acute flaccid paralysis mbbs lecture
TRANSCRIPT

ACUTE FLACID PARALYSIS
Dr. Muhammad Sajjad Sabir MBBS , DCH , MCPS, FCPSAssist Prof of Paediatrics
ACUTE- Rapid in onset
FLACCIDPARALYSIS
ACUTEFLACCID-PARALYSIS
Droopingwithout spasticity
ACUTEFLACCIDPARALYSIS-Loss of ability to
move a body part
What is AFP?a clinical syndrome characterized by
Rapid onset of weakness including (less frequently) weakness of the muscles of respiration & swallowing
Progressing to maximum severity within several days to weeks
Sudden onset of weakness or paralysis over a period of 15 days in a patient aged less than 15 years age
Flaccid paralysis evolving over hours or a few days
suggests involvement of the lower motor neuron complex
DEFINITION
Anterior horn cells AHC (spinal cord) acute poliomyelitisacute transverse myelitisPeripheral Nervesroots: GBS (post-infectious)toxins: Diphteria, porphyriaN-M junction:botulinum toxin , tick toxinMetabolic: Periodic paralysisMuscular: myositis (rare)A lesion compressing the spinal cord must be ruled out
Syndromes Presenting as AFP (DD)
Most common
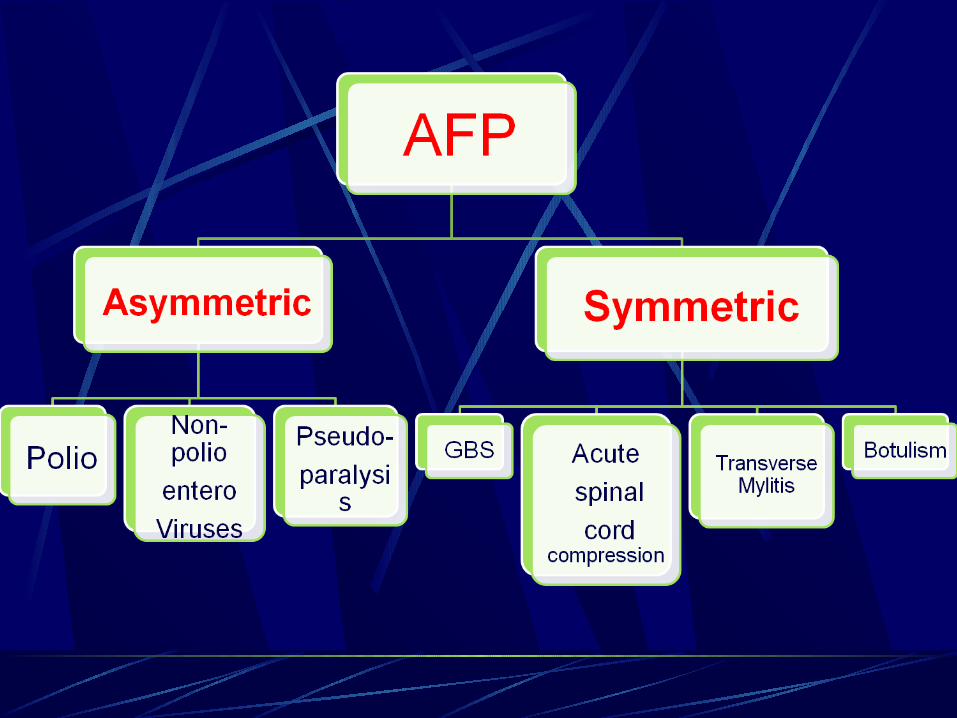
Poliomyelitis Guillain-Barre SyndromeTransverse myelitis
Acute Flaccid Paralysis(AFP)Differential diagnosis
AFP in <15yrs age child is
notify-able disease to WHO
Polio surveillance officers—all districts

Poliomyelitis
Poliomyelitis
Polio= gray matter
Myelitis= inflammation of the spinal cord
Most affects children < the age of 5
Global eradication in near future
Etiology Enterovirus (RNA)
Three serotypes: 1, 2, 3
Clinical Classification of Poliomyelitis
Asymptomatic infection (Inapparent) (90- 95%)
Abortive poliomyelitis (5%)
Non- paralytic poliomyelitis (aseptic meningitis) (1- 4%)
Paralytic poliomyelitis (0.1-1%) Spinal form Bulbar form Bulbospinal form Encephalitic form
Poliovirus infections may follow one of several courses
Paralytic poliomyelitis
Prodromal period Preparalytic period Paralytic period Convalescent period Sequela period
Commonly known as PolioOnly 1/1,000 to 1/100 (0.1% to 1%) infected individuals develop paralytic disease
Preparalytic period
High fever Cutaneous hyperesthesia or paresthesia in the
extremities Muscular pain is common Muscles are tender even to gentle palpation Severe headache & vomiting Lethargy Signs of meningeal irritation
(neck stiffness, Kerning & Brudzinski signs positive)
Paralytic poliomyelitis
Weakness of one or more muscle groups (spinal or cranial)
Loose & Floppy Limbs, hypotonia-- Flaccid paralysis
Asymmetric paralysis
Paralysis is complete – fever normalizes
Weakness persists
Respiratory & vasomotor changes
Bladder & bowel dysfunction
Tendon reflexes are absent with paralysis.
