ar 2009 eurotranspolant
TRANSCRIPT

EUR
OT
RA
NSP
LAN
T IN
TER
NA
TIO
NA
L FOU
ND
AT
ION
An
nu
al Rep
ort 2
00
9
63082 om 2005 29-06-2006 13:40 Pagina 1
2009
EUR
OT
RA
NSP
LAN
T IN
TER
NA
TIO
NA
L FOU
ND
AT
ION
An
nu
al Rep
ort 2
00
9
63082 om 2005 29-06-2006 13:40 Pagina 1
2009
EUR
OT
RA
NSP
LAN
T IN
TER
NA
TIO
NA
L FOU
ND
AT
ION
An
nu
al Rep
ort 2
00
9
63082 om 2005 29-06-2006 13:40 Pagina 1
2009

electronic,
2009
Edited by
Arie Oosterlee and Axel Rahmel

2
CIP-GEGEVENS KONINKLIJKE BIBLIOTHEEK, DEN HAAG
Annual Report/Eurotransplant International Foundation.–Leiden:Eurotransplant Foundation. -III., graf., tab.Published annuallyAnnual report 2009 / ed. by Arie Oosterlee and Axel RahmelISBN-13: 978-90-71658-29-7Keyword: Eurotransplant Foundation; annual reports.
electronic,
2009
Edited by
Arie Oosterlee and Axel Rahmel
“The PerfecT MaTch”
LegaLLy founded: May 12, 1969ISo certified 9001:2008

3
Table of contents
- Board of EuroTransplanT InTErnaTIonal foundaTIon 7
- TRANSPLANT PROGRAMS AND THEIR DELEGATES IN 2009 8
- Renal programs 8- Heart programs 9- Lung programs 10- Liver programs 11- Pancreas (islet) programs 12- Tissue typing laboratories 12
- forEword 15
1. rEporT of ThE Board and ThE cEnTral offIcE of 16 sTIchTIng EuroTransplanT InTErnaTIonal foundaTIon
1.1 Report of the Eurotransplant Board 161.2 ReportoftheEurotransplantoffice 181.3 Future policy 201.4 Quality Assurance & Safety 201.5 Advisory Committees 211.6 Recommendations approved 24
2. BasIc prIncIplEs of ThE EuroTransplanT communITy 27
2.1 Eurotransplant mission statement 272.2 Basic Mandate of Eurotransplant 272.3 Joint Declaration on cooperation within the framework of Eurotransplant International Foundation 30
3. EuroTransplanT: donaTIon, waITIng lIsTs and TransplanTs 32
- Introduction 32Table 3.1 Number of deceased organ donors used for a transplant, by donor country, from 2005 to 2009 33Figure 3.1 Median age of deceased donors in Eurotransplant, used for a transplant 33Table 3.2(i) Number of deceased organ donors used for a transplant, by organ, from 2005 to 2009 33Table 3.2(ii) Number of deceased organ donors used for a transplant, by organ and donor country, in 2009 33Table 3.3(i) Demographic data on deceased organ donors, used for a transplant, from 2005 to 2009 34Table 3.3(ii) Demographic data on deceased organ donors, used for a transplant, in 2009 34Table 3.4a(i) Number of donors, used for a transplant, by type of donor, from 2005 to 2009 35Table 3.4a(ii) Number of donors, used for a transplant, by type and donor country, in 2009 35Table 3.4b(i) Number of deceased donors, used for a transplant, by type of donor, from 2005 to 2009 35Table 3.4b(ii) Number of deceased donors, used for a transplant, by type and donor country, in 2009 35 Table 3.4c(i) Non-heart beating (NHB) donors, used for a transplant, from 2005 to 2009 35Table 3.4c(ii) Non-heart beating donors, used for a transplant, by donor country, in 2009 36Table 3.4d(i) Transplants from NHB donors, from 2005 to 2009 36Table 3.4d(ii) Transplants from NHB donors, by donor country, in 2009 36Table 3.5(i) Active Eurotransplant waiting list, by organ, as per December 31, from 2005 to 2009 36 Table 3.5(ii) Active Eurotransplant waiting list, by organ, as per December 31, 2009 37Table 3.6(i) Registration events on the Eurotransplant waiting list, by organ, from 2005 to 2009 38Table 3.6(ii) Registration events on the Eurotransplant waiting list, by organ and country, in 2009 38Table 3.7(i) Number of transplanted organs**, by organ, by donor type, from* 2005 to 2009 39

4
Table 3.7(ii) Number of transplanted organs**, by organ, by donor type, by country of transplant, in* 2009 39Table 3.8(i) Transplants from 2005 to 2009 39Table 3.8(ii) Transplants in 2009, by transplant country 40Table 3.9(i) Mortality on the Eurotransplant waiting list, by date of death, from 2005 to 2009 40Table 3.9(ii) Mortality on the Eurotransplant waiting list in 2009, by country 41Figure 3.2 Median age of patients on active waiting list 41Figure 3.3 Median age of transplant recipients (deceased donor transplants) 41Figure 3.4 Median waiting time for patients on active waiting list at year end 42Figure 3.5 Median waiting time to transplant (deceased donor transplants) 42
4. KIdnEy: donaTIon, waITIng lIsTs and TransplanTs 43
Table 4.1(i) Deceased donors / kidneys in Eurotransplant, from 2005 to 2009 43Table 4.1(ii) Deceased donors / kidneys in Eurotransplant in 2009 43Figure 4.1 Kidney waiting list, number of patients at year end, by urgency 44Figure 4.2 Kidney waiting list, percentage of patients at year end, by urgency 44Table 4.2(i) Active kidney transplant waiting list, as per December 31, from 2005 to 2009 - characteristics 44Table 4.2(ii) Active kidney transplant waiting list, as per December 31 , 2009 - characteristics 45Table 4.3(i) Active kidney-only transplant waiting list, as per December 31, from 2005 to 2009 - characteristics 45Table 4.3(ii) Active kidney-only transplant waiting list, as per December 31, 2009 - characteristics 45Figure 4.3 Number of deceased donor kidney transplants, by recipient urgency at transplant 46Figure 4.4 Percentage of deceased donor kidney transplants, by recipient urgency at transplant 47Table 4.4(i) Kidney transplant characteristics from 2005 to 2009 47Table 4.4(ii) Kidney transplant characteristics - 2009 48Table 4.5(i) Living donor kidney transplants - kidney-only from 2005 to 2009 49Table 4.5(ii) Living donor kidney transplants - kidney-only - 2009 50Figure 4.5 Dynamics of the Eurotransplant kidney transplant waiting list and transplants between 1969 and 2009 50
5. ThoracIc organs: donaTIon, waITIng lIsTs and TransplanTs 51
Table 5.1(i) Deceased donors / hearts in Eurotransplant from 2005 to 2009 51Table 5.1(ii) Deceased donors / hearts in Eurotransplant in 2009 51Table 5.2(i) Deceased donors / lungs in Eurotransplant from 2005 to 2009 51Table 5.2(ii) Deceased donors / lungs in Eurotransplant in 2009 52Figure 5.1 Heart waiting list, number of patients at year end, by urgency 52Figure 5.2 Heart waiting list, percentage of patients at year end, by urgency 53Table 5.3(i) Active heart transplant waiting list, as per December 31, from 2005 to 2009 - characteristics 53Table 5.3(ii) Active heart transplant waiting list as per December 31, 2009 - characteristics 53Table 5.4(i) Active heart-only transplant waiting list as per December 31 - characteristics 53Table 5.4(ii) Active-heart only transplant waiting list as per December 31, 2009 - characteristics 54Table 5.5(i) Active heart + lung transplant waiting list, as per December 31, from 2005 to 2009 - characteristics 54Table 5.5(ii) Active heart + lung transplant waiting list, as per December 31, 2009 - characteristics 55Table 5.6(i) Active heart + lung transplant waiting list, as per December 31, from 2005 to 2009 - characteristics 55Table 5.6(ii) Active heart + lung transplant waiting list as per December 31, 2009 - characteristics 55Figure 5.3 Lung waiting list, number of patients at year end, by urgency 56Figure 5.4 Lung waiting list, percentage of patients at year end, by urgency 56Table 5.7(i) Active lung transplant waiting list as per December 31, from 2005 to 2009 - characteristics 57Table 5.7(ii) Active lung transplant waiting list as per December 31, 2009 - characteristics 57Table 5.8(i) Active lung-only transplant waiting list, as per December 31, from 2005 to 2009 - characteristics 57Table 5.8(ii) Active lung-only transplant waiting list, as per December 31, 2009 - characteristics 57Figure 5.5 Number of deceased donor heart transplants, by recipient urgency at transplant 58Figure 5.6 Percentage of deceased donor heart transplants, by recipient urgency at transplant 59Table 5.9(i) Heart transplants from 2005 to 2009 - characteristics 59Table 5.9(ii) Heart transplants 2009 - characteristics 60Table 5.10(i) Heart + lung transplants from 2005 to 2009 - characteristics 60Table 5.10(ii) Heart + lungs transplants 2009 - characteristics 61Figure 5.7 Number of deceased donor lung transplants, by recipient urgency at transplant 62Figure 5.8 Percentage of deceased donor lung transplants, by recipient urgency at transplant 62Table 5.11(i) Lung transplants from 2005 to 2009 - characteristics 62Table 5.11(ii) Lung transplants 2009 - characteristics 63
5
Figure 5.9 Dynamics of the Eurotransplant heart waiting list and transplants between 1991 and 2009 64Figure 5.10 Dynamics of the Eurotransplant heart + lung waiting list, heart + lung transplants, lung waiting list and 64 lung transplants, between 1991 and 2009
6. lIvEr and InTEsTInE: donaTIon, waITIng lIsTs and TranplanTs 65
Table 6.1(i) Deceased donors / livers in Eurotransplant from 2005 to 2009 65Table 6.1(ii) Deceased donors / livers in Eurotransplant in 2009 65Figure 6.1 Liver waiting list, number of patients at year end, by urgency 66Figure 6.2 Liver waiting list, percentage of patients at year end, by urgency 66Table 6.2(i) Active liver transplant waiting list, as per December 31, from 2005 to 2009 - characteristics 67Table 6.2(ii) Active liver transplant waiting list, as per December 31, 2009 - characteristics 67Table 6.3(i) Active liver-only transplant waiting list as per December 31, from 2005 to 2009 - characteristics 67Table 6.3(ii) Active liver-only transplant waiting list as per December 31, 2009 - characteristics 68Figure 6.3 Number of deceased donor liver transplants, by recipient urgency at transplant 68Figure 6.4 Percentage of deceased donor liver transplants, by recipient urgency at transplant 69Table 6.4(i) Liver transplants from 2005 to 2009 - characteristics 69Table 6.4(ii) Liver transplants 2009 - characteristics 70Table 6.5(i) Living donor liver transplants - liver-only - from 2005 to 2009 70Table 6.5(ii) Living donor liver transplants - liver-only - 2009 71Figure 6.5 Dynamics of the Eurotransplant liver waiting list and liver transplants between 1991 and 2009 72- Intestine transplants 2009 73Table 6.6 Number of intestinal transplants in 2009 73
7. pancrEas and IslETs: donaTIon,waITIng lIsTs and TransplanTs 74
Table 7.1(i) Deceased donors / pancreas in Eurotransplant from 2005 to 2009 74Table 7.1(ii) Deceased donors / pancreas in Eurotransplant in 2009 74Figure 7.1 Pancreas waiting list, number of patients at year end, by urgency 75Figure 7.2 Pancreas waiting list, percentage of patients at year end, by urgency 75Table 7.2(i) Active pancreas transplant waiting list as per December 31, from 2005 to 2009 - characteristics 75Table 7.2(ii) Active pancreas transplant waiting list as per December 31, 2009 - characteristics 76Table 7.3a(i) Active pancreas-only transplant waiting list as per December 31, from 2005 to 2009 - characteristics 76Table 7.3a(ii) Active pancreas-only transplant waiting list as per December 31, 2009 - characteristics 76Table 7.3b(i) Active kidney + pancreas transplant waiting list as per December 31, from 2005 to 2009 - characteristics 77Table 7.3b(ii) Active kidney + pancreas transplant waiting list as per December 31, 2009 - characteristics 77Figure 7.3 Number of deceased donor pancreas transplants, by recipient urgency at transplant 78Figure 7.4 Percentage of deceased donor pancreas, by recipient urgency at transplant 79Table 7.4a(i) Pancreas transplants 2005 to 2009 - characteristics 79Table 7.4a(ii) Pancreas transplants 2009 - characteristics 80Table 7.4b(i) Pancreas islet transplants, from 2005 to 2009 80Table 7.4b(ii) Pancreas islet transplants in 2009 80Table 7.4c(i) Pancreas transplants from 2005 to 2009 - characteristics 81Table 7.4c(ii) Pancreas transplants 2009 - characteristics 81Figure 7.5 Dynamics of the Eurotransplant pancreas+kidney and islet+kidney waiting list, pancreas+kidney, 82 islet+kidney, pancreas and islet-only transplants between 1991 and 2009
8. hIsTocompaTIBIlITy TEsTIng 83
8.1 Introduction 838.2 EurotransplantExternalProficiencyTestingSchemes 838.2.1 ExternalProficiencyTestingonHLAtyping 838.2.2 ExternalProficiencyTestingoncrossmatching 83Table 8.1 Report of the crossmatch results (DTT = dithiothreitol). 84 8.2.3 ExternalProficiencyTestingExerciseonscreening 84Table8.2 AnalysisofthedatareportedbytheparticipantswithrespecttoHLAantigensrecognized(=specificities) 848.3 Program for the highly sensitized patients in Eurotransplant 84Table 8.3 Evolution of the Acceptable Mismatch Program 85 8.4 Other activities 85

6
9. scIEnTIfIc ouTpuT In 2009 86
- Publications - Articles / Abstracts 86- Invited Lectures 88- Chairmenships 89 - Oral Presentations 90- Poster Presentations 91
10. EuroTransplanT pErsonnEl rElaTEd sTaTIsTIcs 92
11. aBBrEvIaTEd fInancIal sTaTEmEnTs 93
- Balance sheet 93- Statement of income and charges 93- Appropriation of the exploitation balance 94- Accounting policies 94- Principles of valuation of assets and liabilities 94- Principles for the determination of the result 95
lIsT of aBBrEvIaTIons 96

7
Board of Eurotransplant International foundation
as per December 31, 2009
Prof.Dr. B. Meiser, Munich president + on behalf of the thoracic section (A)
Prof.Dr. A.P.W.P. van Montfort, Utrecht secretary / treasurer (D)
Prof.Dr. U. Heemann, Munich on behalf of the kidney section (A)
Prof.Dr. F. Mühlbacher, Vienna on behalf of the kidney section (A)
Prof.Dr. D. Ysebaert, Antwerp on behalf of the kidney section (A)
Prof.Dr. W. Schareck, Rostock on behalf of the pancreas section (A)
Prof.Dr. G. Laufer, Innsbruck on behalf of the thoracic section (A)
Prof.Dr. D. Van Raemdonck, Leuven on behalf of the thoracic section (A)
Prof.Dr. K-W. Jauch, Munich on behalf of the liver section (A)
Prof.Dr. X. Rogiers, Ghent on behalf of the liver section (A)
Prof.Dr. C. Süsal, Heidelberg on behalf of the tissue typing section (A)
Prof.Dr. P. Schotsmans, Leuven ethics advisor (D)
Prof.Dr. R. Steininger, Vienna on behalf of the Austrian Transplant Society (B)
Prof.Dr. R. Troisi, Ghent on behalf of the Belgian Transplant Society (B)
Prof.Dr. R. Porte, Groningen on behalf of the Dutch Transplant Society (B)
VACANCY on behalf of the German Transplant Society (B)
Dr. V. Sojar, Ljubljana on behalf of the Slovenian Transplant Society (B)
Dr. M. Bušić, Zagreb on behalf of the Republic of Croatia (B)
Prof.Dr. F.H.J. Claas, Leiden on behalf of the Eurotransplant Reference Laboratory (C)
The Board of Stichting Eurotransplant International Foundation consists of:10 members A: members representing organ / tissue typing sections6 members B: members representing national transplant societies1 member C: head of the Eurotransplant Reference Laboratory2 members D: one member being financial expert, one member representing society (ethicist)

8
transplant programs anD their Delegates in 2009
Definitions (according to Articles of Association of Stichting Eurotransplant International Foundation, version September 14, 2007)
Program:Any of the following transplantation areas:kidney, heart, lungs, liver, intestine, pancreas or any part of a specific organ and/or Tissue Typing, which have the approval of the competent and relevant authorities. (Article 2)
Delegate:Each center shall have the right to delegate one natural person in the Assembly for each program in which it performed transplantations during a year. On each reference date, the number of persons delegated (the “delegates”) by a center in the Assembly shall be reviewed. (Article 5.1)(If no name is indicated, then no delegate was appointed by transplant/tissue typing program or it concerns a new program in 2009)
renal programs DelegateAustria GA Medizinische Universitätsklinik, Graz S. HornIB Chirurgische Universitätsklinik, Innsbruck C. BösmüllerOE Krankenhaus der Elisabethinen, Linz OL Allgemeines Krankenhaus, Linz E. PohankaWG Universitätsklinik für Chirurgie, Wien F. Mühlbacher
BelgiumAN Universitair Ziekenhuis Antwerpen, Edegem D. YsebaertBJ Universitair Ziekenhuis Brussel, Campus Jette J. SennesaelBR ULB, Hôpital Erasme, Bruxelles D. AbramowiczGE Universitair Ziekenhuis, Gent P. PeetersLA Cliniques Universitaires St. Luc, Bruxelles M. MouradLE Kinderdialyse Universitair Ziekenhuis Gasthuisberg, Leuven R. Van Damme-LombaertsLG Centre Hospitalier Universitaire, LiègeLM Universitair Ziekenhuis Gasthuisberg, Leuven Y. Vanrenterghem
GermanyAK Universitätsklinikum der Rheinisch-Westfälischen TH, Aachen A. HomburgAU Zentralklinikum, Augsburg H. WeihprechtBB Ruhr Universität, Bochum P. SchenkerBC Charité-Campus Virchow Klinikum der Humboldt Universität, BerlinBE Universitätsklinikum Benjamin Franklin, Berlin M. van der GietBM Kliniken der Freien Hansestadt, Bremen F. ZantvoortBO Klinikum der Urologischen und Medizinischen Universität, Bonn R. WoitasDR Technischen Universität, Dresden S. LeikeDU Med. Einrichtungen der Heinrich-Heine-Universität, Düsseldorf K. IvensER/NB Med. Einrichtungen der Universität Erlangen-Nürnberg, Erlangen K. PressmarES Universitätsklinikum, Essen O. WitzkeFD Klinikum Fulda, Fulda FM Klinikum der Johann-Wolfgang-Goethe-Universität, Frankfurt E. ScheuermannFR Klinikum der Albert-Ludwigs-Universität, Freiburg P. PisarskiGI Klinikum der Justus-Liebig-Universität, Gießen F. RennerGO Klinikum der Georg-August-Universität, Göttingen A. ObedHA Klinikum der Martin-Luther-Universität, Halle A. HamzaHB Klinikum der Ruprecht-Karls-Universität, Heidelberg C. MorathHG Universitäts-Krankenhaus Eppendorf, Hamburg F. ThaissHM Nephrologisches Zentrum Niedersachsen, Hann. Münden V. KliemHO Klinikum der Medizinischen Hochschule, Hannover F. LehnerHS Klinikum der Universität des Saarlandes, Homburg/Saar U. SesterJE Klinikum der Friedrich-Schiller-Universität, Jena U. Ott

9
KI Klinikum Christian-Albrechts-Universität, Kiel F. BraunKL Klinik der Universität Köln-Lindenthal, Köln W. ArnsKM Kliniken der Stadt Köln gGmbH, Krankenhaus Merheim, Köln-Merheim, Köln W. ArnsKK Klinik und Poliklinik für Kinderheilkunde der Universität Köln-Lindenthal, Köln W. ArnsKS Westpfalz-Klinikum, Kaiserslautern Th. RathLP Klinikum der Universität, Leipzig M. BartelsLU Klinikum der Medizinischen Universität, Lübeck M. NitschkeMA Klinikum der Stadt, Mannheim P. SchnülleMH Klinikum Rechts der Isar der Technischen Universität, München U. HeemannML Klinikum Großhadern der Ludwig-Maximilians-Universität, München K.-W. JauchMN Klinikum der Westfälischen Wilhelms-Universität, Münster H. WoltersMR Klinikum Lahnberge der Philipps-Universität, Marburg J. HoyerMZ Klinikum der Johannes-Gutenberg-Universität, Mainz O. SchreinerRB Klinikum der Universität, Regensburg B. BanasRO Klinikum der Universität, Rostock O. HakenbergST Katharinenhospital, Stuttgart J. WilhelmTU Klinikum der Eberhard-Karls-Universität, Tübingen S. NadalinUL Klinikum der Universität, Ulm M. WittauWZ Klinikum der Julius-Maximilians-Universität, Würzburg K. Lopau
Luxembourg LX Centre Hospitalier de Luxembourg P. Duhoux
The Netherlands AV VU Medisch Centrum, Amsterdam S. NurmohamedAW Academisch Medisch Centrum, Amsterdam F. BemelmanGR Academisch Ziekenhuis, Groningen J. Homan van der HeideLB Leids Universitair Medisch Centrum, Leiden J. de FijterMS Academisch Ziekenhuis, Maastricht M. ChristiaansNY Universitair Medisch Centrum St. Radboud, Nijmegen A. HoitsmaRD Erasmus Medisch Centrum, Rotterdam W. WeimarRS Sophia Kinderziekenhuis, Rotterdam K. CransbergUT Universitair Medisch Centrum, Utrecht A. van ZuilenUW Wilhelmina Kinderziekenhuis, Utrecht M. Lilien
Slovenia LO University Medical Center, Ljubljana D. Kovač
Croatia OS University Hospital, Osijek J. GalićRI University Clinical Hospital, Rijeka L. OrlićZA University Clinical Cospital, Zagreb J. PasiniZM Clinical Hospital Zagreb Merkur, Zagreb M. Knotek
heart programs Delegate
AustriaGA Chirurgische Universitätsklinik, Graz A. WaslerIB Chirurgische Universitätsklinik, Innsbruck L. MüllerWG Universitätsklinik für Chirurgie, Wien A. Zuckermann
BelgiumAN Universitair Ziekenhuis Antwerpen, Edegem I. RodrigusAS Onze Lieve Vrouw Ziekenhuis, Aalst I. DeblierBR Université Libre de Bruxelles, Hôpital Erasme, Bruxelles M. AntoineGE Universitair Ziekenhuis, Gent F. CaesLA Cliniques Universitaires St. Luc, Bruxelles A. PonceletLG Centre Hospitalier Universitaire, Liège J. DefraigneLM Universitair Ziekenhuis Gasthuisberg, Leuven J. Vanhaecke

10
Germany AK Universitätsklinikum der Rheinisch-Westfälischen TH, Aachen A. MozaBA Herz- & Diabeteszentrum Nordrhein-Westfalen, Bad Oeynhausen U. SchulzBD Deutsches Herzzentrum, Berlin BH Kerckhoff Klinik, Bad Nauheim M. RichterDR Universitätsklinikum Carl Gustav Carus, Dresden S. BroseER/NB Med. Einrichtungen der Universität Erlangen-Nürnberg, Erlangen R. TandlerES Universitätsklinikum, Essen M. KamlerFM Klinikum der Johann-Wolfgang-Goethe-Universität, Frankfurt M. SchererFR Klinikum der Albert-Ludwigs-Universität, Freiburg F. BeyersdorfGI Klinikum der Justus-Liebig-Universität, Gießen J. BauerGO Klinikum der Georg-August-Universität, Göttingen HB Klinikum der Ruprecht-Karls-Universität, Heidelberg HG Universitäts-Krankenhaus Eppendorf, Hamburg F. WagnerHO Klinikum der Medizinischen Hochschule, Hannover A. SimonHS Klinikum der Universität des Saarlandes, Homburg/Saar F. LangerJE Klinikum der Friedrich-Schiller-Universität, Jena A. LichtenbergKI Klinikum der Christian-Albrechts-Universität, Kiel A. ReineckeKL Klinik der Universität Köln-Lindenthal, Köln Th. WittwerLP Klinikum der Universität, Leipzig M. BartenMD Deutsches Herzzentrum, München ML Klinikum Großhadern der Ludwig-Maximilians-Universität, München B. MeiserMN Klinikum der Westfälischen Wilhelms-Universität, Münster S. KlotzMZ Klinikum der Johannes-Gutenberg-Universität, Mainz U. MehlhornRB Klinikum der Universität, Regensburg S. HirtWZ Universitätsklinikum, Würzburg V. Lange
The Netherlands GR Academisch Ziekenhuis, Groningen J. BrügemannRD Erasmus Medisch Centrum, Rotterdam A. MaatUT Universitair Medisch Centrum, Utrecht N. de Jonge
Slovenia LO University Medical Center, Ljubljana I. Knezević Croatia ZA University clinical hospital, Zagreb D. MilicicZD Clinical Hospital Dubrava, Zagreb Z. Sutlic
lung programs DelegateAustriaIB Chirurgische Universitätsklinik, Innsbruck L. MüllerWG Universitätsklinik für Chirurgie, Wien A. Zuckermann
Belgium AN Universitair Ziekenhuis Antwerpen, Edegem P. Van SchilBR ULB, Hôpital Erasme, Bruxelles M. EstenneLA Cliniques Universitaires St. Luc, Bruxelles P. EvrardLM Universitair Ziekenhuis Gasthuisberg, Leuven D. Van Raemdonck
Germany BD Deutsches Herzzentrum, Berlin DR Universitätsklinikum Carl Gustav Carus, Dresden S. BroseES Universitätsklinikum, Essen M. KamlerFR Klinikum der Albert-Ludwigs-Universität, Freiburg A. KirschbaumGI Klinikum der Justus-Liebig-Universität, Gießen R. SchulzHG Universitäts-Krankenhaus Eppendorf, Hamburg F. WagnerHO Klinikum der Medizinischen Hochschule, Hannover A. SimonHS Klinikum Universität des Saarlandes, Homburg/Saar

11
JE Klinikum der Friedrich-Schiller-Universität, Jena M. BreuerKI Klinikum der Christian-Albrechts-Universität, Kiel LP Klinikum der Universität, Leizpig H. BittnerML Klinikum Großhadern der Ludwig-Maximilians-Universität, München B. MeiserMN Klinikum der Westfälischen Wilhelms-Universität, Münster MZ Klinikum der Johannes-Gutenberg-Universität, Mainz M. Dahm
The Netherlands GR Academisch Ziekenhuis, Groningen M. ErasmusRD Erasmus Medisch Centrum, Rotterdam J. BekkersUT Universitair Medisch Centrum, Utrecht E. van de Graaf
liver programs Delegate
AustriaGA Chirurgische Universitätsklinik, Graz F. IbererIB Chirurgische Universitätsklinik, Innsbruck W. MarkWG Universitätsklinik für Chirurgie, Wien R. Steininger
Belgium AN Universitair Ziekenhuis Antwerpen, Edegem D. YsebaertBR ULB, Hôpital Erasme, Bruxelles V. DonckierGE Universitair Ziekenhuis, Gent X. RogiersLA Cliniques Universitaires St. Luc, Bruxelles J. LerutLG Centre Hospitalier Universitaire, Liège O. DetryLM Universitair Ziekenhuis Gasthuisberg, Leuven J. Pirenne
Germany BC Charité-Campus Virchow Klinikum der Humboldt Universität, Berlin D. SeehoferBO Chirurgische Universitätsklinik, Bonn N. SpeidelER/NB Chirurgische Klinik der Universität Erlangen-Nürnberg, Erlangen V. MüllerES Universitätsklinikum, Essen A. PaulFM Klinikum der Johann-Wolfgang-Goethe-Universität, Frankfurt C. MönchGO Klinikum der Georg-August-Universität, Göttingen A. ObedHB Klinikum der Ruprecht-Karls-Universität, Heidelberg J. SchmidtHG Universitäts-Krankenhaus Eppendorf, Hamburg L. FischerHO Klinikum der Medizinischen Hochschule, Hannover Th. BeckerHS Klinikum Universität des Saarlandes, Homburg/Saar O. KollmarJE Friedrich Schiller Universität, Jena U. SettmacherKI Klinikum der Christian-Albrechts-Universität, Kiel F. BraunKL Klinik der Universität Köln-Lindenthal, Köln D. StippelLP Klinikum der Universität, Leipzig S. JonasMB Klinikum Otto-von-Guericke Universität, Magdeburg H. LippertMH Klinikum Rechts der Isar der Technischen Universität, München P. BüchlerML Klinikum Großhadern der Ludwig-Maximilians-Universität, München K.-W. JauchMN Klinikum der Westfälischen Wilhelms-Universität, Münster H. WoltersMZ Klinikum der Johannes-Gutenberg-Universität, Mainz M. HeiseRB Klinikum der Universität, Regensburg M. SchererTU Klinikum der Eberhard-Karls Universität, Tübingen S. Nadalin
The Netherlands GR Academisch Ziekenhuis, Groningen R. PorteLB Leids Universitair Medisch Centrum, Leiden J. RingersRD Erasmus Medisch Centrum, Rotterdam G. Kazemier
Slovenia LO University Medical Centre, Ljubljana S. Markovič

