aromatase inhibitor therapy for early breast cancer. giorgio mustacchi centro oncologico università...
TRANSCRIPT

Aromatase inhibitor therapy for early breast cancer.
Giorgio Mustacchi
Centro Oncologico
Università di Trieste

LowLow
IntermediateIntermediate
HighHigh
Node –Node –HER2 –HER2 –LVI absentLVI absent
Node –, HER2+ or LVI presentNode + (1-3) and HER2 -
Node + (1-3) and HER2 +Node + 4
G1G1TT22
AGE < 35G2-3 T>2
RRIISSKK
RRIISSKK
ST. GALLEN 2005:ST. GALLEN 2005: DEFINITIONS OF RISK DEFINITIONS OF RISK

2000 Oxford Overview: ER Status is not a prognostic factor
N- N+
EBCTCG, Lancet 2005EBCTCG, Lancet 2005
No Treatment arm

Overall survival ∆:
MA-17 N+ (HR: 0.61, p=0.04), IES (HR: 0.83, p=0.05)
Trial Design F/U N ∆ in DFS
ATAC
(Lancet 2005)A vs T vs AT
(double-blind)~ 5 yr 9366
2.5%-3.0%
BIG 1-98
(ESMO 2006)
T vs Let
(double-blind)~ 4 yr
8028
(4922)~ 3%
ABCSG-8 ARNO95
(Lancet 2005)
T Ana vs T
(open label)~ 3 yr 3224 3%
IES
(ASCO 2006)T Exe vs T (double-blind)
~ 5 yr
(2-3 post-treat)
4724 3.5%
MA.17
(JNCI 2005)L vs Placebo
(double-blind)~ 3 yr 5187 4.6%
Key Aromatase Inhibitors TrialsAll Favor AI Arm
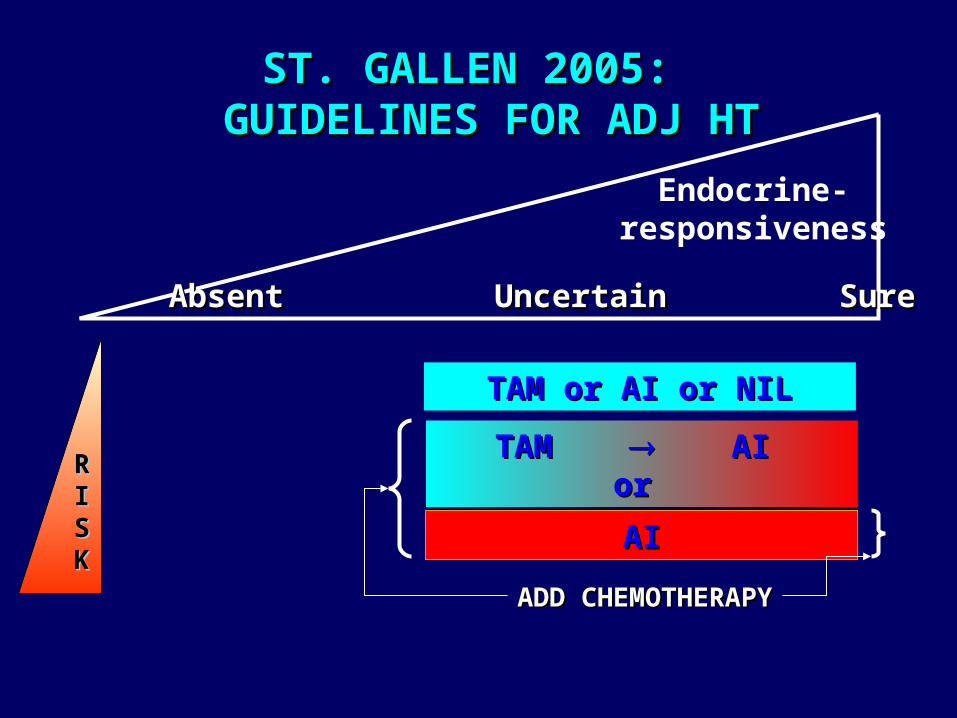
RRIISSKK
TAM or AI or NILTAM or AI or NIL
TAM TAM AI AI or or
ADD CHEMOTHERAPYADD CHEMOTHERAPY
AIAI
Endocrine-responsiveness
AbsentAbsent Uncertain Uncertain SureSure
ST. GALLEN 2005: ST. GALLEN 2005: GUIDELINES FOR ADJ HT GUIDELINES FOR ADJ HT

