aph
DESCRIPTION
APHTRANSCRIPT

121
SYNOPSIS
Uteroplacental haemorrhage 121Placenta praevia 121Abruptio placentae 124
Other causes of antepartum haemorrhage127Unexplained antepartum haemorrhage 127Vaginal infections 127Cervical lesions 127
Essential information 128
Haemorrhage from the vagina after the 24th week ofgestation is classified as antepartum haemorrhage. Thefactors that cause antepartum haemorrhage may bepresent before 24 weeks, but the original distinctionbetween a threatened miscarriage and an antepartumhaemorrhage was based on the potential viability of thefetus.
Vaginal bleeding may be due to:
• Haemorrhage from the placental site and uterinecavity
• Lesions of the vagina or cervix• Fetal bleeding from vasa praevia.
UTEROPLACENTAL HAEMORRHAGE
The major causes of uterine bleeding are:
• Placenta praevia• Abruptio placentae or accidental haemorrhage• Uterine rupture• Unknown aetiology.
Placenta praevia
The placenta is said to be praevia when all or part of theplacenta implants in the lower uterine segment andtherefore lies in front of the presenting part (Fig. 9.1)
Incidence
Approximately 1% of all pregnancies are complicatedby clinical evidence of a placenta praevia. Unlike theincidence of placental abruption, which varies ac-cording to social and nutritional factors, the incidenceof placenta praevia is remarkably constant.
Placenta praevia occurs more commonly in multi-parous women, in the presence of multiple pregnancyand where there has been a previous caesarean section.
Aetiology
Placenta praevia is due to delay in implantation of theblastocyst so that this occurs in the lower part of the
9 Antepartum haemorrhage
F07147-09.qxd 7/23/03 2:06 PM Page 121
uterus. It is commoner in high parity and in conditionswhere the placental area is large, such as multiplepregnancy or placenta membranacea.
Classification
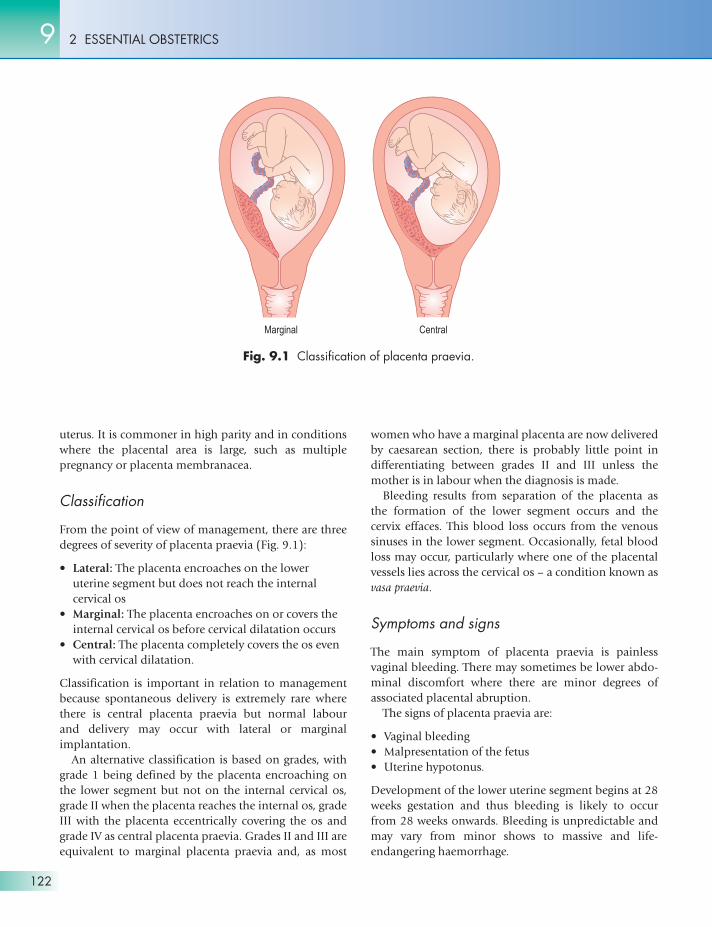
From the point of view of management, there are threedegrees of severity of placenta praevia (Fig. 9.1):
• Lateral: The placenta encroaches on the loweruterine segment but does not reach the internalcervical os
• Marginal: The placenta encroaches on or covers theinternal cervical os before cervical dilatation occurs
• Central: The placenta completely covers the os evenwith cervical dilatation.