12
CroatiaZA University Clinical Hospital, Zagreb ZM Clinical Hospital Merkur, Zagreb B. KocmanZP University Clinical Hospital Pediatric, Zagreb
pancreas (islet) programs Delegate
AustriaGA Chirurgische Universitätsklinik, Graz F. IbererIB Chirurgische Universitätsklinik, Innsbruck W. MarkWG Universitätsklinik für Chirurgie, Wien F. Mühlbacher
Belgium AN Universitair Ziekenhuis Antwerpen, Edegem D. YsebaertBR ULB, Hôpital Erasme, Bruxelles A. HoangBP Academisch Ziekenhuis der Vrije Universiteit, Brussel D. PipeleersGE Universitair Ziekenhuis, Gent C. RandonLA Cliniques Universitaires St. Luc, Bruxelles L. De PauwLG Centre Hospitalier Universitaire, Liège LM Universitair Ziekenhuis Gasthuisberg, Leuven
Germany BB Knappschaftskrankenhaus, Bochum P. SchenkerBC Charité-Campus Virchow Klinikum der Humboldt Universität, Berlin A. KahlDR Universitätsklinikum Carl Gustav Carus, Dresden S. KerstingER/NB Chirurgische Klinik der Universität Erlangen-Nürnberg, Erlangen V. MüllerES Universitätsklinikum, Essen A. PaulFM Klinikum der Johann-Wolfgang-Goethe-Universität, Frankfurt C. MönchFR Klinikum der Albert-Ludwigs-Universität, Freiburg P. PisarskiHB Klinikum der Ruprecht-Karls-Universität, Heidelberg J. SchmidtHG Universitäts-Krankenhaus Eppendorf, Hamburg L. FischerHO Klinikum der Medizinischen Hochschule, Hannover Th. BeckerJE Friedrich Schiller Universität, Jena U. SettmacherKI Klinikum der Christian-Albrechts-Universität, Kiel F. BraunKL Klinik der Universität Köln-Lindenthal, Köln D. StippelKM Kliniken der Stadt Köln gGmbH, Krankenhaus Merheim, Köln-Merheim, Köln D. StippelLP Klinikum der Universität, Leipzig D. UhlmannLU Klinikum der Medizinischen Universität, Lübeck MH Klinikum Rechts der Isar der Technischen Universität, München P. BüchlerML Klinikum Großhadern der Ludwig-Maximilians-Universität, München H. ArbogastMR Klinikum Lahnberge der Philipps-Universität, Marburg J. HoyerMZ Klinikum der Johannes-Gutenberg-Universität, Mainz M. HeiseRB Klinikum der Universität, Regensburg S. FarkasRO Klinikum der Universität, Rostock E. KlarTU Klinikum der Eberhard-Karls-Universität, Tübingen S. Nadalin
The Netherlands GR Academisch Ziekenhuis, Groningen R. PloegLB Leids Universitair Medisch Centrum, Leiden J. Ringers
Croatia ZM Clinical Hospital Merkur, Zagreb S. Jadrijević
tissue typing laboratories Delegate
AustriaGA Universitätsklinik, Abteilung für Transfusionsmedizin und Immunohämatologie, Graz A. HelmbergIB Universitätsklinik, HLA Labor, Innsbruck A. Mühlbacher
13
OL Allgemeines Krankenhaus, Blutzentrale, Linz C. GabrielOW Allgemeines Krankenhaus, HLA Labor, Wels R. LoizenbauerWG Institut für Blutgruppenserologie, Wien W. Mayr
Belgium BJ Universitair Ziekenhuis Brussel, Bloedtransfusiecentrum Jette C. DemanetBR Hôpital Erasme, Tissue typing laboratory, Bruxelles M. AndrienLA Université de Louvain, Tissue typing laboratory, Bruxelles D. LatinneLG Laboratoire des Groupes Sanguins, Liège G. MaggipintoME Rode Kruis Vlaanderen, Laboratory for Histocompatibility & Immunogenetics (HILA), Mechelen M.-P. Emonds
Germany BC Charité-Campus Virchow Klinikum der Humboldt Universität, Berlin C. SchönemannDU Institut für Transplantationsdiagnostik und Zelltherapeutika, Düsseldorf J. RoxER/NB Institut für Klinische Immunologie, Erlangen B. SpriewaldES Universitätsklinikum, Institut für Immunologie, Essen F. HeinemannFM Immunohaematologie, Blutspendedienst Hessen, Frankfurt C. SeidlFR Blutspendedienst, Labor für Gewebetypisierung, Freiburg F. EmmerichGI Institut für Klinische Immunologie und Transfusionsmedizin, Gießen S. WienzekGO Klinikum der Universität, HLA Labor, Göttingen H. NeumeyerHA Institut für Phathologische Biochemie, Interdisziplinäres Typisierungslabor, Halle W. AltermannHB Institut für Immunologie und Serologie, Heidelberg C. SüsalHG Universitäts-Krankenhaus Eppendorf, HLA Labor, Hamburg T. BinderHO Klinikum der Medizinischen Hochschule, Immunohaematologie/Blutbank, Hannover M. HallenslebenKI Klinikum der Christian-Albrechts-Universität, HLA Labor, Kiel M. MargetKM Institut für Transfusionsmedizin, Köln-Merheim, Köln U. BauerfeindKS Institut für Rechtsmedizin, Transplantationsimmunologie, Kaiserslautern B. ThieleLU Institut für Immunologie und Transfusionsmedizin, Lübeck M. ZiemannML Kinderklinik der Ludwig-Maximilians-Universität, HLA Labor, München M. SpannaglGMN Institut für Transfusionsmedizin, Münster MZ Klinikum der Johannes-Gutenberg Universität, HLA Labor, Mainz W. HitzlerRO Klinikum der Universität, Abteilung für Transfusionsmedizin, HLA Labor, Rostock ST Klinikum Stuttgart, Zentralinstitut für Transfusionsmedizin und Blutspendedienst, Stuttgart A. EnderTU Klinikum der Eberhard-Karls-Universität, Abt. für Transfusionswesen und Blutbank, Tübingen UL DRK Blutspendezentrale, Transplantationsimmunologie, Ulm J. Mytilineos
Luxembourg LX Centre Hospitalier, HLA Lab, Luxembourg F. Hentges
The Netherlands AW Centraal Laboratorium Bloedtransfusiedienst, Nederlandse Rode Kruis, Amsterdam N. LardyGR Laboratorium voor transplantatie-immunologie, Groningen S. LemsLB Leiden University Medical Centre, Immunohaematologie, Leiden F. ClaasMS Academisch Ziekenhuis, Laboratorium voor weefseltypering, Maastricht M. TilanusNY Academisch Ziekenhuis St. Radboud, Bloedtransfusiedienst, Nijmegen W. AllebesUT Academisch Ziekenhuis, Bloedbank, Utrecht H. Otten
Slovenia LO Tissue Typing Centre, Blood Transfusion Centre, Ljubljana B. Vidan-Jeras
Croatia RI Clinical Hospital Center, Tissue Typing Laboratory, Rijeka N. KatalinićZA University Clinical Hospital, Zagreb R. Zunec
ETRL Eurotransplant Reference Laboratory, Leids Universitair Medisch Centrum, Leiden, The NetherlandsF. Claas, I. Doxiadis

14

15
foreword
We hereby present to you the Annual Report report of 2009 of the Eurotransplant (ET) International Foundation. The objective of this report is to be accountable for the activities and initiatives that were undertaken in 2009 in Austria, Belgium, Croatia, Germany, Luxembourg, the Netherlands and Slovenia towards the internal and external parties with a vested interest in the Foundation such as:
the national regulating transplant authorities;•the national representatives of the transplant societies;•the financing authorities;•the donor hospitals;•the transplant centers;•the tissue typing laboratories;•the employees of the ET office.•
As always, many people have worked systematically to achieve our mission to encourage organ transplantation and to reach the goals associated with its mission. Obviously the good work was done by doctors and nurses of the donor hospitals and the transplant centers, the tissue typers, the transplant coordinators and many others such as people working at the ET office. Our Advisory Committee members put a lot of time and effort in setting organ allocation- and procurement as well as ethical, financial and ICT standards. We gratefully thank all people involved!
ET conducted many activities in line with the steps described in the ET Policy Plan 2009-2013. Our objectives were to address the organizational issues and risks that were identified in this plan in order to prepare our organization adequately for the future. Also, following the request of two potential new member states, discussions on possibilities to cooperate were started with the republics of Estonia and Serbia.
Finally, we hope – with support from all of you – to realize as many as possible challenging achievements in the year 2010!
Prof.Dr. Bruno Meiser Dr. Axel Rahmel Arie Oosterlee, MD MBAPresident Medical Director General Director
Leiden, April 2010

16
1. report of the Board and the central office of Stichting Eurotransplant International (ET) foundation
E. Houwaart, R. Cranendonk and A. Oosterlee, Eurotransplant International Foundation, the Netherlands
The Board of Stichting Eurotransplant International Foundation met on January 22, May 18 and September 30 & October 2, 2009. Three Board members A were (re)-elected by the Assembly. Prof.Dr. Uwe Heemann and Prof.Dr. Caner Süsal were elected as members A in the kidney and tissue typing section respectively. Prof.Dr. Günther Laufer was re-elected in the thoracic section. The Board took leave of Prof.Dr. Rutger Ploeg and Dr. Joannis Mytilineos. Prof.Dr. Guus van Montfort was re-elected by the Board as a member D in the field of finance. Prof.Dr. Uwe Heemann was elected as chairman of the ETKAC in succession to Prof.Dr. Hans de Fijter.
1.1 report of the eurotransplant board
During its first meeting in 2009, the Board continued the discussion on the position of the intestine in relation to the organ allocation sequence. It was explained that due to the fact that from pediatric organ donors only either the pancreas or the intestine can be offered, pediatric patients awaiting an intestine transplantation are in a disadvantage. The discussion resulted in the formulation of an interim solution [RET01.09 (ad int)] firstly to be discussed by the ELIAC and the EPAC.
Reviewing the minutes of the Board meeting, the Board recognized that some topics concern several Advisory Committees. It was therefore decided to organize one meeting with all ET Advisory Committees and the Board of ET in order to discuss new recommendations and changes in a transparent and time efficient way. This joint meeting was organized for the first time on October 2, 2009 in conjunction with the annual ET meeting. The meeting was considered to be an opportunity to discuss topics from different perspectives, which might lead to valuable new insights. One of the topics discussed was the above mentioned pancreas/intestine procurement and rescue allocation. With regard to pancreas/intestine procurement, the Board decided to take a decision on RET01.09 (ad int.) during the Board meeting in Alpbach, Austria on January 27, 2010.
During the year 2009, the Board was informed about the progress of several projects:
EFRETOSThe Board was informed on the progress of the European FRamework for the EvaluaTion of Organ transplantS (EFRETOS – www.efretos.org). The general objective of this project is to evaluate the results of transplantation, by promoting a registry of registries on the follow-up of organ recipients. The project officially started in May 2009 after a kick-off meeting which was attended by all leaders of the work packages. Completion of the project was expected to be a fact within 24 months.
Friends of EurotransplantThe Board approved the constitution of the Board of the Friends of Eurotransplant Foundation, in which initially four members have a seat. The Board will continue to search for further Board members of the Friends of Eurotransplant Foundation.
Implementation of the ET general conditionsDuring the first 2009 meeting, the Board was informed that one ET country had not yet accepted and another had only acknowledged the general conditions. The general conditions are important to ET as in these conditions the distribution of responsibilities and thus liabilities between ET and the transplant centers are clearly defined (e.g. the centers rather than ET are responsible for patient data in the ET waiting lists). In the course of the year, the chairman of the German Bundesärztekammer informed ET that the general conditions contain two issues that cannot be approved by Germany. These issues concern limitation of liability and the fact in case of a dispute the Dutch law is valid. Subsequently, discussions took place in order to find a solution which resulted in a new draft of the general conditions. German approval of this version is still pending.
17
The possible hosting of an ISHLT database and setting up a VAD registry project was postponed. The current global financial crisis made the ISHLT decide not to initiate any new projects for the time being.
The Board several times discussed the entering of potential ET member states. There had been contacts with several European countries – among others Estonia and Serbia – in order to establish possible cooperation. This is a continuing process, on which the Board will be kept updated. ET will furthermore research the possibility to get official support by EU for opening up to new countries.
A representative of the Estonian transplant community had been invited to one of the Board meetings to give a presentation on the Estonian organ donation and transplantation system. This presentation resulted in the Board agreement to go ahead with negotiating on a possible cooperation with Estonia.
The Serbian Minister of Health was invited to another Board meeting to give a presentation on the Serbian organ donation and transplantation system. It was decided to also continue the establishment of cooperation with Serbia and to evaluate the progress during the Board meeting in Alpbach, Austria on January 27, 2010. Furthermore, the Board decided that other European countries will be visited in order to set up or maintain relations and research the possibility for cooperation.
In view of these possible entries of potential member states, the Board agreed upon a list of prerequisites for preliminary cooperation.
The establishment of cooperation with potential new ET member states also resulted in the idea of setting up an ET college for the training of medical professionals in the field of organ donation and transplantation. It was decided to bring this issue forward to the Council of ESOT and investigate the possibility for cooperation.
The Eurotransplant Information Exchange Platform (EuTIEP) met three times. During these meetings presentations from all ET countries and Spain were given. The purpose of information exchange had been fulfilled and there was no need to continue the platform. In order to maintain a direct communication structure with the competent national authorities within ET, the Board accepted the proposal to install an ET Council in which the Board of ET and these authorities are represented.
The ET Council met for the first time in September 2009. The ET contract partners and the Board members B were invited to the meeting. The participants acknowledged the council as an official body. The main topics discussed during the first meeting were approval of the ET Basic Mandate and the expansion of the ET region.
With regard to ET’s financial situation, the Board was informed that the budget negotiations for 2009 had taken place. As a result, ET will be able to implement the most important recommendations from ET’s policy planning project, such as reinforcement of several departments and establishing a central communication function. The Board was also informed that the reserves of ET increased in the course of 2009. In this respect the Board decided to further increase the reserves in the coming years, in order to be able to deal with any unexpected events. In the course of the year 2009 the Board approved the annual accounts 2008 as well as the final budget proposal 2009.
A new model for future budget proposals was presented to the financial authorities, which was very positively received. This new model consists of a basic part, a project compartment and country specific parts. Only large projects will have to be negotiated separately in the future. As a consequence of implementing this new budgetary system, it was necessary to formalize the mandate for basic services (Basic Mandate) which ET provides to its member states.
Following the ET policy planning project a document on the Basic Mandate of ET was composed and presented to the Board. After processing the comments of the Board members, it was decided to proceed with the development of the Basic Mandate which has the support of all national authorities within ET. This ET Basic Mandate was approved by the ET contract partners during the first meeting of the ET Council.
With regard to the lung transplant cooperation between Vienna and several non-ET countries, it was decided to grant the Vienna lung transplant program an extra year for establishing twinning agreements.
The Board approved twinning agreements on lung transplantation between Vienna – Estonia, Vienna – Cyprus and Vienna – Bratislava. The Board furthermore approved the establishment of cooperation between Vienna and Croatia regarding lung transplantation. The aim of this cooperation is that all Croatian patients awaiting lung transplantation will be transplanted in Vienna. All lungs from Croatian donors will be handled as local donors of the Vienna lung transplant program.

18
Following a request of the Belgian Transplantation Society, the Board approved support of the Belgian cross-over program by ET.
A new version of a document on practical handling of data analysis requests including a classification overview of types of requests was presented and approved. This overview describes which type of requests will be carried out in the framework of ET’s Basic Mandate and which type of requests have to be paid for by the requestors. The main idea is that requests involving substantial workload for the data analysis on the side of ET should only be done if the request is approved by the respective ET scientific Advisory Committee. For larger projects every effort should be made to find external financial sources to compensate for the costs involved at ET (for example by finding study sponsors). If such an external financing cannot be provided or found, the ET Financial Committee has to approve the performance of the data analysis (and thereby the involved costs).
The format of the Henk Schippers Young Investigators (HSYI) award has changed. The Board decided to give the award to the best paper composed by authors from the ET region and published in the last year. A selection committee had been formed and consists of four Board members. The 2009 winner of the HSYI award was Dr. Pieter Gillard from the University Hospital, Leuven, Belgium.
With regard to the subject of cross-border migration of Dutch and Belgian transplant patients it was decided to organize a consensus meeting in Belgium to which all Belgian specialists in the field of organ donation and transplantation were to be invited. Creating complete transparency is one of the major aims of this meeting.
In this respect, the idea was brought up to promote the establishment of a European social security number within the EU. With this social security number absolute transparency can be created in the social health care provided by EU countries to EU citizens. It will also give a clear insight in the national balances between donors and transplanted patients.
On request of the ETEC, the Board endorsed the Declaration of Istanbul and decided to send a letter to the ET transplant centers in order to ask for their endorsement as well.
The Board decided to implement the ET Senior DR-matching (ESDP) program in the ET allocation system in the course of 2009.
It was discussed by the Board whether ET should establish a reference laboratory for virology testing. Also, since it was determined that laboratory values vary, it was discussed whether ET should set standards for laboratory values. It was decided to research current standards for laboratory values and to further discuss this issue in the OPC and during the ET winter meeting in Alpbach, Austria.
In view of increasing activities in transplanting composite tissues, for example for hand or face transplantation, it was suggested to draw the attention of the European Commission to the fact that ET has the aspiration to become the responsible organization for allocation of hepatocytes, islets and composite grafts. Since ET has the experience and facilities for quick guidance of the process from donation to transplantation this is considered to be a logical addition to the services ET provides.
The Board was informed about a visit by the ET medical director to the United Network for Organ Sharing in Boston, MA, USA. UNOS is interested in cooperation with ET in respect to exchanging knowledge and experience.
1.2 ReportoftheEurotransplantoffice
For ET, 2009 can be seen as a year in which many steps were taken to specify and further professionalize its services to professionals as well as to national authorities. The activities directly came forth from the ‘Eurotransplant Policy Plan 2009-2013; Phase 1: Milestone 4’. Practically all goals for 2010 were met. In some areas this was noticed and appreciated by our users.
An important step was the formal specification of the responsibilities and main services of ET in ET’s so-called Basic Mandate (published in chapter 2 of this Annual Report). This mandate is the point of reference for many of ET’s activities.
In the area of planning & control several steps regarding organization and responsibilities were taken. A department was set up (Information Services) to prepare and implement policies in the field of business and information activities, which acts as an intermediary between the primary and supportive processes. Program management was introduced and project management was reinforced. Functional and technical application maintenance and support was restructured and the testing process improved.

19
The following processes and activities are reported according to the services mentioned in the Basic Mandate.
Allocation servicesThe allocation process improved through reinforcement of the staff of the Medical Administration with the long term focus of a 24/7 regular staff attendance. An electronic donor log application was developed for registration per donor of deviations in the allocation process which previously was done on paper. This contributes to the quality of the process and makes analysis easier.The Donation Procedure Application (DPA) was introduced in Luxembourg. An application to support the planned Belgian kidney living donor cross-over program was developed and made available.
Development of allocation processIn the area of data collection and analysis a ‘Registry Policy Plan’ was developed and preparations for executing the plan were made. Meanwhile projects and pilots were started to anticipate the implementation of the policy. The European EFRETOS project and the ET registry policy were harmonized wherever appropriate. Reinforcement of the biostatistical capacity was started by initiating the hiring of an additional biostatistician. A study (ESDP) on evaluating different ways of allocating kidneys of elderly (>65 years of age) donors to elderly patients was started. Centers provide data via a web application to ET where data analysis is done.Through the ET Registry for Islets and Pancreas (ETRIP) project a pan-European follow-up application and database for islets and pancreas allocation was developed and implemented by December 2009, thus filling the existing gap.
External networkingIn the field of external networking several important developments took place: the ET Council was established giving national authorities a formal platform to discuss issues and concerns on a supranational level with the Board of ET. This Council met once and formalized ET’s above mentioned Basic Mandate.
Another formal step taken was the formalization of a service level agreement (SLA) between the Nederlandse Transplantatie Stichting (NTS) and ET. In this document the terms of the contract between ET and the NTS are annually specified. It also distinguishes in basic and country specific services that the NTS asks ET to provide.
The ET annual meeting was organized in Leiden in October, just like it had been in the past years. The concept and venue of ET’s winter meeting however, was changed after 25 years. In contrast to previous winter meetings, this meeting was opened up to everyone with an interest in ET. The audience was welcomed in the professional congress center Alpbach, Tirol and was presented with an interesting program. One element of the new concept was the inclusion of workshops into the program.
In line with ET’s 5 years strategy, the so-called Friends of Eurotransplant Foundation was registered and had its first meeting. Friends of Eurotransplant will shortly develop an action plan for the coming period.
In the field of communication a future vision together with a detailed stepwise approach was developed with help of an external consultant. A start was made with hiring a regular communication officer. Also a plan was developed and partially carried out to evaluate our corporate design and the external website and member site.
Information and qualityIn the field of information management, steps were taken to improve cooperation via a method of sharing documents and preliminary steps were made on information policy and information architecture.
The ICT infrastructure was reinforced, as well as the staff supporting it. A start was made with a storage area network (SAN) combined with virtualization of servers to increase availability and service and reduce the number of physical servers and maintenance.
ET underwent several external audits in 2009. ET’s quality assurance system was externally audited by Veritas. Our systems were positively evaluated. A recommendation for improvement was in the meantime been addressed. As from February 2010 ET is accredited for ISO 9001: 2008. In 2009, the German as well as the Dutch national transplant authorities audited ET’s organization and services. Both the German ‘Prüfungskommission’ as well as the NTS determined that ET was delivering its services according to its formal obligations.
FinanceIn the financial field, steps were taken in the enhancement of systems for budgeting, reporting and costing. Budget forecasting was increased by appointing budget responsible persons. Also the hour registration-system was adapted to get more insight. The financial reserves of ET were replenished and a preliminary analysis of the reserves was performed aiming at a (re)definition of reserves and reserve policy in 2010. Progress was made on workforce management and a workforce strategy and policy.

20
PersonnelIn 2009 a start has been made to adapt the staffing of the duty desk according to strategy. It is intended to expand this function to each shift in the future to further assure the quality of our allocation process.
Information services The planning and control systems for functional and technical development as well as maintenance of ET’s software applications were given a boost this year. A function was set up for project and program management as well as test coordination. In its short existence a significant improvement in management information was achieved which strongly enhances prioritization, planning and decision making by the directors.
1.3 Future policy
Also in 2011, the ET Policy Plan 2009-2013 will provide guidance for developing plans and activities. The consolidation strategy will be sustained, whereas we will remain open for discussion with countries that want to explore possibilities for cooperating with ET.
Regarding the internal organization three related developments will specifically demand attention in the coming period:Due to legislative developments in the Netherlands, the economies of scale and scope that ET experienced by sharing 1. personnel with two other organizations are currently under discussion. As ET, NTS and NBF-BIS currently also share vital infrastructure i.e. computer hardware and software, 2. telecommunication equipment etc., a vision for the near future on how to develop a comprehensive separation process will have to be developed and – after the consequences have been thoroughly assessed – implemented.The lease contract for housing ends in 2011. As the ‘housing capacity’ is no longer sufficient for ET, currently 3. alternatives are being investigated.
1.4 Quality assurance & safety
Apart from the yearly regular quality issues, such as updating the ET-manual, the year 2009 was characterized by two special issues.
First the implementation process of the ISO 9001:2008 regulations was continued. Secondly the evaluation of several aspects of our internal and external communication as well as the evaluation of our incidents management system took place. During the past two years the risk awareness of our employees significantly increased. The incident registration system was analyzed and further developed in order to support systematic improvement of the allocation process. The improvements will be implemented in 2010.
Safety management and patient safetySafety management covers different area’s, such as patient safety, minimization of liability risks and financial safety. ET services countries with different legislative systems and with certain country specific allocation rules.In the automated matching process all these country-specific laws and rules are taken into account. The ET-manual gives a transparent and crystal clear outline of all rules and criteria regarding every organ.
IncidentsThe risk awareness of the employees further improved as the number of near-incidents and incidents identified and reported increased (see table below). For this reason it is essential to develop a system for continuous learning, which will be implemented in 2010.
Reported near-incidents and incidents
With an 2007 2008 2009
Internal cause 293 289 347
External cause 263 236 244
Internal & External cause 24 17 20
Total 580 542 611

21
Almost all of the incidents with an internal cause were incidents in incomplete administration, which led to extra administrative operations, such as re-examining the donor log. Incidents with an external cause were discussed with the responsible parties/persons/organizations, such as transplant coordinators and transport companies.
ComplaintsSince October 1, 2008 an e-mail address ([email protected]) for complaints and suggestions is placed on the member site together with an explanation of the purpose of that e-mail address.
In 2009 eight complaints were registered; three by e-mail and five complaints were received by conventional mail. In all cases complaints were made to ET concerning third parties. ET passed on these complaints to (national authorities, hospital, etc) whom they concerned. All complaints were related to communication issues.
Audits by third parties Although certification according to ISO 9001:2000 is valid for another year, ET is now certified according to ISO 9001:2008.The yearly investigation by the German Prüfungskommission led to a satisfactory outcome.The audit by the NTS was successful as well.
Internal auditsBesides the regular audit issues a theme audit, concerning communication, was done. Several weak points were discerned and acted upon.
1.5 advisory committees
The Board discussions, among other issues, concentrated on the proposed recommendations by the various Advisory Committees. Obviously, the work done in these committees contributes to improve the core of the business, namely: state of the art allocation. The Board is grateful for all the time and efforts the Committee members have provided to this important part of the work of ET.
ET positions itself as an independent scientifically oriented organization. Various organ Advisory Committees, of which the chairmen hold a position in the Board of ET, meet several times a year and discuss the impact of new scientific developments in the field of organ allocation, organ procurement as well as transplant ethics. Their conclusions are proposed as recommendations to the Board of ET. In the respective member states national transplant authorities authorize recommendations approved by the ET Board, sometimes with slight adaptations to the national circumstances. A complete list of all recommendations approved in 2009 is published under section 1.6 of this chapter.
Through this practice transplant regulations throughout ET have a great degree of uniformity.
In 2009, the various Advisory Committees met 19 times and submitted 20 recommendations, 19 of which were approved and 1 of which was postponed.
The composition of the various Advisory Committees as per December 31, 2009 was as follows:
KIDNEY ADVISORY COMMITTEE (ETKAC)
Name As of RemarksProf.Dr. U. Heemann, Munich 05.2009 chairman, representative BoardProf.Dr. F. Mühlbacher, Vienna 09.1994 representative Austria Prof.Dr. A. Rosenkranz, Innsbruck 01.2008 representative AustriaDr. P. Duhoux, Luxembourg 09.1994 representative LuxembourgDr. K. Wissing, Brussels (BJ) 01.2004 representative BelgiumDr. P. Peeters, Ghent 02.2006 representative BelgiumVacancy 05.2009 representative GermanyProf.Dr. U. Kunzendorf, Kiel 01.2002 representative GermanyProf.Dr. B. Krämer, Bochum 01.2006 representative GermanyProf.Dr. P. Fornara, Halle 11.2006 representative GermanyDr. J. Homan van der Heide, Groningen 04.2005 representative the NetherlandsDr. L. Hilbrands, Nijmegen 01.2006 representative the NetherlandsDr. M. Arnol, Ljubljana 01.2006 representative SloveniaProf.Dr. J. Pasini, Zagreb 04.2008 representative Croatia