Neoadjuvant IMPACT:Short Term Predictors for ATAC?
HR 95.2% CI P Value
ANA vs TAM 0.83 0.71-0.96 0.0129Comb vs TAM 1.02 0.88-1.18 0.7718
Anastrozole
Tamoxifen
Combination
Time to event (mo)
Pro
po
rtio
n e
ve
nt-
fre
e (
%)
0
80
85
90
95
100
0 6 12 18 24 30 36 42
ATACn 9366 pts DFS 33 mo
A C
IMPACTn 330 pts Clinical OR 12 wks Biological Ki67 2 wks
T
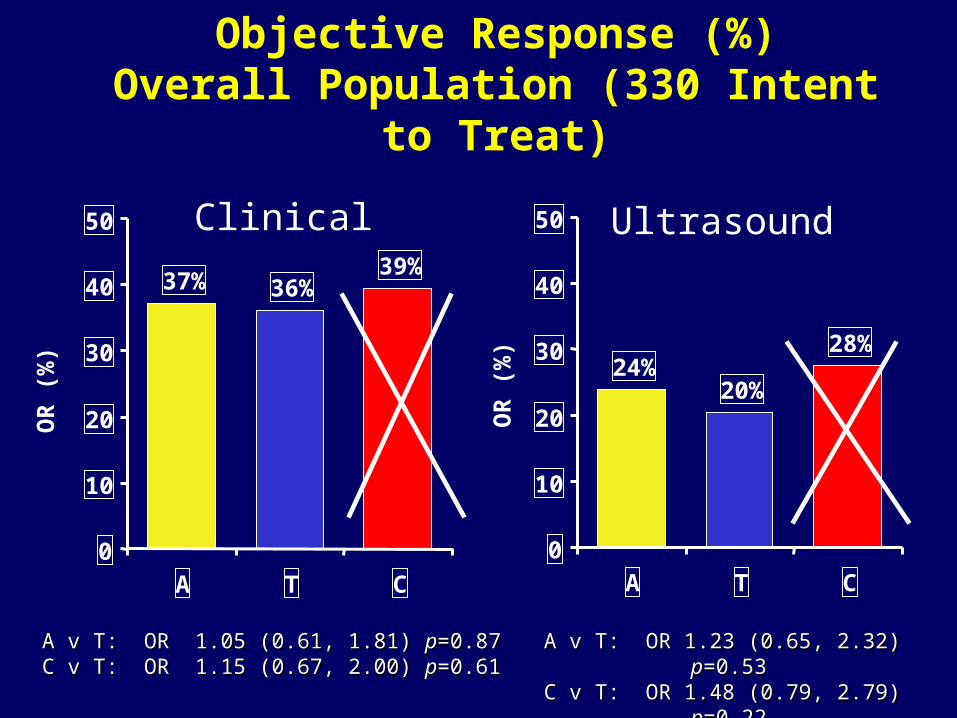
24%20%
28%
0
10
20
30
40
50
A T C
39%36%37%
0
10
20
30
40
50
A T C
Objective Response (%)Overall Population (330 Intent to Treat)
OR
(%
)
A v T: OR 1.05 (0.61, 1.81) A v T: OR 1.05 (0.61, 1.81) pp=0.87=0.87 C v T: OR 1.15 (0.67, 2.00) C v T: OR 1.15 (0.67, 2.00) pp=0.61 =0.61
OR
(%
)
A v T: OR 1.23 (0.65, 2.32) A v T: OR 1.23 (0.65, 2.32) pp=0.53=0.53C v T: OR 1.48 (0.79, 2.79) C v T: OR 1.48 (0.79, 2.79) pp=0.22=0.22
Clinical Ultrasound