Classification is important in relation to managementbecause spontaneous delivery is extremely rare wherethere is central placenta praevia but normal labour and delivery may occur with lateral or marginalimplantation.
An alternative classification is based on grades, withgrade 1 being defined by the placenta encroaching onthe lower segment but not on the internal cervical os,grade II when the placenta reaches the internal os, gradeIII with the placenta eccentrically covering the os andgrade IV as central placenta praevia. Grades II and III areequivalent to marginal placenta praevia and, as most
women who have a marginal placenta are now deliveredby caesarean section, there is probably little point indifferentiating between grades II and III unless themother is in labour when the diagnosis is made.
Bleeding results from separation of the placenta asthe formation of the lower segment occurs and thecervix effaces. This blood loss occurs from the venoussinuses in the lower segment. Occasionally, fetal bloodloss may occur, particularly where one of the placentalvessels lies across the cervical os – a condition known asvasa praevia.
Symptoms and signs
The main symptom of placenta praevia is painlessvaginal bleeding. There may sometimes be lower abdo-minal discomfort where there are minor degrees ofassociated placental abruption.
The signs of placenta praevia are:
• Vaginal bleeding• Malpresentation of the fetus• Uterine hypotonus.
Development of the lower uterine segment begins at 28weeks gestation and thus bleeding is likely to occurfrom 28 weeks onwards. Bleeding is unpredictable andmay vary from minor shows to massive and life-endangering haemorrhage.
2 ESSENTIAL OBSTETRICS9
122
Fig. 9.1 Classification of placenta praevia.
F07147-09.qxd 7/23/03 2:06 PM Page 122

DiagnosisClinical findings
Painless bleeding occurs suddenly and tends to berecurrent. When labour starts and the cervix dilates,profuse haemorrhage may occur, although sometimesin a lateral placenta praevia the presenting partcompresses the placental site and bleeding is controlled.
Abdominal examination
• Displacement of the presenting part: The presenceof the placenta in the lower segment tends todisplace the presenting part and, when the placenta
is posterior, the head is pushed forward over thepelvic brim and is easily palpable. When the placentais anterior, the presenting part is difficult to feel.Lateral placement of the placenta results incontralateral displacement of the presenting part.Where there is a central placenta praevia, the fetalhead is held away from the pelvic brim and the liemay be transverse or oblique. If the head does notapproach the pelvic brim when the placenta isanterior, the presenting part is difficult to palpate.
• Flaccidity of the uterus: Uterine muscle tone isusually low and the fetal parts are easy to palpate.
Diagnostic procedures
• Ultrasound scanning: This is predominantly used tolocalize the placenta and has largely replaced othertechniques. Errors in diagnosis are most likely tooccur in posteriorly situated placentae because ofdifficulties in identifying the lower segment.Anteriorly, the bladder provides an importantlandmark for the lower segment and diagnosis ismore accurate. Localization of the placental site inearly pregnancy may result in inaccurate diagnosis,as fundal development may lead to an apparentupward displacement of the placenta.
• Magnetic resonance imaging: This is the mostaccurate method of placental localization becausethe internal cervical os can be clearly visualized.However, it is not as yet widely available or used andwould only be relevant if the ultrasound image wasinconclusive.
Management
When antepartum haemorrhage of any type occurs, thediagnosis of placenta praevia should be suspected andhospital admission advised. The diagnosis should beestablished by ultrasound imaging. Vaginal examina-tion should be performed only in an operating theatreprepared for caesarean section, with blood cross-matched. There are only two indications for performinga vaginal examination:
• When there is serious doubt about the diagnosis• When bleeding occurs in established labour.
It is, in fact, often difficult to establish a diagnosis ofplacentae praevia by vaginal examination where theplacenta is lateral, and there is a serious risk of preci-pitating massive haemorrhage if the placenta is central.