22
Prof.Dr. F.H.J. Claas, Leiden (ETRL) 09.1994 representative TT AssemblyDr. J. de Boer, Eurotransplant 12.2005 secretary
LIVER INTESTINE ADVISORY COMMITTEE (ELIAC)
Name As of RemarksProf.Dr. R. Rogiers, Ghent 09.2007 chairman, representative BoardProf.Dr. R. Steininger, Vienna 11.2004 representative AustriaDr. O. Detry, Liège 01.2000 representative BelgiumProf.Dr. P. Michielsen, Antwerp 01.2008 representative Belgium Prof.Dr. P. Neuhaus, Berlin 09.1994 representative Germany Prof.Dr.N. Senninger, Münster 01.2004 representative GermanyProf.Dr. G. Otto, Mainz 01.2008 representative Germany Prof.Dr. R. Porte, Groningen 01.2006 representative the NetherlandsDr. V. Sojar, Ljubljana 01.2008 representative SloveniaDr. B. Kocman, Zagreb 04.2008 representative CroatiaDr. A. Rahmel, Eurotransplant 02.2007 secretary a.i.
PANCREAS ADVISORY COMMITTEE (EPAC)
Name As of RemarksProf.Dr. W. Schareck, Rostock 12.2005 chairman, representative BoardProf.Dr. P. Hengster, Innsbruck 11.2004 representative AustriaProf.Dr. C. Mathieu, Leuven 02.2006 representative BelgiumDr. H. Arbogast, Munich 03.2009 representative GermanyProf.Dr. R. Viebahn, Bochum 11.2004 representative GermanyDr. A. Kahl, Berlin 01.2006 representative GermanyDr. J. Ringers, Leiden 04.1998 representative the NetherlandsDr. A. Tomazič, Ljubljana 01.2007 representative SloveniaDr. S. Jadrijević, Zagreb 04.2008 representative CroatiaProf.Dr. F.H.J. Claas, Leiden (ETRL) 08.1994 representative TT AssemblyDr. K. Kovac, Eurotransplant 10.2009 secretary
THORACIC ADVISORY COMMITTEE (EThAC)
Name As of RemarksProf.Dr. G. Laufer, Vienna 10.2001 chairman, representative BoardProf.Dr. A. Wasler, Graz 11.2001 representative AustriaProf.Dr. A. Zuckermann, Vienna 01.2008 representative AustriaProf.Dr. P. Evrard, Brussels (LA) 01.2004 representative BelgiumProf.Dr. M. Depauw, Ghent 01.2006 representative BelgiumDr. P. Überfuhr, Munich 02.2006 representative GermanyDr. U. Schulz, Bad Oeynhausen 05.2006 representative GermanyProf.Dr. H. Reichenspurner, Hamburg 02.2008 representative GermanyDr. H. Bittner, Leipzig 02.2008 representative GermanyDr. W. van der Bij, Groningen 06.2001 representative the NetherlandsDr. N. de Jonge, Utrecht 01.2004 representative the NetherlandsProf.Dr. I. Kneževič, Ljubljana 07.2007 representative SloveniaProf.Dr. Z. Sutlić, Zagreb 04.2008 representative CroatiaDr. J. Smits, Eurotransplant 07.2002 secretary
ORGAN PROCUREMENT COMMITTEE (OPC)
Name As of RemarksProf.Dr. D. Ysebaert, Antwerp 10.2005 chairman, representative BoardProf.Dr. G. Berlakovich, Vienna 11.2009 representative TC’s AustriaMs. G. Van Beeumen, Antwerp 02.2006 representative TC’s BelgiumDr. N. Frühauf, Hanover 01.2008 representative DSO GermanyProf.Dr. E. Klar, Rostock 01.2008 representative TC’s GermanyMs. J. Hagenaars, Rotterdam 04.2008 representative TC’s NL

23
Dr. B. Trotovšek, Ljubljana 01.2008 representative SloveniaDr. Z. Zupan, Rijeka 04.2008 representative CroatiaProf.Dr. F. Mühlbacher, Vienna 11.2009 representative ETKACDr. O. Detry, Liège 01.2000 representative ELIACDr. J. Ringers, Leiden 04.2002 representative EPACProf.Dr. A. Zuckermann, Vienna 04.2008 representative EThACProf.Dr. I. Doxiadis, Leiden (ETRL) 02.1998 representative TTACDr. I. Tieken, Eurotransplant 09.2007 secretary
COMPUTER SERVICES WORKING GROUP (CSWG)
Name As of RemarksProf.Dr. F. Mühlbacher, Vienna 09.1995 chairman, representative Board + ETKACDr. R. Kramar, Wels 09.1995 representative AustriaMr.W. Van Donink, Antwerp 10.2009 representative BelgiumDr. M. Schenk, Tübingen 01.2008 representative GermanyDr. A. Hoitsma, Nijmegen 09.1995 representative the NetherlandsMr. T. Campelj, Ljubljana 01.2006 representative SloveniaVacancy representative ELIACDr. W. van der Bij, Groningen 05.2002 representative EThACDr. S. Lems, Groningen 06.1996 representative TTACDrs. T. Valkering, Eurotransplant 05.2008 secretary
TISSUE TYPING ADVISORY COMMITTEE (TTAC)
Name As of RemarksProf.Dr. F.H.J. Claas, Leiden (ETRL) 09.1995 chairman, representative BoardProf.Dr.W. Mayr, Vienna 01.2008 representative AustriaProf.Dr. M.-P. Emonds, Leuven 02.2006 representative BelgiumDr. F. Hentges, Luxembourg 09.1995 representative LuxembourgDr. C. Schönemann, Berlin 11.2002 representative GermanyDr. J. Mytilineos, Ulm 01.2006 representative GermanyDr. S. Lems, Groningen 09.1995 representative the NetherlandsDr. B. Vidan Jeras, Ljubljana 12.1999 representative SloveniaProf.Dr. R. Zunec, Zagreb 04.2008 representative CroatiaProf.Dr. I.I.N. Doxiadis, Leiden (ETRL) 09.1995 secretary
ETHICS COMMITTEE (ETEC)
Name As of RemarksProf.Dr. P. Schotsmans, Leuven 01.2001 chairman, representative BoardDrs. M. Bos, The Hague 05.1995 vice-chairman, representative the NetherlandsProf.Dr. W. Schaupp, Vienna 04.1998 representative AustriaProf.Dr. I. Kerremans, Ghent 03.2004 representative BelgiumProf.Dr. R. Viebahn, Bochum 11.2006 representative GermanyDr. D. Rigler Pleterski, Ljubljana 01.2000 representative SloveniaDr. J. Stoić Brezak, Zagreb 04.2008 representative CroatiaDr. A. Rahmel, Eurotransplant 12.2006 secretary a.i.
FINANCIAL COMMITTEE (FC)
Name As of RemarksProf.Dr. A.P.W.P. van Montfort, Utrecht 05.2003 chairman, representative BoardMag. O. Postl, Vienna 05.1995 representative AustriaProf.Dr. D. Ysebaert, Antwerp 05.1995 representative BelgiumProf.Dr. B. Reichart, Munich 03.2009 representative GermanyMs. M. Konda, Ljubljana 01.2006 representative SloveniaDrs. T. Valkering, Eurotransplant 05.2008 secretary

24
1.6 recommendations approved
In 2009, the following recommendations were submitted by the Advisory Committees and approved by the Board of Eurotransplant International Foundation:
Kidney advisory committee (etKac)
rKac01.09If one or more consecutive kidney transplants fail requiring maintenance dialysis within 3 months after transplantation, and the recipient is re-entered on the waiting list, waiting time will be returned starting from the dialysis time before the first failed transplant.
rKac02.09 Children either on dialysis or registered on the ET waiting list before the age of 16, should be granted a pediatric status until their first successful graft, irrespective of their age at the time of an offer. In case of a pre-emptive registration on the kidney waiting list, the pediatric status will end on the 17th birthday, if dialysis is not initiated before this date.Recipients on dialysis or registered on the waiting list after their 16th birthday will be granted the pediatric status provided that they are proven to be in maturation. This proof has to be delivered by the transplant center by a report of a competent radiologist or pediatric endocrinologist on an X-ray of the left hand that has to be sent to and judged on by two independent auditors appointed by ET. In case of a split decision a third auditor has to be consulted for a final decision. The pediatric status will be withdrawn when dialysis does not start within one year after registration, but will be restored when the recipient fulfils above criteria for maturation at time of institution of dialysis.
The effect of these changes should be evaluated after 2 years.
rKac03.09In case of a donor <16 years of age recipients having the pediatric status are listed directly after 000 HLA mismatched recipients, provided that the recipient specific donor profile on maximum donor age and accepted HLA mismatches is entered into ENIS. The ranking order among these recipients should be according to the ETKAS overall point score system.
rKac04.09The current, age dependent, pediatric bonus should be replaced by a uniform bonus of 100 points for al recipients having the pediatric status.
liver intestine advisory committee (eliac)
rlac01.09 Establishment of a liver transplant follow-up registry (ET Liver-FU Registry)
The dataset to be collected by the ET Liver-FU Registry will be defined by the ELIAC taking into account the needs of 1. established registries (ELTR, CTS). The ELIAC takes the function of the scientific advisory committee of this registry.Liver transplant centers have to report outcome of deceased 2. and living donor transplantation to ET at 3 months after TXP, at one year after TXP and yearly thereafter until the death of the patient. Data have to be delivered within one month of the due data. Non-adherence to this rule will result in informing the ELIAC. The ELIAC strongly suggests that for each country the respective competent national authority will be informed in case of non-compliance.The data delivered to ET Liver-FU Registry will be handled confidentially. As defined in the general ET-data analysis and 3. delivery rules, patient- and center-specific data will only be delivered to the respective transplant center, unless consent is given by the individual patients/centers.ET will offer the option of transfer of the necessary datasets to other registries (e.g. ELTR, CTS). Data exchange with 4. another registry will only take place on explicit request of a transplant center.Studies involving data delivered to ET Liver-FU Registry will be published in the name of the ET liver transplant 5. community. They will require the approval of the ELIAC before publication. Strict rules regarding authorship will be established.
rlac03.09In case for a patient an ACO status for combined transplantation is granted according to the established ACO rules and the patient in addition receives the HU status according to the organ specific criteria for one of the organs for which the ACO status is granted, the patient will be listed in HU status for all the organs he/she is waiting for.

25
In case of a pediatric patient (recipient at time of listing below the age of 12) the initial match MELD shall reflect an expected 3-month mortality of 35%. The matchMELD shall then be increased 3-monthly according to an increase in expected mortality on the waiting list by 15%.
pancreas advisory committee (epac)
rpac01.09The EPAC recommends abandoning granting (international) SU-status for pancreas islet retransplantation.
rpac02.09Any pancreas, independent of donor age and BMI, should first be offered to ACO (Approved Combined Organ) and SU status recipients.
thoracic advisory committee (ethac)
rthac02.07 rephrasedUpon the request for upgrading of an urgency status for heart and/or lung transplant candidates auditors need to provide an answer to the ET allocation office within 6 hours after the request has been sent. In case auditors have additional questions related to the request, these will be forwarded to the requesting center by ET and the requesting center has to answer within 6 hours after these questions were received. In case the requesting center does not agree with the auditors’ decision, the requesting center has maximal one opportunity of putting forward its objection. The auditors’ decision in the second round is the final decision.
rthac01.09All patients needing a cross-match must be reported to ET.•Of all patients needing a cross-match, serum must be sent around to the ET HLA labs responsible for the initial donor •cross-match.It is the responsibility of the transplant centers to ensure that the most recent serum is sent around.•If a sensitized patient is selected in the match and serum for a cross-match is not available in the donor region then no •organ offer will be made or the conditional offer will be withdrawn.The center that has the reserve offer as well as the center with the primary offer should accept that the other center •retrieves the organ. Both teams should decide who is to retrieve the organ. (In case of conflict the center with the primary offer has priority).
rthac02.09The EThAC recommends using the ET Code of Conduct for Thoracic Auditors as a leading document for addressing HU requests.
organ procurement committee (opc)
ropc03.08*Recommendation performing pathology research in case of tumor:In case a tumor is found, it is strongly recommended to perform a pathology research to have a clear diagnosis on this tumor.
ropc04.08*a. If a procured organ can not be transplanted, it is mandatory to contact ET directly and only with approval of ET this organ
can be discarded.b. Discarding an organ is only possible in four ways: 1. Leave the organ with the donor; 2. Send the organ for destruction, a confirmation report is needed; 3. Use for research in case of consent; 4. Allocation is changed towards donation of cells or tissues in case of consent.c. The confirmation report of destruction should be forwarded to ET. ET is responsible for the documentation of these
reports of discarded organs.
26
tissue typing advisory committee (ttac)
rttac01.09In case the HLA-typing is available prior to the start of allocation, a kidney match has to be performed first. If there is a recipient on the AM-mismatch kidney transplant waiting list, who is in need of a combined transplantation, the kidney and non-renal organ(s) will be offered to this recipient first, independent of the non-renal organ ranking.
Financial committee (Fc)
rFc04.08*
The Financial Committee recommends adopting the new model of budget proposal (8037FC08).
rFc01.09The Financial Committee recommends the Board to approve the final budget proposal 2009.
rFc02.09The Financial Committee recommends the Board to approve the annual accounts 2008.
rFc03.09The Financial Committee recommends the Board to approve the budget proposal 2010.
*Submitted by the end of 2008, but accepted by the beginning of 2009.

27
2. Basic principles of the Eurotransplant community
This chapter gives some general information on the ET mission, on the services we provide and on the relationship with our member states. The Eurotransplant International Foundation is responsible for the mediation and allocation of organ donation procedures in Austria, Belgium, Croatia, Germany, Luxembourg, the Netherlands and Slovenia. In this international collaborative framework, the participants include all transplant hospitals, tissue typing laboratories and hospitals where organ donations take place. The ET region numbers well over 124.5 million.
In the following paragraphs the following topics are covered:ET’s mission, aims and goals;1. The basic services that ET provides to its member states as laid down in ET’s Basic Mandate;2. Formal support to ET by the ministries of Health of ET’s member states: the so-called ‘Joint Declaration’.3.
2.1 eurotransplant mission statement
MissionEurotransplant is a service organization for transplant candidates through the collaborating transplant programs within the organization.
Eurotransplant AimsEurotransplant is an international, non-profit exchange organization whose aim is to encourage organ transplantation. It encourages the international exchange of donor organs across a region with 124.5 million inhabitants. Eurotransplant provides services to transplant centers and their associated tissue typing laboratories and donor hospitals in Austria, Belgium, Croatia, Germany, Luxembourg, the Netherlands and Slovenia.
GoalsTo achieve an optimal use of available donor organs and tissues.•To secure a transparent and objective selection system, based upon medical criteria.•To assess the importance of factors which have the greatest influence on waiting list mortality and transplant results. •To support donor procurement to increase the supply of donor organs and tissues.•To further improve the results of transplantation through scientific research and to publish and present these results.•Promotion, support and coordination of organ donation and transplantation in the broadest sense of terms.•
The following document was agreed upon by all National Authorities of Eurotransplant. It describes that basic services that every member states expects Eurotransplant to provide. The budget for Eurotransplant’s basic services is guaranteed by all National Authorities. Specific wishes from member states are often laid down in country specific Service Level Agreements.
2.2 basic mandate of eurotransplant
The Basic Mandate of Eurotransplant includes the following elements:Assignment1. Services 2. Support 3.
1. AssignmentThe processET’s primary assignment is to coordinate the international exchange and allocation of donor organs. To carry out this assignment ET performs activities related to the whole process of organ donation and transplantation. The process includes the following responsibilities:
Coordination of donor procedures and support of donor procurement;•Maintaining a waiting list;•Receiving donor offers;•Providing central support and advice for the transplant centers, tissue typing laboratories and donor hospitals;•International coordination of transportation;•

Allocating the organs;•Following up of the transplantation;•Evaluating the transplantation results;•Improving the results of transplantation through scientific research.•
The environmentET interacts with various stakeholders such as patients, national regulating transplant authorities, national representatives of the transplant societies, financing authorities, donor hospitals, transplant centers, tissue typing laboratories, other allocation organizations, scientific societies and the employees of the Leiden office. ET allocates organs based on rules set by national and international legislation. ET is in continuous interaction with the outside world to analyze and further develop the allocation policy.ET delivers its services in a social and political framework which demands transparency. Therefore comprehensive quality and patient safety management systems will be in place and maintained.
Competences of the organizationTo perform its mandate, the organization of ET has to be in a position to:
Perform allocation in a 24-hour service framework;1. Continuously update and improve the process of allocation;2. Establish and maintain an external network;3. Report on and account for the outcome of its services.4.
This means the organization shall:Operate and sustain its services continuously;•Manage an influx of complex information from different sources. This incoming information varies in its format, structure •and content; Perform the activities to realize it’s international and external orientation;•Maintain close communication with regulatory and legislative authorities – nationally as well as at European Union and •international level;Implement, comply with and support the development of (inter)national rules and regulations;•Disseminate the knowledge of ET concerning allocation;•Participate in international cooperation and the European framework on topics as standards/best practices, issuing of •rules, shortage of organs and international harmonization;Coordinate international cooperation;•Gather data in order to perform the allocation process, to report on outcome of the process, to account for the outcome and •in order to further develop the process. The analyses have to be within the framework of EU and national legislation.
2. Services To be able to perform its mandate ET sustains an efficient, effective and proportionate organization. ET follows the relevant ISO standards (ref. ISO 9001:2000). Its activities are aimed at realizing effective services with adequate quality regarding issues such as patient-safety, accuracy, speed and efficiency.
Important aspects of ET’s quality system involve the ET Reference Laboratory (ETRL) and the audit system for evaluating the High Urgent status of the patients on the waiting list.
The main mandated tasks performed by ET are described below.
Allocation servicesTo be able to perform the services 24 hours a day, seven days a week ET maintains a staff of medical doctors, an allocation service desk and a medical administration function.To support this primary process supportive services are required in the area of housing, facilities, information and communication.
In realizing continuity of its services ET complies with all relevant rules and regulations concerning labor conditions in the Netherlands.
The ET Reference Laboratory provides 24 hours a day, 7 days a week immunological support to the allocation office and to the transplant centers. The ETRL is responsible for the proficiency testing of all histocompatibility laboratories associated to ET and the evaluation of highly immunized patients to be included in the acceptable mismatch program.The development of ET’s allocation processes is driven by the evaluation of post transplant results. For this purpose ET sustains a transplant follow-up registry.
28

Development of allocation processTo continuously update and improve the allocation process ET develops and maintains a network of experts. Because the allocation process differs per organ on allocation rules and specific details, the network represents these different scientific areas. The fields of experience relate to the different organs and ET Advisory Committees are formed along these lines: kidney, thoracic, liver and intestine, pancreas. Also on more general topics committees are organized: on organ procurement, tissue typing and ethical issues. To advise on supporting functions there are also Advisory Committees on finance and information services.
All of these committees meet regularly. The ET staff prepares and conducts the meetings and guides recommendations through the organization and the governance structure.
ET takes care of checking the recommendations on their compliance with the different national and international legislative and regulatory frameworks that are concerned.
ET actively joins in European projects related to organ transplantation. It is also actively involved in national and international regulatory projects. In this way ET works at the improvement of its services, at standardization of processes and methods and at setting as well as learning from, best practices of organizations outside the ET network.
External networkingET performs activities to establish and maintain international relations that can help ET to improve the allocation process, but also get understanding of, and support for its activities.
Therefore ET organizes twice a year congresses focusing on the professional, scientific, and political communities in the field of organ transplantation within its member states. These congresses are held in autumn and winter in a way that enhances networking between the participants and the staff of ET, thus contributing to mutual trust and understanding within the organization. ET furthermore issues a Newsletter to inform its stakeholders on the recommendations made by the ET Board. ET has also developed a website to inform its stakeholders.
On behalf of its members ET actively makes itself known to, and establishes connections with, the European Community and its representatives who are acting in the field of organ transplantation and issuing rules.
In order to enable benchmarking as well as identification and dissemination of best practices, ET sustains an external network with international organ exchange organizations in the area of donation and transplantation.
Reporting and accountingET accounts for the results of its services in various ways and with various reports. They make standard reports on all kind of topics concerning the transplantation process. These reports are made available to the members and the outside world via the ET public website or the member site (extranet) or via alternate routes agreed upon with those concerned.
ET also disseminates the services and their results through (co)publishing and giving lectures on congresses and meetings.
Every year ET reports on the preceding year in an annual report in which account is given, both on the allocation process as well as the financial developments. In the annual report account is also given for the realization of the general policy in the field of allocation and its supportive processes.
Every year ET sees to it that the financial accounts of the preceding year are approved by an external auditor.
To coordinate all external contacts ET develops and maintains a communication policy and actively pursues this policy.
3. Support To facilitate the process of allocation and the related processes and thereby the organization and people working in it, ET organizes several supportive processes. These processes are detailed below in the sub-sections Clearing house, Information and quality and Other..Clearing houseTo facilitate the international exchange of organs, ET supports the centers with international transport logistics. ET fulfills and sustains a clearing house function concerning the settlements of costs between the donating and receiving centers in the event of international organ exchange within the organization.
Information and qualityAllocation of organs is an information intensive process which needs substantial support of automated systems. Therefore ET develops and maintains the information systems that are required. They support the analysis of processes, of allocation
29

30
rules and of other information and transform this into effective information systems. To operate the information systems an adequate infrastructure for information and communication is realized and maintained.
ET will adequately test all procedures and systems and maintains a quality system to assure this.
OtherTo enable ET to operate as a service organization its supportive functions have to be sustained. Therefore ET maintains and sustains a supporting organization in fields of management (planning & control), housing, human resource management, finance, ICT and facilities.
4. GovernanceET has a governance structure1 with an international external board representing the member states, the so-called Board of ET. The Board of ET is responsible for the management of the Foundation and supervises the Board of Directors. The Board of Directors is responsible for the day-to-day management of the organization and is composed of two directors, a general and a medical director. The Board of ET meets on a regular basis with the two directors. These meetings are prepared by the directors and staff of ET.
5. FinancesET’s activities are entirely financed by the health insurance companies in the participating countries. The organization’s budget and the resulting registration fees are negotiated annually with the financers and/or the national authorities.
The following document was signed during the conference Eurotransplant organized on the occasion of its 40th anniversary in Sint Gerlach for the ministers of Health Care of the Eurotransplant member states. The ministers affirmed the cooperation with the other member states and the perceived importance of Eurotransplant for each of them.
2.3 Joint Declaration on cooperation within the framework of eurotransplant international Foundation
The Minister of Social Affairs and Public Health of the Kingdom of Belgium,
The Minister of Health and Social Welfare of the Republic of Croatia,
The Federal Minister of Health of the Federal Republic of Germany,
The Minister of Health and Social Security of the Grand Duchy Luxembourg,
The Minister of Health, Welfare and Sport of the Kingdom of the Netherlands,
The Federal Minister of Health, Family and Youth of the Republic of Austria andThe Minister of Health of the Republic of Slovenija,
issue the following Joint Declaration on cooperation within the framework of Eurotransplant International Foundation:
We, Ministers of Health, wish to express our recognition of the activities performed by the Eurotransplant International Foundation (ETI) in Leiden, the Netherlands.
We are of the opinion that the subjects addressed in the Joint Declaration of November 2000 are today undiminished valid.
We emphasize:that the importance of international cooperation on organ transplantation within the Eurotransplant International •Foundation framework has been demonstrated and should be continued;the necessity and added value of a fruitful cooperation between the professionals and the national authorities within the •framework of Eurotransplant as opposed to separate agreements;
Note
1. This governance structure is described in ET’s Articles of Assocation

that it is of crucial importance for the acceptance of transplantation medicine in the participating countries and in the •interest of the patients that distribution of the allocated donor organs is performed as fairly as possible within a transparent and objective allocation system according to medical criteria;the necessity of having systems operational for quality and safety in the area of organ donation. The state of a donor •organ eligible to be allocated by Eurotransplant International Foundation must comply with those safety and quality requirements that are or might be imposed in accordance with the most recent advancements in medical science;our involvement as Ministers of Health with Eurotransplant International Foundation, its transparent and unambiguous •allocation system and the responsibility of Eurotransplant International Foundation towards the participating member states.
Given the above considerations and the need to take into account national regulatory frameworks as well as efforts directed at the implementation of appropriate measures to improve the existing opportunities for post-mortem organ donation, we, Ministers of Health
agree that the mutual exchange of practices in the area of post-mortem organ donation between the Eurotransplant •International Foundation member states is valuable and supported by us;agree that Eurotransplant International Foundation fulfils an important role as a platform for the exchange of knowledge •and practices; encourage the realization of a collection system for transplant results within Eurotransplant International Foundation.•
This declaration was signed on September 24, 2007 in Valkenburg aan de Geul, the Netherlands:
Dr. Dirk Cuypers
on behalf of the Minister of Social Affairs and Public Health of the Kingdom of Belgium, President of the Board of Directors of the Federal Public Service Health, Food Chain, Safety and Environment
Prof. Dr. Neven Ljubičić
The Minister of Health and Social Welfare of the Republic of Croatia,
Mrs. Ulla Schmidt
The Federal Minister of Health of the Federal Republic of Germany
Mr. Mars di Bartolomeo
The Minister of Health and Social Security of the Grand Duchy of Luxembourg
Dr. Ab Klink
The Minister of Health, Welfare and Sport of the Kingdom of the Netherlands
Dr. Andrea Kdolsky
The Federal Minister of Health, Family and Youth of the Republic of Austria
Mrs. Zofija Mazej Kukovič
The Minister of Health of the Republic of Slovenija
31

32
3. Eurotransplant: donation, waiting lists and transplants
introduction
‘A picture paints a thousand words’ - therefore we introduced several new figures in this year’s Annual Report. We hope these figures will further improve the value of this report and will make the developments in transplantation and the work of Eurotransplant even more transparent to you. For example figure 3.1 shows at a glance the dramatic increase in the median donor age over the last 20 years for the different organs. The aging of donors used for transplantation is most pronounced for liver and kidney transplantation while for pancreas transplantation the donor age only shows a minimal increase. With the exception of heart transplant recipients the median age of the transplanted patients has gone up in the same period of time, although less pronounced than the donor’s age (figure 3.3).
For the first time, all figures regarding the number of patients on the waiting list also depict the number of ‘not transplantable’ patients. For example figure 4.2 shows that more than 30% of the patients on the kidney waiting list are currently reported as ‘not transplantable’ and the fraction of the ‘not transplantable’ patients among all patients on the waiting list has been steadily increasing over the past 20 years. ET would like to encourage all centers to carefully check for all patients currently listed as ‘not transplantable’ whether they could be listed in an active waiting list status or whether they should even be removed from the waiting list.
A problem related to this high rate of ‘not transplantable’ patients on the waiting list is the late reporting of ‘death on the waiting list’, especially in this group of patients. This delay in reporting of a patient’s death date is the main reason why numbers on waiting list mortality for 2008 (table 3.9) are almost 10% higher as reported in our previous Annual Report. We would therefore like to remind all transplant centers that reporting of all urgency changes of their patients should be done in a timely fashion to the ET office!
After the dramatic drop in organ donation in almost all countries in 2008 the number of deceased organ donors used for a transplant increased again in 2009. The most pronounced increase took place in Austria (+26.2%), but also in the Netherlands (+7.0%) and Belgium (+4.2%) a substantial increase in donation could be observed resulting in an overall rise of the number of donors by 3.5% in the ET area (table 3.1). The details for the different organs can be found in the organ specific tables and corresponding figures.
On first view it might be surprising that the development of the median waiting time of patients on the active waiting list (figure 3.4) and the median waiting time to transplant (figure 3.5) is not running in parallel. But this observation reflects of course the fact that the allocation rules of ET do not only take into account waiting time, but also other factors like matching and urgency. In kidney transplantation the increasing number of transplants in the framework of the Eurotransplant Senior Program (ESP) is of additional importance, because the waiting time in the ‘old-for-old’ program is as expected shorter than waiting times for patients who receive their organ via the standard ETKAS allocation.
There are some additional small changes in this report compared to the previous years: for the calculation of the HLA mismatches between donor and recipients in kidney transplantation (table 4.4) the new HLA nomenclature as introduced by the TTAC has been used. As a consequence there are now some small changes when comparing these data to previous reports. Please be aware that this table also includes kidney transplants allocation via the ESP and via rescue allocation. According to both schemes HLA matching is not taken into account. HLA matching for those recipients who received their kidneys via the standard ETKAS allocation is even better than shown here for the over-all kidney recipient group.
We would like to encourage you to give us feedback on the changes introduced in this year’s Annual Report including suggestions for further improvements so that we can further increase the usability and adapt it to your wishes!

