the snare catheter to prevent it from sliding up along the conduit wall. C, Fontan conduit; HV, hepatic vein; ICE, intracardiac echocardiography; IVC, inferior vena cava; LPA, left pulmonary artery; RA, right atrium.
A B C
Ao RA RAV
rV rVLA LA
V
PA c c
A B
C D
LPA
C
HVIVC
ICE
Needle
Snare
Needle
Snare
Sheath
Sheath
Needle
RA
ECG
& E
P C
ASE
S
40 The Official Journal of Korean Heart Rhythm Society
hours. He had experienced several episodes of
palpitationsduringthepastyear.Hisbloodpres-
sure was 82/49mmHg. The electrocardiogram
(ECG)showedregular,narrowQRStachycardia
witharateof160beats/minandashortRPin-
terval(Figure1A).Intheemergencyroom,the
tachycardia spontaneously converted into sinus
rhythm(Figure1B).TheQRSmorphologyofthe
tachycardiawassimilartothatinsinusrhythm.
When he was 10 days old, he was diagnosed
withdouble-inletleftventricle(DILV),complete
transposition of the great arteries (TGA), and
large ventricular septal defect (VSD).Whenhe
was5monthsold,thebidirectionalcavopulmo-
naryshuntandinteratrialseptectomywereper-
formedforpalliation.At theageof1year,an
extracardiacconduitFontanprocedurewasper-
formedwiththeautologouspericardium.Wede-
cidedtoperformtheEPstudyfordiagnosisand
treatmentofthetachycardia.Cardiaccomputed
tomography(CT)wasperformedforassessment
oftheheartanatomy,showingfindingscompat-
iblewithTGA,DILV,largeVSD,functionalsingle
ventricle,andextracardiacFontanconduit(Fig-