Sensory defects do not occur in poliomyelitis
Paralytic poliomyelitis Paralytic period
Spinal type: most common
Paralysis of extremities (muscle groups ) leg > arm proximal > distal Asymmetric paralysis
Paralysis of diaphragmatic & intercostal
muscles affects respiratory movement
Paralysis of abdominal muscle -- stubborn constipation
Paralytic poliomyelitis
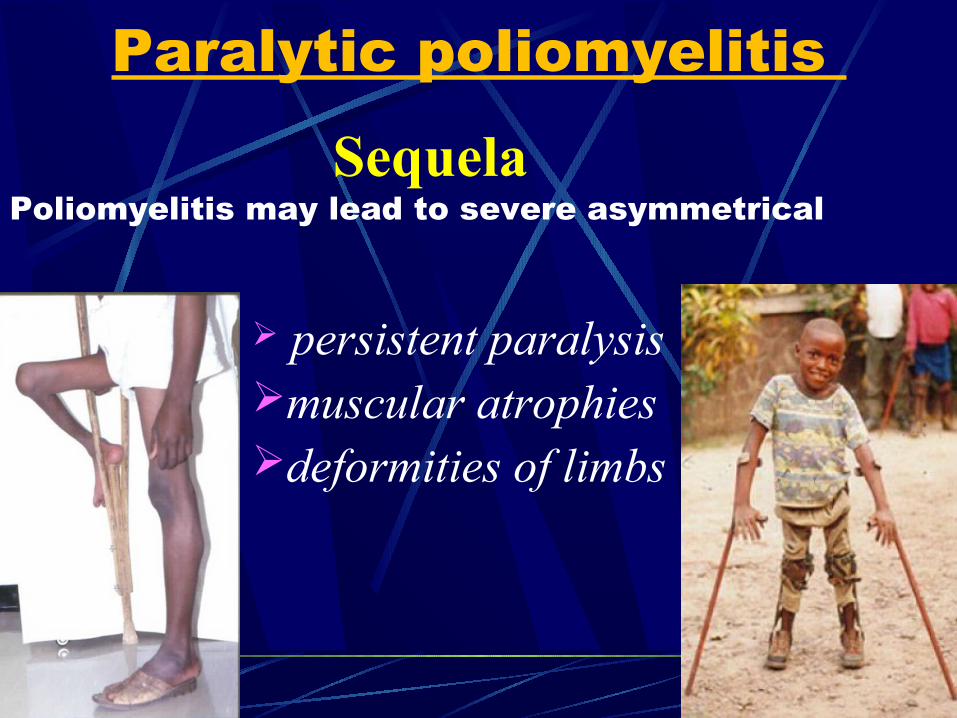
Sequela Poliomyelitis may lead to severe asymmetrical
persistent paralysismuscular atrophies deformities of limbs
Paralytic poliomyelitis
Diagnosis
WHO recommends diagnosis of poliomyelitis be confirmed by isolation and identification of poliovirus in the stool, with specific identification of wild-type and vaccine type strains
Polioviruses may be isolated from 80 to 90% of acutely ill patients
whereas less than 20% may yield virus within 3-4 wk after onset of paralysis
Identification of poliovirus in stool
Stool examination
Two samples 24 hr apart
Within 14 days of onset of paralysis
8-10 grams or thumb size
Collected in a clean wide mouth bottle – (plastic or glass) with screw cap
Sample stored below 8°C
No dessication or leakage till received at WHO Accredited Lab
Collection of sample
Laboratory FindingsCerebrospinal fluid