33
table 3.1 number of deceased organ donors used for a transplant, by donor country, from 2005 to 2009
Donor country population (millions) 2005 2006 2007 2008 2009 pmp 2008/2009
a austria 8.4 200 201 181 168 212 25.4 26.2 %B belgium 10.8 237 273 291 265 276 25.7 4.2 % croatia 4.4 0 0 33 79 77 17.4 -2.5 %D germany 82.0 1185 1227 1285 1184 1196 14.6 1.0 %L luxembourg 0.5 3 6 1 9 0 -100.0 % netherlands 16.5 217 200 257 201 215 13.0 7.0 % slovenia 2.0 21 30 22 36 33 16.2 -8.3 %
et 124.6 1863 1937 2070 1942 2009 16.1 3.5 %non-et 82 84 69 61 65 6.6 %
total 1945 2021 2139 2003 2074 3.5 %
Figure 3.1 median age of deceased donors in eurotransplant, used for a transplant
25
30
35
40
45
50
55
60
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
Kidney
Heart
Lung
Liver
Pancreas
years
table 3.2(i) number of deceased organ donors used for a transplant, by organ, from 2005 to 2009
year of registration 2005 2006 2007 2008 2009 2008/2009
organ donors, total 1945 2021 2139 2003 2074 3.5 %
Kidney 1753 1833 1930 1833 1859 1.4 %heart 562 587 598 583 580 -0.5 %lung 438 454 503 508 513 1.0 %liver 1302 1395 1569 1550 1631 5.2 %pancreas 305 245 255 257 226 -12.1 %
table 3.2(ii) number of deceased organ donors used for a transplant, by organ and donor country, in 2009
Donor country a B D L non-et total
organ donors, total 212 276 77 1196 0 215 33 65 2074
Kidney 193 237 74 1117 0 202 31 5 1859heart 81 70 23 346 0 39 9 12 580lung 64 89 10 244 0 60 4 42 513liver 159 230 62 1004 0 143 22 11 1631pancreas 34 36 13 119 0 21 3 0 226

34
table 3.3(i) Demographic data on deceased organ donors, used for a transplant, from 2005 to 2009
age (years) 2005 2006 2007 2008 2009 2008/2009
0-15 91 67 77 73 70 -4.1 %16-55 1157 1202 1239 1145 1089 -4.9 %56-64 333 337 396 371 399 7.5 %≥65 364 415 427 414 516 24.6 %
total 1945 2021 2139 2003 2074 3.5 %
gender 2005 2006 2007 2008 2009 2008/2009
Female 891 930 969 903 976 8.1 %male 1054 1091 1170 1100 1098 -0.2 %
total 1945 2021 2139 2003 2074 3.5 %
blood group 2005 2006 2007 2008 2009 2008/2009
a 850 906 933 835 855 2.4 %ab 127 103 125 98 110 12.2 %b 213 216 230 248 241 -2.8 %o 755 796 851 822 868 5.6 %
total 1945 2021 2139 2003 2074 3.5 %
cause of death 2005 2006 2007 2008 2009 2008/2009
accident 475 423 471 459 385 -16.1 %natural 1388 1536 1612 1480 1621 9.5 %suicide 59 42 29 47 43 -8.5 %other 23 20 27 17 25 47.1 %
total 1945 2021 2139 2003 2074 3.5 %
table 3.3(ii) Demographic data on deceased organ donors, used for a transplant, in 2009
age a B D L non-et total %
0-15 3 11 2 37 0 7 0 10 70 3.4 %16-55 122 157 40 580 0 127 19 44 1089 52.5 %56-64 37 59 22 222 0 41 8 10 399 19.2 %≥65 50 49 13 357 0 40 6 1 516 24.9 %
total 212 276 77 1196 0 215 33 65 2074 100.0 %
gender a B D L non-et total %
Female 101 122 40 566 0 109 12 26 976 47.1 %male 111 154 37 630 0 106 21 39 1098 52.9 %
total 212 276 77 1196 0 215 33 65 2074 100.0 %
blood group a B D L non-et total %
a 104 101 33 500 0 81 13 23 855 41.2 %ab 14 13 3 69 0 7 0 4 110 5.3 %b 22 25 11 145 0 25 8 5 241 11.6 %o 72 137 30 482 0 102 12 33 868 41.9 %
total 212 276 77 1196 0 215 33 65 2074 100.0 %
cause of death a B D L non-et total %
accident 48 82 15 168 0 41 12 19 385 18.6 %natural 154 159 59 1026 0 164 17 42 1621 78.2 %suicide 7 26 3 0 0 4 3 0 43 2.1 %other 3 9 0 2 0 6 1 4 25 1.2 %
total 212 276 77 1196 0 215 33 65 2074 100.0 %

35
table 3.4a(i) number of donors, used for a transplant, by type of donor, from 2005 to 2009
2005 2006 2007 2008 2009 2008/2009
Deceased 1945 2021 2139 2003 2074 3.5 %Domino 16 10 10 7 3 -57.1 %living 972 1007 1123 1161 1244 7.1 %
total 2933 3038 3272 3171 3321 4.7 %
Note: Living donors are now counted by date of transplant, previously this was by date of registration
table 3.4a(ii) number of donors, used for a transplant, by type and donor country, in 2009
Deceased % Domino % living % total
austria 212 73.4 % 0 77 26.6 % 289belgium 276 78.9 % 2 0.6 % 72 20.6 % 350croatia 77 83.7% 0 15 16.3 % 92germany 1196 64.4 % 1 0.1 % 660 35.5 % 1857luxembourg 0 0 0 0netherlands 215 33.9 % 0 420 66.1 % 635slovenia 33 100.0 % 0 0 33
non-et 65 100.0 % 0 0 65
total 2074 62.5 % 3 0.1 % 1244 37.4 % 3321
table 3.4b(i) number of deceased donors, used for a transplant, by type of donor, from 2005 to 2009
2005 2006 2007 2008 2009 2008/2009
soD 637 617 597 461 487 5.6 %moD 1308 1404 1542 1542 1587 2.9 %
total 1945 2021 2139 2003 2074 3.5 %
table 3.4b(ii) number of deceased donors, used for a transplant, by type and donor country, in 2009
soD % moD % total % of total
austria 46 21.7 % 166 78.3 % 212 10.2 %belgium 65 23.6 % 211 76.4 % 276 13.3 %croatia 15 19.5 % 62 80.5 % 77 3.7 %germany 222 18.6 % 974 81.4 % 1196 57.7 %luxembourg 0 0.0 % 0 0.0 % 0 0.0 %netherlands 67 31.2 % 148 68.8 % 215 10.4 %slovenia 11 33.3 % 22 66.7 % 33 1.6 %
non-et 61 93.8 % 4 6.2 % 65 3.1 %
total 487 23.5 % 1587 76.5 % 2074 100.0 %
moD - multiple organ donor - a donor from which more than one organ type has been used in a transplantsoD - single organ donor
table 3.4c(i) non-heart beating (nhb) donors, used for a transplant, from 2005 to 2009
nhb category 2005 2006 2007 2008 2009 2008/2009
i - Dead on arrival 0 1 1 0 0 0.0 %ii - unsuccesful resuscitation 10 8 8 8 4 -73.3 %iii - awaiting heart arrest 99 113 131 115 140 -9.1 %iv - heart arrest in brain dead donor 2 1 0 0 0 0.0 %
total 111 123 140 123 144 -14.8 %

36
table 3.4c(ii) nhb donors, used for a transplant, by donor country, in 2009
nhb category a B total %
ii - unsuccesful resuscitation 1 1 2 4 2.8 %iii - awaiting heart arrest 0 57 83 140 97.2 %
total 1 58 85 144 100.0 %
Note: NHB donors are now counted only when used for a transplant, previously this was the total number reported
table 3.4d(i) transplants from nhb donors, from 2005 to 2009
2005 2006 2007 2008 2009 2008/2009
Kidney kidney 206 222 244 200 243 21.5 %kidney en bloc 1 1 3 1 3 200.0 %
total 207 223 247 201 246 22.4 %
liver split liver 1 0 0 0 0 0.0 %whole liver 25 33 36 46 69 50.0 %
total 26 33 36 46 69 50.0 %
liver + Kidney liver + kidney 0 0 0 1 0 -100.0 %
total 0 0 0 1 0 -100.0 %
lung single lung 0 0 1 4 4 0.0 %double lung 4 4 9 12 29 141.7 %
total 4 4 10 16 33 106.3 %
pancreas pancreas 2 0 2 7 2 -71.4 %
total 2 0 2 7 2 -71.4 %
total 239 260 295 271 350 29.15 %
table 3.4d(ii) transplants from nhb donors, by donor country, in 2009
recipient country type of transplant a B total %
austria Kidney 2 10 3 15 6.1 %belgium 0 69 2 71 28.9 %netherlands 0 11 149 160 65.0 %
total Kidney 2 90 154 246 100.0 %
belgium liver 0 39 2 41 59.4 %netherlands 0 2 26 28 40.6 %
total liver 0 41 28 69 100.0 %
belgium lung 0 13 2 15 45.5 %netherlands 0 0 18 18 54.5 %
total lung 0 13 20 33 100.0 %
belgium pancreas 0 1 1 2 100.0 %
total pancreas 0 1 1 2 100.0 %
table 3.5(i) active eurotransplant waiting list, by organ, as per December 31, from 2005 to 2009
type composition 2005 2006 2007 2008 2009 2008/2009
heart heart 864 904 933 989 1121 13.3 %heart + kidney 18 15 24 16 27 68.8 %heart + liver 0 1 2 2 4 100.0 %heart + lung 64 59 55 57 38 -33.3 %heart + lung + kidney 0 0 0 0 1 0.0 %
heart total 946 979 1014 1064 1191 11.9 %

37
table 3.5(i) (continued)
Kidney kidney 11515 11069 10910 10687 10533 -1.4 %kidney + heart 18 15 24 16 27 68.8 %kidney + heart + lung 0 0 0 0 1 0.0 %kidney + liver 60 62 67 72 97 34.7 %kidney + liver + pancreas 1 1 0 2 1 -50.0 %kidney + lung 3 2 3 5 2 -60.0 %kidney + pancreas 217 242 304 300 349 16.3 %
Kidney total 11814 11391 11308 11082 11010 -0.6 %
liver liver 2066 2249 2351 2354 2525 7.3 %liver + heart 0 1 2 2 4 100.0 %liver + kidney 60 62 67 72 97 34.7 %liver + lung 3 5 4 8 6 -25.0 %liver + pancreas 4 1 5 4 8 100.0 %liver + pancreas + kidney 1 1 0 2 1 -50.0 %
liver total 2134 2319 2429 2442 2641 8.1 %
lung lung 668 758 849 846 964 13.9 %lung + heart 64 59 55 57 38 -33.3 %lung + heart + kidney 0 0 0 0 1 0.0 %lung + kidney 3 2 3 5 2 -60.0 %lung + liver 3 5 4 8 6 -25.0 %
lung total 738 824 911 916 1011 10.4 %
pancreas pancreas 59 48 43 55 68 23.6 %pancreas + kidney 217 242 304 300 349 16.3 %pancreas + kidney + liver 1 1 0 2 1 -50.0 %pancreas + liver 4 1 5 4 8 100.0 %
pancreas total 281 292 352 361 426 18.0 %
table 3.5(ii) active eurotransplant waiting list, by organ, as per December 31, 2009
type composition a B D L total %
heart heart 61 50 14 920 0 58 18 1121 94.1 %heart + kidney 4 6 0 16 0 0 1 27 2.3 %heart + liver 1 0 0 3 0 0 0 4 0.3 %heart + lung 0 2 0 34 0 2 0 38 3.2 %heart + lung + kidney 0 0 0 1 0 0 0 1 0.1 %
heart total 66 58 14 974 0 60 19 1191 100.0 %
Kidney kidney 801 806 321 7652 0 901 52 10533 95.7 %kidney + heart 4 6 0 16 0 0 1 27 0.2 %kidney + heart + lung 0 0 0 1 0 0 0 1 0.0 %kidney + liver 2 24 2 66 0 3 0 97 0.9 %kidney + liver + pancreas 0 0 0 1 0 0 0 1 0.0 %kidney + lung 0 0 0 2 0 0 0 2 0.0 %kidney + pancreas 20 30 1 276 0 22 0 349 3.2 %
Kidney total 827 866 324 8014 0 926 53 11010 100.0 %
liver liver 102 166 54 2083 0 105 15 2525 95.6 %liver + heart 1 0 0 3 0 0 0 4 0.2 %liver + kidney 2 24 2 66 0 3 0 97 3.7 %liver + lung 1 1 0 3 0 1 0 6 0.2 %liver + pancreas 0 0 0 7 0 1 0 8 0.3 %liver + pancreas + kidney 0 0 0 1 0 0 0 1 0.0 %
liver total 106 191 56 2163 0 110 15 2641 100.0 %
lung lung 72 92 0 617 0 183 0 964 95.4 %lung + heart 0 2 0 34 0 2 0 38 3.8 %lung + heart + kidney 0 0 0 1 0 0 0 1 0.1 %lung + kidney 0 0 0 2 0 0 0 2 0.2 %lung + liver 1 1 0 3 0 1 0 6 0.6 %

38
table 3.5(ii) (continued)
lung total 73 95 0 657 0 186 0 1011 100.0 %
pancreas pancreas 12 16 0 30 0 10 0 68 16.0 %pancreas + kidney 20 30 1 276 0 22 0 349 81.9 %pancreas + kidney + liver 0 0 0 1 0 0 0 1 0.2 %pancreas + liver 0 0 0 7 0 1 0 8 1.9 %
pancreas total 32 46 1 314 0 33 0 426 100.0 %
table 3.6(i) registration events on the eurotransplant waiting list, by organ, from 2005 to 2009
all registration events 2005 2006 2007 2008 2009 2008/2009
Kidney 5209 5335 6212 5808 5849 0.7 %heart 1053 1009 1015 1052 1121 6.6 %lung 723 739 805 846 843 -0.4 %liver 2302 2515 2631 2675 2923 9.3 %pancreas 374 317 365 341 334 -2.1 %
total 9661 9915 11028 10722 11070 3.2 %
new registration events 2005 2006 2007 2008 2009 2008/2009
Kidney 4354 4553 5398 4967 4941 -0.5 %heart 1025 975 992 1030 1094 6.2 %lung 681 696 748 799 787 -1.5 %liver 1994 2203 2338 2372 2592 9.3 %pancreas 304 273 304 281 291 3.6 %
total 8358 8700 9780 9449 9705 2.7 %
re-registration events 2005 2006 2007 2008 2009 2008/2009
Kidney 855 782 814 841 908 8.0 %heart 28 34 23 22 27 22.7 %lung 42 43 57 47 56 19.1 %liver 308 312 293 303 331 9.2 %pancreas 70 44 61 60 43 -28.3 %
total 1303 1215 1248 1273 1365 7.2 %
table 3.6(ii) registration events on the eurotransplant waiting list, by organ and country, in 2009
all registration events a B D L total %
Kidney 463 636 185 3409 0 1123 33 5849 52.8 %heart 102 107 34 791 0 60 27 1121 10.1 %lung 138 124 0 477 0 104 0 843 7.6 %liver 205 338 89 2099 0 164 28 2923 26.4 %pancreas 31 53 10 209 0 30 1 334 3.0 %
total 939 1258 318 6985 0 1481 89 11070 100.0 %
new registration events a B D L total %
Kidney 369 540 182 2878 0 939 33 4941 50.9 %heart 100 102 33 773 0 59 27 1094 11.3 %lung 122 120 0 443 0 102 0 787 8.1 %liver 184 306 84 1854 0 138 26 2592 26.7 %pancreas 27 37 10 190 0 26 1 291 3.0 %
total 802 1105 309 6138 0 1264 87 9705 100.0 %
re-registration events a B D L total %
Kidney 94 96 3 531 0 184 0 908 66.5 %heart 2 5 1 18 0 1 0 27 2.0 %lung 16 4 0 34 0 2 0 56 4.1 %liver 21 32 5 245 0 26 2 331 24.2 %pancreas 4 16 0 19 0 4 0 43 3.2 %
total 137 153 9 847 0 217 2 1365 100.0 %
Registrations for multiple organs are counted on each waiting list respectively

39
table 3.7(i) number of transplanted organs**, by organ, by donor type, from* 2005 to 2009
Deceased 2005 2006 2007 2008 2009 2008/2009
Kidney 3406 3539 3728 3522 3590 1.9 %heart 563 587 598 581 581 0.0 %lung 839 871 960 972 999 2.8 %liver 1364 1436 1625 1606 1691 5.3 %pancreas 304 247 255 256 227 -11.3 %
total 6476 6680 7166 6937 7088 2.2 %
living 2005 2006 2007 2008 2009 2008/2009
Kidney 866 901 1032 1091 1148 5.2%heart (domino) 1 0 0 0 0 0.0%liver (partial and domino) 121 116 101 82 98 19.5%lung 0 0 0 0 1 0.0%
total 988 1017 1133 1173 1247 6.3%
table 3.7(ii) number of transplanted organs**, by organ, by donor type, by country of transplant, in* 2009
Deceased a B D L non-et total %
Kidney 363 435 157 2192 2 398 43 0 3590 50.6 %heart 73 68 20 363 0 36 18 3 581 8.2 %lung 209 169 0 505 0 114 0 2 999 14.1 %liver 146 220 60 1118 0 129 18 0 1691 23.9 %pancreas 33 42 13 117 0 20 2 0 227 3.2 %
total 824 934 250 4295 2 697 81 5 7088 100.0 %
living a B D L non-et total %
Kidney 69 49 13 600 0 417 0 0 1148 92.1 %liver (partial and domino) 7 25 2 61 0 3 0 0 98 7.9 %lung 1 0 0 0 0 0 0 0 1 0.1 %
total 77 74 15 661 0 420 0 0 1247 100.0 %
* based on transplant registration date ** each liver split counted as one ** each liver split counted as one ** each double lung counted as two
table 3.8(i) transplants from 2005 to 2009
Deceased Donors 2005 2006 2007 2008 2009 2008/2009
heart 531 539 562 544 553 1.7 %Kidney 3094 3220 3415 3179 3302 3.9 %Kidney en bloc 22 20 24 28 29 3.6 %single lung 103 120 89 82 79 -3.7 %Double lung 345 338 410 419 435 3.8 %liver 1196 1273 1439 1405 1515 7.8 %split liver 119 90 105 113 121 7.1 %heart + single kidney 10 15 13 10 8 -20.0 %heart + double lung 21 30 21 23 20 -13.0 %heart + liver 1 1 2 3 0 -100.0 %Kidney + single lung 0 0 1 0 0 0.0 %Kidney + double lung 1 3 0 1 2 100.0 %Kidney + liver 41 61 64 73 45 -38.4 %Kidney + split liver 2 2 4 4 1 -75.0 %liver + kidney en bloc 1 1 1 2 0 -100.0 %liver + single lung 0 1 0 0 0 0.0 %liver + double lung 1 2 4 1 3 200.0 %heart + double lung + kidney 0 0 0 1 0 -100.0 %heart + double lung + liver 0 2 0 0 0 0.0 %pancreas 31 31 29 20 13 -35.0 %pancreas + kidney 209 195 180 194 172 -11.3 %pancreas + liver 2 2 5 5 4 -20.0 %pancreas + liver + kidney 1 1 1 0 2 --pancreas islets 17 5 15 17 18 5.9 %pancreas islets + kidney 2 0 0 0 0 0.0 %
total (deceased donors) transplants 5750 5952 6384 6124 6322 3.2 %

40
table 3.8(i) (continued)
living Donors 2005 2006 2007 2008 2009 2008/2009
heart (domino) 1 0 0 0 0 0.0 %Kidney 866 901 1032 1090 1148 5.3 %Kidney + liver 0 0 0 1 0 -100.0 %liver (partial and domino) 121 116 101 81 98 21.0 %lung 0 0 0 0 1 --
total (living donors) transplants 988 1017 1133 1172 1247 6.4 %
all donors 2005 2006 2007 2008 2009 2008/2009
total transplants 6738 6969 7517 7296 7569 3.7 %
table 3.8(ii) transplants in 2009, by transplant country
Deceased donor transplants a B D L non-et total% of
deceased donor
transplants
heart 72 65 20 341 0 34 18 3 553 8.7 %Kidney 326 402 141 2008 2 382 41 0 3302 51.8 %Kidney en bloc 0 7 1 20 0 1 0 0 29 0.5 %single lung 9 11 0 39 0 20 0 0 79 1.2 %Double lung 98 78 0 213 0 45 0 1 435 6.8 %liver 140 203 58 979 0 117 18 0 1515 23.8 %split liver 0 12 1 99 0 9 0 0 121 1.9 %heart + single kidney 0 2 0 6 0 0 0 0 8 0.1 %heart + double lung 1 1 0 16 0 2 0 0 20 0.3 %heart + liver 0 0 0 0 0 0 0 0 0 0.0 %Kidney + single lung 0 0 0 0 0 0 0 0 0 0.0 %Kidney + double lung 0 0 0 2 0 0 0 0 2 0.0 %Kidney + liver 5 4 1 32 0 3 0 0 45 0.7 %Kidney + split liver 0 0 0 1 0 0 0 0 1 0.0 %liver + kidney en bloc 0 0 0 0 0 0 0 0 0 0.0 %liver + single lung 0 0 0 0 0 0 0 0 0 0.0 %liver + double lung 1 0 0 2 0 0 0 0 3 0.0 %heart + double lung + kidney 0 0 0 0 0 0 0 0 0 0.0 %heart + double lung + liver 0 0 0 0 0 0 0 0 0 0.0 %pancreas 1 0 0 8 0 4 0 0 13 0.2 %pancreas + kidney 32 12 13 102 0 11 2 0 172 2.7 %pancreas + liver 0 0 0 4 0 0 0 0 4 0.1 %pancreas + liver + kidney 0 1 0 1 0 0 0 0 2 0.0 %pancreas islets 0 12 0 2 0 4 0 0 18 0.3 %pancreas islets + kidney 0 0 0 0 0 0 0 0 0 0.0 %
total (deceased donors) transplants 685 810 235 3875 2 632 79 4 6322 100.0 %
living donor transplants a B D L non-et total% of living
donor transplants
Kidney 69 49 13 600 0 417 0 0 1148 92.1 %liver (partial and domino) 7 25 2 61 0 3 0 0 98 7.9 %lung 1 0 0 0 0 0 0 0 1 0.1 %
total (living donors) transplants 77 74 15 661 0 420 0 0 1247 100.0 %
all donors a B D L non-et total
total transplants 762 884 250 4536 2 1052 79 4 7569
table 3.9(i) mortality on the eurotransplant waiting list, by date of death, from 2005 to 2009
Waiting list 2005 2006 2007 2008 2009 2008/2009
Kidney 566 563 525 536 474 -11.6 %liver 456 470 436 495 522 5.5 %pancreas 20 22 19 27 26 -3.7 %heart 222 252 222 212 217 2.4 %lung 154 123 119 167 131 -21.6 %
total 1418 1430 1321 1437 1370 -4.7 %
total patients 1357 1361 1259 1374 1302 -8.8 %

41
table 3.9(ii) mortality on the eurotransplant waiting list in 2009, by country
Waiting list a B D L total
Kidney 28 27 8 319 0 88 4 474liver 41 51 15 383 0 24 8 522pancreas 2 1 0 20 0 3 0 26heart 6 18 11 169 0 4 9 217lung 8 9 0 95 0 19 0 131
total 85 106 34 986 0 138 21 1370
total patients 82 99 34 931 0 135 21 1302
Figure 3.2 median age of patients on active waiting list
25
30
35
40
45
50
55
60
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
Kidney
Heart
Lung
Liver
Pancreas
years
Figure 3.3 median age of transplant recipients (deceased donor transplants)
25
30
35
40
45
50
55
60
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
Kidney
Heart
Lung
Liver
Pancreas
years

42
Figure 3.4 median waiting time for patients on active waiting list at year end
0
6
12
18
24
30
36
42
48
54
60
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
Kidney
Heart
Lung
Liver
Pancreas
months
Basedontimesincefirstdialysisforkidneypatients,otherwisetimeonwaitinglist
Figure 3.5 median waiting time to transplant (deceased donor transplants)
0
6
12
18
24
30
36
42
48
54
60
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
Kidney
Heart
Lung
Liver
Pancreas
months
Basedontimesincefirstdialysisforkidneypatients,otherwisetimeonwaitinglist

43
4. Kidney: donation, waiting lists and transplants
table 4.1(i) Deceased donors / kidneys in eurotransplant, from 2005 to 2009
Donors
year of registration 2005 2006 2007 2008 2009 2008/2009
all donors 2249 2299 2411 2233 2305 3.2 %non-kidney donors 252 242 216 217 243 12.0 %Kidney donors 1997 2057 2195 2016 2062 2.3 %Kidney donors not used 244 224 265 183 203 10.9 %One kidney used 104 121 145 138 131 -5.1 %Two kidneys used 1649 1712 1785 1695 1728 1.9 %total kidney donors used 1753 1833 1930 1833 1859 1.4 %
Kidneys
year of registration 2005 2006 2007 2008 2009 2008/2009
reported 3960 4081 4365 3999 4103 2.6 %offered 3835 3946 4208 3912 4026 2.9 %accepted 3599 3713 3952 3711 3800 2.4 %transplanted 3402 3545 3715 3528 3587 2.4 %
table 4.1(ii) Deceased donors / kidneys in eurotransplant in 2009
Donors
Donor country a B D total et non-et total % all donors
all donors 225 302 80 1248 255 36 2146 159 2305 100.0 %non-kidney donors 15 33 2 41 9 1 101 142 243 10.5 %Kidney donors 210 269 78 1207 246 35 2045 17 2062 89.5 %Kidney donors not used 17 32 4 90 44 4 191 12 203 8.8 %One kidney used 14 20 2 70 19 2 127 4 131 5.7 %Two kidneys used 179 217 72 1047 183 29 1727 1 1728 75.0 %total kidney donors used 193 237 74 1117 202 31 1854 5 1859 80.7 %
Kidneys
Donor country a B D total et non-et total % reported
reported 415 534 155 2405 492 70 4071 32 4103 100.0 %offered 413 524 151 2394 445 69 3996 30 4026 98.1 %accepted 394 486 146 2284 417 63 3790 10 3800 92.6 %transplanted 372 454 146 2164 385 60 3581 6 3587 87.4 %

44
Figure 4.1 Kidney waiting list, number of patients at year end, by urgency
0
2000
4000
6000
8000
10000
12000
14000
16000
18000
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009
High Urgency
Highly Immunized
Immunized
Transplantable
Not Transplantable
Figure 4.2 Kidney waiting list, percentage of patients at year end, by urgency
0%
20%
40%
60%
80%
100%
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009
High Urgency
Highly Immunized
Immunized
Transplantable
Not Transplantable
table 4.2(i) active kidney transplant waiting list, as per December 31, from 2005 to 2009 - characteristics
type of transplant 2005 2006 2007 2008 2009 2008/2009
Kidney 11515 11069 10910 10687 10533 -1.4 %Kidney + heart 18 15 24 16 27 68.8 %Kidney + heart + lung 0 0 0 0 1 --Kidney + liver 60 62 67 72 97 34.7 %Kidney + liver + pancreas 1 1 0 2 1 -50.0 %Kidney + lung 3 2 3 5 2 -60.0 %Kidney + pancreas 217 242 304 300 349 16.3 %
total 11814 11391 11308 11082 11010 -0.6 %

45
table 4.2(ii) active kidney transplant waiting list, as per December 31 , 2009 - characteristics
type of transplant a B D total %
Kidney 801 806 321 7652 901 52 10533 95.7 %Kidney + heart 4 6 0 16 0 1 27 0.2 %Kidney + heart + lung 0 0 0 1 0 0 1 0.0 %Kidney + liver 2 24 2 66 3 0 97 0.9 %Kidney + liver + pancreas 0 0 0 1 0 0 1 0.0 %Kidney + lung 0 0 0 2 0 0 2 0.0 %Kidney + pancreas 20 30 1 276 22 0 349 3.2 %
total 827 866 324 8014 926 53 11010 100.0 %
table 4.3(i) active kidney-only transplant waiting list, as per December 31, from 2005 to 2009 - characteristics
blood group 2005 2006 2007 2008 2009 2008/2009
a 4423 4082 3924 3770 3707 -1.7 %ab 212 213 144 175 189 8.0 %b 1313 1287 1307 1265 1258 -0.6 %o 5567 5489 5535 5477 5379 -1.8 %
total 11515 11069 10910 10687 10533 -1.4 %
% pra current 2005 2006 2007 2008 2009 2008/2009
0-5 % 10341 9964 9741 9347 9063 -3.0 %6-84 % 1006 959 997 1182 1243 5.2 %85-100 % 134 95 113 100 188 88.0 %not reported 34 51 59 58 39 -32.8 %
total 11515 11069 10910 10687 10533 -1.4 %
sequence 2005 2006 2007 2008 2009 2008/2009
First 9596 9262 9159 8943 8751 -2.1 %repeat 1919 1807 1751 1744 1782 2.2 %
total 11515 11069 10910 10687 10533 -1.4 %
Waiting time (years) basis dialysis date2005 2006 2007 2008 2009 2008/2009
pre-emptive 286 239 275 326 329 0.9 %0-1 2699 2516 2401 2363 2319 -1.9 %2-4 5523 5319 5269 5054 4799 -5.0 %5+ 3007 2995 2965 2944 3086 4.8 %
total 11515 11069 10910 10687 10533 -1.4 %
Waiting time (years) basis date put on Wl2005 2006 2007 2008 2009 2008/2009
0-1 5101 4825 5047 5069 4861 -4.1 %2-4 4624 4494 4197 3950 3917 -0.8 %5+ 1790 1750 1666 1668 1755 5.2 %
total 11515 11069 10910 10687 10533 -1.4 %
table 4.3(ii) active kidney-only transplant waiting list, as per December 31, 2009 - characteristics
blood group a B D total %
a 289 244 114 2774 266 20 3707 35.2 %ab 13 17 10 134 15 189 1.8 %b 107 76 60 869 138 8 1258 11.9 %o 392 469 137 3875 482 24 5379 51.1 %
total 801 806 321 7652 901 52 10533 100.0 %

