acute generalized exanthematous pustulosis associated with pseudoephedrine
TRANSCRIPT
CASE REPORT
Acute generalized exanthematous pustulosis associatedwith pseudoephedrine
M . A . P A D I A L , J . A L V A R E Z - F E R R E I R A , * B . T A P I A , R . B L A N C O , C . M A N A S ,
M . B L A N C A † A N D T . B E L L O N
Departments of Allergy and *Pathology, Hospital Universitario �La Paz�, P �Castellana 261, 28046 Madrid, Spain
†Department of Allergy, Hospital Carlos Haya, Malaga, Spain
Accepted for publication 25 July 2003
Summary Acute generalized exanthematous pustulosis (AGEP) is an uncommon skin disorder most often
caused by drugs. Few adverse reactions to sympathomimetic drugs have been reported, despite their
extensive use. Although the aetiology of AGEP remains uncertain, recent data have reported
involvement of drug-specific T cells and interleukin (IL)-8 production. We characterized an adverse
reaction to pseudoephedrine both clinically and immunologically. Histological analysis of skin
biopsies confirmed the clinical entity as AGEP, while epicutaneous tests confirmed the specificity of
the reaction to the drug. Moreover, immunohistochemical studies showed a mononuclear infiltrate
consisting of activated memory T cells in addition to polymorphonuclear cells. Reverse
transcription-polymerase chain reaction revealed an increased expression of IL-8 in AGEP-
affected skin.
Key words: acute generalized exanthematous pustulosis, interleukin-8, lymphocytes,
pseudoephedrine, pustulosis
Acute generalized exanthematous pustulosis (AGEP) is
an uncommon skin disease involving sterile pustules
on an erythematous background. It is mainly caused
by drugs, particularly antibacterial drugs such as
aminopenicillins and macrolides, by acute infection
with enteroviruses, or by mercury.1 Positive skin patch
tests and lymphocyte transformation tests suggest
involvement of T cells in AGEP.2 Moreover, a high
expression of the potent neutrophil-attracting chemo-
kine interleukin (IL)-8 has been detected in keratino-
cytes and infiltrating mononuclear cells in positive
patch-test samples from patients with AGEP.2
Pseudoephedrine is a sympathomimetic drug widely
found in pharmacological preparations for the common
cold. Adverse reactions to sympathomimetic drugs are
rare despite extensive use. Nonpigmented fixed exan-
thema,3,4 and generalized scarlatiniform5 or eczema-
tous eruptions6 have been reported.
We describe a woman who presented with AGEP
after administration of pseudoephedrine. Patch testing
with pseudoephedrine and other sympathomimetic
drugs was performed to identify cross-reactivity. The
immunohistochemical study of the positive patch test
and analysis of cytokine profiles and lymphocyte
proliferation results are reported.
Case report
A 42-year-old woman with no relevant medical history
was referred because of a suspected adverse drug
reaction. Two months previously she had had an upper
airway infection, for which her physician prescribed
Vincigrip (Salvat Laboratory, Barcelona, Spain) con-
taining paracetamol, pseudoephedrine, chlorphenam-
ine and several excipients. Ten hours after the first dose
she developed fever above 38 �C and a pustular
eruption with erythema located on the face, trunk and
proximal extremities. She was admitted by the derma-
tologist to the emergency room where a skin biopsy was
performed and treatment was commenced with oralCorrespondence: Dr Teresa Bellon.
E-mail: [email protected]
British Journal of Dermatology 2004; 150: 139–142.
� 2004 British Association of Dermatologists 139

corticosteroids, with total recovery in 10 days. The
content of the superficial pustules was sterile and the
histopathological findings were spongiform superficial
pustules and papillary oedema with focal necrosis of
keratinocytes (not shown); a diagnosis of AGEP related
to drugs was made. As the patient had taken both
paracetamol and chlorphenamine since the reaction,
pseudoephedrine was suspected to be the culprit drug.
Materials and methods
Patch testing
Patch tests were performed at least 2 months after
recovery with the pharmacological preparation Vinci-
grip (paracetamol, pseudoephedrine, chlorphenamine
and excipients), pseudoephedrine and other sympath-
omimetic drugs (phenylephrine, ephedrine, epineph-
rine and norepinephrine) diluted to 20% and 50% in
petrolatum. The freshly prepared drug ⁄ petrolatum
mixtures were applied on the upper back in the patch
test plaster Leukotest (Beiersdorf, Hamburg, Germany).
