
Aromatase inhibitor therapy for early breast cancer.
Giorgio Mustacchi
Centro Oncologico
Università di Trieste

LowLow
IntermediateIntermediate
HighHigh
Node –Node –HER2 –HER2 –LVI absentLVI absent
Node –, HER2+ or LVI presentNode + (1-3) and HER2 -
Node + (1-3) and HER2 +Node + 4
G1G1TT22
AGE < 35G2-3 T>2
RRIISSKK
RRIISSKK
ST. GALLEN 2005:ST. GALLEN 2005: DEFINITIONS OF RISK DEFINITIONS OF RISK

2000 Oxford Overview: ER Status is not a prognostic factor
N- N+
EBCTCG, Lancet 2005EBCTCG, Lancet 2005
No Treatment arm

Overall survival ∆:
MA-17 N+ (HR: 0.61, p=0.04), IES (HR: 0.83, p=0.05)
Trial Design F/U N ∆ in DFS
ATAC
(Lancet 2005)A vs T vs AT
(double-blind)~ 5 yr 9366
2.5%-3.0%
BIG 1-98
(ESMO 2006)
T vs Let
(double-blind)~ 4 yr
8028
(4922)~ 3%
ABCSG-8 ARNO95
(Lancet 2005)
T Ana vs T
(open label)~ 3 yr 3224 3%
IES
(ASCO 2006)T Exe vs T (double-blind)
~ 5 yr
(2-3 post-treat)
4724 3.5%
MA.17
(JNCI 2005)L vs Placebo
(double-blind)~ 3 yr 5187 4.6%
Key Aromatase Inhibitors TrialsAll Favor AI Arm
RRIISSKK
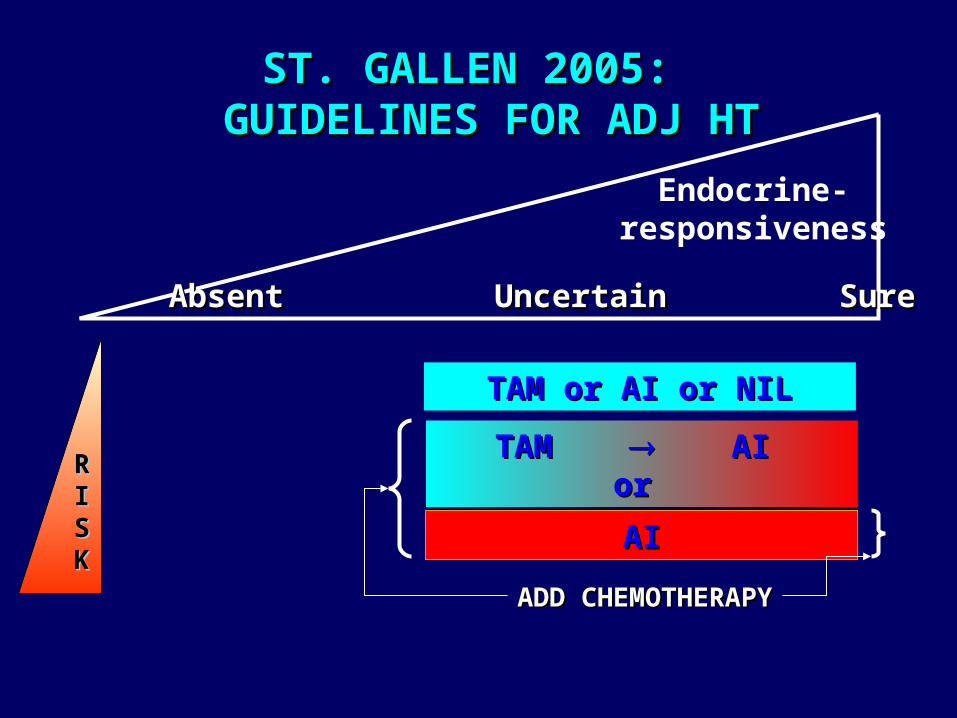
TAM or AI or NILTAM or AI or NIL
TAM TAM AI AI or or
ADD CHEMOTHERAPYADD CHEMOTHERAPY
AIAI
Endocrine-responsiveness
AbsentAbsent Uncertain Uncertain SureSure
ST. GALLEN 2005: ST. GALLEN 2005: GUIDELINES FOR ADJ HT GUIDELINES FOR ADJ HT