46
table 4.3(ii) (continued)
% pra current a B D total %
0-5 % 686 610 272 6682 767 46 9063 86.0 %6-84 % 99 118 37 862 121 6 1243 11.8 %85-100 % 13 77 6 83 9 0 188 1.8 %not reported 3 1 6 25 4 0 39 0.4 %
total 801 806 321 7652 901 52 10533 100.0 %
sequence a B D total %
First 608 624 316 6431 721 51 8751 83.1 %repeat 193 182 5 1221 180 1 1782 16.9 %
total 801 806 321 7652 901 52 10533 100.0 %
Waiting time (years) basis dialysis datea B D total %
pre-emptive 26 90 1 132 77 3 329 3.1 %0-1 295 321 93 1309 292 9 2319 22.0 %2-4 383 314 161 3497 416 28 4799 45.6 %5+ 97 81 66 2714 116 12 3086 29.3 %
total 801 806 321 7652 901 52 10533 100.0 %
Waiting time (years) basis date put on Wla B D total %
0-1 460 513 189 3230 442 27 4861 46.2 %2-4 282 228 130 2896 359 22 3917 37.2 %5+ 59 65 2 1526 100 3 1755 16.7 %
total 801 806 321 7652 901 52 10533 100.0 %
Figure 4.3 number of deceased donor kidney transplants, by recipient urgency at transplant
0
500
1000
1500
2000
2500
3000
3500
4000
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009
High Urgency
Highly Immunized
Immunized
Transplantable

47
Figure 4.4 percentage of deceased donor kidney transplants, by recipient urgency at transplant
0%
20%
40%
60%
80%
100%
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009
High Urgency
Highly Immunized
Immunized
Transplantable
table 4.4(i) Kidney transplant characteristics from 2005 to 2009
Deceased donor kidney transplants
type of transplant 2005 2006 2007 2008 2009 2008/2009
Kidney-only 3094 3220 3415 3179 3302 3.9 %Kidney en bloc 22 20 24 28 29 3.6 %Kidney + pancreas 211 195 180 194 172 -11.3 %Kidney + heart 10 15 13 10 8 -20.0 %Kidney + split liver 2 2 4 4 1 -75.0 %Kidney + whole liver 41 61 64 73 45 -38.4 %Kidney en bloc + whole liver 1 1 1 2 -- -100.0 %Kidney + pancreas + whole liver 1 1 1 -- 2 0.0 %Kidney + single lung -- -- 1 -- -- 0.0 %Kidney + double lungs 1 3 -- 1 2 100.0 %Kidney + heart + double lungs -- -- -- 1 -- -100.0 %
total 3383 3518 3703 3492 3561 1.98 %
Kidney-only transplant (including kidney en bloc)
hla - a, b, Dr mismatches 2005 2006 2007 2008 2009 2008/2009
0 477 520 460 451 439 -2.7 %1 229 234 259 251 229 -8.8 %2 763 760 748 751 731 -2.7 %3 893 908 1007 886 1011 14.1 %4 429 463 528 485 496 2.3 %5 216 214 297 261 303 16.1 %6 62 96 105 99 99 0.0 %not calculated 47 45 35 23 23 0.0 %
total 3116 3240 3439 3207 3331 3.9 %
blood group 2005 2006 2007 2008 2009 2008/2009
a 1361 1435 1530 1404 1445 2.9 %ab 247 202 243 185 204 10.3 %b 374 395 413 431 424 -1.6 %o 1134 1208 1253 1187 1258 6.0 %
total 3116 3240 3439 3207 3331 3.9 %

48
table 4.4(i) (continued)
pra 2005 2006 2007 2008 2009 2008/2009
0-5% 2841 2887 3097 2883 2909 0.9 %6-84% 242 312 293 286 366 28.0 %85-100% 28 34 39 35 55 57.1 %not reported 5 7 10 3 1 -66.7 %
total 3116 3240 3439 3207 3331 3.9 %
Waiting time (months) 2005 2006 2007 2008 2009 2008/2009
pre-emptive 35 42 38 43 38 -11.6 %0-5 48 45 47 45 46 2.2 %6-11 93 107 131 108 88 -18.5 %12-23 315 369 407 350 422 20.6 %24-59 1231 1244 1262 1149 1282 11.6 %60 + 1394 1433 1554 1512 1455 -3.8 %
total 3116 3240 3439 3207 3331 3.9 %
sequence 2005 2006 2007 2008 2009 2008/2009
First 2670 2717 2903 2731 2841 4.0 %repeat 446 523 536 476 490 2.9 %
total 3116 3240 3439 3207 3331 3.9 %
table 4.4(ii) Kidney transplant characteristics - 2009
Deceased donor kidney transplants
type of transplant a B D L total et non-et total %
Kidney-only 326 402 141 2008 2 382 41 3302 0 3302 92.7 %Kidney en bloc 0 7 1 20 0 1 0 29 0 29 0.8 %Kidney + pancreas 32 12 13 102 0 11 2 172 0 172 4.8 %Kidney + heart 0 2 0 6 0 0 0 8 0 8 0.2 %Kidney + both lungs 0 0 0 2 0 0 0 2 0 2 0.1 %Kidney + split liver 0 0 0 1 0 0 0 1 0 1 0.0 %Kidney + whole liver 5 4 1 32 0 3 0 45 0 45 1.3 %Kidney + pancreas + whole liver
0 1 0 1 0 0 0 2 0 2 0.1 %
total 363 428 156 2172 2 397 43 3561 0 3561 100.0 %
Kidney-only transplant (including kidney en bloc)
hla - a, b, Dr mismatches a B D L total et non-et total %
0 37 35 9 306 0 50 2 439 0 439 13.2 %1 22 36 11 125 0 32 3 229 0 229 6.9 %2 70 126 29 411 1 85 9 731 0 731 21.9 %3 92 163 50 559 1 130 16 1011 0 1011 30.4 %4 53 39 27 318 0 48 11 496 0 496 14.9 %5 32 9 13 224 0 25 0 303 0 303 9.1 %6 9 1 1 79 0 9 0 99 0 99 3.0 %not calculated 11 0 2 6 0 4 0 23 0 23 0.7 %
total 326 409 142 2028 2 383 41 3331 0 3331 100.0 %
blood group a B D L total et non-et total %
a 167 158 53 919 1 130 17 1445 0 1445 43.4 %ab 17 22 15 126 0 24 0 204 0 204 6.1 %b 39 44 21 260 1 55 4 424 0 424 12.7 %o 103 185 53 723 0 174 20 1258 0 1258 37.8 %
total 326 409 142 2028 2 383 41 3331 0 3331 100.0 %

49
table 4.4(ii) (continued)
pra a B D L total et non-et total %
0-5% 279 349 126 1778 2 338 37 2909 0 2909 87.3 %6-84% 41 48 16 214 0 43 4 366 0 366 11.0 %85-100% 6 12 0 35 0 2 0 55 0 55 1.7 %not reported 0 0 0 1 0 0 0 1 0 1 0.0 %
total 326 409 142 2028 2 383 41 3331 0 3331 100.0 %
Waiting time (months) a B D L total et non-et total %
pre-emptive 7 13 0 18 0 8 0 46 0 46 1.4 %0-5 15 26 2 34 0 9 2 88 0 88 2.6 %6-11 48 121 12 185 1 51 4 422 0 422 12.7 %12-23 180 177 43 648 1 216 17 1282 0 1282 38.5 %24-59 70 58 85 1133 0 92 17 1455 0 1455 43.7 %60 + 6 14 0 10 0 7 1 38 0 38 1.1 %
total 326 409 142 2028 2 383 41 3331 0 3331 100.0 %
sequence a B D L total et non-et total %
First 244 359 140 1742 2 314 40 2841 0 2841 85.3 %repeat 82 50 2 286 0 69 1 490 0 490 14.7 %
total 326 409 142 2028 2 383 41 3331 0 3331 100.0 %
table 4.5(i) living donor kidney transplants - kidney-only from 2005 to 2009
Kidney-only 2005 2006 2007 2008 2009 2008/2009
related 500 517 587 609 612 0.5 %non-related 366 384 445 482 536 11.2 %
total 866 901 1032 1091 1148 5.2 %
related 2005 2006 2007 2008 2009 2008/2009
brother / sister 155 156 181 195 195 0.0 %Father 102 115 128 136 110 -19.1 %mother 178 187 211 209 223 6.7 %son / daughter 32 26 26 39 32 -17.9 %grandfather / -mother 6 10 5 6 9 50.0 %grandchild 1 0 0 0 0 0.0 %uncle / aunt 13 12 11 14 17 21.4 %nephew / niece 12 9 15 4 15 275.0 %cousin 0 0 0 2 9 350.0 %blood related: nos* 1 2 10 4 2 -50.0 %
total 500 517 587 609 612 0.5 %
non-related 2005 2006 2007 2008 2009 2008/2009
anonymous donor 0 0 6 20 25 25.0 %Friend 0 0 29 41 42 2.4 %not blood related family 17 26 29 33 44 33.3 %not blood related: nos* 8 3 4 3 6 100.0 %not related 72 74 63 51 35 -31.4 %spouse / partner 269 281 314 334 384 15.0 %
total 366 384 445 482 536 11.2 %
* NOS - Not otherwise specified

50
table 4.5(ii) living donor kidney transplants - kidney-only - 2009
Kidney-only a B D total %
related 39 31 8 337 197 612 53.3 %non-related 30 18 5 263 220 536 46.7 %
total 69 49 13 600 417 1148 100.0 %
related a B D total %
brother / sister 10 9 1 94 81 195 31.9 %Father 8 2 1 68 31 110 18.0 %mother 15 13 4 147 44 223 36.4 %son / daughter 1 3 0 6 22 32 5.2 %grandfather / -mother 1 0 0 5 3 9 1.5 %uncle / aunt 1 2 1 6 7 17 2.8 %nephew / niece 2 1 0 4 8 15 2.5 %cousin 1 1 0 6 1 9 1.5 %blood related: nos* 0 0 1 1 0 2 0.3 %
total 39 31 8 337 197 612 100.0 %
non-related a B D total %
anonymous donor 0 0 0 0 25 25 4.7 %Friend 0 0 0 21 21 42 7.8 %not blood related family 5 2 0 21 16 44 8.2 %not blood related: nos* 0 0 0 2 4 6 1.1 %not related 1 1 1 4 28 35 6.5 %spouse / partner 24 15 4 215 126 384 71.6 %
total 30 18 5 263 220 536 100.0 %
* NOS - Not otherwise specified
Figure 4.5 Dynamics of the eurotransplant kidney transplant waiting list and transplants between 1969 and 2009
1969 1971 1973 1975 1977 1979 1981 1983 1985 1987 1991 1993 1995 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009Kidney waiting list 450 892 1147 1200 934 1929 2135 2928 5150 6740 8376 9418 10510 11324 11975 12313 12524 12450 12653 12382 12251 11814 11393 11308 11082 11010Living donor transplants 9 5 11 33 33 33 53 108 150 161 129 127 212 411 526 579 569 617 697 646 803 866 901 1032 1091 1148Deceased donor transplants 102 228 454 583 800 1050 1263 1645 1965 2665 3395 3293 3064 3110 3068 3050 3145 3121 3047 3352 3185 3383 3518 3703 3492 3561
0
2000
4000
6000
8000
10000
12000
14000
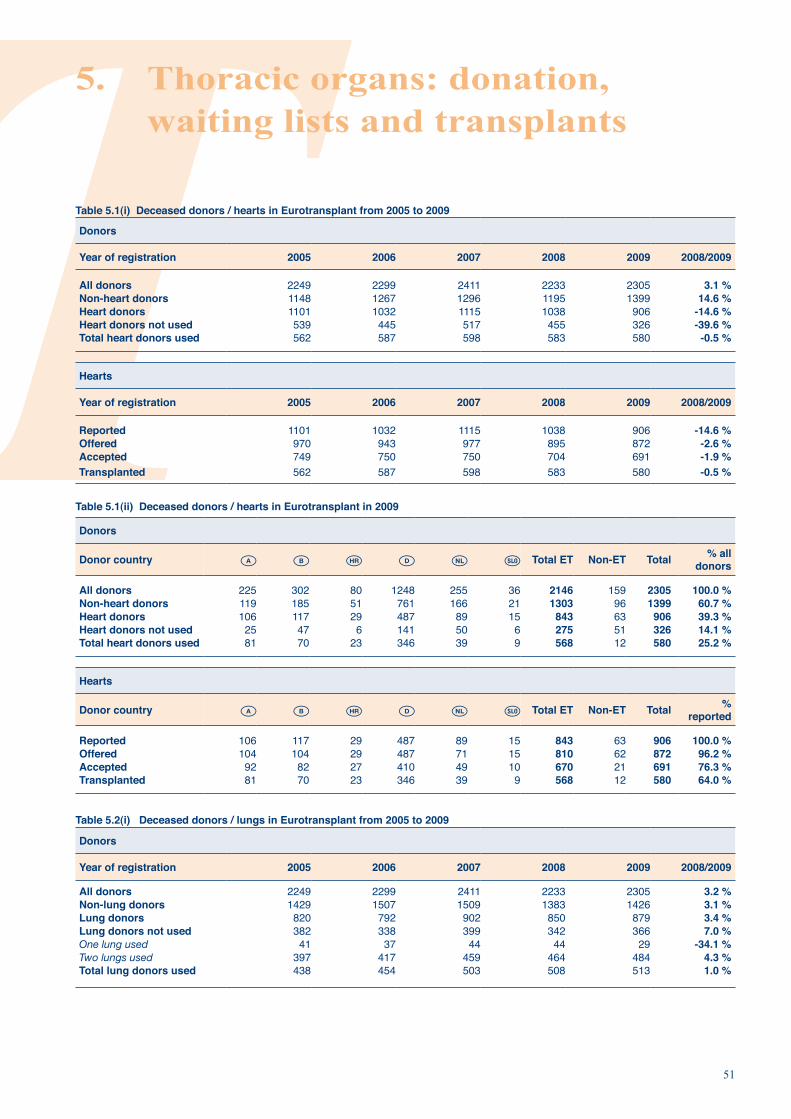
51
5. Thoracic organs: donation, waiting lists and transplants
table 5.1(i) Deceased donors / hearts in eurotransplant from 2005 to 2009
Donors
year of registration 2005 2006 2007 2008 2009 2008/2009
all donors 2249 2299 2411 2233 2305 3.1 %non-heart donors 1148 1267 1296 1195 1399 14.6 %heart donors 1101 1032 1115 1038 906 -14.6 %heart donors not used 539 445 517 455 326 -39.6 %total heart donors used 562 587 598 583 580 -0.5 %
hearts
year of registration 2005 2006 2007 2008 2009 2008/2009
reported 1101 1032 1115 1038 906 -14.6 %offered 970 943 977 895 872 -2.6 %accepted 749 750 750 704 691 -1.9 %transplanted 562 587 598 583 580 -0.5 %
table 5.1(ii) Deceased donors / hearts in eurotransplant in 2009
Donors
Donor country a B D total et non-et total % all donors
all donors 225 302 80 1248 255 36 2146 159 2305 100.0 %non-heart donors 119 185 51 761 166 21 1303 96 1399 60.7 %heart donors 106 117 29 487 89 15 843 63 906 39.3 %heart donors not used 25 47 6 141 50 6 275 51 326 14.1 %total heart donors used 81 70 23 346 39 9 568 12 580 25.2 %
hearts
Donor country a B D total et non-et total % reported
reported 106 117 29 487 89 15 843 63 906 100.0 %offered 104 104 29 487 71 15 810 62 872 96.2 %accepted 92 82 27 410 49 10 670 21 691 76.3 %transplanted 81 70 23 346 39 9 568 12 580 64.0 %
table 5.2(i) Deceased donors / lungs in eurotransplant from 2005 to 2009
Donors
year of registration 2005 2006 2007 2008 2009 2008/2009
all donors 2249 2299 2411 2233 2305 3.2 %non-lung donors 1429 1507 1509 1383 1426 3.1 %lung donors 820 792 902 850 879 3.4 %lung donors not used 382 338 399 342 366 7.0 %One lung used 41 37 44 44 29 -34.1 %Two lungs used 397 417 459 464 484 4.3 %total lung donors used 438 454 503 508 513 1.0 %

52
table 5.2(i) (continued)
lungs
year of registration 2005 2006 2007 2008 2009 2008/2009
reported 1609 1556 1787 1677 1734 3.4 %offered 1553 1516 1758 1646 1716 4.3 %accepted 1141 1154 1333 1283 1342 4.6 %transplanted 835 871 962 972 997 2.6 %
table 5.2(ii) Deceased donors / lungs in eurotransplant in 2009
Donors
Donor country a B D total et non-et total % all donors
all donors 225 302 80 1248 255 36 2146 159 2305 100.0 %non-lung donors 127 164 62 839 152 20 1364 62 1426 61.9 %lung donors 98 138 18 409 103 16 782 97 879 38.1 %lung donors not used 34 49 8 165 43 12 311 55 366 15.9 %One lung used 2 5 1 15 4 0 27 2 29 1.3 %Two lungs used 62 84 9 229 56 4 444 40 484 21.0 %total lung donors used 64 89 10 244 60 4 471 42 513 22.3 %
lungs
Donor country a B D total et non-et total % reported
reported 196 271 36 814 199 32 1548 186 1734 100.0 %offered 196 268 36 812 199 32 1543 173 1716 99.0 %accepted 171 210 26 650 150 20 1227 115 1342 77.4 %transplanted 126 173 19 473 116 8 915 82 997 57.5 %
Figure 5.1 heart waiting list, number of patients at year end, by urgency
0
200
400
600
800
1000
1200
1400
1600
1800
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009
High Urgency
Urgent
Transplantable
Not Transplantable

53
Figure 5.2 heart waiting list, percentage of patients at year end, by urgency
0%
20%
40%
60%
80%
100%
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009
High Urgency
Urgent
Transplantable
Not Transplantable
table 5.3(i) active heart transplant waiting list as per December 31 from 2005 to 2009 - characteristics
2005 2006 2007 2008 2009 2008/2009
heart 846 904 933 989 1121 13.3 %heart + kidney 18 15 24 16 27 68.8 %heart + liver 0 1 2 2 4 100.0 %heart + lung 64 59 55 57 38 -33.3 %heart + lung + kidney 0 0 0 0 1 --
total 946 979 1014 1064 1191 11.9%
table 5.3(ii) active heart transplant waiting list as per December 31, 2009 - characteristics
a B D total %
heart 61 50 14 920 58 18 1121 94.1 %heart + kidney 4 6 0 16 0 1 27 2.3 %heart + liver 1 0 0 3 0 0 4 0.3 %heart + lung 0 2 0 34 2 0 38 3.2 %heart + lung + kidney 0 0 0 1 0 0 1 0.1 %
total 66 58 14 974 60 19 1191 100.0 %
table 5.4(i) active heart-only transplant waiting list as per December 31, from 2005 to 2009 - characteristics
blood group 2005 2006 2007 2008 2009 2008/2009
a 419 434 442 469 528 12.6 %ab 17 17 22 22 25 13.6 %b 105 89 93 97 121 24.7 %o 323 364 376 401 447 11.5 %
total 864 904 933 989 1121 13.3 %
% pra current 2005 2006 2007 2008 2009 2008/2009
0-5 % 527 554 561 613 665 8.5 %6-84 % 18 15 16 22 16 -27.3 %85-100 % 1 2 0 0 1 --not reported 318 333 356 354 439 24.0 %
total 864 904 933 989 1121 13.3 %

54
table 5.4(i) (continued)
sequence 2005 2006 2007 2008 2009 2008/2009
First 849 885 923 979 1106 13.0 %repeat 15 19 10 10 15 50.0 %
total 864 904 933 989 1121 13.3 %
Waiting time (months) basis date put on Wl 2005 2006 2007 2008 2009 2008/2009
0-5 346 298 330 303 372 22.8 %6-11 190 180 168 209 230 10.0 %12-23 218 228 203 216 226 4.6 %24+ 110 198 232 261 293 12.3 %
total 864 904 933 989 1121 13.3 %
table 5.4(ii) active-heart only transplant waiting list as per December 31, 2009 - characteristics
blood group a B D total %
a 31 23 8 431 27 8 528 47.1 %ab 2 1 21 1 25 2.2 %b 5 8 1 97 7 3 121 10.8 %o 25 17 4 371 23 7 447 39.9 %
total 61 50 14 920 58 18 1121 100.0 %
% pra current a B D total %
0-5 % 14 12 7 578 52 2 665 59.3 %6-84 % 0 1 0 13 2 0 16 1.4 %85-100 % 0 0 0 1 0 0 1 0.1 %not reported 47 37 7 328 4 16 439 39.2 %
total 61 50 14 920 58 18 1121 100.0 %
sequence a B D total %
First 60 49 14 907 58 18 1106 98.7 %repeat 1 1 0 13 0 0 15 1.3 %
total 61 50 14 920 58 18 1121 100.0 %
Waiting time (months) basis date put on Wl a B D total %
0-5 28 30 9 281 20 4 372 33.2 %6-11 21 18 4 174 10 3 230 20.5 %12-23 6 2 0 199 15 4 226 20.2 %24+ 6 0 1 266 13 7 293 26.1 %
total 61 50 14 920 58 18 1121 100.0 %
table 5.5(i) active heart + lung transplant waiting list, as per December 31, from 2005 to 2009 - characteristics
type of transplant 2005 2006 2007 2008 2009 2008/2009
heart + lung 64 59 55 57 38 -33.3 %heart + lung + kidney 0 0 0 0 1 --
total 64 59 55 57 39 -31.6 %
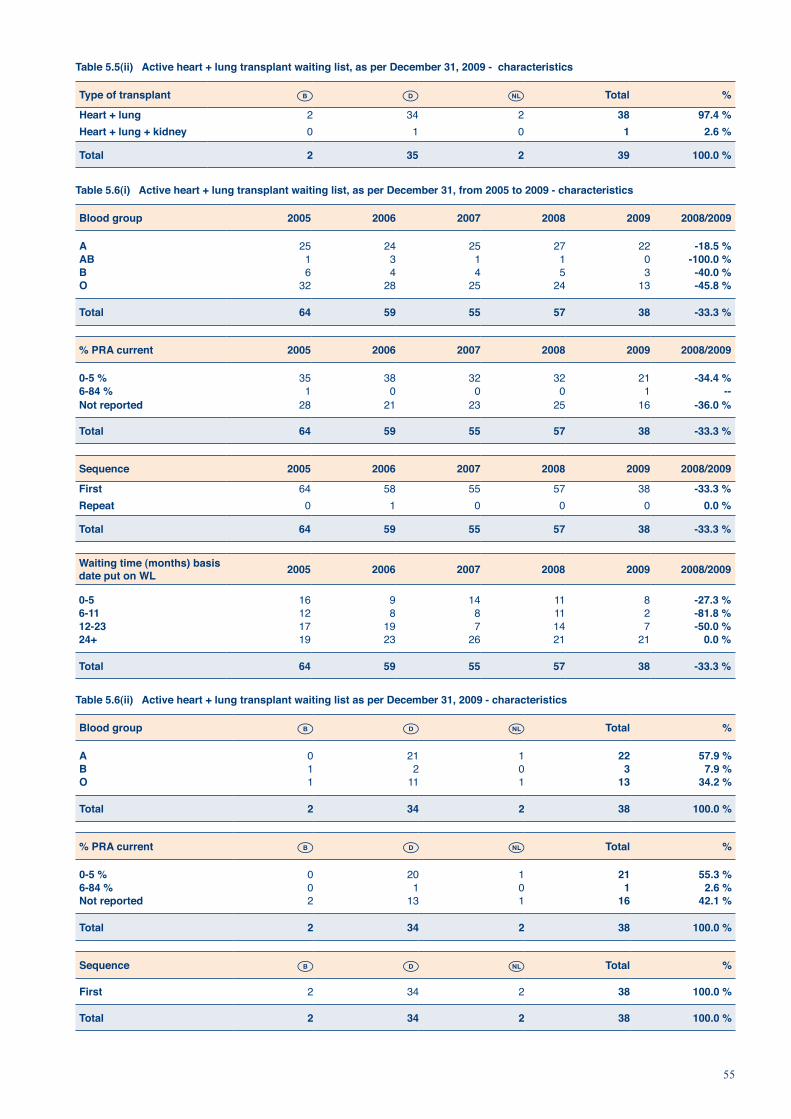
55
table 5.5(ii) active heart + lung transplant waiting list, as per December 31, 2009 - characteristics
type of transplant B D total %
heart + lung 2 34 2 38 97.4 %heart + lung + kidney 0 1 0 1 2.6 %
total 2 35 2 39 100.0 %
table 5.6(i) active heart + lung transplant waiting list, as per December 31, from 2005 to 2009 - characteristics
blood group 2005 2006 2007 2008 2009 2008/2009
a 25 24 25 27 22 -18.5 %ab 1 3 1 1 0 -100.0 %b 6 4 4 5 3 -40.0 %o 32 28 25 24 13 -45.8 %
total 64 59 55 57 38 -33.3 %
% pra current 2005 2006 2007 2008 2009 2008/2009
0-5 % 35 38 32 32 21 -34.4 %6-84 % 1 0 0 0 1 --not reported 28 21 23 25 16 -36.0 %
total 64 59 55 57 38 -33.3 %
sequence 2005 2006 2007 2008 2009 2008/2009
First 64 58 55 57 38 -33.3 %repeat 0 1 0 0 0 0.0 %
total 64 59 55 57 38 -33.3 %
Waiting time (months) basis date put on Wl 2005 2006 2007 2008 2009 2008/2009
0-5 16 9 14 11 8 -27.3 %6-11 12 8 8 11 2 -81.8 %12-23 17 19 7 14 7 -50.0 %24+ 19 23 26 21 21 0.0 %
total 64 59 55 57 38 -33.3 %
table 5.6(ii) active heart + lung transplant waiting list as per December 31, 2009 - characteristics
blood group B D total %
a 0 21 1 22 57.9 %b 1 2 0 3 7.9 %o 1 11 1 13 34.2 %
total 2 34 2 38 100.0 %
% pra current B D total %
0-5 % 0 20 1 21 55.3 %6-84 % 0 1 0 1 2.6 %not reported 2 13 1 16 42.1 %
total 2 34 2 38 100.0 %
sequence B D total %
First 2 34 2 38 100.0 %
total 2 34 2 38 100.0 %

56
table 5.6(ii) (continued)
Waiting time (months) basis date put on Wl B D total %
0-5 0 8 0 8 21.1 %6-11 1 1 0 2 5.3 %12-23 0 6 1 7 18.4 %24+ 1 19 1 21 55.3 %
total 2 34 2 38 100.0 %
Figure 5.3 lung waiting list, number of patients at year end, by urgency
0%
20%
40%
60%
80%
100%
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009
High Urgency
Urgent
Transplantable
Not Transplantable
Figure 5.4 lung waiting list, percentage of patients at year end, by urgency
0%
20%
40%
60%
80%
100%
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009
High Urgency
Urgent
Transplantable
Not Transplantable