EARLY BREAST CANCER TREATMENT:LESSONS LEARNED FROM CLINICAL TRIALS
An intervention produces, on average, a 50% An intervention produces, on average, a 50% relative risk reduction in relapserelative risk reduction in relapse
Higher risk women will, on Higher risk women will, on average, derive a greater absolute average, derive a greater absolute
benefit
20%20%
10%10%
40%40%
20%20%
Initial riskInitial riskFinal riskFinal risk
N-N- N+N+
There is heterogeneity in the There is heterogeneity in the magnitude of treatment magnitude of treatment
benefit !benefit !
Subset A:70% relative
risk reduction
Subset A:70% relative
risk reduction
Subset B:Subset B:<30% <30% relative risk reductionrisk reduction
Subset B:Subset B:<30% <30% relative risk reductionrisk reduction

# Gene profile = # pCR
Molecular Type % pCR 95% CI
Basal-like 45 24-68
HER2 + 45 24-68
Luminal A & B 6 1 - 21
Rouzier , Clin Cancer Res. 2005
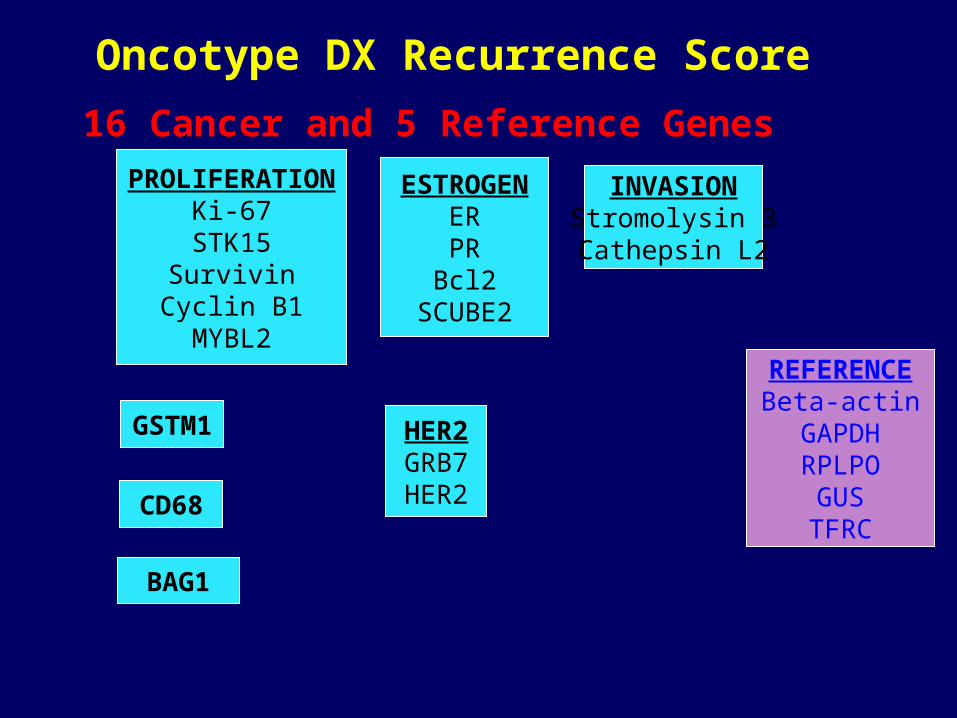
Oncotype DX Recurrence Score
REFERENCEBeta-actinGAPDHRPLPO
GUSTFRC
PROLIFERATIONKi-67
STK15Survivin
Cyclin B1MYBL2
ESTROGENERPR
Bcl2SCUBE2
INVASIONStromolysin 3Cathepsin L2
HER2GRB7HER2
BAG1
GSTM1
CD68
16 Cancer and 5 Reference Genes

0 2 4 6 8 10 12 14 16
Years
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
DR
FS
Low R isk (R S < 18) Intermediate R isk (R S 18 - 30) H igh R isk (RS 31)
NSABP B14-Results: Benefit from Tamoxifen
Paik, NEJM 2005
Tam:High RS
DFS = Placebo

AROMATASE INHIBITORS AND TAMOXIFEN: AROMATASE INHIBITORS AND TAMOXIFEN: HETEROGENEITY IN THE TREATMENT EFFECTHETEROGENEITY IN THE TREATMENT EFFECT
A
B
Subset A : Subset A : 70 % reduction ?70 % reduction ?
Subset B : Subset B : 30 % reduction ?30 % reduction ?
On average :On average :50 % reduction 50 % reduction in the odds of in the odds of
relapserelapse
molecular signature ?molecular signature ?
PGR ?PGR ? HER-2 ? HER-2 ? Other molecular markers ?Other molecular markers ?