Neoadjuvant IMPACT:Short Term Predictors for ATAC?
HR 95.2% CI P Value
ANA vs TAM 0.83 0.71-0.96 0.0129Comb vs TAM 1.02 0.88-1.18 0.7718
Anastrozole
Tamoxifen
Combination
Time to event (mo)
Pro
po
rtio
n e
ve
nt-
fre
e (
%)
0
80
85
90
95
100
0 6 12 18 24 30 36 42
ATACn 9366 pts DFS 33 mo
A C
IMPACTn 330 pts Clinical OR 12 wks Biological Ki67 2 wks
T
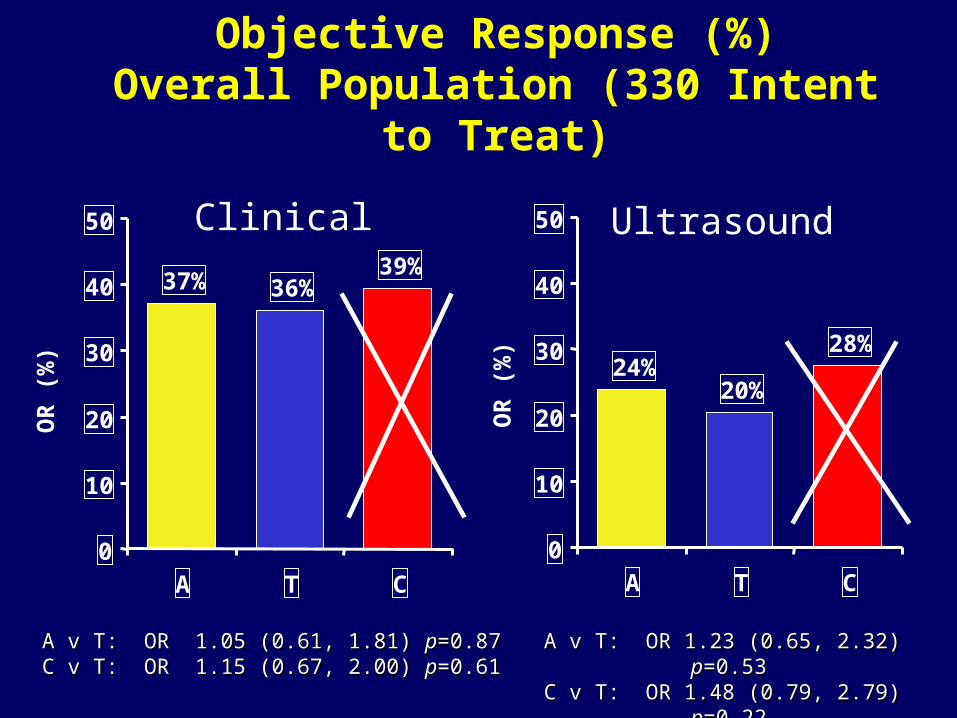
24%20%
28%
0
10
20
30
40
50
A T C
39%36%37%
0
10
20
30
40
50
A T C
Objective Response (%)Overall Population (330 Intent to Treat)
OR
(%
)
A v T: OR 1.05 (0.61, 1.81) A v T: OR 1.05 (0.61, 1.81) pp=0.87=0.87 C v T: OR 1.15 (0.67, 2.00) C v T: OR 1.15 (0.67, 2.00) pp=0.61 =0.61
OR
(%
)
A v T: OR 1.23 (0.65, 2.32) A v T: OR 1.23 (0.65, 2.32) pp=0.53=0.53C v T: OR 1.48 (0.79, 2.79) C v T: OR 1.48 (0.79, 2.79) pp=0.22=0.22
Clinical Ultrasound

EARLY BREAST CANCER TREATMENT:LESSONS LEARNED FROM CLINICAL TRIALS
An intervention produces, on average, a 50% An intervention produces, on average, a 50% relative risk reduction in relapserelative risk reduction in relapse
Higher risk women will, on Higher risk women will, on average, derive a greater absolute average, derive a greater absolute
benefit
20%20%
10%10%
40%40%
20%20%
Initial riskInitial riskFinal riskFinal risk
N-N- N+N+
There is heterogeneity in the There is heterogeneity in the magnitude of treatment magnitude of treatment
benefit !benefit !
Subset A:70% relative
risk reduction
Subset A:70% relative
risk reduction
Subset B:Subset B:<30% <30% relative risk reductionrisk reduction
Subset B:Subset B:<30% <30% relative risk reductionrisk reduction