9ANTEPARTUM HAEMORRHAGE
123
Case studyPlacenta praevia
Janet Y was admitted to hospital at 28 weeksgestation with a substantial painless vaginalhaemorrhage in her first pregnancy. Thepresenting part was high but central and theuterine tone was soft. A diagnosis of placentapraevia was made and she was advised to stayin hospital under observation until delivery. Therewas no further bleeding and, at 32 weeksgestation, she asked to go home to marry herpartner. As this necessitated a 1 hour flight, shewas strongly advised against this action so herpartner flew to Janet instead and the weddingwas arranged in a church close to the hospital.At the wedding, Janet had a further substantialbleed as she walked down the aisle and wasrushed back into hospital. The bleeding againsubsided but, at 35 weeks gestation, Janet had amassive haemorrhage in the ward to the extentthat blood soaked her bed linen and flowed overthe side of the bed. The resident staff insertedtwo intravenous lines and she was rushed totheatre. She was shocked and hypotensive and itwas extremely difficult to maintain her bloodpressure. A ‘crash section’ was performed andthe diagnosis of central placenta praevia wasconfirmed. A healthy male infant was delivered.Had Janet been at home, it is very unlikely thatshe would have survived.
F07147-09.qxd 7/23/03 2:06 PM Page 123

If the placenta is lateral, then it may be possible torupture the membranes and allow spontaneous vaginaldelivery.
Conservative management of placenta praevia in-volves keeping the mother in hospital with blood cross-matched until fetal maturity is adequate, and thendelivering the child by caesarean section. Providingthere is no active bleeding, there is no need to keep themother in bed and she should remain ambulant, as sheis as likely to bleed lying supine. Blood loss should betreated by transfusion where necessary so that anadequate haemoglobin concentration is maintained.
Postpartum haemorrhage is also a hazard of the low-lying placenta, as contraction of the lower segment isless effective than contraction of the upper segment.
There is an increased risk of placenta accreta whereplacental implantation occurs over the site of a previousuterine scar.
Out of 7.5 million pregnancies in the USA, the inci-dence of placental abruption has been recorded as6.5/1000 births with a perinatal mortality of 119/1000births.
The incidence of placental abruption is increased inthe presence of pre-eclampsia or essential hypertension.It must be remembered that hypertension and protein-uria may develop as a result of abruption.
Whatever factors predispose to placental abruption,they are well-established before the abruption occurs.The fetus is more likely to be male and the birthweightis often low, indicating pre-existing growth retardation.A history of a placental abruption in a previous preg-nancy is a predictor for a further abruption. The prog-nosis for fetal survival is significantly worse in thosewomen who smoke cigarettes during pregnancy. Traumais a relatively uncommon cause of abruption and in the
2 ESSENTIAL OBSTETRICS9
124
Placenta praevia accreta is one of the most lethalconditions in obstetrics. It commonly occurswhere the placenta is implanted over a previoussection scar. The trophoblast grows into the scartissue, making it almost impossible to separatethe placenta from the uterine wall and, as aconsequence, massive bleeding may occur. Theonly way this bleeding can be controlled is byhysterectomy. The condition carries a highmortality rate. The important management issueis to be prepared. Caesarean section associatedwith anterior implantation of a placenta praeviaand a previous section scar should be performedby an experienced obstetric surgeon with amplesupplies of blood on standby.
!
Abruptio placentae
Abruptio placentae or accidental haemorrhage is de-fined as haemorrhage resulting from premature separa-tion of the placenta. The term ‘accidental’ impliesseparation as the result of trauma, but most cases do notinvolve trauma and occur spontaneously.
Aetiology
Placental abruption tends to occur more frequentlyunder conditions of social deprivation in associationwith dietary deficiencies. Folic acid deficiency, inparticular, has been implicated.
Case studyAbruptio placentae
Mandy, a 23-year-old primigravida, wasadmitted to hospital at 35 weeks gestation with acomplaint that she had developed severeabdominal pain followed by substantial vaginalbleeding. On examination, she was restless andin obvious pain. Her blood pressure was150/90 and the uterus was rigid and tender.Her pulse rate was 100 bpm and she lookedpale and tense. The uterine fundus was palpableat the level of the xiphisternum. The fetal lie waslongitudinal, with the head presenting. The fetalheart beat could not be detected. An intravenousline was established and blood cross-matched asa matter of urgency. Mandy was given painrelief and her blood picture and clotting profilewere examined. Vaginal examination showedthat the cervix was effaced and 3 cm dilated andthe membranes were bulging through the os. Aforewater rupture was performed and blood-stained amniotic fluid was released. Labourensued and Mandy was delivered 3 hours laterof a stillborn male infant. A large amount of clotwas delivered with the placenta, and some 50%of the placenta appeared to have been avulsedfrom the uterine wall.