ure2).
Both femoral veins were punctured. Conduit
angiography was performed with a Berman-
typeangiographycatheter(ArrowInternational,
Reading,PA,USA)(Figure3A).TwoSR-0Swartz
transseptalintroducersheath(StJudeMedical,St
Paul,MN,USA),asnarecatheter(PFMMedi-
cal,Nonnweiler,Germany),andanintracardiac
echocardiography catheter (AcuNav, Siemens,
MountainView,CA,USA)wereinsertedintothe
Fontanconduitviathefemoralveins.ABRK-1
Brockenbroughtransseptalneedle(StJudeMedi-
cal)wasinsertedintotheSwartzsheath,andthe
dilatortipoftheSwartzsheathwasheldwiththe
snarecathetertopreventitfromslidingupalong
theconduitwall(Figure3BandD).Wepunctured
thewallbetweentheconduitandtherightatrium
withtheBrockenbroughtransseptalneedleunder
intracardiac echocardiography guidance (Figure
3C).Right and left atriographywas performed
with thepigtail catheter via the trans-conduit
puncture. A deflectable decapolar catheter (St
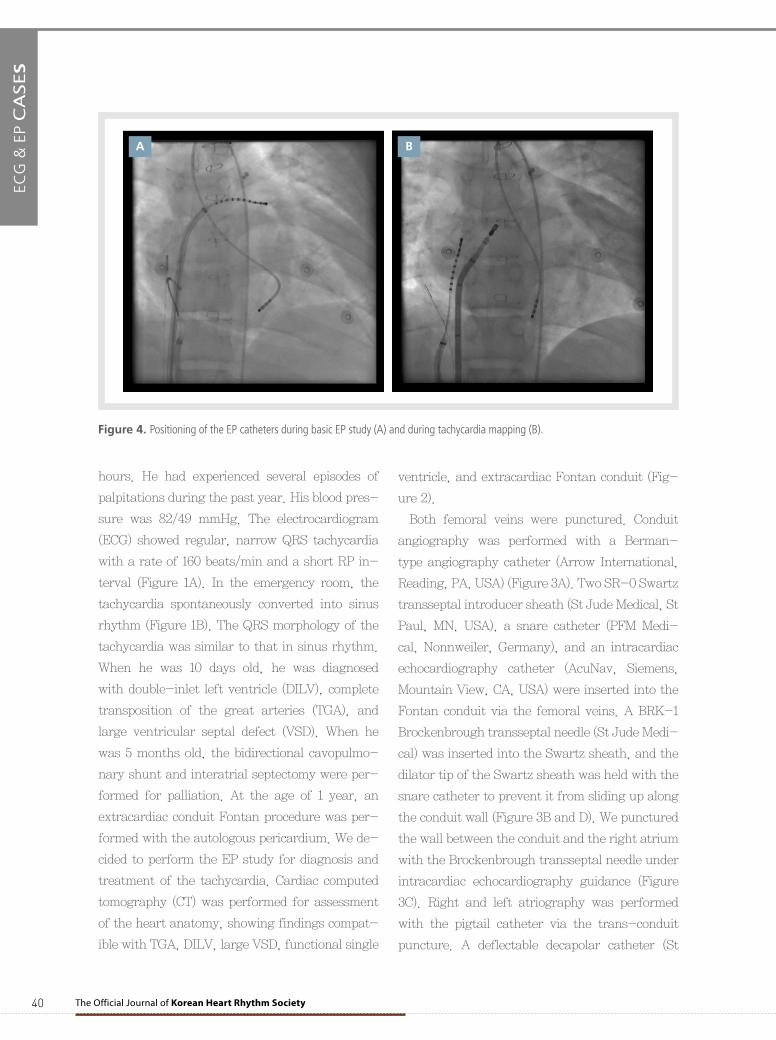
Figure 4. Positioning of the EP catheters during basic EP study (A) and during tachycardia mapping (B).
A B
41
ECG
& E
P C
ASE
S
VOL.15 NO.4
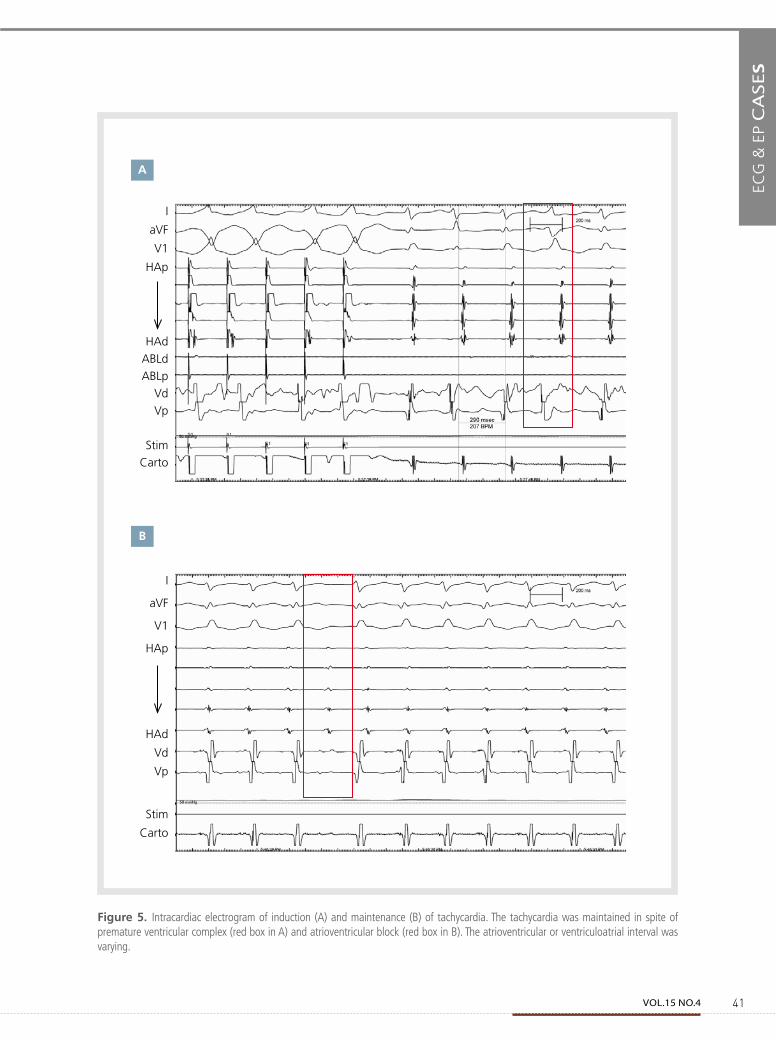
Figure 5. Intracardiac electrogram of induction (A) and maintenance (B) of tachycardia. The tachycardia was maintained in spite of premature ventricular complex (red box in A) and atrioventricular block (red box in B). The atrioventricular or ventriculoatrial interval was varying.