# Gene profile = # pCR
Molecular Type % pCR 95% CI
Basal-like 45 24-68
HER2 + 45 24-68
Luminal A & B 6 1 - 21
Rouzier , Clin Cancer Res. 2005
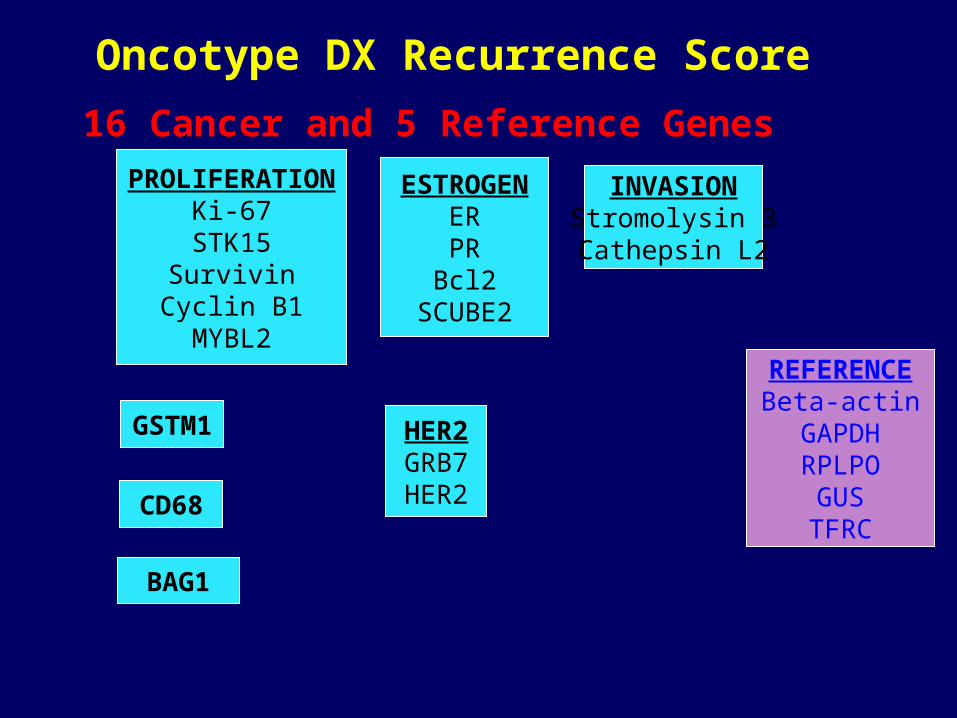
Oncotype DX Recurrence Score
REFERENCEBeta-actinGAPDHRPLPO
GUSTFRC
PROLIFERATIONKi-67
STK15Survivin
Cyclin B1MYBL2
ESTROGENERPR
Bcl2SCUBE2
INVASIONStromolysin 3Cathepsin L2
HER2GRB7HER2
BAG1
GSTM1
CD68
16 Cancer and 5 Reference Genes

0 2 4 6 8 10 12 14 16
Years
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
DR
FS
Low R isk (R S < 18) Intermediate R isk (R S 18 - 30) H igh R isk (RS 31)
NSABP B14-Results: Benefit from Tamoxifen
Paik, NEJM 2005
Tam:High RS
DFS = Placebo

AROMATASE INHIBITORS AND TAMOXIFEN: AROMATASE INHIBITORS AND TAMOXIFEN: HETEROGENEITY IN THE TREATMENT EFFECTHETEROGENEITY IN THE TREATMENT EFFECT
A
B
Subset A : Subset A : 70 % reduction ?70 % reduction ?
Subset B : Subset B : 30 % reduction ?30 % reduction ?
On average :On average :50 % reduction 50 % reduction in the odds of in the odds of
relapserelapse
molecular signature ?molecular signature ?
PGR ?PGR ? HER-2 ? HER-2 ? Other molecular markers ?Other molecular markers ?

EG
FR
HE
R2
Tam-S Tam-R
Knowlden et al. Endocrinology 144:1032, 2003
10% ‘conversion rate’ to HER2 overexpression in breast cancers that recur (early) on adjuvant tamoxifen (Gutierrez et al. J Clin Oncol 2005; 23:2469)
Tamoxifen-resistant breast tumors acquireErbB receptor overexpression


De Laurentiis et al. Clin. Cancer Res. 11:4741, 2005
ER+/HER2+ BC and endocrine therapy
N=1,925