aseptic menigitis pleocytosis: 50~500×109/L protein: normal or slightly increase glucose and chloride; normal albuminocytologic dissociation
Serological TestsNeutralizing antibodies (IgG) Antibodies to C antigen (IgM) Anti-D antibodies

Management
Isolation
Rest in bed
Neutral positioning of the limbs
Good nursing
No I.M Injection or surgery
Relief of pain and spasm of muscles
Physiotherapy
Treatment symptomatic and supportive
Prevention
control of source of infection: isolation: 40 days after the onset of illness
protection of susceptible population- vaccination : attenuated live vaccine by
Oral -- OPV
killed virus vaccine Injectable -- IPV
Guillain-Barre Syndrome (GBS)
Guillain-Barre Syndrome (GBS)
Post-infectious
acute, rapidly progressing
ascending
potentially fatal form of polyneuritis
involving mainly motor but sometimes also sensory and autonomic nervesalso known as: Acute inflammatory demyelinating polyneuropathy (AIDP)

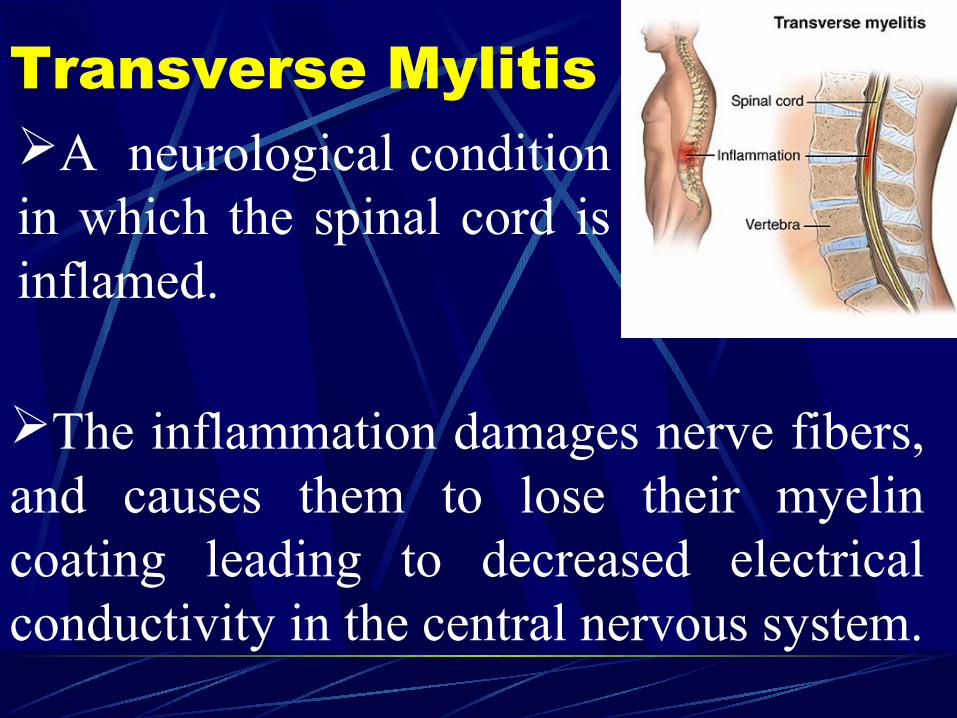
Transverse MylitisA neurological condition in which the spinal cord is inflamed.
The inflammation damages nerve fibers, and causes them to lose their myelin coating leading to decreased electrical conductivity in the central nervous system.