EG
FR
HE
R2
Tam-S Tam-R
Knowlden et al. Endocrinology 144:1032, 2003
10% ‘conversion rate’ to HER2 overexpression in breast cancers that recur (early) on adjuvant tamoxifen (Gutierrez et al. J Clin Oncol 2005; 23:2469)
Tamoxifen-resistant breast tumors acquireErbB receptor overexpression


De Laurentiis et al. Clin. Cancer Res. 11:4741, 2005
ER+/HER2+ BC and endocrine therapy
N=1,925

HER2 + : predictive of resistence to any hormonal treatment ?
0
20
40
60
80
100
% RR
Letrozole Tam
Neoadjuvant Letrozole VS Tamoxifen
HER 2/3+ HER -
Ellis, JCO Sep 2001
020406080
100
% RR
ANA TAM
FISH + Overall
Dowsett, S. Antonio 03Neoadjuvant
Anastrozole VS Tamoxifen

ER+/PR- and hormonal treatment (ATAC trial)
From Cui et al. JCO 23:7721, 2005

Data are HRs and 95% CIs
HR Log Scale
Exemestane
better
Tamoxifen better
0.64 (0.51-0.79)
0.67 (0.39-1.16)
0.58 (0.38-0.90)
0.66 (0.51-0.87)
HR (95% CI)
0.4 0.6 0.8 1.0 1.2
Subgroup (n)
All ER+ (3853)
ER+/PgR unknown (499)
ER+/PgR- (735)
ER+/PgR+ (3853)
Coombes RC, et al. N Engl J Med. 2004;350:1081-1092.
IES 031: DFS According to ER/PgR
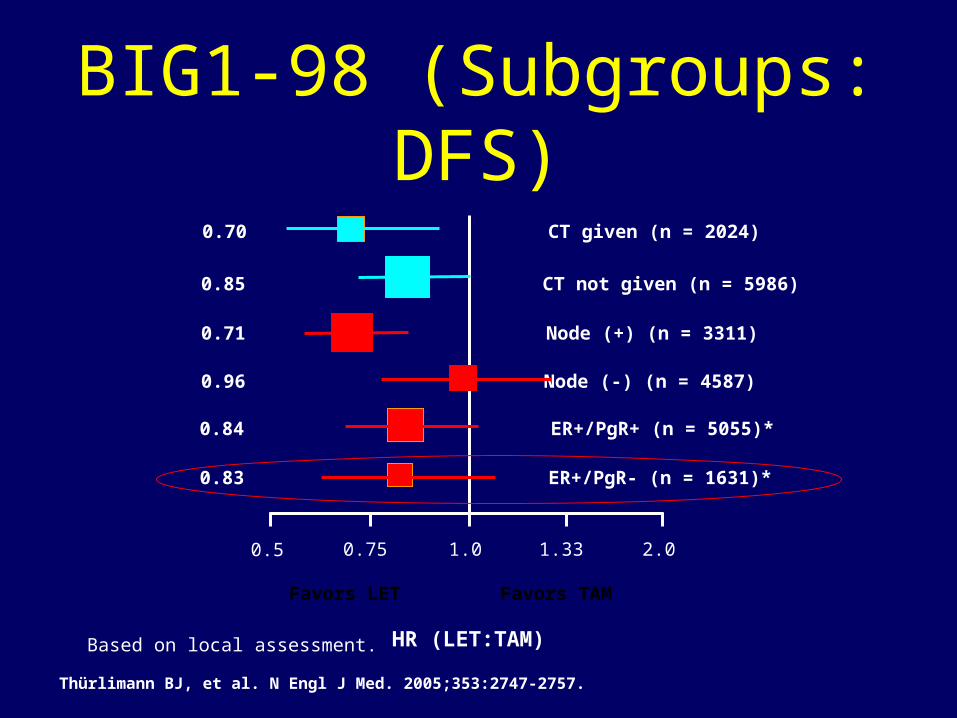
*Based on local assessment.
1.00.5 0.75 1.33 2.0
CT given (n = 2024)
CT not given (n = 5986)
0.70
0.85
Node (+) (n = 3311)
Node (-) (n = 4587)
0.71
0.96
ER+/PgR+ (n = 5055)*
ER+/PgR- (n = 1631)*
0.84
0.83
Favors LET Favors TAM
HR (LET:TAM)
Thürlimann BJ, et al. N Engl J Med. 2005;353:2747-2757.
BIG1-98 (Subgroups: DFS)