A
B
I
aVF
V1
HAp
HAd
ABLd
ABLp
Vd
Vp
Stim
Carto
I
aVF
V1
HAp
HAd
Vd
Vp
Stim
Carto
ECG
& E
P C
ASE
S
42 The Official Journal of Korean Heart Rhythm Society
A B
JudeMedical)wasplacedinthehighleftatrium
viatheSwartzsheathandadecapolarcatheter
(StJudeMedical)wasplacedintheventriclevia
the aorta (Figure 4A). The initial rhythmwas
normal sinus rhythm.During ventricular pac-
ingandsingleventricularextrastimuli,theatrial
electrogramshowedone-to-oneventriculoatrial
conductionwithdecrementalproperties.During
theatrialpacingof240msandinfusionofiso-
proterenolatarateof2μg/min,tachycardiawith
a290mscyclelengthwasinduced.Tachycardia
wasmaintaineddespitethepresenceofapre-
matureventricularcomplexandatrioventricular
block (Figure 5A and B). Therefore, atrioven-
tricularreentranttachycardiacouldbeexcluded.
Duringtachycardia,theatrioventricularorven-
triculoatrialintervalvaried(Figure5B).Itwasnot
compatiblewithatrioventricularnodalreentrant
tachycardia.Thetachycardiawasnotentrainable
byventricularpacing.Thedecapolarcatheterwas
movedtotherightatrium(RA)sideintheFontan
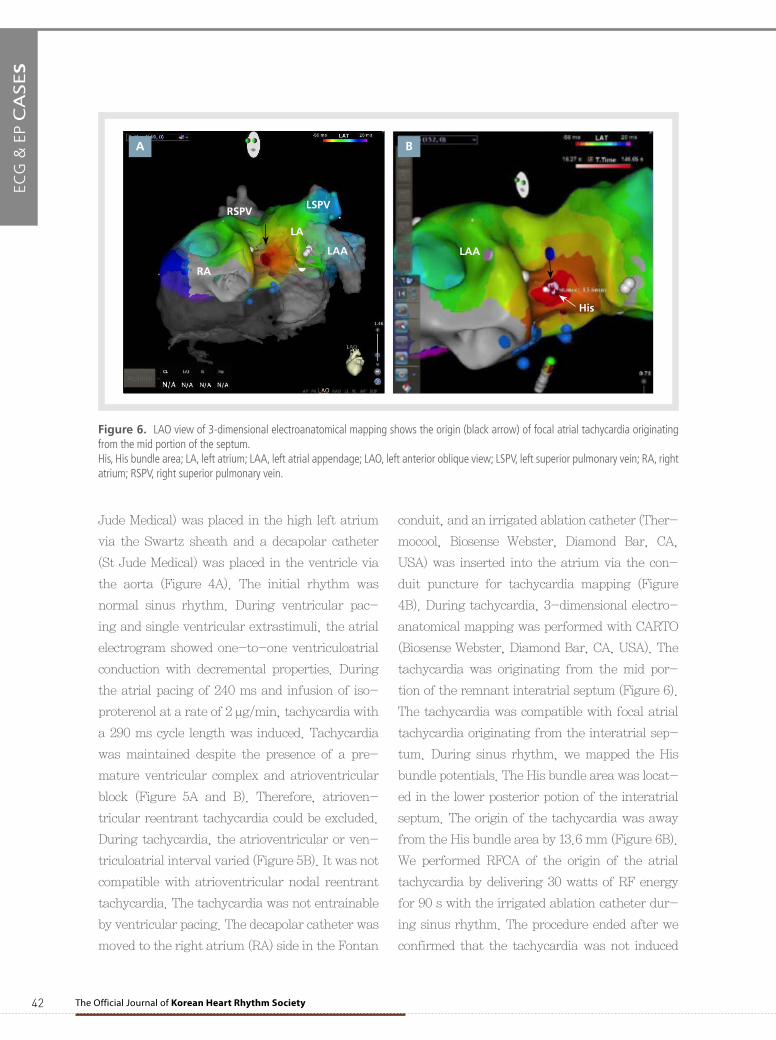
conduit,andanirrigatedablationcatheter(Ther-
mocool, Biosense Webster, Diamond Bar, CA,
USA)wasinsertedintotheatriumviathecon-
duit puncture for tachycardiamapping (Figure
4B).Duringtachycardia,3-dimensionalelectro-
anatomicalmappingwasperformedwithCARTO
(BiosenseWebster,DiamondBar,CA,USA).The
tachycardiawasoriginatingfromthemidpor-
tionoftheremnantinteratrialseptum(Figure6).
