approch to a patient with acut comlications of dm
TRANSCRIPT
Diabetic ketoacidosis, DKA
MODULATOR DR. YARED(INTERNIST)

OUTLINE
Objectives
Introduction
Definition
etiology
Pathophysiology
Diagnosis Clinical features
Investigations
treatment

objectives
At the end of this seminar students are expected to: have a general view of diabetes
define what a DKA is
understand the pathophysiology of DKA
know basics of approach to a patient with DKA
manage a patient with DKA

Introduction
Diabetes Mellitus: is a common endocrine disorder characterized by: Hyperglycemia
Manifesting often with symptoms and signs of osmotic diuresis such as polyuria and polydypsia
Calorie loss, generalized weakness, polyphagia and weight loss.

Classification Type 1 (beta cell destruction, usually leading to absolute insulin
deficiency)
Type 2 (may range from predominantly insulin resistance with relative insulin deficiency to a predominantly insulin secretory defect with insulin resistance)
Other specific type A. Genetic defects of beta cell function characterized by mutations in: B. Genetic defects in insulin action. C .Diseases of the exocrine pancreas. D .Endocrinopathies E.Drug F.Infections G.Uncommon forms of immune-mediated diabetes— "stiff-person
Syndrom”
GDM

Epidemiology
The worldwide prevalence of DM has risen dramatically over the past two decades, from an estimated 30 million cases in 1985 to 285 million in 2010.
Based on current trends, the International Diabetes Federation projects that 438 million individuals will have diabetes by the year 2030

Although the prevalence of both type 1 and type 2 DM is increasing worldwide,
The prevalence of type 2 DM is rising much more rapidly, presumably because of
increasing obesity,
reduced activity levels as countries become more industrialized, and
the aging of the population.

Complications of DM
Acute Complications DKA (diabetic ketoacidosis )
HHS (hyperglycemic hyperosmolar state)
Hypoglycemia

Chronic complicationMicrovascular Macrovascular Other
Eye disease Coronary heart disease Gastrointestinal (gastroparesis, diarrhea)
Retinopathy (nonproliferative/proliferative)
Peripheral arterial disease
Genitourinary (uropathy/sexual dysfunction)
Macular edema Cerebrovascular disease
Dermatologic
Neuropathy Infectious
Sensory and motor (mono- and polyneuropathy)
Cataracts
Autonomic Glaucoma
Nephropathy Periodontal disease
Hearing loss
Diabetic ketoacidosis
The most frequent endocrine emergency seen by the primary care physician
May be the 1st presentation of type 1 DM
Result from absolute insulin deficiency or increase requirement

three cardinal biochemical features of DKA:
Hyperglycemia
Ketosis
Acidosis
Results from: hormonal imbalance Insulin deficiency Excessive counter-regulatory hormones

Precipitating causes for DKA
Lack of insuline/ drug omission most common PPt factor Infection chest(TB, pneumonia), UTI Trauma infarction inadequate food intake and skipping of injection reduction in the dose of insulin severe emotional stress

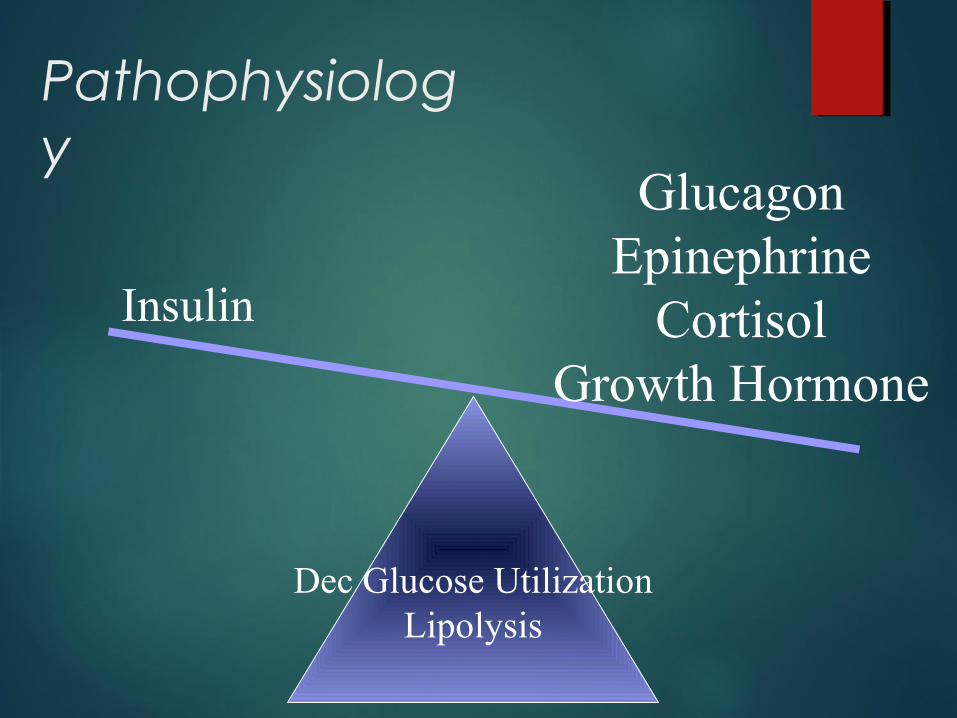
Pathophysiology
Insulin
GlucagonEpinephrine
CortisolGrowth Hormone
Pathophysiology
Dec Glucose UtilizationLipolysis
Insulin
GlucagonEpinephrine
CortisolGrowth Hormone