HER2 + : predictive of resistence to any hormonal treatment ?
0
20
40
60
80
100
% RR
Letrozole Tam
Neoadjuvant Letrozole VS Tamoxifen
HER 2/3+ HER -
Ellis, JCO Sep 2001
020406080
100
% RR
ANA TAM
FISH + Overall
Dowsett, S. Antonio 03Neoadjuvant
Anastrozole VS Tamoxifen

ER+/PR- and hormonal treatment (ATAC trial)
From Cui et al. JCO 23:7721, 2005

Data are HRs and 95% CIs
HR Log Scale
Exemestane
better
Tamoxifen better
0.64 (0.51-0.79)
0.67 (0.39-1.16)
0.58 (0.38-0.90)
0.66 (0.51-0.87)
HR (95% CI)
0.4 0.6 0.8 1.0 1.2
Subgroup (n)
All ER+ (3853)
ER+/PgR unknown (499)
ER+/PgR- (735)
ER+/PgR+ (3853)
Coombes RC, et al. N Engl J Med. 2004;350:1081-1092.
IES 031: DFS According to ER/PgR
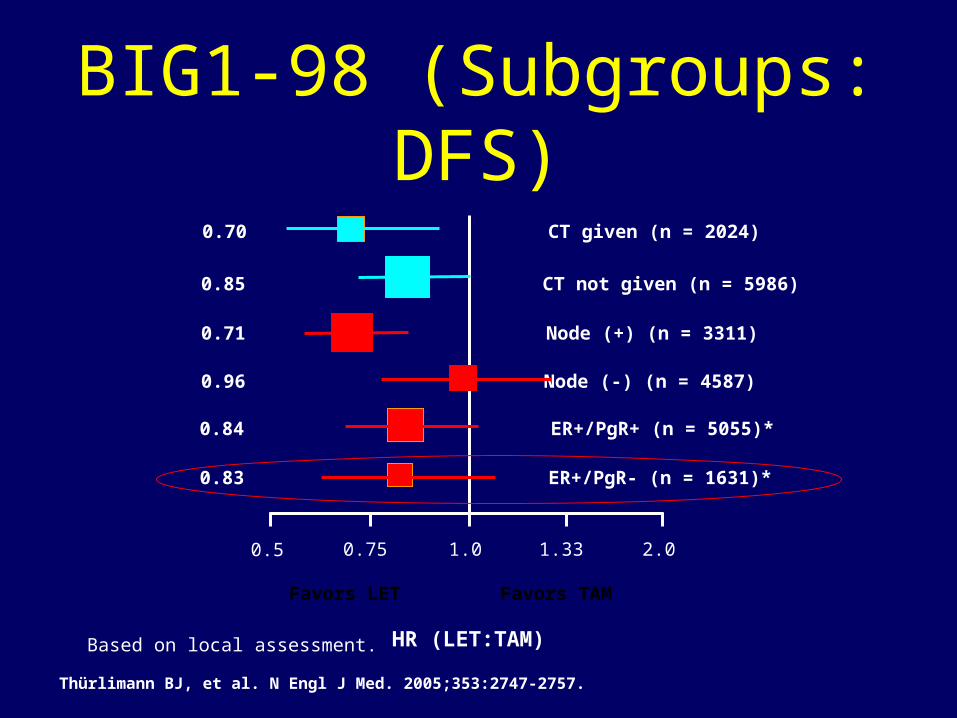
*Based on local assessment.
1.00.5 0.75 1.33 2.0
CT given (n = 2024)
CT not given (n = 5986)
0.70
0.85
Node (+) (n = 3311)
Node (-) (n = 4587)
0.71
0.96
ER+/PgR+ (n = 5055)*
ER+/PgR- (n = 1631)*
0.84
0.83
Favors LET Favors TAM
HR (LET:TAM)
Thürlimann BJ, et al. N Engl J Med. 2005;353:2747-2757.
BIG1-98 (Subgroups: DFS)

Viale G, et al. SABCS 2005. Abstract 44.
Disease-Free SurvivalHazard Ratio (95% CI) Letrozole vs Tamoxifen
All patients (N = 4399) 0.71 (0.57-0.88)
ER+/PgR+ (n = 3330) 0.67 (0.51-0.88)
ER+/PgR- (n = 832) 0.88 (0.55-1.41)
ER+/HER2- (n = 3971) 0.72 (0.56-0.91)
ER+/HER2+ (n = 234) 0.68 (0.33-1.41)
• The difference is not significant.
• No tamoxifen resistance observed in ER+/PgR- tumors (??)
BIG 1-98: Central Review of ER, PgR, and HER2