Thetachycardiawascompatiblewithfocalatrial
tachycardiaoriginatingfromtheinteratrialsep-
tum.Duringsinusrhythm,wemappedtheHis
bundlepotentials.TheHisbundleareawaslocat-
edinthelowerposteriorpotionoftheinteratrial
septum.Theoriginofthetachycardiawasaway
fromtheHisbundleareaby13.6mm(Figure6B).
WeperformedRFCAof theoriginof theatrial
tachycardiabydelivering30wattsofRFenergy
for90swiththeirrigatedablationcatheterdur-
ingsinusrhythm.Theprocedureendedafterwe
confirmedthatthetachycardiawasnotinduced
Figure 6. LAO view of 3-dimensional electroanatomical mapping shows the origin (black arrow) of focal atrial tachycardia originating from the mid portion of the septum. His, His bundle area; LA, left atrium; LAA, left atrial appendage; LAO, left anterior oblique view; LSPV, left superior pulmonary vein; RA, right atrium; RSPV, right superior pulmonary vein.
RA
RSPVLSPV
LAA LAA
His
LA

43
ECG
& E
P C
ASE
S
VOL.15 NO.4
bytheprogrammedelectricstimulationandiso-
proterenolinfusion.Thepatienthadnosymptom
andmaintainedsinusrhythmfor6monthsafter
RFCA.
Discussion
Thecasewasfocalatrialtachycardiaoriginat-
ingfromtheseptuminapatientwhohadunder-
goneanextracardiacconduitFontanprocedure.
WeperformedanEPstudyandRFCAoftheori-
ginofthefocalatrialtachycardiasuccessfullyvia
thetrans-conduitpuncture.
The lifelong prevalence of atrial tachycardia
inpatientswithextracardiacFontancirculation
is approximately 50%,2-4 and it is considerably
higherthaninthenormalpopulation.Inpatients
withextracardiacconduitFontancirculation, it
isdifficulttoperformanEPstudy,becausethe
heart iscompletelyexcluded fromthesystemic
venous system. There were previous case re-
portsofEPstudiesandRFCAviavariousroutes
in patients with Fontan circulation, including
viaatrans-thoracicpuncture,sternotomyap-
proach, trans-apical access and trans-conduit
puncture.5-8TheEPcatheterscanbetransvas-
cularlyplacedvia2pathways:thetrans-conduit
puncture and retrograde transaortic approach.
Theapproachviathetrans-conduitpunctureis
suitableforgainingaccesstotheatriumandthe
retrograde transaortic approach is suitable for
gainingaccesstotheventricle.Itischallenging
topuncturetheFontanconduitbecausefibrosis
formsaroundtheconduit.Inaddition,thecon-
duitwallisvertical—unliketheinteratrialsep-
tum—andthetransseptalneedletendstoslideup
alongtheconduitwallinsteadofpuncturingit.
TheuseofaBrockenbroughtransseptalneedle
whileholdingthedilatortipoftheSwartzsheath
with a snare catheter is a useful method for
puncturing theFontanconduit.9A large-curve
BRK-1transseptalneedleissuperiortoasmall-
curveBRKneedle.Moreover,theradiofrequency
transseptalneedlecanbeagoodoptionforpunc-
turingthefibroticFontanconduit.
Inpatientswithcongenitalheartdisease,the
EPstudyandRFCAareverychallengingbecause
oftheunusualanatomyoftheheart.Inaddition,
itiscommonforpatientstohavevascularanom-
aliesincludingapersistentleftsuperiorvenacava
andinferiorvenacavainterruption.Itisimpor-
tantthattheoperatorbecompletelyawareofthe
anatomy of heart and vessels of each patient.