Pathophysiology
GluconeogenesisGlycogenolysis
LipolysisKetogenesis
Insulin
GlucagonEpinephrine
CortisolGrowth Hormone

Clinical features
Signs and symptoms of DKA are related to the degree of
hyperosmolality, volume depletion, and acidosis.

Symptoms of DKA
Polyuria Polydypsia Nausea/Vomiting Abdominal Pain Fatigue Confusion Obtundation
17

Physical Examination in DKA Hypotension, tachycardia
Kussmaul breathing (deep, labored breaths)
Fruity odor to breath (due to acetone)
Dry mucus membranes
Confusion
Abdominal tenderness
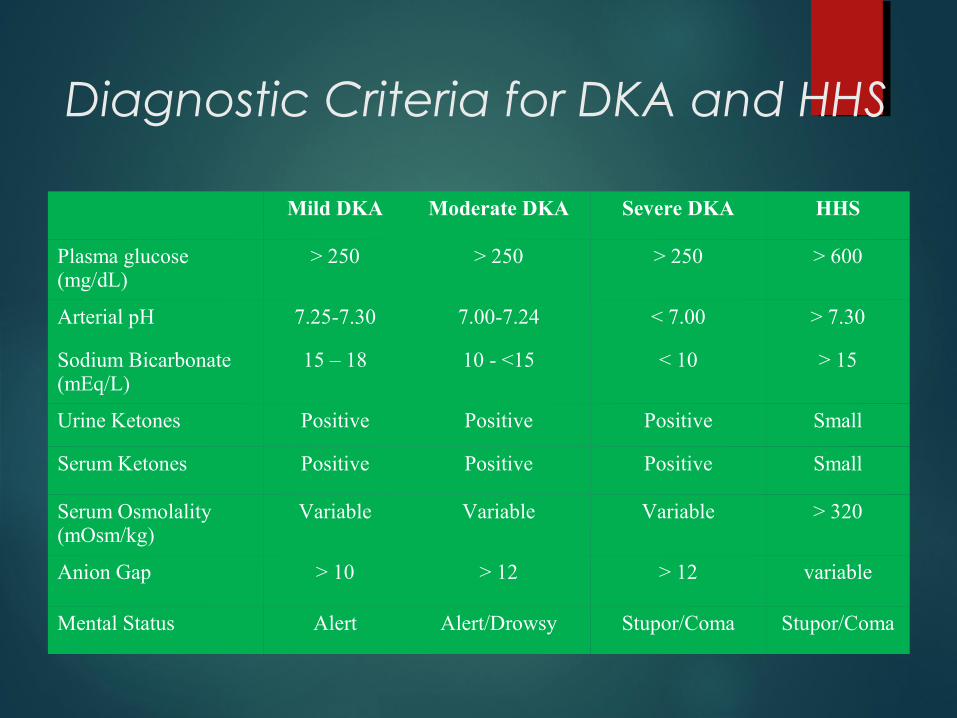
Diagnostic Criteria for DKA and HHS
Mild DKA Moderate DKA Severe DKA HHS
Plasma glucose (mg/dL)
> 250 > 250 > 250 > 600
Arterial pH 7.25-7.30 7.00-7.24 < 7.00 > 7.30
Sodium Bicarbonate (mEq/L)
15 – 18 10 - <15 < 10 > 15
Urine Ketones Positive Positive Positive Small
Serum Ketones Positive Positive Positive Small
Serum Osmolality (mOsm/kg)
Variable Variable Variable > 320
Anion Gap > 10 > 12 > 12 variable
Mental Status Alert Alert/Drowsy Stupor/Coma Stupor/Coma