F07147-09.qxd 7/23/03 2:06 PM Page 124
majority of cases no specific predisposing factor can beidentified for a particular episode.
Clinical types and presentation
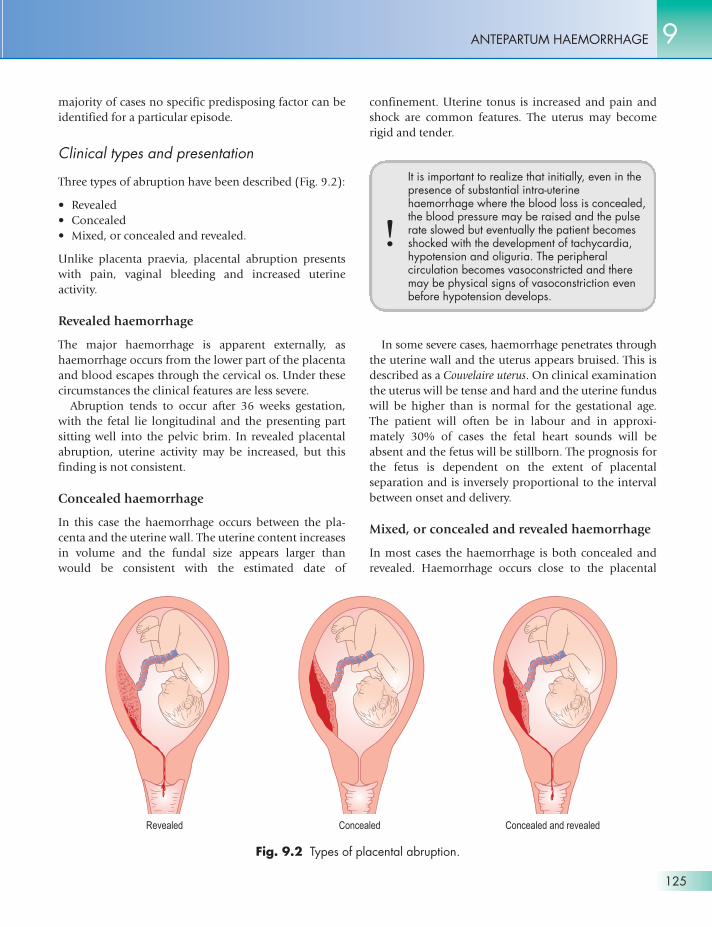
Three types of abruption have been described (Fig. 9.2):
• Revealed• Concealed• Mixed, or concealed and revealed.
Unlike placenta praevia, placental abruption presentswith pain, vaginal bleeding and increased uterineactivity.
Revealed haemorrhage
The major haemorrhage is apparent externally, ashaemorrhage occurs from the lower part of the placentaand blood escapes through the cervical os. Under thesecircumstances the clinical features are less severe.
Abruption tends to occur after 36 weeks gestation,with the fetal lie longitudinal and the presenting partsitting well into the pelvic brim. In revealed placentalabruption, uterine activity may be increased, but thisfinding is not consistent.
Concealed haemorrhage
In this case the haemorrhage occurs between the pla-centa and the uterine wall. The uterine content increasesin volume and the fundal size appears larger thanwould be consistent with the estimated date of
confinement. Uterine tonus is increased and pain andshock are common features. The uterus may becomerigid and tender.
9ANTEPARTUM HAEMORRHAGE
125
Fig. 9.2 Types of placental abruption.
It is important to realize that initially, even in thepresence of substantial intra-uterinehaemorrhage where the blood loss is concealed,the blood pressure may be raised and the pulserate slowed but eventually the patient becomesshocked with the development of tachycardia,hypotension and oliguria. The peripheralcirculation becomes vasoconstricted and theremay be physical signs of vasoconstriction evenbefore hypotension develops.
!
In some severe cases, haemorrhage penetrates throughthe uterine wall and the uterus appears bruised. This isdescribed as a Couvelaire uterus. On clinical examinationthe uterus will be tense and hard and the uterine funduswill be higher than is normal for the gestational age.The patient will often be in labour and in approxi-mately 30% of cases the fetal heart sounds will beabsent and the fetus will be stillborn. The prognosis forthe fetus is dependent on the extent of placentalseparation and is inversely proportional to the intervalbetween onset and delivery.