Patch test reactions were read at 48 and 96 h and
scored according to the International Contact Derma-
titis Research Group.7
Immunohistochemistry
Punch biopsy specimens were fixed in 10% formalin,
routinely processed, paraffin-embedded and stained
with haematoxylin and eosin for standard histological
analysis. Immunostaining was performed in 5-lm
sections from the positive epicutaneous test reaction
for CD3, CD4, CD8, CD25, CD45RO and CD45RA using
a horseradish peroxidase-based detection technique
and EnVisionTM+ system (Dako Cytomation; Dako,
Glostrup, Denmark).
Reverse transcription-polymerase chain reaction
Sections of 5 lm from paraffin-embedded tissues were
cut with disposable blades, collected on glass slides,
deparaffinized with xylene, washed with ethanol, and
rehydrated in deionized water. The moist tissue was
scraped off the glass slides with a sterile blade. RNA
was extracted in 200 lL TriReagent� according to the
manufacturer’s instructions and reverse transcribed
with random primers and avian myeloblastosis virus
reverse transcriptase. IL-8 mRNA was amplified by
polymerase chain reaction (PCR) using primers 5¢-AAG
GAACCATCTCACTGTGTG-3¢ and 5¢-GGTGGAAAGGT
TTGGAGTATG-3¢. Human cutaneous T cell-attracting
chemokine (CTACK) transcripts were detected with
primers 5¢-CTGTACTCAGCTCTACCGAAAGC-3¢ and
5¢-GTGGATGCAGATGCTGCGTTG-3¢. One hundred
and eighty base pairs of the b2-microglobulin gene
were amplified as a loading control with the primers
5¢-CCAGCAGAGAATGGAAGGTC-3¢ and 5¢-CAGTGGG
GGTGAATTCAGTG-3¢.
Lymphocyte proliferation assays
Peripheral blood mononuclear cells (PBMC) were
isolated from heparinized blood by Ficoll–Hypaque
(Pharmacia, Uppsala, Sweden) density gradient cen-
trifugation. PBMC were seeded at 106 cells mL)1 in
triplicate in round-bottomed 96-well plates at a final
volume of 200 lL. The culture medium was RPMI plus
5% autologous serum and different concentrations of
drugs, ranging from 500 to 1 lg mL)1. The cultures
were incubated for 5 days at 37 �C in 5% CO2 and
1 lCi 3H-thymidine was added to each well 18 h prior
to cell harvesting. The cultures were harvested on to
glassfibre filters and 3H incorporation was estimated by
scintillation counting.
Phytohaemagglutinin and tetanus toxoid were used
as positive controls. The stimulation index (SI) was
calculated as the ratio between the mean values of
counts per minute in cultures with antigen and those
obtained without antigen. An SI > 2 was regarded as a
positive response.
Results
Patch testing with both the commercial preparation
Vincigrip and pseudoephedrine showed an intense
positive result at 48 h, with erythema and papules
that persisted for 96 h. However, the epicutaneous
tests with other sympathomimetic drugs were negative.
Patch tests were also performed on two atopic patients
and two healthy individuals as control subjects, with
negative responses in all cases. Oral challenge with
phenylephrine (7Æ5 mg) and ephedrine (5 mg) were
negative. The patient was also tested with subcuta-
neous epinephrine 1 ⁄ 1000 (0Æ3 mL), with a negative
response.
A punch biopsy specimen (4 mm) was obtained from
the positive epicutaneous test reaction with pseudo-
ephedrine. Histopathology showed subcorneal pustules,
papillary oedema, focal necrosis of keratinocytes and
the presence of subepidermal polymorphonuclear neu-
trophils with a perivascular infiltrate of mononuclear
1 4 0 M . A . P A D I A L et al.