Cont…
Hyperglycemia
Ketonuria and ketonemia
Acidosis (PH< 7.3 or bica < 15 mmol/l)

Laboratory finding
Plasma glucose level (mg/dl)
Plasma ketones (mmol/l)
Blood pH
Urine ketone and glucose levels
Cr and BUN
Serum Na,K, HCO3 (mEq/l)

Complication
Hypoglycemia
Electrolyte imbalance
Metabolic acidosis
Cerebral edema
Hypoxemia
ARDs

Treatment of DKA
Aims of treatmentFluid replacement Electrolyte correctionAcidosis correctionInsulin therapy for
hyperglycemiaTreatment of ppt cause
1. Confirm diagnosis (plasma glucose, positive serum ketones, metabolic acidosis).
2. Admit to hospital; intensive-care setting may be necessary for frequent monitoring or if pH <7.00 or unconscious.
3. Assess:
Serum electrolytes (K+, Na+, Mg2+, Cl–, bicarbonate, phosphate)
Acid-base status—pH, HCO3–, PCO2, -hydroxybutyrate
Renal function (creatinine, urine output)

4. Replace fluids: 2–3 L of 0.9% saline over first 1–3 h ? (15–20 mL/kg per hour),
subsequently, 0.45% saline at 250–500 mL/h;
change to 5% glucose and 0.45% saline at 150–250 mL/h when plasma glucose reaches 200 mg/dL
5. Administer short-acting insulin: IV (0.1 units/kg),
then 0.1 units/kg per hour by continuous IV infusion; increase two- to threefold if no response by 2–4 h.
If the initial serum potassium is <3.3 meq/L, do not administer insulin until the potassium is corrected.
If the initial serum potassium is >5.2 meq/L, do not supplement K+ until the potassium is corrected.

6. Assess patient: What precipitated the episode
noncompliance
infection
trauma
infarction and
cocaine
Initiate appropriate workup for precipitating event(cultures,CXR, ECG).
7. Measure
capillary glucose every 1–2 h;
measure electrolytes (especially K+, bicarbonate, phosphate) and anion gap every 4 h for first 24 h.

8. Monitor: Bp, pulse, RR,mental status, fluid intake and out put Q 1-4h.
9. Replace K+: 10 meq/h when plasma K+ < 5.0–5.2 meq/L (or 20–30 meq/L of infusion fluid),
ECG normal, urine flow and normal creatinine documented; administer 40–80 meq/h when plasma K+ < 3.5 meq/L.
10. Continue above until patient is stable, glucose goal is 150–250 mg/dL, and acidosis is resolved. Insulin infusion may be decreased to 0.05–0.1 units/kg per hour.
11. Administer long-acting insulin as soon as patient is eating. Allow for overlap in insulin infusion and SC insulin injection

DKA management protocol
General measures Stabilize ABC of life
Obtain iv access
Put them on cardiac monitor control if available
Monitor RBS every hour,urine ketone every four hour,vital signs Q2-4hr.
Identify and treat precipitating cause.
Replete fluid deficit
Give as much as NS rapidly for a patient in shock
Give at least 3 bags of NS in the first 3-4hrs unless there is acardiac compromise.
Change toDNS when blood sugar fall below 200
Replace ongoing fluid loss
The usual fluid deficit is about 3-6 litter

Replet K deficit If baseline kis <3.3mEq/l avoid insulin and administer 20-
30mEq/l per hour until k is above 3.3mEq/l
If baseline k is 3.3-5.3 mEq/l or is unkown administer 40mEq/l to run over 4-8hr after conofirming adequate urine output(≥50ml/hr or give po kcl)
if baseline k is above 5.3mEq/l don’t administer k
The target is to keep it b/n 4-5mEq/l
The k should be supplemented by second iv line not to compromise the fluid resuscitation
If abaseline serum k is unknown do ECG and check signs of hypo or hyperkalemia

Give insulin Give initial bolus of 10iu iv and 10iu im of regular insulin
Then give 5iu iv every 1hr until blood sugar <200mg/dl and ketone urine twice negative
If blood sugar doesn’t drop or is persistently above 350-400mg/dl double the dose of insulin
Overlap the last dose with the standing dose of long acting insulin
In pts with known DM who where previously treated with insulin may be given the same dose they were given before
For newly diagnosed pts insulin should be started at dose of 0.5-0.8 iu/kg/day
Measure RBS every 4-6hrs aday and give correctional dose of regular insulin(1-2iu for every 50mg/dl rise above 200mg/dl)