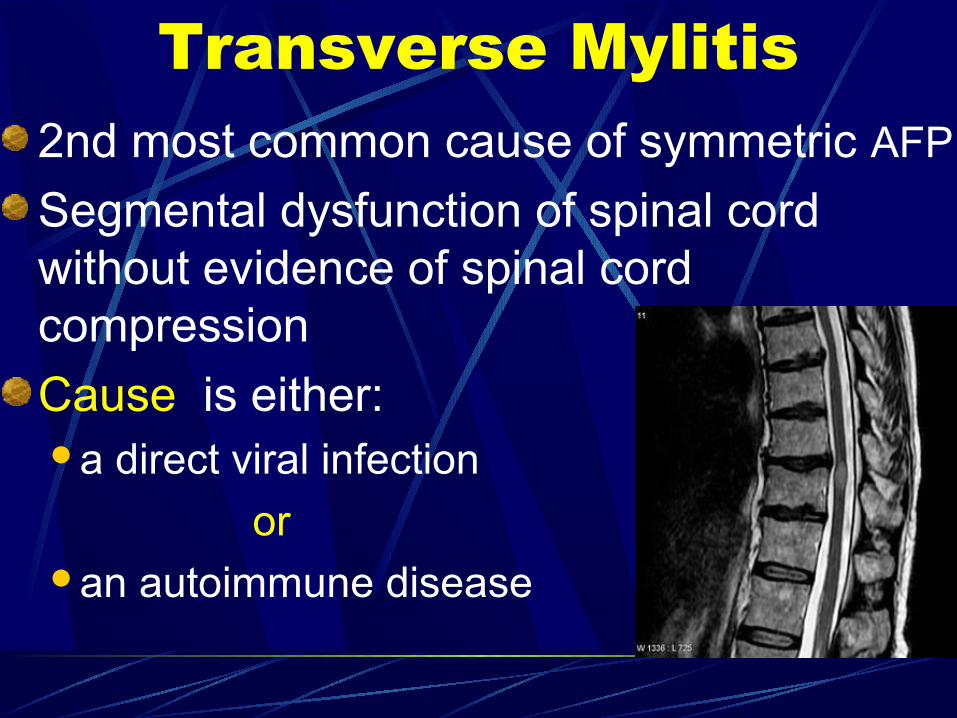
2nd most common cause of symmetric AFP
Segmental dysfunction of spinal cord without evidence of spinal cord compression
Cause is either:a direct viral infection
or an autoimmune disease
Transverse Mylitis
Transverse MylitisParalysis usually affect only Lower Limbs (Paraplegia)
Rare above C-5→quadriplegia
Initially flaccid but gradual change to spasticity over few weeks
Sensory loss (with sensory level on the trunk) and
Autonomic disturbance (urinary retention and stool incontinence) usually present
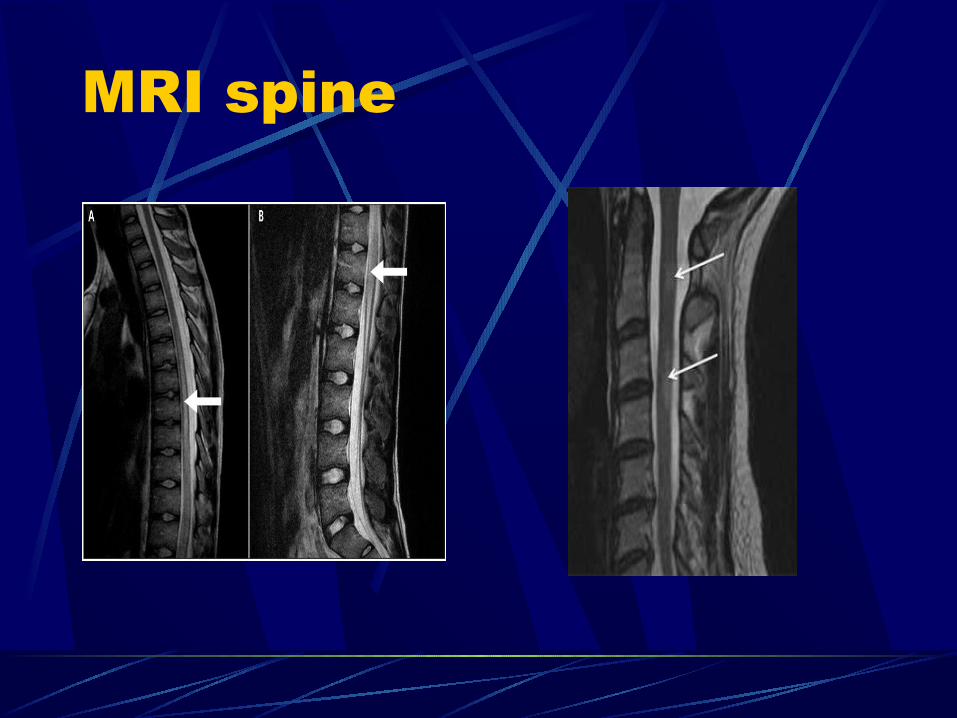
MRI spine
Treatment Intravenous SteroidsHigh-dose I.V methyl-prednisolone for 3-5 days
Plasma Electrophoresis
Prolonged course
Complete recovery in 60% of cases

Botulism
BotulismIt’s a toxic neuromuscular blockade caused by Clostridium botulinum (anaerobic gram positive)
According to the type of infection, there are 3 types Infant B. due to exposure to soil , honeyFood-borne B. due to ingestion improperly