� 2004 British Association of Dermatologists, British Journal of Dermatology, 150, 139–142
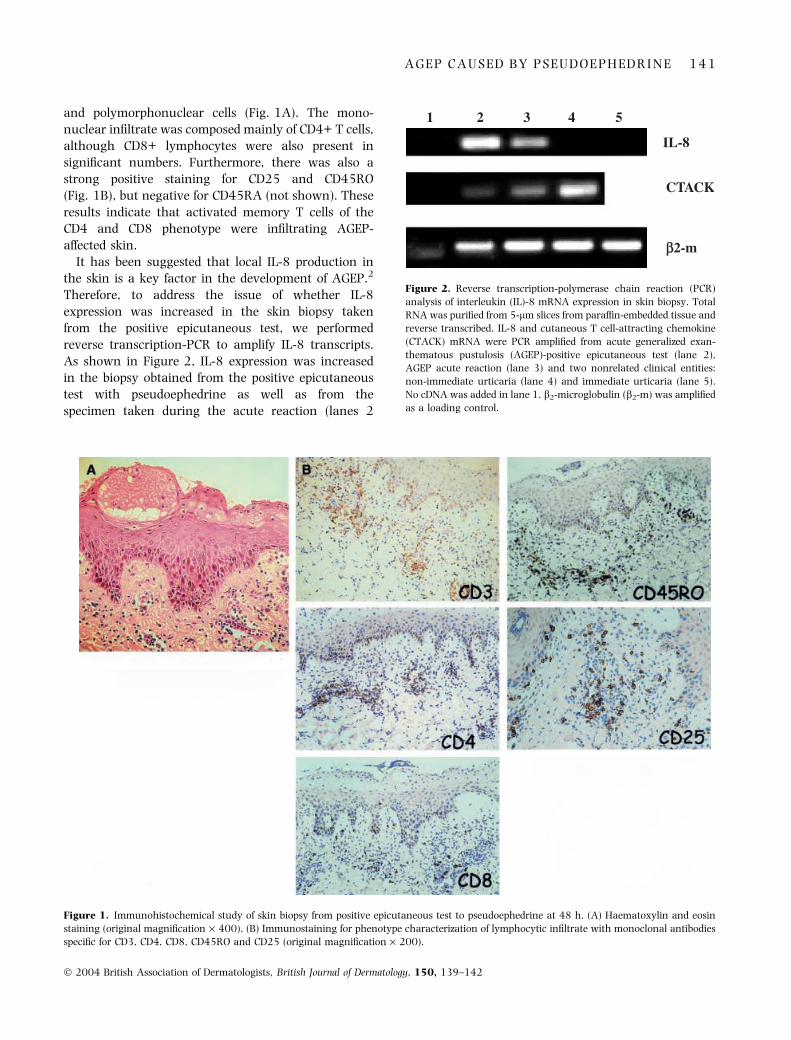
and polymorphonuclear cells (Fig. 1A). The mono-
nuclear infiltrate was composed mainly of CD4+ T cells,
although CD8+ lymphocytes were also present in
significant numbers. Furthermore, there was also a
strong positive staining for CD25 and CD45RO
(Fig. 1B), but negative for CD45RA (not shown). These
results indicate that activated memory T cells of the
CD4 and CD8 phenotype were infiltrating AGEP-
affected skin.
It has been suggested that local IL-8 production in
the skin is a key factor in the development of AGEP.2
Therefore, to address the issue of whether IL-8
expression was increased in the skin biopsy taken
from the positive epicutaneous test, we performed
reverse transcription-PCR to amplify IL-8 transcripts.
As shown in Figure 2, IL-8 expression was increased
in the biopsy obtained from the positive epicutaneous
test with pseudoephedrine as well as from the
specimen taken during the acute reaction (lanes 2
Figure 1. Immunohistochemical study of skin biopsy from positive epicutaneous test to pseudoephedrine at 48 h. (A) Haematoxylin and eosin
staining (original magnification · 400). (B) Immunostaining for phenotype characterization of lymphocytic infiltrate with monoclonal antibodies
specific for CD3, CD4, CD8, CD45RO and CD25 (original magnification · 200).
1 2 3 4 5
IL-8
CTACK
ββ2-m
Figure 2. Reverse transcription-polymerase chain reaction (PCR)
analysis of interleukin (IL)-8 mRNA expression in skin biopsy. Total
RNA was purified from 5-lm slices from paraffin-embedded tissue and
reverse transcribed. IL-8 and cutaneous T cell-attracting chemokine
(CTACK) mRNA were PCR amplified from acute generalized exan-
thematous pustulosis (AGEP)-positive epicutaneous test (lane 2),
AGEP acute reaction (lane 3) and two nonrelated clinical entities:
non-immediate urticaria (lane 4) and immediate urticaria (lane 5).
No cDNA was added in lane 1. b2-microglobulin (b2-m) was amplified
as a loading control.
A G E P C A U S E D B Y P S E U D O E P H E D R I N E 1 4 1
� 2004 British Association of Dermatologists, British Journal of Dermatology, 150, 139–142

and 3) in comparison with two samples obtained from
nonrelated clinical entities for which IL-8 mRNA was
not detected (lane 4, non-immediate urticaria; and lane
5, immediate urticaria). In contrast, expression of
CTACK, a chemokine constitutively expressed in kera-
tinocytes, was detected in all cases (lanes 2, 3 and 4).
Lymphocyte proliferation assays were performed in
which PBMC from the patient after resolution of the
disease were cultured in the presence of different doses
of pseudoephedrine and other sympathomimetic drugs.
After 5 days of culture no specific cell proliferation was
detected in response to pseudoephedrine or the different
drug analogues tested (not shown).
Discussion
Pseudoephedrine was the agent responsible for this
severe reaction in our patient, as confirmed by
clinical and patch test data. Histopathological findings
confirmed AGEP as the clinical entity involved.
