acute generalized exanthematous pustulosis induced by ingestion of bamifylline
TRANSCRIPT
634
© 2002 European Academy of Dermatology and Venereology
CAS E REPO R T
JEADV
(2002)
16
, 634–637
Blackwell Science, Ltd
Acute generalized exanthematous pustulosis induced by ingestion of bamifylline
C
Galvão,†
RFJ
Criado,†
PR
Criado,‡*
NYS
Valente,‡ JF
de Mello,†
MFM
Fernandes†
†
Allergy and Immunology Unit,
‡
Dermatology Unit, Hospital do Servidor Público Estadual de São Paulo, Brazil.
*
Corresponding author, Rua Xingú,
245/182, Bairro Valparaíso, Santo André, São Paulo, 09060-050, Brazil, tel./fax +55 11 50888293; E-mail: [email protected]
ABSTRACT
We report a case of acute generalized exanthematous pustulosis (AGEP) in a 64-year-old woman, associatedwith the use of bamifylline. To the best of our knowledge there have been no previous reports of AGEPinduced by the ingestion of bamifylline in the medical literature. We, therefore, add this drug to the list ofcauses for AGEP.
Key words:
acute generalized exanthematous pustulosis, bamifylline, neutrophilic drug eruptions
Received: 11 December 2001, accepted 15 February 2002
Introduction
Acute generalized exanthematous pustulosis (AGEP) is charac-
terized by a widespread sterile pustular rash occurring suddenly,
accompanied by fever and neutrophilia on scarlatiniform
erythema.
1,2
AGEP is a potentially severe disease caused by drug
intake in about 80% of cases,
3
particularly by antibiotics, and
also by mercurial antiseptics,
1
topical bufexamac,