Viale G, et al. SABCS 2005. Abstract 44.
Disease-Free SurvivalHazard Ratio (95% CI) Letrozole vs Tamoxifen
All patients (N = 4399) 0.71 (0.57-0.88)
ER+/PgR+ (n = 3330) 0.67 (0.51-0.88)
ER+/PgR- (n = 832) 0.88 (0.55-1.41)
ER+/HER2- (n = 3971) 0.72 (0.56-0.91)
ER+/HER2+ (n = 234) 0.68 (0.33-1.41)
• The difference is not significant.
• No tamoxifen resistance observed in ER+/PgR- tumors (??)
BIG 1-98: Central Review of ER, PgR, and HER2

ER/PgR
HER2 &
Tamoxifen
DFS in tamoxifen-
treated patients
Arpino, G. et al. J Natl Cancer Inst 2005;97:1254-1261
ER+/PR+
ER+/PR+
ER+/PR-
ER+/PR-
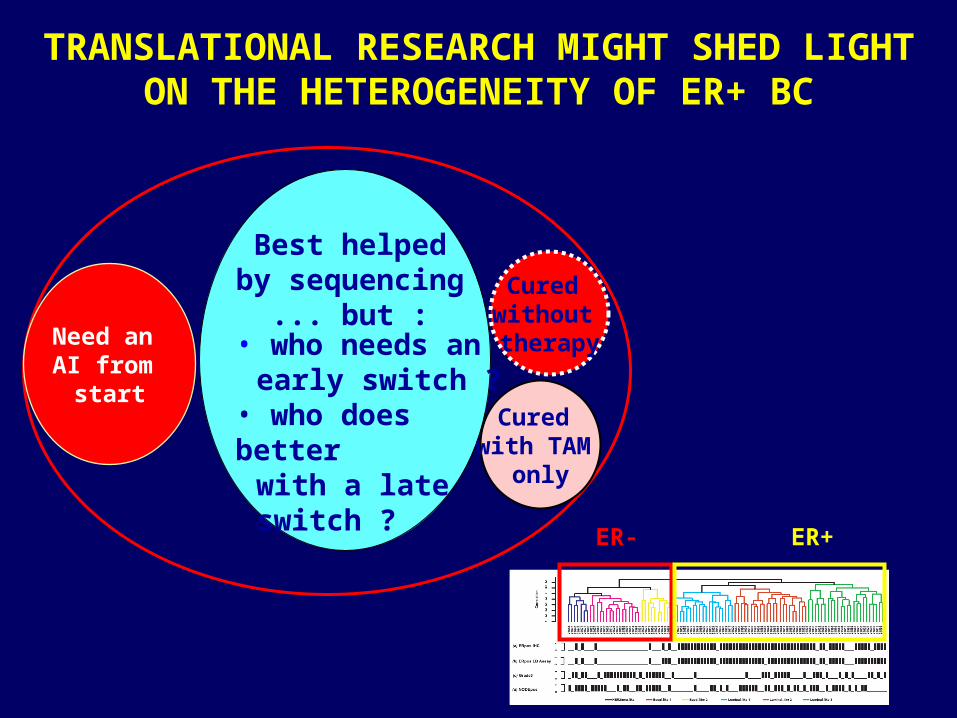
Need an AI from
start
Cured without therapy
Cured with TAM
only
TRANSLATIONAL RESEARCH MIGHT SHED LIGHT ON THE HETEROGENEITY OF ER+ BC
• who needs an early switch ?
• who does better with a late
switch ?
Best helpedby sequencing
... but :
ER- ER+

AROMATASE INHIBITOR VERSUS TAMOXIFEN AROMATASE INHIBITOR VERSUS TAMOXIFEN WAITING FOR THE FINAL BENEFIT/RISK WAITING FOR THE FINAL BENEFIT/RISK
ASSESSMENTASSESSMENT
Osteoporosis risk Musculo-skeletal events Cost
NeurocognitionSexual function
Lipid metabolismCardiovascular disease
DVT Stroke Endometrial Ca Hot flashes
TAMOXIFENTAMOXIFEN
AROMATASE AROMATASE INHIBITORINHIBITOR
??