ER/PgR
HER2 &
Tamoxifen
DFS in tamoxifen-
treated patients
Arpino, G. et al. J Natl Cancer Inst 2005;97:1254-1261
ER+/PR+
ER+/PR+
ER+/PR-
ER+/PR-
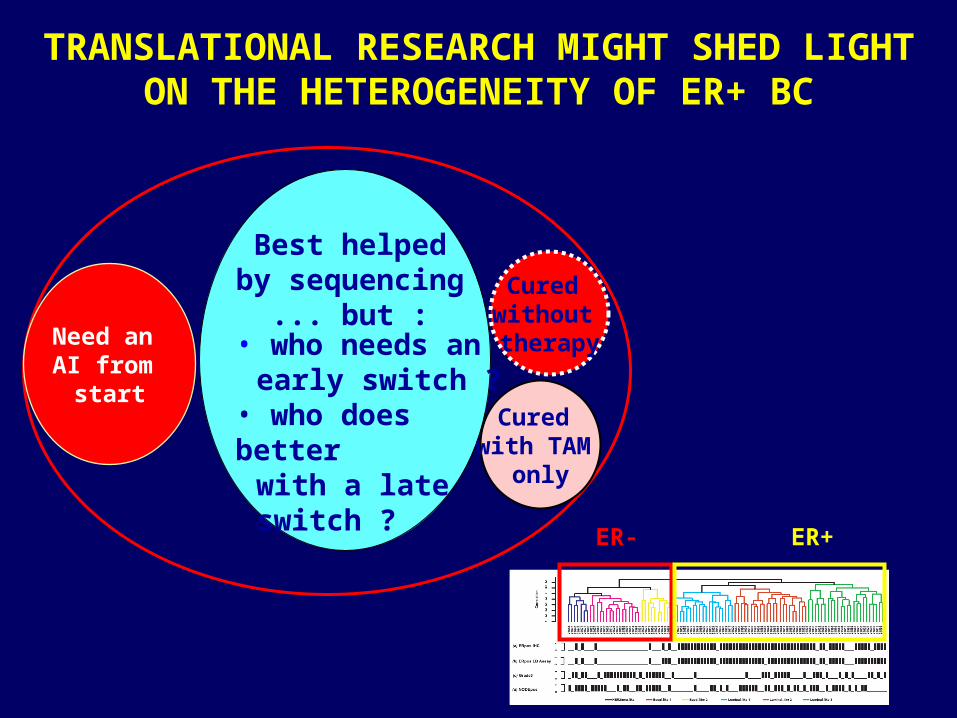
Need an AI from
start
Cured without therapy
Cured with TAM
only
TRANSLATIONAL RESEARCH MIGHT SHED LIGHT ON THE HETEROGENEITY OF ER+ BC
• who needs an early switch ?
• who does better with a late
switch ?
Best helpedby sequencing
... but :
ER- ER+

AROMATASE INHIBITOR VERSUS TAMOXIFEN AROMATASE INHIBITOR VERSUS TAMOXIFEN WAITING FOR THE FINAL BENEFIT/RISK WAITING FOR THE FINAL BENEFIT/RISK
ASSESSMENTASSESSMENT
Osteoporosis risk Musculo-skeletal events Cost
NeurocognitionSexual function
Lipid metabolismCardiovascular disease
DVT Stroke Endometrial Ca Hot flashes
TAMOXIFENTAMOXIFEN
AROMATASE AROMATASE INHIBITORINHIBITOR
??

Arguments in favour of the switching strategy
• First OS advantage demonstration vs tamoxifen– ITT 15% (-2% – 29%) p = 0.08– ER+/Unknown 17% (0% – 31%) p =
0.05
• To minimize the adverse risk of both agents
• To monitoring the menopausal status in patients with chemo-induced amenorrhea

HR for recurrence in switched adjuvant trials of AIs vs tamoxifen
ABCSG 8 / ARNO 951
(anastrozole)
ITA2
(anastrozole)
IES3
(exemestane)
0.60*
0.35*
0.75†
HRFollow-up (months)
*all patients; †HR+ve patients
28
36
56
1Jakesz R et al. Lancet 20052Boccardo F et al. J Clin Oncol 2005
3Coombes RC et al. Lancet 2007
Trial

MA 17: Postunblinding results(Switch vs Placebo)

EFS ABCSG 8 Trial(Switch vs Sequence)