57
Table 5.7(i) Active lung transplant waiting list as per December 31, from 2005 to 2009 - characteristics
Type of transplant 2005 2006 2007 2008 2009 2008/2009
Lung 668 758 849 846 964 13.9 %Lung + kidney 3 2 3 5 2 -60.0 %Lung + liver 3 5 4 8 6 -25.0 %Lung + heart 64 59 55 57 38 -33.3 %Lung + heart + kidney 0 0 0 0 1 --
Total 738 824 911 916 1011 10.4 %
Table 5.7(ii) Active lung transplant waiting list as per December 31, 2009 - characteristics
Type of transplant a B D Total %
Lung 72 92 617 183 964 95.4 %Lung + kidney 0 0 2 0 2 0.2 %Lung + liver 1 1 3 1 6 0.6 %Lung + heart 0 2 34 2 38 3.8 %Lung + heart + kidney 0 0 1 0 1 0.1 %
Total 73 95 657 186 1011 100.0 %
table 5.8(i) active lung-only transplant waiting list, as per December 31, from 2005 to 2009 - characteristics
blood group 2005 2006 2007 2008 2009 2008/2009
a 247 281 322 333 391 17.4 %ab 16 25 21 10 21 110.0 %b 74 78 84 76 74 -2.6 %o 331 374 422 427 478 11.9 %
total 668 758 849 846 964 13.9 %
% pra current 2005 2006 2007 2008 2009 2008/2009
0-5 % 321 411 475 486 568 16.9 %6-84 % 5 4 9 10 12 20.0 %85-100 % 1 0 0 0 1 --not reported 341 343 365 350 383 9.4 %
total 668 758 849 846 964 13.9 %
sequence 2005 2006 2007 2008 2009 2008/2009
First 644 731 822 821 936 14.0 %repeat 24 27 27 25 28 12.0 %
total 668 758 849 846 964 13.9 %
Waiting time (months) basis date put on wl 2005 2006 2007 2008 2009 2008/2009
0-5 252 264 289 265 319 20.4 %6-11 140 157 171 179 183 2.2 %12-23 146 164 181 203 222 9.4 %24+ 130 173 208 199 240 20.6 %
total 668 758 849 846 964 13.9 %
table 5.8(ii) active lung-only transplant waiting list, as per December 31, 2009 - characteristics
blood group a B D total %
a 25 38 255 73 391 40.6 %ab 4 2 12 3 21 2.2 %b 4 7 55 8 74 7.7 %o 39 45 295 99 478 49.6 %
total 72 92 617 183 964 100.0 %

58
table 5.8(ii) (continued)
% pra current a B D total %
0-5 % 9 9 388 162 568 58.9 %6-84 % 0 0 10 2 12 1.2 %85-100 % 0 0 1 0 1 0.1 %not reported 63 83 218 19 383 39.7 %
total 72 92 617 183 964 100.0 %
sequence a B D total %
First 70 91 593 182 936 97.1 %repeat 2 1 24 1 28 2.9 %
total 72 92 617 183 964 100.0 %
Waiting time (months) basis date put on wl a B D total %
0-5 40 45 186 48 319 33.1 %6-11 18 28 97 40 183 19.0 %12-23 12 17 143 50 222 23.0 %24+ 2 2 191 45 240 24.9 %
total 72 92 617 183 964 100.0 %
Figure 5.5 number of deceased donor heart transplants, by recipient urgency at transplant
0
100
200
300
400
500
600
700
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009
High Urgency
Urgent
Transplantable

59
Figure 5.6 percentage of deceased donor heart transplants, by recipient urgency at transplant
0%
20%
40%
60%
80%
100%
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009
High Urgency
Urgent
Transplantable
table 5.9(i) heart transplants from 2005 to 2009 - characteristics
Deceased donor heart transplants
type of transplant 2005 2006 2007 2008 2009 2008/2009
heart 531 539 562 544 553 1.7 %heart + kidney 10 15 13 10 8 -20.0 %heart + whole liver 1 1 2 3 0 -100.0 %heart + both lungs 21 30 21 23 20 -13.0 %heart + both lungs + kidney 0 0 0 1 0 -100.0 %heart + both lungs + whole liver 0 2 0 0 0 --
total 563 587 598 581 581 0.0 %
heart-only transplants
blood group 2005 2006 2007 2008 2009 2008/2009
a 254 231 271 219 238 8.7 %ab 35 41 39 37 38 2.7 %b 71 85 68 81 83 2.5 %o 171 182 184 207 194 -6.3 %
total 531 539 562 544 553 1.7 %
Waiting time (months) 2005 2006 2007 2008 2009 2008/2009
0-5 324 306 325 314 304 -3.2 %6-11 94 104 107 105 102 -2.9 %12-23 74 93 82 78 83 6.4 %24-59 39 35 45 46 56 21.7 %60+ 0 1 3 1 8 700.0 %
total 531 539 562 544 553 1.7 %
sequence 2005 2006 2007 2008 2009 2008/2009
First 520 529 549 535 542 1.3 %repeat 11 10 13 9 11 22.2 %
total 531 539 562 544 553 1.7 %

60
table 5.9(ii) heart transplants 2009 - characteristics
Deceased donor heart transplants
type of transplant a B D non-et total %
heart 72 65 20 341 34 18 3 553 95.2 %heart + kidney 0 2 0 6 0 0 0 8 1.4 %heart + both lungs 1 1 0 16 2 0 0 20 3.4 %
total 73 68 20 363 36 18 3 581 100.0 %
heart-only transplants
blood group a B D non-et total %
a 38 24 7 145 13 10 1 238 43.0 %ab 6 5 3 22 1 1 0 38 6.9 %b 10 11 4 49 6 2 1 83 15.0 %o 18 25 6 125 14 5 1 194 35.1 %
total 72 65 20 341 34 18 3 553 100.0 %
Waiting time (months) a B D non-et total %
0-5 41 35 11 182 18 14 3 304 55.0 %6-11 15 20 5 57 4 1 0 102 18.4 %12-23 12 8 4 51 7 1 0 83 15.0 %24-59 2 2 0 45 5 2 0 56 10.1 %60+ 2 0 0 6 0 0 0 8 1.4 %
total 72 65 20 341 34 18 3 553 100.0 %
sequence a b hr D nl slo non-et total %
First 72 63 20 333 33 18 3 542 98.0 %repeat 0 2 0 8 1 0 0 11 2.0 %
total 72 65 20 341 34 18 3 553 100.0 %
table 5.10(i) heart + lung transplants from 2005 to 2009 - characteristics
Deceased donor heart + lung transplants
type of transplant 2005 2006 2007 2008 2009 2008/2009
heart + both lungs 21 30 21 23 20 -13.0 %
total 21 30 21 23 20 -13.0 %
heart + lung transplants
blood group 2005 2006 2007 2008 2009 2008/2009
a 15 11 10 10 7 -30.0 %ab 1 2 1 4 1 -75.0 %b 0 2 3 1 2 100.0 %o 5 15 7 8 10 25.0 %
total 21 30 21 23 20 -13.0 %
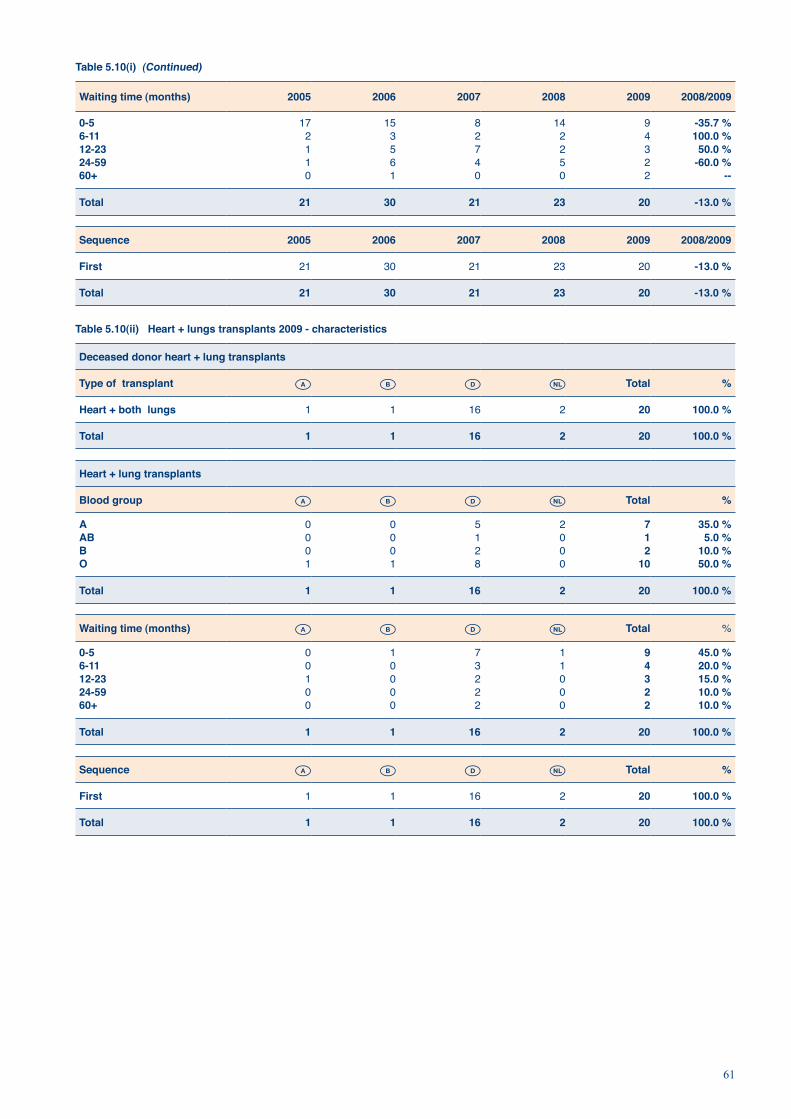
61
table 5.10(i) (continued)
Waiting time (months) 2005 2006 2007 2008 2009 2008/2009
0-5 17 15 8 14 9 -35.7 %6-11 2 3 2 2 4 100.0 %12-23 1 5 7 2 3 50.0 %24-59 1 6 4 5 2 -60.0 %60+ 0 1 0 0 2 --
total 21 30 21 23 20 -13.0 %
sequence 2005 2006 2007 2008 2009 2008/2009
First 21 30 21 23 20 -13.0 %
total 21 30 21 23 20 -13.0 %
table 5.10(ii) heart + lungs transplants 2009 - characteristics
Deceased donor heart + lung transplants
type of transplant a B D total %
heart + both lungs 1 1 16 2 20 100.0 %
total 1 1 16 2 20 100.0 %
heart + lung transplants
blood group a B D total %
a 0 0 5 2 7 35.0 %ab 0 0 1 0 1 5.0 %b 0 0 2 0 2 10.0 %o 1 1 8 0 10 50.0 %
total 1 1 16 2 20 100.0 %
Waiting time (months) a B D total %
0-5 0 1 7 1 9 45.0 %6-11 0 0 3 1 4 20.0 %12-23 1 0 2 0 3 15.0 %24-59 0 0 2 0 2 10.0 %60+ 0 0 2 0 2 10.0 %
total 1 1 16 2 20 100.0 %
sequence a B D total %
First 1 1 16 2 20 100.0 %
total 1 1 16 2 20 100.0 %

62
Figure 5.7 number of deceased donor lung transplants, by recipient urgency at transplant
0
100
200
300
400
500
600
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009
High Urgency
Urgent
Transplantable
Figure 5.8 percentage of deceased donor lung transplants, by recipient urgency at transplant
0%
20%
40%
60%
80%
100%
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009
High Urgency
Urgent
Transplantable
table 5.11(i) lung transplants from 2005 to 2009 - characteristics
Deceased donor lung transplants
type of transplant 2005 2006 2007 2008 2009 2008/2009
single lung 103 120 89 82 79 -3.7 %both lungs 345 338 410 419 435 3.8 %single lung + kidney 0 0 1 0 0 --single lung + whole liver 0 1 0 0 0 --both lungs + heart 21 30 21 23 20 -13.0 %both lungs + kidney 1 3 0 1 2 100.0 %both lungs + whole liver 1 2 4 1 3 200.0 %both lungs + heart + kidney 0 0 0 1 0 -100.0 %both lungs + heart + whole liver 0 2 0 0 0 --
total 471 496 525 527 539 2.3 %

63
table 5.11(i) (continued)
lung-only transplants (including single and both lungs)
blood group 2005 2006 2007 2008 2009 2008/2009
a 192 206 229 219 220 0.5 %ab 33 28 36 24 30 25.0 %b 62 61 59 61 62 1.6 %o 161 163 175 197 202 2.5 %
total 448 458 499 501 514 2.6 %
Waiting time (months) 2005 2006 2007 2008 2009 2008/2009
0-5 236 225 235 240 238 -0.8 %6-11 95 102 112 107 112 4.7 %12-23 68 79 89 89 89 0.0 %24-59 48 46 58 53 71 34.0 %60+ 1 6 5 12 4 -66.7 %
total 448 458 499 501 514 2.6 %
sequence 2005 2006 2007 2008 2009 2008/2009
First 430 436 459 474 483 1.9 %repeat 18 22 40 27 31 14.8 %
total 448 458 499 501 514 2.6 %
table 5.11(ii) lung transplants 2009 - characteristics
Deceased donor lung transplants
type of transplant a B D non-et total %
single lung 98 78 213 45 1 435 80.7 %both lungs 9 11 39 20 0 79 14.7 %both lungs + heart 1 1 16 2 0 20 3.7 %both lungs + kidney 0 0 2 0 0 2 0.4 %both lungs + whole liver 1 0 2 0 0 3 0.6 %
total 109 90 272 67 1 539 100.0 %
lung-only transplants (including single and both lungs)
blood group a B D non-et total %
a 45 30 115 30 0 220 42.8 %ab 5 1 19 5 0 30 5.8 %b 13 10 30 9 0 62 12.1 %o 44 48 88 21 1 202 39.3 %
total 107 89 252 65 1 514 100.0 %
Waiting time (months) a B D non-et total %
0-5 71 40 114 12 1 238 46.3 %6-11 21 37 45 9 0 112 21.8 %12-23 10 9 48 22 0 89 17.3 %24-59 5 3 44 19 0 71 13.8 %60+ 0 0 1 3 0 4 0.8 %
total 107 89 252 65 1 514 100.0 %

64
table 5.11(ii) (continued)
sequence a B D non-et total %
First 98 85 236 63 1 483 94.0 %repeat 9 4 16 2 0 31 6.0 %
total 107 89 252 65 1 514 100.0 %
Figure 5.9 Dynamics of the eurotransplant heart waiting list and transplants between 1991 and 2009
1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009Active waiting list 499 552 672 723 709 744 744 721 609 489 424 423 568 728 882 920 959 1007 1154Heart transplants 806 753 773 696 732 759 782 759 708 623 596 580 570 553 542 555 577 557 561
0
200
400
600
800
1000
1200
1400
Figure 5.10 Dynamics of the eurotransplant heart + lung waiting list, heart + lung transplants, lung waiting list and lung transplants, between 1991 and 2009
1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009Lung waiting list 90 141 203 227 224 204 216 224 350 377 430 462 517 592 674 765 856 859 972Heart+Lung waiting list 48 48 49 71 79 71 66 60 46 42 43 43 45 54 64 59 55 57 39Lung transplants 71 109 119 138 125 154 155 228 239 258 272 358 382 418 450 464 504 503 519Heart+Lung transplants 24 32 28 43 42 34 43 20 28 20 21 24 23 18 21 32 21 24 20
0
200
400
600
800
1000
1200

65
6. liver and intestine: donation, waiting lists and tranplants
table 6.1(i) Deceased donors / livers in eurotransplant from 2005 to 2009
Donors
year of registration 2005 2006 2007 2008 2009 2008/2009
all donors 2249 2299 2411 2233 2305 3.2 %non-liver donors 494 423 422 361 321 -11.1 %liver donors 1755 1876 1989 1872 1984 6.0 %liver donors not used 453 481 420 322 353 9.6 %One split used 3 2 3 5 2 -60.0 %Both splits used 59 45 53 56 60 7.1 %Whole liver used 1240 1348 1513 1489 1569 5.4 %
total liver donors used 1302 1395 1569 1550 1631 5.2 %
Donor procedures
year of registration 2005 2006 2007 2008 2009 2008/2009Whole liver procedure 1686 1827 1932 1808 1919 6.1 %split liver procedure 68 49 57 64 65 1.6 %
total 1754 1876 1989 1872 1984 6.0 %
Whole livers
year of registration 2005 2006 2007 2008 2009 2008/2009
reported 1686 1827 1932 1808 1919 6.1 %offered 1670 1793 1901 1799 1913 6.3 %accepted 1543 1682 1835 1739 1861 7.0 %transplanted 1240 1348 1513 1489 1569 5.4 %
split livers
year of registration 2005 2006 2007 2008 2009 2008/2009
available split livers 136 98 114 128 130 1.6 %split liver not used 15 6 5 11 8 -27.3 %split liver transplanted 121 92 109 117 122 4.3 %
table 6.1(ii) Deceased donors / livers in eurotransplant in 2009
Donors
Donor country a B D total et non-et total % all donors
all donors 225 302 80 1248 255 36 2146 159 2305 100.0 %non-liver donors 28 26 5 62 70 0 191 130 321 13.9 %liver donors 197 276 75 1186 185 36 1955 29 1984 86.1 %liver donors not used 38 46 13 182 42 14 335 18 353 15.3 %One split used 0 0 0 1 0 0 1 1 2 0.1 %Both splits used 4 10 2 35 8 1 60 0 60 2.6 %Whole liver used 155 220 60 968 135 21 1559 10 1569 68.1 %total liver donors used 159 230 62 1004 143 22 1620 11 1631 70.8 %
Donor procedures
Donor country a B D total et non-et total %
Whole liver procedure 193 265 73 1149 177 34 1891 28 1919 96.7 %split liver procedure 4 11 2 37 8 2 64 1 65 3.3 %
total 197 276 75 1186 185 36 1955 29 1984 100.0 %

66
table 6.1(ii) (continued)
Whole livers
Donor country a B D total et non-et total % reported
reported 193 265 73 1149 177 34 1891 28 1919 100.0 %offered 192 264 72 1148 176 34 1886 27 1913 99.7 %accepted 190 256 72 1126 164 33 1841 20 1861 97.0 %
transplanted 155 220 60 968 135 21 1559 10 1569 81.8 %
split livers
Donor country a B D total et non-et total %
available split livers 8 22 4 74 16 4 128 2 130 100.0 %split liver not used 0 2 0 3 0 2 7 1 8 6.2 %split liver transplanted 8 20 4 71 16 2 121 1 122 93.8 %
Figure 6.1 liver waiting list, number of patients at year end, by urgency
0
500
1000
1500
2000
2500
3000
3500
2000
2001
2002
2003
2004
2005
01.1
2.20
06
31.1
2.20
06
2007
2008
2009
High Urgency
----
Pre-Meld T2
Pre-Meld T3
Pre-Meld T4
----
Meld 30+
Meld 25-29
Meld 19-24
Meld 11-18
Meld 06-10
Not Transplantable
<---- Pre-MELD | MELD ---->
Figure 6.2 liver waiting list, percentage of patients at year end, by urgency
0%
20%
40%
60%
80%
100%
2000
2001
2002
2003
2004
2005
01.1
2.20
06
31.1
2.20
06
2007
2008
2009
High Urgency
----
Pre-Meld T2
Pre-Meld T3
Pre-Meld T4
----
Meld 30+
Meld 25-29
Meld 19-24
Meld 11-18
Meld 06-10
Not Transplantable
<---- Pre-MELD | MELD ---->

67
table 6.2(i) active liver transplant waiting list, as per December 31, from 2005 to 2009 - characteristics
type of transplant 2005 2006 2007 2008 2009 2008/2009
liver 2066 2249 2351 2354 2525 7.3 %liver + heart 0 1 2 2 4 100.0 %liver + kidney 60 62 67 72 97 34.7 %liver + lung 3 5 4 8 6 -25.0 %liver + pancreas 4 1 5 4 8 100.0 %liver + kidney + pancreas 1 1 0 2 1 -50.0 %
total 2134 2319 2429 2442 2641 8.1 %
table 6.2(ii) active liver transplant waiting list, as per December 31, 2009 - characteristics
type of transplant a B D total %
liver 102 166 54 2083 105 15 2525 95.6 %liver + heart 1 0 0 3 0 0 4 0.2 %liver + kidney 2 24 2 66 3 0 97 3.7 %liver + lung 1 1 0 3 1 0 6 0.2 %liver + pancreas 0 0 0 7 1 0 8 0.3 %liver + kidney + pancreas 0 0 0 1 0 0 1 0.0 %
total 106 191 56 2163 110 15 2641 100.0 %
table 6.3(i) active liver-only transplant waiting list as per December 31, from 2005 to 2009 - characteristics
blood group 2005 2006 2007 2008 2009 2008/2009
a 863 909 988 944 1075 13.9 %ab 53 59 40 46 54 17.4 %b 273 282 275 267 280 4.9 %o 877 999 1048 1097 1116 1.7 %
total 2066 2249 2351 2354 2525 7.3 %
% pra current 2005 2006 2007 2008 2009 2008/2009
0-5 % 561 594 613 620 580 -6.5 %6-84 % 26 34 43 42 43 2.4 %85-100 % 3 0 0 2 3 50.0 %not reported 1476 1621 1695 1690 1899 12.4 %
total 2066 2249 2351 2354 2525 7.3 %
sequence 2005 2006 2007 2008 2009 2008/2009
First 1955 2120 2234 2233 2392 7.1 %repeat 111 129 117 121 133 9.9 %
total 2066 2249 2351 2354 2525 7.3 %
Waiting time (months) basis date put on Wl 2005 2006 2007 2008 2009 2008/2009
0-5 711 783 690 665 733 10.2 %6-11 382 416 398 363 433 19.3 %12-23 542 458 551 462 389 -15.8 %24+ 431 592 712 864 970 12.3 %
total 2066 2249 2351 2354 2525 7.3 %

68
table 6.3(ii) active liver-only transplant waiting list as per December 31, 2009 - characteristics
blood group a B D total %
a 29 62 28 916 36 4 1075 42.6 %ab 10 2 1 40 1 54 2.1 %b 23 10 8 233 6 280 11.1 %o 40 92 17 894 63 10 1116 44.2 %
total 102 166 54 2083 105 15 2525 100.0 %
% pra current a B D total %
0-5 % 15 12 33 457 63 0 580 23.0 %6-84 % 1 2 7 28 5 0 43 1.7 %85-100 % 0 0 0 3 0 0 3 0.1 %not reported 86 152 14 1595 37 15 1899 75.2 %
total 102 166 54 2083 105 15 2525 100.0 %
sequence a B D total %
First 92 153 54 1982 97 14 2392 94.7 %repeat 10 13 0 101 8 1 133 5.3 %
total 102 166 54 2083 105 15 2525 100.0 %
Waiting time (months) basis date put on Wl a B D
total %
0-5 54 69 16 550 39 5 733 29.0 %6-11 27 27 6 347 20 6 433 17.1 %12-23 11 25 14 321 14 4 389 15.4 %24+ 10 45 18 865 32 0 970 38.4 %
total 102 166 54 2083 105 15 2525 100.0 %
Figure 6.3 number of deceased donor liver transplants, by recipient urgency at transplant
0
200
400
600
800
1000
1200
1400
1600
1800
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009
High Urgency
----
Pre-Meld T2
Pre-Meld T3
Pre-Meld T4
Transplantable
----
Meld 30+
Meld 25-29
Meld 19-24
Meld 11-18
Meld 06-10
<---- Pre-MELD | MELD ---->

69
Figure 6.4 percentage of deceased donor liver transplants, by recipient urgency at transplant
0%
20%
40%
60%
80%
100%
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009
High Urgency
----
Pre-Meld T2
Pre-Meld T3
Pre-Meld T4
Transplantable
----
Meld 30+
Meld 25-29
Meld 19-24
Meld 11-18
Meld 06-10
<---- Pre-MELD | MELD ---->
table 6.4(i) liver transplants from 2005 to 2009 - characteristics
Deceased donor liver transplants
type of transplant 2005 2006 2007 2008 2009 2008/2009
split liver 119 90 105 113 121 7.1 %Whole liver 1196 1273 1439 1405 1515 7.8 %split liver + kidney 2 2 4 4 1 -75.0 %Whole liver + kidney 41 61 64 73 45 -38.4 %Whole liver + kidney en bloc 1 1 1 2 0 -100.0 %Whole liver + pancreas 2 2 5 5 4 -20.0 %Whole liver + heart 1 1 2 3 0 -100.0 %Whole liver + lung 0 1 0 0 0 0.0 %Whole liver + both lungs 1 2 4 1 3 200.0 %Whole liver + kidney + pancreas 1 1 1 0 2 0.0 %Whole liver + heart + both lungs 0 2 0 0 0 0.0 %
total 1364 1436 1625 1606 1691 5.3 %
liver-only transplants (whole and split)
blood group 2005 2006 2007 2008 2009 2008/2009
a 579 603 656 655 654 -0.2 %ab 114 90 131 103 125 21.4 %b 170 208 219 192 233 21.4 %o 452 462 538 568 624 9.9 %
total 1315 1363 1544 1518 1636 7.8 %
Waiting time (months) 2005 2006 2007 2008 2009 2008/2009
0-5 759 801 1057 999 1098 9.9 %6-11 212 221 194 238 289 21.4 %12-23 228 198 185 160 136 -15.0 %24-59 114 138 98 107 84 -21.5 %60+ 2 5 10 14 29 107.1 %
total 1315 1363 1544 1518 1636 7.8 %

70
table 6.4(i) (continued)
sequence 2005 2006 2007 2008 2009 2008/2009
First 1127 1191 1351 1336 1431 7.1 %repeat 188 172 193 182 205 12.6 %
total 1315 1363 1544 1518 1636 7.8 %
table 6.4(ii) liver transplants 2009 - characteristics
Deceased donor liver transplants
type of transplant a B D total %
split liver 0 12 1 99 9 0 121 7.2 %Whole liver 140 203 58 979 117 18 1515 89.6 %split liver + kidney 0 0 0 1 0 0 1 0.1 %Whole liver + kidney 5 4 1 32 3 0 45 2.7 %Whole liver + pancreas 0 0 0 4 0 0 4 0.2 %Whole liver + both lungs 1 0 0 2 0 0 3 0.2 %Whole liver + kidney + pancreas 0 1 0 1 0 0 2 0.1 %
total 146 220 60 1118 129 18 1691 100.0 %
liver-only transplants (whole and split)
blood group a B D total %
a 68 78 20 442 38 8 654 40.0 %ab 11 11 12 77 13 1 125 7.6 %b 13 23 9 169 15 4 233 14.2 %o 48 103 18 390 60 5 624 38.1 %
total 140 215 59 1078 126 18 1636 100.0 %
Waiting time (months) a B D total %
0-5 82 150 47 728 76 15 1098 67.1 %6-11 34 43 8 176 27 1 289 17.7 %12-23 17 15 4 85 13 2 136 8.3 %24-59 6 7 0 63 8 0 84 5.1 %60+ 1 0 0 26 2 0 29 1.8 %
total 140 215 59 1078 126 18 1636 100.0 %
sequence a B D total %
First 126 197 54 930 107 17 1431 87.5 %repeat 14 18 5 148 19 1 205 12.5 %
total 140 215 59 1078 126 18 1636 100.0 %
table 6.5(i) living donor liver transplants - liver-only - from 2005 to 2009
liver-only 2005 2006 2007 2008 2009 2008/2009
Domino 15 10 10 7 3 -57.1 %non-related 15 20 13 9 12 33.3 %related 91 86 78 66 83 25.8 %
total 121 116 101 82 98 19.5 %

71
table 6.5(i) (continued)
related 2005 2006 2007 2008 2009 2008/2009
brother / sister 14 11 10 6 9 50.0 %Father 23 21 18 21 29 38.1 %mother 19 19 27 24 25 4.2 %son / daughter 30 28 15 10 11 10.0 %grandfather / -mother 2 2 1 0 4 --nephew / niece 2 2 4 2 1 -50.0 %uncle / aunt 0 2 1 3 4 33.3 %blood related : nos* 1 1 2 0 0 0.0 %
total 91 86 78 66 83 25.8 %
non-related 2005 2006 2007 2008 2009 2008/2009
Friend 0 0 1 1 1 0.0 %spouse / partner 11 11 9 4 7 75.0 %not blood related family 2 3 3 3 3 0.0 %not blood related : nos* 2 6 0 1 1 0.0 %
total 15 20 13 9 12 33.3 %
*NOS Not otherwise specified
table 6.5(ii) living donor liver transplants - liver-only - 2009
liver-only a B D total %
related 7 21 2 52 1 83 84.7 %non-related 0 2 0 8 2 12 12.2 %Domino 0 2 0 1 0 3 3.1 %
total 7 25 2 61 3 98 100.0 %
related a B D total %
brother / sister 0 1 0 8 0 9 10.8 %Father 2 8 0 18 1 29 34.9 %mother 4 7 1 13 0 25 30.1 %son / daughter 0 4 0 7 0 11 13.3 %uncle / aunt 1 0 1 2 0 4 4.8 %nephew / niece 0 0 0 1 0 1 1.2 %grandfather / -mother 0 1 0 3 0 4 4.8 %
total 7 21 2 52 1 83 100.0 %
non-related a B D total %
Friend 0 0 0 0 1 1 8.3 %spouse / partner 0 1 0 6 0 7 58.3 %not blood related family 0 1 0 2 0 3 25.0 %not blood related : nos* 0 0 0 0 1 1 8.3 %
total 0 2 0 8 2 12 100.0 %
*NOS Not otherwise specified