Patient education
Advise on adherence and appropriate storage of insulin
Advise on what to do when they have poly symptom and other symptoms of DKA
Advise on self monitoring of blood sugar

Hyperglycemic Hyperosmolar State
BY ABUBEKER M
33

Introduction
Extremely high blood glucose level (600-2000 mg/dL)
Absence of or small amounts of ketones Profound dehydration Pts have sufficient insulin to prevent
lipolysis and ketosis Occurs in older patients with type 2
diabetes Treatment: hydration and small doses of
insulin to correct the hyperglycemia
34

Clinical Features
Symptoms a several-week history of polyuria
weight loss, and
diminished oral intake that culminates in
mental confusion,
lethargy, or coma.
35

physical examination
reflects profound dehydration and
hyperosmolality and
reveals hypotension
, tachycardia,
and altered mental status.
36

precipitated by
HHS is often precipitated by a serious, concurrent illness such as
myocardial infarction or
stroke.
prior stroke or
Dementia
Pneumonia
sepsis
37

Laboratory Abnormalities and Diagnosis
plasma glucose may be >55.5 mmol/L (1000 mg/dL)],
hyperosmolality (>350 mosmol/L)
prerenal azotemia
The measured serum sodium may be normal or slightly low despite the marked hyperglycemia.
38

The corrected serum sodium is usually increased [add 1.6 meq to measured sodium for each 5.6-mmol/L (100 mg/dL) rise in the serum glucose].
In contrast to DKA,
acidosis and ketonemia are absent or mild.
39

A small anion-gap metabolic acidosis.
Moderate ketonuria.
40

Managing Acute Complications
41

Treatment: Hyperglycemic Hyperosmolar State
Treatment involves
• Fluid replacement : administration of IV fluids and
• Bringing down the blood sugar rapidly by using rapidly acting insulin preparations
• Identifying and treating the precipitating factor
42

Underlying or precipitating problems should be aggressively sought and treated.
In HHS, fluid losses and
dehydration are usually more pronounced than in DKA.
due to the longer duration of the illness.
43

The patient with HHS is usually
older, more likely to have mental status changes, and
more likely to have a life-threatening precipitating event with accompanying comorbidities.
Even with proper treatment, HHS has a substantially higher mortality rate than DKA (up to 15% in some clinical series).
44

Fluid replacement
Fluid replacement should initially stabilize the hemodynamic status of the patient (1–3 L of 0.9% normal saline over the first 2–3 h).
Because the fluid deficit in HHS is accumulated over a period of days to weeks, the rapidity of reversal of the hyperosmolar state
must balance the need for free water repletion with the risk that too rapid a reversal may worsen neurologic function.
45

If the serum sodium > 150 mmol/L (150 meq/L), 0.45% saline should be used.
After hemodynamic stability is achieved,
the IV fluid administration is directed at reversing the free water deficit using hypotonic fluids
(0.45% saline initially, then 5% dextrose in water, D5W).
46

calculated free water deficit
(which averages 9–10 L) should be reversed over the next 1–2 days
(infusion rates of 200–300 mL/h of hypotonic solution).
47
Insulin
As in DKA, rehydration and volume expansion lower the plasma glucose initially,
but insulin is also required.
A reasonable regimen for HHS begins with an IV insulin bolus of 0.1 units/kg
followed by IV insulin at a constant infusion rate of 0.1 units/kg per hour.
48

. If the serum glucose does not fall, increase the insulin infusion rate by twofold.
As in DKA, glucose should be added to IV fluid when the plasma glucose falls to 13.9–16.7 mmol/L (250–300 mg/dL), and
the insulin infusion rate should be decreased to 0.05–0.1 units/kg per hour.
49

The insulin infusion should be continued until the patient has resumed eating and can be transferred to a SC insulin regimen.
The patient should be discharged from the hospital on insulin, though some patients can later switch to oral glucose-lowering agents.
50

A 62 year-old man is brought to the emergency department by his family because he is confused. His wife had not noticed any fever,chills,nausia or vomiting.
He appears very lethargic, he is arousable but responds incoherently to questions. He only orient to his home.
T:98.9 F BP:102/62 mmHg P:122/min RR:18/min
His lung examinations is normal. His heart has RRR. There are no focal neurologic signs. And The reast of his PE is unremarkable.
51