home preserved foods containing the toxinsWound B. due to wound contamination with
the organism
All three types of botulism result in
symmetric
descending
Flaccid paralysis of motor and autonomic nerves always beginning with cranial nerves
These symptoms preceded by constipation (infant botulism)
If untreated - paralysis of respiratory → death
Botulism
Pseudoparalysis
PseudoparalysisNot a true paralysis
May follow Unrecognized traumaFractureSprainToxic synovitis of hip or knee Acute osteomylitis
Careful exam show focal tenderness
Usually painful limping gait
Neurological exam → normal

Acute spinal cord compression
Trauma to the backSpinal epidural abscessVascular anomalies of the cordSpinal cord tumors
Clinically difficult to differentiate from Transverse Mylitis
CT scan/ MRI spine: Sensitive Can show nature of obstruction
Acute spinal cord compression
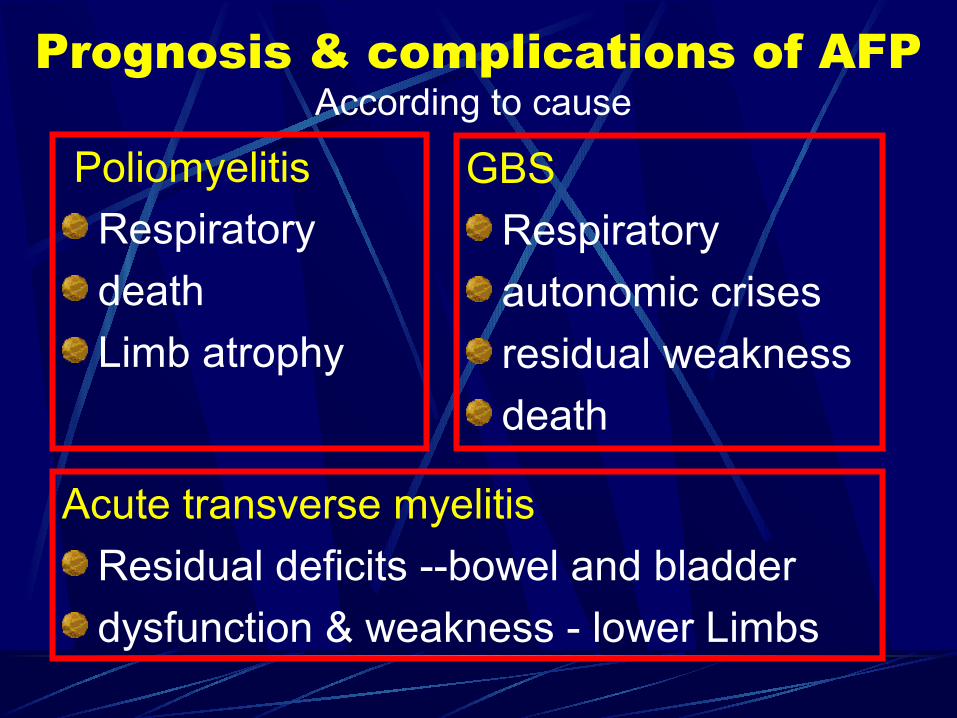
Prognosis & complications of AFPAccording to cause
Poliomyelitis
Respiratory
death
Limb atrophy
GBS
Respiratory