Arguments in favour of the switching strategy
• First OS advantage demonstration vs tamoxifen– ITT 15% (-2% – 29%) p = 0.08– ER+/Unknown 17% (0% – 31%) p =
0.05
• To minimize the adverse risk of both agents
• To monitoring the menopausal status in patients with chemo-induced amenorrhea

HR for recurrence in switched adjuvant trials of AIs vs tamoxifen
ABCSG 8 / ARNO 951
(anastrozole)
ITA2
(anastrozole)
IES3
(exemestane)
0.60*
0.35*
0.75†
HRFollow-up (months)
*all patients; †HR+ve patients
28
36
56
1Jakesz R et al. Lancet 20052Boccardo F et al. J Clin Oncol 2005
3Coombes RC et al. Lancet 2007
Trial

MA 17: Postunblinding results(Switch vs Placebo)

EFS ABCSG 8 Trial(Switch vs Sequence)

Arguments in favour of the upfront strategy
• Contraindication to TAM
• Previous therapy with SERMs
• Risk of early relapse (adverse prognostic
factors)
• Biological rationale (PGR-, HER2+)
• Results based on unselected patients

Smoothed event rates for recurrence (HR*-positive population)
0 1 2 3 4 5 6Follow-up time (years)
Annualhazardrates(%)
Anastrozole
Tamoxifen 0.5
1.0
1.5
2.0
2.5
3.03.0
0
*HR=hormone receptor


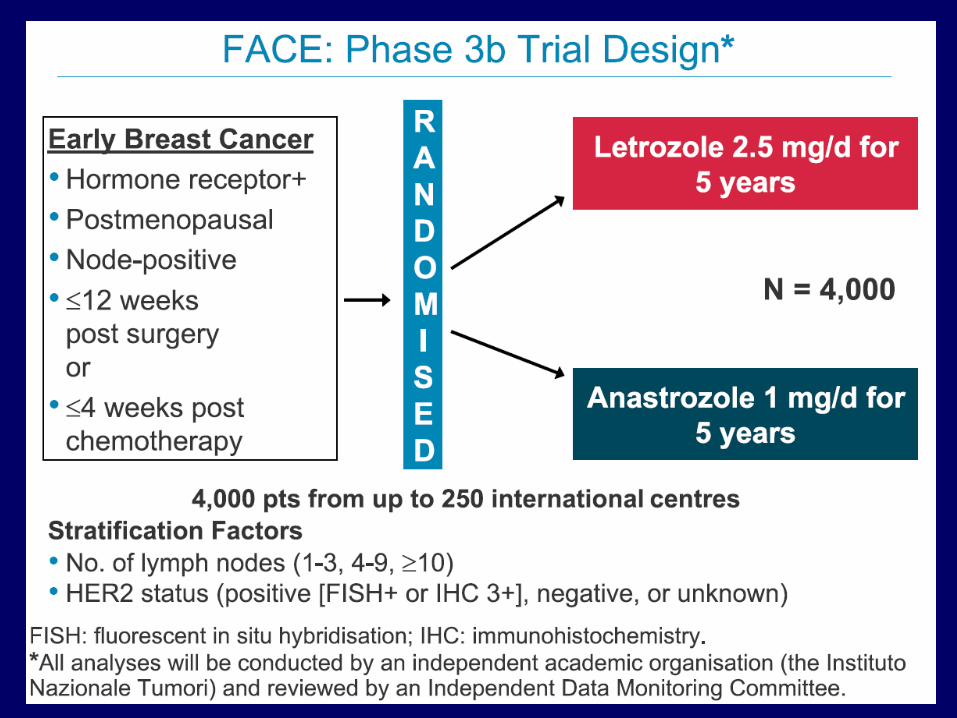
• Postmenopausal women
• Histologically or cytologically confirmed, receptor-positive, adequately excised, primary breast cancer
N = 6350*5 years
Exemestane 25 mg/day
Anastrozole 1 mg/day
Surgery ± RT ±
chemo-therapy
MA.27: Study Design
Ran
do
miz
atio
n
*Closed to accrual. Primary endpoint: event-free survival