72
Figure 6.5 Dynamics of the eurotransplant liver waiting list and liver transplants between 1991 and 2009
*including domino transplants1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009
Liver waiting list 229 253 203 212 263 327 374 492 593 803 1093 1366 1714 2035 2134 2319 2429 2442 2641Deceased donor transplants 710 765 878 892 944 1032 1097 1071 1132 1168 1112 1136 1264 1262 1364 1436 1625 1606 1691Living donor transplants* 5 15 14 24 25 22 41 38 64 116 124 129 133 106 121 116 101 82 98
0
500
1000
1500
2000
2500
3000

73
intestine transplants 2009
On January 1, 2009, 21 recipients were on the waiting list for an intestinal transplant (13 in Germany, 5 in Belgium, 1 in Austria, 2 in the Netherlands). During the year 2009, 35 recipients were registered for either an intestinal transplant (N=14) or for a combined intestinal transplant (N=21).As per December 31, 2009, 33* recipients were awaiting either an isolated intestinal transplant (N=20) or in combination with another organ (N=13).
table 6.6 number of intestinal transplants in 2009
country center total
Austria AIBTP - Innsbruck 1
Belgium BLGTP - Liege 9
Germany
GBCTP - Berlin 2
GFMTP- Frankfurt 2
GKITP - Kiel 1
GMNTP - Münster 1
GTUTP - Tübingen 3
Netherlands NGRTP - Groningen 1
Total 12
Six transplants concerned isolated intestine transplants and six concerned combined intestine transplants. In 2008, nine isolated intestine transplants were performed and eight combined intestine transplants.
Nine patients deceased while awaiting a transplant (one recipient deceased in 2008, this was registered in 2009). Two patients were removed from the waiting list.
* Urgency status of patients on the waiting list as per December 31, 2009:Intestine-only: 17 patients registered T, 3 patients registered NT Combined: 10 patients registered T, 3 patients registered NT

74
7. pancreas and islets: donation, waiting lists and transplants
table 7.1(i) Deceased donors / pancreas in eurotransplant from 2005 to 2009
Donors
year of registration 2005 2006 2007 2008 2009 2008/2009
all donors 2249 2299 2411 2233 2305 3.2 %non-pancreas donors 1314 1311 1373 1312 1429 8.9 %pancreas donors 935 988 1038 921 876 -4.9 %pancreas donors not used 630 743 783 664 650 -2.1 %Pancreatic islet donors used 63 16 40 38 35 -7.9 %Whole pancreas donors used 242 229 215 219 191 -12.8 %total pancreas donors used 305 245 255 257 226 -12.1 %
pancreas
year of registration 2005 2006 2007 2008 2009 2008/2009
reported 933 987 1038 921 876 -4.9 %offered 889 951 981 880 835 -5.1 %accepted 600 571 548 551 501 -9.1 %transplanted 305 245 255 257 226 -12.1 %
table 7.1(ii) Deceased donors / pancreas in eurotransplant in 2009
Donors
Donor country a B D total et non-et total % all donors
all donors 225 302 80 1248 255 36 2146 159 2305 100.0 %non-pancreas donors 155 123 51 830 95 20 1274 155 1429 62.0 %pancreas donors 70 179 29 418 160 16 872 4 876 38.0 %pancreas donors not used 36 143 16 299 139 13 646 4 650 28.2 %Pancreatic islet donors used 1 16 0 11 7 0 35 0 35 1.5 %Whole pancreas donors used 33 20 13 108 14 3 191 0 191 8.3 %total pancreas donors used 34 36 13 119 21 3 226 0 226 9.8 %
pancreas
Donor country a B D total et non-et total % reported
reported 70 179 29 418 160 16 872 4 876 100.0 %offered 68 173 29 391 154 16 831 4 835 95.3 %accepted 52 99 18 241 85 6 501 0 501 57.2 %transplanted 34 36 13 119 21 3 226 0 226 25.8 %

75
Figure 7.1 pancreas waiting list, number of patients at year end, by urgency
0
100
200
300
400
500
600
700
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009
Special Urgency
Transplantable
Not Transplantable
Figure 7.2 pancreas waiting list, percentage of patients at year end, by urgency
0%
20%
40%
60%
80%
100%
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009
Special Urgency
Transplantable
Not Transplantable
table 7.2(i) active pancreas transplant waiting list as per December 31, from 2005 to 2009 - characteristics
type of transplant 2005 2006 2007 2008 2009 2008/2009
pancreas 59 48 43 55 68 23.6 %pancreas + liver 4 1 5 4 8 100.0 %pancreas + kidney 217 242 304 300 349 16.3 %pancreas + liver + kidney 1 1 0 2 1 -50.0 %
total 281 292 352 361 426 18.0 %

76
table 7.2(ii) active pancreas transplant waiting list as per December 31, 2009 - characteristics
type of transplant a B D total %
pancreas 12 16 0 30 10 68 16.0 %pancreas + liver 0 0 0 7 1 8 1.9 %pancreas + kidney 20 30 1 276 22 349 81.9 %pancreas + liver + kidney 0 0 0 1 0 1 0.2 %
total 32 46 1 314 33 426 100.0 %
table 7.3a(i) active pancreas-only transplant waiting list as per December 31, from 2005 to 2009 - characteristics
blood group 2005 2006 2007 2008 2009 2008/2009
a 27 19 24 23 27 17.4 %ab 2 2 2 4 3 -25.0 %b 8 8 3 7 9 28.6 %o 22 19 14 21 29 38.1 %
total 59 48 43 55 68 23.6 %
% pra current 2005 2006 2007 2008 2009 2008/2009
0-5 % 49 44 39 48 55 14.6 %6-84 % 5 4 4 7 8 14.3 %85-100 % 0 0 0 0 1 --not reported 5 0 0 0 4 --
total 59 48 43 55 68 23.6 %
sequence 2005 2006 2007 2008 2009 2008/2009
First 30 23 20 26 38 46.2 %repeat 29 25 23 29 30 3.4 %
total 59 48 43 55 68 23.6 %
Waiting time (months) basis date put on Wl
2005 2006 2007 2008 2009 2008/2009
0-5 16 7 8 13 13 0.0 %6-11 17 9 9 11 15 36.4 %12-23 13 20 7 5 17 240.0 %24+ 13 12 19 26 23 -11.5 %
total 59 48 43 55 68 23.6 %
table 7.3a(ii) active pancreas-only transplant waiting list as per December 31, 2009 - characteristics
blood group a B D total %
a 5 5 13 4 27 39.7 %ab 0 0 3 0 3 4.4 %b 1 2 4 2 9 13.2 %o 6 9 10 4 29 42.6 %
total 12 16 30 10 68 100.0 %
% pra current a B D total %
0-5 % 11 8 26 10 55 80.9 %6-84 % 1 3 4 0 8 11.8 %85-100 % 0 1 0 0 1 1.5 %not reported 0 4 0 0 4 5.9 %
total 12 16 30 10 68 100.0 %

77
table 7.3a(ii) (continued)
sequence a B D total %
First 5 13 14 6 38 55.9 %repeat 7 3 16 4 30 44.1 %
total 12 16 30 10 68 100.0 %
Waiting time (months) basis date put on Wl
a B D total %
0-5 2 6 4 1 13 19.1 %6-11 3 5 6 1 15 22.1 %12-23 2 1 9 5 17 25.0 %24+ 5 4 11 3 23 33.8 %
total 12 16 30 10 68 100.0 %
table 7.3b(i) active kidney + pancreas transplant waiting list as per December 31, from 2005 to 2009 - characteristics
blood group 2005 2006 2007 2008 2009 2008/2009
a 91 97 127 116 132 13.8 %ab 2 3 9 10 8 -20.0 %b 35 40 48 50 71 42.0 %o 89 102 120 124 138 11.3 %
total 217 242 304 300 349 16.3 %
% pra current 2005 2006 2007 2008 2009 2008/2009
0-5 % 197 224 276 263 318 20.9 %6-84 % 16 15 21 29 22 -24.1 %85-100 % 0 2 5 8 5 -37.5 %not reported 4 1 2 0 4 --
total 217 242 304 300 349 16.3 %
sequence 2005 2006 2007 2008 2009 2008/2009
First 200 232 276 273 324 18.7 %repeat 17 10 28 27 25 -7.4 %
total 217 242 304 300 349 16.3 %
Waiting time (months) basis date put on Wl
2005 2006 2007 2008 2009 2008/2009
0-5 85 76 90 72 78 8.3 %6-11 84 79 87 91 77 -15.4 %12-23 32 69 94 93 119 28.0 %24+ 16 16 33 44 75 70.5 %unknown 0 2 0 0 0 0.0 %
total 217 242 304 300 349 16.3 %
table 7.3b(ii) active kidney + pancreas transplant waiting list as per December 31, 2009 - characteristics
blood group a B D total %
a 4 17 0 104 7 132 37.8 %ab 0 1 0 6 1 8 2.3 %b 8 4 1 56 2 71 20.3 %o 8 8 0 110 12 138 39.5 %
total 20 30 1 276 22 349 100.0 %

78
table 7.3b(ii) (continued)
% pra current a B D total %
0-5 % 12 26 1 257 22 318 91.1 %6-84 % 7 3 0 12 0 22 6.3 %85-100 % 1 1 0 3 0 5 1.4 %not reported 0 0 0 4 0 4 1.1 %
total 20 30 1 276 22 349 100.0 %
sequence a B D total %
First 12 29 1 261 21 324 92.8 %repeat 8 1 0 15 1 25 7.2 %
total 20 30 1 276 22 349 100.0 %
Waiting time (months) basis date put on Wl
a B D total %
0-5 4 10 1 57 6 78 22.3 %6-11 6 5 0 58 8 77 22.1 %12-23 7 7 0 98 7 119 34.1 %24+ 3 8 0 63 1 75 21.5 %
total 20 30 1 276 22 349 100.0 %
Figure 7.3 number of deceased donor pancreas transplants, by recipient urgency at transplant
0
50
100
150
200
250
300
350
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009
Special Urgency
Special Urg. Islets
Islets
Transplantable
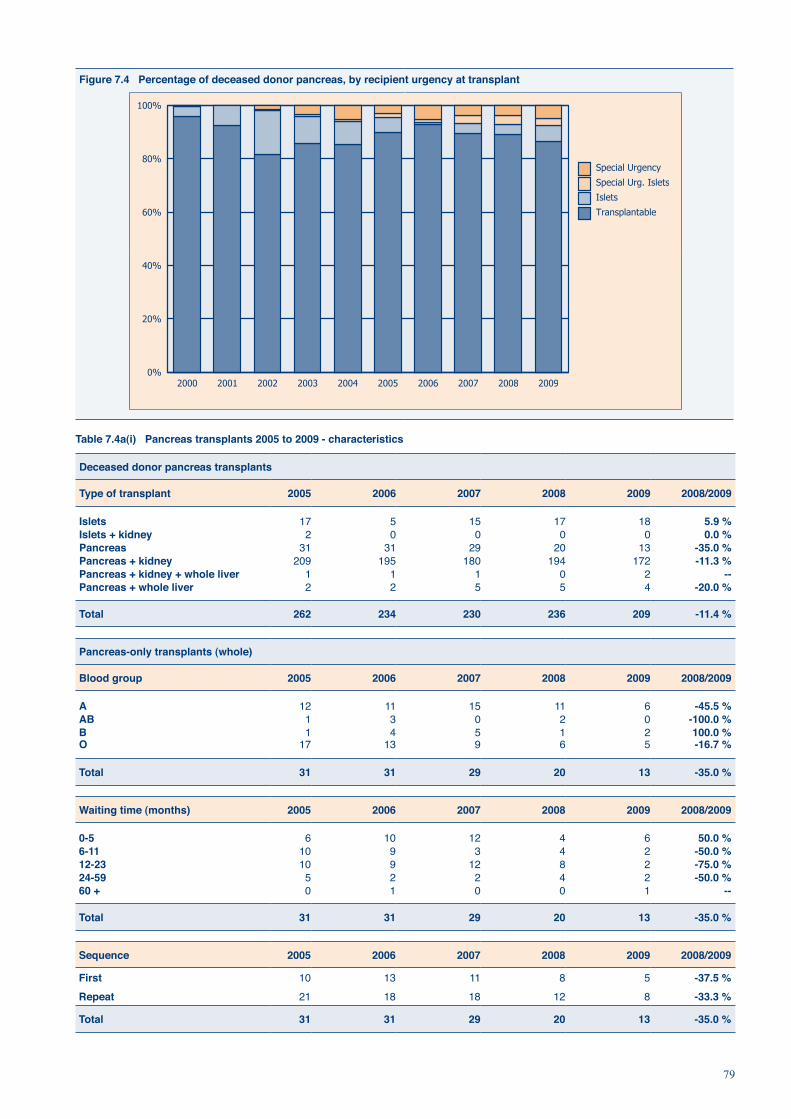
79
Figure 7.4 percentage of deceased donor pancreas, by recipient urgency at transplant
0%
20%
40%
60%
80%
100%
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009
Special Urgency
Special Urg. Islets
Islets
Transplantable
table 7.4a(i) pancreas transplants 2005 to 2009 - characteristics
Deceased donor pancreas transplants
type of transplant 2005 2006 2007 2008 2009 2008/2009
islets 17 5 15 17 18 5.9 %islets + kidney 2 0 0 0 0 0.0 %pancreas 31 31 29 20 13 -35.0 %pancreas + kidney 209 195 180 194 172 -11.3 %pancreas + kidney + whole liver 1 1 1 0 2 --pancreas + whole liver 2 2 5 5 4 -20.0 %
total 262 234 230 236 209 -11.4 %
pancreas-only transplants (whole)
blood group 2005 2006 2007 2008 2009 2008/2009
a 12 11 15 11 6 -45.5 %ab 1 3 0 2 0 -100.0 %b 1 4 5 1 2 100.0 %o 17 13 9 6 5 -16.7 %
total 31 31 29 20 13 -35.0 %
Waiting time (months) 2005 2006 2007 2008 2009 2008/2009
0-5 6 10 12 4 6 50.0 %6-11 10 9 3 4 2 -50.0 %12-23 10 9 12 8 2 -75.0 %24-59 5 2 2 4 2 -50.0 %60 + 0 1 0 0 1 --
total 31 31 29 20 13 -35.0 %
sequence 2005 2006 2007 2008 2009 2008/2009
First 10 13 11 8 5 -37.5 %repeat 21 18 18 12 8 -33.3 %
total 31 31 29 20 13 -35.0 %
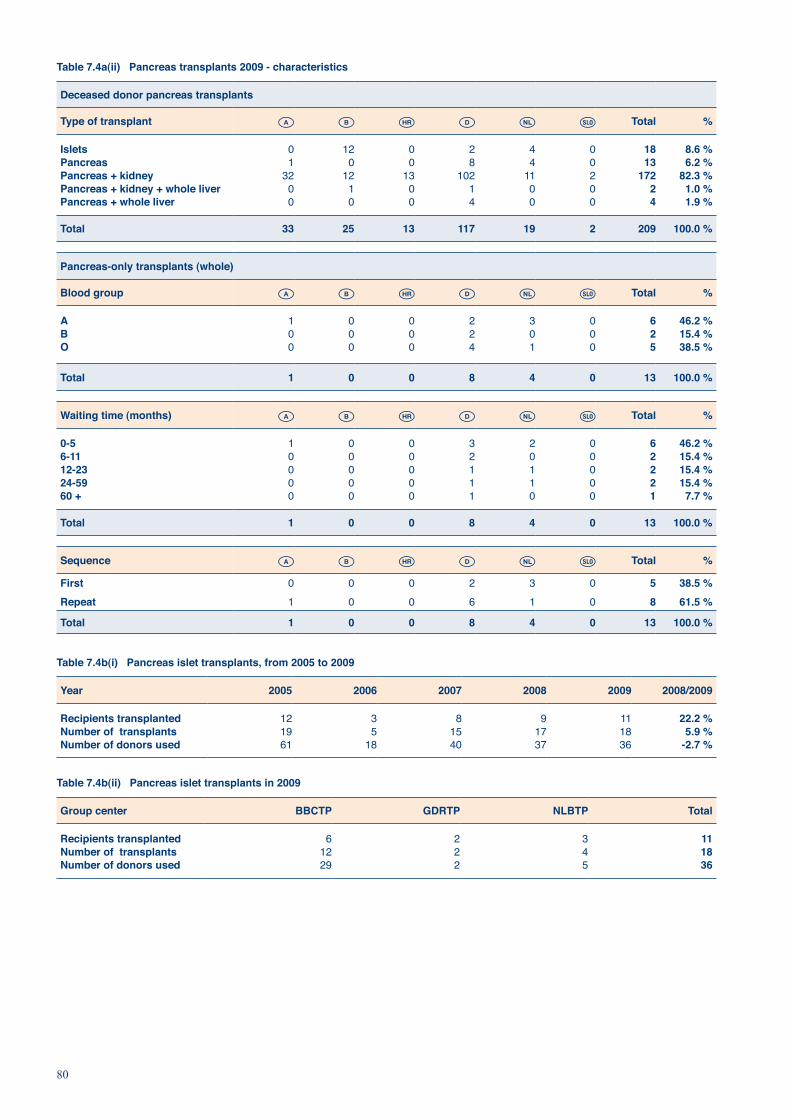
80
table 7.4a(ii) pancreas transplants 2009 - characteristics
Deceased donor pancreas transplants
type of transplant a B D total %
islets 0 12 0 2 4 0 18 8.6 %pancreas 1 0 0 8 4 0 13 6.2 %pancreas + kidney 32 12 13 102 11 2 172 82.3 %pancreas + kidney + whole liver 0 1 0 1 0 0 2 1.0 %pancreas + whole liver 0 0 0 4 0 0 4 1.9 %
total 33 25 13 117 19 2 209 100.0 %
pancreas-only transplants (whole)
blood group a B D total %
a 1 0 0 2 3 0 6 46.2 %b 0 0 0 2 0 0 2 15.4 %o 0 0 0 4 1 0 5 38.5 %
total 1 0 0 8 4 0 13 100.0 %
Waiting time (months) a B D total %
0-5 1 0 0 3 2 0 6 46.2 %6-11 0 0 0 2 0 0 2 15.4 %12-23 0 0 0 1 1 0 2 15.4 %24-59 0 0 0 1 1 0 2 15.4 %60 + 0 0 0 1 0 0 1 7.7 %
total 1 0 0 8 4 0 13 100.0 %
sequence a B D total %
First 0 0 0 2 3 0 5 38.5 %repeat 1 0 0 6 1 0 8 61.5 %
total 1 0 0 8 4 0 13 100.0 %
table 7.4b(i) pancreas islet transplants, from 2005 to 2009
year 2005 2006 2007 2008 2009 2008/2009
recipients transplanted 12 3 8 9 11 22.2 %number of transplants 19 5 15 17 18 5.9 %number of donors used 61 18 40 37 36 -2.7 %
table 7.4b(ii) pancreas islet transplants in 2009
group center bbctp gDrtp nlbtp total
recipients transplanted 6 2 3 11number of transplants 12 2 4 18number of donors used 29 2 5 36

81
table 7.4c(i) pancreas transplants from 2005 to 2009 - characteristics
Whole pancreas + kidney (deceased donor) transplants
blood group 2005 2006 2007 2008 2009 2008/2009
a 86 81 75 90 76 -15.6 %ab 10 11 11 12 12 0.0 %b 30 26 21 12 16 33.3 %o 83 77 73 80 68 -15.0 %
total 209 195 180 194 172 -11.3 %
Waiting time (months) 2005 2006 2007 2008 2009 2008/2009
0-5 50 35 32 34 35 2.9 %6-11 84 70 29 36 24 -33.3 %12-23 59 76 97 83 80 -3.6 %24-59 14 14 20 38 28 -26.3 %60+ 2 0 2 3 5 66.7 %
total 209 195 180 194 172 -11.3 %
sequence 2005 2006 2007 2008 2009 2008/2009
First 202 181 179 187 165 -11.8 %repeat 7 14 1 7 7 0.0 %
total 209 195 180 194 172 -11.3 %
table 7.4c(ii) pancreas transplants 2009 - characteristics
Whole pancreas + kidney (deceased donor) transplants
blood group a B D total %
a 16 4 4 47 5 0 76 44.2 %ab 2 0 1 8 0 1 12 7.0 %b 2 2 1 10 1 0 16 9.3 %o 12 6 7 37 5 1 68 39.5 %
total 32 12 13 102 11 2 172 100.0 %
Waiting time (months) a B D total %
0-5 13 3 10 8 0 1 35 20.3 %6-11 11 2 2 7 2 0 24 14.0 %12-23 8 5 1 59 6 1 80 46.5 %24-59 0 2 0 23 3 0 28 16.3 %60+ 0 0 0 5 0 0 5 2.9 %
total 32 12 13 102 11 2 172 100.0 %
sequence a B D total %
First 30 12 13 97 11 2 165 95.9 %repeat 2 0 0 5 0 0 7 4.1 %
total 32 12 13 102 11 2 172 100.0 %

82
Figure 7.5 Dynamics of the eurotransplant pancreas+kidney and islet+kidney waiting list, pancreas+kidney, islet+kidney, pancreas and islet-only transplants between 1991 and 2009
1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009
Islet+Kidney & Pancreas+Kidney waiting list 120 141 112 98 85 110 127 155 193 195 144 219 176 203 217 242 304 300 349Islet transplants 0 1 6 5 15 6 9 7 2 9 18 46 33 23 17 5 15 17 18Pancreas transplants 4 4 2 3 1 8 15 17 13 16 19 39 35 34 31 31 29 20 13Islets+Kidney transplant 0 0 0 1 5 9 13 4 4 4 5 4 3 4 2 0 0 0 0Pancreas+Kidney transplants 70 62 92 87 98 131 189 230 282 302 264 208 247 229 209 195 180 194 172
0
50
100
150
200
250
300
350
400

83
8. Histocompatibility Testing
I.I.N. Doxiadis, PhD and F.H.J. Claas, PhD, Eurotransplant Reference Laboratory, Department of Immunohaematology and Blood Transfusion, Leiden University Medical Center, Leiden, The Netherlands
8.1 introduction
An ongoing task of the Eurotransplant Reference Laboratory (ETRL) is the improvement and maintenance of the high quality of transplantation relevant parameters as HLA typing, screening for relevant antibodies and cross matching within Eurotransplant (ET) and its affiliated centers. This task is addressed by organizing schemes for External Proficiency Testing exercises (EPT) for the collaborating Tissue Typing Centers (TTC). Furthermore, the ETRL initiates studies and promotes discussions for possible new recommendations with the help of the Tissue Typing Advisory Committee (TTAC). In addition, for almost 30 years the ETRL has addressed the problem of highly sensitized patients, by organizing and promoting the Acceptable Mismatch (AM) program within and outside ET. Finally, visits to the affiliated TTC belong to its duties. For example in 2009 a TTTC of Germany was visited upon invitation to help overcome transplantation immunology related problems. Furthermore, laboratories of Eastern Europe, e.g. Estonia were visited for eventual participation in ET. Finally, the ETRL provides 24 hours a day, 7 days a week duty for all transplantation relevant immunological aspects for all patients within ET.
8.2EurotransplantExternalProficiencyTestingSchemes
The results of the EPT Exercises, applied in 2009, to determine the individual performance of the TTC’s were:
8.2.1ExternalProficiencyTestingonHLAtyping
For this EPT each participating laboratory received 12 peripheral blood samples from healthy donors for typing and was asked to report the results prior to a certain deadline. For the analysis of the results the typing provided by the ETRL was taken as correct, as proposed by the External Proficiency Testing Committee of the European Federation for Immunogenetics (www.efiweb.eu). The participants had to report their results on the basis of matching determinants (http://etrl.eurotransplant.nl/cms/index.php?page=services), a transcription of molecular typing results to serological equivalents, which are used in the ET matching algorithm and the report of the screening results.
In the period 2009, for HLA-A, B, (C) typing 54/55 participants used molecular methods, 44 of them additionally complement dependent cytotoxicity (CDC). For HLA-DR, (DQ) 54/55 used molecular techniques and 15 in addition CDC. The concordance rates were HLA-A=99%; HLA-B=97%; HLA-C=96%; HLA-DR=97% and HLA-DQ=98%. All of the observed discrepancies could be attributed to clerical errors. The use of molecular and serological typing indicate that laboratories affiliated to ET as well as to other organ exchange organizations use the results of the serological typing (expression of antigens in the cell surface) to evaluate the cross matches.
8.2.2ExternalProficiencyTestingoncrossmatchingThe participants of this External Proficiency Testing Exercise were asked to perform cross matches using sera of 4 different patients of the kidney waiting list from ET selected by the ETRL and the cells provided for the EPT on typing as targets. The TTC were asked to use the local crossmatch techniques, as described in their Standard Operation Procedures (SOP) to simulate the day-to-day practice. The TTC perform the test using CDC with and without dithiothreitol (DTT). This agent destroys IgM specific antibodies. The TTC were free to use unseparated peripheral blood cells, separated T and/or B cells but they had to report a final crossmatch result as it is done for organ donor procedures. Incidentally a flow cytometry crossmatch was used. Therefore, the average number of reports per category varies (table 8.1). In total 48 sera had to be crossmatched per participant. For the centers not receiving the sera of the patients on the waiting list, i.e. German centers performing patient histocompatibility work only, Scandia Transplant laboratories, and centers from other organ exchange organizations such as the Czech Republic, 8 sera were selected by the ETRL and sent to the participants. These participants could report 48 cross matches in total. The target cells and the respective results are presented in table 8.1.

84
table 8.1 report of the crossmatch results (Dtt = dithiothreitol). The numbers represent the discrepancy rates (%) per target cell used.
unseparated t cells b cells Final results
(-) Dtt (+) Dtt (-) Dtt (+) Dtt (-) Dtt (+) Dtt (-) Dtt (+) Dtt
TTC performing donor HLA typing 4.3 3.9 3.5 2.5 5.1 3.7 5.2 3.5
TTC performing patient HLA typing only 4.2 5.4 3.4 4.8 3.8 4.3 4.1 5.3
8.2.3ExternalProficiencyTestingExerciseonscreening
In 2009 the scheme of the EPT on screening for HLA specific antibodies comprised 3 shipments of 6 sera, instead of the usual two shipments. The ETRL had to adhere to the recommendations of the External Proficiency Testing Committee of the European Federation for Immunogenetics to release certificates on the basis of the calendar year. The HLA typing of the serum donor, the immunizing partner and of one of the children is known in almost all instances, and is reported to the participants beforehand. The ETRL received results from 67 participants cooperating with solid organ transplant centers within and outside ET. Currently, the methods for screening for HLA specific antibodies are evolving rapidly, the reason why standardized analyses cannot be done yet. Besides CDC, solid phase assays (SPA) of different commercial companies were used. Nine participants reported results of a single method, 37 two, 17 three and 4 participants reported data using four different tests (CDC, ELISA, Single antigen beads and flow PRA). The %-PRA value remains an unreliable parameter. The virtual PRA value (http://etrl.eurotransplant.nl/cms/index.php) is more and more accepted and will be the future parameter for sensitization within ET.
For the question whether the sera contained antibodies directed against class I or class II the reports differed in numbers. For antibodies directed against class I (HLA-A, B, C; 870 results) a discrepancy rate of 2.4% was reported. For class II (HLA-DR, DQ; 671 results) the discrepancy rate was 3.4%. In Table 8.2 the consensus results for the reports on the HLA specificities are presented.
table 8.2 analysis of the data reported by the participants with respect to hla antigens recognized (=specificities)The numbers in the table represent the percentage discrepancy to the consensus result.
Consensus
Methods 75% 95%
4 Methods 1.8 7.3
CDC 2.5 2.8
CDC/ELI 3.0 3.4
CDC/ELI/LUM 2.5 5.5
LUM 5.6 30.0
There are two different consensus reports for the EPT on screening with respect to the specificities reported. If 75% of the participants report a given specificity as recognized by the serum then the specificity is quoted as positive. In case 95% of the participants report a serum does not recognize a given specificity (=antigen) then the specificity is quoted as negative.
In the period 2009 all participants were able to report specificities. With respect to specificities reported the least problems were observed when CDC was used either alone or in combination with other methods. The use of Luminex based methods being single antigen beads or generic seems to create more problems than expected. After a learning period the results will improve. The relevance, however, of specificities recognized by this method in solid transplantation is not yet shown.
8.3 program for the highly sensitized patients in eurotransplant
In 2009 the Acceptable Mismatch Program (AM) program organized and controlled by the ETRL has been an efficient tool for a number of highly sensitized patients. This program is open for all patients of ET. Information for participation can be obtained directly from the ETRL, the ET Medical Administration, or from the ET website (http://etrl.eurotransplant.nl/cms/index.php).