1
ingestion
of lacquer chicken,
2
ultraviolet light exposure and viral infections.
4
The patch test is an elegant alternative to prove the causative
role of a suspect drug,
5
but it is performed rarely in AGEP and
most of it reproduces eczematiform lesions.
6
Oral rechallenge is
not ethical because it may provoke a generalized eruption, even
at a low dose.
5
We describe a case of AGEP provoked by bamifylline, an
bronchodilator derivative of theophylline, formerly named 8-
benzyl-7-[2-(
N
-ethyl-
N
-2 hydroxyethyamino) ethyl] theophyl-
line, with longer mean elimination half-life (20.5 h) and high
estimated potency.
7
Case report
A 64-year-old white woman was admitted with a febrile erup-
tion (38.5
°
C) of acute onset. Three days before the admission,
the patient initiated treatment with bamifylline for asthma con-
trol and noticed that 12 h after taking one tablet of the medication,
a cutaneous rash suddenly began. She did not have a past history
of personal or family psoriasis or contact dermatitis. Clinical
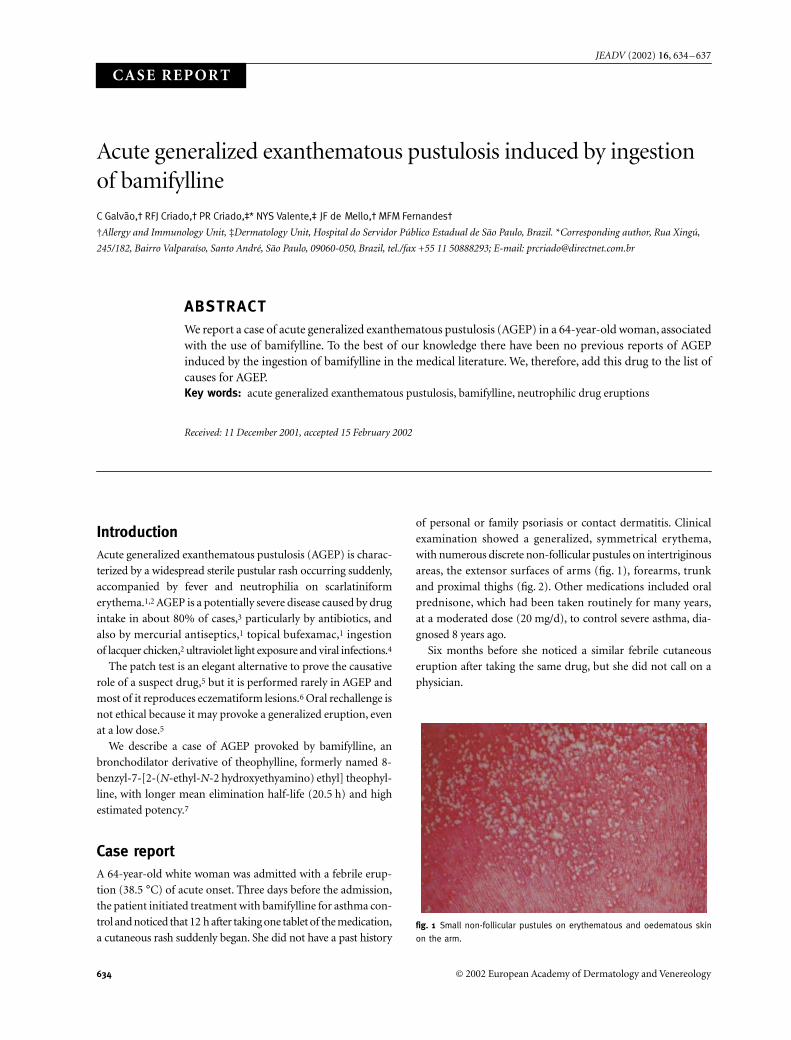
examination showed a generalized, symmetrical erythema,
with numerous discrete non-follicular pustules on intertriginous
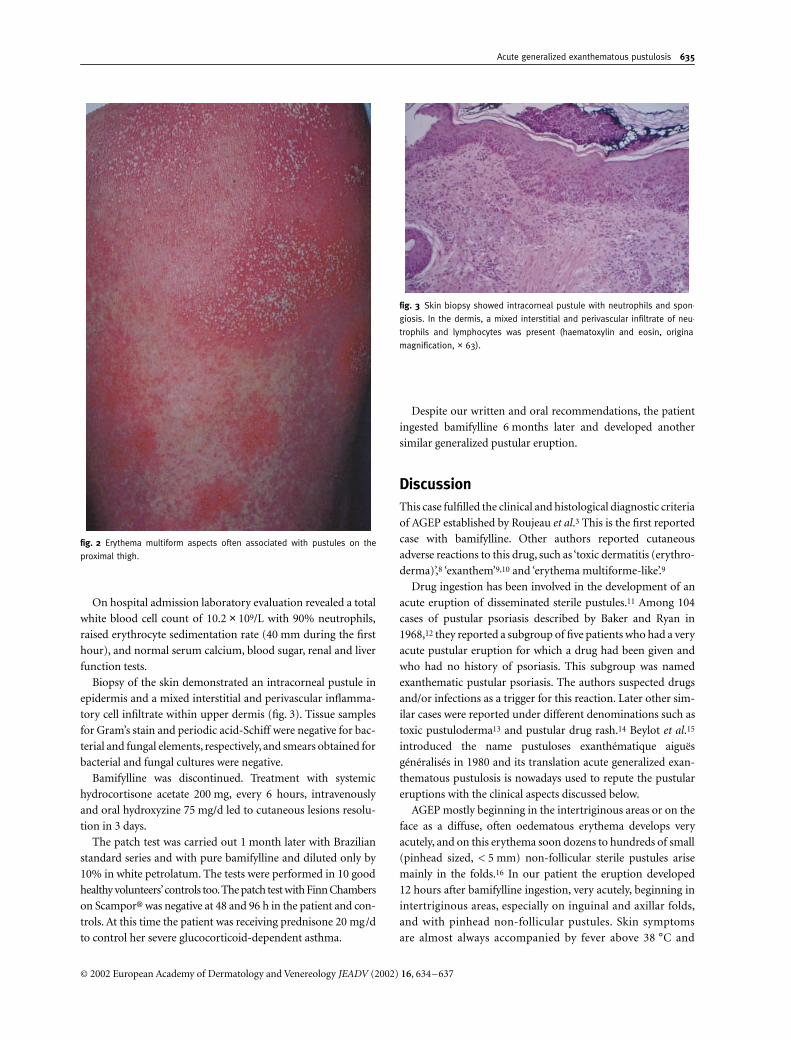
areas, the extensor surfaces of arms (fig. 1), forearms, trunk
and proximal thighs (fig. 2). Other medications included oral
prednisone, which had been taken routinely for many years,
at a moderated dose (20 mg/d), to control severe asthma, dia-
gnosed 8 years ago.
