apheresen - roteskreuz.at · lp(a) ig antibodies diabetic foot syndrome hypercholesterolemia pure...
TRANSCRIPT

Apheresen
OA Dr. Volker Witt St. Anna Kinderspital
Wien, Österreich
Einführung in die Blutwäsche
• APHERESE: griechisch für „wegnehmen“
Sumerer 4000 Jahre v. Chr.

De Laval Cream Seperator

For centrifugation systems

The Anatomie of the Interface

Zentrifugen System
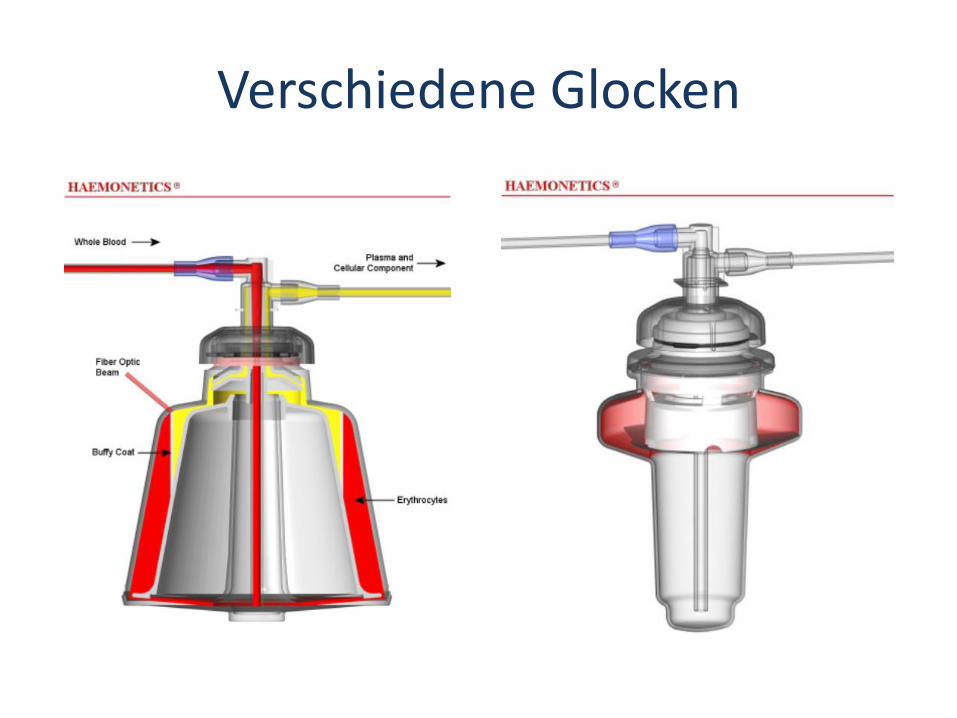
Verschiedene Glocken

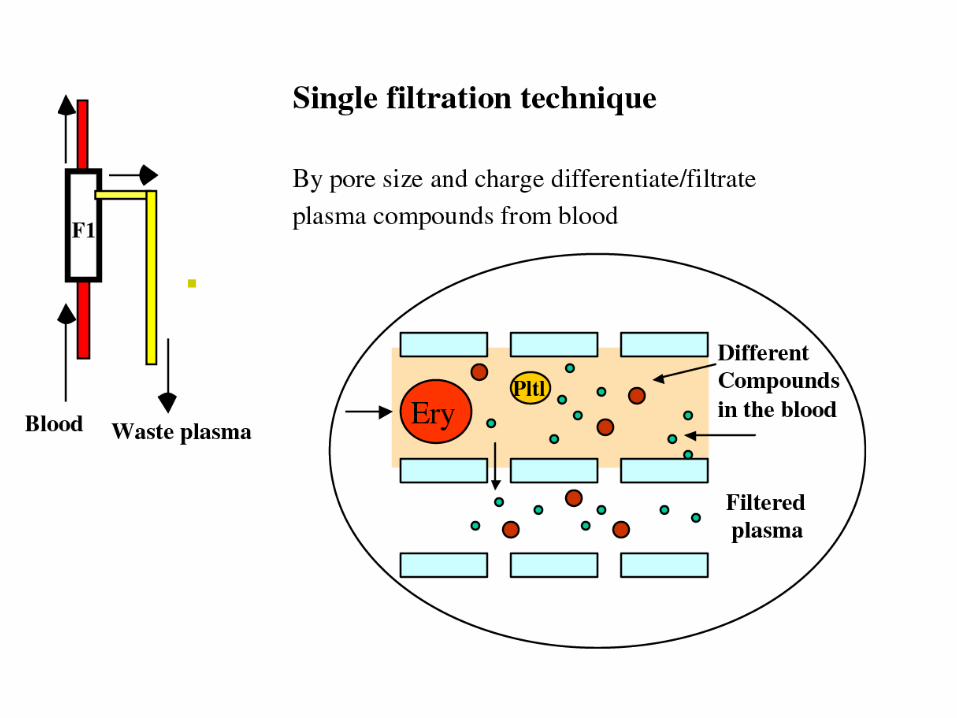
Plasmapherese Systeme (Filtration)