Everypatienthasauniqueheartstructure,even
thoughthispatientgrouphasthesamediagnosis
ofcongenitalheartdisease.Theoperatorneeds
to review and understand the previous cardiac
surgery and intervention. The operator should
makeameticulousplanfortheprocedure,taking
intoconsiderationthetypesofEPcatheterstobe
usedforeachchamber,pathwaystobeusedfor
positioningoftheEPcatheters,andappropriate
anglesfortheX-raybeamtoimprovevisualiza-
tion.Theoperatorneedstodiscussthecurrent
hemodynamicsand long-termprognosisof the
patientwiththepediatriccardiologists.Giventhe
complexheartanatomy,cardiacCTanda3-di-
mensional electroanatomicmapping systemare
necessaryforguidingtheprocedure.Intracardiac
echocardiography can be helpful for real-time
visualizationof theanatomyandEPcatheters.
Theactivatedcoagulationtimeshouldbemain-
tainedat350–400msbyheparininfusionduring
theEPstudyinpatientswithasingleventricle,
asthecathetersareplacedinthesystemiccham-
bers.
In the present case, the remnant interatrial
septummightbecomearrhythmogenicaftersep-
tectomyduetodegenerativechangesofthein-
teratrialseptum.Thispatientislikelytodevelop

ECG
& E
P C
ASE
S
44 The Official Journal of Korean Heart Rhythm Society
atrial tachyarrhythmia originating from other
parts of the atrium. In addition, an advanced
atrioventricular block can occur in the future,
althoughtheperi-proceduralECGshowedfirst
degreeatrioventricularblock.Thus,thepatient
willrequirelong-termfollow-up.
Conclusion
EPstudiesandRFCAarefeasibleviaatrans-
conduit puncture in patients with extracardiac
conduitFontancirculation.
References
1. Mackie AS, Ionescu-Ittu R, Therrien J, Pilote L, Abrahamowicz M, Marelli AJ. Children and adults with congenital heart disease lost to follow-up; who and when? Circulation. 2009;120:302-309.
2. Gelatt M, Hamilton RM, McCrindle BW, Gow RM, Williams WG, Trusler GA, Freedom RM. Risk factors for atrial tachyarrhythmias after the Fon-tal operation. J Am Coll Cardiol. 1994;24:1735-1741.
3. Weipert J, Noebauer C, Schreiber C, Kostolny M, Zrenner B, Wacker A, Hess J, Lange R. Occurrence and management of atrial arrhythmia after long-term Fontan circulation. J Thorac Cardiovasc Surg. 2004;127:457-464.
4. Lasa JJ, Glatz AC, Daga A, Shah M: Prevalence of arrhythmias late after the Fontan operation. Am J Cardiol. 2014;133:1184-1188.
5. Nehgme R, Carboni MP, Care J, Murphy JD. Transthoracic percutane-ous access for electroanatomic mapping and catheter ablation of atrial tachycardia in patients with a lateral tunnel Fontan. Heart Rhythm. 2006;3:37-43.
6. Khairy P, Fournier A, Ruest P, Vobecky SJ. Transcatheter ablation via a sternotomy approach as a hybrid procedure in a univentricular heart. Pacing Clin Electrophysiol. 2008;31:639-640.
7. Brown SC, Boshoff DE, Rega F, Eyskens B, Budts W, Heidbuechel H, Meyns B, Gewillig M. Transapical left ventricular access for difficult to reach interventional targets in the left heart. Catheter Cardiovasc In-terv. 2009;74:137-142.
8. Dave AS, Aboulhosn J, Child JS, Shivkumar K. Transconduit puncture for catheter ablation of atrial tachycardia in a patient with extracardiac Fontan palliation. Heart Rhythm. 2010;7:413-416.
9. Aoki H, Nakamura Y, Takeno S, Takemura T. A new procedure for a trans-conduit puncture by grasping the dilator tip with a snare catheter: an alternative access method during catheter ablation of supraventricular tachycardias after an extracardiac Fontan operation. Heart Rhythm. 2013. doi: 10.1016/j.hrthm.2013.10.036 [Epub ahead of print] .