autonomic crises
residual weakness
death
Acute transverse myelitis
Residual deficits --bowel and bladder
dysfunction & weakness - lower Limbs
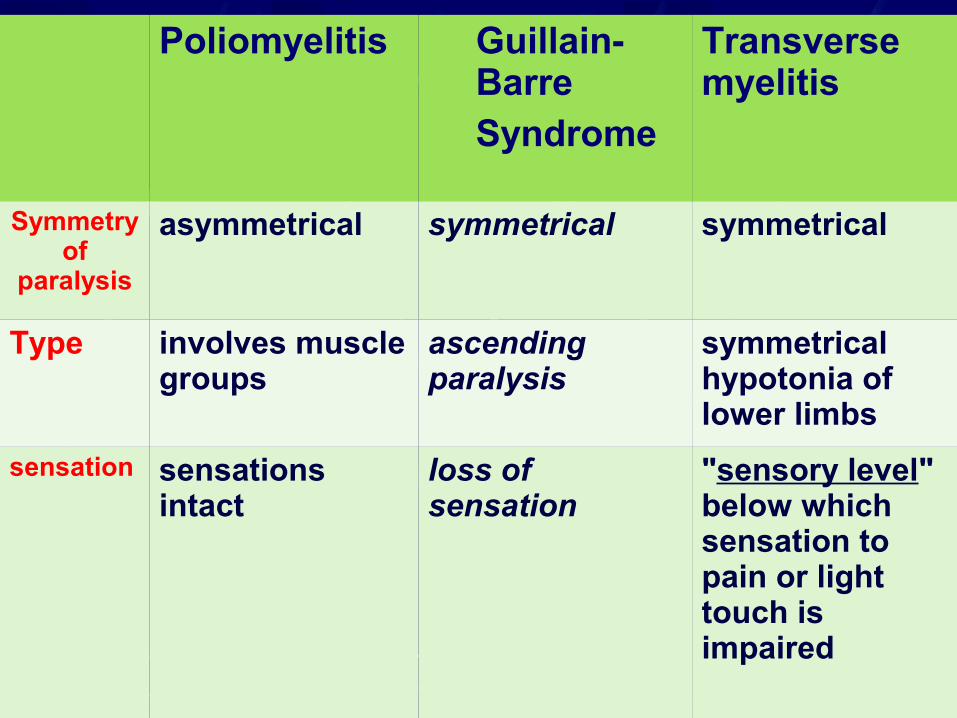
Poliomyelitis Guillain-Barre Syndrome
Transverse myelitis
Symmetry of
paralysis
asymmetrical symmetrical symmetrical
Type involves muscle groups
ascending paralysis
symmetrical hypotonia of lower limbs
sensation sensations intact
loss of sensation
"sensory level" below which sensation to pain or light touch is impaired
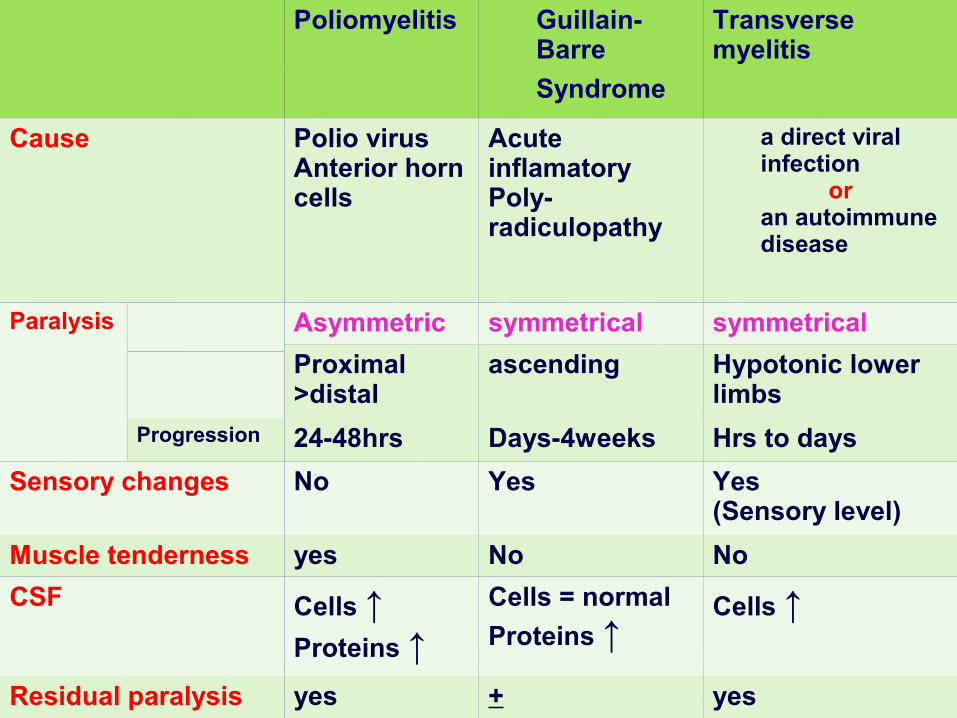
Poliomyelitis Guillain-Barre
Syndrome
Transverse myelitis
Cause Polio virusAnterior horn cells
Acute inflamatoryPoly-radiculopathy
a direct viral infection
or an autoimmune disease
Paralysis
Asymmetric symmetrical symmetrical
Proximal >distal
ascending Hypotonic lower limbs
Progression 24-48hrs Days-4weeks Hrs to days
Sensory changes No Yes Yes(Sensory level)
Muscle tenderness yes No No
CSF Cells ↑Proteins ↑
Cells = normal
Proteins ↑Cells ↑
Residual paralysis yes + yes
