arthrographic hydrodistension for frozen shoulder · pdf filearthrographic hydrodistension for...
TRANSCRIPT
ARTHROGRAPHIC HYDRODISTENSION FOR FROZEN SHOULDERA Physiotherapy-led initiative in Primary Care
Authors:
Eoin Ó Conaireeoin.o’[email protected]
Dr. Jeremy [email protected]
The Challenge
Frozen shoulder is a common shoulder problem characterised by relentless pain, severe sleep disturbance, substantial morbidity and loss of function for a protracted period of up to two years (Neviaser 1987). The genders are affected equally with a peak onset of 52 years for men and 55 for women. Prevalence rates are reported as 2% - 5% for the general population and 10% - 20% for people with diabetes (Anton 1993). Encouragingly, early intervention in the form of guided glenohumeral intra-articular distension procedures has demonstrated significant improvement (Buchbinder 2004) with a numbers needed to treat figure of 2 for pain reduction and 3 for improvement in movement and function .
Current practiceGlenohumeral joint distension is currently performed in hospitals. The care pathway typically involves referral by the GP to Orthopaedics followed by referral to Radiology followed by review in Orthopaedics. The current pathway is time consuming (up to 18 weeks) and expensive.
The ResponseAppropriately trained physiotherapists to perform arthrographic joint distension for people with frozen shoulder in primary care.
Earlier, more efficient and cost effective care closer to the patient’s home using one location for assessment, intervention and follow-up.
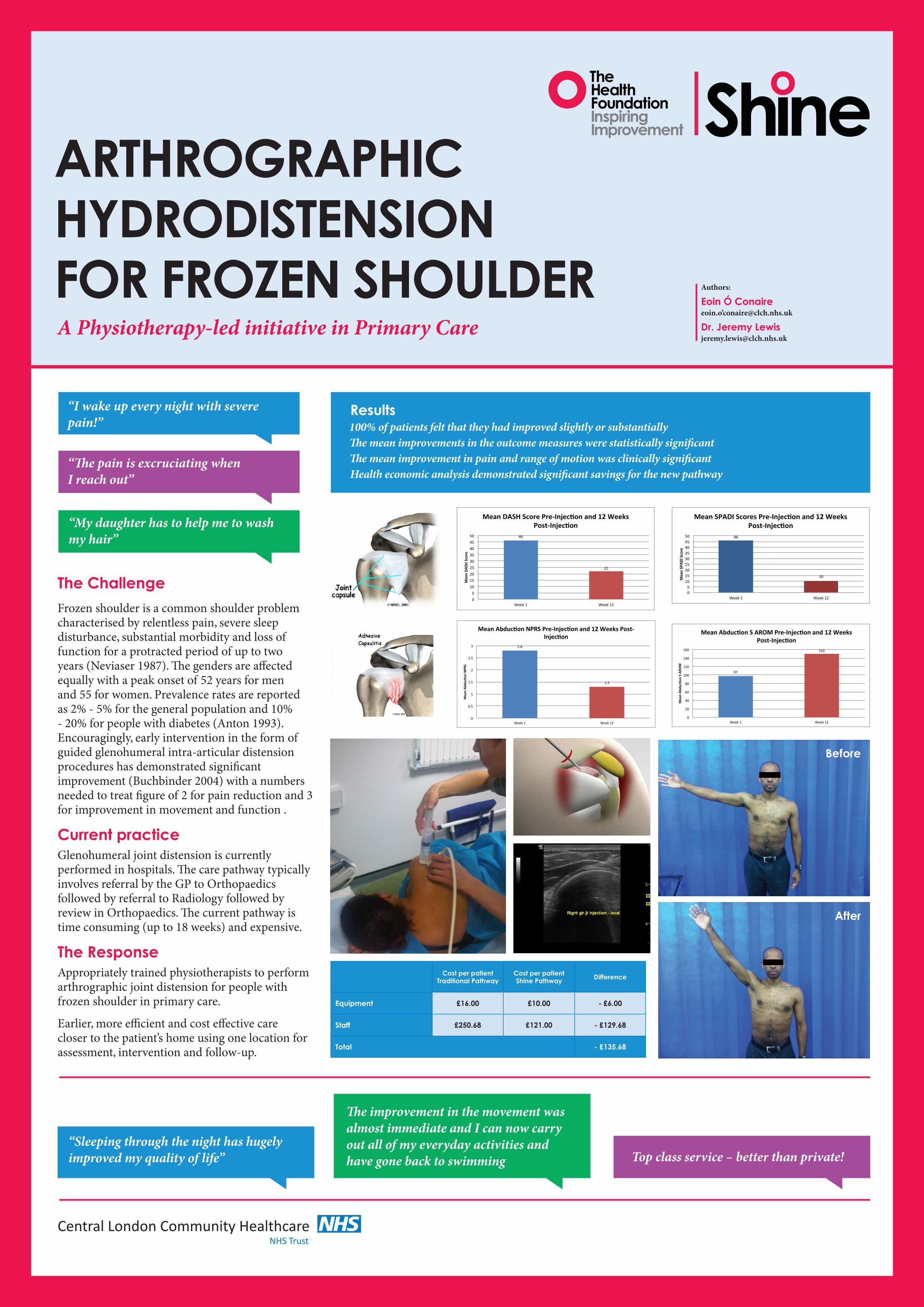
Results100% of patients felt that they had improved slightly or substantiallyThe mean improvements in the outcome measures were statistically significantThe mean improvement in pain and range of motion was clinically significantHealth economic analysis demonstrated significant savings for the new pathway
“I wake up every night with severe pain!”
“The pain is excruciating when I reach out”
“My daughter has to help me to wash my hair”
“Sleeping through the night has hugely improved my quality of life”
The improvement in the movement was almost immediate and I can now carry out all of my everyday activities and have gone back to swimming Top class service – better than private!
Cost per patient Traditional Pathway
Cost per patient Shine Pathway Difference
Equipment £16.00 £10.00 - £6.00
Staff £250.68 £121.00 - £129.68
Total - £135.68
46
22
0
5
10
15
20
25
30
35
40
45
50
Week1 Week12
MeanDASHScore
MeanDASHScorePre‐Injec1onand12Weeks
Post‐Injec1on
97
150
0
20
40
60
80
100
120
140
160
Week1 Week12
MeanAbduc+onSAROM
MeanAbduc+onSAROMPre‐Injec+onand12Weeks
Post‐Injec+on2.8
1.3
0
0.5
1
1.5
2
2.5
3
Week1 Week12
MeanAbduc+onNPRS
MeanAbduc+onNPRSPre‐Injec+onand12WeeksPost‐
Injec+on
46
10
0
5
10
15
20
25
30
35
40
45
50
Week1 Week12
MeanSPADIScore
MeanSPADIScoresPre‐Injec1onand12Weeks
Post‐Injec1on
Central London Community HealthcareNHS Trust
Before
After