TEAM• Phase III, open-label, randomized trial
of 5 years’ adjuvant exemestane vs adjuvant tamoxifen followed by exemestane
• Postmenopausal women with hormone receptor–positive, early-stage breast cancer
• Sample size = 1240; closed to accrual
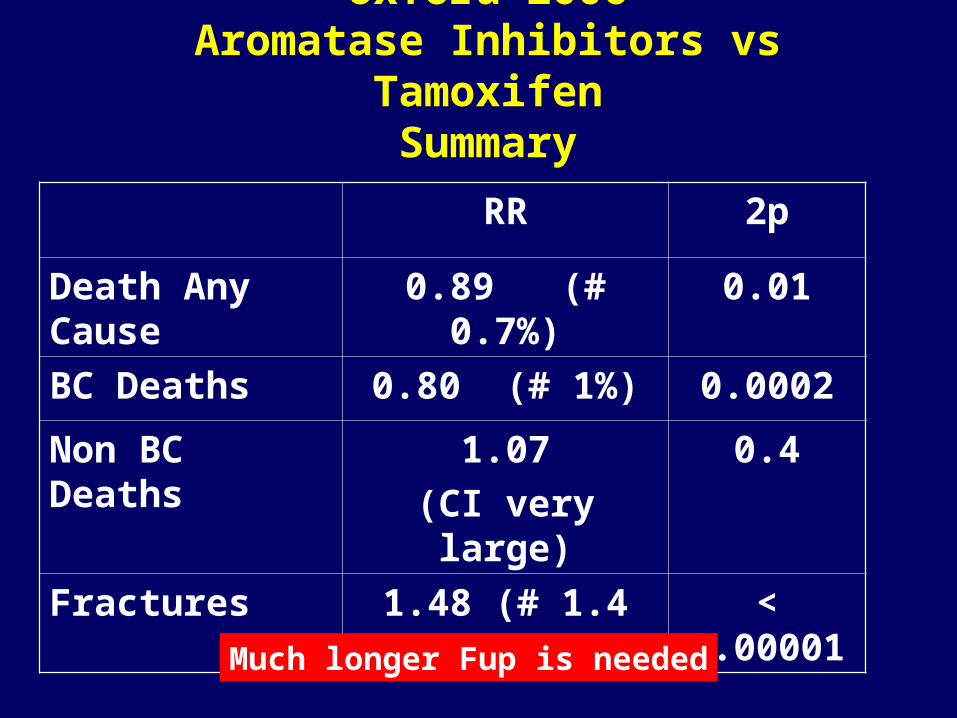
Oxford 2006Aromatase Inhibitors vs Tamoxifen
Summary
RR 2p
Death Any Cause 0.89 (# 0.7%) 0.01
BC Deaths 0.80 (# 1%) 0.0002
Non BC Deaths 1.07
(CI very large)
0.4
Fractures 1.48 (# 1.4 %) < 0.00001
Much longer Fup is needed

Patient on day 0 Patient on day 0 of adjuvant ETof adjuvant ET
• High risk• Contra-indication to TAM• Doubt about TAM sensitivity
(e.g. HER2+ and/or PR-)
Anastrozole or Letrozole
Other patientsOther patientsTamoxifen with switch to Ana/Exe at later time
Patient on Patient on adjuvant TAMadjuvant TAM
• Medium to high risk and/or• Doubt about TAM sensitivity
Switch Switch encouraged
Very low risk
Discussion with more Discussion with more weight on known / weight on known /
unknown drug side-unknown drug side-effects profileseffects profiles
Ana/Exeif early switch
(2-3y)
Letrozoleif late switch
(4-6y)
Possible Algorithm for Adj Ht in Postmenopausal pts