Discus filtration (Life18™)

Cascade filtration

Zellapheresen
Zellseparator
Patient
Plasma Rest
SPENDE
12

Blutspenden durch Apherese
• Erythrozyten – 1 EK / 2 EK
• Thrombozyten – 1 Spender bis zu 3 Präparate
• Granulozyten / Leukozyten • Plasma
– FFP – Source Plasma zur Fraktionierung
• Multikomponentenspende – EK /Plasma

Therapeutische Zellapheresen
Zellseparator
Patient
Plasma Rest
Zielzellen
14

Zellapheresen
Spende von Geweben
• Human Progenitor Cells (HPC) – Autolog
– Allogen
• Lymphozyten – Autolog
– Allogen
• Monozyten – autolog
Depletion von Zellen
• Erythroyzten – Polyzythämie
– Hämochromatose
• Thromboyzten – Hyperthrombozytose
• Leukozyten – Hyperleukozytose
• Maligne (Blasten)
• Nicht-maligne (Pertussis)

Plasmapheresen
Zellseparator
Patient
16
Rest
Spende
Zellen

Therapeutische Plasmapherese
Separator
Patient
Zellen Patient Plasma
Plasma substituted
17

Zell- und Plasmaseparatoren


Plasmapherese Systeme (Filtration)
20

GENERAL PRINCIPLE OF TPE


Replacement fluid
• Saline solution
• Human albumin
• Hydroxyethyl starc
• Fresh frozen plasma
• Risk of Hemodilution
– Anemia
– Coagulopathy
– Elektrolyte disturbance
– Dysproteinemia
• Transmission of pathogens
Allergic reactions can occure in every situation

TPE, how many times we should exchange the plasma volume?
yo = absolute initial concentration
yabs = absolute final concentration
y% = relative final concentration [%]
e = base of natural logarithms
x = number of times the patient‘s total plasma volume is exchanged
y% = e(-x)
yabs = yo * (100 - y%)
0
10
20
30
40
50
60
70
80
90
100
0 0,5 1 1,5 2 2,5 3 3,5 4
% p
ath
og
en
number of times the patient‘s total plasma volume is exchanged
Tronier W., Goodfellow E., Larson K. Apheresis Math and Useful Physical constants in Principles of Apheresis Technology, 4th edition Linz W. (editor) 2010

Alteration in Blood Constituents by a 1-Plasma-Volume Exchange
*McLeod C. Bruce Apheresis Principles and Practice 2nd edition 2003

Every second day 1 TPE with 0.5, 1, 1.5 or 2 PV treated
0
1000
2000
3000
4000
5000
6000
1 1,5 2 2,5 3 3,5
IgG
[m
g/d
l]
day
0.5 PV
1 PV
1.5 PV
2 PV
Recovery of IgG => 45% in 48 hours

Recommandation
• 1 to 2 times the Plasma volume
• Start with 2 to 3 procedures and than think about the interval if not given by treatment scedule

Therapeutische Sekundärapherese
Primärseparation
Patient
Zellen Plasma plus
Pathogen
Plasma minus
Pathogen
Sekundärseprartion
28


Immunadsorption with regenerative columns

Prediction of processed Plasma Volume needed
0,0
10,0
20,0
30,0
40,0
50,0
60,0
70,0
80,0
90,0
0 2000 4000 6000 8000 10000
Processed Plasma volume [ml]
Ig conc after %
11.5 % rest with 1350 ml treated => 1.6 x PV

„Apheresis Dose“
• TPE 1 to 1.5 to 2 times the PV
• IA 2 to 6 times the PV
• Lipid-A 2 to 6 times the PV
Time axis
START MAINTAINANCE TAPPERING