Mixed, or concealed and revealed haemorrhage
In most cases the haemorrhage is both concealed andrevealed. Haemorrhage occurs close to the placental
F07147-09.qxd 7/23/03 2:06 PM Page 125
edge and, after an interval when the haemorrhage isconcealed, blood loss soon appears vaginally.
Differential diagnosis
The diagnosis is made on the history of vaginalbleeding, abdominal pain, increased uterine tonus,proteinuria and the presence of a longitudinal lie. Thismust be distinguished from placenta praevia, where thehaemorrhage is painless, the lie unstable and the uterushypotonic. Occasionally, some manifestations ofplacental abruption may arise where there is a low-lyingplacenta. In other words, placental abruption can arisewhere there is low placental implantation and, on theseoccasions, the diagnosis can only really be clarified byultrasound location of the placenta.
The diagnosis should also be differentiated fromother acute emergencies such as acute hydramnios,where the uterus is enlarged, tender and tense but thereis no haemorrhage. Other acute abdominal emergenciessuch as perforated ulcer, volvulus of the bowel andstrangulated inguinal hernia may simulate concealedplacental abruption, but these problems are rare duringpregnancy.
Management
The patient must be admitted to hospital and thediagnosis established on the basis of the history andexamination findings (Fig. 9.3). Mild cases may betreated conservatively and the placental site localized toconfirm the diagnosis. If the haemorrhage is severe,resuscitation is the first prerequisite.
It is often difficult to assess the amount of blood lossaccurately and intravenous infusion should be startedwith normal saline, Hartmann’s solution or blood sub-stitutes until blood is cross-matched and transfusioncan be commenced. Fluid replacement should be moni-tored by the use of a central venous pressure line.Unlike placenta praevia, any significant abruptionshould be treated by delivering the fetus as soon aspossible.
If the fetus is alive and there are no clinical signs offetal distress, or if the fetus is dead, surgical induction oflabour is performed as soon as possible and, wherenecessary, uterine activity is stimulated with a diluteSyntocinon infusion. If the fetus is alive, it should bemonitored and caesarean section should be performedif signs of fetal distress develop. If induction is notpossible because the cervix is closed, then delivery
should be effected by caesarean section. Pain relief isachieved by the use of opiates. Epidural anaesthesiashould not be used until a clotting screen is available.
Complications
The complications of placental abruption are summa-rized in Figure 9.4.
Afibrinogenaemia
In afibrinogenaemia, severe placental abruption resultsin significant placental damage and the release ofthromboplastin into the maternal circulation. This inturn may lead to intravascular coagulation and todefibrination, with the development of hypo- andafibrinogenaemia. The condition may be treated by theinfusion of fresh frozen plasma, platelet transfusionand fibrinogen transfusion but can only be reversed bydelivering the fetus. It may lead to abnormal bleeding ifoperative delivery is attempted or may result in
2 ESSENTIAL OBSTETRICS9
126
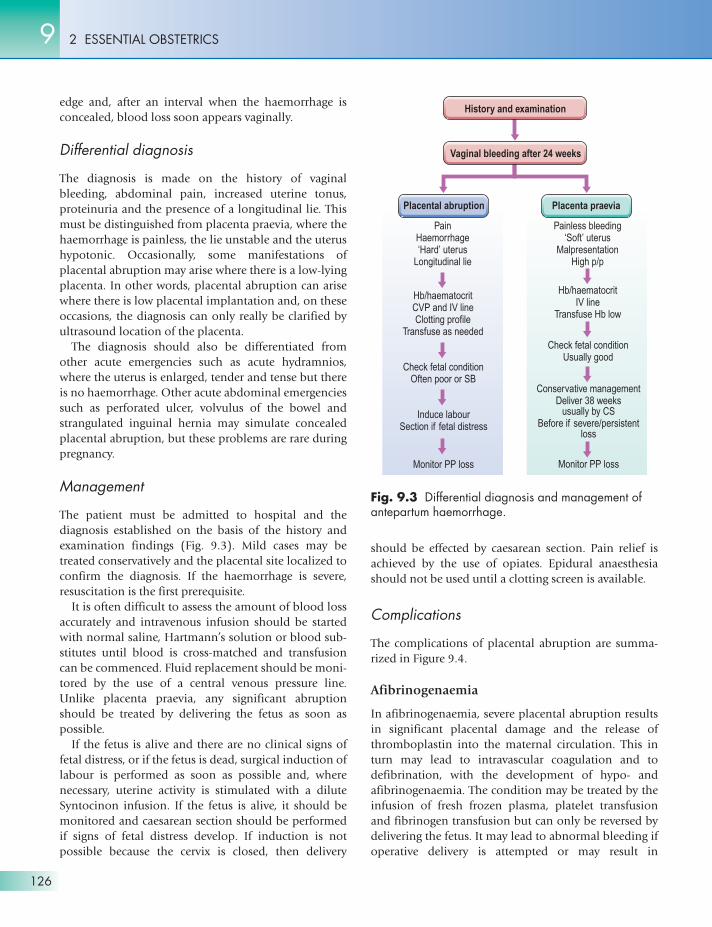
Fig. 9.3 Differential diagnosis and management ofantepartum haemorrhage.