Six months before she noticed a similar febrile cutaneous
eruption after taking the same drug, but she did not call on a
physician.
fig. 1 Small non-follicular pustules on erythematous and oedematous skin
on the arm.
JDV_518.fm Page 634 Friday, October 25, 2002 8:58 PM
Acute generalized exanthematous pustulosis
635
© 2002 European Academy of Dermatology and Venereology
JEADV
(2002)
16
, 634–637
On hospital admission laboratory evaluation revealed a total
white blood cell count of 10.2
×
10
9
/L with 90% neutrophils,
raised erythrocyte sedimentation rate (40 mm during the first
hour), and normal serum calcium, blood sugar, renal and liver
function tests.
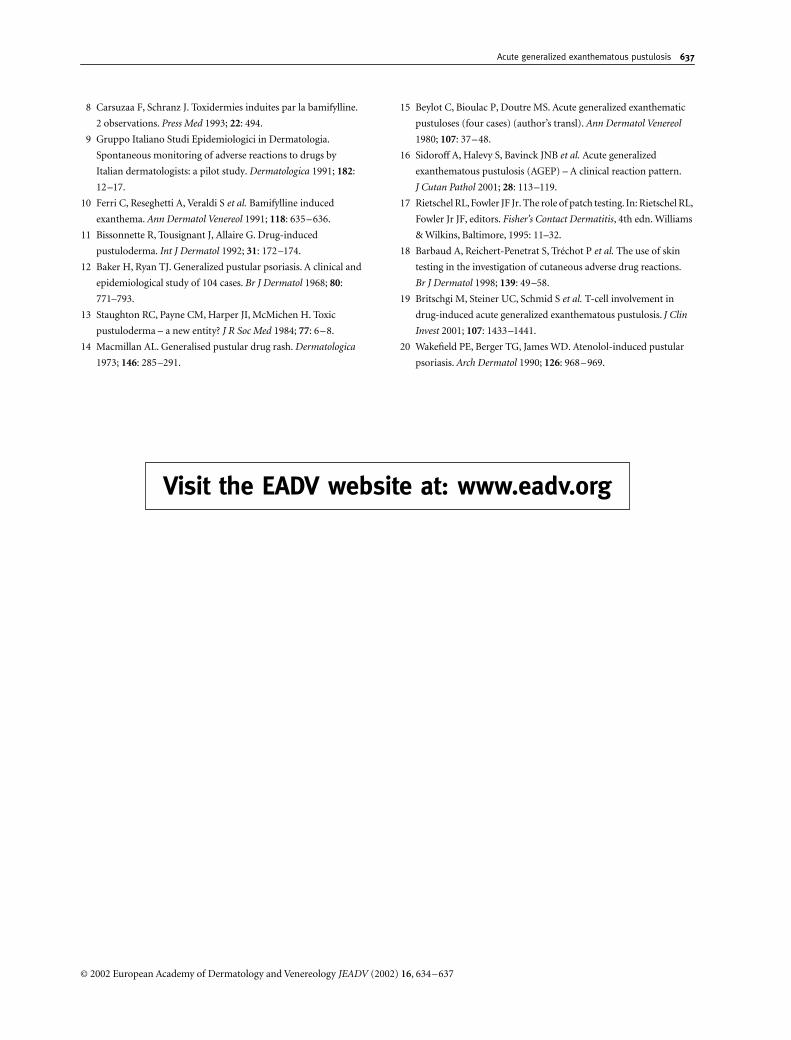
Biopsy of the skin demonstrated an intracorneal pustule in
epidermis and a mixed interstitial and perivascular inflamma-
tory cell infiltrate within upper dermis (fig. 3). Tissue samples
for Gram’s stain and periodic acid-Schiff were negative for bac-
terial and fungal elements, respectively, and smears obtained for
bacterial and fungal cultures were negative.