Indikationen
• Nephrologie • Rheumatologie • Kardiologie • Hämatologie • Neurologie • Intensivmedizin • Infektiologie • Stoffwechselerkrankungen • …

Target indications for TPE
and IA
Rheo Fibrinogen,
CRP
LDL Lp(a)
Ig antibodies
Diabetic Foot
Syndrome
Hypercholesterolemia
Pure Lp(a)
Solid Organ
Transplantation
Hemophilia
Pulmonary
Hypertension
Thrombangitis
(Buerger’s
disease)
Pemphigus
Dilated
Cardiomyopathy
Systemic Sclerosis
Atopic dermatitis
Peripheral
Arterial Disease
Venous leg
ulcer
Sudden
hearing loss
Neurology
Plasma Exchange
IgE
Atopic dermatitis
Allergic asthma
Severe chronic urticaria
Lupus erythematosus
ITP/TTP
Hemolytic anemia
Pulmonary hypertension Raynaud’s syndrome in SSc
Myasthenia gravis
Guillain-Barré syndrome
Lambert-Eaton syndrome
Devic’s syndrome
Multiple sclerosis
Encephalitis
CIPD
HUS
Sjögren’s syndrome
Wegener’s granulomatosis
Goodpasture’s syndrome
Kidney
Heart
Lung
Liver
Intestine
34

Tandem Model St. Anna Kinderspital
35

Tandem Model St. Anna Kinderspital
36

Tandem Model St. Anna Kinderspital
dialysis
apheresis
37

EXTRACORPORALE PHOTOPHERESE
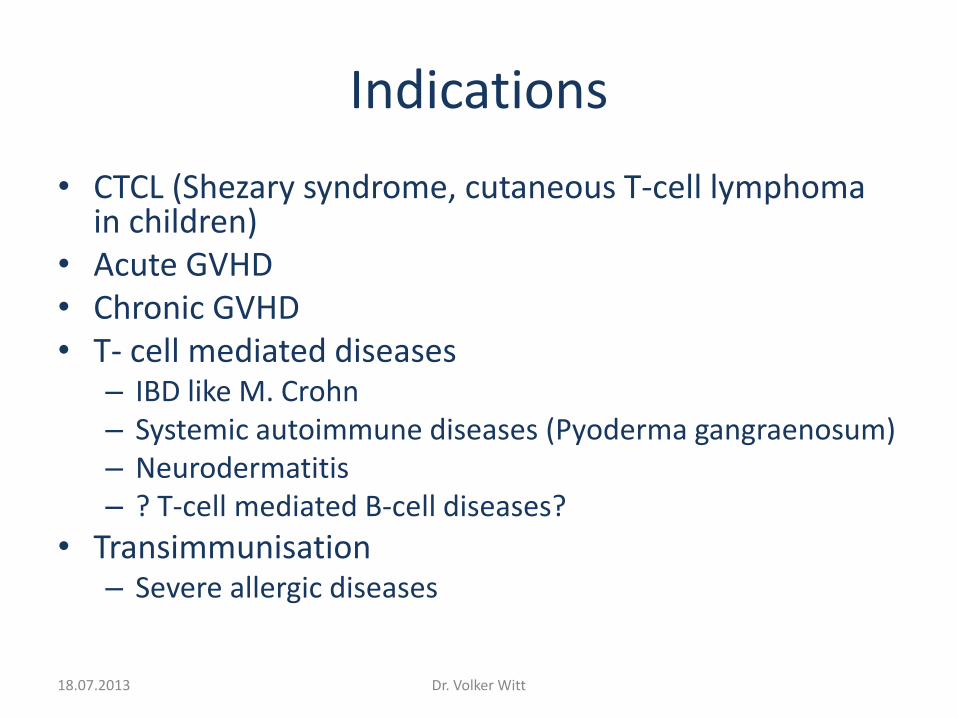
Indications
• CTCL (Shezary syndrome, cutaneous T-cell lymphoma in children)
• Acute GVHD • Chronic GVHD • T- cell mediated diseases
– IBD like M. Crohn – Systemic autoimmune diseases (Pyoderma gangraenosum) – Neurodermatitis – ? T-cell mediated B-cell diseases?
• Transimmunisation – Severe allergic diseases
18.07.2013 Dr. Volker Witt