85
The evolution of the AM over the years is presented in table 8.3. A significant increase both in patients included in the AM as well as transplantation via this program is observed. A point of worries is the number of patients not fulfilling the AM criteria but who are proposed by the different centers. These patients have in general HLA specific antibodies observed in SPA only. According to the understanding of the ETRL, the TTAC, and the Tissue Typers Community within ET, these antibodies are risk factors and not a contraindication for transplantation. Therefore, patients with SPA defined antibodies only are not eligible for the AM (see below).
table 8.3 evolution of the acceptable mismatch program
N 2006 2007 2008 2009
On AM Waiting List 194 224 252 309
New patients accepted 77 105 93 179
Patients denied access* 10 14 18 36
Transplanted 44 67 71 98
The main reason for the significant increase in the number of patients on the AM waiting list and the number of transplants performed via the program is the increased acceptance of the program in Germany.
8.4 other activities
The ETRL siteThe site of the ETRL (http://etrl.eurotransplant.nl/cms/index.php) is open for all laboratories working in the field of organ transplantation immunology and histocompatibility. Besides important information on the duties of the ETRL, the participants of the EPT can download the respective forms for the report of the results as well as the final analysis. Further information of future meetings within ET as well as reports of these meetings is found there. Two new programs already used for several years at the ETRL were put on the public site: the virtual-PRA, which is based on the HLA typing results of organ donors procured in the ET area (N=4000) but which also allows PRA calculations on the national data bases of Austria, Belgium, Germany and the Netherlands. The second program allows the calculation of the chance a highly sensitized patient has to obtain a crossmatch negative organ, when HLA type, blood group and acceptable mismatches are defined.
Annual Tissue Typers MeetingThe Annual Tissue Typers Meeting was held in October 2009 in Leiden. Over a 160 participants from the different TTC within and outside ET were present. The topic was, as in the past years, the relevance of HLA specific and other antibodies in kidney transplantation. The new techniques leading to a high virtual PRA value were discussed. Patients having antibodies found in solid phase assays only cannot be accepted in the AM Program, even if their virtual PRA value exceeds 85%. In addition the dispatch of patient sera for crossmatches in the donor center was discussed. Finally a short report on the EPT activities was delivered. A summary of this meeting is presented on the site of the ETRL.
Tissue Typing Advisory Committee (TTAC)The reports of the meetings of the TTAC and the accepted recommendations have been published in the ET Newsletter. The TTAC discussed a possible change in the allocation procedure where more effort should be given to the humoral immunity. Whether it is feasible to omit crossmatches for sensitized patients in the donor center (which would mean no shipment of crossmatch sera anymore) will be tested in the Netherlands. The new version of the Manual for Histocompatibility Testing was accepted.

86
9. Scientific Output in 2009ThenamesofauthorswhoworkattheEurotransplantcentralofficeorEurotransplantReferencelaboratory are in Italic.
publications - articles / abstracts
Moers C, Smits JM, Maathuis MH, Treckmann J, van Gelder F, Napieralski BP, van Kasterop-Kutz M, van der Heide JJ, Squifflet JP, van Heurn E, Kirste GR, Rahmel A, Leuvenink HG, Paul A, Pirenne J, Ploeg RJMachine perfusion or cold storage in deceased-donor kidney transplantationN Engl J Med. 2009 Jan 1;360(1):7-19
Beimler JH, Morath C, Schmidt J, Ovens J, Opelz G, Rahmel A, Zeier M, Süsal CSuccessful deceased-donor kidney transplantation in crossmatch-positive patients with peritransplant plasma exchange and RituximabTransplantation. 2009 Mar 15;87(5):668-71
Claas FH, Doxiadis IIHLA antibody detection and kidney allocation within EurotransplantHum Immunol. 2009 Apr 15 [Epub ahead of print]
Vermeulen BA, Hogen Esch CE, Yuksel Z, Koning F, Verduijn W, Doxiadis II, Schreuder GM, Mearin MLPhenotypic variance in childhood coeliac disease and the HLA-DQ/DR dose effectScand J Gastroenterol. 2009;44(1):40-5
Spaderna H, Weidner G. Zahn D, Smits JPsychological characteristics and social integration of patients with ischemic and non-ischemic heart failure newly listed for heart transplantation: The waiting for a new heart studyApplied Psychology: Health and Well-being, 2009;1:188-210
D’Orsogna LJ, Amir AL, Zoet YM, van der Meer-Prins PM, van der Silk AR, Kester MG, Heemskerk MH, Doxiadis II, Roelen DL, Claas FHNew tools to monitor the impact of viral infection on the alloreactive T-cell repertoireTissue Antigens. 2009 Jul 15. [Epub ahead of print]
Claas FH, Doxiadis IIManagement of the highly sensitized patientCurr Opin Immunol. 2009 Aug 12. [Epub ahead of print]
Heemskerk MB, Haase-Kromwijk BJ, Claas FH, Doxiadis II, Haasnoot GW, Homan van der Heide JJ, Weimar WW, Hoitsma AJRegional kidney allocation based only on full HLA-DR compatibility is not feasibleTransplantation. 2009 Aug 27;88(4):600-1
Claas FH, Rahmel A, Doxiadis IIEnhanced kidney allocation to highly sensitized patients by the acceptable mismatch programTransplantation. 2009 Aug 27;88(4):447-52
Claas FH, Doxiadis IIHuman leukocyte antigen antibody detection and kidney allocation within EurotransplantHum Immunol. 2009 Aug; 70(8):636-9. Epub 2009 Apr 16.
Doxiadis II, Claas FHTransplantation of highly sensitized patients via the acceptable mismatch program or desensitization? We need bothCurr Opin Organ Transplant. 2009 Aug; 14(4):410-3
Van Rood JJ, Stevens CE, Smits J, Carrier C, Carpenter C, Scaradavou AReexposure of cord blood to noninherited maternal HLA antigens improves transplant outcome in haematological malignanciesProc Natl Acad Scri USA. 2009 Nov 24;106(47):19952-7

87
Hoefer D, Ruttmann-Ulmer E, Smits JM, Devries E, Antretter H, Laufer GDonor hypo- and hypernatremia are predictors for increased 1-year mortality after cardiac transplantationTransplant Int. [Epub ahead of print]
Vinkers M, Smits J, Tieken I, de Boer J, Ysebaert D, Rahmel AKidney donation and transplantation in Eurotransplant 2006-2007: Minimizing discard rates by using a rescue allocation policyProg Transplant. 2009 Dec; 19(4):365-70
Schnuelle P, Gottmann U, Hoeger S, Boesebeck D, Lauchart W, Weiss C, Fischereder M, Jauch KW, Heemann U, Zeier M, Hugo C, Pisarski P, Krämer BK, Lopau K, Rahmel A, Benck U, Birck R, Yard BA Effects of donor pre-treatment with dopamine on graft function after kidney transplantation: a randomized controlled trial JAMA 2009 Sep 9; 302(10):1067-75
Doxiadis GG, de Groot N, Dauber EM, van Eede PH, Fae I, Faner R, Fischer G, Grubic Z, Lardy NM, Mayr W, Palou E, Swelsen W, Stingl K, Doxiadis II, Bontrop REHigh resolution definition of HLA-DRB haplotypes by a simplified microsatellite typing techniqueTissue Antigens 2009 Sep 24 [Epub ahead of print]
Spaderna H, Mendell NR, Zahn D, Wang Y, Kahn J, Smits JM, Weidner GSocial isolation and depression predict 12-month outcomes in the “Waiting for a New Heart Study”J Heart Lung Transplant. 2009 Oct 3 [Epub ahead of print]
Hertz MI, Aurora P, Christie JD, Dobbels F, Edwards LB, Kirk R, Kucheryavaya AY, Rahmel AO, Rowe AW, Stehlik J, Taylor DOScientific registry of the International Society for Heart and Lung Transplantation: Introduction to the 2009 Annual ReportsJ Heart Lung Transplant. 2009 Oct; 28(10):989-992
Kirk R, Edwards LB, Aurora P, Taylor DO, Christie JD, Dobbels F, Kucheryavaya AY, Rahmel AO, Stehlik J, Hertz MIRegistry of the International Society for Heart and Lung Transplantation: Twelfth official pediatric heart transplantation report-2009J Heart Lung Transplant. 2009 Oct; 28(10):993-1006
Taylor DO, Stehlik J, Edwards LB, Aurora P, Christie JD, Dobbels F, Kirk R, Kucheryavaya AY, Rahmel AORegistry of the International Society for Heart and Lung Transplantation: Twenty-sixth Official Adult Heart Transplant Report-2009J Heart Lung Transplant. 2009 Oct; 28(10):1007-1022
Aurora P, Edwards LB, Christie JD, Dobbels F, Kirk R, Rahmel AO, Stehlik J, Taylor DO Kucheryavaya AY, Hertz MIRegistry of the International Society for Heart and Lung Transplantation: Twelfth Official Pediatric Lung and Heart/Lung Transplantation Report-2009J Heart Lung Transplant. 2009 Oct; 28(10):1023-1030
Christie JD, Edwards LB, Aurora P, Dobbels F, Kirk R, Rahmel AO, Stehlik J, Taylor DO, Kucheryavaya AYThe Registry of the International Society for Heart and Lung Transplantation : Twenty-sixth Official Adult Lung and Heart-Lung Transplantation Report-2009J Heart Lung Transplant. 2009 Oct; 28(10):1031-1049
Mulder A, Kardol MJ, Arn JS, Eijsink C, Franke ME, Schreuder GM, Haasnoot GW, Doxiadis II, Sachs DH, Smith DM, Claas FHHuman monoclonal HLA antibodies reveal interspecies crossreactive swine MHC class I epitopes relevant for xenotransplantationMol Immunol. 2009 Nov 19. [Epub ahead of print]
Smits JM, van der Bij W, Rahmel AOAllocation of donor lungsEur Respir Mon. Lung Transplantation; 2009, Vol 45, 88-103

88
Verduin EP, Schonewille H, Lindenburg I, Lopriore E, Doxiadis II, Brand ALong term RBC and HLA antibody follow-up after intra-uterine transfusionsTransfusion, Sept 2009, Vol. 49, S3: 125A-126nA
Campos EF, Doxiadis II, Temin J, Plothow A, Bellintani E. Fumeiro L, Miyamoto Y, Dantas L, Medina-Pestana J, Gerbase-DeLima MAcceptable HLA mismatches algorithm for increasing the transplantability of highly sensitized patientsHuman Immunology, Nov 2009, Vol. 70, S1: S14
Heidt S, Roelen D, Doxiadis II, Claas F, Mulder ABortezomib affects the function of human B cells: Possible implications for desensitization protocolsHuman Immunology, Nov 2009, Vol. 70, S1: S157
inviteD lectures
Annual Symposium Organ Donation and Transplantation 1. February 4, 2009, Leuven, Belgium The Eurotransplant regulations on transplantation of non-residents Rahmel A
5th Expert Summit on Viral Hepatitis 2. February 6 and 7, 2009, Munich, Germany MELD-score Rahmel A
Walter-Brendel-Kolleg für Transplantationsmedizin 3. March 6-11, 2009, Wildbad Kreuth, Germany Organ Verteilung durch Eurotransplant Rahmel A
Bootcongres Nederlandse Transplantatie Vereniging 4. March 25-27, 2009, Zeewolde, the Netherlands Transplantatie over de grenzen heen: de cijfers Rahmel A
95. th Congress of the Polish Transplantation Society May 14-16, 2009, Cracow, Poland Organ procurement and transplantation – Eurotransplant experience Rahmel A
Eastern European Transplant Coordinators meeting 6. June 1, 2009, Prague, Czech Republic Extended criteria donors and their allocation Smits J
19. Transplantationstreffen: Bridging zur Herztransplantation7. June 10, 2009, Münster, Germany Considerations for patients awaiting heart transplantation Smits J
Berner Symposium für Transplantationsmedizin 8. September 10, 2009, Bern, Switzerland Der alte Organspender bei Eurotransplant: bis zu welchem Alter ist die Allokation (Zuteilung) von welchen Organen noch sinnvoll? Rahmel A
Journée des Assises de la Transplantation 9. September 24, 2009, Paris, France Analysis of survival after organ transplantation: Methodology or how formulas can help in understanding transplantation-related problems Smits J

89
CD-P-TO Meeting 10. October 2-4, 2009, Berlin, Germany International organ exchange – Safety and quality for organs, tissues and cells transportation Rahmel A
Organ Donation Congress 11. October 4-7, 2009, Berlin, Germany Benefits and challenges of an international cooperation in organ allocation and transplantation Rahmel A
DiaTransplant Congress 12. October 15-18, 2009, Opatija, Croatia Croatia and Eurotransplant: what is done and what has to be done? Rahmel A
Kick-off Meeting EDD Ljubljana 13. October 16-18, 2009, Ljubljana, Slovenia Introduction of a European Donation Day Rahmel A
18. Jahrestagung Deutsche Transplantationsgesellschaft 14. October 29-31, 2009, Berlin, Germany Mitgliederversammlung October 29, 2nd ELPAT Invitational Conference 2009, Bericht von ET Rahmel A
Podiumsdiskussion Transplantationswesen 15. November 30, 2009, Regensburg, Germany Rahmel A
les Journées de l´Agence de la biomédecine 16. December 14-15, 2009, Paris, France L´expérience d´Eurotransplant Rahmel A
chairmenships
Transplant Symposium Freiburg 1. January 8-9, 2009, Freiburg, Germany Session III: Clinical strategies regarding heart transplantation of HLA-sensitized patients Rahmel A
Symposium 25 Jahre Herztransplantation 2. March 18-19, 2009, Vienna, Austria Member at a ‚Podiumsdiskussion’ Rahmel A
Wintermeeting ‘Thorakale Organtransplantation – wo stehen wir heute?’ 3. January 16, 2009, Hamburg, Germany Referent: ‚Aktuelle Situation der Organspende’ Rahmel A
74. th Starnberg Workshop Pancreas Transplantation June 11-12, 2009, Starnberg, Germany Workshop Session I Criteria for appropriate donor selection Rahmel A

90
oral presentations
Eurotransplant Winter Meeting 1. January 22-24, 2009, Alpbach, Austria Machine preservation Rahmel A
12. st Seminar on diverse strategies for fighting organ shortage in Europe: organizational and ethical questions May 5 – 6, 2009, Paris, France Organ shortage – increasing the use of available donor organs by organ allocation strategies within Eurotransplant Rahmel A
Hesperis – Advanced Training Course in Organ Transplantation 3. May 6, 2009, Leuven, Belgium How to allocate organs Rahmel A
23rd European Immunogenetics and Histocompatibility Conference (EFI) 4. 17th Annual Meeting of the German Society for Immunogenetics (DGI) May 9 – 12, 2009 Educational Session IV Blood Sweat and Tears 2009 Crossmatching and screening O’Neill D, Doxiadis I
41. gemeinsame Jahrestagung Deutsche Gesellschaft für Internistische Intensivmedizin und Notfallmedizin, 5. Österreichische Gesellschaft für Internistische und Allgemeine Intensivmedizin June 10 – 13, 2009, Hamburg, Germany Probleme der Organspende aus Sicht von Eurotransplant Rahmel A
20. Workshop für experimetnelle und klinische Lebertransplantation und Hepatologie 6. June 25 – 27, 2009, Wilsede, Germany Bedeutung der Spenderkriterien mit ECD-Kriterien auf die Allokation: wie geht es weiter? Rahmel A
15th Annual International Congress ILTS (International Liver Transplantation Society) 7. July 8 – 11, 2009, New York, USA Two-year experience with MELD-based liver allocation in Eurotransplant shows a substanial decrease in mortality on the waiting list in the first 6 months after listing. Rahmel A
Catholic University of Curitiba 8. August 2009, Curitiba, Brazil The Acceptable Mismatch Program Doxiadis I
30 years of stem cell transplantation 9. August 2009, Curitiba, Brazil Antibodies in transplantation Doxiadis I Immunity and transplantation (how to get confused) Doxiadis I
1410. th Congress of the European Society for Organ Transplantation (ESOT) August 30 – September 2, 2009, Paris, France Kidney donor allocation and transplantation: Minimizing discard rates by using a rescue allocation policy Smits J Increasing the donor pool by the use of a lung donor score Smits J

91
Machine perfusion versus cold storage preservation in non-heart-beating kidney donation and transplantation: first results of a multicentre trial in Eurotransplant Pirenne J, Smits J, Moers C, Maathuis MH, Treckmann J, Napieralski B, van Kasterop-Kutz M, Homan van der Heide J, van Heurn E, Kirste G, Rahmel A, Leuvenink H, Paul A, Monbaliu D, Jochmans I, Squifflet J-P, Ploeg R Preliminary results of a study for liver donor quality within the Eurotransplant database: Striking differences with the UNOS liver donor quality! Braat A, Blok J, Kooreman N, Dubbeld J, Putter H, Rahmel A, Porte R, Rogiers X, Ringers J
2009 Organ Donation Congress: 1011. th ISODP & 16th ETCO October 4 – 7, 2009, Berlin, Germany Kidney donor allocation and transplantation: Minimizing discard rates by using a rescue allocation policy Smits J Increasing the donor pool by the use of a lung donor score Smits J
poster presentations
141. th Congress of the European Society for Organ Transplantation (ESOT) August 30 – September 2, 2009, Paris, France Short and long term cost-effectiveness of hypothermic machine perfusion versus static cold storage in kidney transplantation Groen H, Moers C, Smits J, Treckmann J, Monbaliu D, Rahmel A, Paul A, Pirenne J, Ploeg R, Buskens E Bortezomib affects the function of human B cells: possible implications for desensitization protocols Heidt S, Roelen D, Doxiadis I, Claas F, Mulder A Combined KIR/HLA genotyping indicates a role for alloreactive natural killer cells in kidney transplantation van Bergen J, Thompson A, Haasnoot G, Roodnat J, de Fijter J, Claas F, Koning F, Doxiadis I

92
10. Eurotransplant personnel related statistics
intake number of new employees
number of employees (Dec. 31, 2009)
intake percentage
Regular 9 70 12.9%
Student 14 25 56.0%
Total 23 95 24.2%
Outflow exit number number of employees (Jan. 1, 2009) Outflowpercentage
Regular 4 66 6.1%
Student 18 29 62.1%
Total 22 95 23.2%
employees on December 31, 2009 numbers Fte Fte*
Students 25 8.95
Part-timer 33 25.33
Full-timer 25 25.00
Full-timer + (>36 hours/week) 12 13.28
Total 95 72.56
* The calculation of the number of fte’s is based on the number of employees actually working for ETI during the year (taking into account the shared services and the exit or entrance of employees during the year).
breakdown of fte gross Fte
recharged or charged *
nett Fte
Personel in fte’s 72.56 12.22 60.34
* The fte’s based on the shared services will partially be recharged to the Dutch Transplant Foundation and NBF-BIS Foundation. Activitities which are done bij personel from the Dutch Transplant Foundation or NBF-BIS are charged to Eurotransplant.
male Female
Divison male/Female nr. % nr. %
Regular 33 47.1% 37 52.9%
Students 10 40.0% 15 60.0%
Total 43 45.3% 52 54.7%
absentee ratesgross
absenteeism* nett absenteeism** average absentee frequencies
average absentee duration
Regular 2.50% 2.50% 1.8 4.9 days
Students 0.30% 0.30% 0.2 2.1 days
* Gross absenteeism concerns all absenteeism caused by illness.
** Nett absenteeism concerns all absenteeism caused by illness, excluding insured absenteeism. In case of insured absenteeism, the employer receives sickness benefits for the absenteeism. This involves absenteeism related to pregnancy or maternity, organ donation or with regard to employees who have a prior history of insured absenteeism.

93
11. Abbreviated financial statements
Abbreviated financial statements of Stichting Eurotransplant International Foundation,for the year ended december 31, 2009
ForafullunderstandingoftheFoundation’sfinancialpositionandresults,theabbreviatedfinancialstatementsshouldbereadinconjunctionwiththefinancialstatementsfromwhichtheabbreviatedfinancialstatementshavebeenderived.
balance sheet
Assets 31.12.2009 31.12.2008x € 1.000 x € 1.000
Fixed assets 555 728Short term receivables 2.403 1.948Liquid assets 1.909 1.011
4.867 3.687
Liabilities 31.12.2009 31.12.2008x € 1.000 x € 1.000
Capital 235 235Reserve funds 2.536 1.949Provisions 55 46Short term liabilities 2.041 1.457
4.867 3.687
statement of income and charges2009 2008
Income x € 1.000 x € 1.000
Registration fees 6.457 5.634Procurement fees 2.347 2.290Miscellaneous 143 59Extra-ordinary income 0 10
8.947 7.993
2009 2008Charges x € 1.000 x € 1.000
Salaries 4.014 3.911Procurement charges 2.334 2.278General expenses 729 622Medical expenses 69 67Transport 12 13Housing 256 236Depreciation 293 296Miscellaneous 448 474Extra-ordinary expenses - -
8.155 7.897
Equalization registrations and audits 205 -
Exploitation balance 587 96

94
appropriation of the exploitation balanceAddition Reserve Fund explantation costs 12 12Release Reserve Fund Reorganization - -25Addition Tariff Equality Reserve 574 74Addition Other reserves - 35
587 96
accounting policies
General accounting principles for the preparation of the financial statementsThe annual accounts have been prepared in accordance with Guideline 640 of the Dutch Accounting Guidelines.
Valuation of assets and liabilities and determination of the result takes place under the historical cost convention. Unless presentedotherwiseattherelevantprincipleforthespecificbalancesheetitem,assetsandliabilitiesarepresentedatfacevalue.
Incomeandexpensesareaccountedforonaccrualbasis.Profitisonlyincludedwhenrealizedonthebalancesheetdate.Lossesoriginatingbeforetheendofthefinancialyeararetakenintoaccountiftheyhavebecomeknownbeforepreparationof the annual accounts.
Financial instrumentsFinancialinstrumentsbebothprimaryfinancialinstruments,suchasreceivablesandpayables,andfinancialderivatives.Fortheprinciplesofprimaryfinancialinstruments,referenceismadetothetreatmentperbalancesheetitem.
Translation of foreign currencyReceivables, liabilities and obligations denominated in foreign currency are translated at the exchange rates prevailing at balance sheet date.
Transactionsinforeigncurrencyduringthefinancialyeararerecognizedinthefinancialstatementsattheexchangeratesprevailing at transaction date. The exchange differences resulting from the translation as of balance sheet date, taking into accountpossiblehedgetransactions,arerecordedintheprofitandlossaccount.
principles of valuation of assets and liabilities
Tangible fixed assetsTangiblefixedassetsarepresentedatcostlessaccumulateddepreciationand,ifapplicable,lessimpairmentsinvalue.Depreciationisbasedontheestimatedusefullifeandcalculatedasafixedpercentageofcost,takingintoaccountanyresidual value. Depreciation is provided from the date an asset comes into use.
Accounts receivableReceivables are included at face value, less any provision for doubtful accounts. These provisions are determined by individual assessment of the receivables.
Other receivables, prepaid expenses, accruals and short term liabilitiesThese items are stated at nominal value.
Reserve FundsReserve Funds are formed for future expenditures which should be covered out of the available assets.The Reserve Funds can be considered as reserves as set out in Dutch Accounting Guideline 640.309 whereas the setting of the objective of each Reserve Fund is determined by the Board of Management.
ProvisionsThe provision for jubilee is based on the expected costs for a series of years. Payments for a jubilee are deducted from theprovision.
Provision for employee benefitsIndustry pension fund scheme:ThepensionplanaccordingtotheCollectiveLaborAgreementforGeneralHospitalsisfinancedthroughcontributionstoanindustrypensionfund.Thepensionplantakencareofbythefundisadefinedbenefitplan.Adefinedbenefitplanhasbeenrecognizedasifitwereadefinedcontributionplan,astheorganizationhasnocommitmenttomakeadditionalcontributionsintheeventofadeficitotherthanhigherfuturepremiums.

95
principles for the determination of the result
Registration feesRegistration fees are taken into account as of the date of entry on the waiting list of Eurotransplant.
Operating (government) grantsOperating grants are included in the statement of income and charges in the year to which the subsidized costs are charged.
ChargesThe general expenses of the Stichting Eurotransplant International Foundation are stated on the basis of transaction costs.Certain general expenses of the Nederlandse Transplantatie Stichting, Stichting Bio Implant Services Foundation and Stichting Eurotransplant International Foundation are made for common account. Such costs are divided between the three foundations on the basis of activity-levels.
Exploitation BalanceTheexploitationbalanceisdefinedasthedifferencebetweenincomeandrelatedcharges,basedontheabovementionedpolicies.
To the Board of Management and Board of Directors of Stichting Eurotransplant International foundation at leiden
auditor’s report
IntroductionWehaveauditedwhethertheaccompanyingabbreviatedfinancialstatementsofStichtingEurotransplantInternationalFoundation, Leiden, for the year 2009 have been derived consistently from the audited annual accounts of Stichting Eurotransplant International Foundation, for the year 2009. In our auditors’ report dated April 12, 2010 we expressed an unqualifiedopinionontheseannualaccounts.Theboardofdirectorsisresponsibleforthepreparationoftheabbreviatedfinancialstatementsinaccordancewiththeaccountingpoliciesasappliedinthe2009annualaccountsofStichtingEurotransplantInternationalFoundation.Ourresponsibilityistoexpressanopinionontheseabbreviatedfinancialstatements.
Scope We conducted our audit in accordance with Dutch law. This law requires that we plan and perform the audit to obtain reasonableassurancethattheabbreviatedfinancialstatementshavebeenderivedconsistentlyfromtheannualaccounts.Webelievethattheauditevidencewehaveobtainedissufficientandappropriatetoprovideabasisforourauditopinion.
OpinionInouropinion,theseabbreviatedfinancialstatementshavebeenderivedconsistently,inallmaterialrespects,fromthefinancialstatements.
emphasis of matter
Forabetterunderstandingofthefoundation’sfinancialpositionandresultsandthescopeofouraudit,weemphasizethattheabbreviatedfinancialstatementsshouldbereadinconjunctionwiththeunabridgedannualaccounts,fromwhichtheabbreviatedfinancialstatementswerederivedandourunqualifiedauditors’reportthereondatedApril12,2010.Ouropinionisnotqualifiedinrespectofthismatter.
Leiden, April 12, 2010
Deloitte Accountants B.V.
Already signeddrs. G.J.W. Coppus RA

96
list of abbreviations
ACO Approved Combined OrganAM Acceptable MismatchCDC Complement Dependent CytotoxicityCSWG Computer Services Working GroupDPA Donation Procedure ApplicationDTT DithiothreitolEFRETOS European FRamework for the EvaluaTion of Organ transplantSELIAC ET Liver Intestine Advisory CommitteeENIS ET Network Information SystemEPAC ET Pancreas Advisory CommitteeEPT External Proficiency TestingESDP ET Senior DR-matching ProgramESOT European Society for Organ TransplantationET EurotransplantETEC ET Ethics CommitteeEThAC ET Thoracic Advisory CommitteeETKAC ET Kidney Advisory CommitteeETKAS ET Kidney Allocation SystemETP ET Policy PlanETRIP ET Registry of Islets and PancreasETRL ET Reference LaboratoryEuTIEP EurotransplanT Information Exchange PlatformFC Financial CommitteeFTE Full Time EquivalentHLA Human Leucocyte AntigenHSYI award Henk Schippers Young Investigators awardISHLT International Society for Heart & Lung TransplantationISO International Organization for StandardizationMELD Model End stage Liver DiseaseNBF-BIS Netherlands Bone Foundation-Bio Implant ServicesNTS Nederlandse Transplantatie StichtingOPC Organ Procurement CommitteePRA Panel Reactive AntibodiesSAN Storage Area NetworkSOP Standard Operation ProceduresSPA Solid Phase AssaysTTAC Tissue Typing Advisory CommitteeTTC Tissue Typing CentersUNOS United Network for Organ SharingVAD Ventricular Assist Device

EUR
OT
RA
NSP
LAN
T IN
TER
NA
TIO
NA
L FOU
ND
AT
ION
An
nu
al Rep
ort 2
00
963082 om 2005 29-06-2006 13:40 Pagina 1
2009
EUR
OT
RA
NSP
LAN
T IN
TER
NA
TIO
NA
L FOU
ND
AT
ION
An
nu
al Rep
ort 2
00
963082 om 2005 29-06-2006 13:40 Pagina 1
2009
EUR
OT
RA
NSP
LAN
T IN
TER
NA
TIO
NA
L FOU
ND
AT
ION
An
nu
al Rep
ort 2
00
963082 om 2005 29-06-2006 13:40 Pagina 1
2009