Bamifylline was discontinued. Treatment with systemic
hydrocortisone acetate 200 mg, every 6 hours, intravenously
and oral hydroxyzine 75 mg/d led to cutaneous lesions resolu-
tion in 3 days.
The patch test was carried out 1 month later with Brazilian
standard series and with pure bamifylline and diluted only by
10% in white petrolatum. The tests were performed in 10 good
healthy volunteers’ controls too. The patch test with Finn Chambers
on Scampor® was negative at 48 and 96 h in the patient and con-
trols. At this time the patient was receiving prednisone 20 mg/d
to control her severe glucocorticoid-dependent asthma.
Despite our written and oral recommendations, the patient
ingested bamifylline 6 months later and developed another
similar generalized pustular eruption.
Discussion
This case fulfilled the clinical and histological diagnostic criteria
of AGEP established by Roujeau
et al
.
3
This is the first reported
case with bamifylline. Other authors reported cutaneous
adverse reactions to this drug, such as ‘toxic dermatitis (erythro-
derma)’,
8
‘exanthem’
9,10
and ‘erythema multiforme-like’.
9
Drug ingestion has been involved in the development of an
acute eruption of disseminated sterile pustules.
11
Among 104
cases of pustular psoriasis described by Baker and Ryan in
1968,
12
they reported a subgroup of five patients who had a very
acute pustular eruption for which a drug had been given and
who had no history of psoriasis. This subgroup was named
exanthematic pustular psoriasis. The authors suspected drugs
and/or infections as a trigger for this reaction. Later other sim-
ilar cases were reported under different denominations such as
toxic pustuloderma
13
and pustular drug rash.
14
Beylot
et al
.
15
introduced the name pustuloses exanthématique aiguës
généralisés in 1980 and its translation acute generalized exan-
thematous pustulosis is nowadays used to repute the pustular
eruptions with the clinical aspects discussed below.
AGEP mostly beginning in the intertriginous areas or on the
face as a diffuse, often oedematous erythema develops very
acutely, and on this erythema soon dozens to hundreds of small
(pinhead sized, < 5 mm) non-follicular sterile pustules arise
mainly in the folds.
16
In our patient the eruption developed
12 hours after bamifylline ingestion, very acutely, beginning in
intertriginous areas, especially on inguinal and axillar folds,
and with pinhead non-follicular pustules. Skin symptoms
are almost always accompanied by fever above 38
°
C and
fig. 2 Erythema multiform aspects often associated with pustules on the
proximal thigh.
fig. 3 Skin biopsy showed intracorneal pustule with neutrophils and spon-
giosis. In the dermis, a mixed interstitial and perivascular infiltrate of neu-
trophils and lymphocytes was present (haematoxylin and eosin, original
magnification, × 63).
JDV_518.fm Page 635 Friday, October 25, 2002 8:58 PM

636
Galvão
et al.
© 2002 European Academy of Dermatology and Venereology
JEADV
(2002)
16
, 634–637
leucocytosis mostly due to neutrophil counts above 7
×
10
9
/L.
16
The fever (38.5
°
C) and the blood neutrophil counts (9180/mm
3
)
combined with hundreds of small non-follicular sterile pustules
led to the diagnosis of AGEP. Lymphadenopathy has been
reported in some cases, slight reduction of the creatinine clear-
ance (< 60 mL/min in
≈
30% of the cases) and a mild elevation
of aminotransferases.
16
The histopathology of AGEP shows spongiform, subcorneal
and/or intraepidermal pustules, an often-marked oedema of
the papillary dermis and perivascular infiltrates of neutrophils
and exocytosis of some eosinophils.
3,16
In our case there were
intracorneal pustules and a mixed interstitial and perivascu-
lar inflammatory cell infiltrate within the upper dermis.