Mechanism of Action of ECP
8-Methoxypsoralen
UV radiation
Cross-linked DNA
Leukocytes
Apoptosis
Phagocytosis
Tolerogenic DC/APC
Tr
Tr Tr
Tr
Tr Tr
Anti-inflammatory cytokines (eg, IL-10, TGF-ß)
Treg
+
1
2 3
4
5
Deletion of T cells
Proinflammatory cytokines (eg, IL-12, IFNγ)
Stimulation T effector cells
Receptor-mediated signaling
Cordially provided by Therakos 18.07.2013 Dr. Volker Witt

18.07.2013
Photosensitizer & UVA induce apoptosis of leukocytes....
Ammi majus
• Direct induction of lymphocyte apoptosis: – Edelson et al: NEJM 1987: 316
• ECP-induced cytokine production: • Increase of inhibitory cytokines (Th2 cells): IL10, 4, TGF-beta • Decrease of pro-inflammatory cytokines (Th1 cells):
IL2, INF-y, TNF-a, IL1 • Craciun et al: Transplantation 2002:74
• Increases donor regulatory T cells: – Erin Gatza et al: Blood August 2008
• ECP modulates dendritic cell populations: – Increase in CD83+, CD86+ plasmacytoid DC2 cells
– Decrease CD80+ monocytoid DC1 cells.
• Carole Berger et al., Blood 2010 116: 4838
Dr. Volker Witt

Indications
• Front (first) line
• Second line
• Third line
• Desperated doctor does not know what to do?
18.07.2013 Dr. Volker Witt

Therapeutische Zellapheresen
Zellseparator
Patient
Plasma Restliche Zellen
ECP
43
Behandlung Zielzellen

ECP = extrcorporeal photopheresis
1
3
2
4 44

15.01.2015 45

ECP: on-line und off-line Methode
On-line (Therakos) Off-line: I° Schritt = MNC collection
Off-line: II° Schritt = 8-MOP und UV-A Bestrahlung
15.01.2015 46
All in one

ECP Programm„offline Methode 1 Apherese 2 Reinfusionen“
Tag 1 Tag 2
aufgeteilt in 2 Beutel gelagert über Nacht +4oC
15.01.2015 47

50 ml PB
densitygradient- centrifugation
8-MOP MNC
2 J/m² 365 nm
48

CP 2012
Years from Transplant HSC
OVERALL SURVIVAL - cGVHD
Responders OS 81.8%
Non responders 21.4%
Outcome Patients Deaths OS (IC: 95%) p
CR 12 2 81.8 (59.0-100) 0.049
PR/NR 15 9 21.4 (0-54.0)
Flowers ME, et al. Blood 2008;112:2667–74.

Outcome of all patients with acute, overlap and chronic GVHD
00,10,20,30,40,50,60,70,80,9
1
0 2 4 6 8 10 12
pro
ba
bili
ty o
ve
rall
su
rviv
al
Interval from date of Tx [years]
improved
not improved
0
0,1
0,2
0,3
0,4
0,5
0,6
0,7
0,8
0,9
1
0 0,5 1 1,5 2 2,5 3 3,5
pro
ba
bil
itiy
patients with acute graft versus host disease Interval first ECP => outcome
acute GVHD
0
0,1
0,2
0,3
0,4
0,5
0,6
0,7
0,8
0,9
1
0 2 4 6 8 10 12
pro
ba
bil
ity
patients with chronic graft versus host disease interval first ECP => outcome
chronic GVHD
improved
notimproved