Although occasionally the aetiology of AGEP appears
to be a viral infection or a hypersensitivity reaction to
mercury, most cases of AGEP (90%) have been
described in association with the intake of drugs,
such as aminopenicillins.8 There is only one previous
report of this unusual reaction due to pseudoephe-
drine, with a positive patch test.9 In our case the
similar histopathological traits found in the biopsy
specimen obtained after oral administration of pseu-
doephedrine and the positive patch test biopsy with
pseudoephedrine validate the reliability of patch
testing in this type of reaction, in agreement with
previous reports.2,10,11
Several studies indicate cross-reactivity between
pseudoephedrine and ephedrine, which have a very
close chemical structure derived from the phenylpro-
panolamine skeleton.12,13 However, in our patient we
were unable to demonstrate any cross-sensitivity to
other sympathomimetic drugs.
Recent studies have involved T cells in the aetio-
pathology of this clinical entity.2 Immunohistochemistry
of the lesions in the positive epicutaneous reaction
confirmed the presence of a perivascular T-cell infiltrate
composed mainly of proliferating activated memory
lymphocytes in addition to the polymorphonuclear
cells. Moreover, we confirmed the increase in the local
production of IL-8 (CXCL-8) in the skin, a chemokine
classically involved in the differentiation and recruit-
ment of neutrophils.
In spite of the presence of a considerable number of
CD25+ T cells in the cutaneous infiltrate, we detected
no positive proliferative response when PBMC from the
patient were cultured in the presence of several
concentrations of pseudoephedrine (not shown). In
contrast, Britschgi et al. reported a positive in vitro
lymphoproliferative response to the culprit drugs in
several cases of AGEP.2 This apparent disagreement
may be due to the sensitivity of the assay. It is possible
that the drug-specific lymphocytes in peripheral blood
are below the detection limit of our proliferation assay
and ⁄ or that pseudoephedrine unmasks a hidden cuta-
neous epitope; thus, infiltrating T cells would recognize
the specific antigen in the skin but not in the in vitro
assay. Further studies are needed to clarify this point.
Acknowledgments
This work was supported by grants FIS01 ⁄ -0014-01
and FIS PI021027. We thank Ian Johnstone for help
with the English language version of the manuscript.
References
1 Roujeau JC, Bioulac-Sage P, Bourseau C et al. Acute generalized
exanthematous pustulosis. Analysis of 63 cases. Arch Dermatol
1991; 127: 1333–8.
2 Britschgi M, Steiner UC, Schmid S et al. T-cell involvement in
drug-induced acute generalized exanthematous pustulosis. J Clin
Invest 2001; 107: 1433–41.
3 Anibarro B, Seoane FJ. Nonpigmenting fixed exanthema induced
by pseudoephedrine. Allergy 1998; 53: 902–3.
4 Vidal C, Prieto A, Perez-Carral C, Armisen M. Nonpigmenting
fixed drug eruption due to pseudoephedrine. Ann Allergy Asthma
Immunol 1998; 80: 309–10.
5 Taylor BJ, Duffil MB. Recurrent pseudo-scarlatina and allergy
to pseudoephedrine hydrochloride. Br J Dermatol 1998; 118:
827–9.
6 Tomb RR. Systemic contact dermatitis from pseudoephedrine.
Contact Dermatitis 1991; 24: 86–8.
7 Wilkinson DS. Terminology of contact dermatitis. Acta Derm
Venereol (Stockh) 1970; 50: 287–92.
8 Roujeau JC. Neutrophilic drug eruptions. Clin Dermatol 2000; 18:
331–7.
9 Assier-Bonnet H, Viguier M, Dubertret L et al. Severe adverse drug
reactions due to pseudoephedrine from over-the-counter medi-
cations. Contact Dermatitis 2002; 47: 165–82.
10 Pichler W, Yawalkar N, Schmid S, Helbling A. Pathogenesis of
drug-induced exanthems. Allergy 2002; 57: 884–93.
11 Barbaud A, Reichert-Penetrat S, Trechot P et al. The use of skin
testing in the investigation of cutaneous adverse drug reactions.
Br J Dermatol 1998; 139: 49–58.
12 Garcia Ortiz JC, Terron M, Bellido J. Nonpigmenting fixed exan-
thema from ephedrine and pseudoephedrine. Allergy 1997; 52:
229–30.
13 Moreno-Escobosa MC, de las Heras M, Figueredo E et al. Gener-
alized dermatitis due to pseudoephedrine. Allergy 2002; 57: 753.
1 4 2 M . A . P A D I A L et al.
� 2004 British Association of Dermatologists, British Journal of Dermatology, 150, 139–142