Lab-Glucose 1,118mg/dl
-K 4.8 mg/dl
-BUN 61, Creatinine 1.5mg/dl
Hco3 24meq/l
Na 130mg/dl
CL 100 mg/dl
Ketones negatives
ECG no IHDChest x ray PUA P
52

Admit ICU
Aggressive IVF 0.9 NS
Insulin IV then IM
EcG
Blood and urine cultures etc
53

hypoglycemia
BY: ABDIFATAH Y.
54

introduction
Hypoglycemia is defined as all episodes of an abnormally low plasma glucose concentration (with or without symptoms) that expose the individual to harm.
Hypoglycemia is a clinical syndrome of diverse causes in which low levels of serum glucose can eventually lead to neuroglycopenia.
55

Clinical classification
Severe hypoglycemia:An event requiring the assistance of another person to actively administer carbohydrate, glucagon or other resuscitative actions is classified as a severe hypoglycemic event.
Documented symptomatic hypoglycemia : An event during which typical symptoms of hypoglycemia are accompanied by a measured (typically with a monitor or with a validated glucose sensor) plasma glucose concentration ≤70 mg/dL (3.9 mmol/L) is classified as a documented symptomatic hypoglycemic event.
56

Cont’d……….
Asymptomatic hypoglycemia : Asymptomatic hypoglycemia is classified as an event not accompanied by typical symptoms of hypoglycemia but with a measured plasma glucose concentration of ≤70 mg/dL (3.9 mmol/L).
Probable symptomatic hypoglycemia : Probable symptomatic hypoglycemia is classified as an event during which typical symptoms of hypoglycemia are not accompanied by a plasma glucose determination (but that was presumably caused by a plasma glucose concentration ≤70 mg/dL [3.9 mmol/L]).
57

Cont’d….
Relative hypoglycemia: Relative hypoglycemia is classified as an event during which the person with diabetes reports typical symptoms of hypoglycemia, and interprets those as indicative of hypoglycemia, but with a measured plasma glucose concentration >70 mg/dL (3.9 mmol/L).
58

Impact and Frequency
Hypoglycemia is the limiting factor in the glycemic management of diabetes.
Hypoglycemia is a fact of life for people with T1DM.
They suffer an average of two episodes of symptomatic hypoglycemia per week and at least one episode of severe, at least temporarily disabling, hypoglycemia each year.
An estimated 6–10% of people with T1DM die as a result of hypoglycemia
59

Cont’d……..
Hypoglycemia occurs less frequently in T2DM.
The frequency of hypoglycemia approaches that in T1DM as persons with T2DM develop absolute insulin deficiency and require more complex treatment with insulin.
60

Conventional Risk Factors
Insulin (or insulin secretagogue) doses are excessive, ill-timed, or of the wrong type.
The influx of exogenous glucose is reduced (e.g., during an overnight fast or following missed meals or snacks.
Insulin-independent glucose utilization is increased (e.g., during exercise).
Sensitivity to insulin is increased (e.g., with improved glycemic control, in the middle of the night, late after exercise, or with increased fitness or weight loss).
61

CONT’D………
Endogenous glucose production is reduced (e.g., following alcohol ingestion).
insulin clearance is reduced (e.g., in renal failure).
62
Causes of Hypoglycemia
Drugs: Insulin or insulin secretagogue, Alcohol, Others.
Critical illness: Hepatic, renal or cardiac failure, Sepsis , Inanition
Hormone deficiency: Cortisol, Glucagon and epinephrine (in insulin-deficient diabetes)
Non–islet cell tumor: Seemingly well individual Endogenous
hyperinsulinism : Insulinoma , Functional beta-cell disorders (nesidioblastosis)
Accidental, surreptitious or malicious hypoglycemia
63

Table 345-2 Physiologic Responses to Decreasing Plasma Glucose Concentrations
Response Glycemic Threshold, mmol/L (mg/dL)
Physiologic Effects Role in the Prevention or Correction of Hypoglycemia (Glucose Counterregulation)
↓Insulin 4.4–4.7 (80–85) ↑Ra (↓ Rd)
Primary glucose regulatory factor/first defense against hypoglycemia
↑Glucagon 3.6–3.9 (65–70) ↑RaPrimary glucose counterregulatory factor/second defense against hypoglycemia
↑EPINEPHRINE 3.6–3.9 (65–70) ↑Ra, ↓Rc
Third defense against hypoglycemia, critical when glucagon is deficient
↑GROWTH HORMONEAND CORTISOL
3.6–3.9 (65–70) ↑Ra,↓ Rc
Involved in defense against prolonged hypoglycemia, not critical
SYMPTOMS 2.8–3.1 (50–55) Recognition of hypoglycemia
Prompt behavioral defense against hypoglycemia (food ingestion)
↓COGNITION <2.8 (<50) ------ (Compromises behavioral defense against hypoglycemia)
64