ASFA EADV Erkrankung Erkrankungsumstände Kategorie Grad Empfehlung
Herztransplantation Abstoßungsprophylaxe
zelluläre oder wiederholte Abstoßung
II
II
2A
1B
Kutanes T-Zell-Lymphom;
Mukosis fungoides, Sezary
Syndrom
Erythrodermie
Ohne Erythrodermie
I
III
1B
2C
First line Therapie in
Erythrodermie Stadium III A und
B und IVA1 und 2
GVHD Haut (chronisch)
Haut (akut)
Nicht – Haut (akut/chronisch)
II
II
III
1B
1C
2B
aGVHD second line Therapie
cGVHD second line Therapie, in
Einzelfällen first line Therapie
(Intoleranz für SIS)
Inflammatorische
Darmerkrankungen
Morbus Crohn III 1C
Lungentransplantat-
Abstoßung
Bronchiolitis obliterans II 1C Salvage Therapie in pat.
Refraktär gegen
Calcineurininhibitoren und Pred
Nephrogene systemische
Fibrose
III 2c
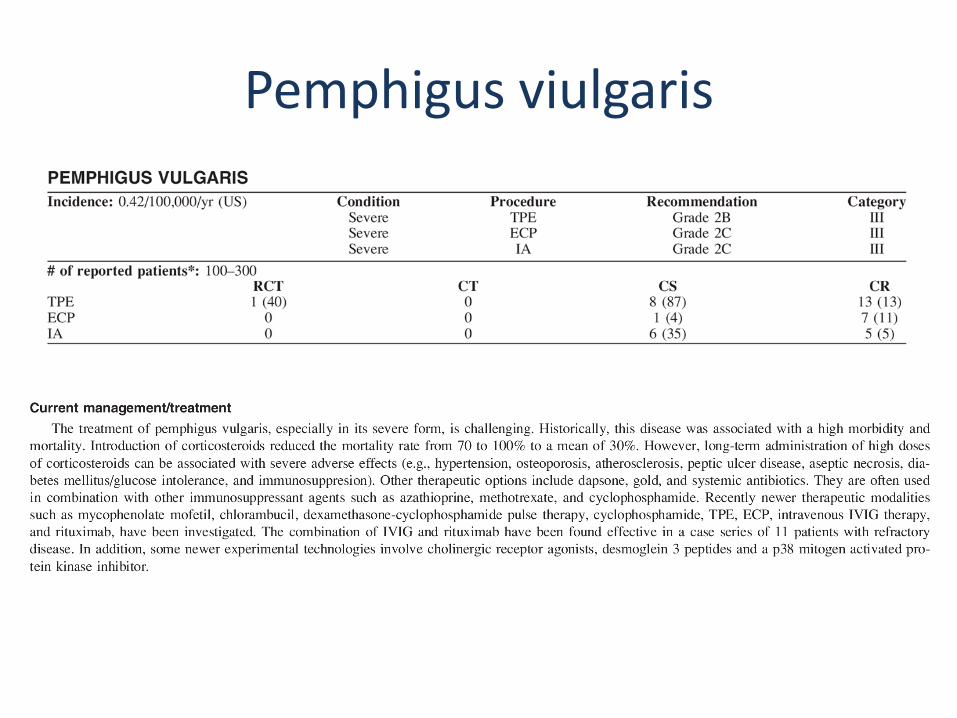
Pemphigus vulgaris Schwere Verlaufsformen III 2c Bei ungenügendem Ansprechen
auf Standardtherapie
Psoriasis III 2B Bei ungenügendem Ansprechen
auf Standardtherapie
Epidermolysis bullosa
acquisita, erociver oraler
Lichen planus
Bei ungenügendem Ansprechen
auf Standardtherapie
Sklerodermie III 2B Second-line Therapie bei Haut,
aber nicht bei Organbefall
Atopische Dermatitis Second line Therapie bei > 12
Monate Dauer und Refraktärität
gegen konventionelle Therapie

RCA
06.06.2013 ÖGBT 2013 52

Erythrozytapherese
Zellseparator
Patient
Plasma pathologische Erythrozyten
frische Erythrozyten



►Infarctive crisis => stroke
►Acute chest syndrome
►Priapism
►Retinal infarction
►Hepatopathy
indications for red cell exchange in HbSS