History and examination
Vaginal bleeding after 24 weeks
Placental abruption Placenta praevia
Painless bleeding‘Soft’ uterus
MalpresentationHigh p/p
Hb/haematocritIV line
Transfuse Hb low
Check fetal conditionUsually good
Conservative managementDeliver 38 weeks
usually by CSBefore if severe/persistent
loss
Monitor PP loss
PainHaemorrhage‘Hard’ uterus
Longitudinal lie
Hb/haematocritCVP and IV lineClotting profile
Transfuse as needed
Check fetal conditionOften poor or SB
Induce labourSection if fetal distress
Monitor PP loss
F07147-09.qxd 7/23/03 2:06 PM Page 126

uncontrollable postpartum haemorrhage unless theclotting defect has been corrected.
Renal tubular or cortical necrosis
This is a complication that must always be considered asa possibility and it is essential to keep careful fluidbalance charts and to take particular note of urinaryoutput. This complication may, on occasion, necessitatehaemodialysis or peritoneal dialysis, but it is becomingincreasingly rare.
OTHER CAUSES OF ANTEPARTUMHAEMORRHAGE
These are summarized in Figure 9.5.
Unexplained antepartumhaemorrhage
In many cases, it is not possible to make a definitediagnosis of abruption or placenta praevia.
These cases involve a significant increase in perinatalmortality and it is therefore important to monitorplacental function and fetal growth. The pregnancyshould not be allowed to proceed beyond term.
Rarely, the bleeding may be fetal in origin and arisesfrom the rupture of an aberrant placental vessel knownas a vasa praevia. The only way that this can be diag-nosed is by detecting the presence of fetal haemoglobinin the vaginal blood loss.
Vaginal infections
Vaginal moniliasis or trichomoniasis may cause blood-stained discharge and, once the diagnosis is established,should be treated with the appropriate therapy.
Cervical lesions
Benign lesions of the cervix such as cervical polyps aretreated by removal of the polyp. Cervical erosions arebest left untreated.
Carcinoma of the cervix is occasionally found inpregnancy. If the pregnancy is early, termination isindicated. If the diagnosis is made late in pregnancy, thediagnosis should be established by biopsy and thelesion treated according to the staging.
9ANTEPARTUM HAEMORRHAGE
127
Fig. 9.4 Complications of placental abruption. CVP,central venous pressure; PPH, postpartumhaemorrhage.
Fig. 9.5 Non-placental causes of antepartumhaemorrhage.
F07147-09.qxd 7/23/03 2:06 PM Page 127

• Vaginal bleeding after 24 weeks.
Placenta praevia
• Lower segment implantation• Incidence 1%• Classification – marginal, central and lateral.• Diagnosis – painless loss, unstable lie, soft uterus.• Diagnosis confirmed by ultrasound or MRI• Management – conservative until 37 weeks• Hospital admission for all major degrees• Blood held – cross-matched• Caesarean section unless marginal• Prognosis for the fetus – good.
Placental abruption
• Incidence 0.5–1.0%• Diagnosis – uterus hypertonic• Normal fetal lie• Commonly associated with maternal hypertension• Management – replace blood loss• Check for DIC• Deliver the infant if abruption severe• Prognosis for fetus poor• Maternal complications• Afibrinogenaemia• Renal tubular necrosis• Scar dehiscence and uterine rupture
Unexplained causes
• Cervical and vaginal lesions• Vasa praevia
2 ESSENTIAL OBSTETRICS9
128
ESSENTIAL INFORMATION
F07147-09.qxd 7/23/03 2:06 PM Page 128