Hypoglycemia in insulin-treated patients with diabetes occurs as a consequence of three factors:
Behavioral issues
Impaired counterregulatory systems
Complications of diabetes.
65

CLINICAL FEATURES
AUTONOMIC(Neurogenic)
Sweating
Trembling
Pounding heart
Hunger
Anxiety
66

CONT’D……
Neuroglycopenic:
Confusion
Drowsiness
Speech difficulty
Inability to concentrate
Incoordination
67

CONT’D……
NON SPECIFIC:
Nausea
Tiredness
Headache
68

Approach to the Patient: Hypoglycemia
In addition to recognition and documentation of hypoglycemia, and often urgent treatment, diagnosis of the hypoglycemic mechanism is critical for choosing a treatment that prevents, or at least minimizes, recurrent hypoglycemia.
69

Recognition and Documentation
Hypoglycemia is suspected: in patients with typical symptoms; in the presence of confusion, an altered level of consciousness, or a seizure; or in a clinical setting in which hypoglycemia is known to occur.
low plasma glucose concentration.
Whipple's triad
70

When the cause of the hypoglycemic episode is obscure:
plasma insulin, C-peptide, proinsulin
As well as screening for circulating oral hypoglycemic agents, and symptoms should be assessed during and after the plasma glucose concentration is raised.
71

Diagnosis of the Hypoglycemic Mechanism
In a patient with documented hypoglycemia, a plausible hypoglycemic mechanism can often be deduced from the history, physical examination, and available laboratory data.
first consideration: Drugs, particularly those used to treat diabetes or alcohol.
Other considerations : include evidence of a relevant critical illness, less commonly hormone deficiencies, and rarely a non–beta-cell tumor that can be pursued diagnostically.
72

CONT’D……
Absent one of these mechanisms, in an otherwise seemingly well individual, one should consider endogenous hyperinsulinism and proceed with measurements and assessment of symptoms during spontaneous hypoglycemia or under conditions that might elicit hypoglycemia.
73

Urgent Treatment
Oral treatment with glucose tablets or glucose-containing fluids, candy, or food is appropriate if the patient is able and willing to take these. A reasonable initial dose is 20 g of glucose.
Intravenous glucose (25 g) should be given and followed by a glucose infusion guided by serial plasma glucose measurements.
If intravenous therapy is not practical, subcutaneous or intramuscular glucagon (1.0 mg in adults) can be used, particularly in patients with T1DM.
74
CONT’D….
These treatments raise plasma glucose concentrations only transiently,
and patients should therefore be urged to eat as soon as is practical to replete glycogen stores.
75
MEASURES FOR AVOIDANCE AND TREATMENT OF HYPOGLYCAEMIA DURING TRAVEL Carry supply of fast-acting carbohydrate (non-
perishable, in suitable containers): Screwtop plastic bottles for glucose drinks Packets of powdered glucose (for use in hot, humid climates). Confectionery (foil wrapping in hot climates).
Companions should carry additional oral carbohydrate, and glucagon .
Frequent blood glucose testing (carry spare meter; visually read strips).
Use fast-acting insulin analogues for long-distance air travel.
76

Prevention of Recurrent Hypoglycemia
Prevention of recurrent hypoglycemia requires an understanding of the hypoglycemic mechanism.
Offending drugs can be discontinued or their doses reduced.
Cortisol and growth hormone can be replaced if they are deficient.
Surgical resection of an insulinoma is curative; medical therapy with diazoxide or octreotide can be used if resection is not possible and in patients with a nontumor beta-cell disorder.
77

Cont’d………….
Surgical, radiotherapeutic,or chemotherapeutic reduction of a nonislet cell tumor can alleviate hypoglycemia even if the tumor cannot be cured; glucocorticoid or growth hormone administration also may reduce hypoglycemic episodes in such patients.
78

complications
recurrent/persistent psychosocial morbidity
Fear of hypoglycemia-barrier for diabetic control.
Seizure
permanent neurologic deficit (including cognitive impairment)
Coma
Death
79
Thank you
80

References 81
Internet sources