course of HbS
HbS [% total Hb]
0
10
20
30
40
50
60
70
80
25.0
1.2
002
25.0
4.2
002
25.0
7.2
002
25.1
0.2
002
25.0
1.2
003
25.0
4.2
003
25.0
7.2
003
25.1
0.2
003
25.0
1.2
004
25.0
4.2
004
25.0
7.2
004
25.1
0.2
004
25.0
1.2
005
HbS
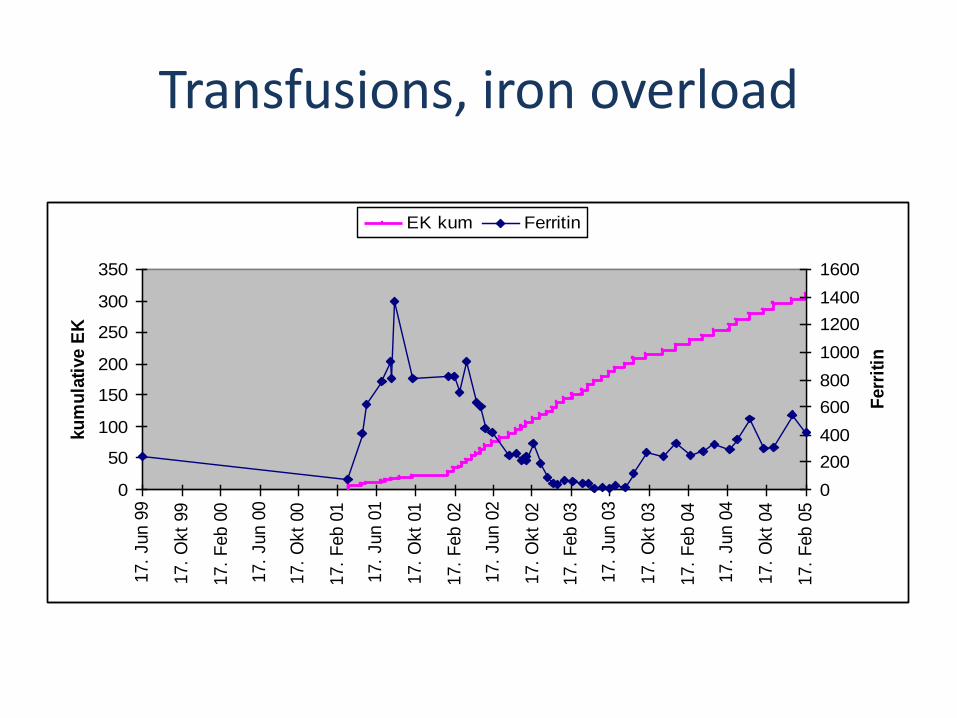
Transfusions, iron overload
0
50
100
150
200
250
300
350
17.
Jun 9
9
17.
Okt
99
17.
Feb 0
0
17.
Jun 0
0
17.
Okt
00
17.
Feb 0
1
17.
Jun 0
1
17.
Okt
01
17.
Feb 0
2
17.
Jun 0
2
17.
Okt
02
17.
Feb 0
3
17.
Jun 0
3
17.
Okt
03
17.
Feb 0
4
17.
Jun 0
4
17.
Okt
04
17.
Feb 0
5
ku
mu
lati
ve E
K
0
200
400
600
800
1000
1200
1400
1600
Ferr
itin
EK kum Ferritin

Plasmodium falciparum


„Evidence based“ therapeutische Apheresen
• Krankmachende Substanz
• Sinnvolle Entfernung
• Klinischer Nutzen

In addition to the strength of the indication, the risk/benefit assessment for TPE must take account of the patient’s ability to tolerate the procedure.

The use of therapeutic apheresis in pediatrics is limited by the lack of universally accepted indications in this patient group and by technical challenges in small subjects, …

… The decision to treat pediatric disease with apheresis is often based on conclusions extrapolated from adult patients; …

Data from the 2003-2007 World Apheresis Registry showed that of a total of 12,448 procedures in 2013 patients, only 612 procedures were performed in 135 patients under 22 years of age.1 Furthermore, only 308 procedures were done in children younger than 16 years old, representing only 2.5% of the total.

WAA regsitry data from 2003 until 2015 n => 54,383 procedures in7,142 patients
168 399
688
1083
1823
2218
2579
3480
4280 4519
5738
6600 6668
6180
4194
2172
1101
399 94
0
1000
2000
3000
4000
5000
6000
7000
0 10 20 30 40 50 60 70 80 90 100
Freq
uen
cy
age
WAA registry data, unpublished


„young“ (< 20 years old) 2269 procedures in 490 patients= 4.2%
168 399
688
1083
1823
2218
2579
3480
4280 4519
5738
6600 6668
6180
4194
2172
1101
399 94
0
1000
2000
3000
4000
5000
6000
7000
0 10 20 30 40 50 60 70 80 90 100
Freq
uen
cy
age
WAA registry data, unpublished

„elderly“ > 65 years old 14140 procedures in 2285 patients = 26 %
168 399
688
1083
1823
2218
2579
3480
4280 4519
5738
6600 6668
6180
4194
2172
1101
399 94
0
1000
2000
3000
4000
5000
6000
7000
0 10 20 30 40 50 60 70 80 90 100
Freq
uen
cy
age
WAA registry data, unpublished

Apheresis procedures (n=3165, 608 patients)
Leukapheresis
MNC apheresis
Donor aphereses
Erythrocyte apheresis
ECP
Leukdepletion by filtration
TPE centrif.
TPE filtrat.
Lipidapheresis
Protein A adsorber
cascade filtration
Ig adsorption
Anti A-Adsorption