Arguments in favour of the upfront strategy
• Contraindication to TAM
• Previous therapy with SERMs
• Risk of early relapse (adverse prognostic
factors)
• Biological rationale (PGR-, HER2+)
• Results based on unselected patients

Smoothed event rates for recurrence (HR*-positive population)
0 1 2 3 4 5 6Follow-up time (years)
Annualhazardrates(%)
Anastrozole
Tamoxifen 0.5
1.0
1.5
2.0
2.5
3.03.0
0
*HR=hormone receptor


• Postmenopausal women
• Histologically or cytologically confirmed, receptor-positive, adequately excised, primary breast cancer
N = 6350*5 years
Exemestane 25 mg/day
Anastrozole 1 mg/day
Surgery ± RT ±
chemo-therapy
MA.27: Study Design
Ran
do
miz
atio
n
*Closed to accrual. Primary endpoint: event-free survival

TEAM• Phase III, open-label, randomized trial
of 5 years’ adjuvant exemestane vs adjuvant tamoxifen followed by exemestane
• Postmenopausal women with hormone receptor–positive, early-stage breast cancer
• Sample size = 1240; closed to accrual
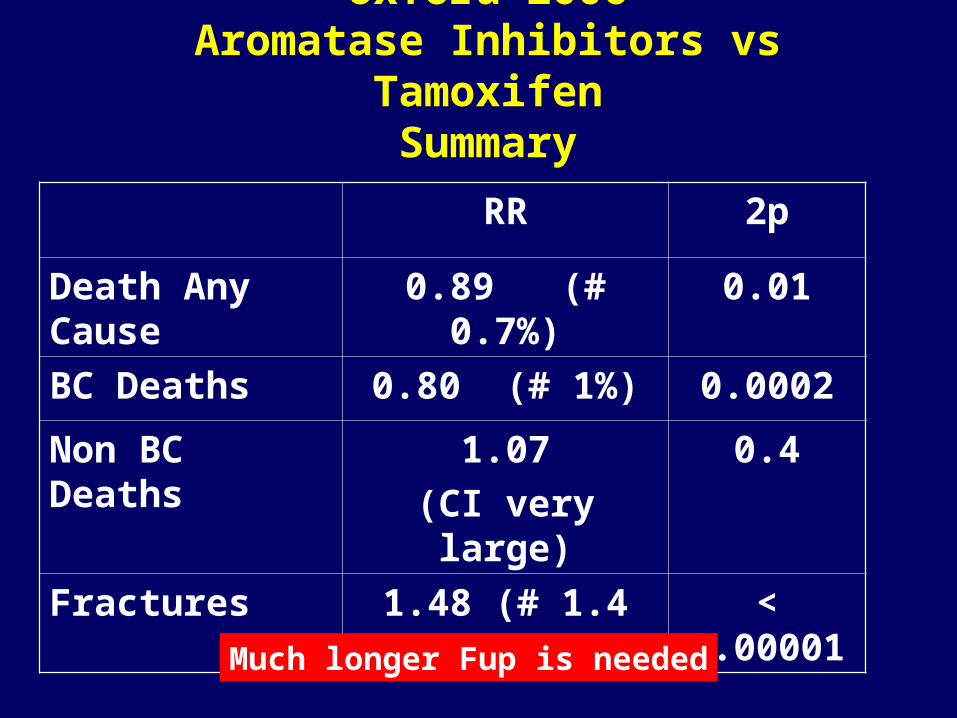
Oxford 2006Aromatase Inhibitors vs Tamoxifen
Summary
RR 2p
Death Any Cause 0.89 (# 0.7%) 0.01
BC Deaths 0.80 (# 1%) 0.0002
Non BC Deaths 1.07
(CI very large)
0.4
Fractures 1.48 (# 1.4 %) < 0.00001
Much longer Fup is needed

Patient on day 0 Patient on day 0 of adjuvant ETof adjuvant ET
• High risk• Contra-indication to TAM• Doubt about TAM sensitivity
(e.g. HER2+ and/or PR-)
Anastrozole or Letrozole
Other patientsOther patientsTamoxifen with switch to Ana/Exe at later time
Patient on Patient on adjuvant TAMadjuvant TAM
• Medium to high risk and/or• Doubt about TAM sensitivity
Switch Switch encouraged
Very low risk
Discussion with more Discussion with more weight on known / weight on known /
unknown drug side-unknown drug side-effects profileseffects profiles
Ana/Exeif early switch
(2-3y)
Letrozoleif late switch
(4-6y)
Possible Algorithm for Adj Ht in Postmenopausal pts