Acanthosis and papillomatosis resembling psoriasis are usually
absent.
1
Some cell necroses of keratinocytes and/or vasculitis
may be present.
3,16
Patch test is a valuable tool, but its sensitivity is about 50%,
and negative tests do not allow a final conclusion.
5
The patient
was receiving prednisone, and this drug could have been inter-
fered in patch tests results; however, Rietschel and Fowler
17
noticed that patch tests could be performed even in patients
using 30 mg/d of prednisone without influencing the results.
False-negative drug patch test results can be attributable to
various causes. The drug being tested may be unable to pene-
trate into epidermis, or the culprit source of the cutaneous
adverse drug reaction was not the native drug itself but one of
its metabolites.
18
The most convincing proof that the bamifylline was probably
the causative agent is substantiated in the observation that after
the first pustular rash, she ingested bamifylline again 6 months
later by accident and in 2 days a new pustular eruption occurred.
Recently, Britschgi
et al
.
19
presented clinical and immuno-
logical data on four patients with AGEP, and demonstrated an
expression of the potent neutrophil-attracting chemokine
interleukin-8 in keratinocytes and infiltrating mononuclear
cells. The authors conclude that AGEP appears to be a reaction
where a cell-bound drug presentation elicits a drug-specific
CD4 and CD8 immune response, which results in an interleukin-
8 elevated expression.
The main differential diagnosis is acute pustular psoriasis
von Zumbusch type.
6
A wide spectrum of cutaneous diseases or
conditions can cause pustular eruptions:
16
all follicular erup-
tions, such as bacterial folliculitis, furunculosis, acne and acnei-
form reactions, dermatophyte infections, Sweet’s syndrome,
localized pustular contact dermatitis, impetiginized eczema,
subcorneal pustular dermatosis (Sneddon–Wilkinson dis-
ease), pustular vasculitis, Behçet’s disease or staphylococcal
scalded skin syndrome and others. Drug hypersensitivity syn-
drome, also referred to as DRESS (
D
rug
R
ash with
E
osinophilia
and
S
ystemic
S
ymptoms) may also show generalized papulo-
pustules being usually less pronounced than in AGEP.
16
Many authors have discussed the differentiation between
AGEP and pustular psoriasis of the von Zumbusch type. Beylot
et al
.
15
discuss the rare but possible occurrence of such a pustu-
losis in patients with a genetic psoriatic predisposition. Sidoroff
et al
.
16
suggests a list of differences that seems to justify the dis-
tinction between AGEP and pustular psoriasis. In AGEP: (i) his-
tory of psoriasis is possible; (ii) pustules predominate in the
folds; (iii) the duration of the pustules and fever is shorter;
(iv) there is a history of drug reaction and recent drug use;
(v) arthritis is rare; and (vi) no papillomatosis and acanthosis
in histopathology. In pustular psoriasis: (i) most patients have
a history of psoriasis; (ii) the distribution of the pustules is more
generalized; (iii) the duration of pustules and fever is longer;
(iv) a history of drug reaction and recent drug use are uncom-
mon; (v) arthritis occurs in approximately 30% of patients; and
(vi) the histopathology shows papillomatosis and acanthosis.
Various drugs, such as lithium and beta-blockers, have also
been reported as being able to induce the development of pus-
tular psoriasis in patients previously known to have psoriasis.
11
Some reports suggest that beta-blockers could also induce a
predominantly pustular eruption in patients with no history of
psoriasis.
20
At this moment there are no precise descriptions
of whether this latter type of eruption is a variant of pustular
psoriasis or if it is true AGEP.
The most important aspect of management of AGEP is the
immediate withdrawal of the suspect drug. It must be empha-
sized that AGEP is defined by a clinical syndrome that is most
often drug induced and we are adding a new drug (bamifylline)
to the list of causes of AGEP.
References
1 Beylot C, Doutre M-S, Beylot-Barry M. Acute generalized
exanthematous pustulosis.
Semin Cutan Med Surg
1996;
15
:
244–249.