Adverse events
2935 3029
148 75 82 61 0
500
1000
1500
2000
2500
3000
3500
adverse events interrupted procedures
no
yes
no answer

Side effects
N= N=
Access problems 18 Tingling 7
Hematoma 16 Hypotonia 3
Phlebitis 1 Abdominal pain 1
Technical problems 3 Nausea 4
Hemolysis 2 Vertigo 2
Chills and fever 1 Synkope 7
Flush 3 Sudoresis 1
Urticaria 31

ASFA Guidelines – An Evidence Based Approach for Clinical Applications of Therapeutic Apheresis

ASFA Guidelines - FACT Sheet Format (since 2007)
• Each disease :
- Single Page Fact Sheet
• Consistent layout &
information
• Goal is to be practical & user-friendly
Szczepiorkowski ZM et al. J Clin Apher 2007;22:96-105

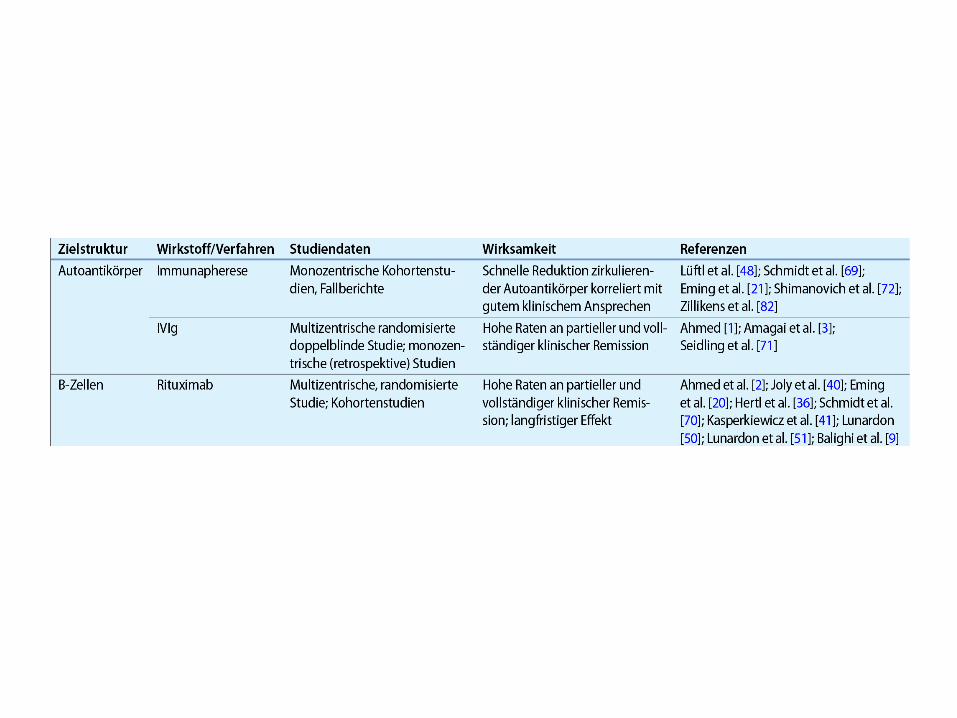
Pemphigus Modellerkrankung für zielgerichtete Therapien
R. Eming Hautarzt 2015 · 66:574–582
Schematische Darstellung möglicher therapeutischer Zielstrukturen in der Immunpathogenese des Pemphigus mit zugehörigen Substanzen/Verfahren. 1 Autoantikörper: Immunapherese und IVIg; 2 B-Zellen: Anti-CD20/CD22-Antikörper; 3 Plasmazellen: Bortezomib, Carfilzomib; 4 B-Zell-Wachstums-, Differenzierungsfaktoren bzw. zugehörige Rezeptoren: Belimumab, Atacicept; 5 Zytokine: z. B. Anti-IL4/-IL13-Antikörper; 6 kostimulatorische Rezeptoren; 7 T-Zellen: immundominante Peptide, Januskinase-Inhibitoren, Sphingosin-1-Phosphat-Analoga; 8 proinflammatorische Zytokine/Akantholyse: Anti-IL1-Antikörper; Desmoglein-homologe Tandempeptide; 9 regulatorische T-Zellen: z. B. Expansion ex vivo und Reinfusion

Pemphigus viulgaris

Thank you for your attention
Questions ?