2 Park YM, Park JG, Kang H
et al.
Acute generalized exanthematous
pustulosis induced by ingestion of lacquer chicken.
Br J Dermatol
2000;
143
: 230–232.
3 Roujeau JC, Bioulac-Sage P, Bourseau C
et al.
Acute generalized
exanthematous pustulosis: analysis of 63 cases.
Arch Dermatol
1991;
127
: 1333–1338.
4 Schawab RA, Vogel PS, Warschaw KE. Clindamycin-induced
acute generalized exanthematous pustulosis.
Cutis
2000;
65
:
391–393.
5 Machet L, Martin L, Machet MC
et al.
Acute generalized
exanthematous pustulosis induced by dextropropoxiphene and
confirmed by patch testing.
Acta Derm Venereol (Stock)
2000;
80
:
224–225.
6 Moreau A, Dompmartin A, Castel B
et al.
Drug-induced acute
generalized exanthematous pustulosis with positive patch tests.
Int
J Dermatol
1995;
34
: 263–266.
7 Weinberger M, Hendeles M. Theophylline and phosphodiesterase
inhibitors. In: Middleton Jr E, Reed CE, Ellis EF
et al.
, editors.
Allergy (Principles and Practice)
, Vol. 1, 5th edn. Mosby-Year Book
Inc., St Louis, 1998: 589–611.
JDV_518.fm Page 636 Friday, October 25, 2002 8:58 PM
Acute generalized exanthematous pustulosis
637
© 2002 European Academy of Dermatology and Venereology
JEADV
(2002)
16
, 634–637
8 Carsuzaa F, Schranz J. Toxidermies induites par la bamifylline.
2 observations.
Press Med
1993;
22
: 494.
9 Gruppo Italiano Studi Epidemiologici in Dermatologia.
Spontaneous monitoring of adverse reactions to drugs by
Italian dermatologists: a pilot study.
Dermatologica
1991;
182
:
12–17.
10 Ferri C, Reseghetti A, Veraldi S
et al.
Bamifylline induced
exanthema.
Ann Dermatol Venereol
1991;
118
: 635–636.
11 Bissonnette R, Tousignant J, Allaire G. Drug-induced
pustuloderma.
Int J Dermatol
1992;
31
: 172–174.
12 Baker H, Ryan TJ. Generalized pustular psoriasis. A clinical and
epidemiological study of 104 cases.
Br J Dermatol
1968;
80
:
771–793.
13 Staughton RC, Payne CM, Harper JI, McMichen H. Toxic
pustuloderma – a new entity?
J R Soc Med
1984;
77
: 6–8.
14 Macmillan AL. Generalised pustular drug rash.
Dermatologica
1973;
146
: 285–291.
15 Beylot C, Bioulac P, Doutre MS. Acute generalized exanthematic
pustuloses (four cases) (author’s transl).
Ann Dermatol Venereol
1980;
107
: 37–48.
16 Sidoroff A, Halevy S, Bavinck JNB
et al.
Acute generalized
exanthematous pustulosis (AGEP) – A clinical reaction pattern.
J Cutan Pathol
2001;
28
: 113–119.
17 Rietschel RL, Fowler JF Jr. The role of patch testing. In: Rietschel RL,
Fowler Jr JF, editors.
Fisher’s Contact Dermatitis
, 4th edn. Williams
& Wilkins, Baltimore, 1995: 11–32.
18 Barbaud A, Reichert-Penetrat S, Tréchot P
et al.
The use of skin
testing in the investigation of cutaneous adverse drug reactions.
Br J Dermatol
1998;
139
: 49–58.
19 Britschgi M, Steiner UC, Schmid S
et al.
T-cell involvement in
drug-induced acute generalized exanthematous pustulosis.
J Clin
Invest
2001;
107
: 1433–1441.
20 Wakefield PE, Berger TG, James WD. Atenolol-induced pustular
psoriasis.
Arch Dermatol
1990;
126
: 968–969.
Visit the EADV website at: www.eadv.org
JDV_518.fm Page 637 Friday, October 25, 2002 8:58 PM